Embed Size (px)
Citation preview

MUSCLE MUSCLE RELAXANTSRELAXANTS
Prepared by: Jeffrey Ian Chua
BSN-IIA

Muscle Relaxants
•What are they used for?–Facilitate intubation of the trachea–Facilitate mechanical ventilation–Optimized surgical working
conditions

Muscle Relaxants• How skeletal muscle relaxation
can be achieved?– High doses of volatile anesthetics– Regional anesthesia– Administration of neuromuscular blocking
agents• Proper patient positioning on the operating
table

Muscle Relaxants
• Muscle relaxants must not be given without adequate dosage of analgesic and hypnotic drugs
• Inappropriately given : a patient is paralyzed but not anesthetized

Muscle Relaxants
•How do they work?– Neuromuscular junction
• Nerve terminal• Motor endplate of a muscle• Synaptic cleft
– Nerve stimulation– Release of Acetylcholine (Ach)– Postsynaptic events

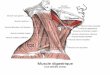
Neuromuscular Junction (NMJ)

Binding of Ach to receptors on muscle end-plate

Muscle Relaxants• Depolarizing muscle relaxant
– Succinylcholine• Nondepolarizing muscle relaxants
– Short acting– Intermediate acting– Long acting

Depolarizing Muscle Relaxant
• Succinylcholine• What is the mechanism of action?
– Physically resemble Ach– Act as acetylcholine receptor agonist– Not metabolized locally at NMJ– Metabolized by pseudocholinesterase in plasma – Depolarizing action persists > Ach– Continuous end-plate depolarization causes
muscle relaxation

Depolarizing Muscle Relaxant• Succinylcholine• What is the clinical use of
succinylcholine?– Most often used to facilitate intubation
• What is intubating dose of succinylcholine?– 1-1.5 mg/kg– Onset 30-60 seconds, duration 5-10
minutes

Depolarizing Muscle Relaxant• Succinylcholine–What is phase I neuromuscular
blockade?
–What is phase II neuromuscular blockade?
• Resemble blockade produced by nondepolarizing muscle relaxant
• Succinylcholine infusion or dose > 3-5 mg/kg

Depolarizing Muscle Relaxant• Succinylcholine–Does it has side effects?
• Cardiovascular• Fasciculation• Muscle pain• Increase intraocular pressure• Increase intragastric pressure• Increase intracranial pressure• Hyperkalemia • Malignant hyperthermia

Nondepolarizing Muscle Relaxants
• What is the mechanism of action?– Compete with Ach at the binding sites– Do not depolarized the motor endplate– Act as competitive antagonist– Excessive concentration causing channel
blockade– Act at presynaptic sites, prevent movement of
Ach to release sites

Nondepolarizing Muscle Relaxants
• Long acting– Pancuronium
• Intermediate acting– Atracurium– Vecuronium– Rocuronium– Cisatracurium
• Short acting– Mivacurium

Nondepolarizing Muscle Relaxants
• Pancuronium– Aminosteroid compound– Onset 3-5 minutes, duration 60-90 minutes– Intubating dose 0.08-0.12 mg/kg– Elimination mainly by kidney (85%), liver
(15%)– Side effects : hypertension, tachycrdia,
dysrhythmia,

Nondepolarizing Muscle Relaxants
• Vecuronium– Analogue of pancuronium – much less vagolytic effect and shorter
duration than pancuronium– Onset 3-5 minutes duration 20-35 minutes– Intubating dose 0.08-0.12 mg/kg– Elimination 40% by kidney, 60% by liver

Nondepolarizing Muscle Relaxants
• Atracurium– Metabolized by
• Ester hydrolysis • Hofmann elimination
– Onset 3-5 minutes, duration 25-35 minutes– Intubating dose 0.5 mg/kg– Side effects :
• histamine release causing hypotension, tachycardia, bronchospasm
• Laudanosine toxicity

Nondepolarizing Muscle Relaxants
• Cisatracurium– Isomer of atracurium– Metabolized by Hofmann elimination– Onset 3-5 minutes, duration 20-35 minutes– Intubating dose 0.1-0.2 mg/kg – Minimal cardiovascular side effects– Much less laudanosine produced

Nondepolarizing Muscle Relaxants
• Rocuronium– Analogue of vecuronium– Rapid onset 1-2 minutes, duration 20-35
minutes– Onset of action similar to that of
succinylcholine– Intubating dose 0.6 mg/kg– Elimination primarily by liver, slightly by
kidney

Alteration of responses• Temperature• Acid-base balance• Electrolyte abnormality• Age• Concurrent diseases• Drug interactions

Alteration of responses• Concurrent diseases
– Neurologic diseases– Muscular diseases
• Myasthenia gravis• Myasthenic syndrome (Eaton-Lambert synrome)
– Liver diseases– Kidney diseases

Alteration of responses
• Drug interactions– Inhalation agents– Intravenous anesthetics– Local anesthetics– Neuromuscular locking drugs– Antibiotics– Anticonvulsants– Magnesium

Monitoring Neuromuscular Function
•What are the purposes of monitoring?– Administer additional relaxant as
indicated– Demonstrate recovery

Monitoring Neuromuscular Function
How to monitor?• Clinical signs• Use of nerve stimulator

Monitoring Neuromuscular Function
• Clinical signs– Signs of adequate recovery
• Sustained head lift for 5 seconds• Lift the leg (child)• Ability to generate negative inspiratory pressure at
least 25 cmH2O, able to swallow and maintain a patent airway
• Other crude tests : tongue protrusion, arm lift, hand grip strength

Monitoring Neuromuscular Function
• Use of nerve stimulator– Single twitch : single pulse 0.2 msec– Tetanic stimulation– Train-of-four : series of 4 twitch, 0.2 msec
long, 2 Hz frequency, administer every 10-15 seconds
– Double burst stimulation– Post tetanic count

Evoked responses during depolarizing and nondepolarizing block

Hierarchy of Neuromuscular Blockade
Fraction of receptor occupied by
nondepolarizing muscle relaxant
Response to nerve stimulator
Whole body signs
99-100 No response Flaccid, extreme relaxation
95 Posttetanic facilitation present
Diaphragm moves, hiccough possible
90 One of four twitch of TOF present
Abdominal relaxation adequate for most prcedure
75 Four twitch of TOF present, TOF ratio 0.7
Tidal volume and vital capacity normal
50 100-Hz tetanus sustained
Passes inspiratory pressure test
30 200-Hz tetanus sustained
Head lift and hand-grip sustained

Antagonism of Neuromuscular Blockade
Effectiveness of anticholinesterases depends on the degree of recovery present when they are administered
• Anticholinesterases– Neostigmine
• Onset 3-5 minutes, elimination halflife 77 minutes• Dose 0.04-0.07 mg/kg
– Pyridostigmine– Edrophonium

Antagonism of Neuromuscular Blockade
• What is the mechanism of action?– Inhibiting activity of acetylcholineesterase– More Ach available at NMJ, compete for sites
on nicotinic cholinergic receptors – Action at muscarinic cholinergic receptor
• Bradycardia• Hypersecretion• Increased intestinal tone

Antagonism of Neuromuscular Blockade
• Muscarinic side effects are minimized by anticholinergic agents– Atropine
• Dose 0.01-0.02 mg/kg– Scopolamine– glycopyrrolate

Reversal of Neuromuscular Blockade
• Goal : re-establishment of spontaneous respiration and the ability to protect airway from aspiration