Embed Size (px)
Citation preview

R
C
N
Pa
b
c
d
a
ARRA
KDCOIC
1
dhctstfwt
s
CH
h0
ARTICLE IN PRESSG ModelESUS-5950; No. of Pages 6
Resuscitation xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Resuscitation
j ourna l h o me pa g e : www.elsev ier .com/ locate / resusc i ta t ion
linical Paper
eurocognitive long term follow-up study on drowned children
ertti K. Suominena,∗, Niina Sutinenb, Saija Vallea, Klaus T. Olkkolac,d, Tuula Lönnqvista
Children’s Hospital, Helsinki University Central Hospital, FinlandHyvinkää Hospital, FinlandUniversity of Turku and Turku University Hospital, FinlandHelsinki University Central Hospital and Institute of Clinical Medicine, University of Helsinki, Helsinki, Finland
r t i c l e i n f o
rticle history:eceived 18 October 2013eceived in revised form 10 March 2014ccepted 23 March 2014
eywords:rowningardiopulmonary resuscitationutcome assessment
ntelligencehild
a b s t r a c t
Aim of the study: Report cognitive and neurological outcome later in life of surviving drowned childrenwho had received CPR either from bystanders or from emergency medical services (EMS) units.Methods: Forty children who had drowned and admitted to pediatric intensive care unit after successfulCPR between 1985 and 2007, were eligible for the study. Of those 21 gave a consent for neurological andneuropsychological examinations. All data are expressed as median (interquartile range). Mann-WhitleyU, Wilcoxon signed ranks and Chi square tests were used.Results: The median age of the 21 patients at drowning was 2.4 (1.8, 5.5) years and 12.5 (8.6, 19.4)years at the time of neurological and neuropsychological examination. The median interval between thedrowning accident and examinations was 8.1 (5.4, 14.4) years. Twelve patients (57.1%) had either signs ofminor (6/21) or major neurological dysfunction (6/21). Eight subjects (40.0%) had full-scale intelligencequotient (FIQ) of less than 80 (range 20–78). The median estimated submersion time of the subjects withnormal FIQ was 3.5 (2.0, 7.5) min, which was significantly shorter than for those with FIQ < 80, 12.5 (5.0,
22.5) min (p = 0.0013). Cognitive or neurologic deficits were detected in 17 of the 21 subjects, although11 of them were reported to have a full recovery at the hospital discharge.Conclusions: This study showed that 57% of the drowned and resuscitated children had neurologicaldysfunction and 40% a low FIQ. Neurological and neuropsychological long term follow-up in drownedchildren is highly recommended.© 2014 Published by Elsevier Ireland Ltd.
. Introduction
Accurate prognosis of a surviving drowned child cannot be pre-icted from the initial presentation or examinations on arrival toospital. Only limited data on the long term neurocognitive out-ome after a drowning incident are available. The variability inhe definitions of the patient population and the outcome mea-urements used in previous studies make it difficult to assess longerm outcome.1–8 The patient populations of earlier studies varied
Please cite this article in press as: Suominen PK, et al. Neurocognitive(2014), http://dx.doi.org/10.1016/j.resuscitation.2014.03.307
rom children who had been subjected to drowning for a short timeithout cardiac arrest to hypothermic children who were brought
o the hospital with ongoing cardiopulmonary resuscitation (CPR)
Abbreviations: CPR, cardiopulmonary resuscitation; EMS, emergency medicalystems; IQ, intelligence quotient; PICU, pediatric intensive care unit.∗ Corresponding author at: Department of Paediatric Anaesthesia and Intensiveare, Children’s Hospital, University of Helsinki, Stenbäckinkatu 11, FI-00029 HUS,elsinki, Finland.
E-mail address: [email protected] (P.K. Suominen).
ttp://dx.doi.org/10.1016/j.resuscitation.2014.03.307300-9572/© 2014 Published by Elsevier Ireland Ltd.
