-
8/2/2019 Mass HCR Plan 2004
1/29
Health Care Reform:Covering the Commonwealths
Uninsured Residents
A Model for the Purpose of Discussion
Executive Ofce of Health and Human Services
Ronald Preston, Secretary
May 3, 2004
-
8/2/2019 Mass HCR Plan 2004
2/29
i
The numbers herein are necessarily estimates. Real numbers can
come only once were closer to
setting up the program. However, in developing these estimates,
we were conservative. Both the
money the initiative will take and the fees needed to generate
this money are deliberately high.
Timing: If we can work with interested parties over the summer,
and the General Court starts its
deliberations in the fall and legislates a program in the
spring, we can have the program up by
the summer of 2006.
-
8/2/2019 Mass HCR Plan 2004
3/29
Introduction 1
INTRODUCTION
Everyone Should Have Health Insurance
Providing access to health insurance for everyone is an
important goal. It is important for
the well being of persons who do not now have health insurance.
It is important to the
competitiveness of our businesses, to health care cost
containment, and to the efciency and
effectiveness of our health care system. It is important to the
comity of the Commonwealth.
Being without health insurance is a hardship for all but the
very wealthy. For any complex need,
health care is expensive. If one cannot pay out of pocket, many
health providers and services are
beyond reach. One is mostly limited to hospitals, which are
often inconvenient and not the bestplace for primary care or even
some specialty care. If one is lucky, a community health center
is nearby. But these are often very busy places. Studies show
that uninsured people use fewer
health services, and more often wait to seek care until small,
less expensive ailments become
life-threatening, more expensive ones. For most people, when
calamity comes, being without
health insurance raises the specter of nancial ruin and endless
problems getting the right care.
Being without health insurance causes great anxiety.
The problems of the uninsured do not belong just to them.
Everyone else is also impacted. First,
there are health concerns. If ones tuberculosis goes untreated,
that endangers everyone. If one
becomes disabled through want of care, one needs the help of
others. Then, there are moneyconcerns. Everyone else pays for the
care the uninsured do receive. These costs are shifted onto
providers and ultimately onto payers. Employers pay more to
cover their employees. Insured
individuals pay more for their coverage. In the Commonwealth,
insurers, hospitals and the state
pay more for the Uncompensated Care Pool.
This cost shifting is fundamentally unfair. Employers who cover
their workers must also cover
the free care provided to the workers of employers who do not
offer coverage. Individuals
must not only pay for their own coverage, they must also pay
higher premiums to subsidize the
care of the uninsured.
Cost shifting obscures the true costs of care. This matters
because clarity is essential to
rationalizing the market for health care. Health care is
stupendously expensive, and relentlessly
becoming more so. Medical advances that everyone wants drive
most of the increase in costs.
But much of it is also driven by medical errors, redundant or
unnecessary tests and treatments,
and administrative disarray. More efciency is needed. A central
means to this efciency is
effective bargaining between the buyers and the providers of
care. Payers cannot negotiate
transparently with providers when costs for the uninsured are
buried in the numbers. Getting
-
8/2/2019 Mass HCR Plan 2004
4/29
Introduction 2
1 Much of this work was supported by a federal state-planning
grant from the Health Resources and Services Administration (HRSA).
Massachusetts was one of the rst elevenstates to receive federal
funding to research and propose models for increasing access to
health insurance. We are one of several states this year that
received a follow-upgrant to continue this effort.
2 The Division of Health Finance and Policy is currently
completing a household survey to determine the current rate of
uninsurance in the Commonwealth. We should havepreliminary gures by
June and complete ndings by fall.
the uninsured insured is necessary for getting everyone at the
table and all the facts on the table.
Thus, a rst step in addressing health costs is to have everyone
insured.
Covering Everyone Is Feasible
The Executive Ofce of Health and Human Services has considered
the feasibility of providing
access to basic, affordable health insurance to all
Massachusetts residents. Our investigation
included literature reviews, discussions with other states,
survey research, and economic
analysis. We reviewed state and federal expansions that have
been proposed over the years. We
looked at the Commonwealth s current health insurance market. We
proled Massachusetts
uninsured population and the states employer market, using
household surveys conducted in
1998, 2000 and 2002, and employer surveys conducted in 2001 and
2003. 1
We have concluded that getting our uninsured covered is a doable
task. Through MassHealth
expansions, reforms to the small-group and non-group markets,
and a strong employer base,
Massachusetts has one of the lowest rates of uninsurance in the
country. In 2002, approximately
418,000 people in Massachusetts were without health insurance.2
This is less than half the size of
our Medicaid enrollment and only 6.7% of the Commonwealths
residents.
These particular 418,000 residents are also less expensive to
insure than other groups. The
uninsured tend to be mostly single, working young adults who
usually need less intensive
services. Uninsured families tend to be small, and small
families cost less to insure than large
families.
Still, insuring everyone will be hard. The federal government
has never managed it. Neither has
any state. A state must contend with federal tax and labor laws,
commerce regulation, Medicare
and Medicaid. Each of these restricts what a state can do. A
state must also be concerned with
other states, and be careful not to competitively disadvantage
its businesses and their employees.
Getting everyone covered is more daunting than complex. What
must be done is straightforward,
but it challenges all parties. For everyone to benet, everyone
must contribute and compromise.
Providers, employers and individuals have their parts. Both
liberals and conservatives must bend.
-
8/2/2019 Mass HCR Plan 2004
5/29
Introduction 3
Guiding Principles
We spoke to health policy experts. They agreed that federal law
and competition from other
states make it hard for any one state to pursue coverage for all
its residents. But they all had
ideas, and from these we drew some basic principles that we
built into our proposal.
The proposal must be simple and clear (1) so that it can be
readily described and (2)
so that the legislative process can esh it out. In part, earlier
efforts to insure everyone
failed because they were too confusing. We should lay out the
basic idea, but then seek
broad participation in the ultimate design both to ensure that
it is thought through and to
engender the buy-in needed for passage.
The coverage offered must be much less expensive than that which
is now available in
the small-group and non-group markets. For this coverage to be
less expensive:
1. Benets must be less broad than state insurance law
requires;
2. All the uninsured must be in the risk pool;
3. The care must be managed;
4. Growth in provider rates must be contained; and
5. Enrollee cost sharing must be signicant.
The program must build on employer-sponsored insurance by
providing coverage
mostly to employees who do not have access to this insurance.
The program must not
substantially damage the market for more comprehensive coverage.
No state has the
means to replace the widespread availability of broad coverage
that employer-sponsoredinsurance has traditionally provided.
