Embed Size (px)
Citation preview

La terapia farmacologica nellaSclerosi Multipla
Enrico Montanari
Sclerosi Multipla:Prospettive terapeutiche,Farmaco sostenibilità e Aspettative del paziente
Ancona 16 Marzo 2018
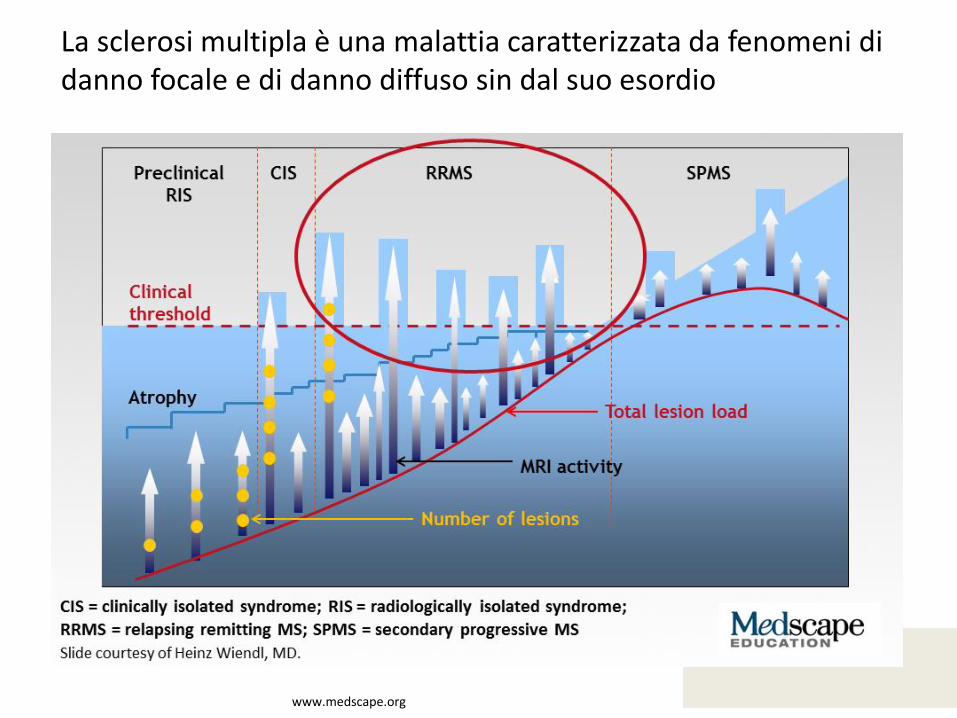
La sclerosi multipla è una malattia caratterizzata da fenomeni di danno focale e di danno diffuso sin dal suo esordio
www.medscape.org
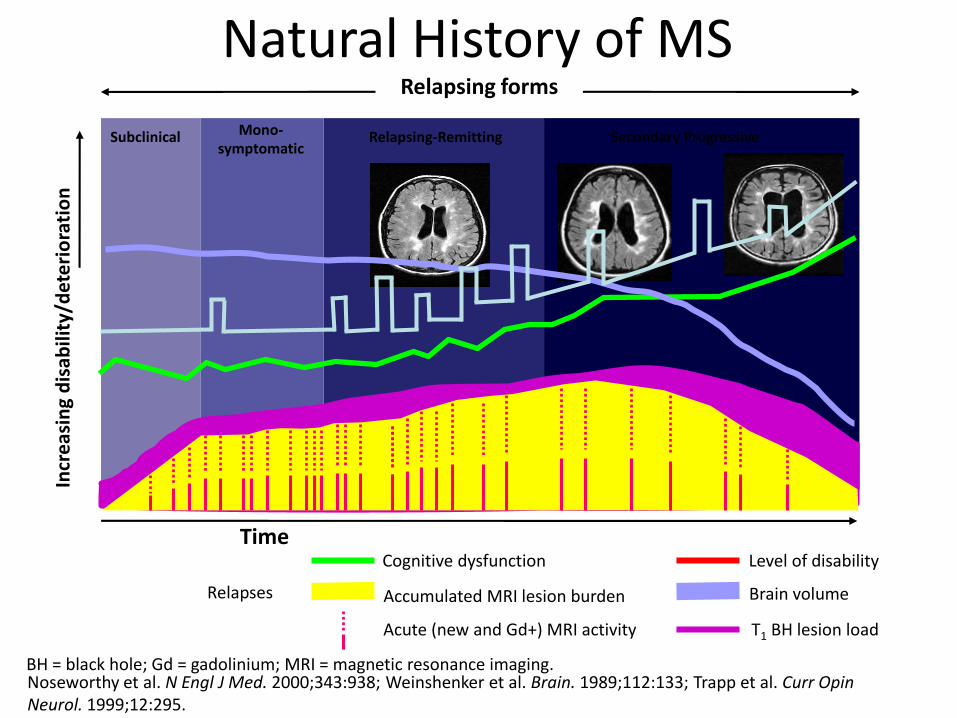
Natural History of MS
BH = black hole; Gd = gadolinium; MRI = magnetic resonance imaging.
Relapsing forms
Time
Incr
eas
ing
dis
abili
ty/d
ete
rio
rati
on
Level of disability
Brain volume
T1 BH lesion load
Accumulated MRI lesion burden
Acute (new and Gd+) MRI activity
Cognitive dysfunction
Subclinical Mono-symptomatic
Relapsing-Remitting Secondary Progressive
Relapses
Noseworthy et al. N Engl J Med. 2000;343:938; Weinshenker et al. Brain. 1989;112:133; Trapp et al. Curr Opin Neurol. 1999;12:295.
