Embed Size (px)
Citation preview
Dirigente medico
Centro Sterilità P. Bertocchi
S.O.C. Ostetricia e Ginecologia, Dipartimento Ostetrico, Ginecologico e Pediatrico
A.O. Arcispedale S.Maria Nuova, Reggio Emilia
MT Villani
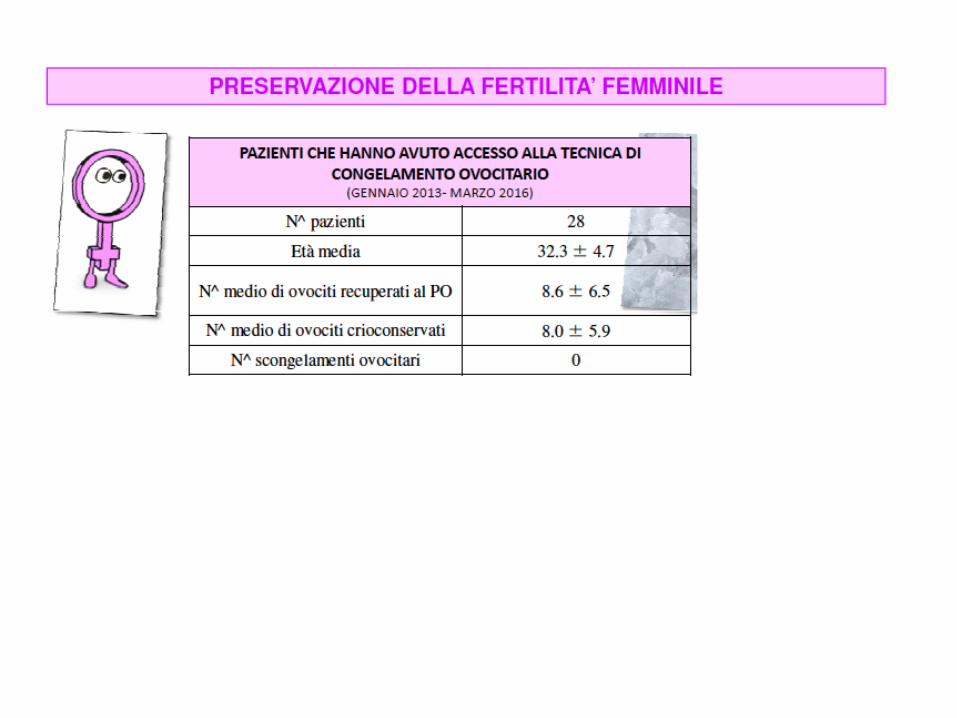
Progetto per la preservazione della fertilità femminile a Reggio Emilia

45%
37%
RODRIGUEZ-‐WALLBERG, 2014
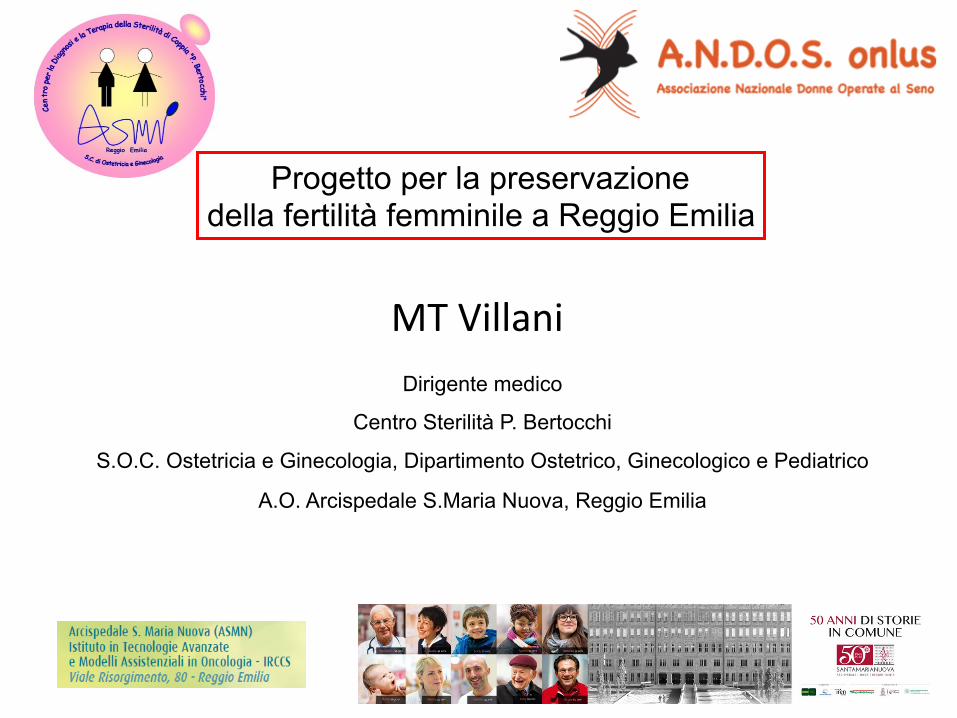
La sopravvivenza a 5 anni dalla diagnosi ha raggiunto
complessivamente il 78% per i tumori in eta' pediatrica e l'82% per i tumori dell'adolescente
Efficacia Possibile sterilita’
L’effeOo gonadotossico di alcuni traOamenP
chemio-‐radioterapici è oggi comprovato.
© 2014 Rodriguez-Wallberg and Oktay. This work is published by Dove Medical Press Limited, and licensed under Creative Commons Attribution – Non Commercial (unported, v3.0) License. The full terms of the License are available at http://creativecommons.org/licenses/by-nc/3.0/. Non-commercial uses of the work are permitted without any further
permission from Dove Medical Press Limited, provided the work is properly attributed. Permissions beyond the scope of the License are administered by Dove Medical Press Limited. Information on how to request permission may be found at: http://www.dovepress.com/permissions.php
Cancer Management and Research 2014:6 105–117
Cancer Management and Research Dovepress
submit your manuscript | www.dovepress.com
Dovepress 105
R E V I E W
open access to scientific and medical research
Open Access Full Text Article
http://dx.doi.org/10.2147/CMAR.S32380
Fertility preservation during cancer treatment: clinical guidelines
Kenny A Rodriguez-Wallberg1,2
Kutluk Oktay3,4
1Karolinska Institutet, Department of Clinical Science, Intervention and Technology, Division of Obstetrics and Gynecology, 2Reproductive Medicine, Karolinska University Hospital Huddinge, Stockholm, Sweden; 3Innovation Institute for Fertility Preservation, Rye and New York, 4Department of Obstetrics and Gynecology, New York Medical College, Valhalla, NY, USA
Correspondence: Kenny A Rodriguez-Wallberg Reproductive Medicine, Karolinska University Hospital Huddinge, Novumhuset Plan 4, SE-141 86 Stockholm, Sweden Email [email protected] Kutluk Oktay Innovation Institute for Fertility Preservation, 139 E 23rd St, New York, NY 10010, USA Email [email protected]