Therefore:
1. Benets must be good enough to be worth the money, but not so
good as to induce
employers or employees to drop commercial insurance coverage;
and
2. To discourage employers from dropping coverage, they must pay
a fee for
employees they do not cover.
Provider rates must be adequate.
The program must strive to improve employers competitive
position vis--vis employersin other states. At a minimum, the
program must not disadvantage our business
community.
The program must be fair. Everyone must share in its benets and
burdens.
1. Employers who currently pay nothing toward their employees
insurance must
contribute something.
-
8/2/2019 Mass HCR Plan 2004
6/29
Introduction 4
3 Dr. Gruber is an economist from MIT whose expertise is in
developing models to assess the impact of various approaches to
increasing access to health insurance (such aschanges in the
private insurance market, tax credits and Medicaid expansions).
2. Both employers who now sponsor insurance and all people who
carry insurance
must be freed of cost shifting for the uninsured.
3. Providers have their services covered for more patients, but
providers rate
increases must be limited.
4. The uninsured get insurance for the services most are likely
to need, and that also
provides protection against catastrophic health costs, but in
that they are able,
these people must share in the costs and accept management of
their care.
We incorporated these principles into various permutations.
Mercer and Lewin provided actuarial
support, and Dr. Jonathan Gruber did the econometric modeling.3
Dr. Gruber was involved early
on in this process and assisted our workgroup in designing the
insurance package. We asked
him to determine cost-effective methods of increasing access to
affordable health insurance in
Massachusetts. Many models were run varying cost sharing,
MassHealth coverage, subsidies,
and benet package components, including the cost effectiveness
of expanding programs such as
the Insurance Partnership (IP) and the State Children s Health
Insurance Program (SCHIP).
-
8/2/2019 Mass HCR Plan 2004
7/29
The Proposal at a Glance 5
THE PROPOSALATA GLANCE
1. BasicHealth: The state establishes a new health plan that is
offered by commercial health
maintenance organizations (HMOs). It is available to all
Massachusetts residents.
Benets: The benets are slimmer than our current health insurance
law requires. They
include hospital inpatient care, limited physician/therapist
visits, and limited pharmacy
benets.
Cost Sharing/Catastrophic Coverage: There is signicant cost
sharing (coinsurance and
deductibles) until these payments reach 4% of household income
for individuals and 8%
for families, after which there is no cost sharing for the rest
of the year.
Premiums: Average $230 per month for an individual, $500 for a
family.
Premium Subsidies: Premiums for BasicHealth are fully paid for
individuals and families
between 100% and 150% of the Federal Poverty Level (FPL).
(People below 100% of
poverty are eligible for MassHealth.) There are sliding-scale
subsidies for individuals
and families with household incomes between 150% and 400% FPL.
No one eligible for
Medicaid is eligible for BasicHealth subsidies.
Availability: Individuals and families must purchase BasicHealth
on their own.Employers cannot offer it.
Rates: The premiums the state pays HMOs for BasicHealth are
based on Medicare
pricing, and increase as Medicare rates do. Plans are
responsible for negotiating provider
rates.
Risk: The Commonwealth shares risk with the HMOs offering
BasicHealth.
Managed Care: Health plans use existing networks or establish
new ones for
BasicHealth.
Administration: The Ofce of Health Insurance (OHI) is
established within the Executive
Ofce of Health and Human Services (EOHHS) to administer the
program.
Demonstrations: The OHI has broad authority to pilot different
models of benets and
services with the HMOs.
-
8/2/2019 Mass HCR Plan 2004
8/29
The Proposal at a Glance 6
2. Individual Participation: All Massachusetts residents must
have health insurance either
through current options or through BasicHealth.
3. Employer Participation: Every employer in Massachusetts pays
a fee of $150 per month for
every full-time employee who does not have coverage through
their employer. This fee is pro-
rated for part-time employees working more than 10 hours but
fewer than 30 hours per week.
4. Medicaid: MassHealth expands to cover all Massachusetts
residents with household incomes
at or below 100% FPL.
5. Insurance Partnership: MassHealth increases current subsidies
for small employers to help
pay for commercial health insurance.
6. Essential Community Providers: A fund is created to support
the special work of forty-six
community health centers and half a dozen safety-net hospitals
that tailor their services to low-
income and other hard to serve populations.
7. Cost: $2.1B
Expanding the MassHealth program to Massachusetts residents with
incomes at or below
100% FPL ($489M);
Providing full premium subsidies to individuals and families
between 100% and 150%
FPL and sliding-scale premium subsidies to individuals and
families between 150% and
400% FPL towards purchase of BasicHealth ($1,035M), of which
some $510M is theinsureds obligation towards their premiums;
Increased participation and support for employer-sponsored
premium assistance programs
including the Insurance Partnership ($337M);
Essential Community Provider Fund ($101M);
Administering BasicHealth ($50M);
Creation of a risk reserve to support risk sharing or premium
collection shortfalls ($70M);and
Participation fee from the State in its role as an employer
($18M).
-
8/2/2019 Mass HCR Plan 2004
9/29
The Proposal at a Glance 7
8. Financing: $2.2B
Using the current funding for the Uncompensated Care Pool
($330M). Hospital
Assessment and the Surcharge Payers Amount are indexed to ensure
that the rate of
industry contribution keeps pace with the rate of overall
revenue growth.
Optimizing all opportunities through federal waivers to obtain
federal matching funds for
expenditures for providing health care coverage and subsidies
($399M).
Premiums paid by residents for BasicHealth coverage ($510M).
Assessing a fee on employers of $150 per month for every
employee they do not cover.
This fee is indexed to account for future growth in health care
costs and is pro-rated for
part-time workers ($951M).
-
8/2/2019 Mass HCR Plan 2004
10/29
The Proposal Discussed 8
THE PROPOSAL DISCUSSED
1. BasicHealth
For all residents to have insurance, people of modest means must
be able to afford it.
BasicHealth is meant to be an affordable last resort. Low-cost,
basic insurance risks inducing
crowd-out4 and adverse selection,5 which are both detrimental to
the viability of broader
insurance coverage. Thus, careful balances must be struck in
every aspect of BasicHealths
design. Still, we must expect some crowd-out and some adverse
selection. Economists tell us
that, even without BasicHealth, more employers will be dropping
comprehensive coverage and
more employees will be opting out of it. The cost of commercial
coverage is becoming too great.
BasicHealth may not even be to blame, they say, but it will be
blamed anyhow. So, we must
steel ourselves to this fact, and accept some run to
BasicHealth. The uninsured number 400,000plus; our models predict a
total enrollment of 500,000 plus in BasicHealth.