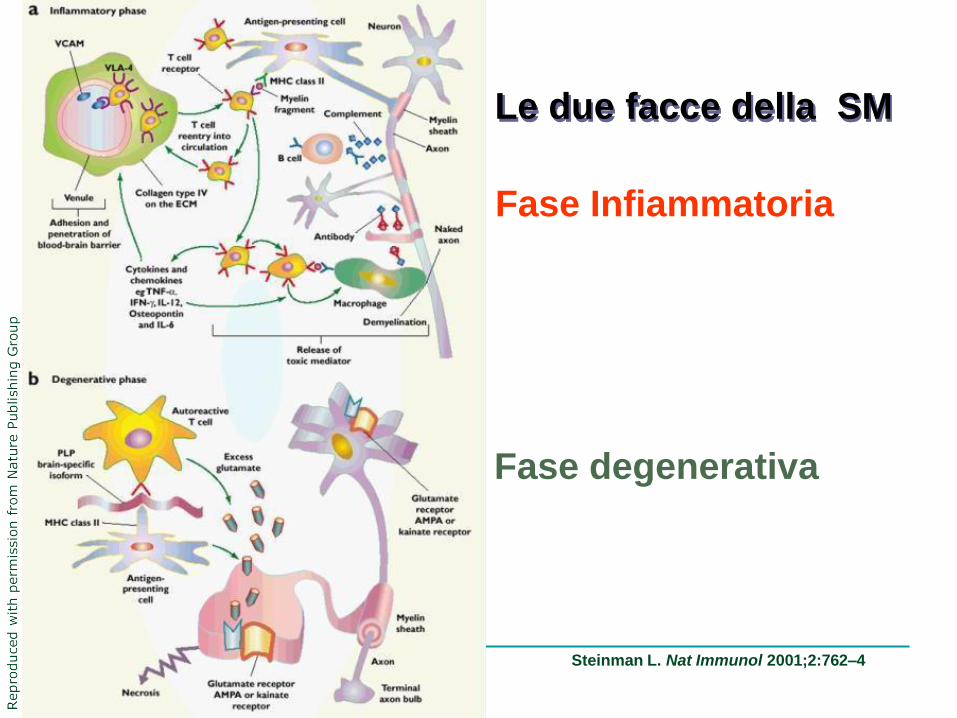
Steinman L. Nat Immunol 2001;2:762–4
Fase Infiammatoria
Fase degenerativa
Le due facce della SM
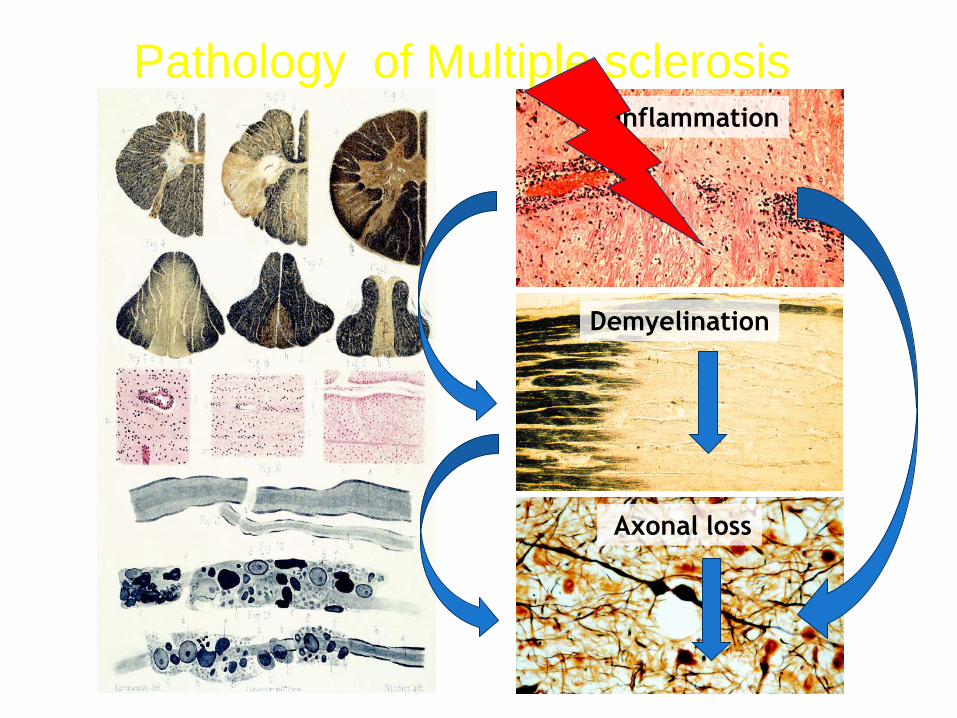
Pathology of Multiple sclerosisInflammation
Demyelination
Axonal loss
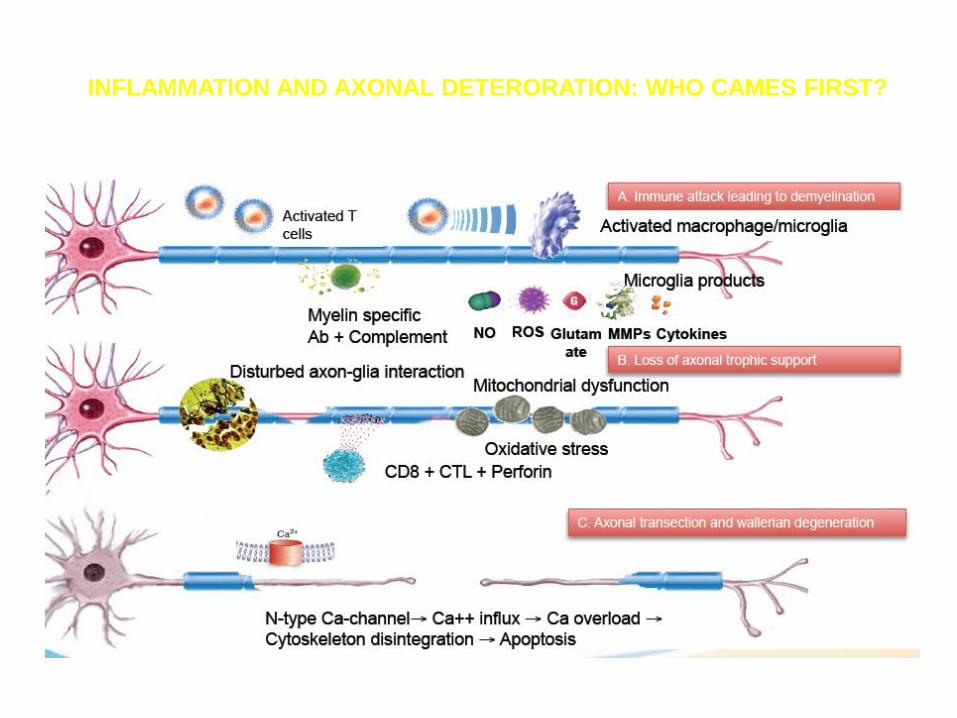
INFLAMMATION AND AXONAL DETERORATION: WHO CAMES FIRST?
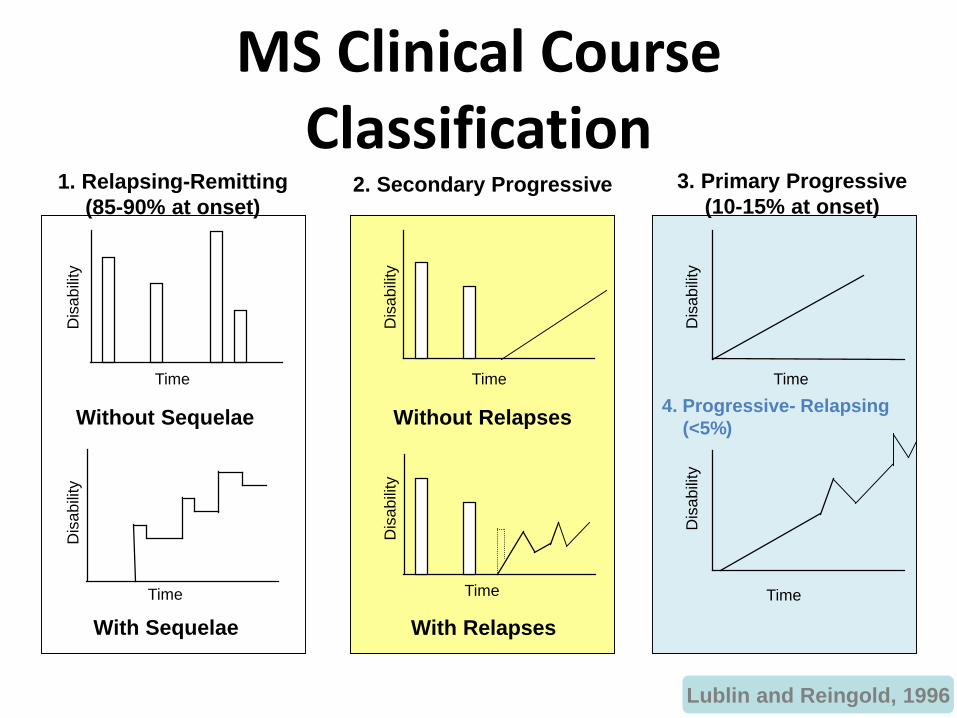
MS Clinical Course Classification
Time
Dis
ab
ility
Time
Dis
ab
ility
Without Sequelae
With Sequelae
Time
Dis
ab
ility
Time
Dis
ab
ility
4. Progressive- Relapsing
(<5%)
TimeD
isa
bili
ty
Time
Dis
ab
ility
Without Relapses
With Relapses
1. Relapsing-Remitting
(85-90% at onset)2. Secondary Progressive 3. Primary Progressive
(10-15% at onset)
Lublin and Reingold, 1996
Early Clinical Predictors and Progression of Disability in MS
• Clinical factors that can be assessed early in the disease are strong predictors of the time from onset of MS to the onset of irreversible disability
• Some factors are fixed
– Gender
– Age
– Initial symptoms and course of disease
– Degree of recovery from the first relapse of the disease
• Some factors can be influenced by therapeutic intervention
– Time from onset of MS to the second neurological episode
– Number of relapses during the first 5 years of the disease
– Time from onset of MS to the assignment of a score of 4 on the Kurtzke Disability Status Scale
• Once a score of 4 has been reached, these variables are no longer predictive of the time course of the subsequent disability progression
Confavreux et al. Brain. 2003;126:751.
