Embed Size (px)
Citation preview
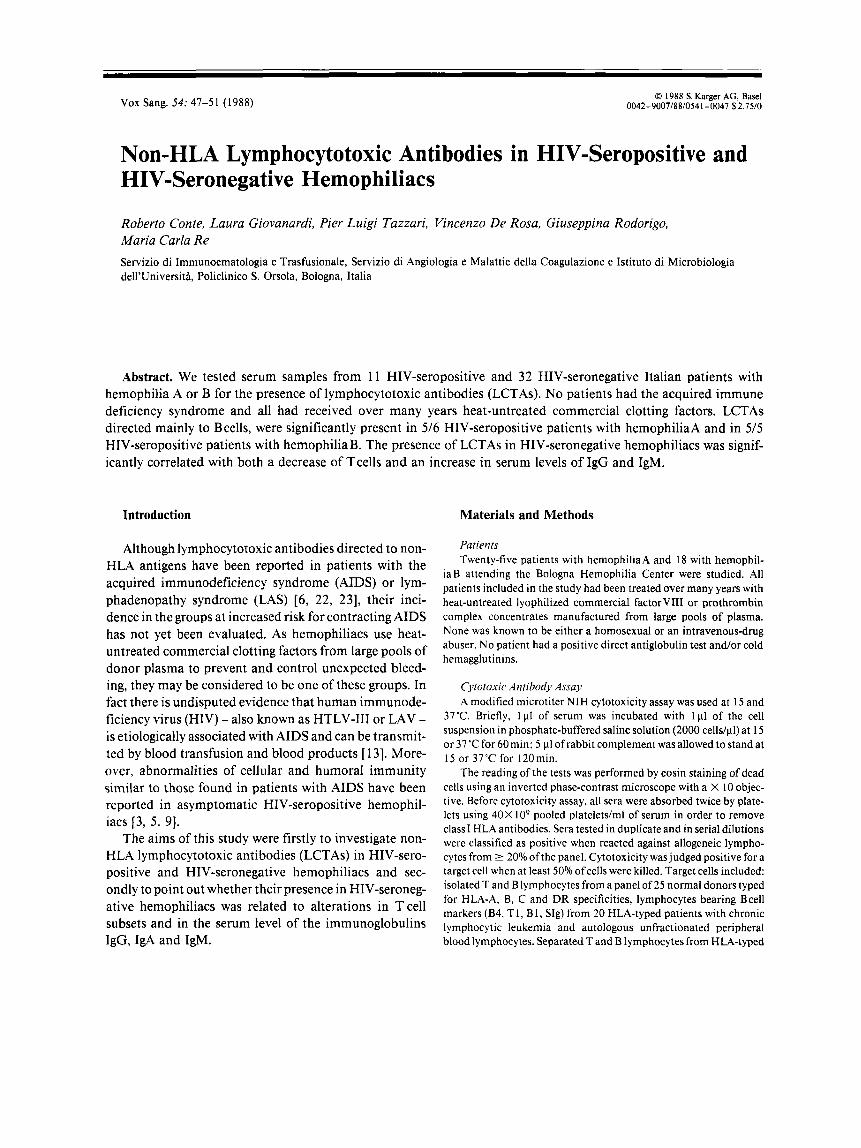
0 I988 S. Karger AG, Basel 0042-9007/88/0541-0047 $2.75/0 Vox Sang. 54: 47-5 1 (1 988)
Non-HLA Lymphocytotoxic Antibodies in HIV-Seropositive and HIV-Seronegative Hemophiliacs
Roberto Conte, Laura Giovanardi, Pier Luigi Tazzari, Vincenzo De Rosa, Giuseppina Rodorigo, Maria Carla Re Servizio di Immunoematologia e Trasfusionale, Servizio di Angiologia e Malattie della Coagulazione e Istituto di Microbiologia dell’Universita, Policlinico S. Orsola, Bologna, Italia
Abstract. We tested serum samples from 1 1 HIV-seropositive and 32 HIV-seronegative Italian patients with hemophilia A or B for the presence of lymphocytotoxic antibodies (LCTAs). No patients had the acquired immune deficiency syndrome and all had received over many years heat-untreated commercial clotting factors. LCTAs directed mainly to B cells, were significantly present in 5/6 HIV-seropositive patients with hemophiliaA and in 5 / 5 HIV-seropositive patients with hemophilia B. The presence of LCTAs in HIV-seronegative hemophiliacs was signif- icantly correlated with both a decrease of Tcells and an increase in serum levels of IgG and IgM.