Benets
This product has a slimmer benet package than those currently
offered in the small-group and
non-group health insurance markets. For each family member
covered, BasicHealth includes
hospital inpatient care, 3 prescriptions a month, and 15
doctor/therapist visits a year for physical
health and another 15 for mental health. Other mandated services
are not covered, such as
substance abuse services, durable medical equipment (DME),
chiropractic, fertility treatments or
early intervention (see Table 1).
A primary goal was to develop a product that is good coverage
for most people, but not so
attractive that large numbers of people prefer it to commercial
plans. BasicHealth must be
thought valuable enough to be worth the effort. On the other
hand, we do not want to undermine
employer-based insurance (crowd-out). We also do not want to
undermine commercial coverage
by having large numbers of healthy people opting out of this
coverage. That would make the
standard plans more expensive for the people who remain in them,
and whose conditions require
broader coverage (adverse selection).
Another primary goal was to develop a product that costs
approximately $200 per member per
monthalmost half the cost of a typical HMO product in the
non-group market. Therefore, itwas necessary to tailor the package
carefully. In designing the benet package we experienced
the predictable trade-offs between affordability and
coverage.
4 Crowd-out: when people drop commercial insurance in favor of
government sponsored insurance.
5 Adverse selection: when sicker individuals gravitate to more
comprehensive policies making them more expensive, or when
healthier individuals forgo more comprehensivepolicies making them
more expensive. In either case, the r isk is spread only among
people who need more services.
-
8/2/2019 Mass HCR Plan 2004
11/29
The Proposal Discussed 9
BasicHealth meets the basic needs of most people. However, it
does not fully meet the needs
of individuals with chronic maladies that require frequent
doctors visits, frequent therapy,
substantial equipment or regular support services. Covering
these would have made the product
too expensive. Low-income people are eligible for MassHealth,
which covers comprehensive
acute services, support services, and long-term care.
Premium Costs
-
8/2/2019 Mass HCR Plan 2004
12/29
The Proposal Discussed 10
Cost Sharing
Signicant coinsurance comes at point of service: 20% for
inpatient services, 40% for outpatientservices, and 50% for
prescription drugs. However, no individual or family has to
spend
more than 4% or 8% respectively of their household income a year
for services covered by
BasicHealth. Table 2 presents maximum out-of-pocket exposure for
individuals and families of
various income levels enrolled in BasicHealth.
Many economists hold that rst dollar coverage is a major driver
of health costs and therefore
health insurance costs. Substantial coinsurance gives people a
stake in what their health care
costs, thus discouraging their overuse of services and
encouraging cost effective care. On the
other hand, the fundamental idea of insurance is to protect
against crushing losses, and therefore,
capping cost sharing is also important.
Acupuncture
Chemical Dependency Services
Chiropractic Services
Dental Services (except emergency treatment)
Durable Medical Equipment
Early Intervention Services
Home Health
Hospice
Infertility ServicesOccupational, Physical and Speech
Therapy
Podiatry
Rehab/Nursing Facility
Vision Services
A Partial List of Services Not Covered
-
8/2/2019 Mass HCR Plan 2004
13/29
The Proposal Discussed 11
100% 150% 200% 250% 300% 350% 400%
Individuals
Annual Gross Income $9,310 $13,965 $18,620 $23,275 $27,930
$32,585 $37,240
Annual Premium $0 $0 $552 $1,104 $1,656 $2,208 $2,760
Out of Pocket Maximum
(4% Gross Income) $0 $559 $745 $931 $1,117 $1,303 $1,490
Total Spending $0 $559 $1,297 $2,035 $2,773 $3,512 $4,250
Total Spending
as a Percent of Gross Income 0% 4% 7% 9% 10% 11% 11%
Family of 4
Annual Gross Income $18,850 $28,275 $37,700 $47,125 $56,550
$65,975 $75,400
Annual Premium $0 $0 $1,202 $2,405 $3,607 $4,809 $6,011
Out-of-Pocket Maximum
(8% Gross Income) $0 $2,262 $3,016 $3,770 $4,524 $5,278
$6,032
Total Spending $0 $2,262 $4,218 $6,175 $8,131 $10,087
$12,043
Total Spending
as a Percent of Gross Income 0% 8% 11% 13% 14% 15% 16%
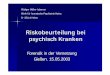
Table 2: Maximum Effect of Average Premiums and
Out-of-PocketContributions on Individuals and Families by Income
Level
Premiums
The state establishes and collects premiums for BasicHealth.
Premiums are community rated,
similar to the rating currently done in the non-group and
small-group markets. Premiums arerated by age, and average $2,700 a
year for individuals and $6,100 for families. The Department
of Revenue collects premiums through payroll deductions and
estimated taxes, and adjusts the
amount based on subsidy eligibility.
Premium Subsidies
All residents, regardless of immigrant status, and their
dependents whose incomes are at or below
150% FPL and who are not eligible for MassHealth do not have to
pay premiums. Sliding scale
subsidies for purchasing BasicHealth are provided for all
non-MassHealth-eligible residents with
incomes between 150% and 400% FPL (see Table 3 for current FPL
levels by family size).
These subsidies cover premiums only. All BasicHealth enrollees
are still required to pay
coinsurance and deductibles.
-
8/2/2019 Mass HCR Plan 2004
14/29
The Proposal Discussed 12
Family of 1 2 3 4
100% FPL $9,310 $12,490 $15,670 $18,850
150% FPL $13,965 $18,735 $23,505 $28,275
200% FPL $18,620 $24,980 $31,340 $37,700
400% FPL $37,240 $49,960 $62,680 $75,400
Table 3: Federal Poverty Level by Family Size
Availability
Any Massachusetts resident can purchase BasicHealth for herself
and her family. Immigrant
status does not matter for eligibility. Any resident can buy
BasicHealth from any of the several
insurers who offer the plan. However, to discourage adverse
selection in the employer-sponsoredmarket, one cannot buy
BasicHealth through an employer, and an employer cannot
directly
subsidize anyones premium. Economic modeling has shown that
allowing this product to be
sold in the small-group market would cause signicant crowd-out
and adverse selection.
To reduce crowd-out further, we thought of requiring employees
to take employer-sponsored
health insurance if it is offered, thus making them ineligible
for BasicHealth. We decided
against this course. Many couples are insured through one
partner. Straightening this out would
be a logistical asco. More importantly, health care reform
should not infringe on individual
discretion any more than is absolutely necessary to our purpose.