and rewarmed by cardiopulmonary bypass.1–8 Consequently, thesurvival rates of these study populations varied between 11% and100%.5,6 A study by Pearn showed that 95% of the children who wereadmitted to hospital after a drowning accident, were completelyneurologically normal and had a median intelligence quotient (IQ)higher than that of the general population.5 However, other studieson drowning children for whom CPR was initiated by emergencymedical services (EMS) unit at the accident site, reported survivalrates with mild or no neurological deficits of only 14–21%.1,2
The quality and timing of outcome evaluation will affect theresults. Complete neurological and neurocognitive examinationsof drowning victims are superior to using outcome scales based onchart reviews. The former are used to assess higher cortical func-tions such as memory or executive functions.9,10 Young drowningsurvivors may function at a level consistent with age-expectationsat discharge, but long-term cognitive sequelae may not manifest
long term follow-up study on drowned children. Resuscitation
until the child enters school or some defects such as executivefunctions do not become fully apparent until early adolescence.8,11
This is the first long term follow-up study of a comprehensivepatient–survivor population of children who underwent drowning

ARTICLE IN PRESSG ModelRESUS-5950; No. of Pages 6
2 P.K. Suominen et al. / Resuscitation xxx (2014) xxx–xxx
Admitted to PICU
n=(64)
Discharged from the
PICU
(n=53)
Alive
(n=43)
Address could not be
located
(n=1)
Exclud ed because of
medical histo ry
prior drowning
(n=2)
Did not pa rti cipat e
to the study
(n=19) - Did not respond to the
enquiry n=11 - Did n ot g ive a cons ent
(n=7) - Gave a consent but died
before the stud y (n=1 )
Died within 6
months (n=9) Lost foll ow-up
(foreigner)
(n=1)
Died in the PICU (n=11)
Participated in the
neurological (n=21)
and
neuropsycholo gical
aEasp
2
HscoUHritrwatt
Ftwmamtt
Table 1The incidence of neurological dysfunction in children who survived drowning(n = 21).
Cluster of dysfunction andsigns according toHadders-Algra12
The number of patients(percent) with clusterabnormality
Dysfunctional muscle tone regulation(≥1 deviations)Muscle tonePosture during sitting, crawling, standingand walking
4 (19.0%)
Reflex abnormalities (≥2 signs)Abnormal intensity and/or threshold orasymmetry in: biceps reflex, knee andankle jerkFoot-sole response: uni- or bilateralBabinski sign
2 (9.5%)
Choreiform dyskinesia (≥1 movements)Spontaneous motor behaviorMovements of face, eyes, tongue
1 (4.8%)
Co-ordination problems (≥2 tests)Finger-nose test, fingertip touching test,diadochokinesis, Romberg, tandem gait,standing one foot
11 (52.4%)
Fine manipulative ability (≥2 tests)Finger opposition test: smoothness andtransitionQuality of hand and arm movementsPincher graspTremor
9 (42.9%)
Rarely occurring miscellaneousdisorders (≥1 signs)Motor behavior of face, eyes, pharynx andtongueAssociated movements during DDK,finger-opposition test, walking on toes orheelsAt least one of the following: Mild cranial
4 (19.0%)
test s (n=20)
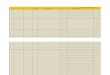
Fig. 1. A scheme for drowned children admitted to PICU.
s a child for whom CPR was attempted either by bystanders or byMS personnel. It aims at determining the neurocognitive outcomefter drowning and whether factors such as the length of submer-ion time are associated with cognitive function and neurologicalresentation later in life.
. Materials and methods
Approval of ethics committee of Helsinki University Centralospital was obtained for the prospective long term follow-up
tudy of the drowned children. The medical records of all drownedhildren who were successfully resuscitated either by a laypersonr by EMS personnel and admitted to the Pediatric Intensive Carenit (PICU) at the Children’s Hospital of Helsinki University Centralospital between the years 1987 and 2007 inclusive, were analyzed
etrospectively. All drowned children were taken to the paediatricntensive care unit (PICU) at the Children’s Hospital as per EMS pro-ocol. Information sources included pre-hospital EMS and medicalecords. The temperatures of lakes, rivers and sea surface watersere obtained from the Finnish Institute of Environment Agency
nd the Finnish Institute of Marine Research. Baltic seawater con-ains little sodium chloride (0.02–0.75%), therefore all incidents inhis study can be considered as freshwater submersions.
Sixty-four patients were admitted to the PICU (Fig. 1). Theinnish Population Register provided the current addresses ofhe survivors, who were discharged alive and information abouthether the child had died later. Two patients had pre-existingedical conditions that seriously impacted upon their physical
Please cite this article in press as: Suominen PK, et al. Neurocognitive(2014), http://dx.doi.org/10.1016/j.resuscitation.2014.03.307
nd cognitive condition prior to the submersion incident; one withoderate neurological defects due to meningitis a few years prior
o the drowning incident and the other with autistim caused byhe Kabuki syndrome. A letter was sent to the 40 survivors, who
nerve palsy and excessive associatedmovements
were alive and whose address were available. One reminder letterwas sent for the non-responders. The letter included a question-naire that covered the health-related quality of life (HRQoL) andeducation level the subjects had attained and also a consent formfor neurological and neuropsychological examinations had to besigned. Twenty-nine subjects returned the complete HRQoL ques-tionnaire and these results were reported earlier.7 Seven subjectsdeclined to participate in the clinical study and one subject diedbefore the clinical study due to a cause that was unrelated to thechildhood submersion incident. The seven subjects who did notgive a consent, were all reported to have full recovery at the hospitaldischarge.