Introduction
Although lymphocytotoxic antibodies directed to non- HLA antigens have been reported in patients with the acquired immunodeficiency syndrome (AIDS) or lym- phadenopathy syndrome (LAS) [6, 22, 231, their inci- dence in the groups at increased risk for contracting AIDS has not yet been evaluated. As hemophiliacs use heat- untreated commercial clotting factors from large pools of donor plasma to prevent and control unexpected bleed- ing, they may be considered to be one of these groups. In fact there is undisputed evidence that human immunode- ficiency virus (HIV) - also known as HTLV-I11 or LAV - is etiologically associated with AIDS and can be transmit- ted by blood transfusion and blood products [ 131. More- over, abnormalities of cellular and humoral immunity similar to those found in patients with AIDS have been reported in asymptomatic HIV-seropositive hemophil- iacs [3, 5, 91.
The aims of this study were firstly to investigate non- HLA lymphocytotoxic antibodies (LCTAs) in HIV-sero- positive and HIV-seronegative hemophiliacs and sec- ondly to point out whether their presence in HIV-seroneg- ative hemophiliacs was related to alterations in Tcell subsets and in the serum level of the immunoglobulins IgG, IgA and IgM.
Materials and Methods
Patients Twenty-five patients with hemophiliaA and 18 with hemophil-
iaB attending the Bologna Hemophilia Center were studied. All patients included in the study had been treated over many years with heat-untreated lyophilized commercial factor VIII or prothrombin complex concentrates manufactured from large pools of plasma. None was known to be either a homosexual or an intravenous-drug abuser. No patient had a positive direct antiglobulin test a n d o r cold hemagglutinins.
Cvtotoxic Antibody Assay A modified microtiter NIH cytotoxicity assay was used at 15 and
