Embed Size (px)
Citation preview

Efficacy of Glycolic Acid Peels in the Treatmentof MelasmaMary E. Hurley, MD; Ian L. Guevara, MD; Rose Mary Gonzales, LVN, LME; Amit G. Pandya, MD
Background: Melasma is an acquired hypermelanosisthat is often recalcitrant to treatment with hypopigment-ing agents.
Objective: To assess the efficacy of 4% hydroquinonecream vs 4% hydroquinone cream combined with gly-colic acid peels as treatment for melasma.
Methods: Twenty-one Hispanic women with bilateralepidermal and mixed melasma were enrolled in a split-faced prospective trial lasting 8 weeks. Patients under-went 20% to 30% glycolic acid peels every 2 weeks toone side of the face only in addition to twice-daily full-face application of 4% hydroquinone cream and sun pro-tective factor 25 UV-B sunscreen each morning. Pigmen-tation was measured objectively using a mexameter andthe Melasma Area and Severity Index and subjectively
using a linear analog scale and physician and patient globalevaluation.
Results: Hydroquinone treatment alone and treatmentwith the combination of hydroquinone and glycolic acidhad a significant effect in reducing skin pigmentation com-pared with baseline (P�.001). However, no significantdifference was found using combination therapy com-pared with hydroquinone alone (P=.75).
Conclusions: Use of 4% hydroquinone and a daily sun-screen is effective in the treatment of melasma; how-ever, the addition of 4 glycolic acid peels did not en-hance the hypopigmenting effect of hydroquinonetreatment alone.
Arch Dermatol. 2002;138:1578-1582
M ELASMA IS a commonpigmentary disordercharacterized by thedevelopment of slowlyenlarging tan-brown
macules and patches.1 The condition isseen most commonly on the face of womenwith Fitzpatrick skin types IV to VI, es-pecially among those living in areas of in-tense UV radiation. The cause of me-lasma is multifactorial and includespregnancy, sunlight exposure, hormonetherapy, cosmetic use, and racial or ge-netic effects. Conventional treatment formelasma includes elimination of any pos-sible causative factors coupled with use ofa sunscreen and hypopigmenting agent, of-ten in combination with other therapies,such as tretinoin, topical corticosteroids,or superficial peeling agents.1-9 Despitethese measures, treatment of this recalci-trant disorder is often difficult and frus-trating for the patient and the clinician.
Hydroquinone (HQ) inhibits conver-sion of dopa to melanin by inhibiting ty-rosinase in melanocytes; it is one of the mosteffective agents in the treatment of me-lasma. The combination of HQ with othercompounds has been reported to enhanceits efficacy.1 Glycolic acid has also been re-ported to interfere with melanin produc-tion and to enhance the treatment of me-
lasma, particularly when administered aspart of a hypopigmenting program thatincludes HQ.6,8 Previous trials2,3 using gly-colic acid for melasma have used subjec-tive measures of clinical improvement,lacked standard photography, studiedpatients from different racial back-grounds, or yielded results that are not sta-tistically significant. The purpose of thisstudy is to evaluate the efficacy of using 4%HQ cream alone or as part of a glycolic acidpeel program in the treatment of epider-mal melasma in Hispanic women. We choseonly Hispanic women for this study be-cause of the high frequency of melasma inthis population and to study a uniformpopulation. We sought to assess the clini-cal response objectively by evaluating pa-tients on a split-faced basis using standardcolor and UV photography, a mexameter(Courage & Khazaka Electronic, Cologne,Germany), and the Melasma Area and Se-verity Index (MASI) and subjectively us-ing a linear analog scale and physician andpatient global evaluation.
METHODS
Patients were eligible for the study if they wereHispanic women, aged 18 to 65 years, with Fitz-patrick skin types IV and V and with moder-ate to severe bilateral and symmetrical epider-mal or mixed melasma, confirmed by noting
STUDY
From the Departmentof Dermatology, University ofTexas Southwestern MedicalCenter, Dallas. Dr Hurley isnow with North DallasDermatology Associates, PA.
(REPRINTED) ARCH DERMATOL / VOL 138, DEC 2002 WWW.ARCHDERMATOL.COM1578
©2002 American Medical Association. All rights reserved. at University of Ulsan Asan Medical Library, on July 16, 2008 www.archdermatol.comDownloaded from

enhancement of lesions with a Wood lamp. The study was per-formed with the approval of the University of Texas South-western Medical Center institutional review board. Exclusion-ary criteria included pregnancy, use of HQ within 3 months ofthe study, or history of chemical peels, microdermabrasion, orfacial laser treatment within 9 months of the study. Use of oralcontraceptives was permitted; however, such medications werenot introduced during the study.
