Embed Size (px)
Citation preview

Respiratory Medicine (2013) 107, 1465e1480
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier .com/locate/rmed
REVIEW
Long-acting bronchodilators improve HealthRelated Quality of Life in patients with COPD
Fulvio Braido a,*,1, Ilaria Baiardini a,1, Mario Cazzola b,Guy Brusselle c, Fiorenza Marugo a, Giorgio Walter Canonica a
aAllergy & Respiratory Diseases Clinic e DIMI e University of Genoa, IRCCS AOU San Martino-IST,Genova, ItalybUnit of Respiratory Clinical Pharmacology, Department of System Medicine, University of Rome‘Tor Vergata’ Rome, ItalycDepartment of Respiratory Medicine, Ghent University Hospital, Ghent, Belgium
Received 8 February 2013; accepted 8 August 2013Available online 31 August 2013
KEYWORDSLong-actingbronchodilators;COPD;Quality of life;Health status
* Corresponding author. Tel./fax: þE-mail address: fulvio.braido@unig
1 Both the authors contributed equa
0954-6111/$ - see front matter ª 201http://dx.doi.org/10.1016/j.rmed.201
Summary
Background: Long-acting bronchodilators are first-line treatment for chronic obstructive pul-monary disease (COPD), and their efficacy on lung function and clinical parameters is recog-nized.Objective: To explore the available evidence about the effects of long acting bronchodilatorson Health Related Quality of Life (HRQoL) and Health Status (HS) in clinical research.Methods: Randomized controlled trials published till December 2012 evaluating HRQoL/HS inCOPD by means of validated questionnaires were analysed.Results: Fifty-one trials on Long acting b2 agonist (LABA) and Long acting Anticholinergic(LAMA) met the inclusion criteria. A total of 37,225 moderate-severe COPD patients testing6 drugs, 12 different devices and 22 different dosages, with a study duration ranging from 4weeks to 4 years were studied. A statistical significant HRQoL/HS improvement was reachedin 93% of the studies. Nevertheless, the Minimal Important Difference (MID) was reached in70,6% of the studies considering the difference between baseline and end of the study, andin 50% when comparing active treatment and placebo.Conclusions: The data coming from the review support the efficacy of long acting bronchodi-lators in improving HRQoL/HS of COPD patients. Further research evaluating HRQoL/HS as pri-mary outcome and according to guidelines on Patient Reported Outcomes is needed.ª 2013 Elsevier Ltd. All rights reserved.
39 0105553524.e.it (F. Braido).lly to this study.
3 Elsevier Ltd. All rights reserved3.08.007
.

1466 F. Braido et al.
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1466
Search strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1466Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1466Long acting beta2 agonists (LABA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1467
Formoterol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1467Salmeterol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1471Indacaterol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1472Long acting anticholinergic(S) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1472
Glycopyrronium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1472Aclidinium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1473Tiotropium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1474Long acting beta2 agonists (LABA) plus long-acting muscarinic antagonist (LAMA) . . . . . . . . . . . . . . . . . . . . . . 1475Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1476Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1477Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1477References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1477
Introduction
Health Related Quality of Life (HRQoL) and Health Status(HS) represent the Patient Reported Outcomes (PROs) mostfrequently assessed in chronic obstructive pulmonary dis-ease (COPD). HRQoL refers to the impacts of a disease andits therapy upon a patient, as perceived by the patienthimself [1e3]. HS is part of the broader concept of HRQoL,and can be defined as the ability of a subject to be skillfulin a variety of physical, emotional and social activities [4].Both PROs are assessed by means of validated question-naires usable for all health conditions (generic question-naires, e.g. SF-36, EQ5D) [5] or specifically addressed toCOPD (specific questionnaires, e.g. the COPD-specificversion of the St. George’s Respiratory Questionnaire -SGRQ) [6].
HRQoL and HS are considered relevant in clinicalresearch, daily practice and regulatory processes [7e16].The European Medicines Agency (EMA) [14] suggests that,especially in non life-threatening chronic conditions, whentwo drugs show similar efficacy, PROs could be useful indefining the drug to be recommended. The role of patient’sperspective is also underlined by the GRADE system [17],which includes all patients’ preferences and values ascornerstones in the process of formulating recommenda-tions, thus contributing to bring scientific research to reallife.
Moreover, the “Global Initiative for Chronic ObstructiveLung Disease” (GOLD) guidelines have recently proposedthat the classification of severity should consider, besidespulmonary function or exacerbation history, symptoms orHS [18].
The aim of the present review was to examine theavailable scientific evidences about the effects of longacting bronchodilators, the mainstay treatment in COPD[18,19], on HRQoL and HS in order to draw considerationsuseful in daily practice and suggest potential areas forfuture research.
Search strategy
Randomized controlled trials evaluating HRQoL/HS inCOPD by means of validated questionnaires and publishedtill December 2012 were searched in PubMed, using thefollowing key words:
B COPDB Chronic obstructive pulmonary diseaseB HRQoLB Health Status (HS)B Long acting b2 agonist (LABA) (salmeterol, formoterol,
indacaterol, vilanterol)B Long acting Anticholinergic Z Long acting muscarinic
antagonist (LAMA) (tiotropium, aclidinium,glycopyrronium)
For each selected study, the following issues were takeninto account:
� HRQoL/HS Total and domains scores (when available)� Minimal Important Difference (MID), that is the smallestdifference that patients perceive as important [20](reported by the authors or calculated by reviewersaccording to figures and tables).
� Presence of complete HRQoL/HS data at each sched-uled visit
� HRQoL/HS total score mean change at the end of thestudy in the treatment group(s)
� Difference in HRQoL/HS total score between active andplacebo group
Results
A total of 44 trials evaluated the impact of LABA and LAMAon HRQoL and HS with validated questionnaires. Table 1reports the characteristics of the questionnaires used inthe 44 trials.

Table 1 HRoL/HS questionnaires used in the examined trials.
Questionnaire Number of items Number ofdomains
Domains scores Total score/s
Chronic Respiratory DiseaseQuestionnaire (CRDQ)
20 4 � Dyspnea� Fatigue� Emotional function� Mastery
Overall score
EQ-5D 5 questions þ 1 VAS e � Mobility� Self care� Usual activities� Pain/discomfort� Anxiety/depression
Global health score
SF-36 36 8 � Physical functioning� Role limitations due tophysical health problems
� Bodily pain� Social functioning� General mental health� Role limitations due toemotional problems
� Vitality� General healthperceptions
� Physical ComponentSummary (PCS)
� Mental ComponentSummary (MCS)
St. George’s RespiratoryQuestionnaire (SGRQ)
50 3 � Symptoms� Activity� Impacts
Total score
Visual Simplified RespiratoryQuestionnaire (VSRQ)
8 e � Dyspnea� Anxiety� Depressed mood� Sleep� Energy� Daily activities� Social activities� Sexual life
Global score
LABA/LAMA effects on COPD health status 1467
Long acting beta2 agonists (LABA)
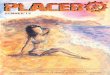
A total of 21 trials fulfilled the selection criteria (8considering formoterol/arformoterol, 7 salmeterol, 6indacaterol), with an overall randomized population of12,213 patients. No studies assessing vilanterol effects onHRQoL/HS have been published yet. The duration of thestudies ranged from 10 weeks to 1 year, and HRQoL/HSwere always evaluated as secondary outcome (Table 2).The change in SGRQ Total score from baseline to the end ofthe study in patients treated with Long acting b2 agonists(LABA) and the difference in SGRQ Total score between theabove mentioned change and that in the placebo group areshown in Figs. 1 and 2.
Formoterol
An overall population of 4314 moderateesevere COPD pa-tients [21] were studied. HRQoL/HS were evaluated in allstudies using the SGRQ. The study duration ranged from 12
weeks to 12 months, and comparators of formoterol wereterbutalin [22], salmeterol [23], ipratropium [24,25],theophylline [26], different formulations of formoterol [27]and placebo [23e29].
Formoterol was tested as dry powder inhaler (DPI) Aer-olizer at dose of 12/24 mg bis in die (BID) [2426,27,28],Novolizer 12/24 mg BID [29], Turbohaler 18 mg BID [25], 9 mgBID or BID þ 4.5 mg prn [22], and nebulized arformoterol viaPARI LC PLUS nebulizer at doses of 15/20/25 mg BID[23,27,28] and 50 mg [23].
Randomized patients could receive concomitant treat-ment with inhaled corticosteroids (ICS) [22e24,26e28] oralsteroids [23,24,27,28], short-acting b2 agonist[22,23,26,27], xanthine [22,27,29], antileukotrienes [27].
Dahl [24] showed that both formoterol 12 and 24 mgsignificantly improved SGRQ total score compared to pla-cebo (43.5 and 41.7 vs 46.8; P Z 0.009 and P < 0.001), witha difference exceeding the MID (�5.06) only with the 12 mgdosage. Compared with ipratropium, formoterol 12 mgshowed a statistically significant improvement thatapproached the MID (�3.79). While formoterol 12 mg

