Embed Size (px)
Citation preview
Multi-Dimensional Multi-Dimensional Congregational Health: Congregational Health:
The New VisionThe New Vision
Dr. James EarlyDr. James Early
University of Kansas School of University of Kansas School of Medicine-WichitaMedicine-Wichita
How reasonable is it to discuss How reasonable is it to discuss “health” in the congregational setting?“health” in the congregational setting?
Companies are getting involved as Companies are getting involved as payers and as agents of change: fitness payers and as agents of change: fitness centers, company doctors, incentives for centers, company doctors, incentives for good health habits, health fairs.good health habits, health fairs.
Schools are involved through nurses, Schools are involved through nurses, education, immunization campaigns.education, immunization campaigns.
The retail sector is becoming involved in The retail sector is becoming involved in healthcare delivery.healthcare delivery.
Source: The Wall Street Journal: Wednesday, October 5, 2005 Personal Journal Section, pg. D1
How reasonable is it to discuss How reasonable is it to discuss “health” in the congregational setting?“health” in the congregational setting?
An increasing number of people are uninsured An increasing number of people are uninsured or underinsured and not appropriately or underinsured and not appropriately accessing our healthcare system.accessing our healthcare system.
Church affiliated indigent clinics are trying to Church affiliated indigent clinics are trying to “pick up the slack”.“pick up the slack”.
The traditional healthcare system was never The traditional healthcare system was never designed to take on prevention.designed to take on prevention.
Decisions on life and death are even Decisions on life and death are even uncomfortably becoming an issue for uncomfortably becoming an issue for legislation.legislation.
Church Initiatives
How can the church become How can the church become involved in health and wellness?involved in health and wellness?
By providing a more comprehensive By providing a more comprehensive understanding of the connection understanding of the connection between physical/emotional health and between physical/emotional health and our social and spiritual lives?our social and spiritual lives?
