Embed Size (px)
Citation preview
Obesita’ Patologica:
l’intervento chirurgico
Prof.Francesco Domenico Capizziwww.chirgastrolaparomaggiore.it www.profcapizzi.it
CHIRURGIA GENERALEGASTROENTEROLOGICA E
LAPAROSCOPICAProf. F.D. Capizzi
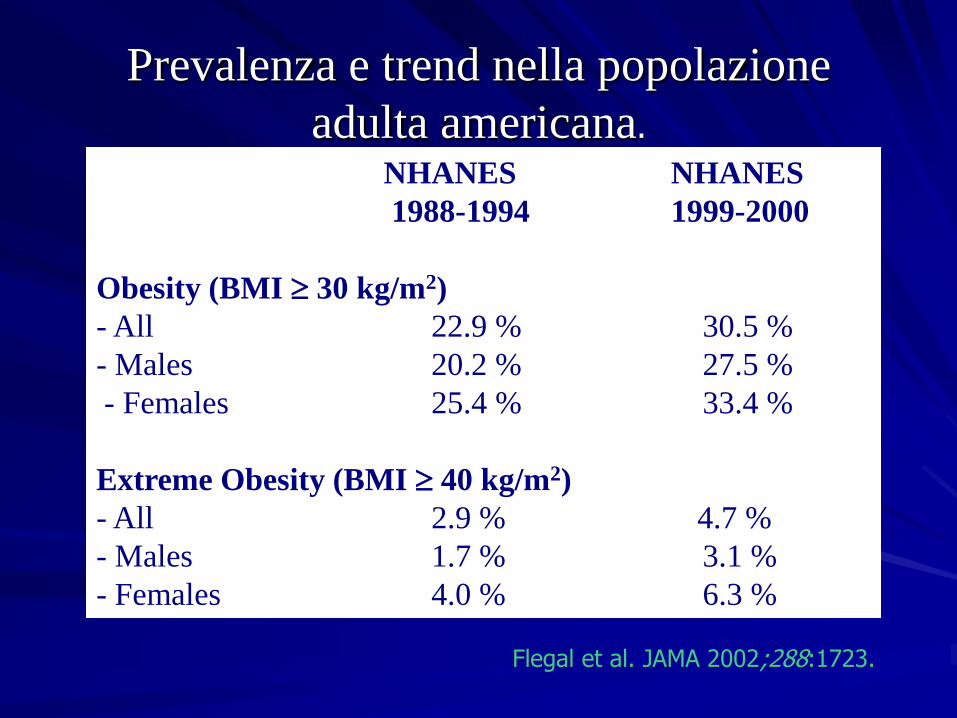
Prevalenza e trend nella popolazione
adulta americana.
Flegal et al. JAMA 2002;288:1723.
NHANES NHANES
1988-1994 1999-2000
