Embed Size (px)
DESCRIPTION
iip
Citation preview

Compliance with Universal/StandardPrecautions among health care workersin rural north IndiaMichelle Kermode, PhD, MPH,a Damien Jolley, MSc, MSci,b Biangtung Langkham, DPH, MBBS,c Mathew SanthoshThomas, MD, MBBS,c Wendy Holmes, MBBS, MSc,d and Sandy M. Gifford, PhD, MA, MPHd
Melbourne, Australia, and New Delhi, India
Background: Universal Precautions (UPs) and more recently Standard Precautions have been widely promoted in high-incomecountries to protect health care workers (HCWs) from occupational exposure to blood and the consequent risk of infection withbloodborne pathogens. In low-income countries, the situation is very different: UPs are often practiced partially, if at all, therebyexposing the HCWs to unnecessary risk of infection. The aim of this study is to describe rural north Indian HCWs knowledge andunderstanding of UPs and identify predictors of compliance to target intervention programs appropriately.
Methods: A cross-sectional survey was undertaken, involving 266 HCWs (response rate, 87%) from 7 rural north Indian health caresettings. Information was gathered regarding compliance with UPs and a range of other relevant variables that potentially influencecompliance (eg, demographic information, perception of risk, knowledge of bloodborne pathogen transmission, perception ofsafety climate, and barriers to safe practice).
Results: Knowledge and understanding of UPs were partial, and UPs compliance was suboptimal, eg, only 32% wore eyeprotection when indicated, and 40% recapped needles at least sometimes. After controlling for confounding, compliance with UPswas associated with being in the job for a longer period, knowledge of bloodborne pathogen transmission, perceiving fewerbarriers to safe practice and a strong commitment to workplace safety climate.
Conclusion: Interventions to improve UPs compliance among HCWs in rural north India need to address not only their knowledgeand understanding but also the safety climate created by the organizations that employ them. (Am J Infect Control 2005;33:27-33.)
Health care workers (HCWs) are potentially exposedto blood in the course of their work and therefore are atrisk of infection with bloodborne pathogens, includinghuman immunodeficiency virus (HIV), hepatitis C virus
From the Australian International Health Institute, School of PopulationHealth, University of Melbourne, Melbourne, Victoria, Australiaa;Monash Institute of Health Services Research, Monash University,Melbourne, Victoria, Australiab; Emmanuel Hospital Association, NewDelhi, Indiac; and Burnet Institute, Melbourne, Victoria, Australia.d
Reprint requests: Michelle Kermode, MPH, NHMRC Public HealthPost-doctoral Fellow, Australian International Health Institute, Schoolof Population Health, University of Melbourne, Level 5/207 Bouverie St,Melbourne, Victoria 3010, Australia. E-mail: [email protected].
At the time of undertaking this research Michelle Kermode was therecipient of a Public Health Postgraduate Research scholarship from theAustralian National Health and Medical Research Council (NHMRC)and a full-time PhD candidate at the School of Health Sciences, DeakinUniversity, Melbourne, Australia.
0196-6553/$30.00
Copyright ª 2005 by the Association for Professionals in InfectionControl and Epidemiology, Inc.
doi:10.1016/j.ajic.2004.07.014
(HCV), and hepatitis B virus (HBV). Exposure to bloodcan occur through a percutaneous injury (needlestickor other sharps injury), a mucocutaneous incident(splash of blood or blood-containing fluids into theeyes, nose, or mouth), or blood contact with nonintactskin. WHO estimates that, among the 35 million healthcareworkers worldwide, approximately 3million expe-rience percutaneous exposure to bloodborne viruseseach year (2 million HBV, 900,000 HCV, and 300,000HIV).1 These injuries are estimated to result in 16,000hepatitis C, 66,000 hepatitis B, and 200 to 5000 HIVinfections. More than 90% of these infections are oc-curring in low-income countries, and most are pre-ventable.1*
Awareness that HCWs are at risk of occupationalinfection with bloodborne pathogens grew during the1970s when an increasing number of HCWs becameinfected with HBV and was further heightened in the
*Low- and high-income countries are those classified as such by the WorldBank on the basis of their 1999 GNP per capita. Low-income countries havea GNP per capita of # US $775, and include most of Africa, the Indiansubcontinent, some Southeast Asian countries, and Mongolia. High-incomecountries have a GNP per capita of $ US $9266 and include NorthAmerica, Western Europe, Japan, and Australia.