By creating a common vision and plan By creating a common vision and plan that congregants may choose to utilize?that congregants may choose to utilize?
And then by fostering And then by fostering long-term long-term knowledge acquisition and skill knowledge acquisition and skill building?building?

Physical Health Mental/Emotional Health
Spiritual Health Social Health
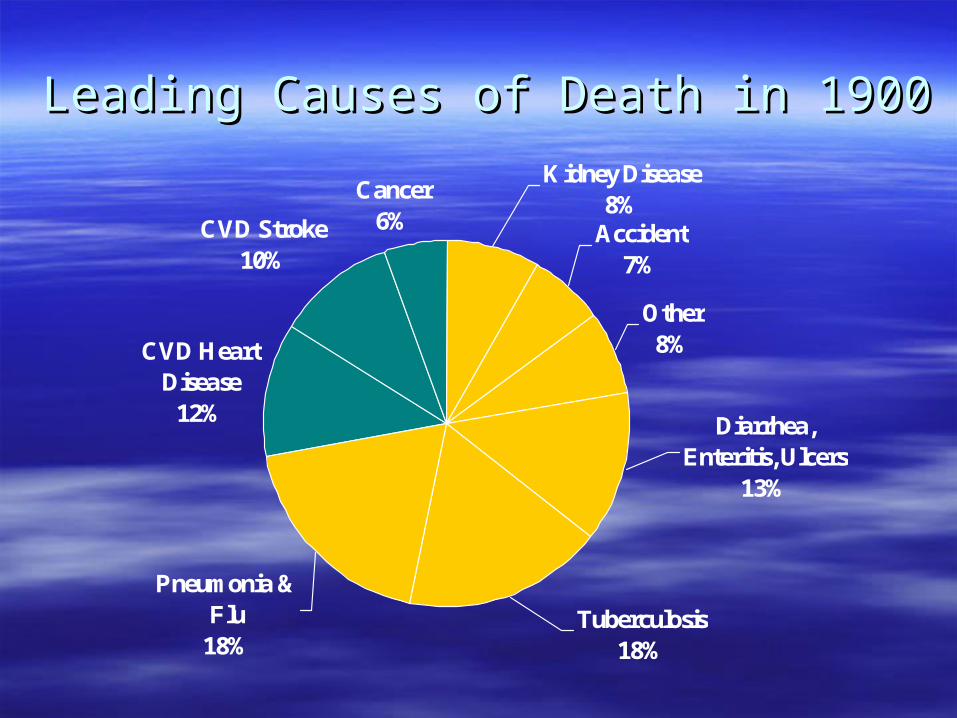
CVD Heart Disease
12%
CVD Stroke10%
Cancer6%
Pneumonia & Flu
18%Tuberculosis
18%
Diarrhea, Enteritis, Ulcers
13%
Other8%
Kidney Disease8%
Accident7%
Leading Causes of Death in 1900Leading Causes of Death in 1900
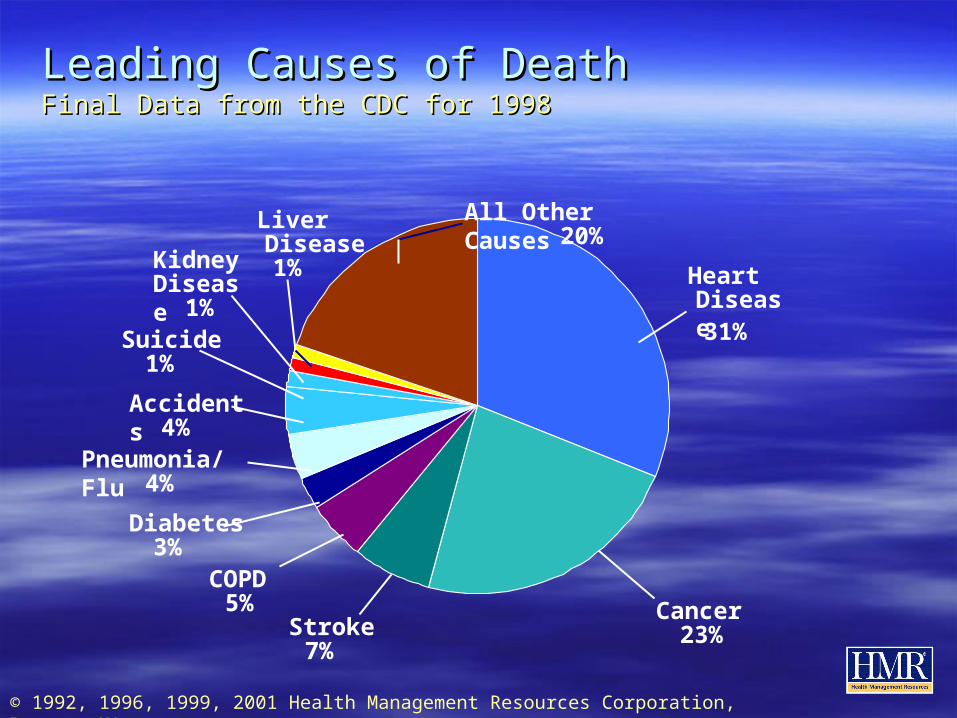
Leading Causes of DeathLeading Causes of DeathFinal Data from the CDC for 1998Final Data from the CDC for 1998
© 1992, 1996, 1999, 2001 Health Management Resources Corporation, Boston, MA
HeartDisease31%
Cancer23%Stroke
7%
COPD5%
Diabetes3%
Pneumonia/Flu4%
Accidents4%
Suicide1%
KidneyDisease
1%
LiverDisease1%
All Other Causes20%
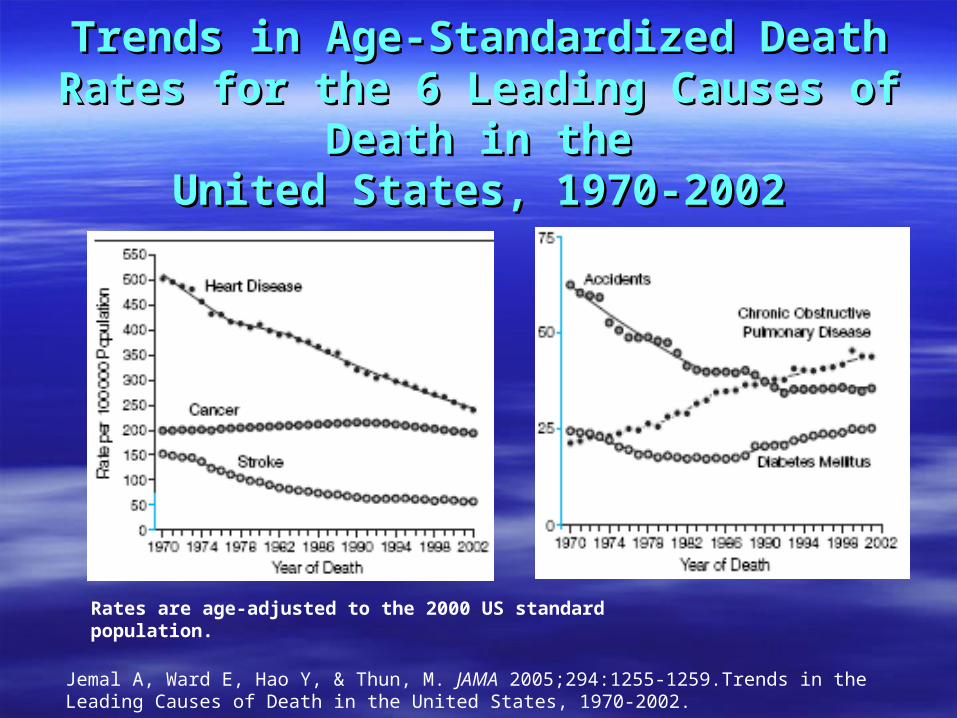
Trends in Age-Standardized Death Rates for Trends in Age-Standardized Death Rates for the 6 Leading Causes of Death in thethe 6 Leading Causes of Death in the
United States, 1970-2002United States, 1970-2002
Rates are age-adjusted to the 2000 US standard population.
Jemal A, Ward E, Hao Y, & Thun, M. JAMA 2005;294:1255-1259.Trends in the Leading Causes of Death in the United States, 1970-2002.
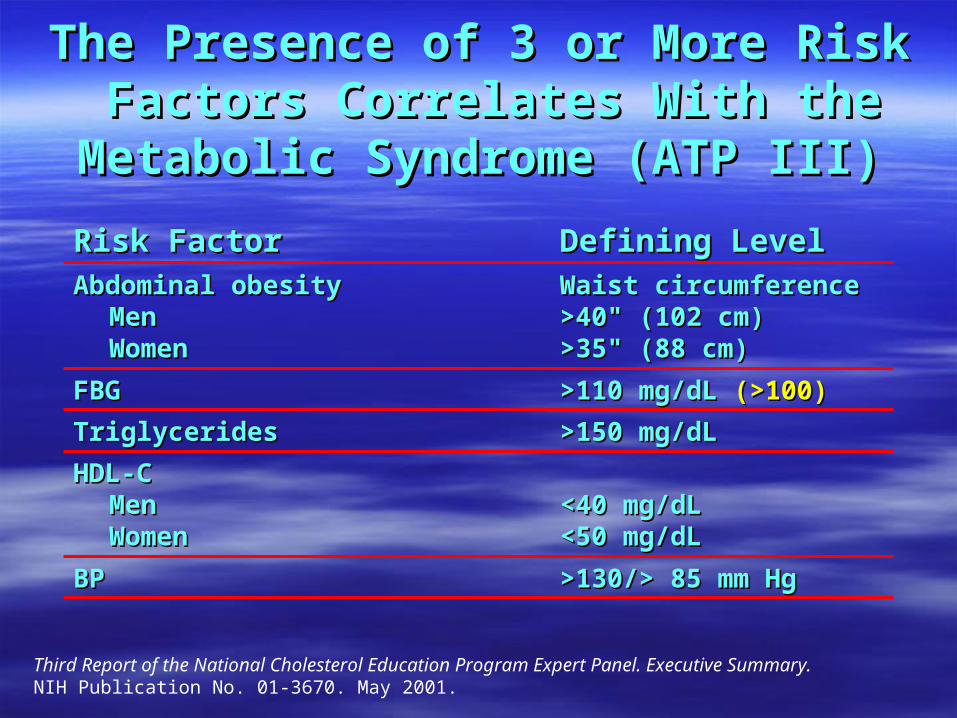
The Presence of 3 or More Risk The Presence of 3 or More Risk Factors Correlates With the Factors Correlates With the Metabolic Syndrome (ATP III)Metabolic Syndrome (ATP III)
>130/> 85 mm Hg>130/> 85 mm HgBPBP
<40 mg/dL<40 mg/dL<50 mg/dL<50 mg/dL
HDL-CHDL-CMenMenWomenWomen
>150 mg/dL>150 mg/dLTriglyceridesTriglycerides
>110 mg/dL>110 mg/dL (>100)(>100)FBGFBG
Waist circumferenceWaist circumference>40>40"" (102 cm) (102 cm)>35>35"" (88 cm) (88 cm)
Abdominal obesityAbdominal obesityMenMenWomenWomen
Defining LevelDefining LevelRisk FactorRisk Factor
Third Report of the National Cholesterol Education Program Expert Panel. Executive Summary. NIH Publication No. 01-3670. May 2001.