Most employers offer
comprehensive health plans and most employees sign up for them.
This includes employersoffering and employees subscribing to
self-funded health plans for which there are virtually
no coverage requirements. Since even self-funded plans tend to
be surprisingly broad, we
thought it best to rely on the desire of most employers to
provide and most employees to have
comprehensive coverage.
Another tactic to counter crowd-out would be to increase the
percentage of employees a small
employer must cover for that employer to offer small-group
health insurance plans. Under
current law insurers can require small businesses to cover 75
percent of their employees who
are eligible to purchase insurance. That percentage could be
raised. We decided not to do this as
it risks some employers giving up on the small-group market
altogether, relegating all of theiremployees to BasicHealth or
MassHealth.
Rates
Payments to health plans providing BasicHealth are pegged to
Medicare both in terms of
immediate payment rates and annual growth in rates. The health
plans, in turn, negotiate service
rates with their network of providers. Since providers know what
the health plans are being paid,
they know what to demand and what to expect in their own
rates.
-
8/2/2019 Mass HCR Plan 2004
15/29
The Proposal Discussed 13
For providers to be willing to participate in BasicHealth, they
will want rates above Medicaids.
In all states, Medicaids charitable mission has meant bare-bones
payments for most services and
most providers. BasicHealth is not a poverty program, and
therefore, BasicHealth provider rates
should be higher.
On the other hand, since BasicHealth must also be affordable,
high-end commercial service rates
are beyond its reach. That leaves middle-range commercial rates,
which is about where Medicare
is. In our meeting with ve of the states commercial insurers,
they felt that Medicare rates would
be sufcient for enough providers to sustain a workable delivery
network.
The rate by which premium rates grow also matters. BasicHealth
cannot sustain the 13 percent
premium growth that has characterized the state s commercial
plans in recent years. Therefore,
pegging BasicHealths growth to the Medicare rate of growth also
makes sense. A composite
Medicare ination factor is used to adjust premiums annually.
This composite is developed using
a weighted average of the Medicare update factors for the
various sectors of covered services,
such as hospitals, physicians, community health centers,
etc.
Nearly everyone we consulted has said we must have restrictions
on premium rates and
their growth, or BasicHealth will become unaffordable. That
being the case, we settled on a
benchmark: Medicare. We wanted to avoid any return to wholesale
provider rate setting by the
state. The Commonwealth gave that up in the early 1990s, and no
reasonable person wants it
back. Comprehensive rate setting is too complicated to be
desirable and too subject to political
winds to be effective.
RiskThe state must share risk with the health plans offering
BasicHealth. Plans do not have
experience covering the uninsured, and therefore do not want to
accept the full risk of covering
them. On the other hand, the plans must have an incentive to
manage costs. To mitigate the
nancial risk associated with covering a new population, the
state provides individual and
aggregate stop-loss protection through a self-funded risk
reserve. Actuaries develop stop-loss
thresholds and reserve amounts. The reserve account is available
to all HMOs to help mitigate
risk associated with outlier cases (e.g., persons with annual
expenses above $50,000) and
aggregate losses in excess of a predetermined amount. Thus, HMOs
are partially protected from
adverse selection, but also partly at risk, and therefore
invested in the close management of
outliers.
Managed Care
BasicHealth covers care that is managed. Affordable health care
demands care coordination, as
does cost control. HMOs offer BasicHealth and use coordinated
networks to provide care. The
HMOs can either use their existing networks, or they can develop
networks just for BasicHealth.
-
8/2/2019 Mass HCR Plan 2004
16/29
The Proposal Discussed 14
Some insurers have expressed an interest in incentive payments
for meeting disease management
or quality goals in their administration of BasicHealth. We
should explore this possibility.
Administration
A new ofce is created within EOHHS to administer BasicHealth:
the Ofce of Health Insurance
(OHI). OHI is responsible for selecting and contracting with
HMOs to provide this new product.
Contract oversight includes review of marketing materials
produced by participating HMOs,
premium setting, reconciliation of stop-loss arrangements,
quality measurement, and ensuring
HMOs maintain provider networks that provide adequate
access.
OHI maintains a registry of insurance coverage for enforcing
individual participation. Members
choosing to meet the individual mandate by purchasing this new
product sign up directly with a
participating HMO and can apply for subsidy assistance through
the HMO.
Eligibility for premium subsidies is determined by the state by
OHI or by MassHealth. Having
subsidy applications go through MassHealth ensures that
applicants who are eligible for
MassHealth are offered MassHealth. MassHealth provides a more
generous benet package and
leverages federal money.
OHI is small and efcient. We do not need an independent or
separate agency with a governing
board. Grandeur is not our aim; neither is any set-up suggestive
of an expanding role. The
objective of OHI is not to dominate health policy, health care
or the health insurance industry. Its
objective is the competent administration of BasicHealth.
OHI competitively selects 4-5 commercial HMOs to offer this new
product. Initially, weconsidered hiring a single third party
administrator. But with potentially 500,000 or more
BasicHealth beneciaries we must consider our states health
insurers. Several of the highest
quality and most well regarded HMOs in the country are based in
Massachusetts, and we must
not disrupt the health insurance market. Spreading BasicHealth
enrollment is necessary to that
end. On the other hand, limiting the number of health plans
selected makes contract oversight
more reasonable. Having 4-5 health plans gives each a
substantial pool of subscribers. Using 4-5
competitively selected commercial HMOs for BasicHealth also
gives us the advantages of their
combined skills, and keeps BasicHealth rmly rooted in the
private sector.
DemonstrationsEvery health policy expert we consulted warned us
that we cannot afford to make comprehensive
insurance (what everyone wants) available to everyone. To do
that we would have to revamp
health care delivery to base it on evidenced-based best
practices, to rationalize its administration
and to reduce error and waste. Such cannot be done in a day or a
year. No mere benets package,
however clever, can drive this change. However, allowing HMOs to
pilot different packages and
networks can foster change.
-
8/2/2019 Mass HCR Plan 2004
17/29
The Proposal Discussed 15
The Ofce of Health Insurance is given broad exibility to pilot
ideas with the HMOs offering
BasicHealth. In that they are willing, these insurers may offer
a second or third BasicHealth plan
that manages given diseases, includes a special delivery
network, or adheres to specic clinical
guidelines or best practices. These other packages may offer
richer benets for the money, or be
available only in certain parts of the state.