Clinical and Neurologic Measures of MS Disease Activity and Progression
• Disease activity
– Gd+ lesions
– New or enlarging T2 lesions
– Relapses
• Disease progression
– T2 lesion volume
– T1/black holes
– Brain atrophy
– Cognitive disability
– Physical disability
Importance of prognosis
• For the patients: to be informed about theirprospect and about the risk/benefit ratio priorto start a treatment
• For the neurologist: to need elements to support a therapeutic decision
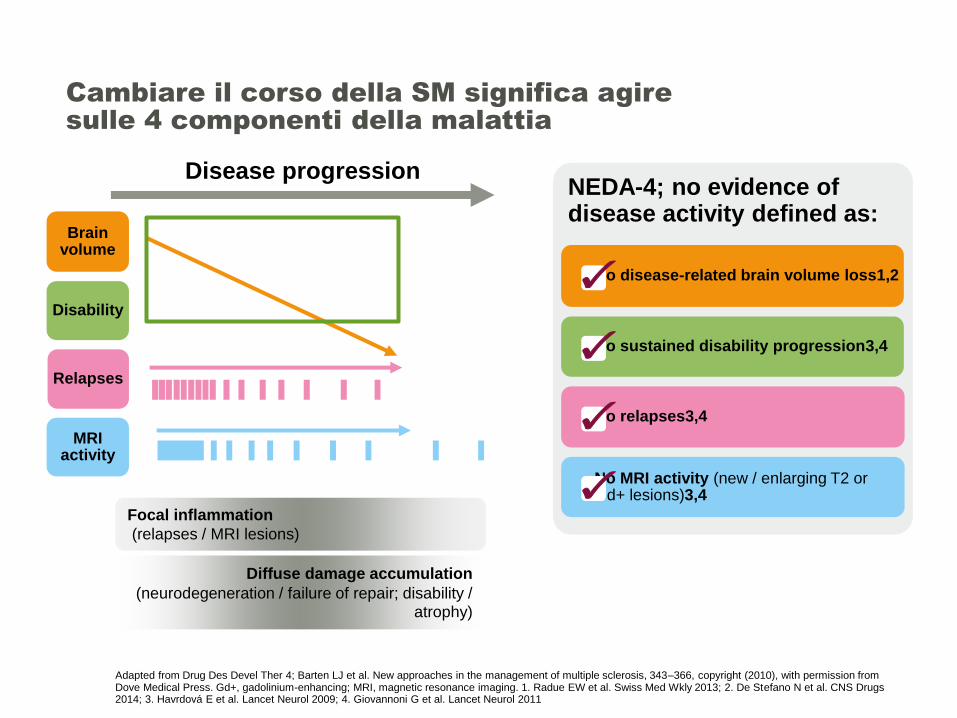
Adapted from Drug Des Devel Ther 4; Barten LJ et al. New approaches in the management of multiple sclerosis, 343–366, copyright (2010), with permission from Dove Medical Press. Gd+, gadolinium-enhancing; MRI, magnetic resonance imaging. 1. Radue EW et al. Swiss Med Wkly 2013; 2. De Stefano N et al. CNS Drugs 2014; 3. Havrdová E et al. Lancet Neurol 2009; 4. Giovannoni G et al. Lancet Neurol 2011
Cambiare il corso della SM significa agire sulle 4 componenti della malattia
Disease progression
Disability
Brain volume
Relapses
MRI activity
Focal inflammation
(relapses / MRI lesions)
Diffuse damage accumulation
(neurodegeneration / failure of repair; disability / atrophy)
NEDA-4; no evidence of disease activity defined as:
No disease-related brain volume loss1,2
No sustained disability progression3,4
No MRI activity (new / enlarging T2 or Gd+ lesions)3,4
No relapses3,4
✓
✓
✓
✓
12
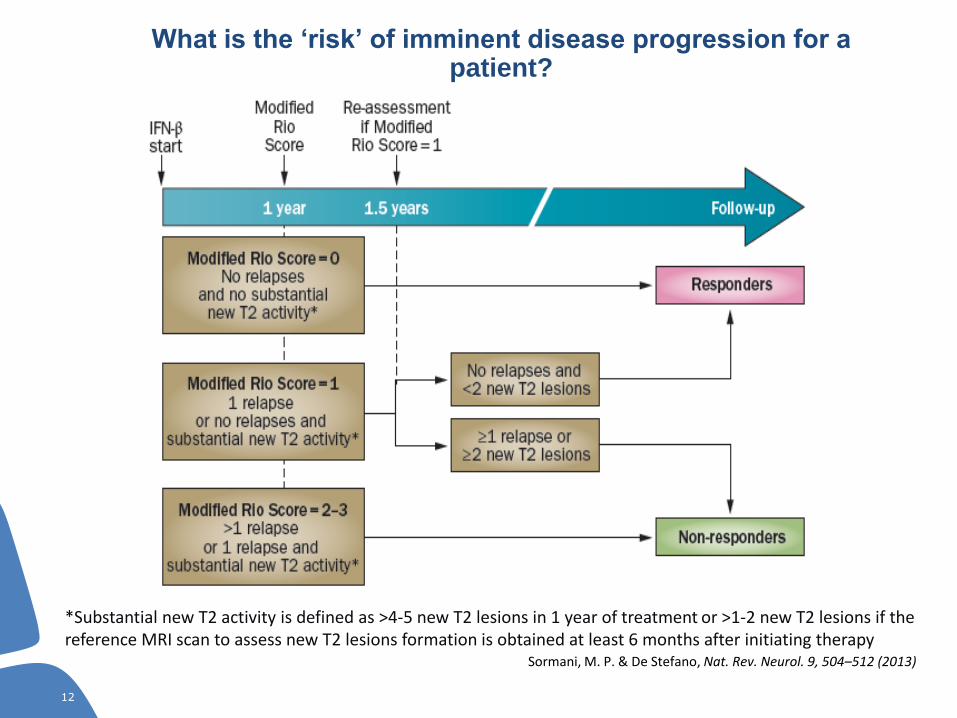
*Substantial new T2 activity is defined as >4-5 new T2 lesions in 1 year of treatment or >1-2 new T2 lesions if the reference MRI scan to assess new T2 lesions formation is obtained at least 6 months after initiating therapy
Sormani, M. P. & De Stefano, Nat. Rev. Neurol. 9, 504–512 (2013)
What is the ‘risk’ of imminent disease progression for a patient?