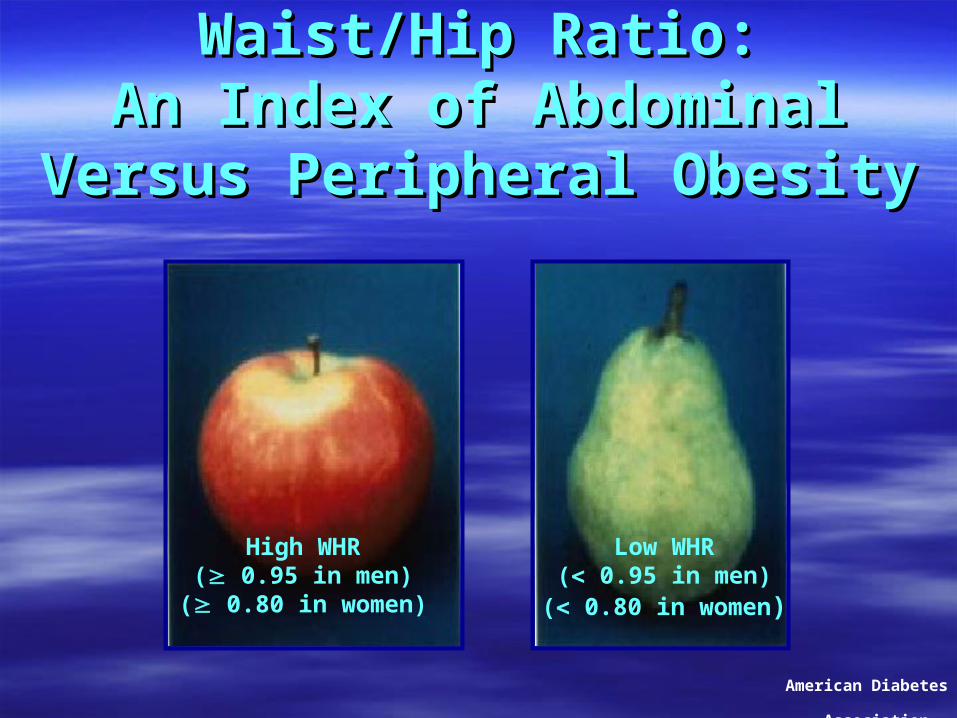
Waist/Hip Ratio:Waist/Hip Ratio:An Index of Abdominal Versus An Index of Abdominal Versus
Peripheral ObesityPeripheral Obesity
High WHR( 0.95 in men)
( 0.80 in women)
Low WHR( 0.95 in men)
( 0.80 in women)
American Diabetes Association
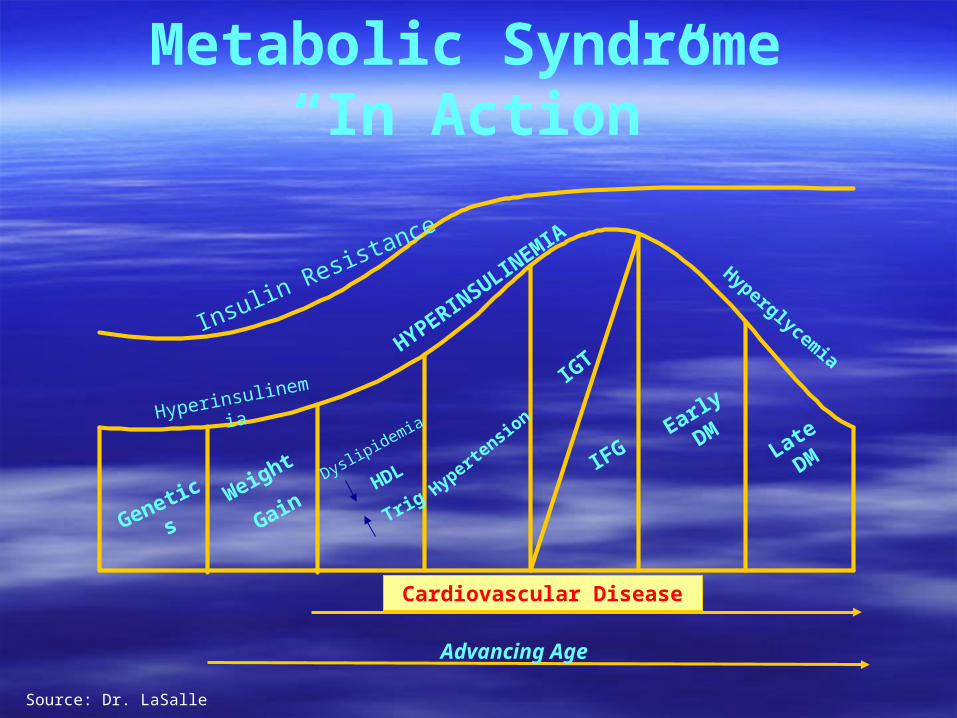
Metabolic Syndrome “In Action”
Genetics Weight
Gain
Dyslipidemia
HDL
TrigHyperte
nsion
IGT
IFGEarly
DMLate
DM
Hyperinsulinemia
HYPERINSULIN
EMIA
Hyperglycemia
Insulin Resistance
Advancing Age
Cardiovascular Disease
Source: Dr. LaSalle
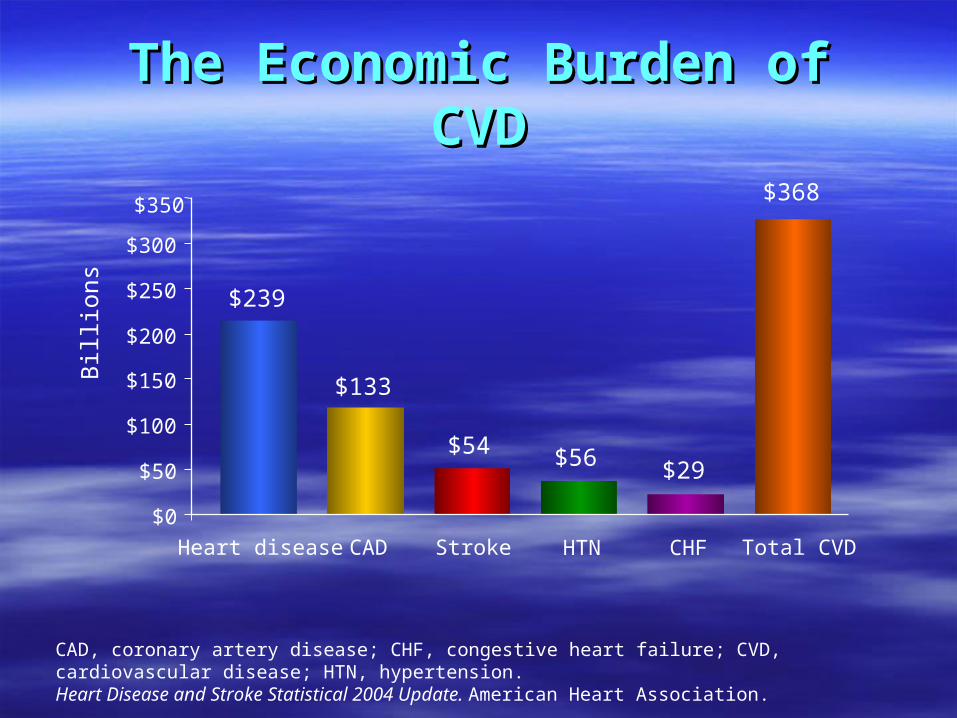
The Economic Burden of CVDThe Economic Burden of CVD
CAD, coronary artery disease; CHF, congestive heart failure; CVD, cardiovascular disease; HTN, hypertension. Heart Disease and Stroke Statistical 2004 Update. American Heart Association.
Heart disease CAD Stroke HTN CHF Total CVD
$0
$50
$100
$150
$200
$250
$300
$350