Neurological (n = 21) and neuropsychological examinations(n = 20) were performed between November 2009 and December2010, except for one patient with severe anoxic brain injury whoneeded full time care in a nursing home. She was unable to attend tothe neurocognitive examinations and her condition was evaluatedby tests done in our hospital in 2002, five years after the drowning.One of the 21 patients who participated in the neurological exami-nation did not attend the neuropsychological examination despiteseveral scheduled appointments and reminders.
All the neurological examinations were done by one pediatricneurologist (coauthor NS) and data were reported according tocriteria for abnormal functional clusters of minor neurological dys-function described by Hadders-Algra (Table 1).12 Subjects with
long term follow-up study on drowned children. Resuscitation
minor neurological dysfunction have one or two cluster abnormal-ities and subjects with major dysfunction have abnormalities inthree or more clusters.

ARTICLE IN PRESSG ModelRESUS-5950; No. of Pages 6
P.K. Suominen et al. / Resuscitation xxx (2014) xxx–xxx 3
Table 2A comparison of patients who participated to neurocognitive follow-up examinations and non-participants (n = 40).
Participants (N = 21) Non participants (N = 19) P-value
Age at the time of accident (years) 2.4 (1.8, 5.5) 5.1 (1.5, 6.8) 0.542Submersion time (min) 5.0 (3.0, 11.3) 2.0 (1.0, 3.0) 0.002Water temperature (◦C) 16.2 (9.3, 20.6) 21.0 (10.5, 27.0) 0.309Resuscitation by layperson (n) 15 18 0.053Received CPR by EMS unit (n) 11 3 0.015Intubated at the scene (n) 15 5 0.004First core temperaturea (◦C) 30.8 (29.0, 33.1) 34.0 (32.2, 36.3) 0.007pHa 7.2 (7.0, 7.3) 7.3 (7.2, 7.3) 0.080Base excessa (mmol/l) −14.2 (−20.4, −5.7) −7.1 (−11.9, −4.6) 0.048Blood glucosea (mmol/l) 10.1 (8.3, 13.8) 9.9 (8.3, 12.7) 0.716Mechanically ventilated at PICU (n) 16 6 0.005Ventilation time (days) 2.5 (1.0, 4.0) 2.0 (1.0, 4.0) 0.653Length of PICU stay (days) 3.0 (1.0, 5.3) 1.0 (1.0, 1.0) 0.006POPC at hospital discharge (n)Normal (POPC = 1)Mild to severe deficit (POPC ≥2)
1110
172
0.011
TPA , eme
wtaptsWotrw
cPnspa(
Fon
a(wUfa
3
t5botwdtac
he data are given as median (interquartile range) or number.-values determined by Mann Whitney U test or Chi square test.bbreviations: ◦C, Celsius; POPC, Pediatric Overall Performance Category Scale; EMSa On arrival to the emergency room.
Neuropsychological examinations were done by coauthor SVho assessed higher cortical functions such as IQ, memory, execu-
ive, verbal, visuospatial and visuoperceptual functions. Four verbalnd four performance Wechsler subtests were used, and verbal anderformance IQ and full-scale IQ (FIQ) were extrapolated accordingo the Wechsler intelligence manual scale for each test. The Wech-ler tests for IQ used were: WPPSI-III for 3–7 year-old children,
ISC-III for 7–16 year-old children and WAIS-III for over 16 year-ld young adults. A low IQ was defined as less than 80.11 A NEPSY-IIest was used for the children aged 3–16 years to analyze their neu-ocognitive function in more detail. The Wechsler Memory scale IIIas used to test memory functions in adults.
The neurological status of the survivors reported in the medi-al charts at discharge were retrospectively evaluated against theediatric Overall Performance Category Scale (POPC) before theeurological and neuropsychological examinations.13 The POPC-cale classifies the quality of life into six categories: (1) good overallerformance, (2) mild overall disability, (3) moderate overall dis-bility, (4) severe overall disability, (5) coma/vegetative state and6) brain death.