Abstract: The majority of children, adolescents, and young adults diagnosed with cancer today will become long-term survivors. The threat to fertility that cancer treatments pose to young patients cannot be prevented in many cases, and thus research into methods for fertility preservation is developing, aiming at offering cancer patients the ability to have biologically related children in the future. This paper discusses the current status of fertility preservation methods when infertil-ity risks are related to surgical oncologic treatments, radiation therapy, or chemotherapy. Several scientific groups and societies have developed consensus documents and guidelines for fertility preservation. Decisions about fertility and imminent potentially gonadotoxic therapies must be made rapidly. Timely and complete information on the impact of cancer treatment on fertility and fertility preservation options should be presented to all patients when a cancer treatment is planned.Keywords: fertility preservation, cancer, cryopreservation, ovarian tissue transplantation, fertility-sparing surgery, cancer survival, quality of life
IntroductionThe number of reported new cancer cases is increasing every year. In the Swedish Cancer Registry, the validity of which relies on the inclusion of approximately 98% of cases having morphologic verification, the average annual increase has been 2.1% for men and 1.5% for women during the last two decades.1 Only about half of this increase is explained by aging of the population and in many cases cancer patients are very young. Similar data have been observed in other European countries and in the US.2 The good news is that the probability of surviving cancer today is high and is continually improving. Rates of survival today are above 80% for various cancer types, in particular for very young patients, such as those presenting with cancer in childhood or early adulthood.3 Survivorship issues have therefore become highly relevant as well as quality of survival encompassing all health aspects.