After gentle cleansing with cleanser (Gly Derm cleanser;ICN Pharmaceuticals Inc, Costa Mesa, Calif), the degree ofpigmentation on both sides of the face was assessed using themexameter and recorded. A third reading was taken from thesuprasternal notch, which is exposed to light but not to studytreatments, as a control. The mexameter provides reproduc-ible, objective measurement of pigment (melanin) based on theabsorption spectra of light and has an accuracy of ±5%. Mex-ameter readings range from 1 to 1000, with 1 representing whiteand 1000 representing black. Mexameter readings were ob-tained, and a linear analog scale was marked at baseline and atweeks 2, 4, 6, and 8.
Standard and UV photographs and the MASI score for theclinical examination were recorded at baseline and at week 8.The MASI is an index devised to more accurately quantify theseverity of melasma and changes during therapy. The index wasmodified by Kimbrough-Green et al,4 who based it on a similarscoring system devised for psoriasis. The MASI is calculated basedon the area (A) of involvement, the darkness (D) of melasma,and the homogeneity (H) of the hyperpigmentation. The rightforehead (rf), right malar region (rm), and right chin (rc) cor-respond to 15%, 30%, and 5% of the total face, respectively. Thesame regions are measured on the left side, giving a total facialsurface area of 100%. The area of involvement in each of these 6areas is given a numerical value of 0 to 6 (0 indicates no involve-ment; 1, 0%-9%; 2, 10%-29%; 3, 30%-49%; 4, 50%-69%; 5, 70%-89%; and 6, 90%-100%). The severity of melasma is also deter-mined by measuring 2 additional variables: darkness (D) andhomogeneity (H), rated on a scale from 1 to 4 (0 indicates ab-sent; 1, slight; 2, mild; 3, marked; and 4, maximum). The MASIscore is calculated by adding the sum of the severity ratings fordarkness and homogeneity, multiplied by the value of the areaof involvement, for each of the 6 facial areas. The values for eachside are then totaled; for example, MASI right = 0.15[D(rf)+H(rf)] A(rf)+0.3 [D(rm)+H(rm)] A(rm)+0.05 [D(rc)+H(rc)] A(rc). The score for each side is 0 to 24.
The patient underwent a 20% glycolic acid peel (Gly Dermglycolic acid pads; ICN Pharmaceuticals Inc) to one half of theface, which was performed by the nonmasked study nurse(R.M.G.). The side to be peeled was determined by a computer-generated randomization code. Other than the gentle cleansingmentioned previously, no further degreasing was performed. Theduration of the peel varied from 3 to 5 minutes, depending onthe patient’s degree of erythema and discomfort. The patient wasgiven a supply of 4% HQ cream (Eldoquin Forte; ICN Pharma-ceuticals) to apply in the morning and evening on both sides ofthe face; moisturizing cream (Hydrotone Lite; ICN Pharmaceu-ticals Inc), with instructions for bilateral application at night atleast 45 minutes after applying the HQ cream; and sun protec-tion factor 25 UV-B sunscreen (Gly Derm Super Sunblock; ICNPharmaceuticals Inc) to apply to both sides of the face in the morn-ing at least 15 minutes after applying the HQ cream.
At the next visit, a 20% glycolic acid peel was repeated tothe same side of the face as in visit 1. The next 2 visits were thesame as visit 2, except that a higher, 30%, glycolic acid peel wasperformed.The final visit includedaglobal evaluationperformedby the masked investigators (M.E.H., A.G.P.) and the patient.
The data were tested to verify that the assumption of nor-mality was tenable. As a result, the various MASI data sets wereanalyzed using the nonparametric Wilcoxon signed rank test.
The other data sets were analyzed using a paired t test. All testswere 1-sided because improvement is directional in nature.
RESULTS
Twenty-one patients were enrolled in the study. Two pa-tients did not follow the protocol completely, and 1 pa-tient was excluded from data analysis because of equip-ment malfunction. The average duration of the glycolicacid peels was 3 minutes in 6 patients, 4 minutes in 9patients, and 5 minutes in 3 patients. As stated previ-ously, the duration varied, depending on the patient’s de-gree of erythema and discomfort during the peel.