Bill
ions
$368
$239
$133
$54 $56 $29

Prevalence of Diagnosed Diabetes Among US
Adults,1991-2001
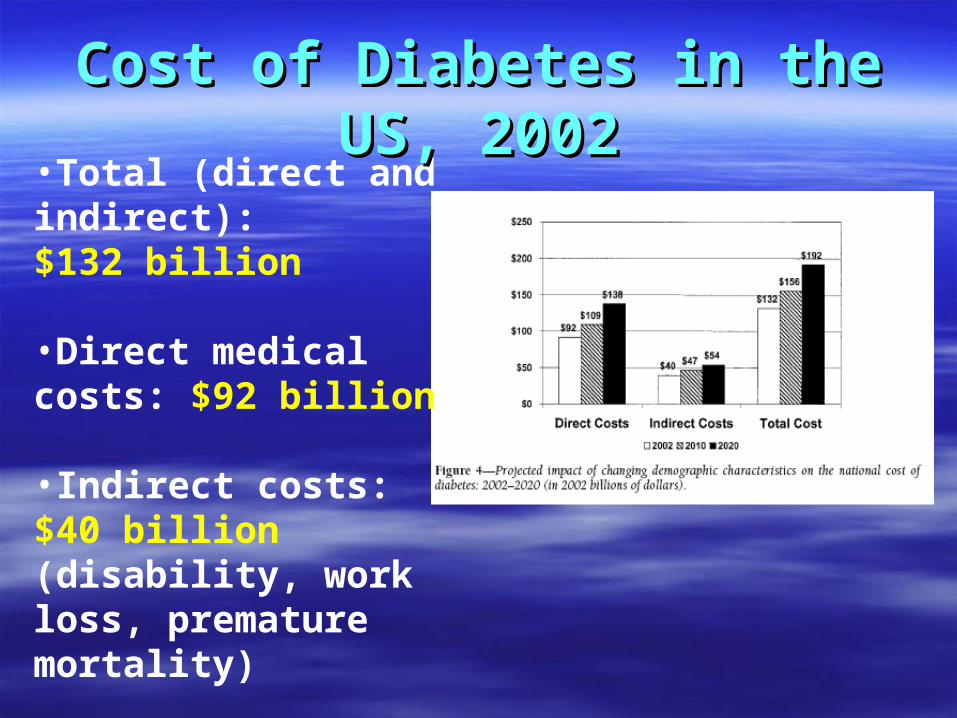
•Total (direct and indirect): $132 billion •Direct medical costs: $92 billion •Indirect costs: $40 billion (disability, work loss, premature mortality)
Cost of Diabetes in the US, 2002Cost of Diabetes in the US, 2002
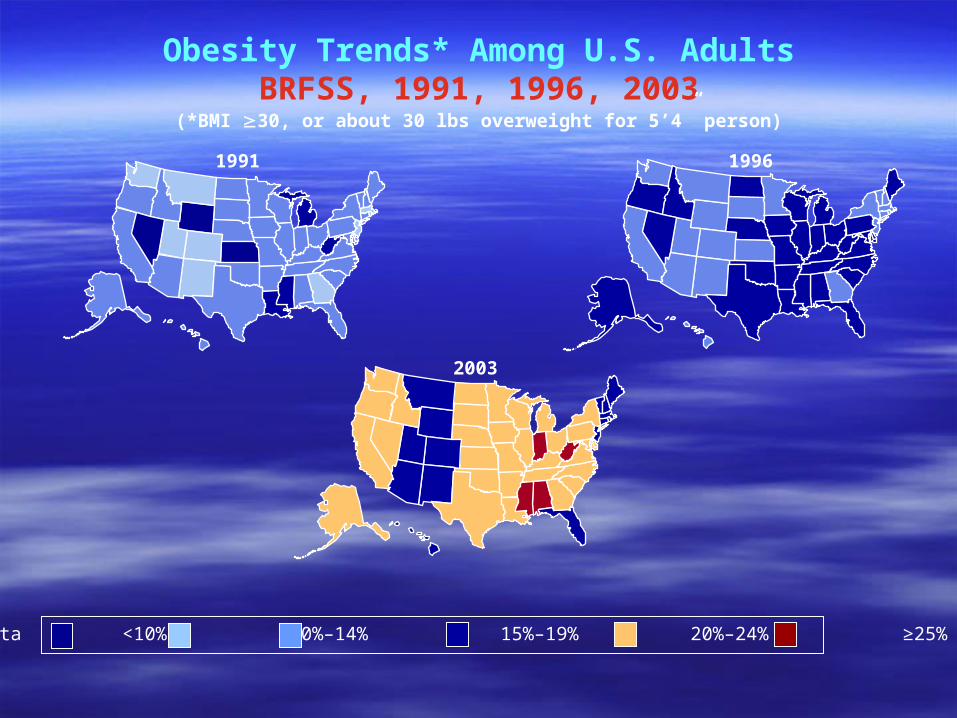
19961991
2003
Obesity Trends* Among U.S. AdultsBRFSS, 1991, 1996, 2003
(*BMI 30, or about 30 lbs overweight for 5’4” person)
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
Economic Cost of ObesityEconomic Cost of Obesity
Economic causes and costs of obesity study Economic causes and costs of obesity study presented at 14presented at 14thth European Congress on European Congress on ObesityObesity
$96.7 billion was spent on obesity in 2003 in $96.7 billion was spent on obesity in 2003 in the U.S.the U.S.
