Embed Size (px)
Citation preview

1
Modul 5.3 eksamen 2014
Titel på kursus: Ernæring og fordøjelsessystemet II
Uddannelse: Bachelor i Medicin
Semester: 5. semester
Eksamensdato: 28-‐01-‐2015
Tid: kl. 09.00 -‐ 12.00
Bedømmelsesform 7-‐trin skala
Vigtige oplysninger
• Husk at opgive studienummer – ikke navn og cpr.nr. – på alle ark, der skal medtages i bedømmelsen
• Husk at aflevere besvarelsen, også hvis du forlader eksamen, før den er slut • Hele eller dele af opgaven kan være formuleret på engelsk (NB! der vil ikke blive
stillet ordbøger til rådighed) • Øvrige hjælpemidler er ikke tilladt • Det er tilladt at skrive besvarelsen på dansk eller engelsk • Ingen former for kommunikation er tilladt
• Besvarelserne indskrives på de angivne rammer. Rammernes størrelse angiver
samtidig de ønskede maksimale længde på besvarelserne af essay spørgsmål. Der må således ikke skrives mere til de enkelte spørgsmål, en det kan rummes inden for den relevante ramme. De dele af svar, der er uden for rammen, indgår ikke i bedømmelsen. Den enkelte opgaves vægt i point er angivet forneden. Rammen achieved point er kun til brug ved censurering.
• Total antal af spørgsmål er 30. Total antal af point = 76 point
NOTE: The most appropriate answers are written in red. For some of the short-‐assay questions, there are other options which are also correct but are not included here.

2
1) A 24-year old female patient has suffered with increased frequency of bowel opening, up to
five times a day, abdominal pain frequently localized to the right lower quadrant and feeling generally unwell for the last 6 months. The patient is clearly unwell – she is pale, underweight, passing loose and greasy stools, and with a painful mass in the right iliac fossa. Investigations: - Hemoglobin (Hb) 109 g/L (130–180) - White cell count 16.9 x 109 /L (4.0–11.0) - Serum C-reactive protein 30 mg/L (< 10) - Positive anti-Saccharomyces cerevisiae antibody
a) What is the most probable diagnosis? b) Provide a reasonable explanation for her weigh loss, low Hb and elevated levels of C-
reactive protein Max point: 4 Achieved point The likelihood that she has pathology affecting her caecum and ileum is high, and Crohn’s disease is the most probable diagnosis (1p)
Weigh loss as consequence of malabsorption of nutrients due to a damaged mucosal surface (1p)
Anemia may reflect chronic inflammation, mucosal blood loss, iron deficiency, or vitamin B12 malabsorption (1p) Elevated C-reactive protein is normal in inflammatory conditions. Secreted by the liver in response to macrophage release of IL6 (1p)
3
2) A 28-year-old patient is suffering a relapse of her moderately-active ulcerative colitis. You prescribe her oral prednisolone explaining that, in contrast to her maintenance medication, this will be a short-time treatment due to many potential side effects.
a) Outline pharmacological agents for maintenance treatment of mild to moderately-active ulcerative colitis.
b) Outline two side effects of long term use of prednisolone Max point: 4 Achieved point a) 5-aminosalicilic acid (5-asa or mesalazine) is the first line treatment. Salicilates suppress the inflammatory response and help alleviate the cramping pain. Immunosupresive agents (6-mercaptopurine or azathioprine), cyclosporine, tacrolimus and infliximab (anti tnf-alpha, Remicade) are also used to induce remission. Also DMARDs (2p) b)
Cushing syndrome Thin and pigmented skin
Development or worsening of diabetes Osteoporosis
Psychological effects (mood changes, agitation, dizziness, changes in sleep patterns, etc) Weak/painful muscles
Hypertension Reduced immune response
(1p each)

4
3) A 46-year-old man with previous history of gallstones presents in the emergency ward with severe epigastric pain radiating to the back and vomiting. Standing and walking worsen the pain. The patient tells you that the onset was abrupt and it was not related to alcohol consumption.