Table 2 Trials evaluating the effect of Long acting b2 agonists and Long Acting Anthicolinergic on HRQoL.
Reference Comparison HRQoLquestionnaires
Randomisedpatients
Studyduration
Formoterol/Arformoterol
Dahl R (2001) Formoterol 12 mg DPI BIDFormoterol 24 mg DPI BIDIpratropium 40 mg MDI QIDPlacebo
SGRQ 780 12 weeks
Rossi A (2002) Formoterol 12 mg DPI BIDFormoterol 24 mg DPI BIDTheophylline 200/300 mg cpPlacebo
SGRQ 854 52 weeks
Wadbo M (2002) Formoterol 18 mg DPI BIDIpratropium 80 mg pMDI TIDPlacebo
SGRQ 183 12 weeks
Campbell M (2005) Formoterol 9 mg DPI BID þTerbutaline 0.5 mg prrnFormoterol 9 mg DPI BID þFormoterol 4.5 mg DPI prnPlacebo þ Terbutaline 0.5 mg prrn
SGRQ 657 27 weeks
Baumgarten RA (2007) Arformoterol 15 mg BID PARI NebArformoterol 25 mg BID PARI NebArformoterol 50 mg QD Pari NebSalmeterol 42 mg MDI BIDPlacebo
SGRQ 724 12 weeks
Gross NJ (2008) Formoterol fumarate inhalationsolution 20 mg BIDFormoterol 12 mg DPI BIDPlacebo
SGRQ 351 12 weeks
Welte T (2008) Formoterol 12 mg BID DPIFormoterol 24 mg OD DPI
SGRQ 321 12 weeks
Hanania NA (2010) Arformoterol 15 mg BID PARI NebArformoterol 25 mg BID PARI NebFormoterol 12 mg DPI BID
SGRQ 444 27 weeks
Salmeterol Jones PW (1997) Salmeterol 50 mg MDI BIDSalmeterol 100 mg MDI BIDPlacebo
SGRQ, SF-36 283 16 weeks
Di Lorenzo G (1998) Salmeterol 50 mg MDI BIDTheophylline
SF-36 178 52 weeks
Taccola M (1999) Salmeterol 50 mg MDI BIDTheophylline
SF-36 138 52 weeks
Rennard SI (2001) Salmeterol 42 mg MDI BID þplacebo MDI BIDIpratropium 36 mg MDI QDPlacebo
CRDQ 405 12 weeks
Gupta RK (2002) Salmeterol 25 mg � 2 MDI BIDPlacebo
SF-36 33 10 weeks
Chapman KR (2002) Salmeterol 50 mg DPI BIDPlacebo
SGRQ 408 24 weeks
Stockley RA (2006) Salmeterol 50 mg DPI BIDPlacebo
SGRQ 634 52 weeks
Indacaterol Donohue JF (2010) Indacaterol150 mg DPI ODIndacaterol 300 mg DPI ODTiotropium 18 mg DPI OD(open label)Placebo
SGRQ 1683 26 weeks
Dahl R (2010) Indacaterol 300 mg DPI ODIndacaterol 600 mg DPI ODFormoterol 12 mg DPI BIDPlacebo
SGRQ 1732 52 weeks
1468 F. Braido et al.

Table 2 (continued )
Reference ComparisonHRQoLquestionnaires
Randomisedpatients
Studyduration
Chapman KR (2011) Indacaterol150 mg DPI ODIndacaterol 300 mg DPI ODPlacebo
SGRQ 415 52 weeks
Kornmann O (2011) Indacaterol150 mg DPI ODSalmeterol 50 mg DPI BIDPlacebo
SGRQ 1002 27 weeks
Kerwin EM (2011) Indacaterol 75 mg DPI ODPlacebo
SGRQ 641 12 weeks
Kinoshita M (2012) Indacaterol 150 mgIndacaterol 300 mgPlacebo
SGRQ 347 12 weeks
Glycopyrronium D’Urzo A (2011) Glycopyrronium bromide 50 mg SDDPI ODPlacebo sddpi OD
SGRQ 822 26 weeks
Kerwin E (2012) Glycopyrronium bromide 50 mg SDDPITiotropium 18 mgPlacebo
SGRQ 1066 52 weeks
Aclidinium Chanez P (2010) Aclidinium 25, 50, 100, 200, or 400 mg ODTiotropium 18 mgPlacebo
SGRQ 464 4 weeks
Jones PW (2011) Aclidinium 200 mg ODPlacebo
SGRQ 1647 42 weeks
Jones PW (2012) Aclidinium 200 mg MDDPI BIDAclidinium 400 mg MDDPI BIDPlacebo
SGRQ 828 24 weeks
Tiotropium Vinken W (2002) Tiotropium 18 mg DPI ODIpratropium 40 mg MDI QD
SGRQ, SF-36 535 52 weeks
Donohue JF (2002) Tiotropium 18 mg DPI ODSalmeterol 50 mg MDI BIDPlacebo
SGRQ 623 27 weeks
Brusasco V (2003) Tiotropium 18 mg DPI ODSalmeterol 50 mg MDI BIDPlacebo
SGRQ 1207 27 weeks
Casaburi R (2002) Tiotropium 18 mg DPI ODPlacebo
SGRQ, SF36 921 52 weeks
Casaburi R (2005) Tiotropium 18 mg DPI QDPlacebo
SGRQ 108 25 weeks
Covelli H (2005) Tiotropium 18 mg DPI ODPlacebo
EQ-5D 196 12 weeks
Verkindre C (2006) Tiotropium 18 mg DPI ODPlacebo
SGRQ 100 12 weeks
Um SW (2007) Tiotropium 18 mg DPI ODTiotropium 18 mg DPI OD þBudesonide 200 mg DPI BID
SGRQ 100 6 weeks
Chan CKN (2007) Tiotropium 18 mg DPI ODPlacebo
SGRQ 913 48 weeks
Johansson G (2008) Tiotropium 18 mg DPI ODPlacebo
EQ-5D 224 12 weeks
Ambrosino N (2008) Tiotropium 18 mg DPI ODPlacebo
SGRQ 234 25 weeks
Tonnel AB (2008) Tiotropium 18 mg DPI ODPlacebo
SGRQ, VSRQ 555 40 weeks
Tashkin DP (2008) Tiotropium 18 mg DPI ODPlacebo
SGRQ 5993 208 weeks
(continued on next page)
LABA/LAMA effects on COPD health status 1469

Table 2 (continued)
Reference ComparisonHRQoLquestionnaires
Randomisedpatients
Studyduration
Kurashima K (2009) Tiotropium 18 mg DPI ODSalmeterol 50 mg DPI BID þFluticasone 200 mg DPI BD
SGRQ 84 21 weeks
Bateman ED (2010) Tiotropium 5 mg Respimat ODTiotropium 10 mg Respimat ODPlacebo
SGRQ 1990 52 weeks
Hoshino M (2010) Tiotropium 18 mg DPI ODTiotropium 18 mg DPI ODþSalmeterol 50 mg þ Fluticasone250 mg DPI BID
SGRQ 36 12 weeks
Bateman ED (2010) Tiotropium 5 mg Respimat ODTiotropium 10 mg Respimat ODPlacebo
SGRQ 3991 48 weeks
Abe T (2011) Tiotropium 18 mg DPI ODTiotropium 18 mg DPI OD þTulobuterol 2 mg OD td
SGRQ 16 8 weeks
1470 F. Braido et al.
improved all SGRQ domains compared both to placebo andipratropium, formoterol 24 mg induced a significantimprovement in Symptoms and Activity only whencompared to placebo.
On the contrary, no difference in SGRQ Total Score,Activity and Impacts were reported between formoterol12 mg, ipratropium 80 mg and placebo by Wadbo [25]. OnlySymptoms showed an improvement of 9 units in ipratropium
Figure 1 SGRQ total score change from basel
bromide vs placebo and 5.7 versus formoterol, but the levelof significance was not reported.
In another trial, both formoterol and theophyllinesignificantly improved SGRQ total score (formoterol 12 mgBID P Z 0.030, formoterol 24 mg BID P Z 0.009, andtheophylline P Z 0.03 respectively) compared to placebo.The SGRQ domains showed different improvements in eachactive group: formoterol 12 mg improved Symptoms
ine to the end of the study in active group.