37°C. Briefly, 1p1 of serum was incubated with 111 of the cell suspension in phosphate-buffered saline solution (2000 cells/pl) at 15 or 37 ‘C for 60 min: 5 p1 of rabbit complement was allowed to stand at 15 or 37’C for 120min.
The reading of the tests was performed by eosin staining of dead cells using an inverted phase-contrast microscope with a X 10 objec- tive. Before cytotoxicity assay, all sera were absorbed twice by plate- lets using 40X lo9 pooled platelets/ml of serum in order to remove class1 HLA antibodies. Sera tested in duplicate and in serial dilutions were classified as positive when reacted against allogeneic lympho- cytes from >_ 20% of the panel. Cytotoxicity was judged positive for a target cell when at least 50% of cells were killed. Target cells included: isolated T and B lymphocytes from a panel of 25 normal donors typed for HLA-A, B, C and DR specificities, lymphocytes bearing Bcell markers (B4, T I , B 1, Slg) from 20 HLA-typed patients with chronic lymphocytic leukemia and autologous unfractionated peripheral blood lymphocytes. Separated T and B lymphocytes from HLA-typed
48 Conte/Giovanardi/Tazzari/De Rosa/Rodorigo/Re
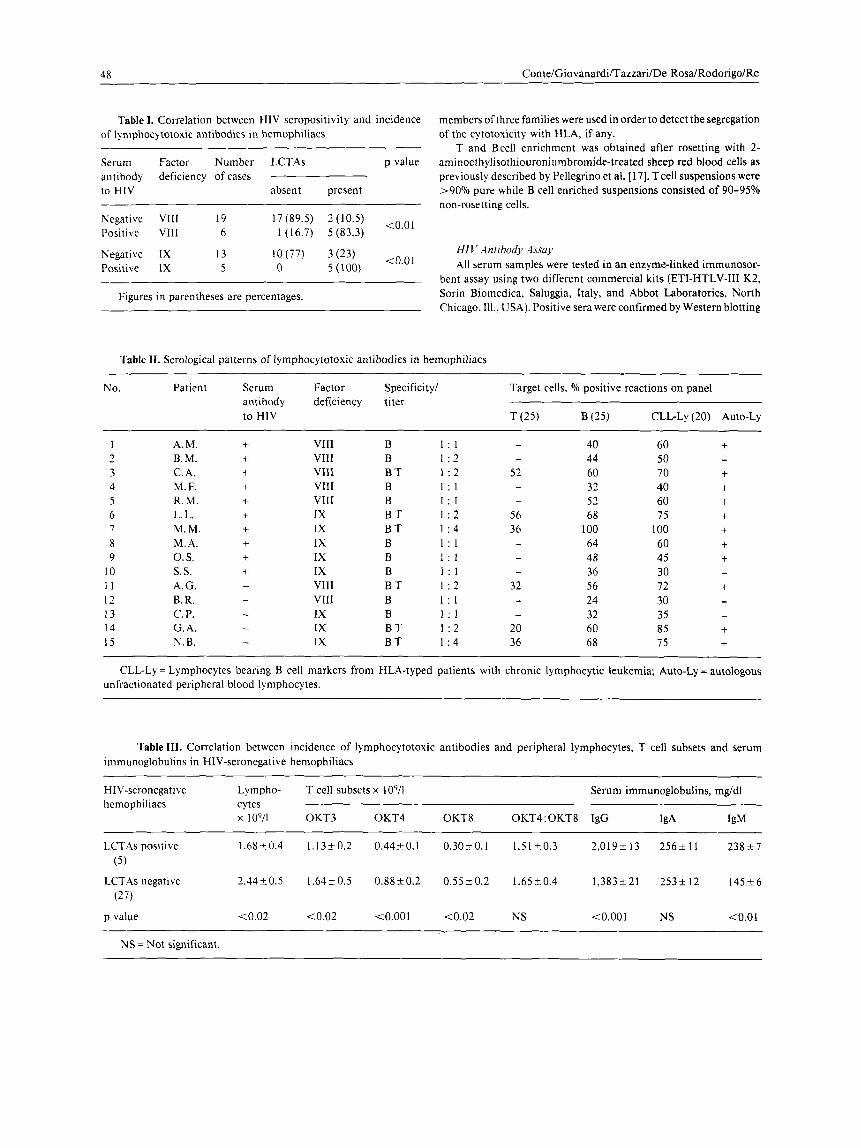
Table I. Correlation between HIV seropositivity and incidence of lymphocytotoxic antibodies in hemophiliacs
Serum Factor Number LCTAs p value antibody deficiency of cases to HIV absent present
t 0 . 0 1 Negative VIII 19 17(89.5) '(10.5) Positive VlII 6 I (16.7) 5 (83.3)
Negative IX 13 lO(77) 3(23) Positive IX 5 0 5(100)
Figures in parentheses are percentages.
members ofthree families were used in order to detect the segregation of the cytotoxicity with HLA, if any.
T and Bcell enrichment was obtained after rosetting with 2- aminoethylisothiouroniumbromide-treated sheep red blood cells as previously described by Pellegrino et a1. [ 171. Tcell suspensions were >90°/o pure while B cell enriched suspensions consisted of 90-95% non-rosetting cells.
