Embed Size (px)
Citation preview

New anticoagulants: Monitoring or not Monitoring?
Not Monitoring
Anna Falanga, MD
Immunohematology and Transfusion Medicine
& Center of Hemostasis and Thrombosis,
Ospedali Riuniti
Bergamo, Italy
The 2nd
World Congress onCONTROVERSIES IN HEMATOLOGY (COHEM)Barcelona, Spain –
September 6‐8, 2012

OLD ORAL ANTICOAGULANT DRUGS: “Warfarin”
- slow onset (and offset) of action: requires bridging therapy with heparins.
- unpredictable pharmacokinetics and pharmacodynamics- interacts with many other drugs- variability in relation to diet and comorbidities- variability in relation to genetic factors (CYP2C9 and VKORC1
polymorphisms)
- narrow therapeutic range- need for laboratory monitoring

What are the characteristics of the ideal anticoagulants?

Prothrombinase
Xa, Valipid
ThrombinProthrombin
FONDAPARINUX
(XIMELAGATRAN)BIVALIRUDINARGATROBANDESIRUDIN
Fibrinformation
Plateletactivation
Fibrinolysisinhibition
Cellulareffects
New Anticoagulants (NOACs)
APIXABANRIVAROXABAN
DABIGATRAN
EDOXABAN

Main pharmacological characteristics of selected new oral anticoagulants
Dabigatran Rivaroxaban Apixaban Edoxaban
Target IIa Xa Xa Xa
Hours to Cmax 2 2‐4 1‐3 1‐2
Prodrug Yes No No No
CYP metabolism NoYes (CYP3A4/A5,
CYP2J2)
YES (CYP3A4, CYP1A2, CYP2J2)
YES (CYP3A4)
Efflux transporter P‐gp Yes Yes Yes Yes
Bioavilability 7% 80% 66% >45%
Protein binding 35% >90% 87% 55%
Half‐life (Hours) 12‐14 9‐13 8‐15 8‐10
Renal elimination 80% 66% 25% 35%
Dosing Twice a day Once a day Twice a day Once a day
Bid= twice daily; od= once daily; Tmax= time to peak plasma concentration

Comparative features of VKAs and NOACs
VKAs NOACs• Need for regular anticoagulation monitoring:‐food and drug interactions‐ narrow therapeutic window‐
inter‐
and intra‐individual variability in dose
response
• Fixed dose regimen without need for routine
monitoring:‐low potential for food and drug interaction‐ wider therapeutic window‐ predictable anticoagulant effect
• Delayed onset of action • Rapid onset of action
• Long half‐life • Short half‐life
• Mainly hepatic metabolism • Mainly renal clearence
• Available antidote • No available antidote
• Anticoagulant monitoring through INR • No standardized monitoring test
INR: international normalized ratio, NOACs: novel oral anticoagulants, VKAs: vitamin K antagonist

Why monitoring drugs?
• Drug monitoring aims to optimize dosage regimens in order to increase efficacy and/or safety
• If
the
plasma
concentration
of
a
drug
can
be accurately
anticipated
from
the
dose
applied
and
the
patient’s
body
weight,
it
does
not
usually require monitoring, even if its therapeutic window is narrow.

Not monitoring
Why not monitoring NOACs?

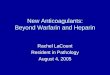
Dabigatran: Predictable Pharmacokinetics
Dose‐proportional increase in Cmax
and AUC indicate linear
pharmacokinetics over a wide range of doses
After a Single Dose
At Steady State
Stangier J.: Clin Pharmacokinet 2008:47:285‐295

Reproducible PK Profile of Dabigatran
PK profile is reproducible
across a wide range of doses1,2
1Stangier et al. Br J Clin Pharmacol 2007:64:292‐3032Stangier Clin Pharmacokinet 2008;47:285‐295

The oral direct thrombin inhibitor Dabigatran has:
• A predictable, linear PK/PD profile
• Quick onset and offset of action

Pharmacokinetics of Rivaroxaban
Kubitza D., et al. Clin Pharmacol Ther 2005
Dose‐proportional and linear PK with no accumulation after multiple dosing

Efficacy and safety
No monitoring has been used in phase III clinical trials that established the efficacy and safety of the NOACs

