-
8/10/2019 neuropatii ereditare
1/9
Review
Hereditary NeuropathiesSafwan S. Jaradeh, MD
Abstract The spec trum of hereditary neuropathi es hasevolved
recently as a result of the exponential growth of genetic research.
For the purpose of thisreview, wewill use Charcot-Marie-Tooth
(CMT), he-reditary liability to pressure palsy (HNPP) and
he-reditary sensory and autonomic neuropathies(HSAN) to illustrate
the current clinical and geneticapproach to such neuropathies.
Key Words: hereditary motor and sensory neurop-
athies, hereditary sensory and autonomic neurop-athies,
peripheral nervous system diseases, genet-ics in neuropathy
( J Clin Neuromusc Dis 2003;5:7280)
Jean Martin Charcot, Pierre Marie, and Henry Tooth described
Charcot-Marie-Tooth neu-ropathy (CMT) in 1886. Their patients
haddistal muscular weakness, peroneal atrophy,and reduced reflexes.
Roussy and Lvy de-scribed patients with sensory motor neurop-
athy associated with profound tremor that re-sembled essential
tremor, and with astasiaand imbalance but without cerebellar
dys-function. Subsequent major classifications of CMT were made by
Dyck and Lambert in1968, and by Thomas in 1974, and werebased on
nerve conduction testing. These au-thors described 2 major types of
Charcot-Marie-Tooth neuropathy: a demyelinatingform associated with
slow nerve conduction(HMSN-I or CMT1) and an axonal form
asso-ciated with normal nerve conduction (HMSN-
II or CMT2).1
A smaller, third group had in-termediate conduction velocities,
and these were found later to represent the X-linked variant of CMT
(CMTX).
CMT is the most common hereditary motor and sensory neuropathy
(HMSN). 1 Theoverall prevalence is 20 to 40 in 100,000 per-sons. 2
Common CMT features include distalmuscle weakness and wasting,
distal sensory
impairment usually greater for the vibrationor proprioceptive
modalities, and absence of ankle jerks. These patients have high
archedfeet or pes cavus and hammertoes. In severecases, the distal
atrophy can progress to thedistal portion of the thigh (inverted
bottle of champagne). Two main types are distin-guished based on
electrophysiological andhistologic criteria. CMT1 is the more
com-mon and is characterized by slowed nerveconduction velocities
(NCV) and hyper-trophic nerves secondary to
demyelin-ation/remyelination and formation of onionbulbs. CMT2 is
characterized by normal or minimally slowed nerve conduction
veloci-ties, and the nerve biopsy shows predomi-nantly chronic
axonal loss.
In CMT1, the onset is usually before age20. The inheritance is
dominant and family history is positive. Pes cavus and
hammertoes
are present in 50% to 75% of the patients. Thehand intrinsic
muscles become involved inup to two thirds of the patients. Sensory
im-pairment is usually asymptomatic, and pa-tients rarely report
numbness or other posi-tive sensory symptoms such as prickling or
tingling. Generalized areflexia can occur in50% of the patients.
Palpable enlarged nervesare present in 25% to 35% of the patients;
thehypertrophy is best appreciated in branchesof the superficial
cervical plexus or thegreater auricular nerve. Approximately
10%
have scoliosis. Essential or postural tremor can be present in
up to one third of patients(Roussy-Lvy variant).
The hallmark of CMT1 is significantslowing of NCV to
-
8/10/2019 neuropatii ereditare
2/9
ing NCV can test the autosomal-dominant na-ture of CMT1. The
penetrance is full and NCV abnormalities present at a very early
age. 5 8
However, there is some variability of NCV, ashigh as 10 to 15
m/s, among affected mem-bers in each pedigree. 5
Three important factors help differenti-ate CMT1 from acquired
demyelinating neu-ropathies. First, there is little change in NCV
over time. One study, which evaluated CMT1subjects over a 25-year
span, found a changeless than 3 to 4 m/s for the peroneal NCV
andless than 2 or 3 m/s for the median NCV. 7
Second, the NCV slowing is uniform betweenhomologous nerves and
within a given limb.Third, conduction block is absent, providedthat
the negative area under the curve of thecompound muscle action
potential is mea-sured, supramaximal stimulation is ensured,and if
confined short segments of the nerveare tested. Practically, a
greater than 50% or 60% drop in the proximal to distal motor
area/amplitude ratio should raise the possibil-ity of conduction
block.