27

28 Vol. 33 No. 1 Kermode et al
Table 1. Health care settings participating in the survey
Hospital State Bed capacity* Specialist services
No. questionnaires
distributed
No. questionnaires
completed (%)
1 Uttaranchal 35 Surgery, obstetrics and gynecology, pediatrics,
ophthalmology, community health, dental
16 16 (100)
2 Uttaranchal 115 Surgery, pediatrics, orthopedics, obstetrics
and gynecology, community health
59 50 (85)
3 Uttar Pradesh 40 Surgery, obstetrics and gynecology 12 12 (100)
4 Jharkhandy 100 Surgery, obstetrics and gynecology, ophthalmology,
community health
39 35 (90)
5 Assamy 70 Surgery, obstetrics and gynecology, orthopedics,
urology, community health
67 54 (81)
6 Chattisgarh 76 Surgery, obstetrics and gynecology, community health,
infectious diseases, orthopedics ophthalmology,
30 25 (83)
7 Madhya Pradeshy 100 Surgery, obstetrics and gynecology, ophthalmology,
dermatology/leprosy, community health, dental
84 74 (88)
Total 307 266 (87)
*Hospitals were not always operating at full capacity.yHospitals with student nurses.
1980s with the onset of the HIV epidemic. In responseto these events, practice guidelines to enhance HCWsafety by minimizing the likelihood of exposure toblood, needles, and sharps were developed and imple-mented. These initiatives emerged predominantly inthe United States but were rapidly adopted and mod-ified for use in other high-income countries. The con-tent and labelling of the guidelines have varied overtime. During the late 1980s and early 1990s, they wereknown as Universal Precautions or Body SubstanceIsolation, but the most recent incarnation is StandardPrecautions.2*
Although the results from studies evaluating theeffectiveness of Universal Precautions (UPs) have beenmixed, it is clear that UPs reduce the extent to whichHCWs are exposed to the blood of others, and, pre-sumably, this in turn reduces their risk of occupationalinfection with bloodborne pathogens.3-5 Although UPshave been routinely practiced in high-income coun-tries for a long time, full compliance has been difficultto achieve. Noncompliance has been associated witha range of factors, including lack of knowledge,6,7
interference with work skills,8,9 risk perception,6,9 con-flict of interest,6,7 not wanting to offend patients,10 lackof equipment9,11 and time,8,9 uncomfortable personalprotective equipment (PPE),8 inconvenience,11 workstress,7 and perceiving a weak organizational commit-ment to safety climate.6,7
*Although the term Standard Precautions has superseded the term UniversalPrecautions in much of the western world, Universal Precautions is preferredin this paper because it is the term most familiar to HCWs in low-incomecountries and is still being used by the World Health Organization and theInternational Council of Nurses. In this paper, Universal Precautions refers tothe system of practices designed to protect patients and staff fromnosocomial infection with a range of pathogens including bloodbornepathogens.
In contrast to the situation in high-income countries,the occupational safety of HCWs in low-income coun-tries remains a neglected issue, even though they areprobably at greater risk of infection with bloodbornepathogens because of higher disease prevalenceamong the patient populations.12 In low-income-country health care settings, UPs tend to be practicedselectively (ie, when a patient is known to be infectedwith a bloodborne pathogen) rather than universally,if they are practiced at all. Awareness of the risksassociated with occupational exposure to blood isoften lacking, supplies of PPE are inadequate, andorganizational support for safe practices is limited.12,13
The aim of this study is to describe the knowledge andunderstanding of UPs among HCWs in rural north Indiaand identify predictors of compliance to target inter-vention programs appropriately.
METHODS
A cross-sectional survey of HCWs was conducted in7 rural north Indian health care settings (hospitals withattached community health projects) during late 2002.All health care institutions participating in the surveyare administered by a single, Indian nongovernmentalorganization, which provides health care and otherservices to the rural poor and is committed tomaximizing the quality of care provided, despitesubstantial resource constraints. The characteristicsof the health care settings are summarized in Table 1.