2. Individual Participation
Every Massachusetts Resident Must Have Health Insurance
The requirement to carry insurance can be satised by any of the
following options:
Maintaining health insurance coverage available in the
commercial health insurance
market (e.g., through ones employer or through the non-group
market);
Purchasing a catastrophic health insurance plan and maintaining
a health savings account
(HSA);
Enrolling in a student health insurance plan though an institute
of higher education;
Enrolling in a public or private retiree health benet plan;
Purchasing BasicHealth; or
Enrolling in a public health insurance program (e.g.,
MassHealth, Medicare, the Medical
Security Plan).
Why Mandate Individual Participation?
Covering the uninsured requires the alternative of an insurance
plan that is more affordable
than what is now available. The size and makeup of the risk pool
is one of the factors thatdetermine the cost of this product.
Virtually all of the uninsured must be included to keep the
cost down. The uninsured include a large portion of healthy
young adults who cost less to cover,
and therefore, their inclusion is vital. However, our modeling
of voluntary programs based on
incentives did not bring in enough uninsured to be viable. Too
many healthy people do not see
the value of insurance. Therefore, requiring insurance coverage
is needed to make BasicHealth
viable.
Enforcement
Most residents le taxes, request state licenses or apply for
state services. Health insurance can
be veried through these dealings. Health providers can also
verify coverage.
Drivers License/State ID/Vehicle Registration
Require applicants to be covered by a health insurance policy as
a prerequisite for a
new or renewed driver s license, learners permit, state
identication card or vehicle
registration. The Registry of Motor Vehicles (RMV) can be
responsible for verifying the
health insurance status of residents. Ideally, the RMV check can
simply be an RMV query
to a separate database for yes/no response to state health
insurance.
-
8/2/2019 Mass HCR Plan 2004
18/29
The Proposal Discussed 16
Tax System
Require state income tax lers to report on their tax return
whether they and their
dependents maintained health insurance coverage during the tax
year for which they
are ling (i.e., retrospectively). The Department of Revenue
(DOR) can conrm health
insurance status. Alternatively, the state may be able to assess
a penalty for those unable
to demonstrate compliance with the mandated health insurance
coverage.
Point of Service
Require hospitals, community health centers and other providers
to conrm the health
insurance status of any individual seeking care. The patient, if
uninsured and eligible,
can be offered enrollment in MassHealth. Other uninsured
patients can be offered
BasicHealth.
Proof of Coverage
The most efcient, accurate and timely method of verifying health
insurance status is to establish
a Central Insurance Registry. The Registry can be accessed
through a computer network, which
is consistent with current efforts to streamline RMV or DOR
administration through computer-
based processes.
3. Employer Participation
All Employers Must Contribute to the Cost of Insuring their
Employees
For each employee, an employer can meet this obligation by
covering this employee with health
insurance that meets the requirements of the federal Employee
Retirement Income Security Act(ERISA). For every employee who is
not offered or does not accept this coverage, the employer
pays the state a fee of $150 a month. This fee is prorated for
part-time workers, working more
than 10 hours but fewer than 30 hours a week$150 is less than a
dollar an hour for a full-time
employee. The Department of Revenue collects the fee. This
ensures greater compliance and a
surer cash ow.
Why the Fee?
To cover the uninsured, there must be new money to subsidize
coverage for low-income people
and to administer the new health plan: BasicHealth. Obtaining
this money through a broad-
based tax would induce employers who are now sponsoring
insurance to drop it, placing an evengreater burden on taxpayers.
Though employer-based health insurance may be an accident of
World War II, it is what we have. No state has the means to
replace this system. No state can
underwrite the widespread availability of broad coverage that
employer-sponsored insurance
has traditionally provided. We want as many people as possible
to have broad coverage,
and therefore, as few as possible to need BasicHealth.
Therefore, our intent is to ll gaps in
employer-sponsored coverage.
-
8/2/2019 Mass HCR Plan 2004
19/29
The Proposal Discussed 17
Fairness is also an issue. Most Massachusetts employers offer
health insurance. In 2003, 98%
of employers with 50 or more employees offered health insurance
to their employees. Even
businesses with fewer than 50 employers are more likely than not
to sponsor coverage: sixty-
six percent do. It is unfair to these businesses that their
insurance costs are higher because
other businesses do not do their part. In 2003, there were
approximately 43,913 Massachusetts
employers who did not provide health insurance or contribute to
the health care costs of their
employees. Seventy-three percent of the uninsured in
Massachusetts are employed, and many
work for employers who do not offer health insurance coverage.
Levying a fee on employers
who do not contribute to the cost of covering an employee
discourages crowd-out, and injects a
measure of fairness into the nancing of health insurance.
ERISA
The biggest potential obstacle to state action is the Employee
Retirement Income Security Act
(ERISA). ERISA regulates employee welfare and benet plans
including those that provide,
medical, surgical, hospital care or benets for plan participants
or their beneciaries through
the purchase of insurance or otherwise.6 The ERISA statute
contains broad language preempting
any and all state laws insofar as they...relate to an employee
benet plan.7
ERISA allows businesses to self insure, which is to bear the
risk themselves for providing
health insurance to their employees. When a business self
insures, state insurance law cannot
specify the scope of this coverage. ERISA itself contains few
stipulations on what must be
included in a self insured benet package. Therefore, self
insured employers can pay very
little of the cost of their plans or offer plans that are far
less adequate than BasicHealth. But if
employers do either, their employees are likely to opt for
BasicHealth and the employers will be
paying a fee for each one who does.
The legality of such a fee has not been tested in federal court.
Nonetheless, theres a solid legal
argument for a states imposing this contribution, with some
approaches being more defensible
than others. The following makes the strongest case:
1. The legislation establishes a publicly nanced health coverage
program that is nanced
partially with employer contributions (taxes) required from all
types of employers.
2. The employer contribution of $150 per employee is imposed on
all employers and does
not make any reference to employer sponsored health plans (i.e.,
the contribution isrequired of all employers not just those who do
not provide health insurance). 8
6 Sec.3 (1) 29 USC Sec.1002 (1).
7 Sec. 514(a), 29 USC 1144
8 Note: the state Constitution may require uniform taxation of
all employers, not just those who do not provide health
insurance.
-
8/2/2019 Mass HCR Plan 2004
20/29
The Proposal Discussed 18
3. The state provides an immediate tax credit for the amount of
the contribution for each
employee the employer covers. The credit should not be
conditioned on the adequacy of
the packages (to avoid binding plan administrator choices).
4. The statute is neutral on whether the employer pays the tax
or provides insurance.9
4. Medicaid
We modify MassHealth to mesh with BasicHealth so that together
they can cover the uninsured
that cannot or will not subscribe to standard health insurance.