H I V Antibody Assay All serum samples were tested in an enzyme-linked immunosor-
bent assay using two different commercial kits (ETI-HTLV-111 K2, Sorin Biomedica, Saluggia, Italy, and Abbot Laboratories, North Chicago, Ill., USA). Positive sera were confirmed by Western blotting
Table 11. Serological patterns of lymphocytotoxic antibodies in hemophiliacs
No. Patient Serum Factor Specificity/ Target cells, O/o positive reactions on panel antibody deficiency titer to HIV T (25) €3 (25) CLL-Ly (20) Auto-Ly
1 2 3 4 5 6 I 8 9
10 I I I2 13 14 15
A.M. B. M. C. A. M. F. R. M. L. L. M. M. M. A. 0. s. s. s. A. G. B. R. c. P. G. A. N. B.
+ + + + + + + + + + - - - - -
VIII VIII VIII VIII VIII IX IX IX IX IX VIII VIII IX IX IX
B 1 : l B 1 : 2 B T 1 : 2 B 1 : l B 1 : 1 B T 1 : 2 B T 1 . 4 B 1 : 1 B 1 : l B 1 : l B T 1 : 2 B 1 : 1 B 1 : l B T 1 : 2 B T 1 : 4
52
- 56 36 -
- 20 36
40 44 60 32 52 68
100 64 48 36 56 24 32 60 68
60 50 70 40 60 75
100 60 45 30 72 30 35 85 75
+ - f
+ + + + + f - +
~ ~ ~~~
CLL-Ly = Lymphocytes bearing B cell markers from HLA-typed patients with chronic lymphocytic leukemia, Auto-Ly = autologous unfractionated peripheral blood lymphocytes.
Table Il l . Correlation between incidence of lymphocytotoxic antibodies and peripheral lymphocytes, T cell subsets and serum immunoglobulins in HIV-seronegative hemophiliacs
HIV-seronegative Lympho- T cell subsets x lo9/] Serum immunoglobulins, mg/dl hemophiliacs cytes
x 10911 OKT3 OKT4 OKT8 OKT4: OKT8 IgG IgA IgM
LCTAs positive 1.68k0.4 1.13a0.2 0.4450.1 0.30i.O.l 1.51t0.3 2,019213 256k11 238a7
LCTAs negative 2.44k0.5 1.64t0.5 0.88k0.2 0.5520.2 1.65k0.4 1,383+21 253a12 145+6
(5)
(27)
p value <0.02 (0.02 <O.OOl <0.02 NS <O.OOl NS (0.01
NS = Not significant.

Non-HLA Lymphocytotoxic Antibodies in HIV-Seropositive and HIV-Seronegative Hemophiliacs 49
technique using both a commercial kit (Dupont Co., Speciality Diag- nostic, Wilmington, De., USA) and laboratory-prepared strips with purified detergent-lysed viral antigens (Sclavo, Siena, Italy). Seropos- itivity was defined as a reaction both with the 24-kilodalton and 41-kilodalton proteins of HIV.
Identification of T Cell Subsets Tcell subsets were assessed by indirect immunofluorescence anal-
ysis on a cytofluorimeter (Ortho Instruments, model SpectrumIII, Westwood, Mass., USA). We used monoclonal antibodies (Ortho, Raritan, N. J., USA) reactive to mature peripheral Tcells (OKT3) and Tcell subsets with helperhducer (OKT4) and suppressorlcytotoxic (OKT8) phenotypes, as previously described [2].
Iininunoglobulin Levels Levels of IgG, IgA and IgM were measured by radial immuno-
diffusion technique (Mancini) using Partigen plates (Behringwerke AG, Marburg, FRG)
Statistical Analysis The x2 test was used to determine the significance of the incidence
of lymphocytotoxic antibodies in HIV-seropositive and HIV-sero- negative hemophiliacs. For other comparisons, the statistical analysis was performed using Student's ttest.
Results
Frequency Table1 shows the incidence of LCTAs in HIV-serone-
gative and HIV-seropositive patients with hemophilia A or B. A significant incidence (p<O.O 1) of these antibodies was found in both groups of HIV-seropositive hemophil- iacs. In fact, in patients with hemophilia A, LCTAs were present in 5 out of 6HIV-seropositive and in 2 out of 19 HIV-seronegative, in patients with hemophilia B, they occurred in 5 out of 5HIV-seropositive and in 3 out of 13 HIV-seronegative. There was no correlation between LCTAs and HLA antigens (classes1 and 11) of hemophil- iacs or replacement therapy in the previous years or occurrence of antibodies against hepatitis B virus, cyto- megalovirus and Epstein-Barr virus (data not shown).