12
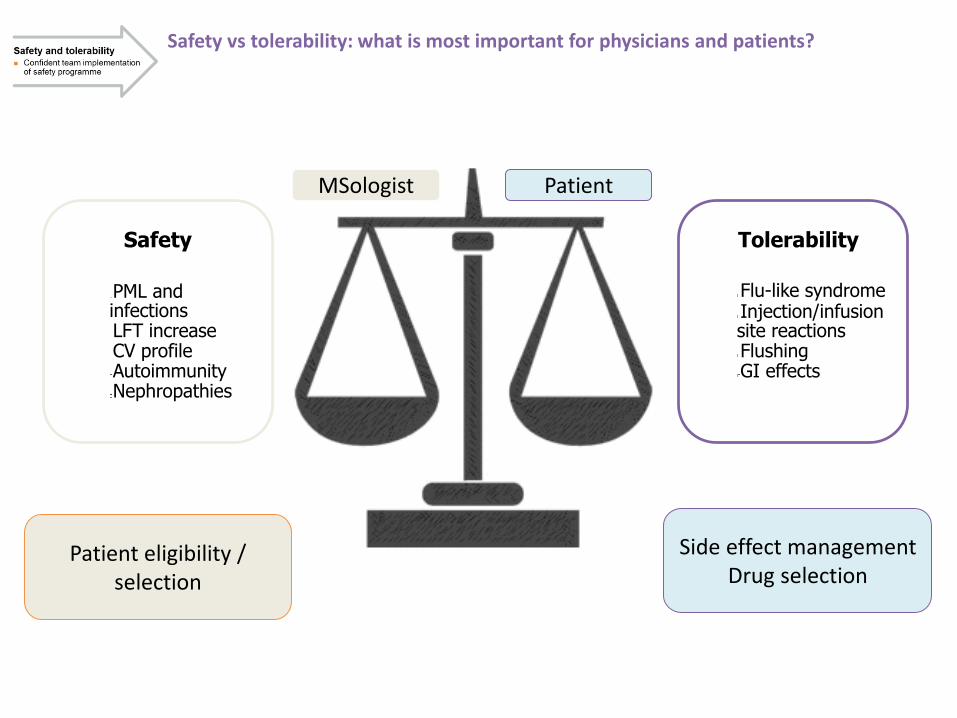
MSologist Patient
Safety vs tolerability: what is most important for physicians and patients?
Patient eligibility / selection
Side effect managementDrug selection
Safety
PML and infectionsLFT increaseCV profileAutoimmunityNephropathies
Tolerability
Flu-like syndromeInjection/infusion site reactionsFlushingGI effects

A continuous balancing between benefit-risk: results influence long-term efficacy
Long-termefficacy
EfficacyShort- and long-termActual and perceived
Safety and tolerabilityConfident team implementationof safety programme
DosingAdministrationFrequency
Adherenceand persistence
World Health Organization. Adherence to long-term therapies: Evidence for action. http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf;Osterberg L and Blaschke T. N Engl J Med 2005
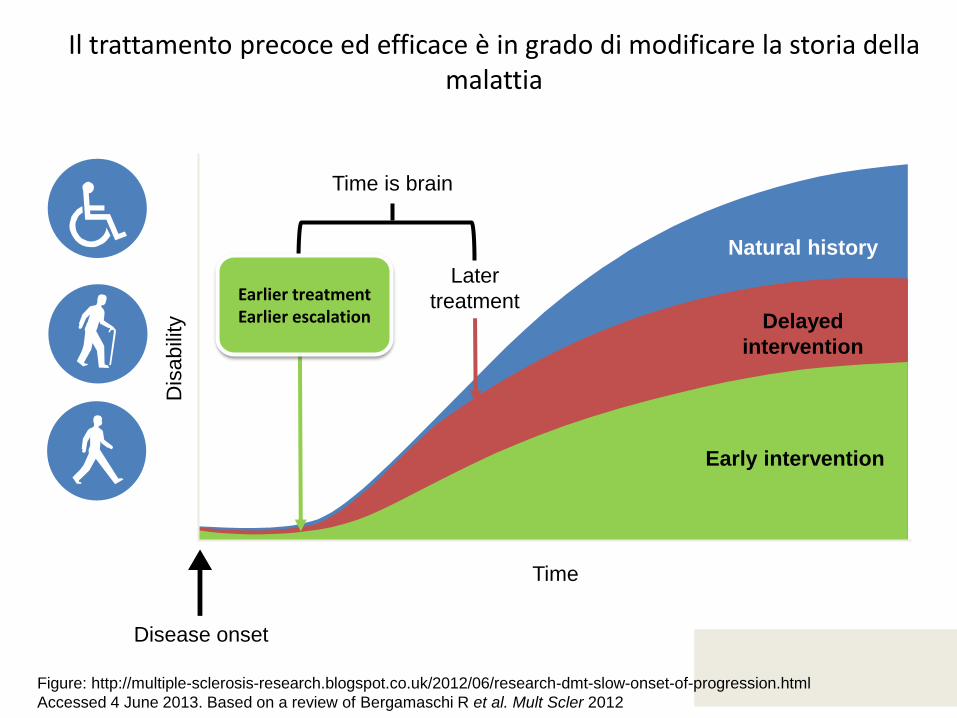
Il trattamento precoce ed efficace è in grado di modificare la storia dellamalattia
Later
treatment
Natural history
Delayed
intervention
Early intervention
Disease onset
Time
Dis
abili
tyTime is brain
Earlier treatmentEarlier escalation
Figure: http://multiple-sclerosis-research.blogspot.co.uk/2012/06/research-dmt-slow-onset-of-progression.html
Accessed 4 June 2013. Based on a review of Bergamaschi R et al. Mult Scler 2012
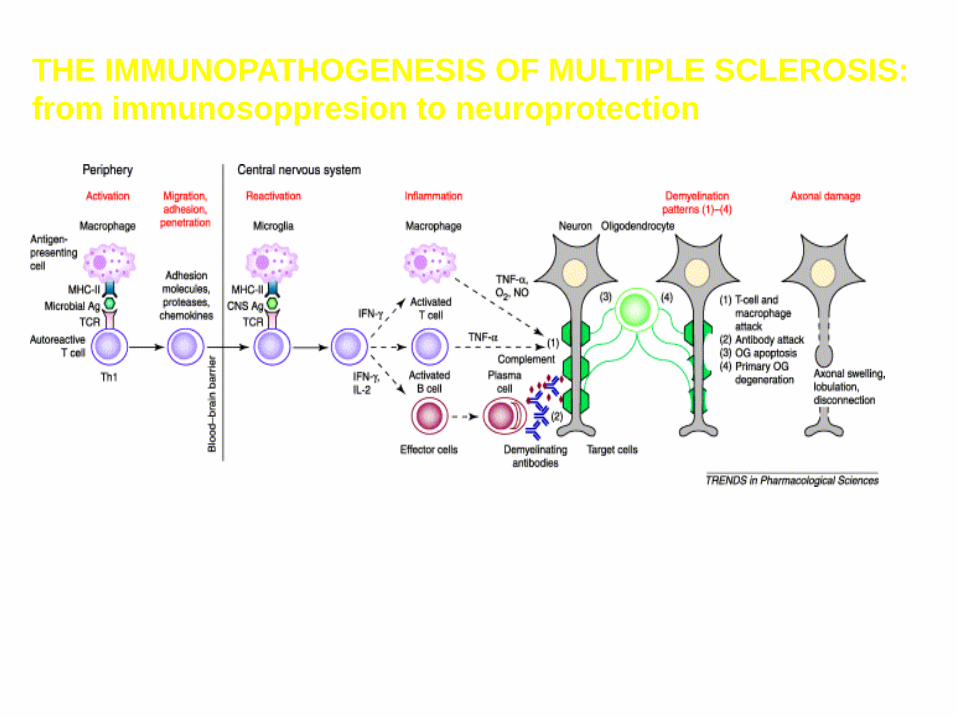
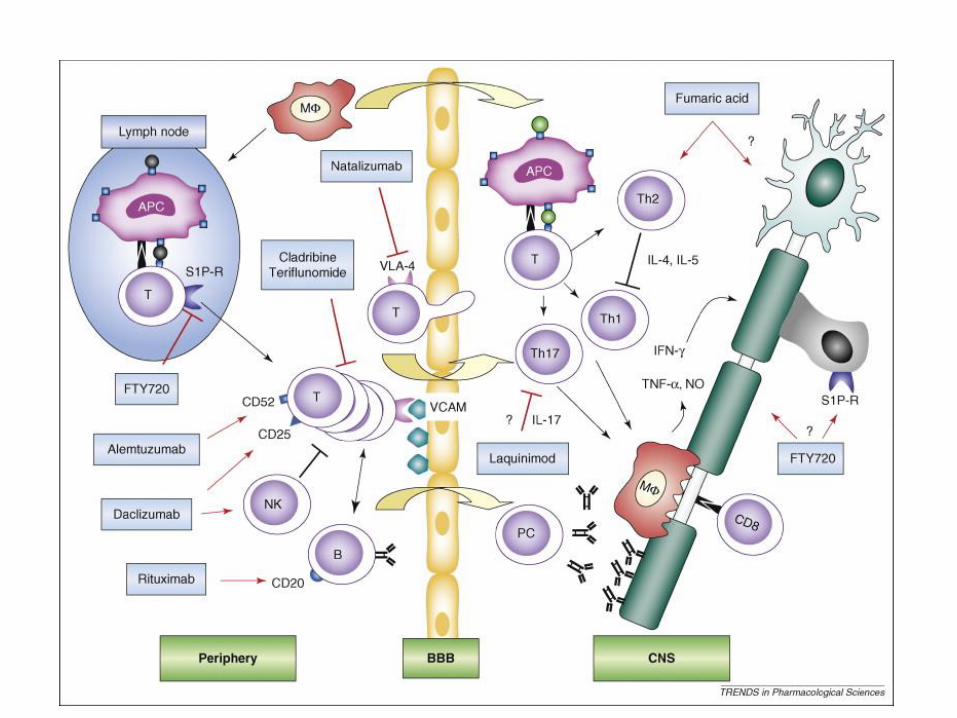
Hartung and colleaguesTrends Pharmacol Sci 2003;24:131-8
THE IMMUNOPATHOGENESIS OF MULTIPLE SCLEROSIS:
from immunosoppresion to neuroprotection
