Embed Size (px)
Citation preview

Endodontic management of maxillary permanent first molarwith 6 root canals: 3 case reportsDenzil Valerian Albuquerque, BDS,a Jojo Kottoor, BDS,a Sonal Dham, BDS,a
Natanasabapathy Velmurugan, MDS,b Mohan Abarajithan, MDS,c and Rajmohan Sudha, MDS,d
Tamil Nadu, IndiaMEENAKSHI AMMAL DENTAL COLLEGE AND HOSPITAL
This article discusses the successful endodontic management of 3 permanent maxillary first molars presentingwith the anatomical variation of 3 roots and 6 root canals. A literature review pertaining to the variable root canalmorphology of the permanent maxillary first molar is also presented. Modifications in the root canal accesspreparation and methods for examination of the pulpal floor with the aid of magnification for identification of
additional canals are emphasized. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:e79-e83)The goal of root canal treatment is to clean and shapethe root canal system and obturate it in all of itsdimensions.1 Aberrant root or root canal morphologywhen present should be adequately detected andtreated. Failure to recognize any unusual canal config-uration would eventually lead to unsuccessful treatmentoutcome.2 Thus, a thorough knowledge of the root androot canal morphology along with their various ana-tomical variations is essential so as to reach this goal.
The root canal anatomy of maxillary first molars hasbeen described as 3 roots with 3 canals and the common-est variation is the presence of a second mesiobuccal canal(MB2). The incidence of MB2 has been reported to bebetween 56.8% and 96.1%.3-5 Apart from these usualpresentations, a wide variation of root canal configurationsof the maxillary first molars have been documented innumerous case reports. These range from a single rootcanal in a single root,6 C-shaped canals,7 2 root canals,2 5root canals,8 and 6 root canals.9 Recently, Kottoor et al.10
reported the endodontic management of a maxillary firstmolar with 7 root canals. Cleghorn et al.3 reported that theincidence of a second root canal in the distobuccal root is
aPostgraduate Student, Department of Conservative Dentistry andEndodontics, Meenakshi Ammal Dental College and Hospital, TamilNadu, India.bProfessor and Head of Department, Department of ConservativeDentistry and Endodontics, Meenakshi Ammal Dental College andHospital, Tamil Nadu, India.cSenior Lecturer, Department of Conservative Dentistry and End-odontics, Meenakshi Ammal Dental College and Hospital, TamilNadu, India.dReader, Department of Conservative Dentistry and Endodontics,Meenakshi Ammal Dental College and Hospital, Tamil Nadu, India.Received for publication Mar 28, 2010; accepted for publication Apr8, 2010.1079-2104/$ - see front matter© 2010 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2010.04.0171.7% and less than 1.0% in the palatal root. This articlediscusses the successful nonsurgical endodontic manage-ment of 3 permanent maxillary first molars presentingwith the anatomical variation of 3 roots and 6 canals.
CASE REPORTSThese are the case reports of 3 patients treated in the Depart-
ment of Conservative Dentistry and Endodontics, MeenakshiAmmal Dental College, Chennai, India. A thorough history wasrecorded, and the cases were examined both clinically and ra-diographically. The medical history of all patients was noncon-tributory. Vitality testing of the involved tooth was carried outwith heated gutta-percha (Dentsply Maillefer, Ballaigues, Swit-zerland), cold test (RC Ice, Prime Dental Products Pvt. Ltd.,Mumbai, India), and electronic pulp stimulation (Parkel Elec-tronics Division, Farmingdale, NY). Local anesthesia was ob-tained with 1.8 mL (30 mg) of 2% lignocaine containing1:200,000 epinephrine (Xylocaine, AstraZeneca Pharma IndLtd, Bangalore, India). The entire procedure in each case wascarried out using rubber dam isolation under a surgical operatingmicroscope (Seiler Revelation Microscope, St. Louis, MO). Theworking length was determined with the apex locator (Root ZX;Morita, Tokyo, Japan) and confirmed radiographically. Cleaningand shaping were performed using a crown-down technique withProTaper series Ni-Ti rotary instruments (Dentsply Maillefer,Ballaigues, Switzerland) with irrigation using normal saline, 3%sodium hypochlorite, and 17% EDTA (Prime Dental ProductPvt. Ltd.). All canals were dried with absorbent points (DentsplyTulsa, Tulsa, OK) and obturated using cold, laterally compactedgutta-percha and AH Plus sealer (Dentsply Tulsa). Each toothwas then restored with a posterior composite resin core (P60; 3MDental Products, St Paul, MN). The patients were asymptomaticin the subsequent follow-up period.