The main outcome measures are neurological dysfunction andIQ. The secondary outcome measures were other neuropsychol-gical deficits and factors associated with cognitive function andeurological presentation later in life.
All data were expressed as medians (interquartile range) andnalyzed by using the statistical program SYSTAT for Windowsversion 10.2; Systat Software, Richmond, CA, USA). P-values < 0.05ere considered statistically significant. We used Mann-Whitley, Wilcoxon signed ranks and Chi square tests to evaluate which
actors were associated with neurological outcome and IQ valuesfter drowning.
. Results
The median age of the 21 victims was 2.4 (1.8–5.5) years at theime of the accident. The estimated median submersion time was.0 (3.0–11.3) min. Six of the victims were submerged in pools oraths and 15 in natural bodies of water. The median temperaturef the water at the time of accident was 14.5 (5.7–19.1) ◦C. Six-een of the 21 patients received bystander CPR, the quality of whichas not recorded. On the arrival of the first EMS-unit, 11 patients
Please cite this article in press as: Suominen PK, et al. Neurocognitive(2014), http://dx.doi.org/10.1016/j.resuscitation.2014.03.307
id not have spontaneous circulation (9 asystole, 1 pulseless elec-rical activity and 1 ventricular fibrillation). A physician staffedmbulance or helicopter unit was at the site of the accident in allases, except one who had recovered after receiving bystander CPR.
rgency medical services.
Fifteen patients were intubated at the scene and one in the emer-gency room (ER). The median length of stay in the PICU was 3.0(1.0–5.3) days.
Those subjects who voluntarily participated in the examinations(n = 21) had significantly longer submersion time, were more likelyto receive CPR by EMS units and lower POPC score at hospital dis-charge than those 19 patients who did not participate in the tests(Fig. 1, Table 2). Thus the participants were more likely to have longterm consequences from the childhood drowning accident thanthose who did not participate.
3.1. Neurologic and cognitive outcome
The median interval between the drowning accident and neuro-logic and neuropsychologic examinations was 8.5 (5.4, 14.4) years.The median age of the 21 subjects at the time of the examinationwas 12.5 (8.6, 19.4) years and 12 were male. Twelve (57.1%) of thesubjects were still children under 16 years of age at the time of theexamination. Six of the 21 subjects had neurological and cognitivedeficits diagnosed before the drowning accident. Five of them haddelay in speech development and one in motor development. Thesedefects did not influence the POPC score at hospital discharge or tothe results of the follow-up study. Two of subjects had no conse-quences from the drowning incident and four of them had eithersevere neurological dysfunction alone or combined with low IQ. Nodeficits prior to the accident were reported in the medical charts ofthe remaining 15 subjects.
Nine (42.9%) of the 21 evaluated subjects were neurologicallyintact upon examination. Table 1 summarizes the clustering ofneurological dysfunction according to Hadders-Algra.12 Twelvepatients (57.1%) patients had either minor neurological dysfunction(6/20) with one or two cluster abnormalities or major neurologi-cal dysfunction (6/20) with three to five cluster abnormalities. Themost common deficits were in co-ordination (52%) and fine motorskills (43%).
The IQ assessment was performed on the 20 patients who par-ticipated in the neuropsychological examination. No significantdifferences emerged between the mean performance and verbalIQ scores in all the subjects (p = 0.85). Eight of the survivors (40%)had an FIQ of less than 80 and four of them had cognitive perform-
long term follow-up study on drowned children. Resuscitation
ances on the level of intellectual disability (FIQ below 70). Four ofall the 20 subjects had no cognitive or neurological deficits at theexaminations (Table 2). Five of the 12 subjects with normal FIQ hadat least moderate difficulties in executive functions (Table 3).

ARTICLE ING ModelRESUS-5950; No. of Pages 6
4 P.K. Suominen et al. / Resuscita
Table 3Cognitive and neurological outcome of 20 drowned childrena after a median follow-up period of 8.1 years.
Cognitive outcome Neurological outcome
Normal (N = 9) Minor deficits(N = 5)
Severe deficits(N = 6)
FIQ <80 (N = 8) 0 3 5
FIQ >80 (N = 12)No deficits 4 0 0Deficits
Memoryb 2 1 0Executive functionc 2 0 0Both deficits 1 1 1
a One of the 21 patients did not attend the neuropsychological examination.b Memory deficits are either verbal or visual or both and they are severe in all
patients (values are -2SD or below of expected values for a normal age-matchedpopulation).
oA
3S
fetndtac
TV
TPA
TV
TPA
c Executive function deficits are at least moderate in all patients (values are -1SDr below of expected values for a normal age-matched population).bbreviations: FIQ, full-scale intelligence quotient; SD, standard deviation.