Figures are comparable in western countries Figures are comparable in western countries with rising rates of obesitywith rising rates of obesity
Wolf, AM. Health Economics of Obesity- New Insights presented at the 14th European Congress on Obesity
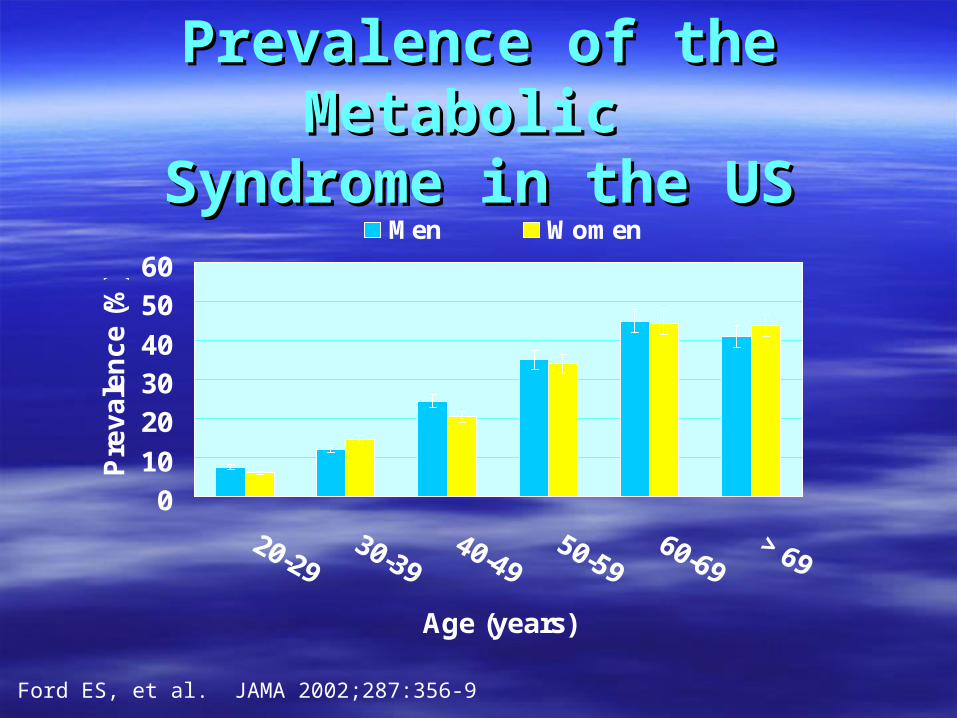
Prevalence of the Metabolic Prevalence of the Metabolic Syndrome in the USSyndrome in the US
010
203040
5060
Age (years)
Pre
va
len
ce
(%
)
Men Women
Ford ES, et al. JAMA 2002;287:356-9

?
Gen
etic
s
Enviro
nmen
t
Dyslipidemia
HDL-C
TG
Hyp
erte
nsio
n
IGT
IFG Ear
ly D
M
Obe
sity
Late
DM
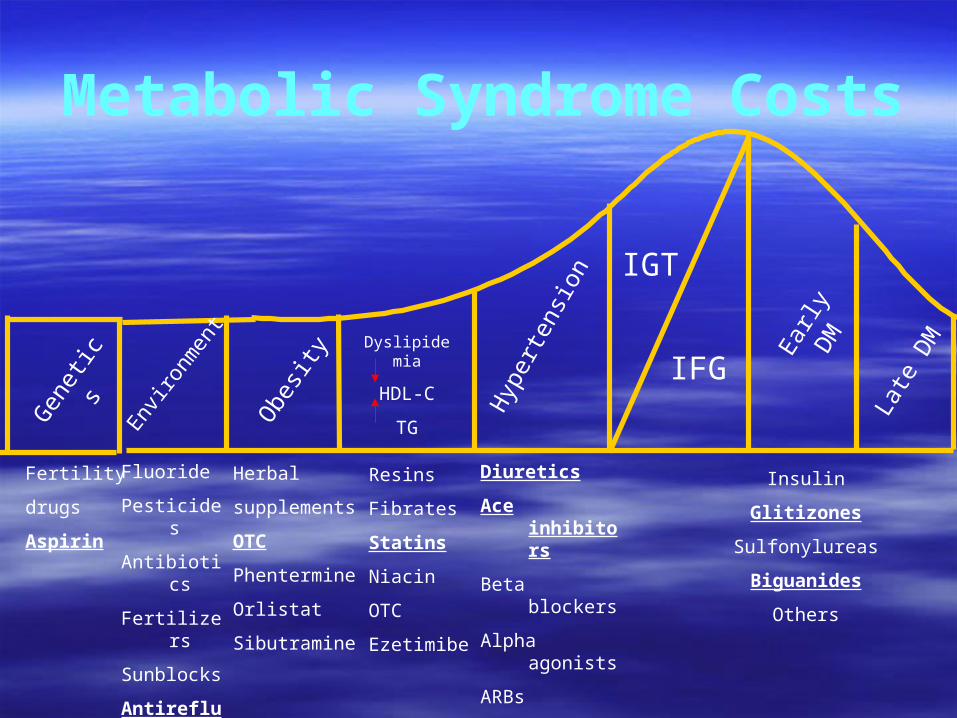
Fertility
drugs
Aspirin
Herbal
supplements
OTC
Phentermine
Orlistat
Sibutramine
Resins
Fibrates
Statins
Niacin
OTC
Ezetimibe
Diuretics
Ace inhibitors
Beta blockers
Alpha agonists
ARBs
Other
Insulin
Glitizones
Sulfonylureas
Biguanides
Others
Fluoride
Pesticides
Antibiotics
Fertilizers
Sunblocks
Antireflux
Metabolic Syndrome Costs
Gen
etic
s
Enviro
nmen
t Dyslipidemia
HDL
Trig
Hyp
erte
nsio
n
IGT
IFG Ear
ly D
M
Obe
sity
Late
DM
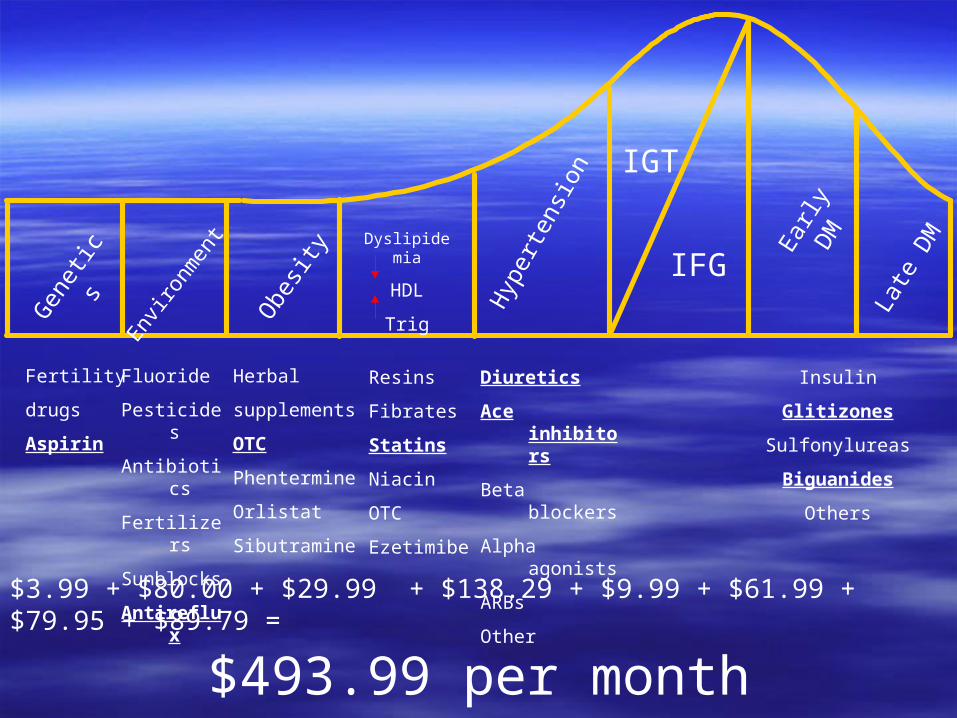
$3.99 + $80.00 + $29.99 + $138.29 + $9.99 + $61.99 + $79.95 + $89.79 =
$493.99 per month
Fertility
drugs
Aspirin
Fluoride
Pesticides
Antibiotics
Fertilizers
Sunblocks
Antireflux
Herbal
supplements
OTC
Phentermine