Case 1A 55-year-old male patient presented with the chief com-
plaint of “toothache in his left upper back tooth.” The painwas continuous and had intensified for 3 days, with a history
of intermittent pain over the preceding 3 months. Clinicale79

gurati
OOOOEe80 Albuquerque et al. October 2010
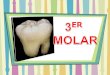
examination revealed deep mesio-occlusal and disto-occlusaldecay in #14. Probing depths and mobility were within phys-iological limits. The tooth was nontender to palpation andpercussion. Thermal tests caused an intense lingering pain,whereas electronic pulp stimulation produced a prematureresponse. Radiographic examination revealed a radiolucentlesion on the mesial and distal aspects of the coronal portionextending toward the pulpal outline. The lamina dura wasintact with no apparent periodontal ligament space widening(Fig. 1, A). These findings led to a diagnosis of symptomaticirreversible pulpitis for which endodontic treatment was sug-gested to the patient.
Caries was excavated from the mesial and distal surfacesof the tooth followed by composite resin restoration (P60; 3MDental Products) to allow for optimal isolation. After obtain-ing adequate anesthesia, an endodontic access cavity wasestablished under isolation with rubber dam. Clinical exam-ination of the pulpal floor with a DG-16 endodontic explorer(Hu-Friedy, Chicago, IL) under a surgical operating micro-scope presented the anatomy of the tooth as follows: 2 orificesin the mesiobuccal root (MB1, MB2), 2 orifices in the disto-buccal root (DB1, DB2), and 2 orifices in the palatal root(mesiopalatal [MP], distopalatal [DP]) (Fig. 1, B). Explora-tion of the canals with a size 10 ISO K-file (Mani, Inc.,Tochigi, Japan) revealed that the canals in each root fusedbefore exit as a single foramen. The working length wasdetermined (Fig. 1, C) and the canals were medicated withcalcium hydroxide and the tooth temporized using interme-diate restorative material (IRM) (Dentsply De Trey GmbH,
Fig. 1. A, Preoperative radiograph of the maxillary left first mof the 6 canal orifices on the pulpal floor. MB, mesiobuccal;length radiograph demonstrating Vertucci Type II canal confi
Konstanz, Germany). At the next visit a week later, under
rubber dam isolation, instrumentation and obturation werecompleted followed by composite restoration (Fig. 1, D).
Case 2A 45-year-old male patient reported with the chief com-
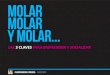
plaint of pain in the right maxillary region for the preceding2 weeks. Clinical examination revealed a carious right max-illary first molar (#3) that was tender to percussion. A diag-nosis of necrotic pulp with symptomatic apical periodontitiswas made necessitating endodontic treatment (Fig. 2, A).Inspection of the pulpal floor with an operating microscoperevealed 6 distinct orifices (Fig. 2, B), similar to the previ-ously described case (MB1, MB2, DB1, DB2, MP, DP). Canalpatency was established with #10 K-file (Mani, Inc.), whichrevealed that the 2 canals in the palatal and the distobuccalroots merged into a single canal before exit from the apicalforamen. However, in the mesiobuccal root, the 2 canalsremained separate along their entire length with 2 portals ofexit at the apex (Fig. 2, C). Working length was confirmed;the canals were instrumented and medicated with calciumhydroxide followed by temporization using IRM (DentsplyDe Trey GmbH). At the second appointment a week later, thepatient was asymptomatic. The canals were obturated andaccess cavity was restored using composite restorative mate-rial (Fig. 2, D).
Case 3A 32-year-old female patient reported with the chief com-
ooth #14). B, Access cavity preparation showing the locationistobuccal; MP, mesiopalatal; DP, distopalatal. C, Workingon in the 3 roots. D, Postoperative radiograph.
olar (tDB, d
plaint of sharp, continuous pain in the upper left region.