The objectives of the survey were to assess theextent of occupational blood exposure among ruralnorth Indian HCWs; identify factors associated withoccupational blood exposure; quantify the risk ofoccupational infection with bloodborne pathogens;assess HCWs compliance with UPs; and identify factors

Kermode et al February 2005 29
Table 2. Proportion providing a correct response to items pertaining to knowledge and understanding of UniversalPrecautions
Item N % Correct
1. I have a good understanding of how to apply Universal Precautions in my work. 249 87.6
2. Universal Precautions is the same as barrier nursing. 245 11.8
3. Universal Precautions are an effective way to protect doctors, nurses and other HCWs from
infection with bloodborne viruses eg, HIV/AIDS
248 94.8
4. We need to protect ourselves against exposure to blood only if the patient has an infectious disease such as HIV/AIDS. 248 52.0
5. It is not practical to treat the blood of all patients as potentially infectious. 247 50.2
6. Routinely testing all surgical and obstetric patients for HIV is a part of Universal Precautions. 249 5.6
7. A mask should be worn for all procedures where blood and body fluids may splash. 250 96.4
8. Gloves should be worn for all procedures that may involve contact with blood and body fluids. 250 97.6
9. Eye protection should be worn for all procedures where blood and body fluids may splash. 253 95.3
10. It is safe to use the same pair of gloves for many patients. 253 90.1
11. Hands should always be washed after gloves are removed. 253 97.2
12. Hands should always be washed after every procedure that involves direct patient contact. 253 98.0
13. Used needles should not be recapped. 252 83.3
14. Used needles and sharps should be disposed of separately from other waste. 253 98.4
15. Blood that has spilled on the ground (eg, in labor room) should be cleaned up immediately. 253 99.2
16. Universal Precautions involve treating the blood and body fluids of all patients as potentially infectious. 249 88.4
associated with noncompliance. This paper reportsfindings related to the last 2 objectives (findings relatedto the first 3 objectives will be reported elsewhere3).
The survey involved self-administration of an anon-ymous written questionnaire. Participating HCWs wereasked to indicate using a 5-point Likert scale (never,rarely, sometimes, often or always), whether or not theyengaged in 1 of 12 behaviors related to the practice ofUPs. An overall compliance score was calculated byassigning a value ranging from 1 to 5 (according to theLikert responses) to each of the 12 items and summingthese values (the highest score possible was 60 and thehigher the score the more compliant the HCW). Thisquestionnaire has been used previously in surveys withU.S. HCWs and has been tested for internal consistencyand reliability.6
Participants were also asked about a range of otherfactors that potentially influence compliance withUPs, including the following: demographic factors,risk perception, knowledge and understanding of UPs,HIV/AIDS and nosocomial transmission, training inUPs, attitudes to caring for people with HIV/AIDS(PWAs), availability of PPE, job satisfaction, job stress,perception of safety climate, and perception of barriersto safe practice. Safety climate is the workers’ per-ception of safety in their workplace, which is pre-sumably mediated by the nature and extent of thesafety-related activities occurring in that workplace. Toassess HCWs perceptions of safety climate and barriersto safe practice, they were asked to agree or disagree(using a 5-point Likert scale) with various statements(see Tables 5 and 6).
The questionnaire was pilot tested in India andmade available in English and Hindi. All HCWs em-ployed by the surveyed health care settings and likely
to be in contact with blood, needles, and sharps wereinvited to participate in the survey, with the exceptionof first-year student nurses, who were excluded be-cause of a relative lack of clinical experience. Wardaides were also excluded because many of them havepoor literacy skills. The questionnaires were distrib-uted and collected in unmarked envelopes by one ofthe authors (M.K.), with the support of senior hospitalpersonnel. Those who did not wish to participate wereencouraged to return the questionnaire unanswered.The survey sample was not a probability sample andtherefore not strictly representative of all HCWs inrural north India, so the study findings should begeneralized with caution. Despite this caveat, it isprobable that the working conditions of these HCWsare similar to (or slightly better than) those of HCWs inother health care settings in the same regions.