a) Give the most likely cause for the patient’s symptoms and outline the pathogenesis. b) Mention at least two physical findings (signs) that might be associated with his
condition Max point: 4 Achieved point
a) Severe epigastric pain radiating to the back is the classical description of acute pancreatitis. Gallstones, produced in the gallbladder, can block the bile duct, stopping pancreatic enzymes from traveling to the small intestine and forcing them back into the pancreas. The enzymes then begin to irritate the cells of the pancreas, causing the inflammation associated with pancreatitis. (2p)
The following physical findings may be noted, varying with the severity of the disease: Fever (76%) and tachycardia (65%); hypotension, Abdominal tenderness, muscular guarding (68%), and distention (65%); diminished or absent bowel sounds, Jaundice (28%), Dyspnea (10%); tachypnea; basilar rales, especially in the left lung. In severe cases, hemodynamic instability (10%) and hematemesis or melena (5%); pale, diaphoretic, and listless appearance. Occasionally, extremity muscular spasm secondary to hypocalcemia. Serum amylase is usually significantly raised but this is not specific as amylase can be raised with other conditions that present with an acute abdomen such as cholecystitis and perforated viscus. (2p)
Here, it was also possible to answer cholecystitis, since symptoms may overlap

5
4) An acutely confused, 15-year-old male patient is admitted to the emergency ward. His father describes that the patient has been feeling unwell for the last couple of days, with flu-like symptoms. You notice a non-blanching skin rash across the patient’s abdomen. Systolic blood pressure 80 mmHg, respiratory rate 25/min, temperature 39°C. The serum lactate levels are elevated. Sepsis is strongly suspected.
a) Provide an explanation for the rise in serum lactate levels b) Describe the immediate actions required for his treatment
Max point: 4 Achieved point
a) Lactic acid is the normal endpoint of the anaerobic breakdown of glucose in the tissues. In solution, lactic acid can lose a proton from the carboxyl group, producing the lactate ion. Elevated lactate is indicative of tissue hypoxia, hypoperfusion, and possible cell damage. (2p)
b) Immediate treatment: Within the first 3 hours:
Administer broad-spectrum antibiotics, administer crystalloids to re-establish fluid balance. Provide adequate ventilation, measure lactate, obtain blood cultures, (1p)
Within 6 hours In the event of persistent arterial hypotension despite fluid resuscitation, apply vasoconstrictors (e.g. IV noradrenalin or dobutamine) and monitor venous pressure (1p)
6
5) The referral of pain to somatic structures is a typical characteristic of visceral painful processes.
a) Outline the mechanisms that explain referred pain from viscera. b) Give an example of referred pain involving an organ of the gastrointestinal system.
Max point: 3 Achieved point
a) Convergence of afferent fibers from viscera and somatic structures entering the CNS at the same level leading to misinterpretation of incoming signals in the higher brain centers. Could be with (convergence/facilitation) or without hypersensitivity (convergence/projection) (1p) b) Examples: Cholecystitis – right shoulder/scapula; gastroesophagic reflux/ulcus – substernal/chest; appendicitis – periumbilical region; pancreas – mid-back; liver/gallbladder – right upper quadrant (1p) 6) Goblet cells, which reside throughout the gastrointestinal (GI) tract, synthesize and secrete mucins.