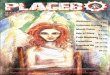
Figure 2 SGRQ differences in change from baseline to the end of the study between active group and placebo.
LABA/LAMA effects on COPD health status 1471
(P Z 0.009), formoterol 24 mg Impacts (P Z 0.016) andtheophylline Activity (P Z 0.003). Neither the significanceof SGRQ score changes for each treatment nor the com-parison among active treatments effect on HRQoL/HS werereported [26].
Formoterol in fixed dose plus as needed showed a similarHRQoL/HS improvement compared to formoterol or pla-cebo in fixed dose plus terbutaline as needed. Significanttreatment differences were reported at the end of thestudy only in Symptoms: formoterol BID þ terbutaline prnvs. placebo (�5.47; P Z 0.002) and formoterolBID þ formoterol prn vs. formoterol BID þ terbutaline(�4.63; P Z 0.007) [22].
Both formoterol administered once daily (OD) and BIDimproved SGRQ total score and domains. The MID wasreached only for the Impacts in patients treated with for-moterol BID. The between-groups comparison was not re-ported [29].
Baumgartner [23] showed a dose-related greaterimprovement in SGRQ total scores (2.6e3.6 units) withnebulized arformoterol than placebo (1.2), but inferior tosalmeterol (4.4). The greatest changes were observed inthe Symptoms for all active treatments, with salmeterol asbest performer.
Similarly, Hanania [27] showed an improvement in alltreatment groups, but clinically significant only for for-moterol 12 mg. The proportion of subjects who reached MIDin SGRQ at week 26 was 45.7% for arformeterol 15 mg, 43.3%for arformeterol 25 mg and 56.7% for formoterol 12 mg.
A 12-week treatment with nebulized formoterol fuma-rate and formoterol DPI BID demonstrated that the firsttreatment was associated with statistically significant andclinically meaningful improvements in Total, Symptoms andImpacts scores compared to placebo (P < 0.03), while nosignificant difference was detected in Activity. FormoterolDPI significantly improved Symptoms, while no significant
differences were found in Total or domain scores betweenactive treatments [28].
Salmeterol
A total of 2079 moderateesevere patients were randomizedin 7 trials. HRQoL/HS were assessed in 3 studies with SGRQ,in 3 with SF-36 and in 1 with Chronic Respiratory DiseaseQuestionnaire (CRDQ) [30]. The duration of the studiesranged from 10 weeks to 12 months, and comparators ofsalmeterol were ipratropium [31], theophylline [32,33] andplacebo [31,34e37].
Salmeterol was tested as MDI 25/42/50/100 mg BID[31e35] and DPI 50 mg BID [36,37].
Randomized patients could receive concomitant treat-ments with ICS [31e37], oral steroids [32,34,36,37],xanthine [34,36,37], short acting anticholinergics [34e38],cromoglycate, nedocromil, ketotifen [32], or short actingb2 agonists prn [31e35,37].
In patients belonging to a large cohort study [38], sal-meterol 50 mg significantly improved SGRQ total and Im-pacts scores, with changes that exceeded the MIDcompared to placebo [34]. No difference was detected inSGRQ scores between placebo and salmeterol 100 mg. Withthe exception of Role Emotional, no significant differencein SF-36 scores between placebo and active groups wasfound. Differences emerged by comparing the two doses ofSalmeterol: changes with salmeterol 50 mg were signifi-cantly greater than those whit salmeterol 100 mg in SGRQTotal score and some SF-36 domains, due to a worsening ofHS with salmeterol 100 mg and an improvement with sal-meterol 50 mg. The same authors published in 2003 afurther analysis of a sub-population of the Boyd’s study,showing that 59% of patients in the salmeterol 50 mg BID

1472 F. Braido et al.
group and only 38% in placebo group reported an improve-ment of SGRQ exceeding the MID [39].
In a one-year trial both salmeterol and theophyllinesignificantly improved all SF-36 dimensions, with differ-ences in favour of Salmeterol group at different timepoints: in Physical Functioning after 3 months (10.34 withSalmeterol vs 3.79 with theophylline, P Z 0.02), in GeneralHealth after 9 months (24.25 vs 14.41; P Z 0.02) and inSocial Functioning after 12 months (15.13 vs 6.84;P Z 0.04). Moreover, the salmeterol group showed a largereffect size in all SF-36 domains [32].
A similar study showed an improvement of SF-36 PhysicalFunctioning and Change in Health in both treatment groups,with a greater improvement in salmeterol, although thesignificance versus comparator and placebo was not re-ported [33].
CRDQ was used [31] to evaluate the efficacy of salme-terol and ipratropium versus placebo. The overall CRDQscore increased in all treatment groups (placebo: 6.8; sal-meterol: 10.3; ipratropium 9.2), without any significantdifference between them. The proportion of patients whoreached the MID was 38, 46 and 41% for placebo, salmeteroland ipratropium, respectively.
Salmeterol administered as an add-on drug to Ipratropiumimproved all SF-36 dimensions, with the exception of RoleLimitation Emotional, whereas in the placebo group RoleLimitations Emotional, Physical Functioning and Role Limita-tion Physical did not improve. Themagnitude of improvementwas significantly greater inpatients treatedwith salmeterol inthe dimensions in which both groups ameliorated [35].
In patients treated with inhaled anticholinergic therapy,salmeterol improved SGRQ Symptoms (P Z 0.003), Impacts(P Z 0.05) and Total score (P Z 0.05), whereas no signifi-cant changes were observed with placebo. Nevertheless,the between-treatment differences in SGRQ were not sta-tistically significant [36].
In a similar study, the addition of salmeterol to usualtreatment (methylxanthines, short acting anticholinergicagents, mucolytics) induced an improvement of SGRQscores at all visits (4, 28 and 52 weeks), which becamestatistically significant at weeks 52 for all dimensions,compared to placebo [37].
Indacaterol
The effect of Indacaterol on HRQoL/HS was explored in 6trials [40e45] randomizing a total of 5820 patients withmoderateesevere COPD. HRQoL/HS were evaluated alwaysas secondary outcome using SGRQ. Study duration rangedfrom 12 weeks to 12 months, and comparators of indaca-terol were different dosages of indacaterol itself[40e42,44], formoterol [40,41], salmeterol [43], tiotropuim[40,42] placebo [40e44]. Indacaterol was tested as 75 [43],150 [40,42,43,45], 300 [40e42,45] or 600 mg OD DPI [41].
HRQoL/HS were evaluated always considering patientswith concomitant ongoing treatments represented by ICS[40e45] and short acting b2 agonist prn [41e45].
In a study performed by Donohue [40], indacaterol 150and 300 mg improved SGRQ scores, compared to placebo, atall assessments (P Z 0.01), while no differences wereregistered versus tiotropium.
At both doses of 300 and 600 mg indacaterol significantlyimproved SGRQ total score compared to placebo, with agreater effect than twice-daily formoterol 12 mg, althoughthe difference did not reach statistical significance [41].
In a one-year study [42], the change in mean SGRQ totalscores was higher with both indacaterol 150 and 300 mg thanwith placebo at all assessments, and significantly higher atweek 26 (150 mg, P Z 0.002; 300 mg, P Z 0.025) and week44 (P Z 0.002 for both). In a shorter trial, SGRQ total scorewas significantly lower than placebo for Indacaterol 150 mg(P Z 0.005) and indacaterol 300 mg (P Z 0.001), with bothdifferences exceeding the MID. This improvement wasconsistent across the three SGRQ domains (P < 0.05). Thepercentage of patients with an improvement from baselineexceeding the MID were consistently higher in indacaterolgroups than placebo, although the difference reached sta-tistical significance only for indacaterol 300 mg [45]. Korn-mann [43] showed that, compared to placebo, Indacaterol150 mg improved SGRQ scores by a margin that was close to(week 4) or exceeded (weeks 8e26) the MID, and a supe-riority to salmeterol (P Z 0.05) at week 12 was reported.
Two identically designed trials tested Indacaterol 75 mgOD versus placebo. At week 4, the SGRQ total score changewas statistically significant versus placebo only in Study 1(P < 0.01), while at week 12 this change was significant inboth studies, with differences of �3.8 and �3.6 (P � 0.01)[44].
Long acting anticholinergic(S)
A total of 23 trials fulfilled the selection criteria (2 glyco-pyrronium, 3 aclidinium, 18 tiotropium), with an overallrandomized population of 22,653 patients. The duration ofthe studies ranged from 4 weeks to 4 years. HRQoL/HS wereinvestigated as primary outcome in 2 out of 23 studies. Thechange in SGRQ Total score from baseline to the end of thestudy in patients treated with Long acting anticholinergicsand the difference in SGRQ Total score between the abovementioned change and that in the placebo group are shownin Figs. 3 and 4.
Glycopyrronium
The effect of glycopyrronium on HRQoL/HS has beenexplored in 2 trials [46,47] randomizing 1888 patients withmoderateesevere COPD. HRQoL/HS were assessed as sec-ondary outcome, using the SGRQ. The comparators of gly-copyrronium were placebo [46,47] and tiotropium [46].
Glycopyrronium was tested as single dose dry powderinhaler (SDDPI) [46,47] at dose of 50 mg OD. Randomizedpatients could receive concomitant treatments with ICS,intranasal corticosterid, H1 antagonist, albuterol, salbuta-mol [46,47].
In the GLOW1 study [46], after 26 weeks, the patientstreated with glycopyrronium bromide 50 mg OD comparedto those treated with placebo reported a significantly lowerSGRQ score (P Z 0.004), with a treatment difference whichdoes not reach the MID (2.81). Moreover, the percentageof patients who reached the MID was significantly higherin the active group vs placebo (56.8% vs 46.3%; oddsratio 1.58).