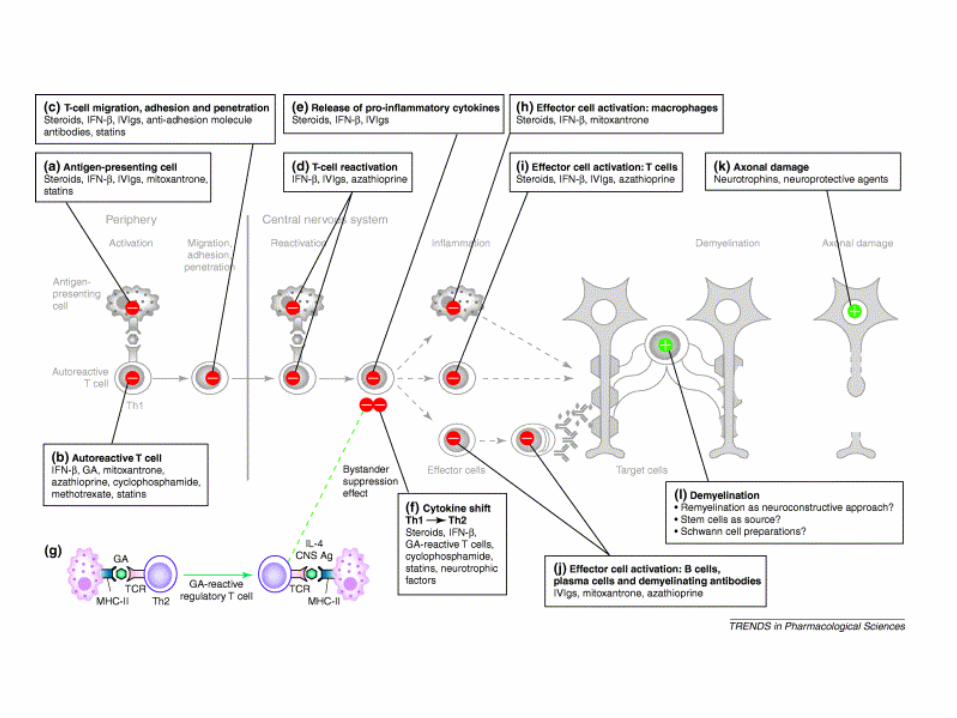
Hartung and colleaguesTrends Pharmacol Sci 2003;24:131-8
Target of MS treatment
Terapia della SM
Terapia della ricaduta
Terapia sintomatica
Terapia modificante il decorso: DMT
Terapia dell’attacco acuto
La comparsa acuta di sintomi neurologici, ricaduta
clinica, si tratta con
METILPREDNISOLONE
1000 mg /DIE per 3-5 gg (Bolo Steroideo)
Razionale :
1. ridurre l’infiammazione , limitando la durata e l’intensità
dei sintomi dell’attacco
2. ridurre la demielinizzazione
Terapia Sintomatica
Terapia dei sintomi cronici molto eterogenei, fastidiosi e
persistenti
La fatica
La spasticità
Parestesie/disestesie
L’atassia
I disturbi genito-urinari
I disturbi gastro-enterici
Il dolore
I disturbi cognitivi
I disturbi affettivo- emozionali
Obiettivi della terapia
1. Inibire precocemente e in maniera completa
la risposta infiammatoria
2. Limitare il danno assono-gliale
3. Sostenere la riparazione mielino-assonica
Farmaci modificanti il decorso (DMT)
Non agiscono sui sintomi già presenti
Obiettivi:
Ridurre la frequenza e la gravità degli
attacchi edlle nuove lesioni alla risonanza
Ridurre la progressione della disabilità
Si distinguono
1. Immunomodulanti
2. Immunosoppressori
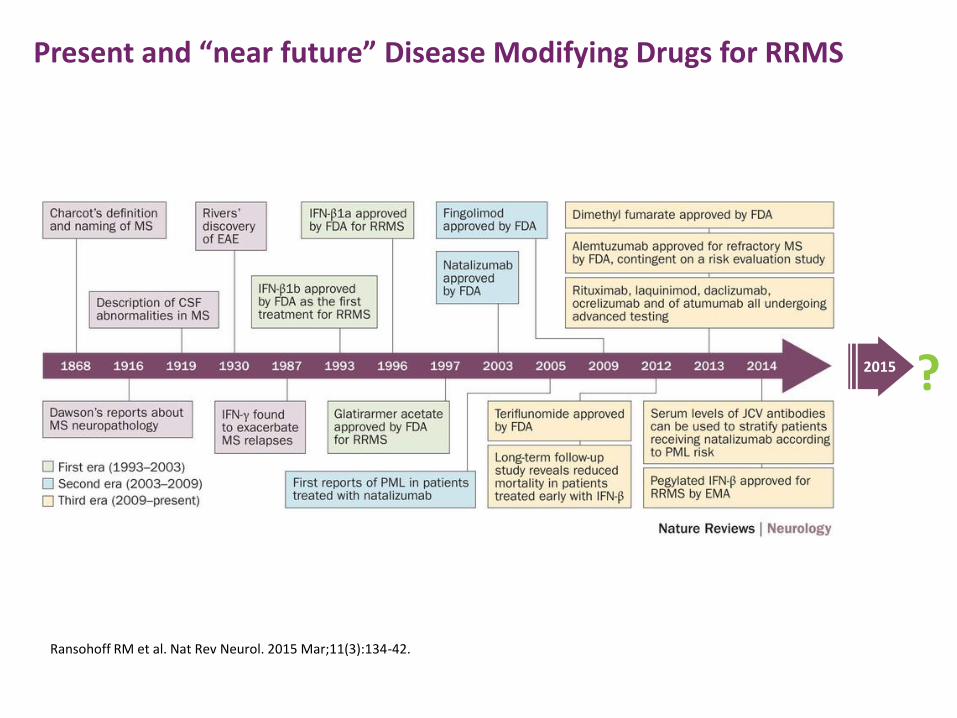
Present and “near future” Disease Modifying Drugs for RRMS
2015 ?
Ransohoff RM et al. Nat Rev Neurol. 2015 Mar;11(3):134-42.

Disease modifying therapies in MS
Class I type A Class I type B
Clinically isolated syndromes(CIS):- IFNb-1a i.m.