a) What are the mucins and which is their physiological role? b) Which disease of the GI tract is associated with a biopsy specimen displaying cells
containing abundant amounts of mucin? Max point: 3 Achieved point a) Mucins are large glycoproteins that assemble into a protective gel-like layer that extends upwards to 150 µm of the epithelial surface (1p)
b) The mucin-containing mucus layer coating the GI epithelium is the front line of innate host defense. Mucins are likely to be the first molecules that invading pathogens interact with at the cell surface and thus, can limit binding to other glycoproteins and neutralize the pathogen (1p)
c) (mucinous/colloid) colon adenocarcinomas (1p)
7
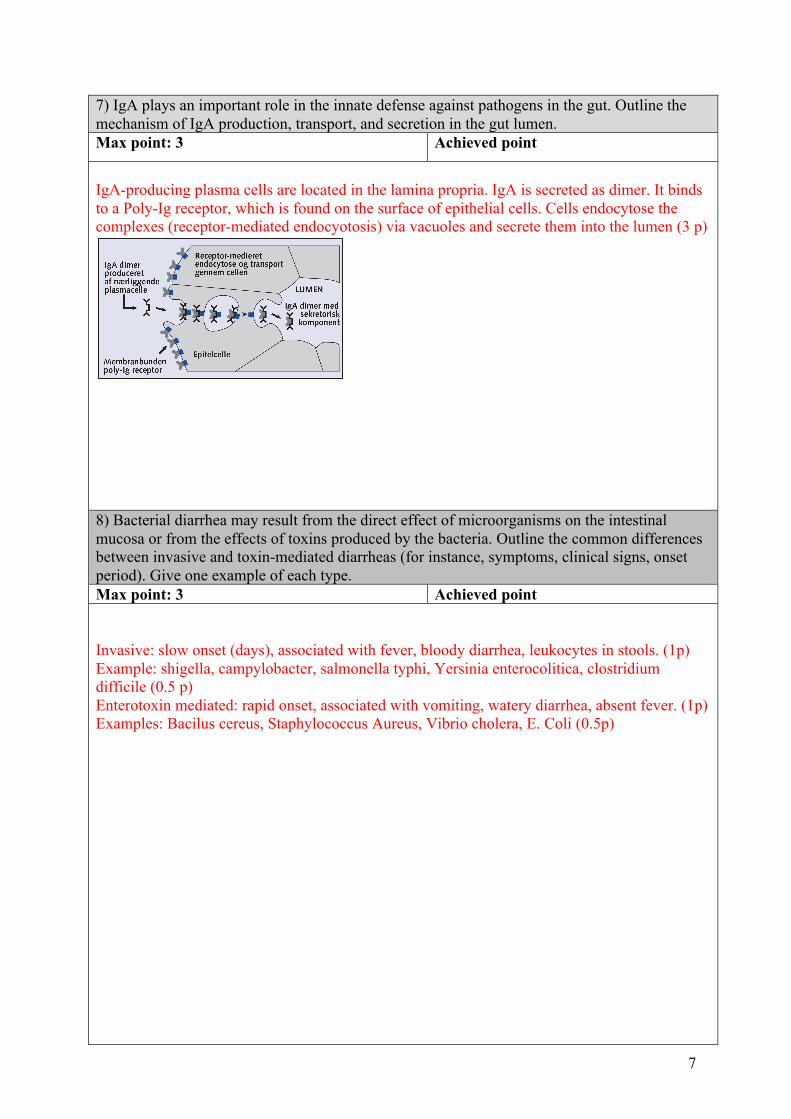
7) IgA plays an important role in the innate defense against pathogens in the gut. Outline the mechanism of IgA production, transport, and secretion in the gut lumen. Max point: 3 Achieved point
IgA-producing plasma cells are located in the lamina propria. IgA is secreted as dimer. It binds to a Poly-Ig receptor, which is found on the surface of epithelial cells. Cells endocytose the complexes (receptor-mediated endocyotosis) via vacuoles and secrete them into the lumen (3 p)
8) Bacterial diarrhea may result from the direct effect of microorganisms on the intestinal mucosa or from the effects of toxins produced by the bacteria. Outline the common differences between invasive and toxin-mediated diarrheas (for instance, symptoms, clinical signs, onset period). Give one example of each type. Max point: 3 Achieved point Invasive: slow onset (days), associated with fever, bloody diarrhea, leukocytes in stools. (1p) Example: shigella, campylobacter, salmonella typhi, Yersinia enterocolitica, clostridium difficile (0.5 p) Enterotoxin mediated: rapid onset, associated with vomiting, watery diarrhea, absent fever. (1p) Examples: Bacilus cereus, Staphylococcus Aureus, Vibrio cholera, E. Coli (0.5p)

8
9) Bacterial overgrowth may lead to a malabsorption syndrome. Define what is a malabsorption syndrome. Outline two more examples. Max point: 3 Achieved point Malabsorption syndromes are disorders in which there is a disorder in digestion (pre-epithelial phase), absorption (epithelial phase), or transport (post-epithelial phase) of nutrients. Strictly speaking, impairment of the first phase is termed maldigestion. (1p) - Pancreatic insufficiency - Lactase deficiency - Bile salt deficiency - Cystic fibrosis - Gluten-sensitive enteropathy (celiaki) - Short bowel syndrome - Bacterial overgrowth (1p each) 10) Explain why bacterial overgrowth in the small intestine may result in malabsorption of fat and steatorrhea. Give an example of a fat-soluble vitamin whose absorption may result impaired and the consequence of its deficiency. Max point: 3 Achieved point Bacterial deconjugation of bile salts may lead to inadequate micelle formation, resulting in decreased fat absorption (1p) Malabsorption of fat soluble vitamins such as A,D, E, K (1p) Example (1p)
9
11) Alcoholic liver disease (ALD) has three main stages. Outline the cellular features of each of these stages. Max point: 3 Achieved point
1. Fatty liver (steatosis): lipogenesis and decreased fatty acid oxidation, lead to accumulation of lipids in hepatocytes. (1p)
2. Alcoholic hepatitis: inflammation, neutrophil infiltration, degeneration and necrosis of hepatocytes (acetaldehyde toxic effects, ROS). Development of intermediate filaments (Mallory bodies), fibrosis. (1p)
3. Cirrhosis: Chronic inflammation and diffuse scarring, obstructing the biliar and vascular channels. Hepatocytes lose capacity of regeneration (1p)
12) Describe the first-pass effect and the consequence for drug bioavailability. Provide an example Max point: 3 Achieved point Following absorption across the gut wall, the portal blood delivers the drug to the liver prior to entry into the systemic circulation. A drug can be metabolized in the gut wall (eg, by the CYP3A4 enzyme system) or even in the portal blood, but most commonly it is the liver that is responsible for metabolism before the drug reaches the systemic circulation. In addition, the liver can excrete the drug into the bile. (1p) Any of these sites can contribute to this reduction in bioavailability. As a consequence larger doses are needed with oral administration than other routes. (1p) Example (1p)

10
13) Describe the how the normal paracetamol metabolism is affected by an overdose leading to hepatocyte damage. Max point: 3 Achieved point Normally paracetamol is metabolized by phase II reactions (glucuronidation and sulfation) to conjugates (1p) but if paracetamol intake far exceeds therapeutic doses (10-15 g), glucuronidation and sulfation pathways are saturated. Alternative P450-dependent pathway becomes important (phase I) producing toxic NAPQI. As long as glutathione (GSH) is available there is little or no hepatotoxicity by NAPQI (1p) But