Embed Size (px)
Citation preview

British Heart J7ournal, 1977, 39, 1390-1393
Myocardial ultrastructural changes inKugelberg-Welander syndrome'HIROMITSU TANAKA, SEIJI NISHI, KOHJI NURUKI, ANDNOBUYUKI TANAKA
From the First Department of Internal Medicine, Faculty of Medicine, Kagoshima University, Usuki-cho,Kagoshima, J7apan
Electron microscopical study of a biopsied specimen of myocardium from a patient with the Kugelberg-Welander syndrome revealed myocardial degeneration, including preferential loss of myosin filaments andabnormalities in the Z bands. Leptomeric fibrils were also observed in the cardiac muscle cell; there does notappear to be a previous report of the finding of such fibrils in human myocardium.
It has been reported that the heart can be involved waddling. The ankle jerks were slightly accentuatedin the Kugelberg-Welander (K-W) syndrome bilaterally.(Matsumoto et al., 1971; Sterz et al., 1971; Sugi- Other deep tendon reflexes were not elicited. Themura et al., 1973), a spinal muscular atrophy des- sensory examination was normal. The electro-cribed by Wohlfart et al. (1955), and Kugelberg myogram showed a neurogenic patter. Muscleand Welander (1956). Recently, we reported 2 cases biopsy revealed mixed neurogenic and myogenicof this syndrome with cardiomyopathy and re- muscular atrophy. The nerve conduction velocityviewed the published reports (Tanaka et al., 1976). was normal. Blood picture, urinalysis, andTo our knowledge, there has not been any report blood chemistry were all within normal range. The
of the fine structural changes of the myocardium in chest x-ray film showed no cardiomegaly. Thethe K-W syndrome. In this communication, we electrocardiogram was also normal. His bundledescribe the results of electron microscopical electrogram showed normal PA, AH, and HVexamination of myocardium from a patient with the intervals. Right cardiac catheterisation showed nor-K-W syndrome. mal pressures. No shunt was seen.
Case historyMETHODS
A 20-year-old man was referred in June 1974 to the After informed consent was obtained, a Konno-Kagoshima University Hospital for investigation of Sakakibara catheter bioptome (Konno and Saka-muscular atrophy. He seemed to have been well kibara, 1963) was inserted into the right ventricleuntil the age of 7 years, when he noticed progressive through the right saphenous vein, and endomyo-clumsiness in running. He first noticed difficulty in cardial biopsy was performed.climbing stairs at the age of 17 years. One year Histological sections of the biopsy specimen werebefore admission, he developed difficulty in getting stained with haematoxylin and eosin. For electronup by himself. He had no symptoms of cardiac dis- microscopical observation, the tissue was fixed inorder. The family history and past history were not 3 per cent glutaraldehyde buffered with 0.1 Mcontributory. He did not drink alcohol. On ad- phosphate (pH 7.4) for 2 hours and postfixed inmission, he was well developed. The pulse was 2 per cent osmium tetroxide for 2 hours. After rapid64/min and regular. The blood pressure was 102/42 dehydration with ethanol and propylene oxide, themmHg. No murmur was audible. Neurological tissue was embedded in Epon 812. A Porter-Blumexamination disclosed weakness and atrophy of the ultramicrotome (Ivan Sorvall, Inc.) was used forproximal muscles of the extremities. The gait was cutting the blocks and the sections were stained on
the grids with uranyl acetate and lead citrate.'Supported in part by Research Grant for Cardiomyopathy from the Electron micrographs were taken with a JEM 100BMinistry of Health and Welfare. electron microscope.
1390
on June 16, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.39.12.1390 on 1 D
ecember 1977. D
ownloaded from