Obesity (BMI 30 kg/m2)
- All 22.9 % 30.5 %
- Males 20.2 % 27.5 %
- Females 25.4 % 33.4 %
Extreme Obesity (BMI 40 kg/m2)
- All 2.9 % 4.7 %
- Males 1.7 % 3.1 %
- Females 4.0 % 6.3 %
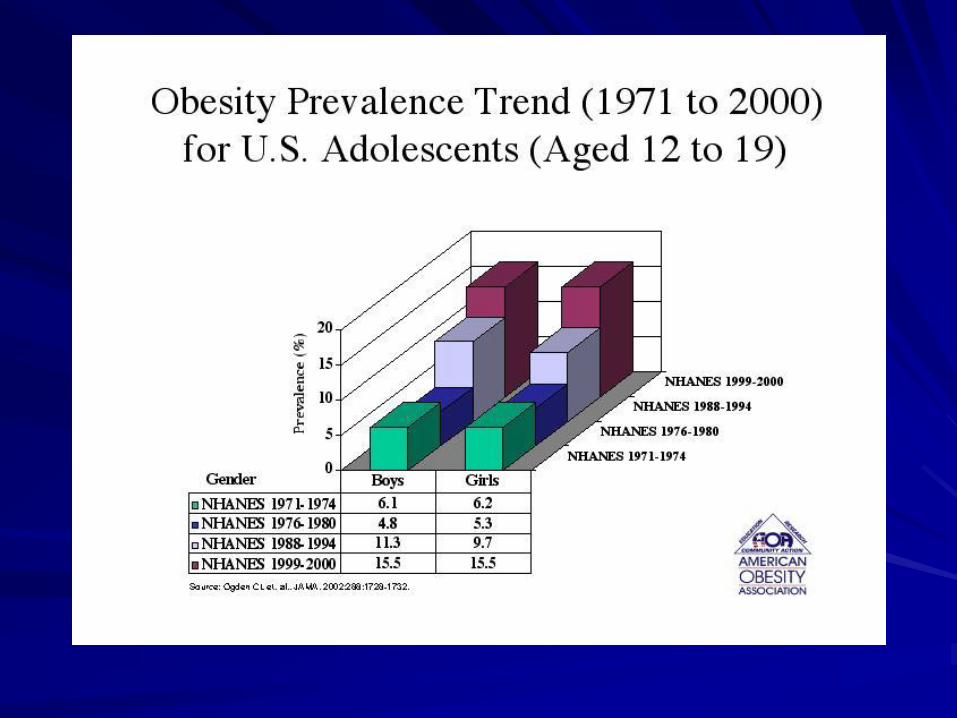
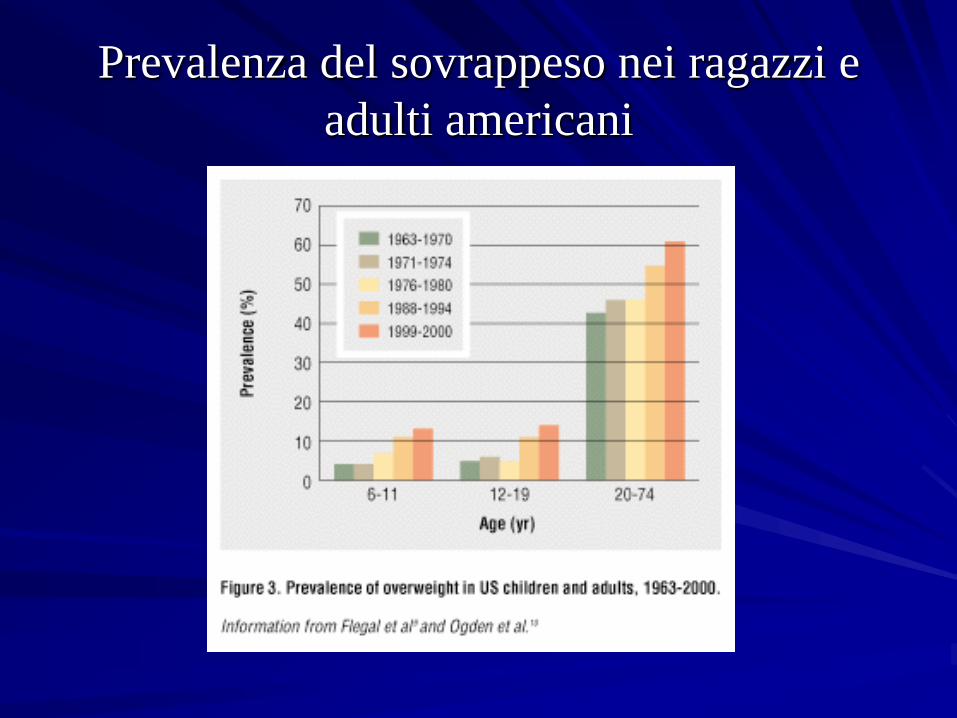
Prevalenza del sovrappeso nei ragazzi e
adulti americani
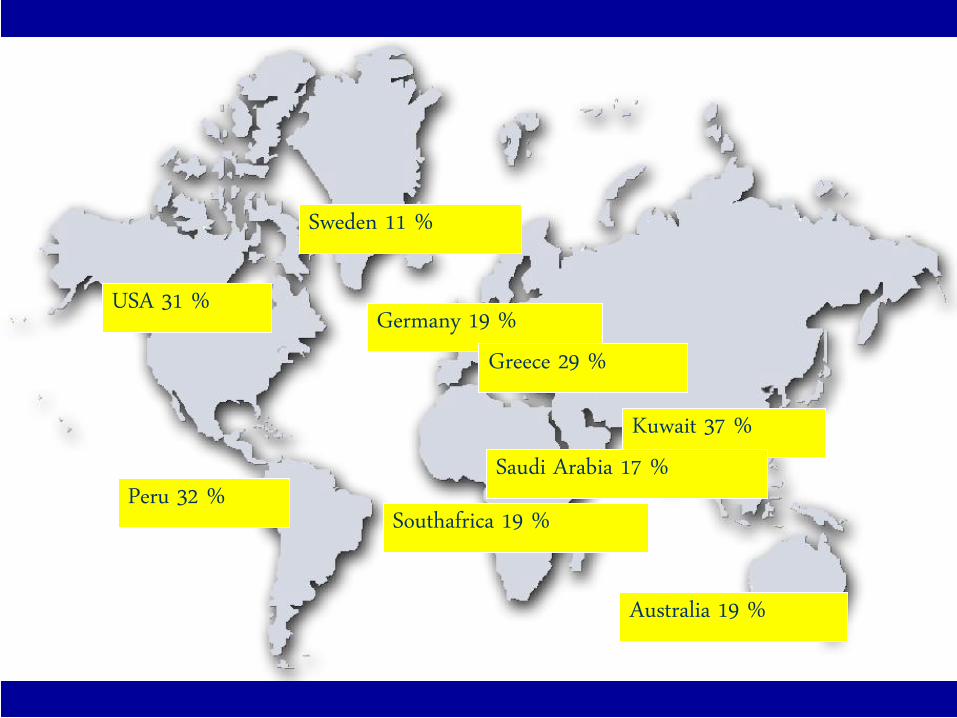
USA 31 %
Southafrica 19 %
Germany 19 %
Peru 32 %