depletion of hepatic GSH leads to accumulation of reactive toxic metabolites that react with nucleophilic groups of cellular proteins and cause hepatotoxicity. Agents that increase GSH: acetylcysteine i.v., methionine i.v.) (1p) 14) You are standing in the line of a fast-food restaurant with a friend. A very loud rumble sound can be heard from his bowel and he tells you that he has not ingested any food in the last three hours. You explain him that this is a completely normal phenomenon, which is caused by activity of the gastrointestinal system in between meals. a) What is the name of this pattern of electromechanical activity occurring in between meals? b) Outline its different phases c) What is its physiological significance? Max point: 3 Achieved point
Migrating motor complex (1p) It consists of three phases: a period of quiescence (I), a period of intermittent activity with increasing frequency (II), and a period of maximal peristaltic activity of the stomach and the small intestine, in which the pylorus remain open (1p)
It sweeps residual undigested material through the digestive tube, which together with gastric, biliary and pancreatic secretions assist in preventing a buildup of bacterial populations in the proximal segments of the digestive tube (1p)
11
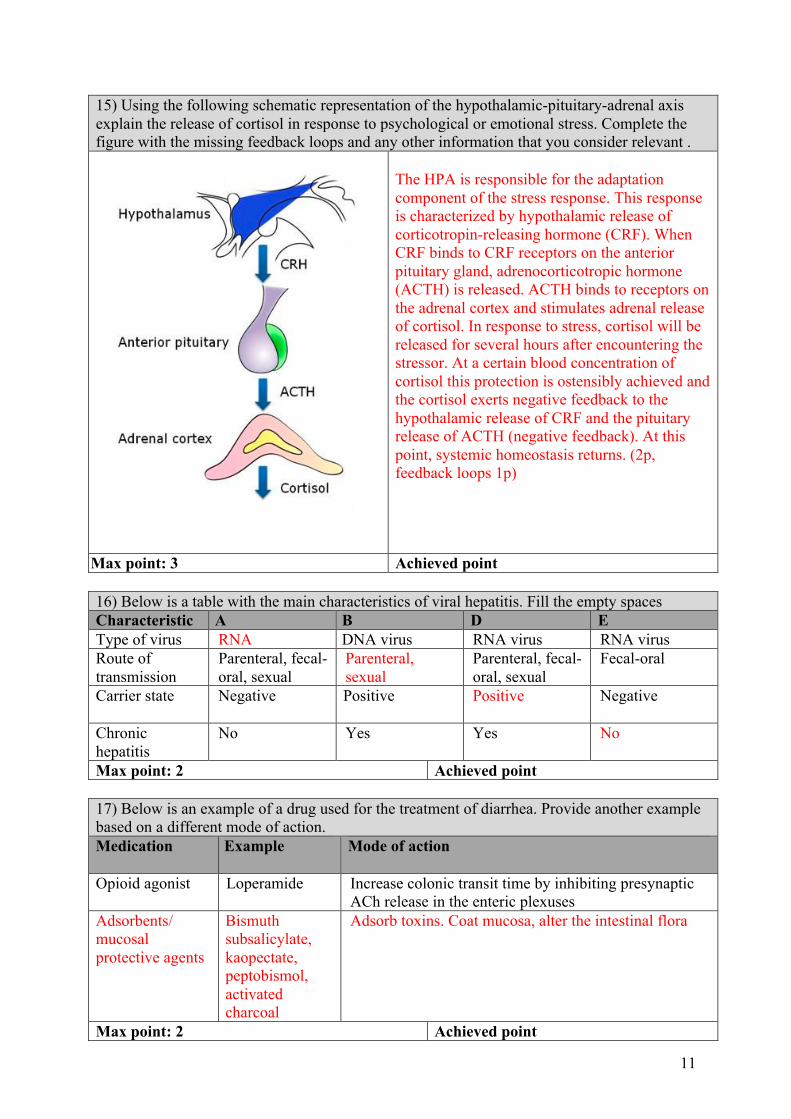
15) Using the following schematic representation of the hypothalamic-pituitary-adrenal axis explain the release of cortisol in response to psychological or emotional stress. Complete the figure with the missing feedback loops and any other information that you consider relevant .
The HPA is responsible for the adaptation component of the stress response. This response is characterized by hypothalamic release of corticotropin-releasing hormone (CRF). When CRF binds to CRF receptors on the anterior pituitary gland, adrenocorticotropic hormone (ACTH) is released. ACTH binds to receptors on the adrenal cortex and stimulates adrenal release of cortisol. In response to stress, cortisol will be released for several hours after encountering the stressor. At a certain blood concentration of cortisol this protection is ostensibly achieved and the cortisol exerts negative feedback to the hypothalamic release of CRF and the pituitary release of ACTH (negative feedback). At this point, systemic homeostasis returns. (2p, feedback loops 1p)