This tailoring simplies the
program and some eligibility expansions. These changes require
approvals by our federal
partners, the Centers for Medicare & Medicaid Services
(CMS).
The Childrens Medical Security Plan (CMSP) is eliminated because
CMSP enrollees, many of
whom are undocumented aliens, are eligible for either MassHealth
or BasicHealth. Also, both
programs provide more comprehensive coverage than CMSP.
We keep the Medical Security Plan (MSP). MSP provides health
insurance to certain
Massachusetts residents with incomes below 400% FPL who are
eligible to receive
unemployment benets. MSP enrollees can receive either partial
premium subsidies toward
COBRA premium payments to continue their previous employers
health coverage, or can
receive direct coverage through a Blue Cross Blue
Shield-contracted indemnity plan. The state
receives federal match for all state expenditures for health
insurance coverage for MSP enrollees.
It therefore makes sense to continue this alternative, rather
than have people who are brieyunemployed purchasing BasicHealth and
then dropping it.
MassHealth Simplication
The Executive Ofce of Health and Human Services consolidates
MassHealth plans. There are
now six benet packages. We want three:
1. MassHealth Standard
All Title XIX (Medicaid), Title XXI (State Childrens Health
Insurance Program or
SCHIP), and CommonHealth eligible (higher income disabled)
members are enrolled in
MassHealth Standard, the most comprehensive MassHealth coverage.
Standard membersreceive benets directly or through premium
assistance if they have cost-effective
9 Blue Cross and Blue Shield Plans v. Travelers Insurance
Company 115 S.Ct. 1671 (1995)
-
8/2/2019 Mass HCR Plan 2004
21/29
The Proposal Discussed 19
employer-sponsored insurance. If they do, Medicaid pays for
commercial insurance
coverage and then pays directly for Medicaid services that this
coverage does not include
(wrap around). Standard Medicaid covers a broader range of
services than are available
through any commercial insurance. Standard Medicaid covers
long-term care and an
array of social supports.
2. MassHealth Essential
All MassHealth beneciaries who are eligible only under the
MassHealth waiver
with income at or below 100% FPL are enrolled in MassHealth
Essential, a less
comprehensive coverage benet. MassHealth Essential does not
cover most long-term
care services and some acute services.10 Essential members
receive benets directly or
through premium assistance if they have cost-effective
employer-sponsored insurance.
3. MassHealth Premium Assistance
All residents with incomes between 100% and 200% FPL who receive
MassHealth
through the waiver and whose employer participates in the
Insurance Partnership are
enrolled in MassHealth Premium Assistance,11 which provides
nancial assistance for the
purchase of standard commercial health insurance.
Increasing MassHealth Eligibility Uniformly to 100% FPL
Every Massachusetts resident whose household income is at or
below 100% FPL is eligible for
MassHealth, regardless of U.S. citizenship status.
We estimate that 148,000 individuals will be enrolled in
MassHealth Essential. This gure
includes individuals already enrolled in MassHealth Essential,
those eligible for it but notenrolled, and the newly covered
populations: aliens and childless adults who are not long-term
unemployed. In addition, another 424,000 individuals may avail
themselves of existing premium
subsidy programs designed to maintain their participation in
their employers plans.
Those eligible under Title XIX and Title XXI are enrolled in the
most generous benet
packageMassHealth Standard, while the remaining residents, who
would otherwise be
uninsured, are enrolled in less-comprehensive MassHealth
Essential. We do not change
MassHealth eligibility rules for residents with incomes greater
than 100% FPL.
The individual participation requirement of health care reform
incents people who are eligible forMassHealth to enroll in
MassHealth. MassHealth-eligible residents do not receive a subsidy
for
the purchase of BasicHealth. This approach is warranted for the
following reasons:
10 NOT COVERED: adult day health, adult foster care, chronic
disease/rehab hospital, day habilitation, early intervention,
hearing aid, home health, hospice, nursing facility,personal care
services, private duty nursing and audiology/hearing aid,
chiropractic, Chapter 766, nurse midwife, orthotic, vision care,
transportation.
11 We preserve the Insurance Partnership, a program for small
employers (i.e. employers with up to 50 full-time employees) that
offer comprehensive health insurance and pay atleast 50% of the
cost for each employee at or below 200% of the FPL.)
-
8/2/2019 Mass HCR Plan 2004
22/29
The Proposal Discussed 20
It is cost effective for the state to encourage
MassHealth-eligible residents to enroll in
MassHealth because the state can get substantial federal
reimbursement for MassHealth,
but not for BasicHealth; and
The MassHealth provider rates are lower than the BasicHealth
provider rates since the
latter are based on Medicare rates.
To maintain equity between BasicHealth and MassHealth, we do not
charge premiums to anyone
in MassHealth or non-MassHealth-eligible residents with incomes
at or below 150% FPL, who
purchase BasicHealth. As noted above, all individuals in the
state with incomes below 100%
FPL are encouraged to enroll in MassHealth Essential (and are
not charged premiums), and
individuals in BasicHealth with incomes between 100% and 150%
FPL receive full premium
subsidies. The sliding scale premium amounts for MassHealth
members with incomes above
150% FPL remain as they are now.
Federal Approval and Budget Neutrality
To make the proposed changes to the MassHealth program and to
receive federal reimbursement
for these changes, the state must receive approval from the
Centers for Medicare & Medicaid
Services (CMS). The intent is to amend the current 1115 waiver
in a manner that maximizes
federal reimbursements.
CMS waiver approval hinges upon demonstrating to CMS that the
proposed MassHealth changes
are budget neutral to the federal government. In general, a
state may not spend more for a
program administered through an 1115 waiver than it would have
spent in the absence of the
waiver. The budget neutrality test caps the amount of waiver
expenditures that can qualify forfederal reimbursement. There
appears to be sufcient room in the budget neutrality cap to
cover
the individuals with incomes at or below 100% FPL and receive
federal reimbursement.
5. Insurance Partnership
The Insurance Partnership (IP) is an existing MassHealth waiver
program. IP helps both
small employers and their low-income employees buy commercial
health insurance. For
each low-income employee who enrolls,12 a subsidy is paid to a
small employer13 that offers
comprehensive health insurance to its employees and pays at
least 50% of the cost of that healthinsurance. Employees must take
up the health insurance offered by these employers, and be
determined eligible for MassHealth. The employee also receives a
subsidy for premiums.
