Embed Size (px)
Citation preview

대 한 방 사 선 의 학 회 지 1992 ; 28 (5) : 794~ 797 Journal 01 Korean Radiological Society, September, 1992
Multiple Hamartomas (Mese야nc야hηlyr U nilateral Chest Wall in Infancy: CT Findings
Myung Joon Kim, M.D. , Choon Sik Yoon , M.D. , Ki Keun Oh, M.D. , Jong Tae Lee, M.D. , Woo Hee Jung, M.D. *
Department 01 Di‘agnostic Radiology, Severaηce Hospital, Yonsei [J,ηjνersity College 01 Medici‘ηe
- Abstract -
A case of multiple hamartomas of the unilateral chest wall in a four month old infant is presented. There
have been a few reports on the CT findings of the chest wall hamartoma in infancy. We describe bone changes
of the ribs and mineralization of this rare tumor on the CT scan , and the locations of two separate masses
Index Words: Infant , newborn , skeletal system
Ribs , neoplasms 474.319
Thorax , CT 47 1. 1211
Hamartoma
Chest wall hamartoma (mesenchymoma) is
very rare in infants. This mass usually presents
at birth and as a single , extrapleural mass aris
ing from one or more ribs. A few cases of multi
ple hamartomas have been reported (1-4). Y et , the cause and incidence of multiple lesions are
unknown.
We have performed whole body bone scan
with 99m Tc-MDP and CT scan , and describe
the CT findings of multiple hamartomas of the
chest wall and the locations of two separate
lesions.
CASE REPORT
A four month old male infant was admitted
to our hospital with productive cough for 1
month. A chest radiograph showed a large mass
(abou t 4 x 5 x 7 cm) of the left thorax , destroy
ing 3rd and 4th ribs , and focal thinning of 2nd ,
* 연세대학교 의과대학 명리학교실
5th ribs (Fig . 1). Another small mass (about
2 x 3 x 3 cm) ansmg from the costovertebral
junction of the left 10th rib , separated from the
above lesion , was found after the whole bone scan
with 99m Tc-MDP (Fig. 2). Adjacent 9th and
11 th posterior ribs were eroded by this mass.
Faint , irregular mineralizations were noted
within these two masses.
On CT scan , the soft tissue masses contain
ing conglomerate , spiculated calcific and ossific
densities were not surrounded by the cortical
bone. Underlying ribs showed the cortical ex
pansion and destruction , and increased density
of medulla (Fig. 3a). Focal low density was
suspected within the large mass. The left
transverse process of the 10th thoracic vertebra
was involved by the small mass located in the
costovertebral junction (Fig. 3b)
Portions of the left 2nd-5th ribs and 9th , 10th
ribs with these masses were removed. The chest
* Department 01 Pathology, Yoηsei University College 01 Mediciηc
이 논문은 1992년 1월 27일 접수하여 1992년 6월 9일에 채 택 되 었 음.
Received January 27. Accepted June 9, 1992
- 794-

Myung Joon Kim , et al : Multiple Hamartomas of the Unilateral Chest Wall in Infancy
tervening stroma were revealed. Fibroblastic pro
liferation with calcifications and ossifying
trabeculae were noted in the chondroid portion.
wall was repaired with Marlex mesh
Gross specimen showed a h emorrhagic por
tion , clearly spearated from a cartilaginous por
tion (Fig. 4). Histologically , a cavernous space
filled with blood and fibrous material in the in-
DISCUSSION
In most of the previous reports , the chest wall
hamartoma had been presented as a single mass
(1-8). In 1964, Hopkins and Freitas (4) reported
a case of bilateral osteochondromas of the ribs
in an infancy. But Dahlin (5) contended that
these bilateral masses most likely were benign
~ ‘ ‘;
’‘ .~
샌흉
”νι향’””깐
싸찮
‘ ‘
υj ””
행!’
""".
Fig. 1. Chest radiograph shows a large mass in the left chest wall with partial destruction of the 3rd and 4th ribs. A small mass (arrows) ansmg from the costovertebral junction of the left 10th rib is poorly seen ‘ Adjacent 2nd , 5th and 9th , 11th ribs are eroded by these masses
~.
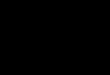
Fig.2. Posterior image of 99m Tc-MDP bone scan shows high activities within two masses
a b
Fig.3. a . Axial CT scan demonstrates a well demarcated mass occupying much of the left hemithorax . Con glomerate , spiculated calcifï c and ossific densiti es are seen within a large mass . Increased density of the intramedullary portion of the 3rd rib (arrow) is noted b. CT scan 6 cm lower than Fig . 3a shows a small mass of the left 10th rib , destroying the left transve rse process of 10th thoracic vertebra. It also contains clumpy calcific and ossific densities
- 795