Another characteristic of the CMT1nerve biopsies is the presence
of hypertro-phic changes in the nerve. There is enlarge-ment of the
endoneurial area. Multiple layers
of Schwann cell processes surround thinly myelinated fibers
resembling onion bulbs. 1
The electrophysiological and histologicchanges pointed to a
genetic defect in themyelin. Peripheral nerve myelin surroundingthe
axon has 3 major components. The mostabundant myelin protein is P0
, which consti-tutes 50% of the total myelin protein, pre-sumed to
be the culprit for CMT1. However,studies on the trembler mouse, in
which there is a signal for arrested myelination,found a defect on
chromosome 11 that coded
for a transmembranous protein called periph-eral myelin protein
22 ( PMP22 ).9 Investiga-tors began to examine the possibility of a
de-fect in PMP22 and chromosome 17, theequivalent of chromosome 11
in the mouse.The concomitant encounter of a severe formof CMT1 in a
patient with trisomy 17 leadingto an abnormal PMP2 confirmed that
CMT1phenotype is mainly linked to the PMP2 on
chromosome 17. 10 Subsequent studies foundthat the PMP2 gene
locus is surrounded by 2repeat sequences, one is distal and one
isproximal. An unequal crossover during meio-sis will end up with
one chromosome 17 thathas and extra PMP22 repeat and will lead toa
CMT1 phenotype. Fluorescent in situ hy-bridization (FISH) permits
labeling these re-peats and allows genetic testing for CMT1. 15
17
Affected subjects will have 3 repeats indica-tive of DNA
duplication leading to excessiveRNA and increased rather than
decreased PMP22. 11
There are occasional cases of CMT1 whose genetic testing reveals
a point muta-tion. 12 Phenotypically, it is difficult to
distin-guish these patients, but they tend to havesomewhat slower
conduction velocities andthinner myelin sheaths compared with
theduplication cases. 13
Subsequently, the role of P0 was inves-tigated, because it is
the major myelin pro-tein. The search was facilitated by the
discov-ery of a link between some cases of CMT1and the Duffy blood
group locus on chromo-some 1. 14 A marker for P0 was found
onchromosome 1q22, and patients with its mu-tation are labeled as
CMT1B. 15 Statistically,
CMT1B is much less common than CMT IA. P0 is a 28-kd protein
with an intramembra-nous component that functions as a struc-tural
molecule, an intracellular componentthat is important in signal
transduction, andan extracellular component, which acts likean
adhesion molecule. Its impairment willlead to a less compact myelin
and slowedconduction velocities. 16 A recent study re- vealed that
the Roussy-L vy family genotypeis actually CMT-1B rather than
CMT1A. 17
A more recent variant of CMT1 was
linked to the chromosome 10q22-q23 regioncontaining the early
growth response 2 gene( EGR2 ), a transcription factor with a key
rolein peripheral nerve myelination. The neurop-athy was severe
with prominent sensory lossand moderately reduced NCV. 18
Rare cases of CMT1 are autosomal-recessive. They present in
early childhood with marked slowing of nerve conduction.
7Journal ofCLINICALNEUROMUSCULARDISEASE
Volume 5, Number 2 December 2003
Hereditary Neuropathies
-
8/10/2019 neuropatii ereditare
3/9
The nerve biopsies show multiple layers of Schwann cell basal
lamina. Some cases weremapped to chromosome 5q23-q33. 19,20
Thegenetic defect leads to abnormal axon Schwann cell signaling,
and the neuregulin-2gene ( NRG2 ) appears to be the candidate for
the 5q23 form. 20 In rare cases, linkage to the PMP22 or EGR2 loci
was found. 21 The origi-nal pedigree linked to chromosome 8q24
isnow considered a variant of CMT4 (see sub-sequently in this
article). 22
In summary, CMT1A can be the resultof either a duplication or
point mutation of PMP22 on chromosome 17p11.2-12. CMT1Bis the
result of a duplication of P0 on chro-mosome 1q22. CMT1C is mapped
to the EGR2 locus on chromosome 10q22-q23. Au-tosomal-recessive
CMT1 is linked to chromo-some 5q23-q33, chromosome 17p11.2-12
or,less often, chromosome 10q22-q23.
The second major type of Charcot-Marie-Tooth is the so-called
axonal variant or CMT2. These patients characteristically haveno
slowing or borderline slowing in their nerve conduction velocities.
CMT2A and 2Bare usually disorders of adulthood and sel-dom begin
before the age of 20. 23 The family history is present in a least
70%, but pes ca-
vus and hammertoes are present in less that50%. Nerve
enlargement is absent. Thetremor is rare and usually parallels the
degreeof intrinsic hand weakness. CMT2C begins inchildhood with
hoarseness and dyspnea thatfollow exercise or emotional stress. 24
This isthe result of early laryngeal and diaphrag-matic weakness.
Sensory loss is quite mild inCMT2A and C, but nociceptive loss in
CMT2Bis significant and often leads to ulceration of the distal
foot. Patients have scoliosis and wasting of their truncal muscles.
The electro-
physiological features show primarily an axo-nal neuropathy. The
sensory nerve action po-tential tends to be reduced or absent in
thefoot, and there are chronic neurogenicchanges as shown by needle
electromyogra-phy, which are greater distally. The nerve bi-opsy
shows loss of myelinated fibers to a vari-able degree. The gene for
CMT2A wasmapped to the Kinesin KIF1B locus on
chromosome 1p35-36, and the defect prob-ably disrupts synaptic
vesicle transport alongthe axons. 25 CMT2B was mapped to 3q13-q22,
but the nature of the genetic defect isnot known. 26 CMT2C has not
been mapped yet.23
Recently, additional phenotypes of au-tosomal-dominant CMT2 were
described.One form, designated CMT2D, presented with greater upper
limb involvement; thisform was mapped to multiple T-cell
gammareceptor genes on chromosome 7p14. 27 An-other variant with
proximal limb involve-ment was mapped to 3q13.1 region. 28
Somefamilies with CMT2 had missense mutationsinvolving the
neurofilament light chain geneon chromosome 8p21; this form was
desig-nated CMT2E. 29 One French family from Nor-mandy presented
after the fourth decade with lancinating pain, pharyngeal
dysphagia,deafness, and Argyll-Robertson pupils. Thedefect was a
mutation in the P0 gene locus. 30
D jerine and Sottas described CMT3 ashypertrophic interstitial
neuropathy or neuri-tis. Most cases are sporadic. The onset is
usu-ally in early childhood but can be neonatal with hypotonia.