n radi
OOOOEVolume 110, Number 4 Albuquerque et al. e81
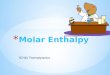
Clinical examination revealed a carious mesio-occlusal lesionin #14. A diagnosis of symptomatic irreversible pulpitis wasmade necessitating endodontic treatment (Fig. 3, A). Inspec-tion of the pulpal floor with an operating microscope revealed6 distinct orifices (Fig. 3, B). Exploration of the canals re-vealed a canal configuration similar to that previously de-scribed in the first case (Fig. 3, C). The canals were instru-mented and obturated. The access cavity was restored usingcomposite restorative material (Fig. 3, D).
DISCUSSIONMartinez-Berna and Ruiz-Badanelli9 were the first to
report 3 cases of maxillary first molars with 6 canals: 3canals in the mesiobuccal root, 2 in the distobuccalroot, and 1 in the palatal root (3 MB, 2 DB, and 1palatal). Other authors have also reported cases with 6or more root canals in the maxillary first molar (sum-marized in Table I).9-14 The present cases describe 3different root canal configurations in the maxillary firstmolar with 6 canals. In the first and third cases, eachroot had 2 canals that fused to form a single canalbefore exit into a single apical foramen (Vertucci TypeII canal configuration).15 In the second case, the palataland distobuccal roots presented with a Vertucci Type IIcanal configuration, whereas the mesiobuccal root had 2
Fig. 2. A, Preoperative radiograph of the maxillary right firstof the 6 canal orifices on the pulpal floor. MB, mesiobuccal;length radiograph showing the Vertucci Type II canal configcanal configuration in the mesiobuccal root. D, Postobturatio
canals that did not fuse along their course and exited as 2
separate foramina (Vertucci Type III canal configura-tion).15 Although the incidence of such root canal varia-tions is rare, as far as the prognosis of individual cases isconcerned, their importance should not be underestimated.
A thorough understanding of tooth morphology16 andmultiple angulated preoperative radiographs17 are invalu-able prerequisites for endodontic treatment. Modified ac-cess cavity preparation is often required for successfulmanagement of teeth with extra canals.18 To achieve astraight-line access, the conventional triangular accesscavity can be modified into many shapes such as cloverleaf–like (shamrock),19 heart,20 trapezoidal,8,21 rectan-gular,22 rhomboidal,23 and ovoid24 shapes, depending on theparticular clinical situation. Pulp chamber floor and wallanatomy provide a guide to determine what morphology isactually present.25 Krasner and Rankow26 put forth lawsthat are valuable aids to the clinician in searching forelusive canals. Weller and Hartwell27 found that examin-ing the grooves and exploring them with ultrasonics in-creases the number of fourth canals found and treated inmaxillary molars.27 Use of magnification was also shownto increase the percentage of located and treated extracanals in maxillary molars.28 The search for an extraorifice is further aided by the use of fiber-optic transillu-
(tooth #3). B, Access cavity preparation showing the locationistobuccal; MP, mesiopalatal; DP, distopalatal. C, Workingin the distobuccal and palatal roots, and Vertucci Type III
ograph.
molarDB, d
uration
mination to locate the developmental line between the

adiogr
, disto
OOOOEe82 Albuquerque et al. October 2010
mesiobuccal and mesiolingual orifices. A DG-16 end-odontic probe used as a pathfinder determines the angle atwhich the canals depart from the main chamber. Adjunc-tive diagnostic measures such as staining the chamberfloor with 1% methylene blue dye, performing the sodiumhypochlorite “champagne bubble test,” and visualizingcanal bleeding points are important aids in locating rootcanal orifices.25 The clinician should be suspicious ofadditional canals if endodontic files are not well centeredin the canal either clinically during exploration of thecanals or radiographically during working length determi-nation.8 Although there are inherent limitations, radio-
Fig. 3. A, Preoperative radiograph of #14. B, Access cavity pfloor. MB, mesiobuccal; DB, distobuccal; MP, mesiopalatal; DType II canal configuration in all 3 roots. D, Postoperative r
Table I. Summary of case reports of maxillary first m
Root configurationNo. ofcanals
Root c
Mesiobuccal Distobuc
3 roots 6 3 2
3 roots 6 2 23 roots 6 2 14 roots (MB, MP, P, DB) 6 MB, MP3 roots 6 2 23 roots 6 2 23 roots 7 3 2
MB, mesiobuccal; MP, mesiopalatal; P, palatal; DB, distobuccal; DP
graphs provide a clue to the type of canal configuration
present.29 In the presented cases, a modified access cavitywas prepared under the surgical operating microscope(Fig. 1, B, Fig. 2, B, Fig. 3, B); ultrasonic troughing of thedentin located between the major orifices was also neededto detect the extra canals.
