Embed Size (px)
Citation preview

KIDNEY BIOPSY:
INDICATIONS AND TECHNIQUE
Belen Ponte
Cheffe de clinique scientifique
Service de Néphrologie - HUG

PLAN
History
Indications and contraindications
Percutanerous Technique: preparationand step by step
Complications
Other techniques

Some history
1924: Jungmann report 1st pathological result of a biopsy
taken during an abdominal operation
1943: Castelman report large series of surgical biopsies
taken during lumbar sympathectomy for hypertension
1944: Alwall did 13 percutaneous biopsies but stop after 1
patient died
1949: Iversen used systematically percutaneous biopsy,
but with patient sitted

Before biopsy:
Urine culture,
coagulation study
Nitrogen products
Blood type + Xmatch
IV pyelogram
Phenolsufonphtalein

Indications: native kidney
Diagnosis Glomerular hematuria and/or proteinuria
Nephritic or nephrotic syndrome
Acute kidney injury of unknown origin
Rapidly progressive glomerulonephritis
Chronic kidney disease
Immunological or paraneoplasic diseases with kidenyinvolvement
Control response to therapy

Primary graft non-function
Proteinuria or glomerular hematuria of unknown origin
Acute kidney injury of unknown origin
Decrease in renal function of unknown origin
No response to antirejection therapy
Protocol biopies (no clear recommandation)
Indications: transplant kidney
Ahmad. Sem Interv Radiol 2004
Racusen et al. CJASN 2006

Contraindications
Relative:
Small kidneys, solitary kidney
Multiple cysts, Renal mass
Hydronephrosis, infection
Uncontrolled hypertension
Pregnancy
Absolute:
Bleeding diathesis
Patient not collaborative

Preparation and control….
Previous us showing 2 kidneys of normal size
BP controlled <140/90. Medication taken as usual.
Hb >100g/l. Blood type and crossmatch (in some centers).
Coagulation and platelets normals
Stop anticoagulation. No anti-aggregants or AINS >5 days
Sterile urine
Signed inform consent
Peripheric venous access. Temesta.
Surveillance 4-6h (transplant) or 12h-overnight (native): BP, FC
every 30min for 2h, then 1x/h for 4h. Check color of urine.

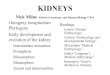
Technique: percutaneous
For native kidneys: Patient lying face down
Localise lower inferior pole of the left kidney with us
Stop breathing when punction (inspirium)
For transplant kidneys: Patient lying back
Localise upper pole of transplant kidney with us
Check with doppler the position of ureter and arteries!

Technique : position

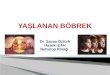
Step by step
16-18 Gauge

1. 2. 3.

With guiding device

Transport in NaCl
3 fragments
4.

Images pbr: mo, immuno, me

Biopsy sampling
95% CI
Madaio. Kint 1990

Complications
Microhematuria 90-100%
Pain 12-18%
Macrohematuria 2-10%
Relevant hematoma 2-7.8%
Need of transfusion 0.4-6%
AV fistula 5-10%
Other tissue lesion <5%
Surgical Intervention
Nephrectomy
<0.2%
1/2000-1/5000
Death 0.1%
Whitthier. JASN 2012.
Tondel. CJASN 2012
Chung. BMC Nephrology 2014
Simard. Nephron Extra 2014

Tondel. CJASN 2012

Risk factors
Simard. Nephron Extra 2014
Tondel. CJASN 2012

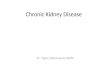
Other techniques
Stiles et al. AJKD 2000
Thompson et al. .AJKD 2004

Right kidney more suitable
Transjugular route

Techniques and complications
Stiles et al. AJKD 2000

CONCLUSIONS
Is the biopsy indicated?
Are they any contraindications?
If yes, which is the safest way for diagnosis?
Minimise the risks
Be careful, Be careful, Be careful…