Embed Size (px)
Citation preview

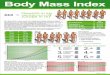
Limitations of BMI in Pregnancy
• Using BMI, in pregnancy in not accurate.
• It should be done pre and post pregnancy.
• BMI does not really convey differences in shape that are relevant to obstetric anaesthetists and for the surgery during normal pregnancy and instrumental delivery or C/S.

The Scale of the Problem
• WHO: “Obesity is a worldwide epidemic”.• 250 Million obese people, 7% of world
population. • USA: 65% of adults are obese or
overweight. NHANES.• UK: Fastest growing obese population.• 16% of obstetric patients >100kg.• 19.6% of women in the reproductive age
are above BMI >30.

• Transition from Overweight to Obesity Worsens Pregnancy Outcome in a BMI-dependent Manner. – Raatikainen K, Heiskanen N, Heinonen S. Obes
Res. 2006 Jan;14(1): 165-71.
– The risk of perinatal death more than doubles in the transition from an overweight to an obese condition.

• Teratology public affairs committee position paper: Maternal obesity and pregnancy. – Scialli AR. Birth Defects Res A Clin Mol Teratol.
2006 Feb; 76(2): 73-7.
• The literature suggests that women with a body mass index (BMI) >/=30 have approximately double the risk of having a child with a neural tube defect (NTD) compared to normal-weight women, and the increased risk associated with higher maternal body weight does not appear to be modified by folic acid supplementation.

• The prevalence and impact of overweight and obesity in an Australian obstetric population. – Callaway LK, Prins JB, Chang AM, McIntyre
HD. E Floor, Clinical Sciences Building, Royal Brisbane and Women’s Hospital, Herston QLD 4029, Australia. [email protected]. Med J Aust. 2006 Jan 16; 184(2): 56-9.
• 11 of 252 women - BP, GDM, hospital admission, C/S, birth defect, preterm delivery, NICU admission.
• BMI should be routinely recorded on perinatal data collection sheets.

Recommendations for Weight Gain During Pregnancy
Description Recommended Total Weight Gain (lbs)
Underweight 28 – 40 (12-17 kgs.)
Normal weight 25 – 35 (11-15 kgs.)
Overweight 15-25 (6.5-11 kgs.)
Obese 15 (6.5 kgs.)
• Note multiple pregnancies.

Recommendations for ALL women (including preconception):
• Inform and counsel women about the health risks associated with overweight and obesity.
• Encourage a healthy diet– Diets that restrict particular food groups are
discouraged, especially during pregnancy.
• Screen for hypertension and diabetes mellitus in women who are at risk.
• Counsel women to consume adequate folic acid, iron and calcium.

cont. Recommendations…
• Encourage regular exercise (30 minutes of moderate physical activity daily)
• Counsel women to quit smoking
• Counsel women to avoid consuming alcohol during pregnancy.
• Discuss recommended weight gain during pregnancy.

After Pregnancy (postpartum)
Recommendations for “for ALL women” PLUS the following:
• Encourage breastfeeding.
• Counsel women to return to a healthy weight
• For women who are attempting to or have quit smoking, continue support to prevent postpartum relapse.



Odds Ratios of Obesity and Overweight vs. Normal Weight Status on Selected Pregnancy Outcomes: Missouri Singleton Pregnancies
1999-2003
Outcome
Obesity vs. Normal Odds Ratio
95 percentconfidence interval
Very low birth weight (<1500 grams) 1.23 1.15 1.32Macrosomia (>4499 grams) 2.52 2.36 2.69Early preterm (<32 weeks) 1.09 1.03 1.16Congenital anomalies 1.17 1.09 1.25Fetal death 1.30 1.17 1.45Neonatal (<28 days) death 1.31 1.15 1.51Post-neonatal (1-11 months) death 1.17 0.97 1.42Perinatal (fetal or neonatal death) 1.31 1.20 1.43Infant (<1 year) death 1.26 1.13 1.42Fetal or infant death 1.29 1.19 1.39
Note: Odds ratios calculated using multivariate logistic regression with the following covariates: race, education, age, marital status, & smoking status of mother and birth order.

• Infertility – PCO
– Early pregnancy loss _________
– Insulin resistant
• Birth defects particularly neural tube defect

• Labor delivery complications– Preterm labour
– Prolonge 2nd stage
– Large babies shoulder dystocia + instrumental delivery
– C/S C.P.D.
– Need for Oxytocin

• Antenatal complications
Maternal D.M. PET Hypertension

Maternal complications
• Preterm Labour – could be iotrogenic due to D.M., PET, HTN.
• Low birth weight
- Women with relatively low pre-pregnancy weight more like to have PTL + L.B.W.

cont. Maternal complications
• Postpartum haemorrhage
• Wound infection
• Post C/S endometritis prolonged hospitalization
• Postpartum thromboembolic manifestation DVT, P.E.

Fetal complications
• Neonatal death
• Birth defect – neural tube defect
• Low Apgar Score
• More NICU admission

• Cedergren MI (2004): A Swedish, population-based cohort study (n=805,275)
Study Group Control Group – Normal Weight
BMI > 40
PET X 5 fold
Still Birth x 3 fold
LGA x 4 folds
Early NND x 3.5 fold

• Baeten JM et al (2001): A population-based cohort study in Washington state based on birth data (n=96,801).
– GDM
– PET
– Eclampsia
– C/S
– LGA infants


![BM1弾 カードチェックリスト · 2020-06-17 · 1.89 d bmi-scp4[cp1 c] bmi-scp8[cp] bmi-hcpi bmi-scps[cpi a bmi cl bmi-scpi c] bmi-scp5[cp] c] bmi-cpi [cpi 12 bmi-cp2tcp]](https://img.pdfslide.tips/doc/110x75/5f0d11867e708231d43885ac/bm1-fffffff-2020-06-17-189-d-bmi-scp4cp1-c-bmi-scp8cp.jpg)