MS RR: - IFNb-1a and 1b- Glatiramer acetate- Mitoxantrone (not
responders)- Natalizumab
MS PS:- IFNb-1a and 1b (active MS)- Mitoxantrone (worsening MS)
MS PP:- Therapy not available
MS PS worsening:
- Cyclophosphamide
Class I type CMS pts not responder orintolerant to first linetheraphy
Mild oral immunosuppressants:
- Methotrexate or Azathioprine
Intravenous Immunoglobulin
Plasmapheresis
Pulses of Methylprednisolone
Combination therapy
Immunomodulators
Interferon beta Glatiramer acetate IVIg
Immunossupressants:
Mitoxantrone Cyclophosphamide Azathioprine Methotrexate Cladribine MycophenolatMT (ASCT)
Neuroprotection
Combination therapy
Results of Clinical Trials in PPMS
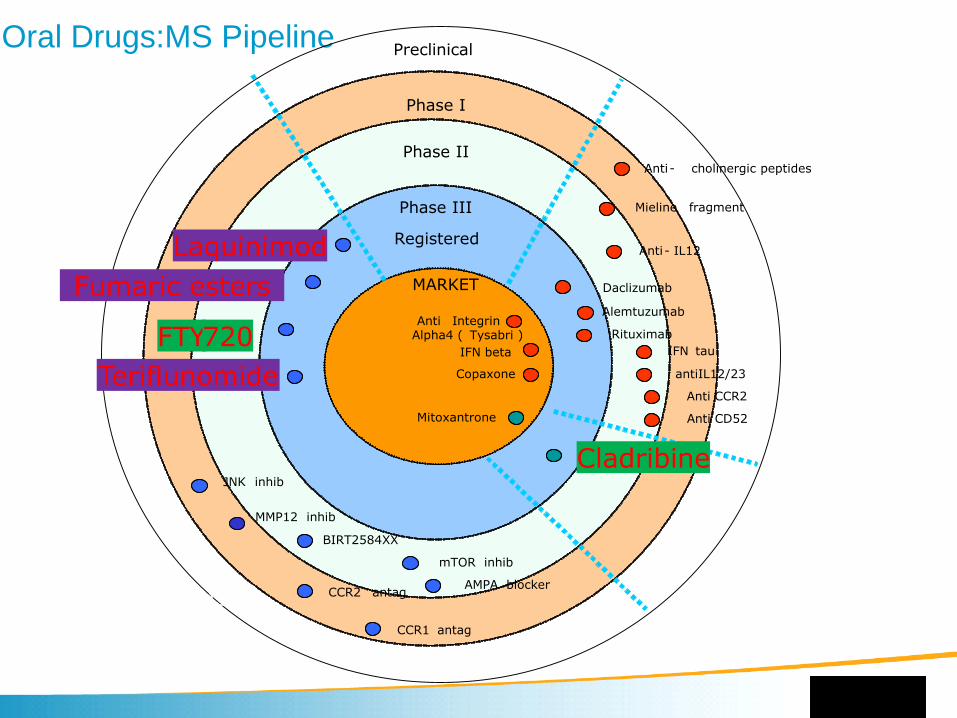
Oral Drugs:MS PipelinePreclinical
Phase I
Phase II
Phase III
Registered
MARKET Protein -based
therapeutcs
IFN beta
Anti IntegrinAlpha4 ( Tysabri )
Copaxone
Mitoxantrone
Cladribine
Rituximab
Anti- IL12
IFN tau
Mieline fragment
antiIL12/23
Daclizumab
Anti CCR2
Anti CD52
Anti- cholinergic peptides
BIRT2584XX
mTOR inhib
AMPA blockerCCR2 antag
JNK inhib
Teriflunomide
FTY -720
Fumaric esters
Laquinimod
CCR1 antag
MMP12 inhib
Alemtuzumab
New oral treatments
Targets of new MS treatments (Linker 2008)
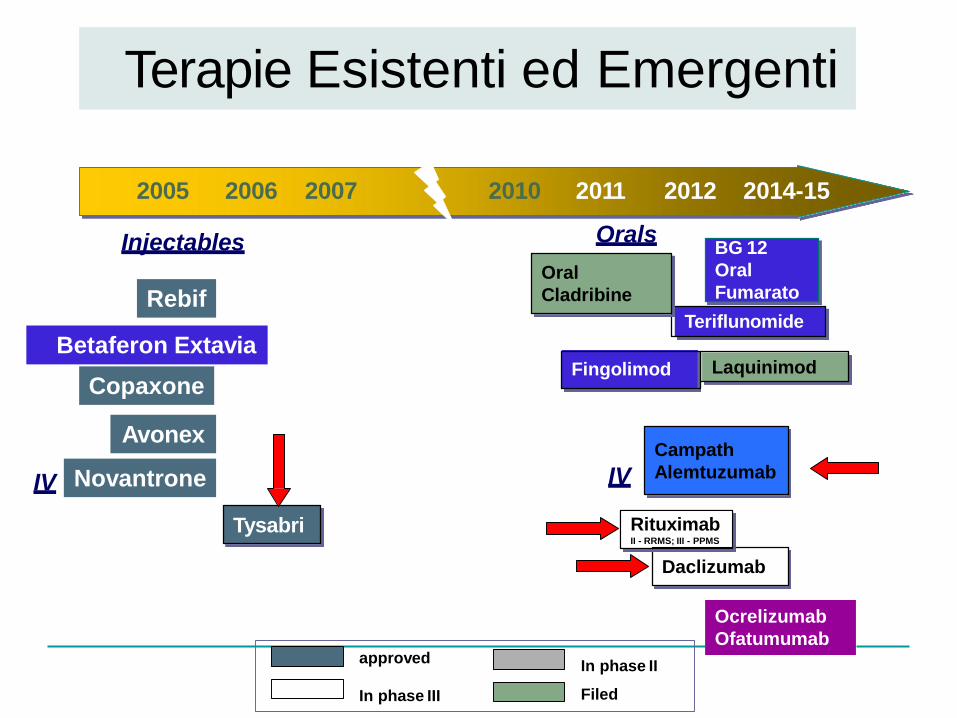
Terapie Esistenti ed Emergenti
IV
Teriflunomide
LaquinimodFingolimod
Oral
Cladribine
Daclizumab
Tysabri
IV
2005 2006 2007
Injectables
Copaxone
Betaferon Extavia
Avonex
Novantrone
RituximabII - RRMS; III - PPMS
Rebif
BG 12
Oral
Fumarato
Filed