Australia 19 %
Greece 29 %
Kuwait 37 %Saudi Arabia 17 %
Sweden 11 %
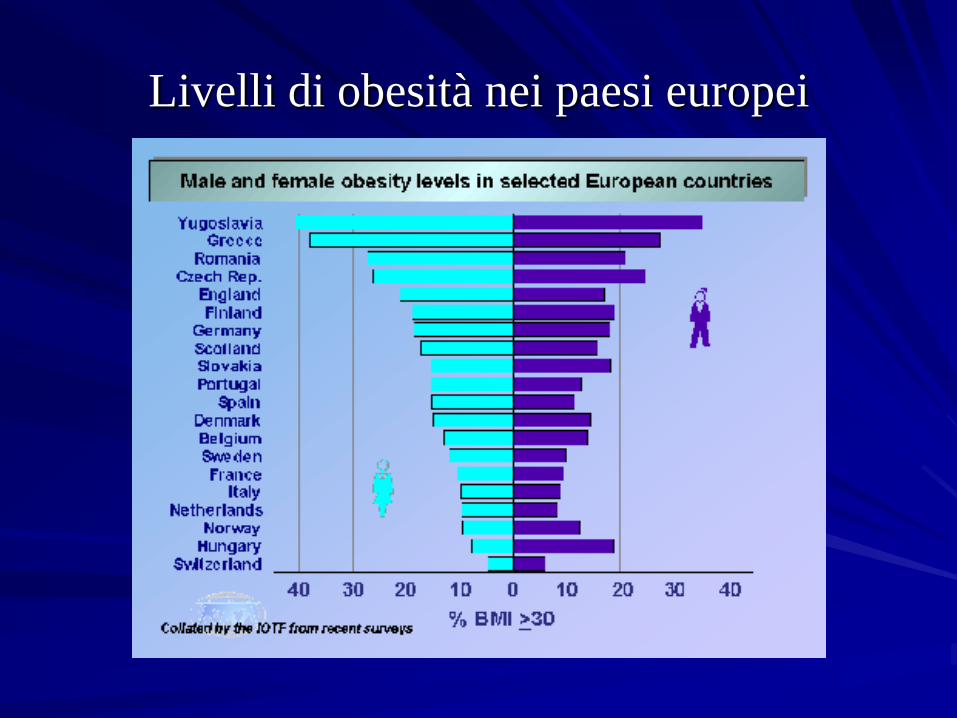
Livelli di obesità nei paesi europei
Obesità patologica in Italia
3millions7%
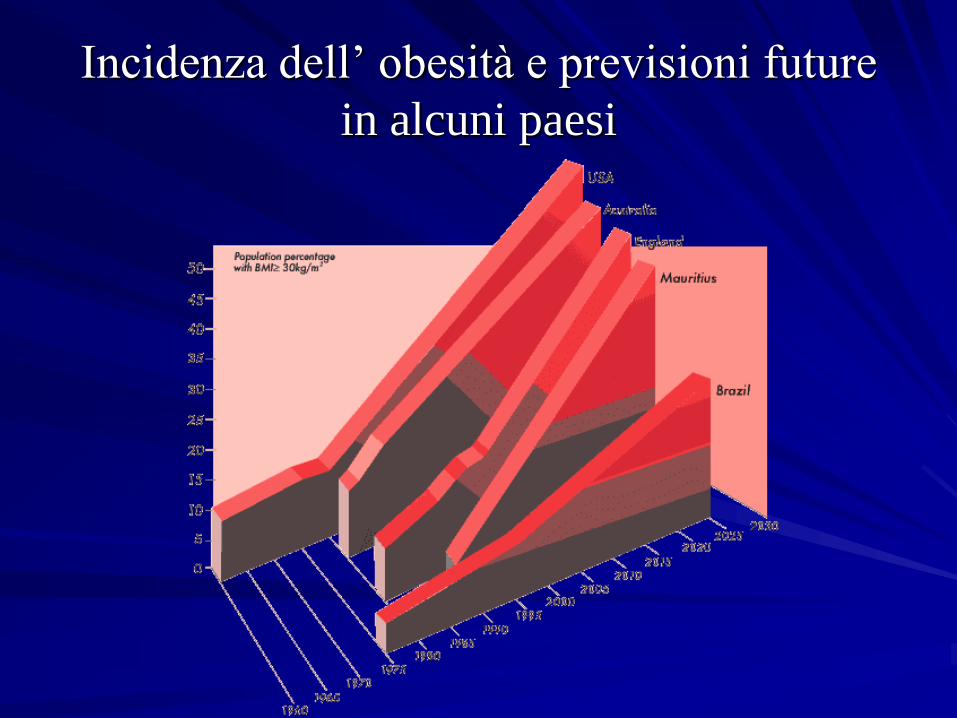
Incidenza dell’ obesità e previsioni future
in alcuni paesi
Comorbidità associate all‘obesità( Hell/Miller; Morbide Adipositas; ecomed, Landsberg 2000
237– 267)Hypertension