Figure 3 SGRQ total score change from baseline to the end of the study in active group.
LABA/LAMA effects on COPD health status 1473
The GLOW2 study [47] evaluated the efficacy of glyco-pirronium bromide compared with placebo and tiotropiumover 52 weeks. At the study end, SGRQ total score wassignificantly improved in patients receiving glycopyrronium(�3.32; P < 0.001) and tiotropium (�2.84; P Z 0.014)compared to placebo. Moreover, the percentage of patientsachieving the MID was higher with glycopyrronium (54.3%)and tiotropium (59.4%) than with placebo (50.8%).
Aclidinium
The effect of aclidinium on HRQoL/HS has been explored in3 trials [48e50] randomizing 2939 patients with moder-ateesevere COPD. HRQoL was assessed as secondaryoutcome in both studies, using the SGRQ. The study dura-tion ranged from 4 [48] to 52 weeks [49], and comparatorsof aclidinium were placebo [48e50] and tiotropium [48].
Figure 4 SGRQ differences in change from baseline to th
Aclidinium was tested as novel multidose dry-powderinhaler at dosed of 25, 50, 100 or 200 mg [47,49], and 200 mg[48e50]. Randomized patients could receive concomitanttreatments with ICS [48e50], oral theophylline [48e50],anthistamines [48], nedocromil [48], ketotifen [48], inhaledsalbutamol [49,50], oral or parenteral corticosteroids[49,50], oxygen therapy [50].
In a 4 weeks’ study, Chanez [48] evaluated the effect offive different doses of aclidinium (25, 50, 100, 200, or 400 mg)OD compared to placebo or tiotropium 18 mg. An HRQoLimprovement was found with all doses of aclidinium. Thepercentage of patients reaching theMID ranged from52.6% inthe 400mg group to 64.4% in the 100mg group.No comparisonswere reported among the different treatment groups.
Jones [49] reported the results of two identical 52-weekstudies comparing aclidinium 200 mg and placebo. At theend of the treatment period, a higher percentage of
e end of the study between active group and placebo.

1474 F. Braido et al.
patients of active group reached the MID in the Study 1(48.1% vs 39.5%, PZ 0.025) but not in Study 2. At week 52,the mean improvement from baseline in SGRQ total scorewas greater for aclidinium compared to placebo in bothstudies, with a significant difference shown only in Study 2(�3.49 vs �1.28; P Z 0.021).
The same author explored the effects of two differentdoses of aclidinium. The improvement SGRQ total score ofaclidinium 200 mg versus placebo was �3.8 ( P < 0.001)While with Aclidinium 400 was �4.6 (P < 0.0001). Thepercentage of patients who reached the MID at the studyend was significantly higher both with aclidinium 200 mg(56%; OR 1.83 P< 0.001) and 400 mg (57.3; 1.87 P < 0.001)compared to placebo [50].
Tiotropium
The effect of tiotropium on HRQoL/HS has been explored in18 trials [51e68] randomizing 17,826 patients with moder-ateesevere COPD (Table 2). HRQoL/HS were evaluatedusing SGRQ in 16 trials, EQ-5D and SF-36 in 2, and the VisualSimplified Respiratory Questionnaire (VSRQ) in one.Importantly, HRQoL/HS were investigated as primaryoutcome in 2 out of 18 studies [62,65]. The study durationranged from 6 weeks to 4 years, and comparators of tio-tropium were ipratropium [51], salmeterol [52,53], placebo[53e57,59e63,65,66], tiotropium plus budesonide [58],salmeterol plus futicasone propionate [64,67], differentdoses of tiotropium [65], or tiotropium plus salmeterol/fluticasone propionate [68].
Tiotropium was tested as 18 mg OD Handihaler[51e64,67,68] or 5e10 mg OD Respimat [65,66], andconcomitant ongoing treatments were represented by ICS[51,52,54e57,59,61e64,68], long acting b2 agonists[56,59,61], oral steroids [51,52,54,55,57e63,65,66], theoph-ylline [51,54e57,59,61e63,65,66], antileukotrienes [65] andshort acting b2 agonist on demand [52,54e61,63,66e68].
The Dutch/Belgian Tiotropium Study Group describedthe combined results of two 1-year trials. The SGRQ totalscore improved both in tiotropium and ipratropium group,but gradually returned towards baseline in patients treatedwith the short acting. At the end of the study, a significantdifference in SGRQ total score (P < 0.05) and in the Impactscore (P Z 0.001) was found between the two groups, witha greater HRQoL/HS improvement in the tiotropium arm.Moreover, a significantly higher percentage of patientstreated with tiotropium reached the MID after 9 and 12months (52% versus 35% respectively at 1 year, P Z 0.001).Patients treated with tiotropium had higher SF-36 in allphysical domains, but at the end of the study the differ-ences between the two treatment arms were significantonly for Role Physical (P Z 0.033) and Physical ComponentSummary (P Z 0.015) [51].
Tiotropium improved SGRQ total score more than pla-cebo (P < 0.05), whereas this effect was not reached by thesalmeterol group (P Z 0.39). The difference between tio-tropium and salmeterol (�1.6) did not reach statisticalsignificance. The improvement in SGRQ Impacts score at 6months was: �5.24 (P < 0.05 vs placebo) in tiotropium,�2.37 (P Z 0.98 vs placebo) in salmeterol and �2.33 inplacebo. The improvements observed with tiotropium
appeared to increase over time, and it was superior toplacebo and salmeterol (P < 0.05) with regard to the pro-portion of patients reaching the MID, whereas salmeterolwas not statistically different from placebo [52].
In a similar study on 1207 patients [53], the SGRQ totalscore improved by 4.2 units in tiotropium group, 2.8 in thesalmeterol, and 1.5 in placebo. A significant difference wasobserved only for tiotropium vs placebo (P < 0.01). Thepercentage of patients achieving the MID was higher in thetiotropium group (P < 0.05 for tiotropium vs placebo) inboth studies, while salmeterol was associated with thisfinding in one.
Casaburi [54] showed that tiotropium induces a signifi-cant improvement of SGRQ total score and domainscompared to placebo. A significantly higher percentage ofpatients in the tiotropium group (49%) showed animprovement exceeding MID compared to placebo (30%).Moreover, patients taking tiotropium had a significantimprovement in Physical health domains of SF-36 comparedto placebo (Physical Function, Role Physical, GeneralHealth and Physical Summary score). No significant differ-ences in Mental Health Summary were detected apart fromVitality and Social Function in favour of tiotropium on 4 outof 5 times of evaluations. 713 patients out of the 921enrolled in this study underwent a pre-planned withdrawalof tiotropium. A worsening of SGRQ, although not signifi-cant, was observed [69].
COPD patients participating in a 8-week pulmonaryrehabilitation program received tiotropium or placebo for24 weeks. At study end the SGRQ total score in the tio-tropium group was better than in the placebo. After pul-monary rehabilitation the SGRQ total score improved by7.27 units in the tiotropium and 3.41 in the placebo groupalthough the difference was not significant. The differencebetween groups at the end of the study exceeded the MIDand approached the statistical significance (P Z 0.055)[55]. A post hoc analysis of this study [70] performed onpatients untreated with respiratory medication or treatedonly with as-needed short-acting beta-agonists prior toenrolment, showed an improvement of �5.2 greater in thetiotropium group compared to placebo (P < 0.05). SGRQActivity and Impacts scores improved significantly more inthose treated with tiotropium than with placebo.
The effect of tiotropium on exercise endurance wasassessed in a 12-week study [57] that evaluated HRQoL/HS atdays 1, 42 and 84 of treatment. A statistically and clinicallysignificant difference in the SGRQ Total and Impacts scoresbetween tiotropium and placebo was found at day 84 and forActivity only at day 42. A greater rate of patients treatedwith tiotropium (59% vs 35%, P < 0.05) reached the MID.
Also Ambrosino [61] compared tiotropium and placebo inenhancing the effects of exercise training. The SGRQ Totalscore improved after treatment and remained stable inboth groups, and trended towards a lower score on eachtest day in tiotropium compared to placebo group. Thechanges at study end were �6.0 (33.1 vs 39.1) and �7.3(31.8 vs 39.1) in the placebo and tiotropium groups,respectively. Improvements in groups exceeded the MIDboth after pulmonary rehabilitation and at the end of thefollow-up period.
Tiotropium was associated with statistically significantimprovements in HRQoL/HS assessed with EQ-5D visual