Serological Characteristics LCTAs were reactive only at 15 "C and were directed
mostly to B cells. They failed to recognize any defined HLA specificity and their titers were weak (1:l-1:4). As shown in tableII, it may be noted that there was no difference in serum reactivity between HIV-seropositive and HIV-seronegative patients, nor between the hemo- phi\iaA or B patients and that all sera were cytotoxic against 24- 100% of the unrelated panel of normal B lym- phocytes and against 30-1 00% of the lymphocyte panel from chronic lymphocytic leukemia patients.
When tested against normal T cells, only 6 sera dis- played alloreactivity. Moreover, the reactivity of LCTAs directed to both B and Tlymphocytes was wider on the B cell panel than on the T cell panel.
Family studies of serum reactivity against T and B cells were inconclusive for segregation with HLA, since cyto- toxicity did not correlate with HLA haplotypes (data not shown).
Autoreactivity against unfractionated peripheral blood lymphocytes was found in 11 out of 15 sera, pre- dominantly in those exhibiting larger allogeneic cytotox- icity.
Immunologic Relevance of LCTAs As shown in table 111, the presence of LCTAs in both
HIV-seronegative patients with hemophilia A or B was associated with some immunologic abnormalities. In fact, the hemophiliacs with these antibodies had a significant reduction in the absolute number of peripheral blood lymphocytes and OKT3+, OKT4+ and OKT8'cells (pt0.02) as compared with those without LCTAs, where- as there was no difference in the OKT4/OKT8 ratio. Furthermore, when LCTAs were present in the HIV- seronegative hemophiliacs, a significant increase in the serum levels of IgG and IgM (pt0.001 and p<O.O1 respectively) was also found.
Discussion
In the present study it was found that sera of HIV- seropositive hemophiliacs contain non-HLA-A, B, C and DR lymphocytotoxic antibodies reactive at 1 5 "C, di- rected principally against B cells and reacting mostly with the autologous lymphocytes. This finding confirms and extends several previous observations on the presence of multiple immunologic abnormalities in HIV-seropositive hemophiliacs eventually leading to a state where oppor- tunistic infections could supervene.
Antibodies reacting in the same way, the significance of which remains still unclear, have been previously reported in a large variety of diseases, including autoim- mune disorders, hematologic malignancies, viral infec- tions and also in less than 10% of healthy subjects [ 16, 181.
The clinical and prognostic significance of LCTAs in hemophiliacs, particularly in the HIV-seropositive ones, is unknown, although antibodies with similar serological char- acteristics have been found in sera from AIDS or LAS pa- tients. Moreover, it is worth pointing out that those HIV- seronegative hemophiliacs who developed LCTAs showed a

50 Conte/Giovanardi/Tazzari/De RosalRodorigoIRe
significant decrease in the absolute number of lymphocytes and T cells (OKT3+, OKT4' and OKT8+) besides a signifi- cant increase of IgG and IgM concentration.
However, since the development of AIDS seems to require an immunodeficient status besides HIV infection [7, 111, LCTAs might play a role in the onset of this syndrome. The effects, if any, of these antibodies on the lymphocytes - mostly B cells - in hemophiliacs are not clear. It is tempting to speculate that they may modify the surface characteristics of target lymphocytes removing them from the circulation or altering their functions. This could also be responsible, at least in part, for the B cell abnormalities found in healthy HIV-seropositive hemo- philiacs [4] and in patients with AIDS [I].