There is proximal limb andtrunk weakness and a characteristic
marked
sensory ataxia. Practically, it is the only CMTin which there is
loss of joint position sensein the fingers at an early age. There
is gener-alized areflexia and nerve enlargement in allpatients and
skeletal changes are prominent.This corresponds to Dr. Dyck s
classificationof HMSN-III. The nerve biopsies show absentor very
thin myelin with markedly prominentonion bulbs.
Electrophysiologically, there issevere slowing of nerve conduction
veloci-ties to less than 10 m/s, and the responses aretemporally
dispersed. By analogy to CMT1,
CMT3A is linked to the PMP 22 gene on chro-mosome 17; CMT3B is
linked to the P0 pro-tein gene on chromosome 1, whereasCMT3C is
linked to a mutation in the EGR2transcription factor. An
interesting discovery was that most sporadic CMT3 cases are
asso-ciated with homologous duplication of either locus, and
therefore represent an autosomal-dominant gene rather than a
recessive one. 31
74 Journal ofCLINICAL
NEUROMUSCULARDISEASE
Volume 5, Number 2 December 2003
Jaradeh
2003 Lippincott Williams & Wilkins
-
8/10/2019 neuropatii ereditare
4/9
The intermediate form of CMT is X-linked. 32 34 There is pes
cavus and distal leg wasting. Patients need a cane by their fifth
decade. There is some wasting in the handintrinsic muscles, but
proximally the patientis very strong. The onset is usually in
child-hood, and women are always either mildly affected or are
asymptomatic. Like mostCMT, the sensory loss is mild. Men lose
their reflexes but women only lose their ankle jerks. Pes cavus and
hammertoes are com-mon particularly in men, and claw hand
de-formity occurs in some men but virtually never in women. Some
recessive cases beginin childhood and have mental retardation
andspasticity. Other recessive cases begin inadulthood with
spasticity without mental re-tardation. The nerve conduction
velocitiescan be slow but are usually faster than 25m/s, which
somewhat differentiate those pa-tients from CMT 1. Again, the
slowing isgreater in the lower limbs, and slowing is very uncommon
in women. The sensory nerve action potential tends to be absent or
reduced in the feet. Subsequent studies 34
found some slowing in the upper extremitiesas the disease begins
in childhood. On nervebiopsy, there is a dropout of nerve
fibers
again, and it gets worse as the disease pro-gresses without
prominent onion bulbs. Elec-tron microscopy shows some wrapping of
Schwann cell processes around thinly myelin-ated fibers but, for
the most part, CMTX is anaxonopathy. CMT X has been linked
primar-ily to the Connexin ( CX32 ) gene on Xq13.CX32 is
predominantly a transmembranousmolecule that belongs to a family of
mem-brane semichannels known as connexons.Cases that map to this
gene locus are knownas CMTX1. The less common childhood-
recessive CMTX has been mapped to theshort arm of chromosome X,
but the genedefect is unknown. 35 Adult-onset cases with spastic
paraparesis are mapped to Xq26 butare not linked to Connexin. The
defect con-sists of point mutation, not duplication, andat least 30
mutations have been described.
CMT4 is autosomal-recessive and rare.It begins in infancy or
childhood with de-
layed motor milestones. Distal weakness andatrophy reach
proximal muscles by the sec-ond decade and adults become
wheelchair-bound. Facial muscles can be involved. Thereis
generalized areflexia, but sensory loss ismild. Other skeletal
abnormalities are com-mon. NCV are slowed to 15 to 30 m/s.
His-tologically, there are irregular redundantloops of myelin on
nerve biopsy. 37 Genotypi-cally, the Tunisian form was described
first; itis termed CMT4A 36 and has been mapped tothe GDAP1 gene on
chromosome 8q13-21.1.The gene encodes proteins expressed in
re-sponse to gangliosides. The European form(CMT4B) is linked to
chromosome 11q22-23 with mutations in the gene for a
phosphataseknown as myotubularin-related protein-2.37,38 One recent
CMT4 family had a muta-tion involving the PRX gene 39 on
chromo-some 19q13.1-13.3. One variant occurs in theLom district in
Bulgaria (CMT4D-Lom), which was mapped to the NDRG1 locus on
chro-mosome 8q24. 22
HEREDITARY NEUROPATHY WITHLIABILITY TO PRESSURE PALSY
Hereditary neuropathy with liability to
pressure palsy (HNPP) is another major he-reditary sensory motor
neuropathy. Theseare patients who usually present with recur-rent
focal neuropathies. 40 The onset can beat any age but often after
the second decade.The neuropathies are at common entrapmentsites.