Previous reports have used recent imaging technol-ogies like spiral computed tomography (SCT)6,21 andcone-beam computed tomography (CBCT)10,30 as anadjunctive aid for detection and management of vari-able root canal morphology. These recent imaging tech-nologies and the use of operating microscopes may behelpful in detecting variations of root canals in doubtful
tion showing the location of the 6 canal orifices on the pulpalopalatal. C, Working length radiograph showing the Vertucciaph.
presenting with 6 or more root canalsatomy
ReferencePalatal
1 Martínez-Berná and Ruiz-Badanelli(1983) (3 cases)9
2 Bond et al. (1988)11
3 (apical third trifurcation) Maggiore et al. (2002)12
, DP, DB Adanir (2007)13
2 de Almeida-Gomes et al. (2009)14
2 Present cases2 Kottoor et al. (2010)10
palatal; M, mesial.
reparaP, dist
olarsanal an
cal
, M, P
circumstances related to unusual root canal anatomy. In

OOOOEVolume 110, Number 4 Albuquerque et al. e83
the present case, radiographs of different angulationsand clinical examination of the floor of the pulp cham-ber clearly depicted the variable anatomy. Hence, ad-vanced imaging techniques (SCT and CBCT) were notused. Although these imaging modalities offer an in-sight into the anatomical variations of the root or rootcanal configuration, they also potentially increase the ef-fective dose of radiation exposure for the patient.31 Addi-tionally, such equipment may not always be present inpractice.
CONCLUSIONReports of cases with unusual morphology have an
important didactic value. Their documentation in casereports may facilitate the recognition and successfulmanagement of similar cases should they require end-odontic therapy. These case reports may intensify thecomplexity of maxillary first molar variation and areintended to reinforce clinicians’ awareness of the vari-able morphology of root canals.
REFERENCES1. Cohen S, Burns RC, editors. Pathways of the pulp. 7th ed. St.
Louis, MO: Mosby Co; 1998. p. 258-368.2. Ma L, Chen J, Wang H. Root canal treatment in an unusual
maxillary first molar diagnosed with the aid of spiral computer-ized tomography and in vitro sectioning: a case report. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2009;107:e68-73.
3. Cleghorn BM, Christie WH, Dong CCS. Root and root canalmorphology of the human permanent maxillary first molar: aliterature review. J Endod 2006;32:813-21.
4. Imura N, Hata GI, Toda T, Otani SM, Fagundes MI. Two canalsin mesiobuccal roots of maxillary molars. Int Endod J1998;31:410-4.
5. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect ofmagnification on locating the MB2 canal in maxillary molars. JEndod 2002;28:324-7.
6. Gopikrishna V, Bhargavi N, Kandaswamy D. Endodontic man-agement of a maxillary first molar with a single root and a singlecanal diagnosed with the aid of spiral CT: a case report. J Endod2006;32:687-91.
7. De Moor RJG. C-Shaped root canal configuration in maxillaryfirst molars. Int Endod J 2002;35:200-8.
8. Johal S. Unusual maxillary first molar with 2 palatal canalswithin a single root: a case report. J Can Dent Assoc 2001;67:211-4.
9. Martinez-Berná A, Ruiz-Badanelli P. Maxillary first molars withsix canals. J Endod 1983;9:375-81.
10. Kottoor J, Velmurugan N, Sudha R, Hemamalathi S. Maxillaryfirst molar with seven root canals diagnosed with cone-beamcomputed tomography scanning: a case report. J Endod 2010;36:915-21.