The diagnosis of cancer at a young age, when individuals may have not yet started their families, poses unique challenges because treatments for cancer may induce ovar-ian or testicular failure by damaging ovarian follicles in females and spermatogonia in the testis in males. Gonadal failure may affect all aspects of reproductive health, including pubertal development, hormone production, and sexual function in adults. When cancer is treated by surgery, fertility may be impaired by removal or damage of the organs needed for reproduction.
The gonadotoxic effects of chemotherapy and radiation therapy are well recognized. These are dose-dependent and have been well characterized regarding the protocols used.3–12 Radiotherapy in females may also damage the uterus.13,14 Gonadotoxicity is
© 2014 Rodriguez-Wallberg and Oktay. This work is published by Dove Medical Press Limited, and licensed under Creative Commons Attribution – Non Commercial (unported, v3.0) License. The full terms of the License are available at http://creativecommons.org/licenses/by-nc/3.0/. Non-commercial uses of the work are permitted without any further
permission from Dove Medical Press Limited, provided the work is properly attributed. Permissions beyond the scope of the License are administered by Dove Medical Press Limited. Information on how to request permission may be found at: http://www.dovepress.com/permissions.php
Cancer Management and Research 2014:6 105–117
Cancer Management and Research Dovepress
submit your manuscript | www.dovepress.com
Dovepress 105
R E V I E W
open access to scientific and medical research
Open Access Full Text Article
http://dx.doi.org/10.2147/CMAR.S32380
Fertility preservation during cancer treatment: clinical guidelines
Kenny A Rodriguez-Wallberg1,2
Kutluk Oktay3,4
1Karolinska Institutet, Department of Clinical Science, Intervention and Technology, Division of Obstetrics and Gynecology, 2Reproductive Medicine, Karolinska University Hospital Huddinge, Stockholm, Sweden; 3Innovation Institute for Fertility Preservation, Rye and New York, 4Department of Obstetrics and Gynecology, New York Medical College, Valhalla, NY, USA
Correspondence: Kenny A Rodriguez-Wallberg Reproductive Medicine, Karolinska University Hospital Huddinge, Novumhuset Plan 4, SE-141 86 Stockholm, Sweden Email [email protected] Kutluk Oktay Innovation Institute for Fertility Preservation, 139 E 23rd St, New York, NY 10010, USA Email [email protected]
Abstract: The majority of children, adolescents, and young adults diagnosed with cancer today will become long-term survivors. The threat to fertility that cancer treatments pose to young patients cannot be prevented in many cases, and thus research into methods for fertility preservation is developing, aiming at offering cancer patients the ability to have biologically related children in the future. This paper discusses the current status of fertility preservation methods when infertil-ity risks are related to surgical oncologic treatments, radiation therapy, or chemotherapy. Several scientific groups and societies have developed consensus documents and guidelines for fertility preservation. Decisions about fertility and imminent potentially gonadotoxic therapies must be made rapidly. Timely and complete information on the impact of cancer treatment on fertility and fertility preservation options should be presented to all patients when a cancer treatment is planned.Keywords: fertility preservation, cancer, cryopreservation, ovarian tissue transplantation, fertility-sparing surgery, cancer survival, quality of life
IntroductionThe number of reported new cancer cases is increasing every year. In the Swedish Cancer Registry, the validity of which relies on the inclusion of approximately 98% of cases having morphologic verification, the average annual increase has been 2.1% for men and 1.5% for women during the last two decades.1 Only about half of this increase is explained by aging of the population and in many cases cancer patients are very young. Similar data have been observed in other European countries and in the US.2 The good news is that the probability of surviving cancer today is high and is continually improving. Rates of survival today are above 80% for various cancer types, in particular for very young patients, such as those presenting with cancer in childhood or early adulthood.3 Survivorship issues have therefore become highly relevant as well as quality of survival encompassing all health aspects.