Brachial plexus involvement occurs inless than 25%. The key feature
is that thepreceding trauma is very minor. Patients would lie on
their arms for 5 minutes andhave radial nerve palsy, or would cross
their legs for 5 to 10 minutes and develop foot-
drop. The neuropathy is often painless. Themore severe cases
have pes cavus and ham-mertoes. There is mild generalized slowing
of nerve conduction studies with disproportion-ately greater
slowing of the distal latency when compared with the proximal
veloc-ity. 41 The slowing is greater for the involvednerve and is
not uniform. Occasional casescan have partial conduction block,
particu-
7Journal ofCLINICALNEUROMUSCULARDISEASE
Volume 5, Number 2 December 2003
Hereditary Neuropathies
-
8/10/2019 neuropatii ereditare
5/9
larly around the area of compression. 42 Thecarriers often
exhibit mild slowing. Thenerve biopsy shows sausage-like swelling
of the myelin sheath described as tomaculousformations (tomacula =
sausage). Teased fi-bers disclose areas of segmental demyelin-ation
adjacent to some of the tomaculae, which explains the focal
conduction block seen in these patients. As shown on
electronmicroscopy, there are redundant loops of my-elin. These
patients were initially tested for duplications of the PMP22 gene
on chromo-some 17, but instead, geneticists found a de-letion of
this gene. It has been proposed thatthere is an unequal crossover
in the region of the responsible gene during meiosis. Thekaryotype
with 3 parts of the PMP22 gene will develop CMT1A, whereas ending
up with only one 1.5-kb segment will result inHNPP. 43 Thus, HNPP
and CMT1A representgenetic reciprocates.
Some cases of familial recurrent bra-chial plexopathy are
painful and are not as-
sociated with a polyneuropathy. This disor-der was recently
mapped to chromosome17q25. 44
Diagnostic Approach to HereditarySensory and Motor
Neuropathies
HMSN should be suspected in any chronic insidious neuropathy. 45
Detailedfamily pedigree should be obtained from thepatient and
relatives. Focused clinical evalu-ation and nerve conduction
studies on thesiblings are very helpful. If the functional de-cline
is rapidly progressive, other causes of neuropathy should be ruled
out.
The age of onset, the presence of proxi-mal and cranial
weakness, and the presenceof choreiform movements are very
usefulclinical clues (see Table 1). Nerve conduc-tion studies are
essential. When conduction velocities are under 25 m/s, CMT1A is
statis-tically the most likely diagnosis. DNA testingfor PMP22 gene
duplication or mutation onchromosome 17 has the highest yield in
this
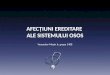
Table 1. Major Hereditary Motor and Sensory Neuropathies
(HMSN)
CMT1 CMT2 CMT3 CMT4 CMTX
Onset Abolescence or adulthood
Adulthood Infancy or childhood
Infancy or childhood
Childhood or adulthood
Sex M = F M = F M = F M = F M > F Weak limb Distal
proximalDistal Distal and
proximalDistal >
proximalDistal
Cranial nerve Vere rare(VIII)
Absent, except2C
Rare(V, VII)
Rare (VII) Absent
Distal sensory loss
Mild Mild, except2B
Moderate tosevere
Mild Mild
Areflexia Distal >proximal
Distal Diffuse Diffuse Distal >proximal
Pyramidalsigns
Rare (1A) Rare (AR) Absent Absent Rare (AR)
Pes cavus Late > early Late Early Early Late > early
Scoliosis Mild Absent, except
2CModerate Moderate Mild
Tremor Common Rare Choreiform Rare RareEnlarged
nervesPresent Absent Present Absent Rare
NCV 75% LLN
-
8/10/2019 neuropatii ereditare
6/9
situation. If negative, testing for P0 or EGR2mutations can be
requested. If still negative,testing for CX32 mutation can be done,
butthe yield is higher in men because women with CMTX do not have
significantly slowedconduction velocities. All these tests are
com-mercially available.
For intermediate conduction velocities(25 35 m/s), testing for
the CX32 mutationshould be done first. If negative, testing for
CMT1 can be pursued as described previ-ously. 46,47
If all testing is negative but family evalu-ation confirms an
inherited etiology, other familial demyelinating neuropathies
shouldbe suspected and tested for. These includemetachromatic
leukodystrophy, Krabbe s dis-ease, Refsum s disease, and
adrenomyeloneu-ropathy.
When nerve conduction velocities arenot significantly slow
(above 35 m/s), asearch for the CX32 mutation can be pur-sued,
particularly in women. If negative, test-ing for the CMT2 gene can
be obtained, butthe yield is lower because only testing for
theneurofilament light gene is commercially available.
If the diagnosis remains elusive, a sural
nerve biopsy should be considered.