Orlistat
Sibutramine
Resins
Fibrates
Statins
Niacin
OTC
Ezetimibe
Diuretics
Ace inhibitors
Beta blockers
Alpha agonists
ARBs
Other
Insulin
Glitizones
Sulfonylureas
Biguanides
Others
Total Yearly Cost for Total Yearly Cost for Our Sample PatientOur Sample Patient
$5,927.88$5,927.88
““The average yearly pharmacy The average yearly pharmacy cost of treating adult patients cost of treating adult patients
over age 20 with metabolic over age 20 with metabolic syndrome exceeds $4,000, syndrome exceeds $4,000,
which is more than 4 times the which is more than 4 times the average annual drug cost for average annual drug cost for
all other patients.”all other patients.”
Medical Research News. May 9, 2005
Two Million Methodists with Two Million Methodists with Metabolic SyndromeMetabolic Syndrome
If 2 million Methodists cut their metabolic If 2 million Methodists cut their metabolic syndrome medications in half…..syndrome medications in half…..
There would be There would be 4 billion dollars4 billion dollars more for more for individuals and congregations to spend individuals and congregations to spend on the church and families.on the church and families.
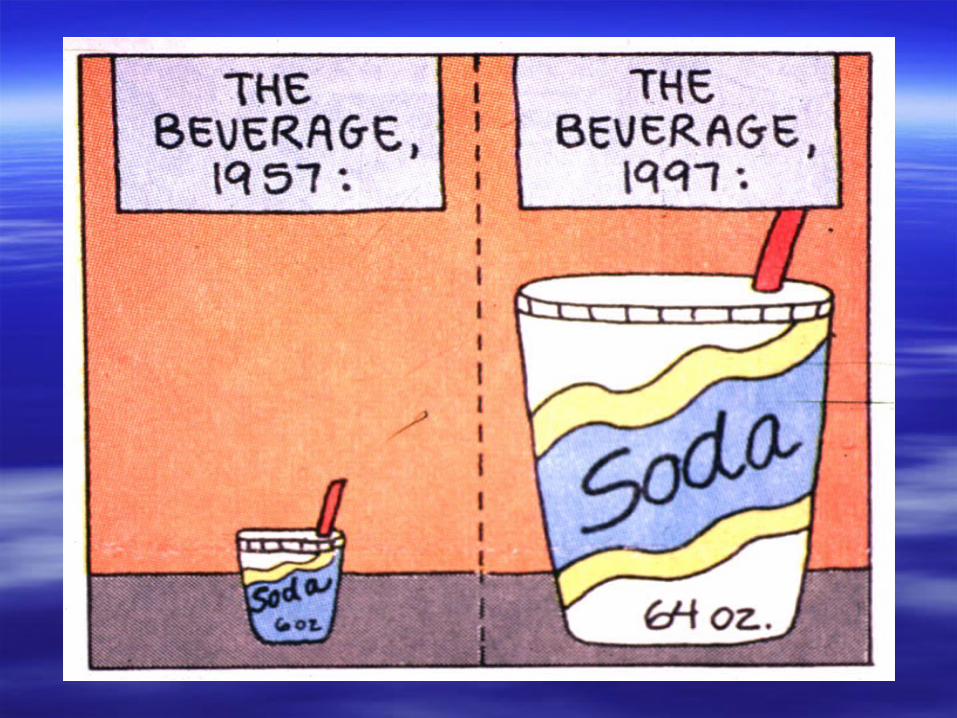
We are beginning to We are beginning to understand the problem….understand the problem….