11. Bond JL, Hartwel G, Portell FR. Maxillary first molar with sixcanals. J Endod 1988;14:258-60.
12. Maggiore F, Jou YT, Kim S. A six-canal maxillary first molar:case report. Int Endod J 2002;35:486-91.
13. Adanir N. An unusual maxillary first molar with four roots andsix canals: a case report. Aust Dent J 2007;52:333-5.
14. de Almeida-Gomes F, Maniglia-Ferreira C, Carvalho de Sousa
B, Alves dos Santos R. Six root canals in maxillary first molar.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e157-9.
15. Vertucci FJ. Root canal anatomy of the human permanent teeth.Oral Surg Oral Med Oral Pathol 1984;5:589-99.
16. Burns RC, Herbranson EJ. Tooth morphology and access cavitypreparation. In: Cohen S, Burns RC, editors. Pathways of thepulp. 8th ed. St Louis, MO: Mosby Inc; 2002. p. 173-229.
17. Fava LR, Dummer PM. Periapical radiographic techniques dur-ing endodontic diagnosis and treatment. Int Endod J 1997;30:250-61.
18. Velmurugan N, Parameswaran A, Kandaswamy D, Smitha A,Vijayalakshmi D, Sowmya N. Maxillary second premolar withthree roots and three separate root canals-case reports. AustEndod J 2005;31:73-5.
19. Ingle JI, Backland LK, Peters DD, Buchanan S, Mullaney TP.Endodontic cavity preparation. In: Ingle JI, Backland LK, edi-tors. Endodontics. 4th ed. Baltimore, MD: Williams and Wilkins;1994. p. 96-8.
20. Neaverth EJ, Kotler LM, Kattenback RF. Clinical investigationof endodontically treated maxillary molars. J Endod 1997;13:506-12.
21. Aggarwal V, Singla M, Logani A, Shah N. Endodontic manage-ment of a maxillary first molar with two palatal canals with theaid of spiral computed tomography: a case report. J Endod2009;35:137-9.
22. Ghoddusi J, Mesgarani A, Gharagozloo S. Endodontic re-treat-ment of maxillary second molar with two separate palatal roots:a case report. Iranian Endodontic Journal 2008;3:83-5.
23. Stropko JJ. Canal morphology of maxillary molars: clinical ob-servations of canal configurations. J Endod 1999;25:446-50.
24. Christie WH, Thompson GK. The importance of endodonticaccess in locating maxillary and mandibular molar canals. J CanDent Assoc 1994;60:527-32, 535-6.
25. Vertucci FJ. Root canal morphology and its relationship to end-odontic procedure. Endod Topics 2005;10:3-29.
26. Krasner P, Rankow HJ. Anatomy of the pulp-chamber floor.J Endod 2004;30:5-16.
27. Weller RN, Hartwell GR. The impact of improved access andsearching techniques on detection of the mesiolingual canal inmaxillary molars. J Endod 1989;15:82-3.
28. Gorduysus MO, Gorduysus M, Friedman S. Operating micro-scope improves negotiation of second mesiobuccal canals inmaxillary molars. J Endod 2001;27:683-6.
29. Hildebolt CF, Vannier MW, Pilgram TK, Shrout MK. Quantita-tive evaluation of digital dental radiograph imaging systems.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1990;70:661-8.
30. Kottoor J, Hemamalathi S, Sudha R, Velmurugan N. Maxillarysecond molar with 5 roots and 5 canals evaluated using conebeam computerized tomography: a case report. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2010;109:e162-5.
31. Patel S, Dawood A, Whaites E, Pitt Ford T. New dimensions inendodontic imaging: part 1. Conventional and alternative radio-graphic systems. Int Endod J 2009;42:447-62.
Reprint requests:
Jojo Kottoor, BDSPostgraduate StudentDepartment of Conservative Dentistry and EndodonticsMeenakshi Ammal Dental College and HospitalAlapakkam Main RoadMaduravoyal, Chennai – 600 095Tamil Nadu, India
[email protected]