Anyway, at present it is not possible to elucidate wheth- er LCTAs are a prime etiological factor in immunologic abnormalities or if they are rather a secondary conse- quence of the immune system impairment, even if the latter possibility seems more likely. In fact immunologic abnormalities, uncorrelated with HIV antibody status, such as decreased helper/suppressor ratios, impaired response to mitogens, hypergammaglobulinemia [ 8, 1 4, 15, 19,201, impaired autologous mixed lymphocytes reac- tions [21] and deficient increase of natural killer cell response to interferonp and y [ 121, have been reported in hemophiliacs treated with commercial clotting factor con- centrates. These abnormalities are likely to result from repeated transfusion of commercial clotting concentrates and to represent the in vivo response to chronic exposure to foreign HLA proteins [ 101 and/or infectious agents.
Thus the presence of LCTAs in 10 out of 11 HIV seropositive hemophiliacs could suggest an immunologic impairment as well as, perhaps, represent a favoring con- dition for HIV infection.
In conclusion, our findings indicate that HIV-seropos- itive and HIV-seronegative hemophiliacs showing immu- nologic abnormalities can develop allo- or auto-LCTAs directed mainly to B cells. Although the clinical signifi- cance of these antibodies is unclear, we would like to suggest that their production could be related to a pro- found derangement of the immune system. Further stud- ies are needed in other high-risk groups for AIDS to understand and evaluate the relationship between LCTAs and HIV infection.
References
1 Amman, A.J.; Schiffman, G.; Abrams, D.; Volberding, P.; Zieg- ler. J.; Conant, M.: B-cell immunodeficiency in acquired immune deficiency syndrome. J. .4m. med. Ass. 251: 1447-1449 (1984).
2 Conte, R.; Tazzari, PL.; Finelli, C.: Deficiency of autologous
3
4
5
6
7
8
9
10
11
mixed lymphocyte reaction in patients with idiopathic autoim- mune hemolytic anemia. Vox Sang, 49: 285-291 (1985). Daniel, V.; Opelz, G.; Schafer, A.; Schimpf, KI.; Wendler, I.; Hunsmann. G.: Correlation of immune defects in hemophilia with HTLV-I11 antibody titers. Vox Sang. 51: 35-39 (1986). Giudizi, M. G.; Biagiotti, R.; Almerigogna, F.; Mazzetti, M.; Alessi. A,; Massai, G.; Longo, G.; Scano, G.; Morfini, M.; Romagnani, S.: HTLV-Ill seropositivity in symptom-free Italian haemophiliacs. Correlation with consumption of commercial concentrates and abnormalities of T and B lymphocytes. Scand. J. Haematol. 36: 198-202 (1986). Horsburgh, C. R.; Davis, K. C.; Hasiba, V.; Weiss, S . H.; Goedert, J . J.; Sarin, P.; Kirkpatrick, C. H.: Altered immunityin hemophil- ia correlates with the presence of antibody to human T-cell lymphotropic virus type111 (HTLV-111). J. clin. Immunol. 6: 37- 47 ( 1 986). Kloster. B. E.; Tomar, R.H.; Spira, T.J.: Lymphocytotoxic anti- bodies in the acquired immune deficiency syndrome (AIDS). Clin. Immunol. Immunopathol. 30: 330-335 (1 984). Lane, H. C.; Fauci, A. S.: Immunologic abnormalities in the acquired immunodeficiency syndrome. Annu. Rev. Immunol 3:
Lechner, K.; Niesser, H.; Bettelheim, P.; Deutsch, E.; Fasching, 1.; Fuhrmann, M.; Hinterberger, W.; Korninger, G.; Neumann, E.: Liszka, K. ; Knapp, W.; Mayr, W. R.; Sting], G.; Zeitlhuber, U .: T-cell alterations in hemophiliacs treated with commercial clotting factor concentrates. Thromb. Haemostasis 50: 552-556 ( 1 983). Ledermann, M. M.; Ratnoff, 0. D.; Scillian, J. J.; Jones, P. K.; Schacter, B.: Impaired cell-mediated immunity in patients with classic hemophilia. New Engl. J. Med. 308: 79-83 (1983). Lee, C. A.; Kernoff, P. B. A.; Karayiannis, P.; Waters, J.; Thomas, H. C.: Abnormal T-lymphocyte subsets in hemophilia/relation to HLA proteins in plasma products. New Engl. J. Med. 310: 1058 ( I 984). Madhok, R.; Gracia, A.; Follett, E.; Lowe, G. D.; Forbes, C. D.: Impaired in vivo cell-mediated immunity in hemophilia in the absence of HTLV-111 LAV infection. Ric. clin. Lab. 16: 173a
477-481 (1985).