.2. A comparison of the Pediatric Overall Performance Categorycale at discharge from the hospital and neurocognitive outcome
Three of the 11 subjects with a POPC score of 1 (normal) at theollow-up examinations had minor neurological dysfunction andight were normal. They all had FIQs of over 80 (range, 81–118). Ofhe four patients classified POPC 2 (mild disability): one had normaleurologic status with an FIQ of 97, two had minor neurological
Please cite this article in press as: Suominen PK, et al. Neurocognitive(2014), http://dx.doi.org/10.1016/j.resuscitation.2014.03.307
ysfunction and the fourth had major neurological dysfunction. Thehree patients with neurological dysfunction had FIQs between 66nd 78. Of the four patients in the POPC 3 (moderate disability)ategory, three had major and one minor neurological dysfunction
able 4ariables associated with neurological outcome after drowning accident (n = 21).
Neurologically intact (N = 9)
Age at the time accident (years) 2.1 (1.5, 3.5)
Age at the time of examination (years) 13.4 (9.5, 19.7)
Submersion time (min) 4.0 (2.0, 6.3)
Water temperature (◦C) 12.3 (3.0, 21.0)
First core temperaturea (◦C) 33.0 (29.3, 34.3)
pHa 7.2 (7.1, 7.3)
Base excessa (mmol/l) −7.6 (−15.3, −4.0)
Blood glucosea (mmol/l) 9.6 (8.5, 11.7)
Mechanical ventilation time (days) 1.0 (1.0, 1.0)
Length of PICU stay (days) 1.0 (1.0, 2.0)
he data are given as median (interquartile range).-values determined by Mann Whitney U test.bbreviations: ◦C; Celsius.a On arrival to the emergency room.
able 5ariables associated with full-scale IQ values after drowning accident (n = 20).
Normal FIQ (N = 12)
Age at the time accident (years) 2.4 (1.5, 5.9)
Age at the time of examination (years) 13.0 (9.1, 19.4)
Submersion time (min) 3.5 (2.0, 7.5)
Water temperature (◦C) 13.9 (5.0, 18.0)
First core temperaturea (◦C) 33.0 (30.0, 34.7)
pHa 7.2 (7.1, 7.3)
Base excessa (mmol/l) −8.7 (−16.0, −4.5)
Blood glucosea (mmol/l) 9.4 (7.8, 12.6)
Mechanical ventilation time (days) 1.0 (1.0, 2.5)
Length of PICU stay (days) 1.0 (1.0, 2.0)
he data are given as median (interquartile range).-values determined by Mann Whitney U test or Chi square test.bbreviations: IQ, full-scale intelligence quotient; ◦C, Celsius.a On arrival to the emergency room.
PRESStion xxx (2014) xxx–xxx
at follow-up. Three of them had an FIQ below 80 (range, 32–78) andone patient had an FIQ of 97. The two patients with severe overalldisability or coma (POPC 4–5) had severe neurological dysfunctionand FIQ scores of 20 and 42.
3.3. Factors associated with neurocognitive deficits
Patients for whom CPR was provided by EMS units (n = 11) hada higher risk of major neurologic dysfunction (p = 0.006) and lowFIQ (p = 0.017) compared with those survivors who received onlybystander CPR (n = 10). Submersion time, base excess on arrival tothe ER, mechanical ventilation time and the length of stay in thePICU were also significantly associated with the neurological andcognitive outcome (Tables 4 and 5).
In a separate analysis of parameters “water temperature below6 ◦C” and “submersion time less than 10 min” were not shown tobe significantly related to FIQ of higher than 80 or survival withoutneurological deficit (P 0.09–1.0).