The data were analyzed using SPSS version 11.5(SPSS Inc, Chicago, IL). The statistical tests used toassess the strength of association between variablesincluded x2, independent samples t test, 1-way ANOVA,and simple linear regression. Multiple regression anal-ysis (general linear modelling) was undertaken to iden-tify the predictors of compliance with UPs.
Ethics approval for the study was granted by theDeakin University Human Research Ethics Committee,and all potential respondents were clearly advised thatparticipation in the survey was voluntary and anony-mous.
RESULTS
Of the 307 questionnaires distributed, 87% werereturned completed (Table 1), 1.6% were returned notcompleted, and 11% were not returned. The average

30 Vol. 33 No. 1 Kermode et al
Table 3. Proportion reporting compliance with components of Universal Precautions
Item N % Compliant
1. I protect myself against the blood and body fluids of all patients, regardless of their diagnosis. 255 80.2
2. I put used needles and other sharp objects into the designated sharps container. 250 90.2
3. I wear gloves whenever there is a possibility of exposure to blood or other body fluids. 255 67.6
4. I wash my hands after removing disposable gloves. 255 93.4
5. I wear a waterproof apron whenever there is a possibility of blood or other body fluids splashing on my clothes. 252 53.9
6. I wear eye protection (goggles/glasses) whenever there is a possibility of blood or other body fluids splashing in my face. 254 32.4
7. I wear a mask whenever there is a possibility of blood or other body fluids splashing in my face. 253 58.7
8. I do not recap needles that have been contaminated with blood. 249 60.2
9. I dispose of all blood-contaminated items into the bag or bucket designated for disposal. 255 94.1
10. I take extra care when using scalpels, needles, razors, or other sharp objects. 252 91.4
11. I promptly wipe up all spills of blood and other body fluids. 250 87.1
12. I cover my broken skin before coming to work. 253 79.4
age of respondents was 30.5 years (range, 18-62 years;SD, 10.3), and the majority was female (77.9%). Theaverage duration of employment was 9.8 years (range,1-38 years; SD, 9.5). Slightly more than half (52.3%)chose to complete the questionnaire in English. Themajority of respondents were nurses (28.5% generalnurse midwives [GNMs], 14.1% auxiliary nurse mid-wives [ANMs], and 32.7% student nurses); 6.1% werelaboratory workers, 12.5% doctors, 1.1% dentists, and4.9% others (operating theatre and ophthalmic tech-nicians, dental assistants, multipurpose workers).
Knowledge and understanding of UniversalPrecautions
More than one tenth of the HCWs (12%) wereunfamiliar with the term ‘‘Universal Precautions,’’ andonly 36% had ever received any training in UPs.Although the HCWs had a good level of knowledgeregarding the practice of UPs, their understanding ofthe underlying principles was partial at best. Thefindings in relation to knowledge and understanding ofUPs are summarized in Table 2.
Compliance with Universal Precautions
Overall compliance with UPs was relatively poor.Only 11% of HCWs reported being compliant (often oralways) with all 12 items. Self-reported compliancewith some practices such as handwashing and wastedisposal was good, but compliance with several otherpractices such as the use of eye protection and notrecapping needles was poor (Table 3).
Compliance with UPs was significantly associatedwith a range of variables. Some hospitals were morecompliant than others (P , .01); student nurses anddoctors were more compliant than trained nurses andlaboratory workers (P, .01), as were those HCWs witha positive attitude to caring for PWAs (P , .05) andthose more satisfied with their job (P , .001).
Compliance was positively associated with length oftime on the job (P , .05), knowledge of occupationalbloodborne pathogen transmission (P = .001), knowl-edge of UPs (P , .001), availability of PPE (P , .001),and perception of safety climate (P , .001) and wasnegatively associated with the perception of barriers tosafe practice (P , .001). UPs compliance was notassociated with having received training in UPs.