Journal of Korean Radiological Society 1992 ; 28 (5) : 794~ 797
Fig.4. Resected tumor , contiguous to the ribs , shows a solid portion and a blood fìlled cystic component (white arrows) . The 3rd rib shows the cortical destruction and the intramedullary calcifìcation (arrows).
chest wall hamartomas. Thereafter a few cases
of multiple hamartomas of the chest wall have
been reported in the English literature (1-4)
The plain radiographic findings were reviewed
by many authors (1-7). But the CT features of the chest wall hamartoma have not been well
documented (3 ,7 ,8). Histopathologically this le
sion typically has cyst-like portion filled with
blood and solid , chondroid area with fibroblastic
proliferation , and significant amounts of
mineralization (1-3 ,5-7).
Initia\l y we missed a sma\l mass of the left
lower thorax on a chest radiograph. But whole
body bone scan with 99m Tc-MDP was helpful
in the reappraisal of chest radiograph due to intense uptakes of radiopharmaceutical by these
masses , even though the mass size varied great
ly . This finding may suggest that extensive
mineraJiza tion and formation of ossifying
trabeculae are present without regard to the mass
size . Gwyther (3) noted that uptake is dependent
on the relative rate of growth and proportion of
cartilagenous and vascular componen t.
Schlesinger et al (7) reported the CT and MR
findings of a case of chest wall hamartoma and
correlated the MR features with gross pathology.
One of the CT findings they described in their
case was that the epicenter of the chest wall mass
was in the rib as cortical bone surrounded the
mass. On the contrary, CT scans of bone win
dow setting did not demonstrate cortical bone
surrounding the periphery of mass in the patient
we presen t. We think that cortical change of the
ribs may depend on the degree of cortical expan
sion and destruction by the intramedullary soft
tlssue mass.
Conglomerate , spiculated calcifications and
ossifications within th masses were more well
defined on the CT scan than those noted on the
plain radiograph. Increased density adjacent to
the intramedullary soft tissue mass was reveal
ed as the mineralized portion of hamartoma.
Focallow density within a large mass correspon
ed to the cyst-like blood filled space of the
speClmen.
Oakley et al (1) reported that it tended to in
volve the main body of the rib and lie away from
the costochondral or costovertebral junction. In
our case , a large mass involved the main body
of the ribs , but a small one was located in the
costovertebral junction of the rib and involved
the left transverse process of 10th thoracic
vertebra . These findings may indicate that the
location of chest wall hamartoma is not unique
Two separate hamartomas of the unilateral
chest wall is extremely rare . Detection of another
small mass , similar to the radiologic pattern of
a large mass , may suggest a metastasis. A benign
hamartoma may be mistaken for a malignant le
sion because of foUowing radiologic findings; cor
tical destruction and involvement of multiple ribs
or adjacent bone as in the case we encountered
But the characteristic plain radiographic and CT
findings such as an extrapleural mass ansmg
from one or more ribs , cortical destruction or
expansion of the ribs , extensive mineralization
and some cyst-like portion within the mass , and
the patient age will aid in making the correct
diagnosis. CT is very helpful in the evaluation
of bony change of the ribs and the areas of
mineralization within hamartoma as well as its
extensIOn.
- 796-

Myung Joon Kim , et al : Multiple Hamartomas of the Unilateral Chest Wall in Infancy
REFERENCES
1. O akley RH , Carty H , Cudmore RE . Multiple
benign mesenchymomata of the ches wall
Pediatr Radiol 1985; 15: 58-60 2 . Brand T , Hatch EI , Schaller RT , StevensonJK ,
Arensman RM , Schwartz MZ. Surgical
management of the infant with mesenchymal
hamartoma of the chest well. J Pediatr Surg
1986;2 1 :556-558 3 Gwyther SJ , H all CM ‘ Mesenchymal hamar
toma of the chest wall in infancy. C lin Radi이
1991 ;43:24-25 4. H opkins SM , Freitas EL. Bilateral osteochon
droma of the ribs in an infant: An unusual cause
〈국문 요약〉
ofcyanosis.J Thorac and Cardiovasc Surg 1965; 49:247-249
5. McLeod RA , Dahlin DC . Hamartoma (mesen
ch ymoma) of the chest wall in infancy.
Radiology 1979; 131:657 -66 1
6. Blumenthal BI , Capitanio MA , Queloz JM ,
Kirkpatrick JA. Intrathoracic mesenchymoma
Observations in two infats. Radiology 1972‘ 104:107-109
7. Schlesinger AE , Smith MB , Genez BM ,
M cMahon DP , Swaney JJ. C hest wall mesen
chymoma (hamartoma) in infancy. CT and MR
findings. Pediatr R ad iol 1989; 19 ‘ 212-213 8 Campbell AN , Wagget J , Mott MG. Benign
mesenchymoma of the chest wall in infancy. J
Surg Oncol 1982;2 1‘ 267-270
유아의 펀측 흉벽에 발생한 다발성 과오종 (간엽종) : 전산화 단층 촬영 소견
연세대학교 의과대학 진단방사선과학교실, 병리학교실*
김영준 • 윤춘식 • 오기근 • 이종태 • 정우희*
소아의 늑골에서 발생하는 과오종(간엽종) 은 늑골 파괴 및 변형, 연조직 종괴등의 소견때문에 악성 골종양으로 오
인하거나 다발성으로 발생한 경우 전이성 병변으로 오진할 수 있는 드문 질환이다. 저자들은 4개월된 환아의 좌측
흉벽에 발생한 다발성 과오종의 단순 촬영, 골주사 및 전산화 단층촬영 소견을 병리소견과 함께 보고하며 특히 두 종
괴의 발병 위치와 전산화 단층 촬영 소견을 중심으로 문헌고찰과 함께 보고한다.
- 797-