Max point: 3 Achieved point 16) Below is a table with the main characteristics of viral hepatitis. Fill the empty spaces Characteristic A B D E Type of virus RNA DNA virus RNA virus RNA virus Route of transmission
Parenteral, fecal-oral, sexual
Parenteral, sexual
Parenteral, fecal-oral, sexual
Fecal-oral
Carrier state Negative
Positive Positive Negative
Chronic hepatitis
No Yes Yes No
Max point: 2 Achieved point 17) Below is an example of a drug used for the treatment of diarrhea. Provide another example based on a different mode of action. Medication Example
Mode of action
Opioid agonist Loperamide Increase colonic transit time by inhibiting presynaptic ACh release in the enteric plexuses
Adsorbents/ mucosal protective agents
Bismuth subsalicylate, kaopectate, peptobismol, activated charcoal
Adsorb toxins. Coat mucosa, alter the intestinal flora
Max point: 2 Achieved point
12
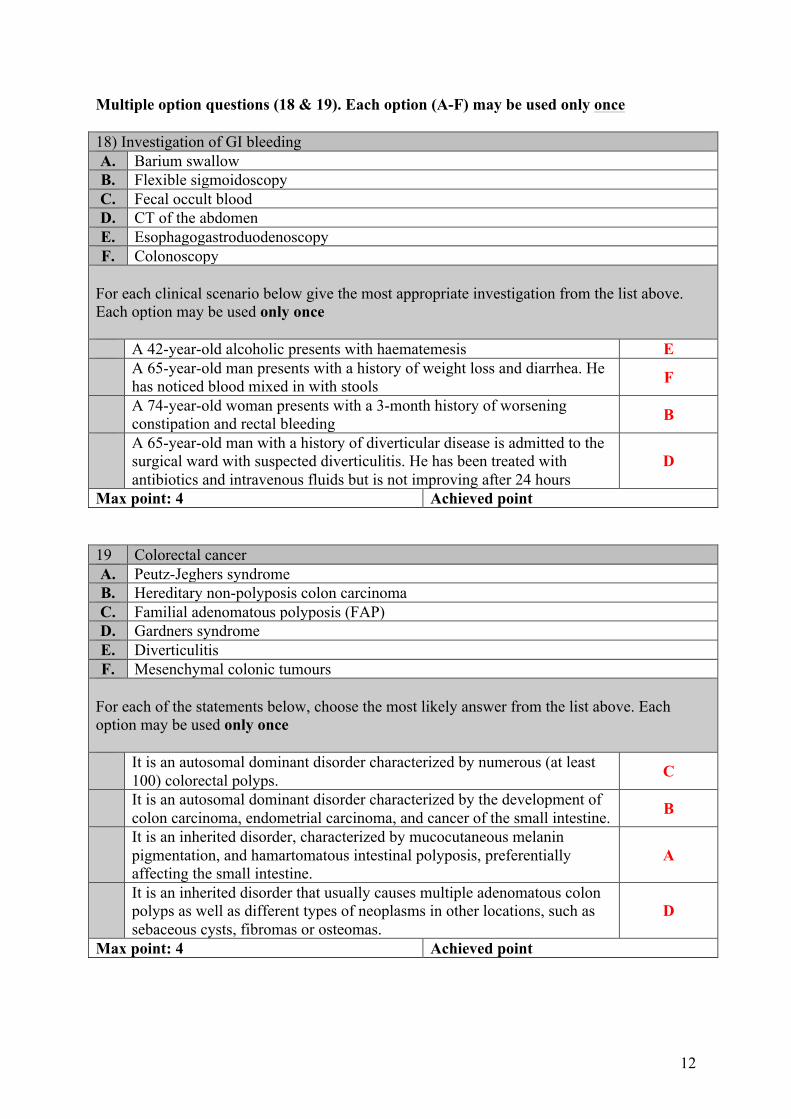
Multiple option questions (18 & 19). Each option (A-F) may be used only once 18) Investigation of GI bleeding A. Barium swallow B. Flexible sigmoidoscopy C. Fecal occult blood D. CT of the abdomen E. Esophagogastroduodenoscopy F. Colonoscopy
For each clinical scenario below give the most appropriate investigation from the list above. Each option may be used only once
A 42-year-old alcoholic presents with haematemesis E A 65-year-old man presents with a history of weight loss and diarrhea. He
has noticed blood mixed in with stools F
A 74-year-old woman presents with a 3-month history of worsening constipation and rectal bleeding B
A 65-year-old man with a history of diverticular disease is admitted to the surgical ward with suspected diverticulitis. He has been treated with antibiotics and intravenous fluids but is not improving after 24 hours
D
Max point: 4 Achieved point 19 Colorectal cancer A. Peutz-Jeghers syndrome B. Hereditary non-polyposis colon carcinoma C. Familial adenomatous polyposis (FAP) D. Gardners syndrome E. Diverticulitis F. Mesenchymal colonic tumours
For each of the statements below, choose the most likely answer from the list above. Each option may be used only once
It is an autosomal dominant disorder characterized by numerous (at least 100) colorectal polyps. C
It is an autosomal dominant disorder characterized by the development of colon carcinoma, endometrial carcinoma, and cancer of the small intestine. B
It is an inherited disorder, characterized by mucocutaneous melanin pigmentation, and hamartomatous intestinal polyposis, preferentially affecting the small intestine.