LABA/LAMA effects on COPD health status 1475
analogue scale scores (P < 0.01) and with nonestatisticallysignificant trends in the five component questions versusplacebo [56]. Viceversa, no difference in EQ-5D betweengroups was found in total score between tiotropium andplacebo in a study that lacks of detailed statistical analysisand patient pre-treatment information [60]. In 913 patientsrandomly assigned to receive tiotropium or placebo for 48weeks, a significant improvement of SGRQ Total score,(40.9 vs 43.7, P < 0.01), Symptoms score (44.4 versus49.3, P< 0,01), and Impacts score (28.5 vs 31.3, P < 0.001)compared to placebo. A score exceeding the MID was ach-ieved by 53% of patients in the active and 44% in placebogroup (P Z 0.052) [59].
HRQoL/HS were the primary outcome of a trial wherepatients treated with tiotropium were compared to pla-cebo. More patients treated with tiotropium (59.1% vs48.2%) reached the MID with a mean change of SGRQ totalscore from baseline of �8.50 for tiotropium vs �4.32 forplacebo (P < 0.05). Tiotropium, compared to placebo,significantly improved all SGRQ subscores (P < 0.05) [62].
In the UPLIFT study HRQoL/HS were explored as a sec-ondary outcome every 6 months using the SGRQ. Significantdifferences in favour of tiotropium versus placebo wereobserved at all points for the mean change in SGRQ totalscore (ranging from 2.3 to 3.3 units, P < 0.001). However,both at 12 and 48 months the SGRQ improvement did notreach the MID. A higher proportion of patients in the tio-tropium than in the placebo group reported an improve-ment exceeding the MID from baseline at 1 year (49% vs41%), 2 years (48% vs 39%), 3 years (46% vs 37%) and 4 years(45% vs 36%) (P < 0.001 for all comparisons) [63]. Pre-specified subpopulation analyses of the UPLIFT populationhave been developed.
Celli showed that, at study end, HRQoL/HS in the tio-tropium group had not returned to the baseline value [71].Decramer focused on the 2039 patients with GOLD stage II.In both tiotropium and control groups, SGRQ total scoresimproved relative to baseline over the first 6 months.Thereafter, a similar, progressive HRQoL/HS deteriorationin both groups was detected. However, at all time pointsHRQoL/HS were better in the tiotropium than in the controlgroup (P � 0.006), with differences ranging from 2.7 to 4.0for the total score [72]. The analysis according to self-reporting smoking habit showed a SGRQ improvement intiotropium greater in continuing smokers (�4.63,P Z 0.0006) than continuing former (�2.74, P < 0.001) andintermittent smokers (�0.60, P Z 0.51) [73].
Troosters focused on 810 COPD patients of the UPLIFTstudy not receiving other maintenance treatment (LABA,short acting b2 agonist e SABA, ICS, xanthines) at random-ization. SGRQ total score improved in the first 6 months inboth groups, with a greater improvement (�2.29) in thetiotropium group, although the MID was not reached.Moreover, SGRQ total score worsened more slowly in thetiotropium arm. The difference between groups exceededthe MID after 25.5 months and remained above the MIDthereafter. Different decline in the Impacts (PZ 0.004) andActivity scores (P < 0.001) significantly favoured the tio-tropium group, whereas no difference for Symptoms wasfound. At 48 months, the difference in total score was 4.6units (P < 0.001) in favour of tiotropium [74]. The influenceof gender on long-term responses to tiotropium was
explored. Both men and women showed statistically sig-nificant improvements in SGRQ total score. Women re-ported a baseline worse HRQoL/HS despite a similar diseaseseverity. Interestingly, total SGRQ score at the study endtended to improve from baseline with tiotropium more inwomen than in men [75].
In 100 patients the effects of tiotropium alone or addedto budesonide was studied. Tiotropium alone was able toimprove the SGRQ total score of 2.8 versus 5.6 when addedto budesonide with a greater proportion of patientsachieving the MID for the last treatment plan (73.2 vs 42.5;P Z 0.007) [58].
In an open cross-over study, significant improvements inSGRQ scores were found both for tiotropium and salmeterol/fluticasone (SFC) (P < 0.001), without differences betweengroups. At study end, patients were asked to choose onetreatment. Patients who selected SFC reported a significantgreater improvement in Symptoms (P < 0.05) and in Impacts(P Z 0.02). Similarly Patients who selected tiotropiumshowed a greater improvement in Activity (P Z 0.03) [64].
Bateman performed three trials using tiotropiumadministered via Respimat. Two identical studies random-ized a total of 1990 patients and had HRQoL among the 4co-primary endpoints. The improvement in SGRQ totalscore for both tiotropium doses was statistically superior toplacebo (�3.5 [Tio 5 mg- placebo] and �3.8 [Tio 10 mg-placebo]; P < 0.0001), and the adjusted mean change frombaseline to week 48 exceeded the MID after active treat-ment in both studies [65].
In another trial 3991 COPD patients were randomised toreceive tiotropium Respimat 5 mg or placebo. Total SGRQscore improved from baseline in both groups, with asignificantly greater change with tiotropium. Mean differ-ences in total scores between tiotropium and placebo were�2.2 at week 24 and -2.9 at week 48 (P < 0.0001 at bothtime points). The proportion of patients who reached theMID was significantly higher in the tiotropium group: 50.9%vs 42% at week 24, and 49.5% vs 41.4% at week 48(P < 0.0001 at both time points) [66].
Hoshino compared the effects on HRQoL/HS of SFC addon with tiotropium and tiotropium alone. Treatment withSFC plus tiotropium, but not tiotropium alone, resulted insignificant improvements of SGRQ scores, compared tobaseline. Between-group comparisons indicated signifi-cantly greater improvements in SGRQ total and domainsscores (P < 0.05) in triple treatment [67].
A Japanese study compared the effects of inhaled tio-tropium added to transdermal Tulobuterol versus tio-tropium alone. Total score and Activity improvedsignificantly following combination therapy, without anysignificant difference between the two groups. Symptomsimproved significantly following tiotropium monotherapy(33.0 vs 34.3; P < 0.01) while Impacts significantlyimproved in combination therapy compared to mono-therapy ( < 0.05) [68].
Long acting beta2 agonists (LABA) plus long-acting muscarinic antagonist (LAMA)
The effects on HRQoL of LABA/LAMA combination treat-ment were explored in 6 trials for a total of 2359

1476 F. Braido et al.
randomized patients [76e81]. Comparator drugs were for-moterol [77,79], tiotropium [77,78], salmeterol and SFC[76,81]. HRQoL/HS were evaluated in all studies as sec-ondary outcome using SGRQ, and the study duration rangedfrom 6 weeks to 12 months.
HRQoL/HS were evaluated considering always patientswith concomitant ongoing treatments represented by ICS[76e80], SABA prn [79e81] and salbutamol [81].
In 449 patients, randomized to receive tiotropium 18 mgDPI OD alone or plus SFC 50/250 mg MDI BID or salmeterol50 mg MDI BID, the association LAMA/LABA and the tripletreatment improved HRQoL more than tiotropium (P < 0.02and 0.01 respectively) [76].
Tashkin studied 130 patients treated with formoterolfumarate 20 mg/2 ml Pari Nebulizer BID/tiotropium18 mg DPIOD or placebo Pari Nebulizer BID/tiotropium 18 mg DPI ODfor 6 weeks. The only statistical and clinical differencebetween treatments was observed in SGRQ Symptoms infavour of formoterol fumarate/tiotropium (PZ 0.004) [77].
847 patients were randomized in 4 groups of treatments(formoterol 10 mg DPI BID, placebo DPI BID, tiotropium 18 mgOD DPI/formoterol 10 mg DPI BID, tiotropium 18 mg OD). Nosignificant differences in SGRQ total score were found be-tween combined therapy and either monotherapy.Compared to placebo, all active treatments significantlyimproved SGRQ total score (P < 0.005) [78].
No difference after the introduction of formoterol fuma-rate 20 mg/2 ml Pari Nebulizer BID or placebo as add ontreatment to tiotropium 18 mg DPI OD was found in a 6 weeksstudy on 155 patients, although a higher percentage of pa-tients receivingLAMA/LABA (61%vs21%) reached theMID [79].
A similar trial was performed by Tashkin on 255 patients.The results of this 12-week study showed that Symptoms wassignificantly improved by LAMA/LABA compared to LAMAalone. However LAMA/LABA group reached the MID for Total,Symptoms and Impacts scores, while in tiotropium alone theMID was reached only in the Activity score [80].
The ILLUMINATE study [81] on 523 patients showed that,after a 26-week treatment with indacaterol plus glyco-pyrronium via Breezhaler 110/50 mg or salmeterole-fluticasone 50/500 mg, SGRQ scores improved in bothtreatment groups, without any significant difference be-tween them [81].
Discussion
The effects of bronchodilators on patient’s HRQoL/HS is acrucial issue. A recent review by Karner [82] showed that,compared to placebo, tiotropium treatment significantlyimproved the mean quality of life and increased the num-ber of participants who reached the MID. Jones [83]reviewed the efficacy of indacaterol compared to placeboas a bronchodilator and reported that the MID was achievedin 2 studies out of 4 in indacaterol 150 mg. On the otherhand, in a review by Chong [84] assessing the relativeclinical effects of tiotropium bromide alone versus LABAalone, due to a high level of heterogeneity amongst studies,it was not possible to pool data for SGRQ quality of lifescore.
A consistent sample of moderate-severe COPD patientshas been studied testing 6 drugs, 12 different devices, 22
different dosages with a study duration ranging from 4weeks to 4 years. SGRQ has been used in 86% of studies and,while total score was always reported, domains wereconsidered in only 60% of cases. A recent review providing acomprehensive evaluation of the content and psychometricproperty of available HRQoL/HS questionnaires for COPDhas recommended the use of specific instruments ratherthan generic ones. The authors underline that no optimalinstrument exists, but the choice of a questionnaire shouldderive from the aims of the study and from the tool char-acteristics in terms of questions and domains. This aspect ismissing in the papers we reviewed, since the use of aquestionnaire is not motivated on the basis of the effectson patients’ life that researchers expected from thetreatment. Each questionnaire focuses on particular areasand ignores other ones. For example, SGRQ, despite beingone of the instruments with the strongest positive evi-dences in terms of structural validity and reliability, doesnot investigate some domains relevant for COPD patientssuch as mobility, social functioning, sleep [85].
The data coming from the above mentioned researchframework support the efficacy of long acting bronchodi-lators in improving HRQoL/HS of COPD patients. This hasbeen shown in 7/8 trials testing formoterol, 7/7 salmeterol,5/6 indacaterol and 17/18 tiotropium, 2/2 glycopyrroniumand 3/3 aclidinium. Pre-post values in active group werereported in 77%, and 75% of trials indicated the differencein HRQoL/HS change between active and placebo groups.
Although a statistical significant HRQoL/HS improvementwas reached in 93% of cases, the MID was reached in 70,6%of the studies considering the difference between baselineand end of the study, and in 50% of the studies comparingactive treatment and placebo. Taking into considerationwhat constitutes important difference in HRQoL scoresbeyond the statistical significance of the result is relevantfor interpreting intervention effects on HRQoL. Since only 2trials [62,65] have explored HRQoL/HS as a primaryoutcome, these results must be carefully considered.Moreover, all randomized patients have been allowed totake concomitant drugs such as ICS. A recent systematicreview, considering all published RCTs of regular ICS inCOPD, showed a small but statistically significant benefitfor HRQoL/HS using ICS. In particular, in those long-termstudies ICS slowed the rate of decline in HRQoL, with aneffect that appears linear, despite the fact that themagnitude of this benefit was relatively small (MID -1.22units/year) [86]. For the above mentioned reasons the ef-fects of bronchodilators on HRQoL/HS could be greater thanthose shown. Interestingly, in some trials comparingdifferent dosages of the same bronchodilator, the higherdosage seems related to worse HRQL/HS [24,25,28,35]. Thisevidence should be explained considering that, from thepatient’s perspective, the burden of a more challengingtreatment could be detrimental.
Although few trials have been published exploring theefficacy of LAMA/LABA combination on HRQoL/HS, thisapproach demonstrates greater efficacy than individualdrugs alone [87]. Tt is likely that the functional improve-ment of clinical parameters may imply an improvement inHRQoL, but, at present, the effect of bronchodilation wasstudied only in a limited number of patients. Despite thepositive results, more data are needed. A recent