After controlling for confounding, compliance withUPs was better among those HCWs who had been inthe job for a longer period of time, had a higher level ofknowledge regarding occupational transmission ofbloodborne pathogens, perceived fewer barriers toimplementation of UPs, and perceived a strong com-mitment to safety climate (Table 4). The R2 value was0.342, ie, this model accounted for 34% of the variancein the UPs compliance scores, which is a robustfinding. The results of the individual items contributingto the overall perception of barriers to safe practice andsafety climate are presented in Tables 5 and 6.
DISCUSSION
When interpreting the findings of this study,a number of limitations should be considered. Actualcompliance with UPs (as opposed to self-reportedcompliance) is probably lower than reported becauseHCWs tend to overestimate the extent to which theycomply with UPs in practice.9 Social desirability biascould well have influenced HCWs’ responses ina number of areas, including UPs compliance, attitudesto PWAs, perception of barriers to safe practice, andsafety climate. Achieving total Hindi/English equiva-lence when translating items in a long and detailedquestionnaire is a challenge, and this may havecompromised the validity of some responses. It wasnot possible to identify characteristics of the HCWswho failed to complete or return the questionnaire, soit was not possible to establish whether they were

Kermode et al February 2005 31
different in some important way from those who didreturn it. However, the response rate (87%) was veryhigh, and there is no obvious reason to suspect thatnonresponders were substantially different from re-sponders.
These findings suggest that rural north Indian HCWsunderstand the practice of UPs much better than theunderlying principles. Some aspects of UPs were wellunderstood by HCWs, especially the need to use PPE(masks, gloves, and eye protection), dispose of sharpswaste separately, promptly clean up blood spills, andhand wash. However, the fact that 17% of HCWsdisagreed with the statement that used needles shouldnot be recapped suggests that knowledge of sharpssafety is incomplete, although it is also possible thatrecapping needles (using a 1-handed technique) isa safer option in places with suboptimal sharpsdisposal systems. It is of concern that 88% agreedthat UPs are the same as barrier nursing, and 48%indicated that they need to protect themselves fromblood only if the patient has an infectious disease suchas HIV/AIDS. Half the survey respondents (50%) agreedthat it is not practical to treat the blood of all patients asinfectious, which may in part explain the selectiveapplication of UPs. However, these findings are some-what contradicted by the 88% who agreed that UPsinvolve treating all blood of all patients as poten-tially infectious. These HCWs appear to be ambiva-lent and possibly confused about the universal principleunderlying the practice of UPs. Strategies are neededto persuade rural north Indian HCWs that full compli-ance with UPs is warranted in their workplace.
The findings also demonstrate a low level of overallcompliance with UPs among rural north Indian HCWsbecause only 11% reported full compliance with allcomponents of UPs. It was encouraging to find thatmore than 90% of respondents reported that they werecompliant with safe disposal of used needles andsharps and other blood-contaminated items, washinghands after removing gloves, and taking extra carewhen handling used needles and sharps. However, it isof concern that 40% reported recapping needles atleast sometimes (compared with 27% of U.S. HCWs),6
given the strong association between needle recappingand percutaneous injury. Compliance with the need touse PPE was very poor both overall and relative tocompliance levels reported in a similar study of U.S.HCWs.6 Only 67% often or always wore gloves whenindicated (compared with 97% in the United States),59% masks (56% in the United States), 54% plasticaprons (62% in the United States), and 32% eye pro-tection (63% in the United States). It is possible that thisdifference in compliance with the need to use PPE isattributable, at least in part, to the relative availabilityof PPE in rural north Indian and US health care settings.