A
It is an inherited disorder that usually causes multiple adenomatous colon polyps as well as different types of neoplasms in other locations, such as sebaceous cysts, fibromas or osteomas.
D
Max point: 4 Achieved point

13
TRUE-FALSE questions (20-23). Indicate T or F for each option (A-D) 20) Indicate TRUE or FALSE A. Both polyps and early-stage cancers may be asymptomatic T B. Stage I of colon cancer is also known as carcinoma in situ F C. The larger the polyp and the greater the degree of dysplasia, the greater
the risk of colorectal carcinoma development T
D. The most common risk factor for anal carcinoma is Crohn disease F Max point: 2 Achieved point 21) Indicate TRUE or FALSE This microorganism can cause food poisoning and gastroenteritis A. Bacillus cereus T B Campylobacter jejuni T C. Clostridium perfringens T D. Staphylococcus aureus T Max point: 2 Achieved point 22) Indicate TRUE or FALSE … is a clinical consequence of the refeeding syndrome A. Hypophosphatemia T B Hypokalemia T C. Hypoglycemia T D. Decreased fat and protein synthesis F Max point: 2 Achieved point 23) Indicate TRUE or FALSE
Studies have provided evidence showing that … is a risk factor for the development of colon cancer:
A. Inflammatory bowel disease T B High fat, low fiber diet T C. Postmenopausal estrogen use F D. Red meat consumption T Max point: 2 Achieved point Multiple choice questions (24-30). Select only one of the options (A-E). 24) A 30-year-old man hosted a barbecue for a football weekend at which he served chicken. On the Tuesday following the event, the patient and several other people who attended the barbecue developed fever and diarrhea. Stools studies form the patient revealed red blood cells and leukocytes, as well as numerous curved, gram-negative rods. After several days, the patient and other attendees recovered without complications. Which of the following organisms is likely to have caused the diarrhea? A. Brucella spp. B. Candida albicans C. Helicobacter pylori D. Campylobacter jejuni ü E. Clostridium difficile Max point: 1 Achieved point

14
25)The single cell type most typically associated with the MALT is the: A. M-cell (microfold cell) ü B. Dendritic cell C. T-cell D. B lymphocyte E. Mast cell Max point: 1 Achieved point 26) Which one is more likely to feature in Crohn’s disease and not in ulcerative colitis? A. Arthralgia B. Anemia C. Rectal bleeding D. Perianal abscesses ü E. Diarrhea Max point: 1 Achieved point 27) Which of these outcomes are expected for a patient being treated for Addison’s disease? A. Avoiding alcohol to decrease the abdominal fat deposition B. Avoiding hot and uncomfortable environments C. Reporting absence of postural hypotension symptoms ü D. Selecting and eating foods high in protein, calcium and vitamin D E. All of the above Max point: 1 Achieved point 28) Sodium and water retention in a patient with Cushing’s syndrome contribute to which of the following disorders? A. Hypoglicemia and dehydration B. Hypotension and hyperglicemia C. Pulmonary edema and dehydration D. Hypertension and heart failure ü E. None of the above Max point: 1 Achieved point 29) Which of the following signs is NOT associated with hypovolemic shock A. Low blood pressure B. Blood loss > 1000 mL C. High respiratory frequency D. Increased heart rate E. Low aldosterone levels ü Max point: 1 Achieved point 30) Enteric motor neurons are final pathways of the enteric nervous system to the GI musculature. Which of the following neurotransmitters are released by inhibitory neurons? A. Acetylcholine and nitric oxide B. Acetylcholine and serotonin (5-HT) C. Acetylcholine and substance P D. Substance P and vasoactive intestinal peptide E. Nitric oxide and vasoactive intestinal peptide ü Max point: 1 Achieved point





