HEREDITARY SENSORY ANDAUTONOMIC NEUROPATHIES
Hereditary sensory and autonomic neu-ropathies (HSAN; formerly
hereditary sensory neuropathies) represent another major cat-egory
of inherited neuropathies. 48 They arefar less common than HMSN. In
HSAN, sen-sory and autonomic ganglia and axons areinvolved. The
discovery of various neuro-
trophic factors and their respective tyrosinekinase (TRK)
receptors led to an increasedunderstanding of these
neuropathies.
HSAN I is the most common type.Symptoms usually begin in the
second tothird decade. Some patients present with neuropathic foot
ulcers that can lead to re-current cellulitis and osteomyelitis.
Other pa-tients present with burning or painful feet.
Pain can involve the hands, but finger ulcer-ations are rare. On
examination, sensory lossis mainly for nociceptive modalities.
Distalanhidrosis with proximal hyperhidrosis iscommon, whereas
visceral autonomic neu-ropathy is infrequently seen.
Sensorineuralhearing loss can be present. Motor strength isusually
preserved. There is distal areflexia.Some patients have pes cavus
and othershave overt Charcot joints. Sensory nerve ac-tion
potentials are reduced or absent distally.Motor conductions are
usually normal, butthe electromyogram could show few largemotor
unit potentials in distal muscles. Suralnerve biopsies reveal
axonal loss of nerve fi-bers, greater for the unmyelinated and
smallmyelinated nerve fibers. 48
Genetically, HSAN I is autosomal-dominant and has been linked to
chromo-some 9q22.1-q22.3. 49 Recently, mutations inthe gene
encoding for the long chain basesubunit-1 of serine
palmitoyltransferase werediscovered. 50 The responsible gene locus
isad jacent to the TRKB recep tor gene(NTRK2).
HSAN II is less common and presentoften in childhood with
painless injuries tothe limbs. Deformed feet occur because re-
peated small fractures lead to bone resorp-tion. There is distal
anhidrosis. Mental retar-dation is rare. Some patients have absence
of the fungiform papillae of the tongue. Facialand corneal
sensations are impaired, andhearing loss can occur. Again,
nociceptivemodalities are affected to a greater extent. Visceral
pain perception and autonomicfunction are impaired. Areflexia is
usually generalized. Muscle strength is normal. Sen-sory nerve
action potentials are absent. Mo-tor nerve conduction and
electromyograms
are similar to HSAN I. Sural nerve biopsiesreveal axonal loss of
nerve fibers, greater for the myelinated nerve fibers. 48
Genetically, HSAN II is autosomal-recessive. The gene has not
yet beenmapped. 51
HSAN III is also known as Riley-Day syn-drome or familial
dysautonomia. Affectedchildren have low birthweight, failure to
7Journal ofCLINICALNEUROMUSCULARDISEASE
Volume 5, Number 2 December 2003
Hereditary Neuropathies
-
8/10/2019 neuropatii ereditare
7/9
thrive, alacrima, swallowing problems, inter-mittent vomiting,
and fever. Emotional upsetcan trigger autonomic dysreflexia with
hy-perhidrosis, hypertension, and blotching of the skin. Later on,
children develop posturalhypotension. Despite the frequency of
frac-tures of the spine and limbs, acral mutilationsare uncommon.
Scoliosis and Charcot s jointscan occur. On examination, there is
absenceof fungiform papillae of the tongue, cornealinsensitivity,
reduced gag reflex, areflexia,and generalized nociceptive
hypesthesia.Nerve conductions show reduced sensory nerve action
potentials amplitudes and bor-derline slowing of the motor
conduction ve-locities. The amplitude of sensory nerve ac-
tion potentials was reduced. Pathologically,there is a severe
loss of unmyelinated nervefibers with reduction of large myelinated
fi-ber diameters to less than 12 m. There isalso a decreased number
of neurons in allautonomic and dorsal root ganglia. 48,52 54
Genetically, HSAN III is autosomal-recessive. It has been mapped
to chromo-some 9q31 and is almost exclusive to Ash-kenazi Jews. The
gene for NTRK2 is locatedon chromosome 9 but is not the
responsible
gene.55
Chadwick et al. recently mapped 2actin genes in the familial
dysautonomia can-didate region on 9q31. 56
HSAN IV presents with congenital in-sensitivity to pain. 48,57
Affected childrenhave recurrent fever as a result of their
anhi-drosis. Hyperhidrosis and alacrima are seenin HSAN III but not
in HSAN IV. The nocicep-tive sensory modalities are diffusely
de-creased. Many patients have a learning dis-ability or mild
mental retardation. Sensory and motor nerve conduction studies are
nor-mal. Anatomically, there is a loss of the first-order
nociceptive neuron. Pathologically,there is an absence of small
neurons in thedorsal root ganglia with corresponding lossof
unmyelinated and small myelinated fibers.The trigeminal nerve is
also involved.
Genetically, HSAN IV is autosomal-recessive. It has been mapped
to chromo-
some 1q21-q22. Responsible mutations affectthe gene for NTRKA
(NTRK1) located onchromosome 1. 58,59
Diagnostic Approach to HereditarySensory andAutonomic
Neuropathies
HSAN should be suspected in any chronic small fiber neuropathy.