LABA/LAMA effects on COPD health status 1477
metanalysis confirmed the above mentioned results un-derlying that although the HRQoL/HS improvement wasstatistically significant it did not reach the MID, and qualityof the evidence according to GRADE was moderate [88].The efficacy of bronchodilators on HRQoL/HS as a measureof overall treatment effectiveness is shown and remains acrucial outcome in clinical research.
Conflict of interest statement
The authors declare that the submitted material is original,is not currently under consideration nor has been acceptedfor publication or published elsewhere. There are nocompeting interests. The authors report no sources offunding.
Acknowledgements
The study was supported by ARMIA (Associazione RicercaMalattie Immunologiche e Allergiche).
The authors thank ASPADIRES (Associazione PazientiDisturbi Respiratori nel Sonno) and acknowledge DrMarianna Bruzzone for linguistic assistance with themanuscript.
References
[1] Schipper H, Clinch J, Olweny CLM. Quality of life studies:definitions and conceptual issues. In: Spilker B, editor.Quality of life and pharmacoeconomics in clinical trials.Philadelphia: Lippincot-Raven Press; 1990. p. 11e23.
[2] Spertus JA, Tooley J, Jones P, Poston C, Mahoney E,Deedwania P, Hurley S, Pitt B, Weintraub WS. Expanding theoutcomes in clinical trials of heart failure: the quality of lifeand economic components of EPHESUS (E Plerenone’s neuroHormonal Efficacy and Survival Study). Am Heart J 2002;143:636e42.
[3] Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. A conceptual model of patient out-comes. JAMA 1995;4(273):59e65.
[4] De Vries J. Quality of life assessment. In: Vingerhoets AJJN,editor. Assessment in behavioural medicine. Hove, UK:Brunner-Routledge; 2001. p. 353e70.
[5] Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 Health Sur-vey. Manual and interpretation guide. Boston: Health Insti-tute, New England Medical Center; 1993.
[6] Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limi-tation. The St. George’s Respiratory Questionnaire. Am RevRespir Dis 1992;145:1321e7.
[7] Cazzola M, MacNee W, Martinez FJ, Rabe KF, Franciosi LG,Barnes PJ, Brusasco V, Burge PS, Calverley PM, Celli BR,Jones PW, Mahler DA, Make B, Miravitlles M, Page CP,Palange P, Parr D, Pistolesi M, Rennard SI, Rutten-vanMolken MP, Stockley R, Sullivan SD, Wedzicha JA, Wouters EF,American Thoracic Society, European Respiratory SocietyTask Force on outcomes of COPD. Outcomes for COPD phar-macological trials: from lung function to biomarkers. EurRespir J 2008;31:416e69.
[8] Curtis JR, Patrick DL. The assessment of health status amongpatients with COPD. Eur Respir J 2003;41:36e45.
[9] Jones PW, Brusselle G, Negro RW, Ferrer M, Kardos P, Levy ML,Perez T, Cataluna JJ, van der Molen T, Adamek L, Banik N.
Patient-centred assessment of COPD in primary care: experi-ence from a cross-sectional study of health-related quality oflife in Europe. Prim Care Respir J 2012;21:329e36.
[10] Jones PW. Activity limitation and quality of life in COPD.COPD 2007;4:273e8.
[11] Braido F, Baiardini I, Menoni S, Bagnasco AM, Balbi F,Bocchibianchi S, Balestracci S, Piroddi MG, Canonica GW.Disability in COPD and its relationship to clinical and patient-reported outcomes. Curr Med Res Opin 2011;27:981e6.
[12] Braido F, Baiardini I, Balestracci S, Menoni S, Balbi F,Ferraioli G, Bocchibianchi S, Canonica GW. Chronic obstruc-tive pulmonary disease patient well-being and its relation-ship with clinical and patient-reported outcomes: a real-lifeobservational study. Respiration 2011;82:335e40.
[13] US Department of Health and Human Services FDA Center forDrug Evaluation and Research, US Department of Health andHuman Services FDA Center for Biologics Evaluation andResearch and US Department of Health and Human ServicesFDA Center for Devices and Radiological Health. Guidance forIndustry: patient reported outcome measures: use in medicalproduct development to support labelling claims: draftguidance. Health Qual Life Outcome. 2006;4:79.
[14] Reflection paper on the regulatory guidance for the use ofhealth-related quality of life (HRQoL) measures in the eval-uation of medicinal products. European Medicines Agency.Committee for medicinal products for human use (CHMP);2005. European Medicines Agency website. Available at:http://www.emea.europa.eu/pdfs/human/ewp/13939104en.pdf. Accessed June 2009.
[15] Preamble to the constitution of theworld healthorganization asadopted by the international health conference, New York, 19Junee22 July 1946; signed on 22 July 1946 by the representa-tives of 61 States (Official Records of the World Health Organi-zation, no. 2, p. 100) and entered into force on 7 April 1948.
[16] Braido F, Bousquet PJ, Brzoza Z, Canonica GW, Compalati E,Fiocchi A, Fokkens W, Gerth van Wijk R, La Grutta S,Lombardi C, Maurer M, Pinto AM, Ridolo E, Senna GE,Terreehorst I, Todo Bom A, Bousquet J, Zuberbier T,Baiardini I. Specific recommendations for PROs and HRQoLassessment in allergic rhinitis and/or asthma: a GA(2)LENtaskforce position paper. Allergy 2010;65:959e68.
[17] Guyatt GH, Oxman AD, Vist G, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. Rating quality of evidence and strength ofrecommendations GRADE: an emerging consensus on ratingquality of evidence and strength of recommendations. BMJ2008;336:924e6.
[18] Global strategy for the diagnosis, management and preven-tion of chronic pulmonary disease. Global Initiative forChronic Obstructive Lung Disease (GOLD); 2011http://www.goldcopd.org/Guidelines/guidelines-resources.html.
[19] O’Reilly J, Jones MM, Parnham J, et al. Management of stablechronic obstructive pulmonary disease in primary and secondarycare: summary of updated NICE guidance. BMJ 2010;340:c3134.
[20] Guyatt GH, Osoba D, Wu AW, Wyrwich KW, Norman GR.,Clinical Significance Consensus Meeting Group. Methods toexplain the clinical significance of health status measures.Mayo Clin Proc 2002;77:371e83.
[21] Global strategy for diagnosis, management, and preventionof COPD update, http://www.goldcopd.org; 2009.
[22] Campbell M, Eliraz A, Johansson G, Tornling G, Nihlen U,Bengtsson T, Rabe KF. Formoterol for maintenance and as-needed treatment of chronic obstructive pulmonary dis-ease. Respir Med 2005;99:1511e20.
[23] Baumgartner RA, Hanania NA, Calhoun WJ, Sahn SA,Sciarappa K, Hanrahan JP. Nebulized arformoterol in patientswith COPD: a 12-week, multicenter, randomized, double-blind, double-dummy, placebo- and active-controlled trial.Clin Ther 2007;29:261e78.