Cardiac Diseases
Dyslipemia
Diabetes (NIDD)
Sleepapnea
Osteoarthritis
Venous Stasis
Gastroesophageal Reflux
Cancer
…..
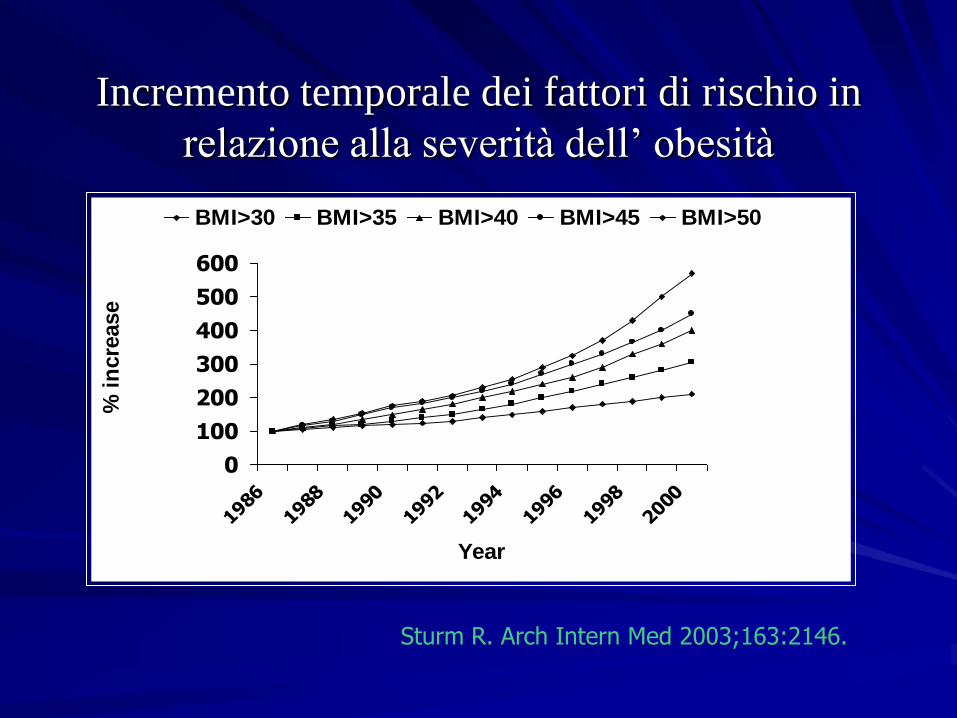
Incremento temporale dei fattori di rischio in
relazione alla severità dell’ obesità
0
100
200
300
400
500
600
1986
1988
1990
1992
1994
1996
1998
2000
Year
% i
ncre
ase
BMI>30 BMI>35 BMI>40 BMI>45 BMI>50
Sturm R. Arch Intern Med 2003;163:2146.