The diagnosis of cancer at a young age, when individuals may have not yet started their families, poses unique challenges because treatments for cancer may induce ovar-ian or testicular failure by damaging ovarian follicles in females and spermatogonia in the testis in males. Gonadal failure may affect all aspects of reproductive health, including pubertal development, hormone production, and sexual function in adults. When cancer is treated by surgery, fertility may be impaired by removal or damage of the organs needed for reproduction.
The gonadotoxic effects of chemotherapy and radiation therapy are well recognized. These are dose-dependent and have been well characterized regarding the protocols used.3–12 Radiotherapy in females may also damage the uterus.13,14 Gonadotoxicity is
ü Nonostante l’evidenza che la perdita della fertilità nei pazienti sopravvissuti a un cancro sia correlata a distress psicologico e peggiori la qualità di vita, molti pazienti oncologici in età riproduttiva non ricevono adeguate informazioni o
non vengono inviati a specialisti per la preservazione della fertilità
ü Questo contrasta con i dati che indicano che circa 3 pazienti oncologici su 4 con età inferiore a 35 anni e senza figli, al momento della terapia per il cancro
sarebbero interessati ad avere un figlio nella loro vita.

La richiesta di preservazione della ferPlità da parte dei pazienP è in
aumento (5% nel 2006 vs 15% nel 2012).
RUDDY, 2014; LAMBERTINI, 2016
TuOavia, esiste una discrepanza nella preservazione della ferPlità
in base al sesso.
L’età media della prima gravidanza nei paesi industrializzati è in costante aumento,
tra il 2006 e il 2010 la percentuale di donne >40 anni che ha avuto la prima gravidanza era circa il 20%
L’incidenza dei tumori prima di aver completato la
propria vita riproduttiva tende ad aumentare
Il Cancer Statistics ha riportato che circa il 10% dei casi di tumori femminili interessano donne <40 anni
Le evidenze scientifiche dimostrano che
una gravidanza dopo una neoplasia non peggiora la prognosi
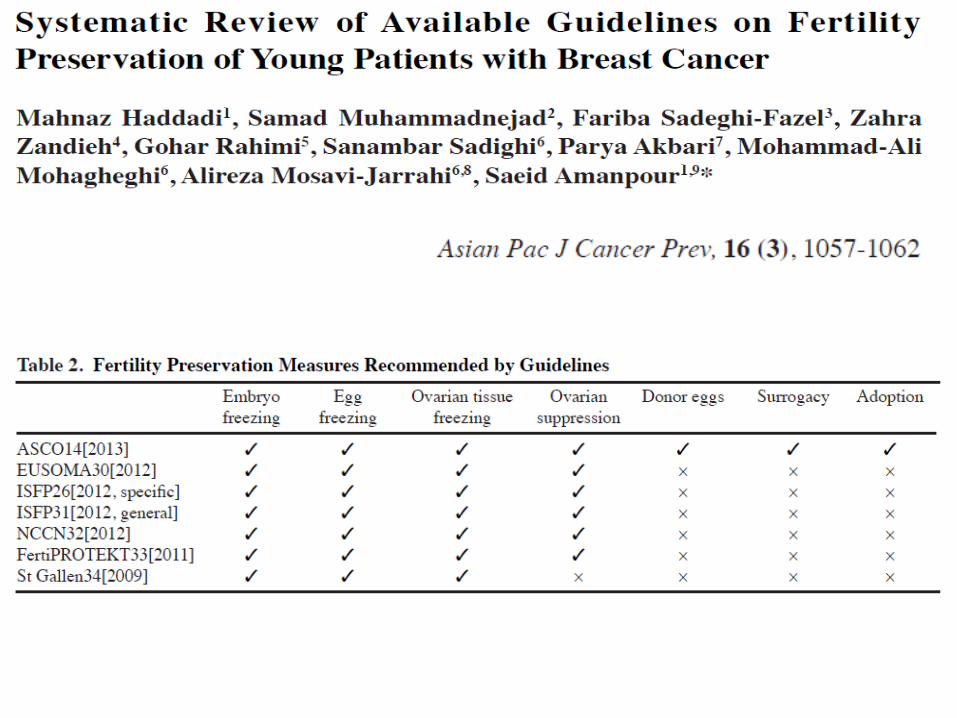
Come indicato da linee guida nazionali ed internazionali, la futura
genitorialità deve essere parte integrante del percorso diagnosPco-‐
terapeuPco del paziente oncologico in età ferPle.