1478 F. Braido et al.
[24] Dahl R, Greefhorst LA, Nowak D, Nonikov V, Byrne AM,Thomson MH, Till D, Della Cioppa G., Formoterol in ChronicObstructive Pulmonary Disease I Study Group. Inhaled for-moterol dry powder versus ipratropium bromide in chronicobstructive pulmonary disease. Am J Respir Crit Care Med2001;164:778e84.
[25] Wadbo M, Lofdahl CG, Larsson K, Skoogh BE, Tornling G,Arwestrom E, Bengtsson T, Strom K, Swedish Society ofRespiratory Medicine. Source effects of formoterol andipratropium bromide in COPD: a 3-month placebo-controlledstudy. Eur Respir J 2002;20:1138e46.
[26] Rossi A, Kristufek P, Levine BE, Thomson MH, Till D,Kottakis J, Della Cioppa G., Formoterol in Chronic Obstruc-tive Pulmonary Disease (FICOPD) II Study Group. Comparisonof the efficacy, tolerability, and safety of formoterol drypowder and oral, slow-release theophylline in the treatmentof COPD. Chest 2002;121:1058e69.
[27] Hanania NA, Donohue JF, Nelson H, Sciarappa K, Goodwin E,Baumgartner RA, Hanrahan JP. The safety and efficacy ofarformoterol and formoterol in COPD. COPD 2010;7:17e31.
[28] Gross NJ, Nelson HS, Lapidus RJ, Dunn L, Lynn L, Rinehart M,Denis-Mize K., Formoterol Study Group. Efficacy and safetyof formoterol fumarate delivered by nebulization to COPDpatients. Respir Med 2008;102:189e97.
[29] Welte T, Metzenauer P, Hartmann U. Once versus twice dailyformoterol via novolizer for patients with moderate to se-vere COPDea double-blind, randomised, controlled trial.Pulm Pharmacol Ther 2008;21:4e13.
[30] Schunemann HJ, PuhanM, Goldstein R, Jaeschke R, Guyatt GH.Measurement properties and interpretability of the chronicrespiratory disease questionnaire (CRQ). COPD 2005;2:81e9.
[31] Rennard SI, Anderson W, ZuWallack R, Broughton J, Bailey W,Friedman M, Wisniewski M, Rickard K. Use of a long-actinginhaled beta2-adrenergic agonist, salmeterol xinafoate, inpatients with chronic obstructive pulmonary disease. Am JRespir Crit Care Med 2001;163:1087e92.
[32] Di Lorenzo G, Morici G, Drago A, Pellitteri ME, Mansueto P,Melluso M, Norrito F, Squassante L, Fasolo A., SLMT02 ItalianStudy Group. Efficacy, tolerability, and effects on quality oflife of inhaled salmeterol and oral theophylline in patientswith mild-to-moderate chronic obstructive pulmonary dis-ease. Clin Ther 1998;20:1130e48.
[33] Taccola M, Bancalari L, Ghignoni G, Paggiaro PL. Salmeterolversus slow-release theophylline in patients with reversibleobstructive pulmonary disease. Monaldi Arch Chest Dis 1999;54:302e6.
[34] Jones PW, Bosh TK. Quality of life changes in COPD patientstreated with salmeterol. Am J Respir Crit Care Med 1997;155:1283e9.
[35] Gupta RK, Chhabra SK. An evaluation of salmeterol in thetreatment of chronic obstructive pulmonary diseases. IndianJ Chest Dis Allied Sci 2002;44:165e72.
[36] Chapman KR, Arvidsson P, Chuchalin AG, Dhillon DP,Faurschou P, Goldstein RS, Kuipers AF., International studygroup. The addition of salmeterol 50 microg bid to anticho-linergic treatment in patients with COPD: a randomized,placebo controlled trial. Chronic obstructive pulmonary dis-ease. Can Respir J 2002;9:178e85.
[37] Stockley RA, Chopra N, Rice L. Addition of salmeterol toexisting treatment in patients with COPD: a 12 month study.Thorax 2006;61:122e8.
[38] Boyd G, Morice AH, Pounsford JC, Siebert M, Peslis N,Crawford C. An evaluation of salmeterol in the treatment ofchronic obstructive pulmonary disease (COPD). Eur Respir J1997;10:815e21.
[39] Jones PW, Wilson K, Sondhi S. Cost-effectiveness of salme-terol in patients with chronic obstructive pulmonary disease:an economic evaluation. Respir Med 2003;97:20e6.
[40] Donohue JF, Fogarty C, Lotvall J, Mahler DA, Worth H,YorganciogluA, Iqbal A, Swales J,OwenR,HigginsM,KramerB.,INHANCE Study Investigators. Once-daily bronchodilators forchronic obstructive pulmonary disease: indacaterol versus tio-tropium. Am J Respir Crit Care Med 2010;182:155e62.
[41] Dahl R, Chung KF, Buhl R, Magnussen H, Nonikov V, Jack D,Bleasdale P, Owen R, Higgins M, Kramer B., INVOLVE (Inda-caterol: Value in COPD: Longer Term Validation of Efficacy andSafety) Study Investigators. Efficacy of a new once-daily long-acting inhaled beta2-agonist indacaterol versus twice-dailyformoterol in COPD. Thorax 2010;65:473e9.
[42] Chapman KR, Rennard SI, Dogra A, Owen R, Lassen C,Kramer B., INDORSE Study Investigators. Long-term safetyand efficacy of indacaterol, a long-acting b2-agonist, insubjects with COPD: a randomized, placebo-controlledstudy. Chest 2011;140:68e75.
[43] Kornmann O, Dahl R, Centanni S, Dogra A, Owen R, Lassen C,Kramer B., INLIGHT-2 (Indacaterol Efficacy Evaluation Using150-mg Doses with COPD Patients) study investigators. Once-daily indacaterol versus twice-daily salmeterol for COPD: aplacebo-controlled comparison. Eur Respir J 2011;37:273e9.
[44] Kerwin EM, Gotfried MH, Lawrence D, Lassen C, Kramer B.Efficacy and tolerability of indacaterol 75 mg once daily inpatients aged �40 years with chronic obstructive pulmonarydisease: results from 2 double-blind, placebo-controlled 12-week studies. Clin Ther 2011;33:1974e84.
[45] Kinoshita M, Lee SH, Hang LW, Ichinose M, Hosoe M, Okino N,Prasad N, Kramer B, Fukuchi Y., Indacaterol Asian COPDStudy Investigators. Efficacy and safety of indacaterol 150and 300 mg in chronic obstructive pulmonary disease patientsfrom six Asian areas including Japan: a 12-week, placebo-controlled study. Respirology 2012;17:379e89.
[46] D’Urzo A, Ferguson GT, van Noord JA, Hirata K, Martin C,Horton R, Lu Y, Banerji D, Overend T. Efficacy and safety ofonce-daily NVA237 in patients with moderate-to-severeCOPD: the GLOW1 trial. Respir Res 2011;12:156.
[47] Kerwin E, Hebert J, Gallagher N, Martin C, Overend T,Alagappan VK, Lu Y, Banerji D. Efficacy and safety of NVA237versus placebo and tiotropium in patients with COPD: theGLOW2 study. Eur Respir J 2012;40:1106e14.
[48] Chanez P, Burge PS, Dahl R, Creemers J, Chuchalin A,Lamarca R, Garcia Gil E. Aclidinium bromide provides long-acting bronchodilation in patients with COPD. Pulm Phar-macol Ther 2010;23:15e21.
[49] Jones PW, Rennard SI, Agusti A, Chanez P, Magnussen H,Fabbri L, Donohue JF, Bateman ED, Gross NJ, Lamarca R,CaractaC,Gil EG.Efficacyand safetyofonce-dailyaclidiniuminchronic obstructive pulmonary disease. Respir Res 2011;12:55.
[50] Jones PW, Singh D, Bateman ED, Agusti A, Lamarca R, deMiquel G, Segarra R, Caracta C, Garcia Gil E. Efficacy andsafety of twice-daily aclidinium bromide in COPD patients:the ATTAIN study. Eur Respir J 2012;40:830e6.
[51] Vincken W, van Noord JA, Greefhorst AP, Bantje TA,Kesten S, Korducki L, Cornelissen PJ., Dutch/Belgian Tio-tropium Study Group. Improved health outcomes in patientswith COPD during 1 yr’s treatment with tiotropium. EurRespir J 2002;19:209e16.
[52] Donohue JF, van Noord JA, Bateman ED, Langley SJ, Lee A,Witek Jr TJ, Kesten S, Towse LA. 6-month, placebo-controlled study comparing lung function and health statuschanges in COPD patients treated with tiotropium or salme-terol. Chest 2002;122:47e55.
[53] Brusasco V, Hodder R, Miravitlles M, Korducki L, Towse L,Kesten S. Health outcomes following treatment for sixmonths with once daily tiotropium compared with twice dailysalmeterol in patients with COPD. Thorax 2003;58:399e404.
[54] Casaburi R, Mahler DA, Jones PW, Wanner A, San PG,ZuWallack RL, Menjoge SS, Serby CW, Witek Jr T. A long-term