Multiple regression analysis was used to identifypredictors of compliance with UPs. Compliance wasbetter among those who had been in the job for alonger period of time, knew more about nosocomialbloodborne pathogen transmission, perceived fewerbarriers to compliance, and had a positive perceptionof the safety climate in their workplace. Studies fromthe United States have also consistently demonstrateda relationship between compliance with UPs andperceived safety climate6,7,14,15 and barriers to safepractices.14,15
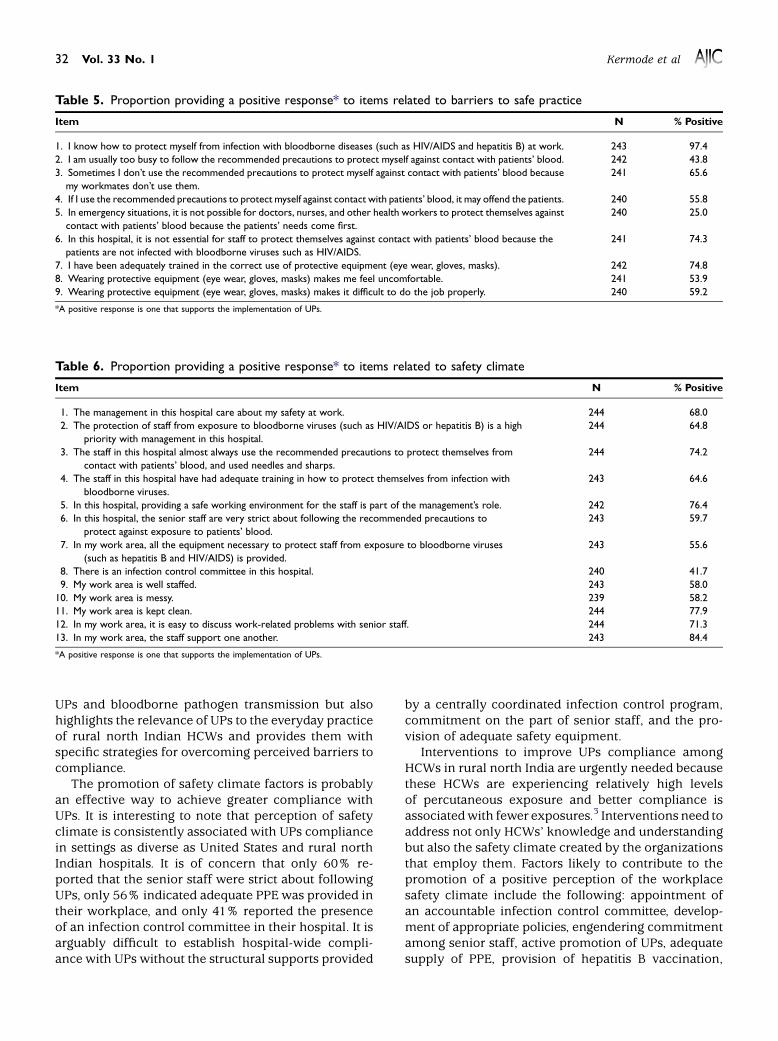
Perceived barriers to the implementation of UPsclearly influence HCWs’ ability and willingness tocomply with them in practice. Of concern is the factthat 75% agreed that it is not possible for HCWs toprotect themselves from blood exposure in an emer-gency situation; 56% were usually too busy to protectthemselves against contact with patients’ blood; 46%found wearing PPE to be uncomfortable; 44% felt thatpracticing UPsmay offend the patients; 41% found thatPPE impeded their work performance; 34% sometimesdid not use the recommended precautions becausetheir colleagues did not; 26% thought that it was notnecessary to protect themselves from patients’ bloodbecause the patients in their hospital were not infectedwith bloodborne pathogens; and 25% were notadequately trained in the correct use of PPE. Thesereasons for noncompliance overlapwith those reportedin studies among both American6-10 and Thai nurses.16
It was interesting to note that compliance was notassociated with having received UPs training. Thus,interventions to improve UPs compliance that focus onthe provision of information alone are unlikely to besuccessful. These findings suggest that training will bemost effective if it not only provides information about
Table 4. Predictors of compliance with UniversalPrecautions
95% Confi-
dence interval
Variable P value b Coefficient Lower Upper
Length of time in job (yr) .014 0.145 0.032 0.259
Knowledge of nosocomial
BBV transmission*
.004 1.073 0.343 1.803
Perception of safety climatey .026 0.135 0.016 0.253
Perception of barriers to
safe practicez.011 0.593 0.137 1.048
*The outcome measure was a score based on responses to 9 items: The highest
possible score was 9, and the higher the score the better the knowledge.yThe outcome measure was a score based on responses to 13 items: The highest
possible score was 65, and the higher the score the more positive the perception of
the organization’s safety climate.zThe outcome measure was a score based on responses to 9 items: the highest
possible score was 9 and the higher the score the fewer perceived barriers to the
implementation of UPs.