Demographic data are given inTable1. The averageage of the patients was 40 years (range, 23-56 years), andthe average time melasma was present before study entrywas11years(range,2-26years).Foreachparticipant,thevisit5 mexameter readings for the sides treated with HQ aloneand HQ plus peels were compared with the correspondingreadingsforthesameareaatbaseline.TheP�.001(observedsignificance) in both sides indicates a statistically signifi-cant treatmenteffect.Thevalues fromthetreatedareaswerecomparedwith thecontrolvaluesobtained fromthesupra-sternal notch at the same visit. The control values did notvarysignificantly fromthemainvalues, indicatingthat therewas no effect from tanning or other factors that might havealtered the results.For improvementon thenonpeeledandpeeled sides of the face compared with control values,P�.001, indicatinga significant treatmenteffect comparedwithcontrolvalues.Thus,treatmentwithHQaloneandwithHQ plus peels reduces skin pigmentation.
For each participant, the improvement in the areatreated with HQ alone was subtracted from the corre-
Table 1. Patient Demographics
VariablePatients, No. (%)
(N = 18)
Fitzpatrick skin typeIV 9 (50)V 9 (50)
Pattern of melasmaCentrofacial 5 (28)Malar 13 (72)Mandibular 0
Duration of melasma, y0-10 7 (39)11-20 10 (55)21-30 1 (6)
Age, y20-30 3 (17)31-40 8 (44)41-50 5 (28)51-60 2 (11)
History of melasma in a first-degree relative 8 (44)Aggravating factors
Pregnancy 8 (44)Hormonal therapy 4 (22)Sun exposure 7 (39)Cosmetic use 1 (6)
Wood lamp examinationEpidermal 16 (89)Mixed 2 (11)Dermal 0
(REPRINTED) ARCH DERMATOL / VOL 138, DEC 2002 WWW.ARCHDERMATOL.COM1579
©2002 American Medical Association. All rights reserved. at University of Ulsan Asan Medical Library, on July 16, 2008 www.archdermatol.comDownloaded from

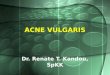
sponding improvement in the area receiving treatmentwith HQ plus peels (P=.75, observed significance); there-fore, there was no significant difference found in the de-gree of lightening of pigmentation using the combina-tion of HQ plus glycolic acid peels compared with HQalone. Figure 1 shows the progression of mean mex-ameter readings, reflecting that although both groups im-proved during the study, there was no statistically sig-nificant difference between treatments.
Figure 2 reveals that there was no significant dif-ference in the MASI scores from baseline to the end ofthe study using treatment with HQ alone compared withHQ plus glycolic acid peels. Similar results were foundwith MASI scores from color and UV slides. The resultsof the linear analog scale also revealed that there was nosignificant difference between the degree of improve-ment when using HQ alone compared with HQ with gly-colic acid peels.
Physician global evaluation results showed that 8patients had more improvement on the peeled side and7 were thought to have more improvement on the non-peeled side compared with baseline photographs(Table 2). Two patients were thought to have no dif-ference between the 2 sides. However, in patient globalevaluation of pigmentation, 11 patients thought that theyhad more improvement on the peeled side and 4 thoughtthat they had more improvement on the nonpeeled side(Table 2). Figure 3 and Figure 4 demonstrate im-provement in 1 patient during the study.
COMMENT
The use of alpha hydroxy acids, particularly glycolic acid,has expanded dramatically during the past decade for thetreatment of skin disorders, including hyperpigmenta-tion. Because of their relative safety profile compared withstronger agents such as trichloracetic acid, glycolic acid peelsare often used by dermatologists, plastic surgeons, aesthe-ticians, and other skin care specialists. Indeed, because mostof the world’s population is brown or dark skinned, a greatdeal of effort and expense for the performance of peels isbeing dedicated to the treatment of disorders of hyperpig-mentation, particularly melasma. Hydroquinone has beenshown to be safe and effective in the treatment of me-lasma and other types of hyperpigmentation.5 Studies evalu-ating the efficacy of glycolic acid peels for melasma thusfar have been uncontrolled trials, have been too small toyield statistically significant results, have used subjectivemethods of evaluation, or have not studied a uniformpatient population.2,3
We sought to perform a randomized, controlled, in-vestigator-masked, split-faced prospective trial using a uni-form population and recently developed objective meth-ods of evaluation to determine whether glycolic acid peelshasten improvement of melasma with concomitant use ofHQ. Our study demonstrated statistically significant im-provement on both sides of the face from baseline, withno significant difference on the side that was peeled. Thisimprovement was also noted on subjective analysis, as phy-sician and patient global evaluations revealed that most pa-tients had at least moderate improvement. We controlledfor sun exposure by using the patient as her own control,measuring pigmentation at the suprasternal notch, a sun-exposed but untreated site. The measurement taken at thesuprasternal notch revealed no significant difference in pig-mentation throughout the study.