Myocardial changes in K-W syndrome 1391
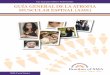
Fig. 1 Electron micrograph showing fine filaments and abnormality in the Z band. Many fine filaments are packed:within the cytoplasm. Some of them are attached almost perpendicularly to the irregular Z-band-like material.The fine filaments are 60 to 80 A in diameter. The Z-band-like material (ZM) is present in an irregular bandand in a cylindrical mass. A few degenerated mitochondria are also present.
Results of morphological examinations material and because of their diameter (60 to 80A).A few mitochondria characterised by cristolysis or
(A) LIGHT MICROSCOPICAL EXAMINATION swelling were scattered within these myocytes. TheThe specimen showed normal structure. No incidence of these myocytes was about 1 or 2 out ofsignificant changes were observed in myocardial 50 myocytes. An additional finding was the presencecells, the interstitial tissues, or in the endocardium. of leptomeric fibrils, which consisted of dense bands
and fine filaments that were attached perpendicu-(B) ELECTRON MICROSCOPICAL EXAMINATION larly to each band and had a regular periodicity ofDegenerated myocytes were occasionally found about 220 mF (Fig. 2). The leptomeric fibrils wereamong apparently normal myocytes. The degene- seen in myocytes which showed degenerativerated myocytes contained many fine filaments, changes, including degeneration of the mitochondriaaccumulations of Z-band-like material, a few ab- and irregularity of the Z bands.normal mitochondria and some vesicles. The Z-band-like material was present in irregular bands or Discussionin cylindrical masses. A great many fine filamentswere packed within the cytoplasm. Some of them Seven cases of the K-W syndrome with cardio-were attached to the Z-band-like material almost myopathy have been reported. Histological studiesperpendicularly. Thick filaments were very few or of myocardium in this syndrome were reported incompletely lost in these cells (Fig. 1). The fine 2 patients. Sugimura et al. (1973) reported a 23-filaments seemed to be actin filaments because of year-old woman who showed first degree atrio-their perpendicular attachment to Z-band-like ventricular block, atrial premature beats, and
on June 16, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.39.12.1390 on 1 D
ecember 1977. D
ownloaded from

1392 Tanaka, Nishi, Nuruki, and Tanaka
* . ; , , . @ . ..... .. ...........s~~~~~~~~~~~~~~~~~~~~~~~~~~. ...... .... ...
Fig. 2 Electron micrograph showing leptomeric fibrils, which consist of dense bands (arrows) connected by finefilaments. They have a regular periodicity of about 220 mp and seem to be connected to the sarcolemma (sectionedobliquely at S) on one side of the disorganised cell.
paroxysmal atrial tachycardia. Fibrosis of the right degenerative neuromyopathic diseases. We conatrium was shown by endomyocardial biopsy. sidered the preferential loss of myosin filamentsUsing light microscopy we noted slight interstitial found in this patient to be a degenerative changefibrosis in the myocardium from another patient, a because other degenerative changes, including26-year-old man with K-W syndrome and cardiac mitochondrial and Z band alterations, were alsochanges (Tanaka et al., 1976). The present study, the present in the myocytes.first report on electron microscopical findings of the Another finding seen in this patient was themyocardium in K-W syndrome, has revealed pre- presence of leptomeric fibrils. Leptomeric fibrilsferential loss of myosin filaments in some degene- were discovered by Ruska and Edwards (1957) inrated myocytes. Recently, Maron et al. (1975) the latissimus dorsi muscle of a young thrush inreported on ultrastructural changes of cardiac 1957. Since then, they have been found in myo-muscle cells in patients with cardiac hypertrophy. cardium as well as in the skeletal muscle of variousThey reviewed the published reports on myofi- mammals (Bogusch, 1975; Saetersdal and Mykle-brillar changes. Preferential loss of myosin filaments bust, 1975). However, we have not found anyhas been reported in various abnormal cardiac cells. previous report of leptomeric fibrils in humanIt has been observed in cardiac muscle cells in hearts. We also observed leptomeric fibrils in thehypoxic rats (Dusek et al., 1971), in the crista myocardium of KK and yellow KK mice whichsupraventricularis in patients with congenital heart were found to have myocardial degenerationdisease (Jones et al., 1975), and in the left ventricle in (Nishi et al.). The function of the leptomeric fibrilspatients who had received daunorubicin therapy is still controversial. The relation between the pre-(Buja et al., 1973; Buja and Ferrans, 1975). How- ferential loss of myosin filaments and the occurrenceever, this finding has not previously been reported of leptomeric fibrils in our patient remains to bein the myocardium of patients with heredofamilial- clarified.
on June 16, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.39.12.1390 on 1 D
ecember 1977. D
ownloaded from