How did we get here?How did we get here?

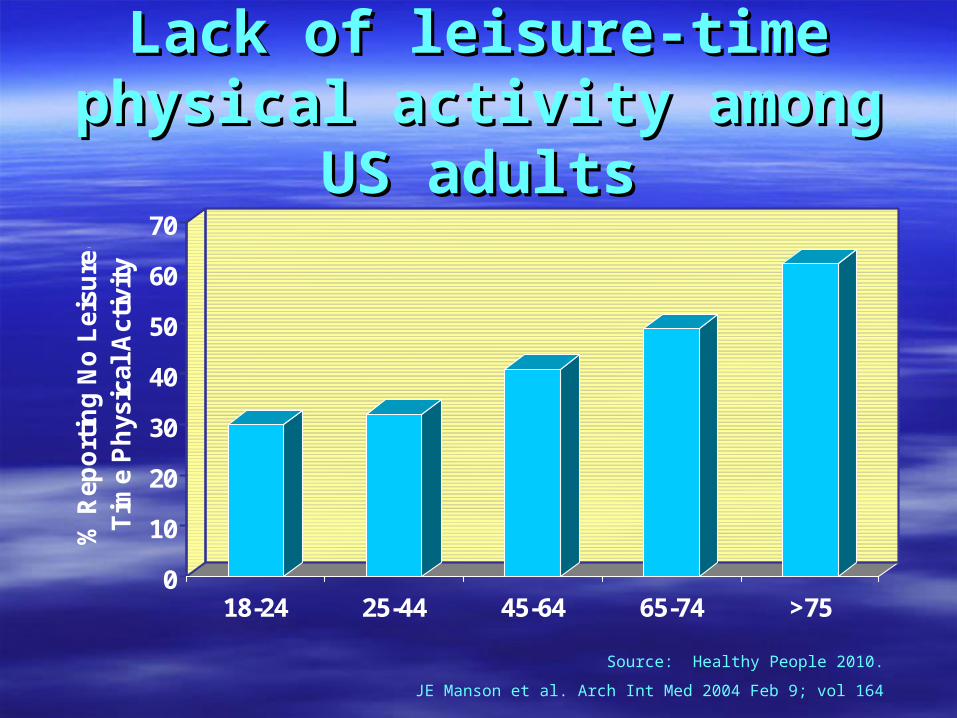
Lack of leisure-time physical Lack of leisure-time physical activity among US adultsactivity among US adults
0
10
20
30
40
50
60
70
% R
epo
rtin
g N
o L
eisu
re-
Tim
e P
hys
ical
Act
ivit
y
18-24 25-44 45-64 65-74 >75
Source: Healthy People 2010.
JE Manson et al. Arch Int Med 2004 Feb 9; vol 164
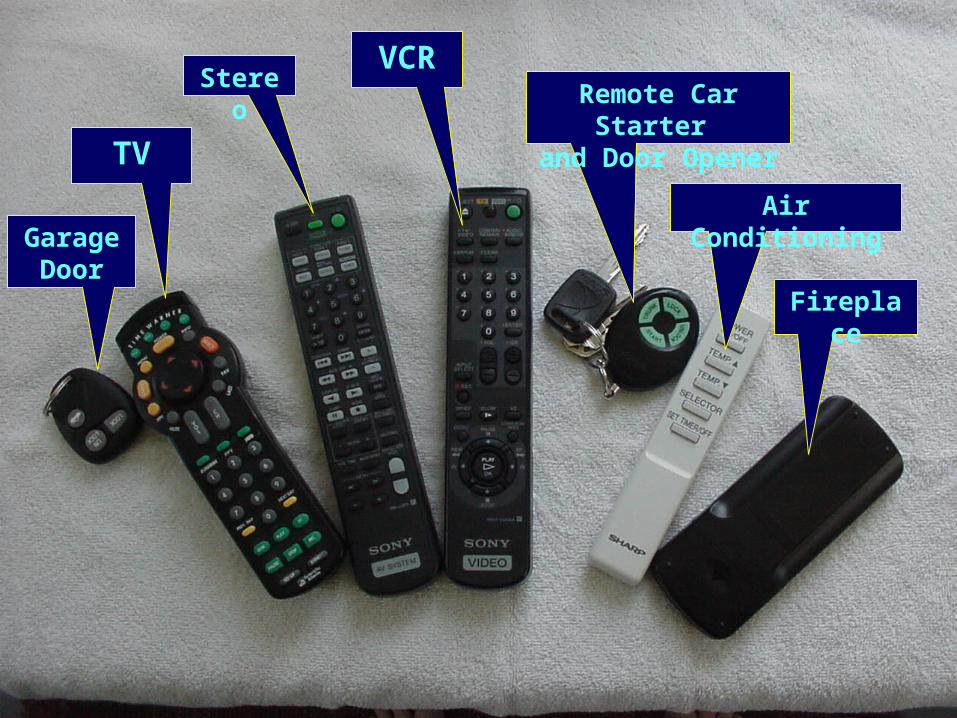
Stereo
TV
Air ConditioningGarage
Door
Remote Car Starter and Door Opener
VCR
Fireplace
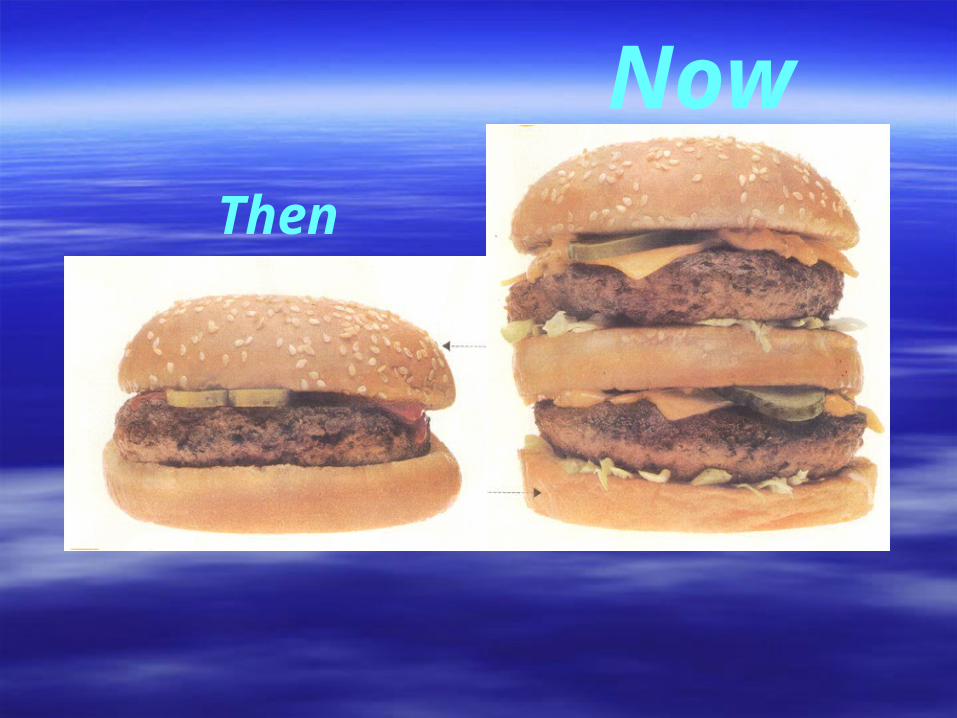
Then
Now
“Genetics loads the gun; the environment pulls the trigger.” George Bray
Physical Health Mental/Emotional Health
Spiritual Health Social Health
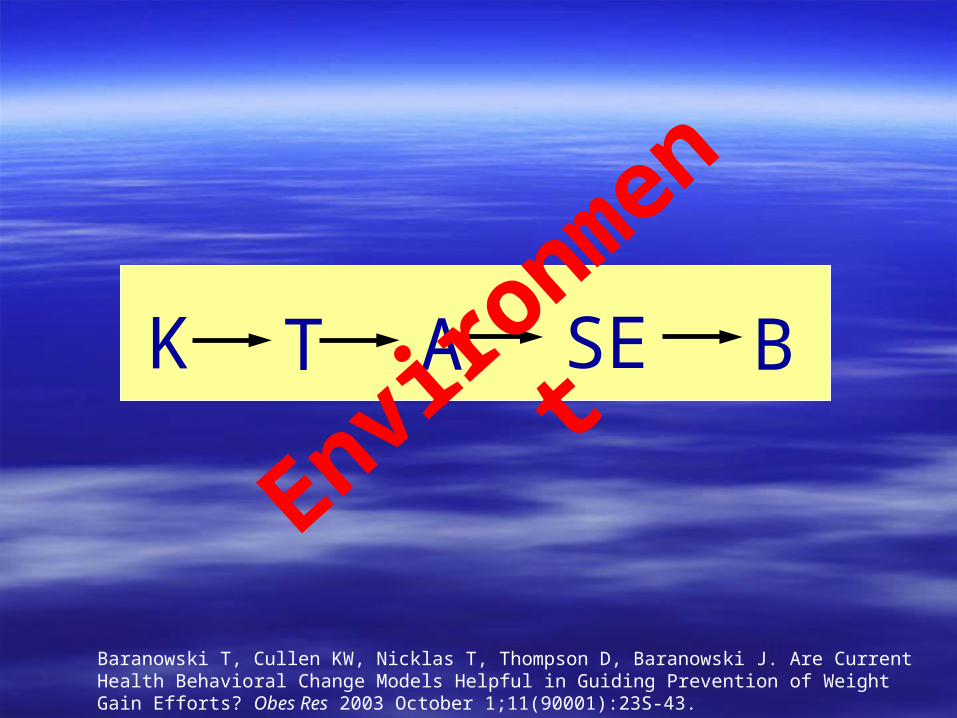
K T A SE B
Enviro
nmen
t
Baranowski T, Cullen KW, Nicklas T, Thompson D, Baranowski J. Are Current Health Behavioral Change Models Helpful in Guiding Prevention of Weight Gain Efforts? Obes Res 2003 October 1;11(90001):23S-43.
Impact of Emotions on Impact of Emotions on Physical HealthPhysical Health
DepressionDepression AnxietyAnxiety AddictionAddiction Stress/Time ManagementStress/Time Management
– FamilyFamily– WorksiteWorksite– CommunityCommunity

Physical Health Mental/Emotional Health
Spiritual Health Social Health
Impact of Social Health on Impact of Social Health on Physical/Emotional well beingPhysical/Emotional well being
ConnectionsConnections– Physical environmentPhysical environment
Built environmentBuilt environment Your “space”Your “space”