approvedIn phase II
In phase III
2010 2011 2012 2014-15
Orals
Campath
Alemtuzumab
Ocrelizumab
Ofatumumab
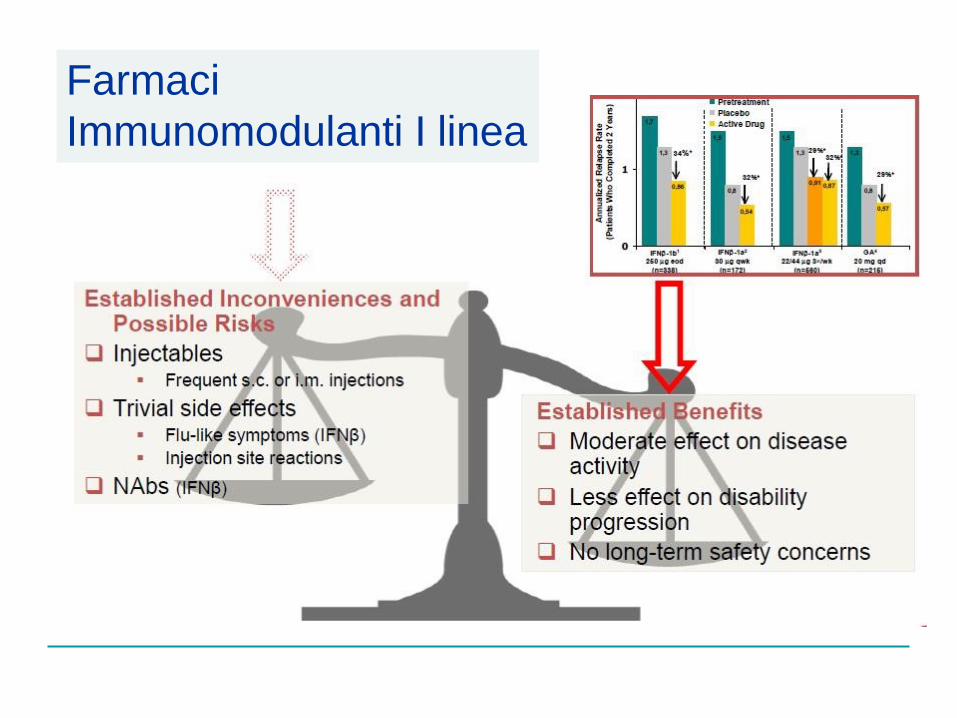
Farmaci
Immunomodulanti I linea
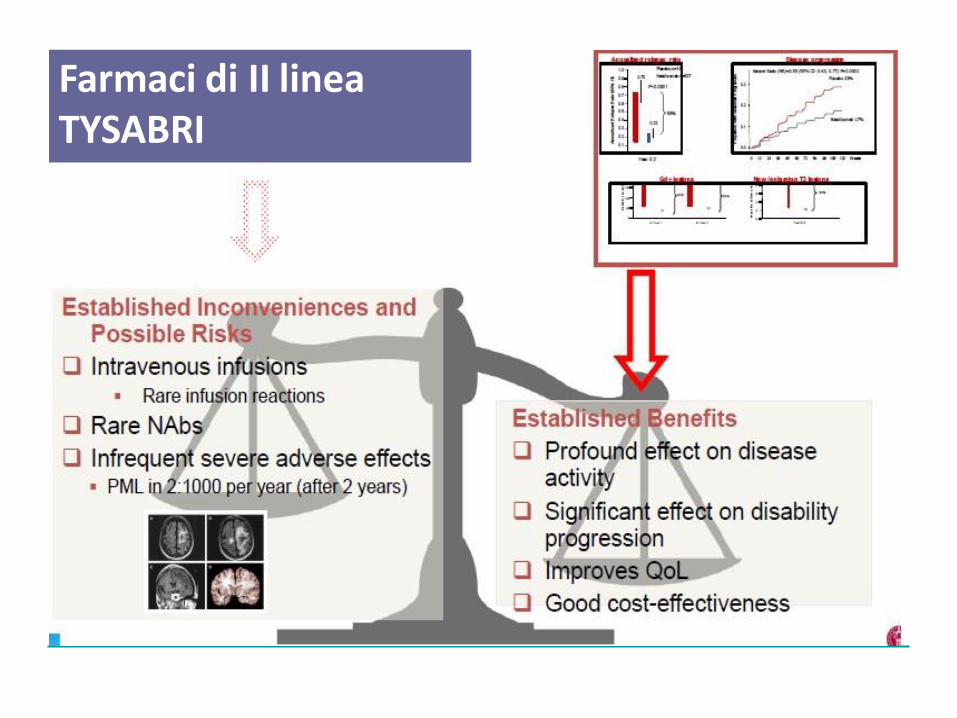
Farmaci di II lineaTYSABRI
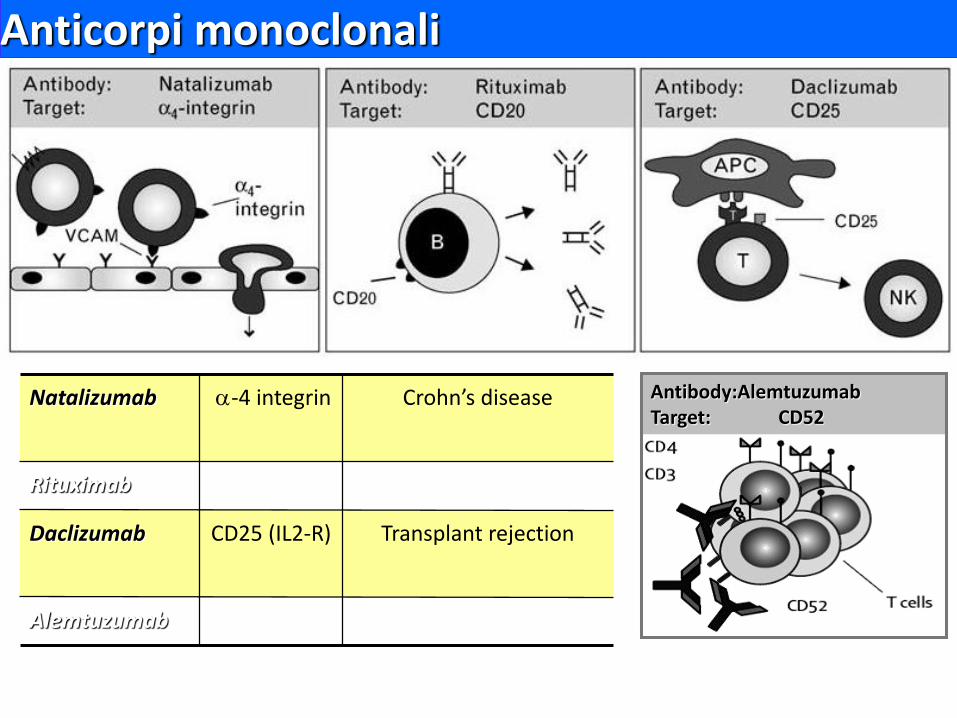
Anticorpi monoclonali
Lutterotti A - Lancet Neurol 2008
Natalizumab -4 integrin Crohn’s disease
Rituximab CD20 B cell lymphoma
Daclizumab CD25 (IL2-R) Transplant rejection
Alemtuzumab CD52 Chronic Leukaemia
Antibody:AlemtuzumabTarget: CD52
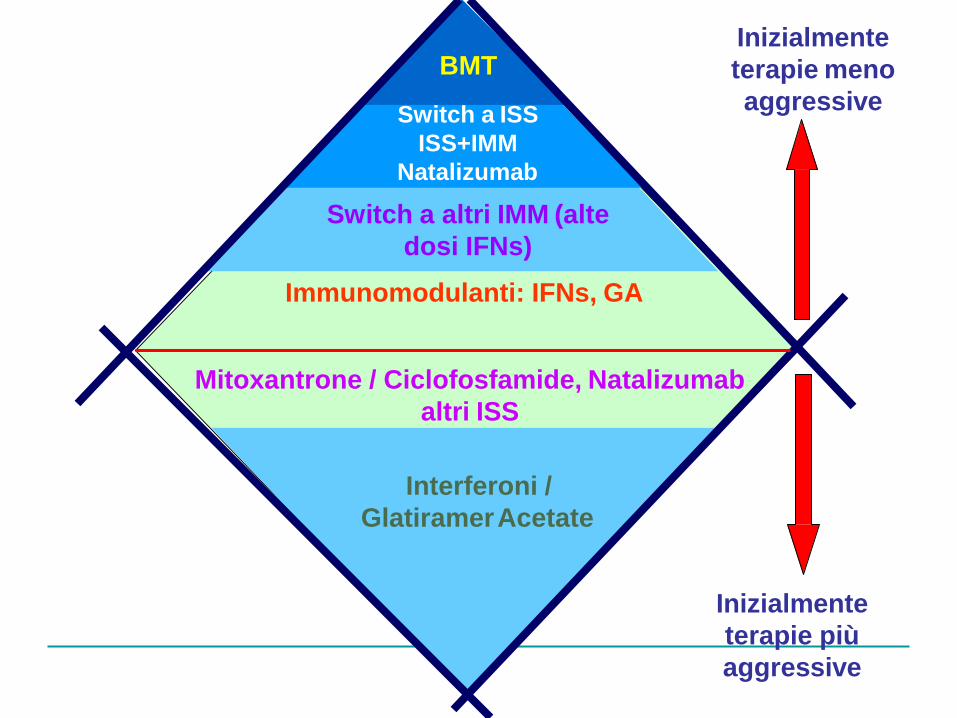
Inizialmente
terapie meno
aggressive
BMT
Switch a ISS
ISS+IMM
Natalizumab
Switch a altri IMM (alte
dosi IFNs)
Immunomodulanti: IFNs, GA
Mitoxantrone / Ciclofosfamide, Natalizumab
altri ISS
Interferoni /
GlatiramerAcetate
Inizialmente
terapie più
aggressive
Induction therapy
• E’ un metodo da anni presente in oncologia nel tentativo di ridurre il numero di cellule cancerogene e rendere la malattia vulnerabile alle terapie
• Questo metodo è ripreso nelle malattie autoimmuni allo stesso scopo ovvero rendere il sistema immunitario maggiormente sensibile alle terapie immunomodulanti o immunosoppressive
Induction therapy
Può essere il primo step per una strategia terapeutica
E’ la prima linea in una malattia aggressiva per ridurre il numero dei linfociti autoimmuni T e B e indurre una «riorganizzazione» del sistema immunitario
Si basa su una rapida somministrazione di alte dosi di farmaviimmunosoppressori che possono creare significativi effetti collaterali per cui necessita di neurologi esperti