45 A detailedfamily pedigree should be obtained from thepatient and
relatives. Noninvasive evaluationof small fiber function by
quantitative auto-nomic testing, particularly measurement of sweat
responses, is more helpful than nerveconduction studies in
establishing the diag-nosis, as well as in the screening of
siblings.
Other hereditary conditions presenting with small-fiber
neuropathies should be evaluated:amyloidosis, Fabry s disease,
Tangier s dis-ease, and porphyria. Once these are ruledout, HSAN
become the likely diagnosis. If au-tonomic testing is not
available, punch skinbiopsies represent a minimally invasive
alter-native that allow direct evaluation of intra-epidermal nerve
fibers. Fat aspirate biopsy isalso minimally invasive and is
helpful for thediagnosis of amyloidosis. Genetic testing for
various HSAN is not yet widely available. Su-ral nerve biopsy
should be done as a last re-sort; it can also diagnose amyloidosis.
Thetreatment is mainly supportive. Prophylaxisof acral ulcers and
mutilation is paramount.Patients should avoid excessive
heating.
REFERENCES1. Dyck PJ, Chance P, Lebo R, et al. Hereditary
motor
and sensory neuropathies. In: Dyck PA, Thomas PK,Griffin JW, et
al., eds. Peripheral Neuropathy, vol 2,3rd ed. Philadelphia: WB
Saunders; 1993:1094 1136.
2. Holmberg BH. Charcot-Marie-Tooth disease in north-
ern Sweden: an epidemiological and clinical study. Acta Neurol
Scand . 1993;87:416 422.
3. Berciano J, Combarros O, Calleja J, et al. The appli-cation
of nerve conduction and clinical studies togenetic counseling in
hereditary motor and sensory neuropathy type I. Muscle Nerve .
1989;12:302 306.
4. Kaku DA, Parry GJ, Malamut R, et al. Nerve conduc-tion
studies in Charcot-Marie-Tooth polyneuropathy associated with a
segmental duplication of chromo-some 17. Neurology . 1993;43:1806
1808.
5. Nicholson GA. Penetrance of the hereditary motor
78 Journal ofCLINICAL
NEUROMUSCULARDISEASE
Volume 5, Number 2 December 2003
Jaradeh
2003 Lippincott Williams & Wilkins
-
8/10/2019 neuropatii ereditare
8/9
and sensory neuropathy type 1A mutation: assess-ment by nerve
conduction studies. Neurology .1991;41:547 552.
6. Hoogendijk JE, de Visser M, Bolhuis PA, et al. He-reditary
motor and sensory neuropathy type 1: Clini-cal and neurographical
features of the 17p duplica-tion subtype. Muscle Nerve . 1994;17:85
90.
7. Killian JM, Tiwari PS, Jacobson S, et al. Longitudinalstudies
of the duplication form of Charcot-Marie-Tooth polyneuropathy.
Muscle Nerve . 1996;19:7478.
8. Birouk N, Gouider R, Le Guern E, et al. Charcot-Marie-Tooth
disease type 1A with 17p11.2 duplica-tion. Clinical and
electrophysiological phenotypestudy and factors influencing disease
severity in 119cases. Brain . 1997;120(part 5):813 823.
9. Valentijn LJ, Baas F, Wolterman RA, et al. Identicalpoint
mutations of the peripheral myelin protein-22in Trembler-J mouse
and Charcot-Marie-Tooth dis-ease. Nat Genet . 1992;2:288 291.
10. Chance PF, Bird TD, Matsunami N, et al. Trisomy 17p
associated with Charcot- Marie-Tooth neuropa-thy I phenotype:
evidence for gene dosage as amechanism in CMT1A. Neurology .
1992;42:2295 2299.
11. Yoshikawa H, Nishimura T, Fujimura H, et al. El-evated
expression of messenger RNA for peripheralmyelin protein 22 in
biopsied peripheral nerve of patients Charcot-Marie-Tooth disease
type 1A. Ann Neurol . 1994;35:445 450.
12. Roa BB, Garcia CA, Suter U, et al. Charcot-Marie-Tooth
disease type 1A. Association with a spontane-ous point mutation in
the PMP22 gene. N Engl J Med . 1993;329:96 101.
13. Gabreels-Festen AA, Bolhuis PA, Hoogendijk JE, et
al.Charcot-Marie-Tooth disease type 1A: morphologi-cal phenotype of
the 17p duplication versus PMP22point mutations. Acta Neuropathol
(Berl) . 1995;90:645 649.
14. Bird TD, Ott J, Giblett ER. Evidence for linkage of
Charcot-Marie-Tooth neuropathy to the Duffy locuson chromosome 1.
Am J Hum Genet . 1982;34:388 394.
15. Hayasaka K, Takada G, Ionasescu VV. Mutation of the myelin
P0 gene in Charcot-Marie-Tooth neurop-athy type 1B. Hum Mol Genet .
1993;2:1369 1372.
16. Tachi N, Kozuka N, Ohya K, et al. Tomaculous neu-ropathy in
Charcot-Marie-Tooth disease with myelinprotein zero gene mutation.
J Neurol Sci . 1997;153:106 109.
17. Plante-Bordeneuve V, Guiochon-Mantel A, LacroixC, et al. The
Roussy-L vy family: from the originaldescription to the gene. Ann
Neurol . 1999;46:770 773.