(1986). 12 Matheson. D. S.; Green, B. J.; Poon, M. C.; Fritzler, M. J.; Hoar,
D. I.; Bowen, T. J.: Natural killer cell activity from hemophiliacs exhibits differential responses to various forms of interferon.
I3 Melief, C. J. M.; Goudsmit, J.: Transmission of lymphotropic retrovirus (HTLV-I and LAV/HTLV-111) by blood transfusion and blood products. Vox Sang. 50: 1-1 1 (1986).
14 Menitove, J.E.; Aster, R.H.; Casper, J.T.; Lauer, S.J.; Gott- schall, J. L.; Williams, J. E.; Gill, J. C.; Wheeler, D. V.; Piaskows- ki, V.; Kirchner, P.; Montgomery, R. R.: T-lymphocyte subpopu- lations in patients with classic hemophilia treated with cryopre- cipitate and lyophilized concentrates. New Engl. J. Med. 308:
15 Moffat, E. H. ; Blom, A. L.; Jones, J.; Matthews, N.; Newcombe, R. C.: A study of cell mediated and humoral immunity in haemo- philia and related disorders. Br. J. Haemat. 61: 157-167 ( 1 985).
I6 Ozturk, G.; Terasaki, P. I.: Non-HLA lymphocyte cytotoxins in various diseases. Tissue Antigens 14: 52-58 (1979).
I7 Pellegrino, M. A.; Ferrone, S.; Theofilopoulous, A. N.: Isolation
Blood 67: 164-167 (1986).
83-86 (1983).

Non-HLA Lymphocytotoxic Antibodies in HIV-Seropositive and HIV-Seronegative Hemophiliacs 51
18
19
20
21
of human T and B lymphocytes by rosette-formation with 2- amino-ethylisothiouroniumbromide (AET) treated sheep red blood cells and with monkey red blood cells. J. immunol. Meth- ods 11: 273-279 (1 976). Prou, 0.: Les lymphocytotoxines froides. Rev. fr. Transf. Immu- no-hkmatol. 22: 167-189 (1979). deShazo, R. D.; Andes, W. A. ; Nordberg, J.; Newton, J.; Daul, C.; Bozelka, B.: An immunologic evaluation of hemophiliac patients and their wives; relationship to the acquired immunodeficiency syndrome. Ann. intern. Med. 99. 159-164 (1983). deShazo, R.D.; Daul, C.; Andes, W.A.; Bozelka, B.: A longitu- dinal immunologic evaluation of hemophiliac patients. Blood 66:
Smolen, J. S.; Bettelheim, P.; Koller, U.; Ermler, D.; Graninger, W.; Knapp, W.; Lechner, K.: Defect in intracellular communica- tions in patients with hemophilia. Fed. Proc. 43: 663-667 ( 1 984).
22
23
993-998 (1 985).
Tomar, R. H.; John, P. A.; Hennig, A. K.; Kloster, B. E.: Cellular targets of antilymphocyte antibodies in AIDS and LAS. Clin. Immunol. Immunopathol. 37: 37-47 (1985). Williams, R. C.; Masur, H.; Spira, I. J.: Lymphocyte-reactive anti- bodies in acquired immune deficiency syndrome. J. clin. Immu- nol. 4. 1 18- 123 (1 984).
Received: May 5, 1987 Revised manuscript received July 10, 1987 Accepted: July 10, 1987
Dr. Roberto Conte Immunohaematology and Transfusion Service Policlinic San Orsola Via Massarenti 9 1-401 38 Bologna (Italy)