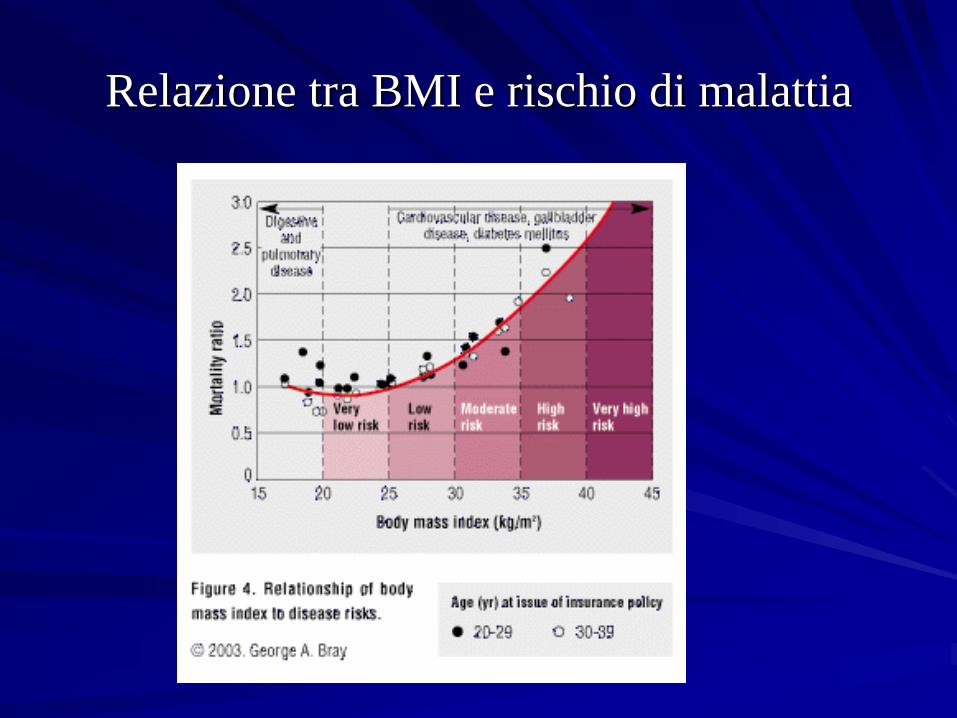
Relazione tra BMI e rischio di malattia
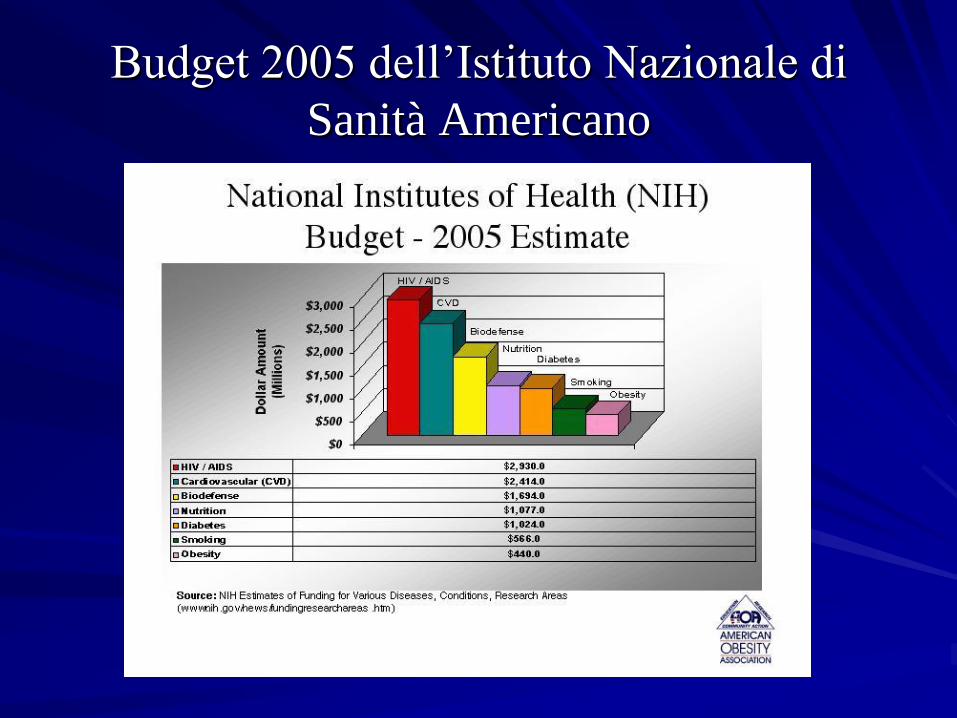
Budget 2005 dell’Istituto Nazionale di
Sanità Americano

Costi diretti ed indiretti dell’obesità