LAMBERTINI, 2016; FRYDMAN, 2016 American Society for ReproducPve Medicine, 2013
American Society of Clinical Oncology, 2013
Associazione Italiana di Oncologia Medica, 2013
European Society for Medical Oncology, 2013
ONCOFERTILITA’/PRESERVAZIONE DELLA FERTILITA’

1936 1938 1945 1949 1953 1962 1983 1985 1986 1987 1990 1992 1996 1776 1999
2003 2013
PRIME OSSERVAZIONI
SUL CONGELAMENTO
CELLULARE (SPALLANZANI)
SOPRAVVIVENZA DI SPERMATOZOI
ANIMALI CONGELATI IN ELIO A -296,5°C
(JAHNEL)
SOPRAVVIVENZA DEGLI
SPERMATOZOI MANTENUTI A
BASSE TEMPERATURE
(-160°C)
GLICEROLO COME
CRIOPROTETTORE PER GLI
SPERMATOZOI (POLGE)
GRAVIDANZA DA
SPERMATOZOI CONGELATI
(BUNGE & SHERMAN)
PRIMA BANCA DEL SEME
GRAVIDANZA DA
EMBRIONI CONGELATI
(TROUNSON)
PROH COME CRIOPROTETTORE
EMBRIONARIO (LASSALLE)
PARTO DA
OVOCITI CONGELATI
(CHEN)
PARZIALE VALIDAZIONE
DELLA VITRIFICAZIONE
OVOCITARIA (ASRM)
CONGELAMENTO ULTRARAPIDO EMBRIONARIO (TROUNSON)
PARTO DA
EMBRIONI VITRIFICATI (GOROTS)
GRAVIDANZA DA
SPERMATOZOI TESTICOLARI CONGELATI (GIL-SALOM)
ICSI (PALERMO)
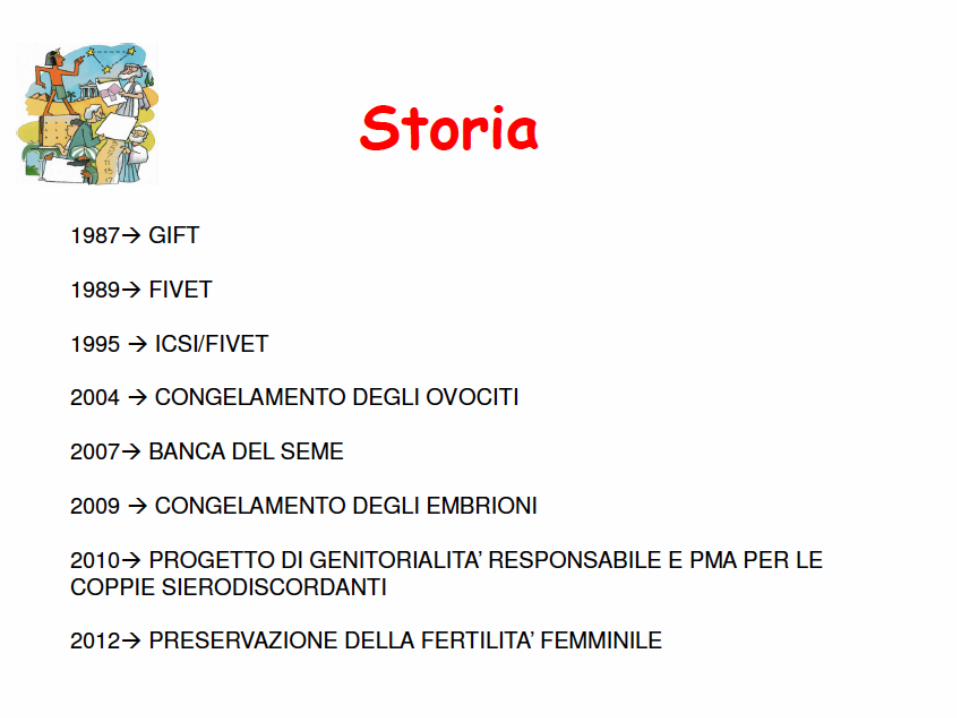
La chiave di svolta nella diffusione della preservazione della ferPlità è stato
il progressivo miglioramento delle procedure di crioconservazione.