4. Discussion
This is the first study to report the comprehensive long termfollow-up on 21 children and young adults who had drowned andsuccessfully resuscitated as a child. Eight (43%) of the survivorswere neurologically intact upon neurological examination and 12(60%) had normal FIQ. The most common neurological dysfunctionsobserved were associated with co-ordination (48%) and fine manip-
long term follow-up study on drowned children. Resuscitation
ulative ability (42%). Only four of the 21 subjects had no cognitiveor neurologic deficits when examined, although 11 of them werereported to have a full recovery at hospital discharge. We found anassociation between submersion time and neurocognitive outcome
Minor or major neurological deficit (N = 12) P-value
3.0 (2.1, 7.6) 0.17710.8 (7.8, 19.0) 0.569
7.5 (4.0, 19.0) 0.03714.9 (6.7, 17.9) 0.88730.7 (26.5, 32.4) 0.297
7.1 (6.9, 7.2) 0.145−17.0 (−23.2, −10.6) 0.047
11.5 (8.0, 14.5) 0.5373.0 (2.0, 7.0) 0.0055.0 (3.0, 7.5) 0.005
Low FIQ <80 (N = 8) P-value
2.5 (1.9, 4.0) 0.87711.3 (8.2, 19.7) 0.75812.5 (5.0, 22.5) 0.01313.3 (3.5, 17.4) 0.53729.0 (24.8, 30.4) 0.017
7.0 (6.8, 7.2) 0.132−21.0 (−25.4, −12.9) 0.025
12.7 (10.5, 15.4) 0.0583.0 (2.5, 6.0) 0.0515.5 (4.5, 7.5) 0.002

ING ModelR
uscita
ltlp
sbpsrasoatoloeu
idisrmalfit
dcebndlipEddoo
rTvWaemvmltd
trrfbt
ARTICLEESUS-5950; No. of Pages 6
P.K. Suominen et al. / Res
ater in life. The other predictive factors such as base excess and coreemperature on arrival to the ER, mechanical ventilation time andength of stay in the PICU were consequences of the duration of therimary insult and CPR.
The present study is in line with the earlier studies that report ahorter duration of submersion was significantly associated with aetter neurocognitive outcome and a good HRQoL2,3,7,14. It is notossible to determine an exact cut-off point for the duration ofubmersion that would be associated with a full neurocognitiveecovery for several reasons. The submersion time is almost alwaysn estimation given by stressed parents or bystanders. The circum-tances of a drowning accident and rescue will affect the changesf survival and therefore a short duration of submersion does notlways guarantee full recovery. For example, a 5-year old boy withhe reasonably short submersion time of 5 min, received 20 min ofngoing bystander CPR on a boat sailing from an island to the main-and before CPR by EMS personnel. Instead of fairly good chancesf intact survival after a submersion time of 5 min, his follow-upxaminations 22 years later revealed he had abnormal fine manip-lative ability and a low FIQ.
Unfortunately, a child’s neurocognitive status before the drown-ng accident is not always known in some of the cases and it is alsoifficult to attribute problems experienced by the survivor later
n life are solely due to the drowning incident. A 10-year old boyubmerged for 3 min in a public swimming pool was successfullyesuscitated by the lifeguard. He had full recovery according to theedical charts at discharge from the hospital. Fifteen years after the
ccident he had drug and alcohol addiction, and psychiatric prob-ems. In the neurological examination he had slightly abnormalne manipulative ability and did not attend the neuropsychologicalests despite several scheduled appointments and reminders.
Icy water temperatures and rapidly developing hypothermia inrowned children may enhance the chances of survival in someases with long submersion times, but generally the beneficialffects of hypothermia on survival of drowned children may haveeen overestimated.15 The heads of drowning young children doot remain above the surface of water during cooling, instead chil-ren cool after submersion.15,16 In the present study, significantly
ower body temperatures were measured on the arrival to the ERn those patients who survived with low FIQ. This is in line with therevious reports whereby a low body temperature on arrival to theR was related to a bad outcome.3,14,15 In a case teenager becomeseeply hypothermic when immersed in icy water below 6 ◦C beforerowning and cardiac arrest, good outcome following long durationf circulatory arrest and rewarming with extracorporeal membranexygenation can be possible.17
Hypoxic-ischemic injury in a child who has been drowned andesuscitated has huge impact on the victim’s family and society.18,19
he most susceptible areas to ischemic injury within the brain areascular end zones, hippocampus, insular cortex, and basal ganglia.ith an increasing severity of hypoxic-ischemia, more extensive
nd global neocortical injury will occur.16,20 Neuropsychologicxaminations after hypoxic brain damage reveals problems withemory, impaired executive functions, and visuospatial and
isuoperceptual performance.10,21 Patterns of cognitive deficitsay also vary between cases.21 Furthermore, diagnostic chal-
enges can be associated with magnetic resonance imaging (MRI)hat can be normal in drowned patients with neurocognitiveeficits.8,10
Timing of cognitive follow-up assessment is crucial. Baselineesting at discharge and a follow-up 3–6 months later has beenecommended for the adult intensive care unit survivors to allow
Please cite this article in press as: Suominen PK, et al. Neurocognitive(2014), http://dx.doi.org/10.1016/j.resuscitation.2014.03.307
ecovery of possible transient cognitive function.22 A three yearollow-up study of children with moderate and severe traumaticrain injury show a strong improvement during the first year afterhe trauma, but negligible improvement over the following two
PRESStion xxx (2014) xxx–xxx 5
years.23 A recent case report on two adult drowned men reportedimprovement of the cognitive performance at one year follow-up, but they both had permanent problems with memory, dividedattention, impaired executive functions and verbal fluency.10 In thepresent study, no neurological or cognitive improvement could bedetected in some of the patients at follow-up.