Myocardial changes in K-W syndrome 1393
References report of a case. Respiration and Circulation, 19, 863-870.(In Japanese with English abstract.)
Bogusch, G. (1975). Electron microscopic investigations on Nishi, S., Tanaka, H., Shinyashiki, T., and Kanehisa, T.leptomeric fibrils and leptomeric complexes in the hen and Histopathological studies of the myocardium in the spon-pigeon heart. Journal of Molecular and Cellular Cardiology, taneously cardiopathic KK mice; a new disease model of7,733-745. idiopathic cardiomyopathy. (In preparation.)
Buja, L. M., and Ferrans, V. J. (1975). Myocardial injury Ruska, H., and Edwards, G. A. (1957). A new cytoplasmicproduced by antineoplastic drugs. In Recent Advances in pattern in striated muscle fibers and its possible relation toStudies on Cardiac Structure and Metabolism, Vol. 6, growth. Growth, 21, 73-88.Pathophysiology and Morphology of Myocardial Cell Saetersdal, T. S., and Myklebust, R. (1975). UlstrastructureAlterations, p. 487. Ed. by A. Fleckenstein and G. Rona. of the pigeon papillary muscle with special reference to theUniversity Park Press, Baltimore. sarcoplasmic reticulum. Journal of Molecular and Cellular
Buja, L. M., Ferrans, V. J., Mayer, R. J., Roberts, W. C., Cardiology, 7, 543-551.and Henderson, E. S. (1973). Cardiac ultrastructural Sterz, H., Harrer, G., Marchet, H., Kaserer, H. P., Schlam-changes induced by daunorubicin therapy. Cancer (Phila- berger, H., Samec, Hj., and Stark, U. (1971). Primaire unddelphia), 32, 771-788. neurogene Skelettmuskelerkrankungen bzw. -paralysen
Dusek, J., Rona, G., and Kahn, D. S. (1971). Healing process mit schweren Kardialen Rhythmusstorungen. Zeitschriftin the marginal zone of an experimental myocardial infarct: fiur Kreislaufforschung, 60, 1-13.findings in the surviving cardiac musde cells. American Sugimura, F., Iijima, M., Ozawa, Y., Ooki, Y., and Watanabe,Journal of Pathology, 62, 321-338. S. (1973). Two cases of Kugelberg-Welander's disease with
Jones, M., Ferrans, V. J., Morrow, A. G., and Roberts, W. C. cardiopathy. Clinical Neurology, 13, 79-86. (In Japanese(1975). Ultrastructure of crista supraventricularis muscle in with English abstract.)patients with congenital heart diseases associated with right Tanaka, H., Uemura, N., Toyama, Y., Kudo, A., Ohkatsu,ventricular outflow tract obstruction. Circulation, 51,39-67. Y., and Kanehisa, T. (1976). Cardiac involvement in the
Konno, S., and Sakakibara, S. (1963). Endomyocardial biopsy. Kugelberg-Welander syndrome. American Journal ofDiseases of the Chest, 44, 345-350. Cardiology, 38, 528-532.
Kugelberg, E., and Welander, L. (1956). Heredofamilial Wohlfart, G., Fex, J., and Eliasson, S. (1955). Hereditaryjuvenile muscular atrophy simulating muscular dystrophy. proximal spinal muscular atrophy. A clinical entity simu-Archives of Neurology and Psychiatry, 75, 500-509. lating progressive muscular dystrophy. Acta Psychiatrica et
Maron, B. J., Ferrans, V. J., and Roberts, W. C. (1975). Neurologica Scandinavica, 30, 395-406.Ultrastructural features of degenerated cardiac muscle cellsin patients with cardiac hypertrophy. American Journal of Requests for reprints to Dr Hiromitsu Tanaka, ThePathology, 79, 387A434. First Department of Internal Medicine, Faculty of
Matsumoto, K., Kakiuchi, F., Kakihana, M., Katayama, S., Medicine., Kagoshima University, Usuki-cho, Kago-Sakamoto, T., and Murao, S. (1971). Kugelberg-Welanderdisease with cardiopathy of unknown etiology. Clinical shima, 890, Japan.
on June 16, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.39.12.1390 on 1 D
ecember 1977. D
ownloaded from













![Home [] · 2018. 12. 4. · Wohlfart, Laoureux, Seybold, Kayser, Kuchler, Nelson, Portnoff, Rieding, Seitz, Sitt e altri). Data la particolarità dello strumento, non previsto nei](https://img.pdfslide.tips/doc/110x75/5fe89fc1bb424c608a5ac45c/home-2018-12-4-wohlfart-laoureux-seybold-kayser-kuchler-nelson-portnoff.jpg)