12 For the IP, low-income employee is dened as an employee with
household income at or below 200% FPL
13 small = 50 or fewer full-time employees
-
8/2/2019 Mass HCR Plan 2004
23/29
The Proposal Discussed 21
For employers meeting the above requirements, the IP pays the
employer a monthly subsidy as
follows: $33.33 per individual, $66.66 per couple, $66.66 for
one adult and one child, and $83.33
per family.
MassHealth effectively subsidizes the employees premium costs up
to the following: $123.00
per individual, $246.00 per couple, $288.00 for one adult and
one child, and $438.00 for a family
of three (two adults and one child).
MassHealth only pays subsidies up to the cost of the employees
share of the premium.
To discourage crowd-out, we increase the IPs employer subsidy by
25%, since these subsidies
have not been increased since the program began the late
1990s.
6. Essential Community Providers
We establish an essential community provider fund (ECPF) to help
pay the warranted but
exceptional costs of essential community providers (ECPs). Seed
money for this fund comes
from the current funding sources of the Uncompensated Care Pool
and employer participation
fees. As much as possible, we augment this seed money with
federal matching funds by using it
to make enhanced Medicaid payments and Disproportionate Share
Hospital (DSH)14 payments,
both of which generate 50 cents on the dollar.
Although their backgrounds and circumstances vary widely, all
modest income residents have
difculty accessing and using health care. The Commonwealths
health centers and safety-
net hospitals15 specialize in meeting the variegated needs of
this population. This proposal forMassHealth and BasicHealth
provides signicant resources to these providers. Nonetheless,
these providers still incur signicant unreimbursed patient care
costs.
Not addressing these extra costs would endanger the missions and
even survival of these
institutions. We would face huge pressure to maintain the
Uncompensated Care Pool (the Pool).
The Pool is an unwieldy anachronism that is impossible to manage
effectively or fairly since it
reimburses hospitals and health centers for self-reported costs
that are impossible to verify or
justify by any uniform standard. Medicaid rates and DSH payments
are more straightforward
mechanisms. They allow us to provide more measured and
purposeful subsidies.
14 DSH payments are for uncompensated care in hospitals serving
a disproportionate share of Medicaid or non-paying patients. Within
certain limits, these DSH payments arefederally matched dollar for
dollar.
15 e.g., Boston Medical Center, Cambridge Health Alliance,
Brockton Hospital, and Lawrence General Hospital.
-
8/2/2019 Mass HCR Plan 2004
24/29
The Proposal Discussed 22
We must abolish the Pool. To do this, everyone must have health
insurance, and we must
establish this residual essential community provider fund to
address residual needs. Essential
Community Providers have extra needs that are both real and
legitimate.
First, for the patients that enroll in BasicHealth, providers
receive no payment for certain
medical services that fall outside the benet package: e.g.,
longer-term mental health needs, all
substance abuse treatments, some pharmacy costs for chronic
diseases; and all outpatient visits
for those with medical conditions requiring more than 15 medical
visits per year. Lower income
patients with complex needs are likely to continue to resort to
Essential Community Providers.
Second, out-of-pocket coinsurance liabilities for most
outpatient and other primary care services
are signicant (40%) and are not subsidized until individuals and
families reach their household
income cap. ECPs currently nd it difcult to collect copayments
from the lower-income patients
who are likely to continue to come to these providers.
Third, both hospitals and federally qualied health centers carry
legal obligations to serve
patients regardless of their ability to pay. Hospitals remain
obligated under the federal
Emergency Medical Treatment and Active Labor Act (EMTALA) to
provide emergency and
stabilization services to all. Community health centers carry
responsibility for primary care and
in some cases, pharmacy services to low-income patients under
Sections 330 and 340B of the
federal Public Health Service Act.
Finally, despite our individual participation requirement, some
residents will not comply; some
will be unaware, disorganized, or simply resistant. Some will
say that they cannot afford their
share of the premiums or copayments. Chances are, however, they
will still head to EssentialCommunity Providers for care.
For both hospital Medicaid rates and DSH payments, there are
limits to federal reimbursements.
We must take care to arrange the rates and payments to maximum
effect.
Caps on hospital Medicaid rates are called upper payment limits
(UPLs). MassHealth has
recently completed 2002, 2003 and 2004 UPL calculations. We
believe that the calculations
are methodologically conservative. The 2004 UPL calculations
revealed substantial room on
inpatient acute hospital spending and a moderate level of room
on outpatient spending, which
will allow the Commonwealth to pay hospitals more in Medicaid
rates.
Caps on uncompensated care costs are called disproportionate
share hospital (DSH) payment
limits. The Commonwealths statewide annual DSH cap for Federal
Financial Year (FFY)
04 through FFY13 is $574.5M. In FFY04, the Commonwealth is using
all but $63M of
this $574.5M. DSH payments must stay within these limits to
maximize the ratio of federal
reimbursement.
-
8/2/2019 Mass HCR Plan 2004
25/29
The Proposal Discussed 23
Costs ($M)Cost Insureds
to the State Obligation Total
MassHealth Expansion $489 $489
BasicHealth $525 $510 $1,035
Employer-sponsored Insurance/Premium Assistance $337 $337
Essential Community Provider Fund $101 $101
Administration and Enforcement $50 $50
Risk Reserve $70 $70
State Employer Participation Fee $18 $18
Total $1,590 $510 $2,100
Sources of Revenue ($M)Revenue Insureds Premium
to the State Contribution Total
Pool Assessment and Surcharge on Payers $330 $330
Federal Financial Participation $399 $399
BasicHealth Premiums $510
Employer Participation Fee $951 $951
Total $1,680 $510 $2,190
Margin $90 $90
Margin as a Percentage of Total Cost 6% 4%
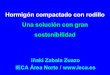
Table 4: Summary of Funding Sources and Spending
for Proposed Model ($M)
Assumptions
MassHealth Expansion: includes individuals new to MassHealth who
are eligible but unenrolled and MassHealth Essential.
BasicHealth: includes all insured who enroll in this new
product. Subsidies will be provided to those between 100% and 400%
FPL who are otherwise ineligible for MassHealth.All insureds with
incomes over 150% FPL contribute towards premium cost. Insureds
over 400% FPL pay full premium cost.
Essential Community Provider Fund:supports the technical and
network development for community health centers and hospitals.
Risk Reserve: allows for risk sharing for catastrophic claims
and nonpayment of premiums.
Administration and Enforcement: includes the Ofce of Health
Insurance; premium collection activities by DOR; contract
management andoversight; and Central Insurance Registry.
State Employer Participation Fee:reects the cost to the state of
the Employer Fee that will be levied for the state employees
who
do not take up GIC sponsored insurance.