18. Bellone E, Di Maria E, Soriani S, et al. A novel muta-tion
(D305V) in the early growth response 2 gene isassociated with
severe Charcot-Marie-Tooth type 1disease. Hum Mutat . 1999;14:353
354.
19. Gabreels-Festen A, van Beersum S, Eshuis L, et al.Study on
the gene and phenotypic characterisationof autosomal recessive
demyelinating motor andsensory neuropathy (Charcot-Marie-Tooth
disease) with a gene locus on chromosome 5q23-q33. J Neu- rol
Neurosurg Psychiatry . 1999;66:569 574.
20. Ring HZ, Chang H, Guilbot A, et al. The human neu-regulin-2
(NRG2) gene: cloning, mapping and evalu-ation as a candidate for
the autosomal recessive
form of Charcot-Marie-Tooth disease linked to 5q. Hum Genet .
1999;104:326 332.
21. Rogers T, Chandler D, Angelicheva D, et al. A novellocus for
autosomal recessive peripheral neuropathy in the EGR2 region on
10q23. Am J Hum Genet .2000;67:664 671.
22. Kalaydjieva L, Nikolova A, Turnev I, et al. Hereditary motor
and sensory neuropathy LOM, a novel de-myelinating neuropathy
associated with deafness ingypsies. Clinical, electrophysiological
and nerve bi-opsy findings. Brain . 1998;121(part 3):399 408.
23. Yoshioka R, Dyck PJ, Chance PF. Genetic heteroge-neity in
Charcot-Marie-Tooth neuropathy type 2. Neurology . 1995;46:569
571.
24. Dyck PJ, Litchy WJ, Minnerath S, et al. Hereditary motor and
sensory neuropathy with diaphragm and vocal cord paresis. Ann
Neurol . 1994;35:608 615.
25. Zhao C, Takita J, Tanaka Y, et al. Charcot-Marie-Tooth
disease type 2A caused by mutation in a mi-crotubule motor KIF1B .
Cell . 2001;105:587 597.
26. Kwon JM, Elliot JL, Yee W, et al. Assignment of asecond
locus for Charcot-Marie-Tooth type II locus
to chromosome 3q. Am J Hum Genet . 1995;57:853 858.27. Ionasescu
V, Searby C, Sheffield VC, et al. Autosomal
dominant Charcot-Marie-Tooth axonal neuropathy mapped on
chromosome 7p (CMT2D). Hum Mol Genet . 1996;5:1373 1375.
28. Takashima H, Nakagawa M, Suehara M, et al. Genefor
hereditary motor and sensory neuropathy (proxi-mal dominant form)
mapped to 3q13.1. Neuromus- cul Disord . 1999;9:368 371.
29. De Jonghe P, Mersivanova I, Nelis E, et al. Further evidence
that neurofilament light chain gene muta-tions can cause
Charcot-Marie-Tooth disease type2E. Ann Neurol. 2001:245 249.
30. Chapon F, Latour P, Diraison P, et al. Axonal phe-notype of
Charcot-Marie-Tooth disease associated
with a mutation in the myelin protein zero gene. J Neurol
Neurosurg Psychiatry . 1999;66:779 782.31. Jaradeh SS. Hereditary
neuropathies. American
Academy of Neurology, Course 7FC.006 . Denver;2002:169 190.
32. Hahn AF, Brown WF, Koopman WJ, et al. X-linkeddominant
hereditary motor and sensory neuropathy. Brain . 1990;113:1511
1525.
33. Dubourg O, Tardieu S, Birouk N, et al. Clinical,
elec-trophysiological and molecular genetic characteris-tics of 93
patients with X-linked Charcot-Marie-Tooth disease. Brain .
2001;124:1958 1967.
34. Nicholson GA, Nash J. Intermediate nerve conduc-tion
velocities define X-linked Charcot-Marie-Tooth neuropathy families.
Neurology . 1993;43:2558 2564.
35. Ionasescu VV, Trofatter JL, Haines JL, et al.
X-linkedrecessive Charcot-Marie-Tooth neuropathy: clinicaland
genetic study. Muscle Nerve . 1992;5:368 373.
36. Baxter RV, Othmane BK, Rochelle JM, et al.
Ganglio-side-induced differentiation-associated protein-1 ismutant
in Charcot-Marie-Tooth disease type4A/8q21. Nat Genet . 2002;30:21
22.
37. Quattrone A, Gambardella A, Bono F, et al. Autoso-mal
recessive hereditary motor and sensory neurop-athy with focally
folded myelin sheaths: clinical,electrophysiologic, and genetic
aspects of a largefamily. Neurology . 1996;46:1318 1324.
7Journal ofCLINICALNEUROMUSCULARDISEASE
Volume 5, Number 2 December 2003
Hereditary Neuropathies
-
8/10/2019 neuropatii ereditare
9/9
38. Bolino A, Brancolini V, Bono F, et al. Localization of a
gene responsible for autosomal recessive demye-linating neuropathy
with focally folded myelinsheaths to chromosome 11q23 by
homozygosity mapping and haplotype sharing. Hum Mol Genet
.1996;5:1051 1054.