In a subsequent case report by Hughes et al. neuropsychologicalexamination was performed 12-years after an accident in which achild (2.5 years-old) had been reported “as recovering completely”in the original case report.8,24 However, subsequent neuropsychol-ogical examination revealed impairment of visual–spatial abilities,mild dyslexic characteristics, dramatic memory impairment, FIQof 85, impulsivity, poor concentration and difficulty in sequentialplanning and organization.8 The subsequent case report and ourfindings suggest that specific neuropsychological and neurologicexaminations should be performed, instead of gross neurologicalevaluation of the survivors at discharge to achieve a realistic pic-ture of the outcome. Furthermore, the follow-up period shouldbe scheduled according to age of the victim. Long-term cognitivesequelae may not manifest until the child enters school or somedefects including impaired executive functions do not becomeapparent until early adolescence.8,11 In earlier studies, neurologicand neurophysiologic follow-up of drowned children was per-formed between 3 and 40 months after the drowning and only someof the children had been at school at the time of neurocognitive test-ing, which may indicate inadequate follow-up duration in most ofthe studies.1,3–6,8 In the present study, only two children were notattending school at the time of neurocognitive testing.
A previous study that included all the drowned patients of thepresent study, found that a good HRQoL was achieved by the major-ity of subjects, although HRQoL was affected by the submersiontime.7 This suggests that survivors feel that their respective HRQoLis better than what the cognitive function might indicate, which isin line with the findings from adult patients who survived out-of-hospital cardiac arrest.25 Drowning survivors frequently postponedthe start of school by a year, received full time special education atschool, and studied in university less commonly than their age-matched peers.7
The limitations of our study are its relatively small populationwith a large variation in the age of the drowned subjects attend-ing the follow-up examinations. The subjects who did not give theirconsent to the neurological and cognitive examinations had shortersubmersion time, less likely received CPR by EMS units and had fullrecovery more often at hospital discharge. Therefore, the presentstudy does not represent the whole population of long term sur-vivors treated in PICU, but rather a follow up study of group ofpatients with the circumstances related to the drowning accidentdescribed in the article. MRI or tomographic scanning of the brainwas not systematically performed on the patients and therefore nocomparisons could be made with the neurocognitive findings.
5. Conclusions
We found that the patient who gave a consent to this follow-up study were more likely to have long term consequences fromthe childhood drowning accident than those who did not partic-ipate. Of the subjects participating to the study 57% had eitherminor or major neurological dysfunction and 40% had an FIQ of lessthan 80. Many of the survivors were behind age-matched peers forskills such as different aspects of memory and executive functions.Neurological and neuropsychological assessment at discharge from
long term follow-up study on drowned children. Resuscitation
hospital, and a follow-up examination 6–12 months later are highlyrecommended. The continuation of the follow-up should be sched-uled according to the results of these examinations and the age ofthe victim.

ING ModelR
6 uscita
C
A
A
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
ARTICLEESUS-5950; No. of Pages 6
P.K. Suominen et al. / Res
onflict of interest statement
The authors have no conflict of interest to disclose.
cknowledgement
This study was partly supported by the Laerdal Foundation forcute Medicine.
eferences
1. Bell TS, Ellenberg L, McComb JG. Neuropsychological outcome after severe pedi-atric near-drowning. Neurosurgery 1985;17:604–8.
2. Suominen P, Korpela R, Silfvast T, Olkkola KT. Does water temperature affectoutcome of nearly drowned children. Resuscitation 1997;35:111–5.