LABA/LAMA effects on COPD health status 1479
evaluation of once-daily inhaled tiotropium in chronicobstructive pulmonary disease. Eur Respir J 2002;19:217e24.
[55] Casaburi R, Kukafka D, Cooper CB, Witek Jr TJ, Kesten S.Improvement in exercise tolerance with the combination oftiotropium and pulmonary rehabilitation in patients withCOPD. Chest 2005;127:809e17.
[56] Covelli H, Bhattacharya S, Cassino C, Conoscenti C, Kesten S.Absenceofelectrocardiographicfindingsand improved functionwith once-daily tiotropium in patients with chronic obstructivepulmonary disease. Pharmacotherapy 2005;25:1708e18.
[57] Verkindre C, Bart F, Aguilaniu B, Fortin F, Guerin JC, LeMerre C, Iacono P, Huchon G. The effect of tiotropium onhyperinflation and exercise capacity in chronic obstructivepulmonary disease. Respiration 2006;73:420e7.
[58] Um SW, Yoo CG, Kim YW, Han SK, Shim YS. The combinationof tiotropium and budesonide in the treatment of chronicobstructive pulmonary disease. J Korean Med Sci 2007;22:839e45.
[59] Chan CK, Maltais F, Sigouin C, Haddon JM, Ford GT., SAFEStudy Group. A randomized controlled trial to assess the ef-ficacy of tiotropium in Canadian patients with chronicobstructive pulmonary disease. Can Respir J 2007;14:465e72.
[60] Johansson G, Lindberg A, Romberg K, Nordstrom L, Gerken F,Roquet A. Bronchodilator efficacy of tiotropium inpatientswithmild to moderate COPD. Prim Care Respir J 2008;17:169e75.
[61] Ambrosino N, Foglio K, Balzano G, Paggiaro PL, Lessi P,Kesten S., Tiotropium Multicentric Italian Study Group. Tio-tropium and exercise training in COPD patients: effects ondyspnea and exercise tolerance. Int J Chron Obstruct PulmonDis 2008;3:771e80.
[62] Tonnel AB, Perez T, Grosbois JM, Verkindre C, Bravo ML,Brun M., TIPHON study group. Effect of tiotropium on health-related quality of life as a primary efficacy endpoint in COPD.Int J Chron Obstruct Pulmon Dis 2008;3:301e10.
[63] Tashkin DP, Celli B, Senn S, Burkhart D, Kesten S, Menjoge S,Decramer M., UPLIFT Study Investigators. A 4-year trial oftiotropium in chronic obstructive pulmonary disease. N Engl JMed 2008;359:1543e54.
[64] Kurashima K, Hara K, Yoneda K, Kanauchi T, Kagiyama N,Tokunaga D, Takayanagi N, Ubukata M, Sugita Y. Changes inlung function and health status in patients with COPD treatedwith tiotropium or salmeterol plus fluticasone. Respirology2009;14:239e44.
[65] Bateman E, Singh D, Smith D, Disse B, Towse L, Massey D,Blatchford J, Pavia D, Hodder R. Efficacy and safety of tio-tropium Respimat SMI in COPD in two 1-year randomizedstudies. Int J Chron Obstruct Pulmon Dis 2010;5:197e208.
[66] Bateman ED, Tashkin D, Siafakas N, Dahl R, Towse L,Massey D, Pavia D, Zhong NS. A one-year trial of tiotropiumRespimat plus usual therapy in COPD patients. Respir Med2010;104:1460e72.
[67] Hoshino M, Ohtawa J. Effects of adding salmeterol/-fluticasone propionate to tiotropium on airway dimensions inpatients with chronic obstructive pulmonary disease.Respirology 2011;16:95e101.
[68] Abe T, Setoguchi Y, Kono Y, Togashi Y, Sugiyama S,Tanakadate M, Soeda S, Nakai M, Sugiyama N, Fujiwara A,Yamaguchi K, Yamaguchi A, Kurita N. Effects of inhaled tio-tropium plus transdermal tulobuterol versus tiotropium aloneon impulse oscillation system (IOS)-assessed measures ofperipheral airway resistance and reactance, lung functionand quality of life in patients with COPD: a randomizedcrossover study. Pulm Pharmacol Ther 2011;24:617e24.
[69] Adams SG, Anzueto A, Briggs Jr DD, Leimer I, Kesten S.Evaluation of withdrawal of maintenance tiotropium inCOPD. Respir Med 2009;103:1415e20.
[70] Adams SG, Anzueto A, Briggs Jr DD, Menjoge SS, Kesten S.Tiotropium in COPD patients not previously receiving
maintenance respiratory medications. Respir Med 2006:1001495e503.
[71] Celli B, Decramer M, Kesten S, Liu D, Mehra S, Tashkin DP.,UPLIFT Study Investigators. Mortality in the 4-year trial oftiotropium (UPLIFT) in patients with chronic obstructive pul-monary disease. Am J Respir Crit Care Med 2009;180:948e55.
[72] Decramer M, Celli B, Kesten S, Lystig T, Mehra S, Tashkin DP.,UPLIFT investigators. Effect of tiotropium on outcomes inpatients with moderate chronic obstructive pulmonary dis-ease (UPLIFT): a prespecified subgroup analysis of a rando-mised controlled trial. Lancet 2009;374:1171e8.
[73] Tashkin DP, Celli B, Kesten S, Lystig T, Mehra S, Decramer M.Long-term efficacy of tiotropium in relation to smoking sta-tus in the UPLIFT trial. Eur Respir J 2010;35:287e94.
[74] Troosters T, Celli B, Lystig T, Kesten S, Mehra S, Tashkin DP,Decramer M. Uplift investigato tiotropium as a first mainte-nance drug in COPD: secondary analysis of the UPLIFT trial.Eur Respir J 2010;36:65e73.
[75] Tashkin D, Celli B, Kesten S, Lystig T, Decramer M. Effect oftiotropium in men and women with COPD: results of the 4-year UPLIFT trial. Respir Med 2010;104:1495e504.
[76] Aaron SD, Vandemheen KL, Fergusson D, Maltais F,Bourbeau J, Goldstein R, Balter M, O’Donnell D, McIvor A,Sharma S, Bishop G, Anthony J, Cowie R, Field S, Hirsch A,Hernandez P, Rivington R, Road J, Hoffstein V, Hodder R,Marciniuk D, McCormack D, Fox G, Cox G, Prins HB, Ford G,Bleskie D, Doucette S, Mayers I, Chapman K, Zamel N,FitzGerald M, Canadian Thoracic Society/Canadian Respira-tory Clinical Research Consortium. Tiotropium in combina-tion with placebo, salmeterol, or fluticasone-salmeterol fortreatment of chronic obstructive pulmonary disease: a ran-domized trial. Ann Intern Med 2007;146:545e55.
[77] Tashkin DP, Littner M, Andrews CP, Tomlinson L, Rinehart M,Denis-Mize K. Concomitant treatment with nebulized for-moterol and tiotropium in subjects with COPD: a placebo-controlled trial. Respir Med 2008;102:479e87.
[78] Vogelmeier C, Kardos P, Harari S, Gans SJ, Stenglein S,Thirlwell J. Formoterol mono- and combination therapy withtiotropium in patients with COPD: a 6-month study. RespirMed 2008;102:1511e20.
[79] Hanania NA, Boota A, Kerwin E, Tomlinson L, Denis-Mize K.Efficacy and safety of nebulized formoterol as add-on ther-apy in COPD patients receiving maintenance tiotropiumbromide. Drugs 2009;69:1205e16.
[80] Tashkin DP, Pearle J, Iezzoni D, Varghese ST. Formoterol andtiotropium compared with tiotropium alone for treatment ofCOPD. COPD 2009;6:17e25.
[81] Vogelmeier CF, Bateman ED, Pallante J, Alagappan VKT,D’Andrea P, Chen H, Banerji DF. Efficacy and safety of once-daily QVA149 compared with twice-daily salmeterolefluticasone in patients with chronic obstructive pulmonarydisease (ILLUMINATE): a randomised, double-blind, parallelgroup study. Lancet Resp Med 2013;1:51e60.
[82] Karner C, Chong J, Poole P. Tiotropium versus placebo forchronic obstructive pulmonary disease. Cochrane DatabaseSyst Rev 2012 Jul 11;7:CD009285.
[83] Jones PW, Barnes N, Vogelmeier C, Lawrence D, Kramer B.Efficacy of indacaterol in the treatment of patients withCOPD. Prim Care Respir J 2011;20:380e8.
[84] Chong J, Karner C, Poole P. Tiotropium versus long-actingbeta-agonists for stable chronic obstructive pulmonary dis-ease. Cochrane Database Syst Rev 2012 Sep 12;9:CD009157.
[85] WeldamSW, SchuurmansMJ, Liu R, Lammers JW. Evaluation ofquality of life instruments for use in COPD care and research: asystematic review. Int J Nurs Stud 2013 May;50:688e707.
[86] Yang IA, Clarke MS, Sim EH, Fong KM. Inhaled corticosteroidsfor stable chronic obstructive pulmonary disease. CochraneDatabase Syst Rev 2012 Jul;7. CD00299.

1480 F. Braido et al.
[87] van der Molen T, Cazzola M. Beyond lung function in COPDmanagement: effectiveness of LABA/LAMA combinationtherapy on patient-centred outcomes. Prim Care Respir J2012 Mar;21:101e8.
[88] Karner C, Cates CJ. Long-acting beta(2)-agonist in additionto tiotropium versus either tiotropium or long-acting beta(2)-agonist alone for chronic obstructive pulmonary disease.Cochrane Database Syst Rev 2012;4:CD008989.