– Interpersonal environmentInterpersonal environment SupportSupport RelationshipsRelationships ResponsibilitiesResponsibilities

Physical Health Mental/Emotional Health
Spiritual Health Social Health
But physical/emotional/social health But physical/emotional/social health may still not be enoughmay still not be enough
Physiological Needs
Safety Needs
Belonging Needs
Esteem Needs
Self-Actualization
Spiritual fulfillment can provide the Spiritual fulfillment can provide the context and meaning to lifecontext and meaning to life
Our spiritual health is reflected in Our spiritual health is reflected in our desire to extend the quality and our desire to extend the quality and quantity of our lives in order to have quantity of our lives in order to have the time to “get it right” and “pass it the time to “get it right” and “pass it on”on”

Physical Health Mental/Emotional Health
Spiritual Health Social Health
Physical Health Mental/Emotional Health
Spiritual Health Social Health
What will it look like if we get it right?

Physical Health Mental/Emotional Health
Spiritual Health Social Health
““In the end, you want your congregational In the end, you want your congregational home to reflect your deepest longings and home to reflect your deepest longings and provide a haven for exploring life in an provide a haven for exploring life in an environment that allows you to bring out the environment that allows you to bring out the best in each other, your families, your best in each other, your families, your communities, your nation, and your world…communities, your nation, and your world…God’s world.”God’s world.”