32 Vol. 33 No. 1 Kermode et al
Table 5. Proportion providing a positive response* to items related to barriers to safe practice
Item N % Positive
1. I know how to protect myself from infection with bloodborne diseases (such as HIV/AIDS and hepatitis B) at work. 243 97.4
2. I am usually too busy to follow the recommended precautions to protect myself against contact with patients’ blood. 242 43.8
3. Sometimes I don’t use the recommended precautions to protect myself against contact with patients’ blood because
my workmates don’t use them.
241 65.6
4. If I use the recommended precautions to protect myself against contact with patients’ blood, it may offend the patients. 240 55.8
5. In emergency situations, it is not possible for doctors, nurses, and other health workers to protect themselves against
contact with patients’ blood because the patients’ needs come first.
240 25.0
6. In this hospital, it is not essential for staff to protect themselves against contact with patients’ blood because the
patients are not infected with bloodborne viruses such as HIV/AIDS.
241 74.3
7. I have been adequately trained in the correct use of protective equipment (eye wear, gloves, masks). 242 74.8
8. Wearing protective equipment (eye wear, gloves, masks) makes me feel uncomfortable. 241 53.9
9. Wearing protective equipment (eye wear, gloves, masks) makes it difficult to do the job properly. 240 59.2
*A positive response is one that supports the implementation of UPs.
Table 6. Proportion providing a positive response* to items related to safety climate
Item N % Positive
1. The management in this hospital care about my safety at work. 244 68.0
2. The protection of staff from exposure to bloodborne viruses (such as HIV/AIDS or hepatitis B) is a high
priority with management in this hospital.
244 64.8
3. The staff in this hospital almost always use the recommended precautions to protect themselves from
contact with patients’ blood, and used needles and sharps.
244 74.2
4. The staff in this hospital have had adequate training in how to protect themselves from infection with
bloodborne viruses.
243 64.6
5. In this hospital, providing a safe working environment for the staff is part of the management’s role. 242 76.4
6. In this hospital, the senior staff are very strict about following the recommended precautions to
protect against exposure to patients’ blood.
243 59.7
7. In my work area, all the equipment necessary to protect staff from exposure to bloodborne viruses
(such as hepatitis B and HIV/AIDS) is provided.
243 55.6
8. There is an infection control committee in this hospital. 240 41.7
9. My work area is well staffed. 243 58.0
10. My work area is messy. 239 58.2
11. My work area is kept clean. 244 77.9
12. In my work area, it is easy to discuss work-related problems with senior staff. 244 71.3
13. In my work area, the staff support one another. 243 84.4
*A positive response is one that supports the implementation of UPs.
UPs and bloodborne pathogen transmission but alsohighlights the relevance of UPs to the everyday practiceof rural north Indian HCWs and provides them withspecific strategies for overcoming perceived barriers tocompliance.
The promotion of safety climate factors is probablyan effective way to achieve greater compliance withUPs. It is interesting to note that perception of safetyclimate is consistently associated with UPs compliancein settings as diverse as United States and rural northIndian hospitals. It is of concern that only 60% re-ported that the senior staff were strict about followingUPs, only 56% indicated adequate PPE was provided intheir workplace, and only 41% reported the presenceof an infection control committee in their hospital. It isarguably difficult to establish hospital-wide compli-ance with UPs without the structural supports provided
by a centrally coordinated infection control program,commitment on the part of senior staff, and the pro-vision of adequate safety equipment.
Interventions to improve UPs compliance amongHCWs in rural north India are urgently needed becausethese HCWs are experiencing relatively high levelsof percutaneous exposure and better compliance isassociatedwith fewer exposures.3 Interventions need toaddress not only HCWs’ knowledge and understandingbut also the safety climate created by the organizationsthat employ them. Factors likely to contribute to thepromotion of a positive perception of the workplacesafety climate include the following: appointment ofan accountable infection control committee, develop-ment of appropriate policies, engendering commitmentamong senior staff, active promotion of UPs, adequatesupply of PPE, provision of hepatitis B vaccination,

Kermode et al February 2005 33
delivery of ongoing training, and development of injurysurveillance systems.