I farmaci in uso sono il Mitoxantrone,Ciclofosfamide,Cladribina e Alentuzumab

Quale potrebbe essere un risultato clinicamente significativo
per il paziente?
Terapie emergenti per la SM
Benefici della terapiaRischi della malattia
Rischi della terapia
I benefici…
Benefici
• Risultati sulle ricadute
• Risultati sulla disabilità
• Effetti sulla MRI
• Ritardo di conversione aSM
clinicamente definita
• Risultati sui disordini cognitivi
• Risultati sulla QoL
• Efficacia a lungo teRrmisinkes
I rischi …
Rischi
• Depressione
• Epatotossicità
• Linfopenia
• Gravidanza
• Non-aderenza
• Sintomi simil-influenzali
• Reazioni nella sede di iniezione
• Reazioni sistemiche• PML
• Aumento dBelerinscehfioitdsiinfezioni
• Neoplasie
• Insufficienza cardiaca
• Altro
Considerazioni sulle terapie per la sclerosi multipla :
evidenze, esperienza, e aspettative future.
In futuro, tecniche di farmacogenetica, proteomica, analisi microarray daranno nuove informazioni sul profilo individuale dei pazienti e aiuteranno a rispondere a specifici quesiti terapeutici:
1. Quale è il miglior trattamento per una specifica persona ?
2. Quale paziente richiede regimi di trattamento intensivi, combinazione di farmaci per ottimizzare il controllo della malattia?
3. Quale è la dose specifica più appropriata per quello specifico paziente?
4. Quale paziente sarà predisposto allo sviluppo di eventi avversi legati aifarmaci
EM Froman e al, 2005





