PARTI DA
OVOCITI VITRIFICATI
(KULESHOVA, YOON)



Studio multicentrico osservazionale.
Centro Coordinatore: Azienda Ospedaliera Universitaria San Martino di Genova – IRCCS – Istituto Nazionale per la Ricerca sul Cancro
Ente proponente: Assessorato alla Salute - Regione Liguria
Studio osservazionale di coorte prospettico sulla preservazione della fertilità nelle pazienti
giovani con patologia oncologica. PREFER (PREgnancy and FERtility).
Durata dello studio: 24 mesi (2012-2014)
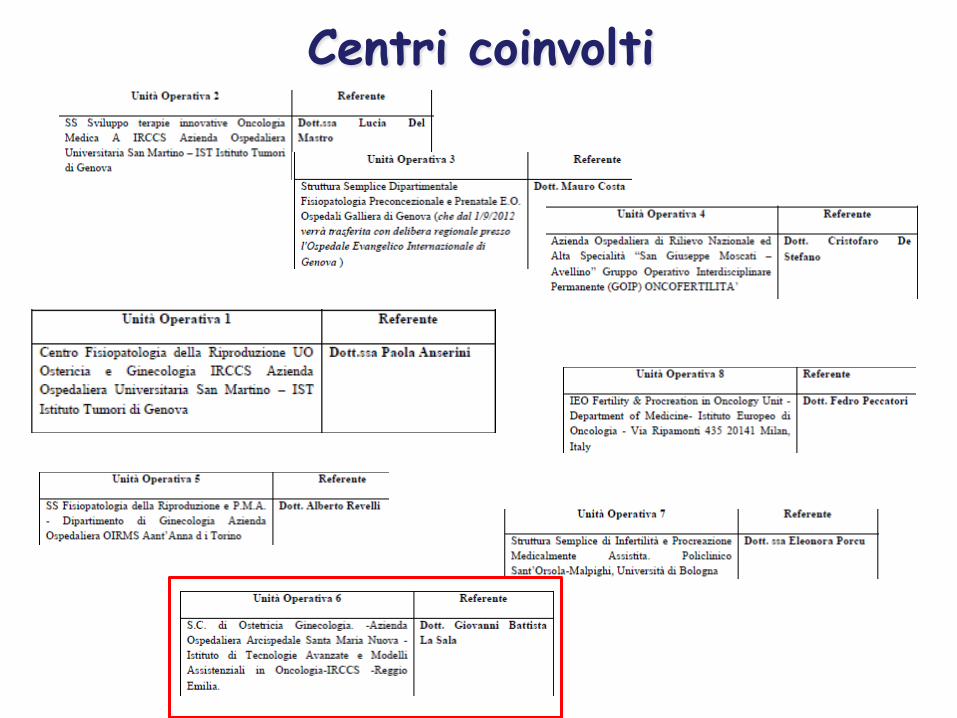
Centri coinvolti
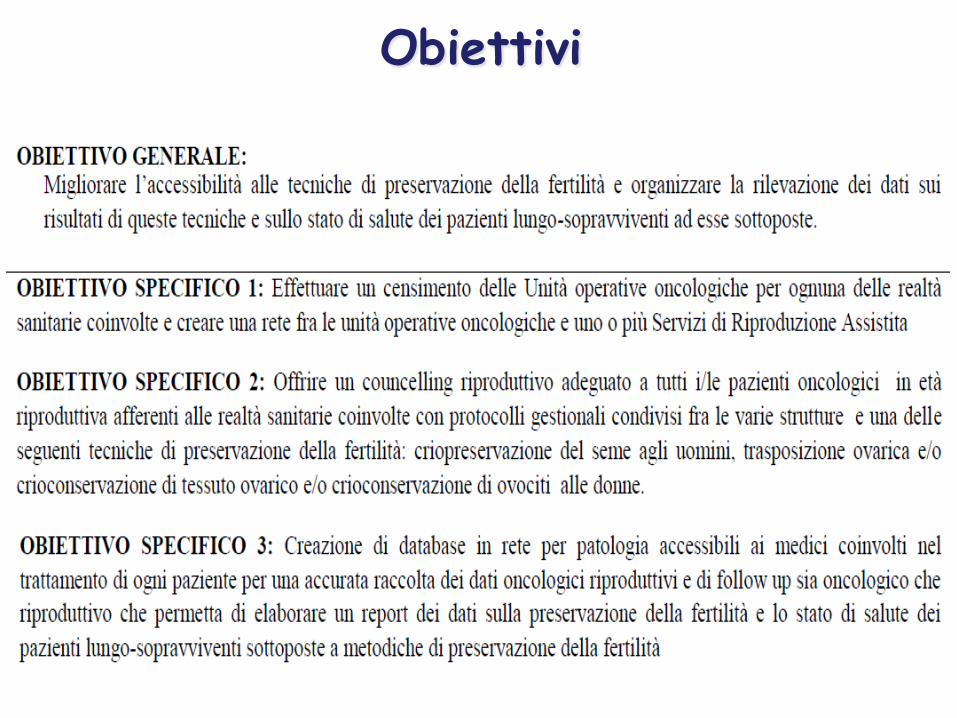
Obiettivi
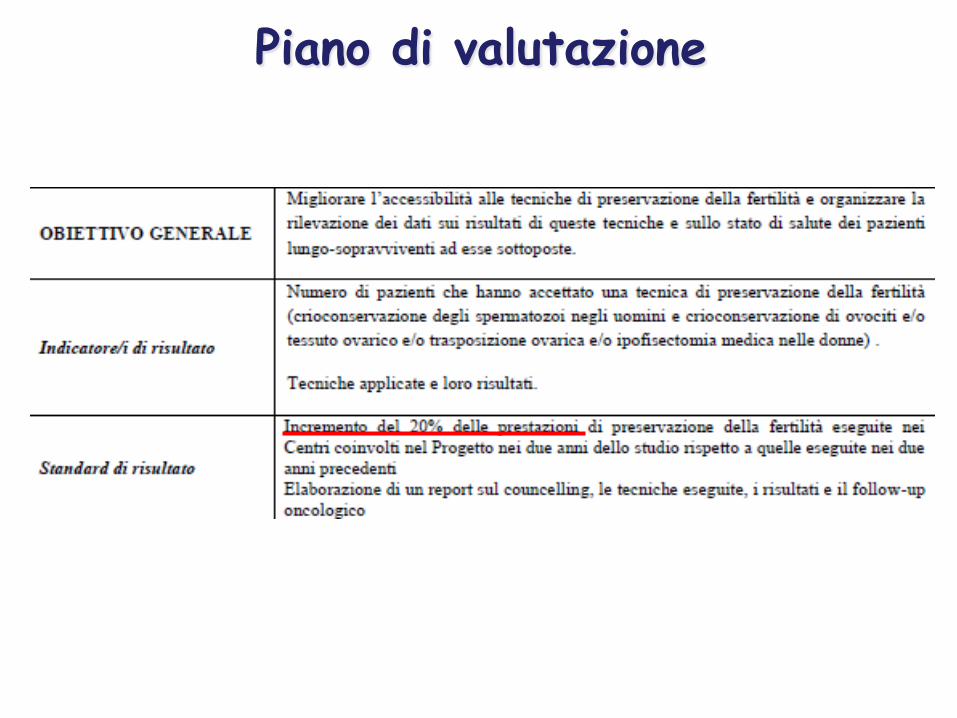
Piano di valutazione

Piano di valutazione

Intervento proposto
Intervento proposto: Counselling riproduttivo con proposta di
protocolli gestionali di preservazione della fertilità.