The authors thank Associate Professor Nick Crofts (Turning Point Alcohol and DrugCentre, Melbourne, Victoria, Australia), Associate Professor Robyn Gershon(Columbia University, New York, NY), Dr. Vinod Shah (Emmanuel HospitalAssociation, New Delhi, India), the senior staff in all hospitals at which the surveywas undertaken, and the health care workers who participated in the survey.
References
1. World Health Report 2002: Reducing risks, promoting healthy life.
Available from: http://www.who.int/whr/en. Accessed October 2003.
2. Garner JS. Guideline for isolation precautions in hospitals: part I.
evolution of isolation practices. Am J Infect Control 1996;24:24-52.
3. Kermode M, Jolley D, Langkham B, Thomas MS, Crofts N.
Occupational exposure to blood and risk of bloodborne virus
infection among health care workers in rural north Indian health
care settings. Am J Infect Control 2005;33:34-41.
4. Beekmann SE, Vlahov D, Koziol DE, McShalley ED, Schmitt JM,
Henderson DK. Temporal association between implementation of
universal precautions and a sustained progressive decrease in
percutaneous exposures to blood. Clin Infect Dis 1994;18:562-9.
5. Kristensen MS, Wernberg NM, Anker-Moller E. Healthcare workers’
risk of contact with body fluids in a hospital: the effect of complying
with the universal precautions policy. Infect Control Hosp Epidemiol
1992;13:719-24.
6. Gershon R, Vlahov D, Felknor SA, Vesley D, Johnson PC, Declos GL,
et al. Compliance with universal precautions among health workers at
three regional hospitals. Am J Infect Control 1995;23:225-36.
7. Michalsen A, Delclos GL, Felknor SA, Davidson AL, Johnson PC,
Vesley D, et al. Compliance with universal precautions among
physicians. J Occup Environ Med 1997;39:130-7.
8. Kelen G, DiGiovanni TA, Celentano DA. Adherence to universal
(barrier) precautions during interventions on critically ill and injured
emergency department patients. J Acquir Immune Defic Syndr 1990;3:
987-94.
9. Henry K, Campbell S, Maki M. A comparison of observed and self-
reported compliance with universal precautions among emergency
department personnel at a Minnesota public teaching hospital:
implications for assessing infection control programs. Ann Emerg
Med 1992;21:940-6.
10. Ramsey PW, McConnell P, Palmer BH, Glen LL. Nurses’ compliance
with universal precautions before and after implementation of OSHA
regulations. Clin Nurs Spec 1996;10:234-9.
11. Nelsing S, Nielsen TL, Nielsen JO. Noncompliance with universal
precautions and the associated risk of mucocutaneous blood
exposure among Danish physicians. Infect Control Hosp Epidemiol
1997;18:692-8.
12. Sagoe-Moses C, Pearson RD, Perry J, Jagger J. Risks to health care
workers in developing countries. N Engl J Med 2001;345:538-41.
13. Huskins WC, O’Rourke EJ, Rhinehart E, Goldmann DA. Infection
control in countries with limited resources. In: Mayhall CG, editor.
Hospital epidemiology and infection control. Philadelphia: Lippincott,
Williams & Wilkins; 1999.
14. Gershon R, Karkashian CD, Grosch JW, Murphy LR, Escamilla-Cejudo
MD, Flanagan PA, et al. Hospital safety climate and its relationship with
safe work practices and workplace exposure incidents. Am J Infect
Control 2000;28:211-21.
15. DeJoy DM, Murphy LR, Gershon RM. The influence of employee,
job/task, and organizational factors on adherence to universal
precautions among nurses. Int J Ind Ergon 1995;16:43-55.
16. Picheansathian W. Compliance with universal precautions by emer-
gency room nurses at Maharaj Nakorn Chiang Mai Hospital. J Med
Assoc Thai 1995;78(Suppl 2):S118-22.





