3. Kruus S, Bergström, Suutarinen T, Hyvönen. The prognosis of near-drownedchildren. Acta Paediatr Scand 1979;68:315–22.
4. Bratton SL, Jardine DS, Morray JP. Serial neurological examinations after neardrowning and outcome. Arch Pediatr Adolesc Med 1994;148:167–70.
5. Pearn J. Neurological and psychometric studies in children surviving freshwaterimmersion accidents. Lancet 1977;1:7–9.
6. Suominen PK, Vallila NH, Hartikainen LM, Sairanen HI, Korpela RE. Outcomeof drowned hypothermic children with cardiac arrest treated with cardiopul-monary bypass. Acta Anaesthesiol Scand 2010;54:1276–81.
7. Suominen PK, Vähätalo R, Sintonen H, Haverinen A, Roine RP. Health-relatedquality of life after drowning incident as a child. Resuscitation 2011;82:1318–22.
8. Hughes SK, Nilsson DE, Boyer RS, et al. Neurodevelopmental outcome forextended cold water drowning: a longitudinal case study. Int Neuropsychol Soc2002;8:588–96.
Please cite this article in press as: Suominen PK, et al. Neurocognitive(2014), http://dx.doi.org/10.1016/j.resuscitation.2014.03.307
9. Suominen PK. Vähätalo neurologic long term outcome after drowning in chil-dren. Scand J Trauma Resusc Emerg Med 2012;20:55.
0. Samuelson H, Nekludov M, Levander M. Neuropsychological outcome follow-ing near-drowning in ice water: two adult case studies. J Int Neuropsychol Soc2008;14:660–6.
2
2
PRESStion xxx (2014) xxx–xxx
1. Odd DE, Lewis G, Whitelaw A, Gunnell D. Resuscitation at birth and cognition at8 years of age: a cohort study. Lancet 2009;373:1615–22.
2. Hadders-Algra M. Developmental coordination disorder: is clumsy motorbehavior caused by a lesion of the brain at early age. Neural Plast2003;10:39–50.
3. Fiser DH. Assessing the outcome of pediatric intensive care. J Pediatr1992;121:68–74.
4. Quan L, Wentz KR, Gore EJ, Copass MK. Outcome and predictors of outcome inpediatric submersion victims receiving prehospital care in King County, Wash-ington. Pediatrics 1990;86:586–93.
5. Suominen P, Baillie C, Korpela R, Rautanen S, Ranta S, Olkkola KT. Impact ofage, submersion time and water temperature on outcome in near-drowning.Resuscitation 2002;52:247–54.
6. Ibsen LM, Koch T. Submersion and asphyxial injury. Crit Care Med2002;30(Suppl.):S402–8.
7. Wanscher M, Agersnap L, Ravn J, et al. Outcome of accidental hypothermia withor without circulatory arrest: experience from the Danish Præstø Fjord boatingaccident. Resuscitation 2012;83:1078–84.
8. Morris M. The reality of non-fatal-drowning. Samuel Morris Foundation; 2013.Available at http://youtu.be/fwccpjKlLXo [accessed 03.01.14].
9. Bierens JJ. Drowning resuscitation requires another state of mind. Resuscitation2013;84:1467–9.
0. Topjian AA, Berg RA, Bierens JJ, et al. Brain resuscitation in drowning victim.Neurocrit Care 2012;17:441–67.
1. Wilson FC, Harpur J, Watson T, Morrow JJ. Adult survivors of severe cerebralhypoxia – case series survey and comparative analysis. Neurorehabilitation2003;18:291–8.
2. Jackson JC, Gordon SM, Ely EW, Burger C, Hopkins RO. Research issues in theevaluation of cognitive impairment in the intensive care unit survivors. IntensiveCare Med 2004;30:2009–16.
3. Jaffe KM, Polissar NL, Fay GC, Liao S. Recovery trends over three years followingpediatric traumatic brain injury. Arch Phys Med Rehabil 1995;76:17–26.
long term follow-up study on drowned children. Resuscitation
4. Bolte RG, Black PG, Bowers RS, Thorne JK, Corneli HM. The use of extracorporealrewarming in a child submerged for 66 min. JAMA 1988;260:377–9.
5. Torgersen J, Strand K, Bjelland TW, et al. Cognitive dysfunction and health relatedquality of life after cardiac arrest and therapeutic hypothermia. Acta Anaesthe-siol Scand 2010;54:721–8.







![Follow Up[1.0]](https://img.pdfslide.tips/doc/110x75/5561462bd8b42a857d8b460a/follow-up10.jpg)