Fruibilità della ricerca
Conoscenza circa le preferenze e le scelte delle giovani pazienti oncologiche.
Aumentare la consapevolezza degli addetti ai lavori circa
l’importanza del (corretto) counselling.
Indirizzare verso la strategia con il miglio rapporto rischio/beneficio.
Traslabilità della ricerca Realizzazione di un sistema clinico strutturato di tipologia “Hub and
Spoke”, allocando le attività in diverse tipologie di strutture del Sistema Sanitario Italiano (Aziende Ospedaliere, IRCCS pubblici e Privati, Istituti Oncologici, Università) dove in questi anni siano già state
compiute sperimentazioni di pratiche e procedure per la conservazione della fertilità.
Le strutture del progetto (HUBS) devono stabilire rapporti funzionali con altra tipologia di strutture (SPOKES), quali, ad esempio, Aziende
sanitarie territoriali o Unità operative oncologiche, chirurgiche, urologiche e pediatriche impossibilitate a realizzare progetti autonomi.
Sarà inoltre compito dell’attività progettuale stabilire un sistema, sotto forma di rete tra le HUBS per la condivisione di protocolli, linee guida, dati, la creazione di un unico database da collegare ai Registri tumori
locali e nazionali per migliorare la rilevazione dei dati dello stato di salute dei pazienti lungo-sopravviventi.

Monitoraggio a cura del Centro Promotore.
I dati raccolti presso il Centro Clinical Trials dell’IRCCS AOU San Martino - IST
Monitoraggio dello studio
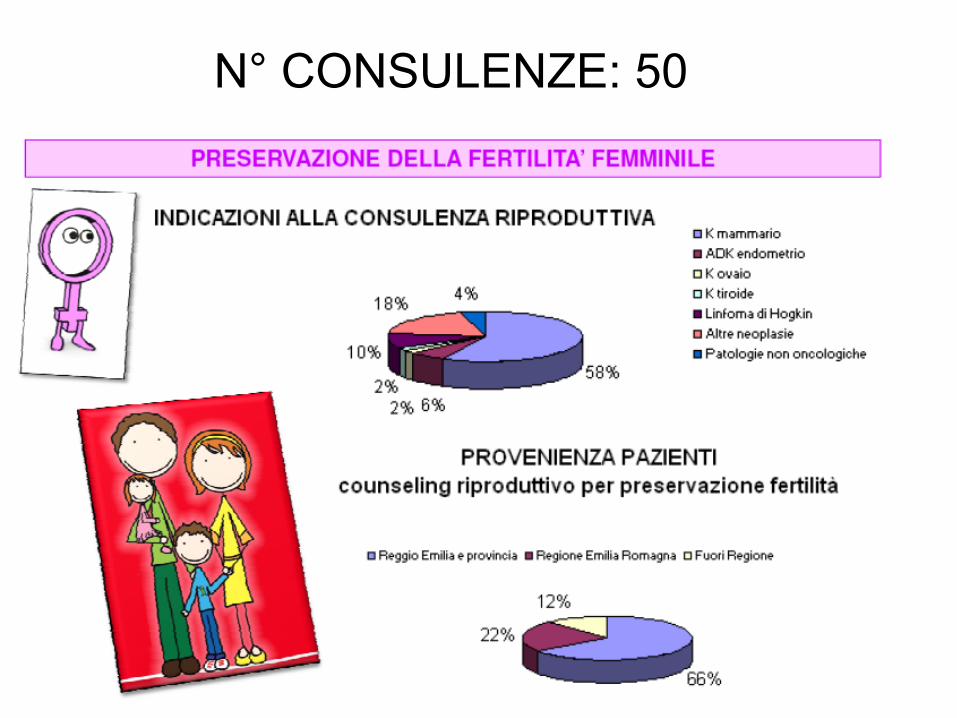
N° CONSULENZE: 50