The results of the linear analog scale correlated withthe other findings in that there was no significant differ-ence in thedegreeof improvementusingHQalonevscom-bination therapy with HQ and glycolic acid peels. Further-more, physician global evaluation results supported thesefindings in that the treatment-masked investigator couldnot detect a greater degree of improvement on either sideof the face.Thepatientglobalevaluation,however, revealedthat almost three fourths of the patients noted improve-ment on the side that was peeled. This subjective patientbias emphasizes the importance of masking and controlsin the performance of clinical trials. It may also explainwhyglycolic acidpeels are sopopular amongpatients.Per-haps the smoothening and softening of the skin producedbythesepeels is responsible for theirhighacceptanceratherthan their ability to reduce hyperpigmentation.
Standardized photographs were taken of all pa-tients with 35-mm color, polarized color, and UV pho-tographs at baseline and at the end of the study (stereo-tactic camera; Canfield Scientific Inc, Fairfield, NJ).Ultraviolet reflectance photography is especially usefulfor detecting changes in pigmentation over time, as epi-dermal melanin detection using UV photography is 10times more sensitive than with visible light.10,11
The use of polarized filters with color photographywas an excellent method of enhancing pigmentation in
550
540
530
520
5101 2 3 4 5
Visit Number
Mex
amet
er R
eadi
ng
Hydroquinone OnlyHydroquinone and Peels
Figure 1. Progression of mean mexameter readings during the study showsthat although both treatment groups improved, there was no statisticallysignificant difference between the 2 groups.
6
5
4
31 5
Visit Number
MAS
I Sco
re
Hydroquinone OnlyHydroquinone and Peels
Figure 2. Improvement in clinical Melasma Area and Severity Index (MASI)scores during the study showed a beneficial effect within both groups(P�.01 for hydroquinone only and P=.02 for hydroquinone and peeled) butno difference between groups (P=.15).
(REPRINTED) ARCH DERMATOL / VOL 138, DEC 2002 WWW.ARCHDERMATOL.COM1580
©2002 American Medical Association. All rights reserved. at University of Ulsan Asan Medical Library, on July 16, 2008 www.archdermatol.comDownloaded from

photographs of patients, as shown in Figure 3 and Fig-ure 4. Ultraviolet reflectance photography is also a valu-able tool to accentuate pigmentation; however, patientsmust wash and degrease the face before photography toprevent reflection from the skin surface, which ob-scures the assessment of pigmentation. The mexameterserved as a reproducible, easy-to-use tool for the objec-tive measurement of pigmentation.
The effect of glycolic acid peels on skin is deter-mined by the concentration of the acid, pH, product for-
mulation, duration of time the acid remains on the skin,skin thickness, and sensitivity.12 The glycolic acid usedin this study was a nonbuffered, nonneutralized gly-colic acid ester with a pH of 1.5 (20%) and 1.1 (30%) inindividually packaged moistened pads. Although higherconcentrations of glycolic acid could have been used, gly-colic acid peels greater than 30% often lead to irritationand may cause paradoxical hyperpigmentation in brown-skinned patients. An adequate peel was obtained in ourpatients using 20% and 30% glycolic acid based on the
Table 2. Physician and Patient Global Evaluation of Which Side Had Improved, and to What Degree,Compared With the Opposite Side*
Variable
Physicians, No. (N = 18) Patients, No. (N = 18)
Peeled Side Nonpeeled Side Total Peeled Side Nonpeeled Side Total
Slight improvement, barely noticeable 1 1 2 0 0 0Moderate improvement, noticeable 1 4 5 2 2 4Obvious improvement 6 2 8 5 2 7Very marked improvement 0 0 0 4 0 4Subtotal 8 7 15 11 4 15No difference between the 2 sides and no improvement NA NA 2 NA NA 1Total 17† 16‡
*NA indicates not applicable.†Physician global evaluation was not performed on 1 patient.‡Patient global evaluation was not performed by 2 patients.