Schulman S et al. NEJM 2009; 361: 2342‐2352
Event rateEvent rateDABIGATRANDABIGATRAN 2.42.4
% %
WARFARINWARFARIN 2.12.1
% %
Efficacy outcomeEfficacy outcomeRecurrent venous thromboembolismRecurrent venous thromboembolism
p< 0.001p< 0.001 for non inferiorityfor non inferiority

EINSTEIN investigators NEJM 2010; 363: 2499‐2510
Efficacy outcomeEfficacy outcome
Safety outcomeSafety outcome
Major bleeding or clinically Major bleeding or clinically relevant nonmajor bleedingrelevant nonmajor bleeding
Recurrent venous Recurrent venous thromboembolismthromboembolism
p< 0.001p< 0.001 for non inferiorityfor non inferiority
P= 0.77P= 0.77
Event rateEvent rateRIVAROXABANRIVAROXABAN 2.12.1
% %
EnoxEnox--
WARFARINWARFARIN 3.03.0
% %
Event rateEvent rateRIVAROXABANRIVAROXABAN 8.18.1
% %
EnoxEnox--
WARFARINWARFARIN 8.18.1
% %

Effects of NOACs on Coagulation Assays

NOACs cause a significant prolongation of coagulation reactions producing misleading results in routine
clotting assays
Direct Thrombin Inhibitors Direct FXa Inhibitors
PT in sec and INR ↑ ↑APTT ↑ ↑Thrombin Time (TT) ↑↑ No
Fibrinogen (Clauss) No/↓ No
D‐dimers No No
These
alterations
do
not
correlate
with
the
drug
concentration,
therefore these tests are not to be performed to determine the drug activity.

Effect of Dabigatran
on APTT

Effects of Dabigatran
on Coagulation Assays
Van Ryn J et al, Thrombs and Haemost 2010
The time curves for aPTT, PT (expressed as international normalised ratio
[INR]), TT and ECT values
parallel the plasma concentration–time curve of dabigatran.
The maximum effect of dabigatran on clotting parameters occurs at the same time as maximal plasma
concentrations, indicating that thrombin inhibition by dabigatran is a direct effect linked to the central
plasma compartment.

Effects of Rivaroxaban
on Coagulation Assays
Harenberg J et al, Expert Rev. Hematol. 2012

“Monitoring”
vs “measuring” the anticoagulant effects of the NOACs

Measurement of the anticoagulant activity after a therapeutic dose of rivaroxaban or dabigatran etexilate
may be informative in cases of:
‐
Patients with low body weights or obese patients‐ Pediatric Patients‐ Renal or hepatic impairment‐ Accidental or deliberate overdose‐ To measure adherence‐ To evaluate patients with hemorrhagic or thrombotic complication‐ Before surgery
However,
in
the
absence
of
specific
antidotes,
a
measured
high
activity
merely allows us to approximate after which time the drug activity will
vanish, according
to its pharmacokinetic properties, which could have
been
calculated
if
the
timing of administration and the exact dose are known.

Current problems with measuring these drugs
• No validated assays
• Each drug has unique effect
• Drug effect on clotting factors is transient
•
Therapeutic ranges are uncertain

WHICH TEST?
• APTT
• Thrombin Time (TT)
• PT-INR
• Ecarin clotting time (ECT)
• Anti-Xa
• Thrombin Generation

DABIGATRAN
Features Test
APTT PT ECT TT
Responsiveness + - ++ ++++Linearity - + + +Standardization - - + -
Availability -+ + +

RIVAROXABAN/APIXABAN
Characteristics Test
PT APTT HepTest DRVVT aXa
Responsiveness + + ++ ++ ++
Linearity + + - - +
Standardization +/- - ? ? +/-
Availability -+ + - -

• ECT might be the choice for Dabigatran
• PT and/or aXa might be the choice for Rivaroxaban/Apixaban
For the time being, and only in case it is needed:

What the users of the new oral anticoagulants need to know
•
The new direct Factor Xa‐
and IIa‐inhibitors affect conventional clotting tests
•
These effects are reagent‐dependent
•
Do not routinely measure aPTT or prothrombin time to detect over‐
or underdose
•
Use specific tests recommended (if available) to detect over‐
or underdose, in particular in special patient
populations
•
However there is no need for routine
monitoring.

NOACs do not need monitoring on a routine basis