39. Guilbot A, Williams A, Ravise N, et al. A mutation
inperiaxin is responsible for CMT4F, an autosomal re-cessive form
of Charcot-Marie-Tooth disease. Hum Mol Genet . 2001;10:415
421.
40. Windebank AJ. Inherited recurrent focal neuropa-thies. In:
Dyck PA, Thomas PK, Griffin JW, et al.,eds. Peripheral Neuropathy,
vol 2, 3rd ed. Philadel-phia, WB Saunders; 1993:1137 1148.
41. Amato AA, Gronseth GS, Callerame KJ, et al.Tomaculous
neuropathy: a clinical and electrophysi-ological study in patients
with and without 1.5-Mbdeletions in chromosome 17p11.2. Muscle
Nerve .1996;19:16 22.
42. Sellman MS, Mayer RF. Conduction block in heredi-tary
neuropathy with susceptibility to pressure pal-sies. Muscle Nerve .
1987;10:621 625.
43. Chance PF, Abbas N, Lensch MW, et al. Two auto-somal
dominant neuropathies result from reciprocalduplication/deletion of
a region of chromosome 17. Hum Mol Genet . 1994;3:223 228.
44. Pellegrino JE, George RA, Biegel J, et al. Hereditary
neuralgic amyotrophy: evidence for genetic homo-geneity and mapping
to chromosome 17q25. HumGenet . 1997;101:277 283.
45. Dyck PJ, Oviatt KF, Lambert EH. Intensive evalua-tion of
unclassified neuropathies yields improved di-agnosis. Ann Neurol .
1981;10:222 226.
46. Ionasescu VV, Ionasescu R, Searby C. Screening of dominantly
inherited Charcot-Marie-Tooth neuropa-thies. Muscle Nerve .
1993;16:1232 1238.
47. Jaradeh SS. Hereditary neuropathies: clinical
andelectrodiagnostic features and rationale testing.
American Association of Electrodiagnostic Medi- cine Course E.
San Diego; 1997:23 27.48. Dyck PJ. Neuronal atrophy and
degeneration pre-
dominantly affecting peripheral sensory and auto-nomic neurons.
In: Dyck PA, Thomas PK, Griffin JW,et al., eds. Peripheral
Neuropathy, vol 2, 3rd ed.Philadelphia: WB Saunders; 1993:1065
1093
49. Nicholson GA, Dawkins JL, Blair IP, et al. The genefor
hereditary sensory neuropathy type I (HSN-I)maps to chromosome
9q22.1-q22.3. Nat Genet .1996;13:101 104.
50. Dawkins JL, Hulme DJ, Brahmbhatt SB, et al. Muta-tions in
SPTLC1, encoding serine palmitoyltransfer-ase, long chain base
subunit-1, cause hereditary sen-sory neuropathy type I. Nat Genet .
2001;27:309 312.
51. Davar G, Shalish C, Blumenfeld A, et al. Exclusion of
p75NGFR and other candidate genes in a family with hereditary
sensory neuropathy type II. Pain . 1996;67:135 139.
52. Brunt PW, McKusick VA. Familial dysautonomia: areport of
genetic and clinical studies, with a review of the literature.
Medicine (Baltimore) . 1970;49:343 374.
53. Axelrod FB, Iyer K, Fish I, et al. Progressive sensory loss
in familial dysautonomia. Pediatrics . 1981;67:517 522.
54. Axelrod FB, Pearson J. Congenital sensory neuropa-thies.
Diagnostic distinction from familial dysauto-nomia. Am J Dis Child
. 1984;138:947 954.
55. Slaugenhaupt SA, Blumenfeld A, Liebert CB, et al.The human
gene for neurotrophic tyrosine kinasereceptor type 2 (NTRK2) is
located on chromosome9 but is not the familial dysautonomia gene.
Genom- ics . 1995;25:730 732.
56. Chadwick BP, Mull J, Helbling LA, et al. Cloning,mapping,
and expression of two novel actin genes,actin-like-7A (ACTL7A) and
actin-like-7B (ACTL7B),from the familial dysautonomia candidate
region on9q31. Genomics . 1999;58:302 309.
57. Rafel E, Alberca R, Bautista J, et al. Congenital
insen-sitivity to pain with anhidrosis. Muscle Nerve . 1980;3:216
220.
58. Mardy S, Miura Y, Endo F, et al. Congenital insensi-tivity
to pain with anhidrosis: novel mutations in theTRKA (NTRK1) gene
encoding a high-affinity recep-
tor for nerve growth factor. Am J Hum Genet . 1999;64:1570
1579.59. Mardy S, Miura Y, Endo F, et al. Congenital insensi-
tivity to pain with anhidrosis (CIPA): effect of TRKA (NTRK1)
missense mutations on autophosphoryla-tion of the receptor tyrosine
kinase for nervegrowth factor . Hum Mol Genet . 2001;10:179
188.
80 Journal ofCLINICAL
NEUROMUSCULARDISEASE
Volume 5, Number 2 December 2003
Jaradeh
2003 Lippincott Williams & Wilkins