Pool Assessment and Surcharge on Payers: Pool assessments and
surcharges will be maintained and increasein future years by a
percentage tied to hospital revenue growth generally.
Employer Participation Fee:at $150 per employee per month for
each employee that the employer does not cover.
Number of Uninsured: if the total number of uninsured
individuals is greater than 418,000, the additional cost to the
program would be approximately $1,300 per person per year,according
to the model.
MassHealth Members in MCOs: the estimates for MassHealth are
based on a fee-for-service environment, not a xed capitated program
with monthly premiums.
Estimates of Increased Take-up of Premium Assistance
Programs:e.g., IP are high. If this doesnt occur, signicantly less
revenue is required.
-
8/2/2019 Mass HCR Plan 2004
26/29
The Proposal Discussed 24
7. Cost: $2.1B
Our estimates are in FY05 dollars for a full year of operation,
and are based on actuarial
estimates of premium costs from Mercer Government Consulting,
modeling work by Dr.
Jonathan Gruber, and EOHHS estimates. Actual program costs need
signicant renement and
adjustment for actual program start dates, but at this point are
very conservative.
Our estimates are based on providing direct coverage to a number
of Massachusetts residents
(including the current MassHealth Essential population),
subsidies to many more, and the cost of
administering and operating the program.
MassHealth Covers Lowest Income Residents
The estimated cost of MassHealth for the 148,000 insureds with
incomes less than 100%
FPL is $489M. For the purposes of this discussion, this estimate
includes all newly
insured individuals and those currently enrolled in MassHealth
Essential who may
ultimately be counted as MassHealth Essential.
BasicHealth
The cost of BasicHealth for individuals and families up to 400%
of FPL is estimated
at $525M. Subsidies are provided on a sliding scale tied to
income and decrease in a
linear relationship to higher income levels. Insureds contribute
another $510M through
premium payments, for a total cost of $1.035B.
Increasing Support and Increased Demand for Premium Assistance
Programs
Supporting continued employer participation in premium
assistance programs includingthe Insurance Partnership through
subsidies is estimated at $337M, including an
additional $2M to increase the employer subsidy by 25%.
Essential Community Provider Fund
Additional funding is needed for essential community providers
(ESPs). Despite our best
efforts, some people will still not have insurance. Moreover,
some medical services will
fall outside the benet package, as described above. Hospitals
and health centers will
remain obligated under applicable federal laws to provide
certain services to all, regardless
of ability to pay. Therefore, the Proposal includes a funding
allowance in the amount of
$101M for the continuing uncompensated costs incurred by
hospitals and health centers.
Administration and Enforcement
Administrative costs are estimated at $50M, approximately 5% of
medical spending.
This supports the new Ofce of Health Insurance, additional
resources for DOR and
DET. Functions include administering the contracts with
participating HMOs, collecting
premiums and employer fees, enforcing the individual mandate,
actuarial services,
marketing, and outreach.
-
8/2/2019 Mass HCR Plan 2004
27/29
The Proposal Discussed 25
Risk Reserve
We have set aside $70M as a risk reserve against several
unknowns including, but
not limited to: failure to pay premiums, out-of-pocket costs in
excess of budgeted
amounts, and one-time rate adjustments to meet the needs of the
newly insured (pent up
demand).
State Employer Participation Fee
Like other employers, the state must pay a fee for every state
employee who does not opt
for state coverage. This obligation is estimated to be $18
million.
8. Financing: $2.2B
Consistent with our goal of sharing the burden of providing
health care for low-income
individuals, the revenue stream to support state costs comes
from existing assessments and
surcharges for uncompensated care, federal nancial participation
for qualifying expenditures,
employer participation fees, and premiums paid by people
enrolled in BasicHealth.
Uncompensated Care Pool Revenue
The Pool has been supported by relatively at assessments on
hospitals and surcharges on
payers (commercial health insurers in Massachusetts). In past
years, $270M to $315M in
annually revenues were raised; in FY05, House I seeks $330M.
Retention of this revenue
stream is a critical component of HCRI nancing. Beginning in
FY06, the assessments
and surcharges will be reformulated as a percentage of total
hospital or insurer revenue
based on the relationship of the FY05 payment to total revenue
for each group. Overtime this will enable this component to grow.
Each dollar of these state revenues, when
expended on Title XIX qualifying programs, will generate a
dollar of federal revenue.
Seek Greater Federal Financial Participation (Assumes Limited
Approval)
We estimate $399M in federal nancial participation. This is
based on allowable
expenditures for any newly covered persons meeting current
MassHealth eligibility
criteria, MassHealth Essential, administrative costs, and the
residual pool. The estimates
assume that some percentage of those who might be eligible for
MassHealth by virtue of
age or income may need to be state-only due to citizenship
issues. Note that this category
includes federal nancial participation previously claimed on the
Pool expenditures;under the Proposal, federal revenues would ow
from BasicHealth and Reserve Fund
expenditures. If we are successful in achieving additional
federal approval, the estimate
of federal nancial participation may increase.
BasicHealth Premiums
We estimate $510M in premium payments from BasicHealth members
with incomes at
150% FPL and above.
-
8/2/2019 Mass HCR Plan 2004
28/29
The Proposal Discussed 26
Employer Fees Encourage Continued Private Market
Participation
Revenue from employers that do not offer health insurance or
that have employees
declining the employers offered insurance form the cornerstone
of the revenue package.
At $150 per employee per month, we estimate that we could
achieve as much as $951M
in new revenue to directly support all aspects of
BasicHealth.
Margin: $90M
-
8/2/2019 Mass HCR Plan 2004
29/29
CONCLUSION
As there is nothing new under the sun, there are no new ideas in
this proposal. Rather, it is thecombination of these ideas that is
unusual, each keeping unlikely company with the others. The
left wing, the right wing and possibly everyone in between will
be affronted by one or another
feature. So will every interested party, be they administrators,
clinicians, insurers, providers,
suppliers, manufacturers, employers, employees, advocates or
academics. On the other hand, all
of these factions and parties will also nd something to
like.
Health reform fails when people differ on their rst choice, but
agree on their secondthat being
to do nothing. We pursue health insurance for everyone, a benet
to everyone. We presume that
to get there, everyone must pay some or give some, and most must
do both.
If our proposal goes anywhere, its elements will undoubtedly be
heated, cooled, split and
recombined. But our premise will stand. Everyone must pay some
or give some, and most must
do both. If we all do our parts, we can do this task. We will
see everyone insured, and we will
thereby lay a foundation for a better commonwealth and better
health care for all.