A B
Figure 3. Standard photography using polarized filters at baseline (A) and at the end of the study (B) on the nonpeeled side of a patient with Fitzpatrick skin type IV.
(REPRINTED) ARCH DERMATOL / VOL 138, DEC 2002 WWW.ARCHDERMATOL.COM1581
©2002 American Medical Association. All rights reserved. at University of Ulsan Asan Medical Library, on July 16, 2008 www.archdermatol.comDownloaded from

observation that most felt some tingling during the peelor developed mild erythema. Indeed, only 3 patients wereable to tolerate a peel duration of 5 minutes. Four pa-tients developed significant erythema with the 20% and30% peels, without epidermolysis or erosions, indicat-ing that higher-strength peels might have resulted ingreater morbidity.
Because improvement was noted on both sides ofthe face after 8 weeks, we conclude that 4% topical HQwith a daily sunscreen is effective in the treatment of me-lasma. The application of 4 glycolic acid peels of 20% to30% in 8 weeks did not enhance the hypopigmenting effectof HQ alone. Further studies using patients of differentracial backgrounds, more peels over a longer period, dif-ferent peeling agents, or combined with recently devel-oped treatments such as microdermabrasion might beconsidered in the future to find better ways of treatingmelasma.
Accepted for publication March 23, 2002.This study was supported by a grant from ICN Phar-
maceuticals Inc.This study was presented as a poster at the 58th an-
nual meeting of the American Academy of Dermatology, SanFrancisco, Calif, March 10-15, 2000.
We thank William H. Frawley, PhD, for assistance withstatistical analysis.
Corresponding author and reprints: Amit G. Pandya,MD, Department of Dermatology, University of Texas South-
western Medical Center, 5323 Harry Hines Blvd, Dallas, TX75390-9190 (e-mail: [email protected]).
REFERENCES
1. Pandya AG, Guevara IL. Disorders of pigmentation. Dermatol Clin. 2000;18:91-98.2. Lawrence N. Treatment of melasma with Jessner’s solution versus glycolic acid:
a comparison of clinical efficacy and evaluation of the predictive ability of Wood’slight examination. J Am Acad Dermatol. 1997;36:589-593.
3. Lim JTE, Tham SN. Glycolic acid peels in the treatment of melasma amongAsian women. Dermatol Surg. 1997;23:177-179.
4. Kimbrough-Green CK, Griffiths CEM, Finkel LJ, et al. Topical retinoic acid (treti-noin) for melasma in black patients. Arch Dermatol. 1994;130:727-733.
5. Engasser PG, Maibach HI. Cosmetics and dermatology: bleaching creams. J AmAcad Dermatol. 1981;5:143-147.
6. Garcia A, Fulton JE. The combination of glycolic acid and hydroquinone or kojicacid for the treatment of melasma and related conditions. Dermatol Surg.1996;22:443-447.
7. Murad H, Shambar AT, Moy LS. Polka-dot syndrome. Cosmet Dermatol. 1993;4:57-58.
8. Van Scott EJ, Yu RJ. Alpha hydroxy acids: procedures for use in clinical prac-tice. Cutis. 1989;43:222-229.
9. Griffiths CEM, Finkel LJ, Ditre CM, Hamilton TA, Ellis CN, Voorhees JJ. Topicaltretinoin (retinoic acid) improves melasma: a vehicle-controlled, clinical trial.Br J Dermatol. 1993;129:415-421.
10. Fulton JE Jr. Utilizing the ultraviolet (UV Detect) camera to enhance the appearanceof photodamage and other skin conditions. Dermatol Surg. 1997;23:163-169.
11. Kollias N, Gillies R, Cohen-Goihman C, et al. Fluorescence photography in theevaluation of hyperpigmentation of photodamaged skin. J Am Acad Dermatol.1997;36:226-230.
12. Becker FF, Langford FPJ, Rubin MG, Speelman P. A histological comparison of50% and 70% glycolic acid peels using solutions with various pHs. DermatolSurg. 1996;22:463-465.
A B
Figure 4. Standard photography using polarized filters at baseline (A) and at the end of the study (B) on the peeled side of a patient with Fitzpatrick skin type IV.
(REPRINTED) ARCH DERMATOL / VOL 138, DEC 2002 WWW.ARCHDERMATOL.COM1582
©2002 American Medical Association. All rights reserved. at University of Ulsan Asan Medical Library, on July 16, 2008 www.archdermatol.comDownloaded from