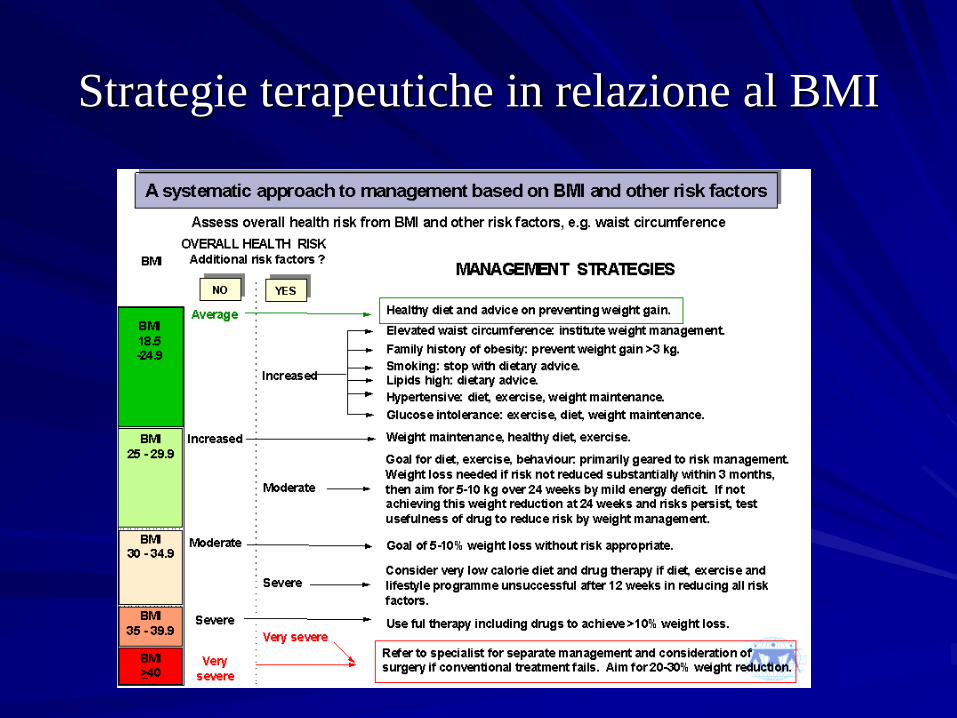
Strategie terapeutiche in relazione al BMI
Trattamento Medico
Ann Intern Med 1993
Oct 1;119:688-93
Treatment of obesity by moderate and severe
caloric restriction. Results of clinical research
trials.
Wadden TA
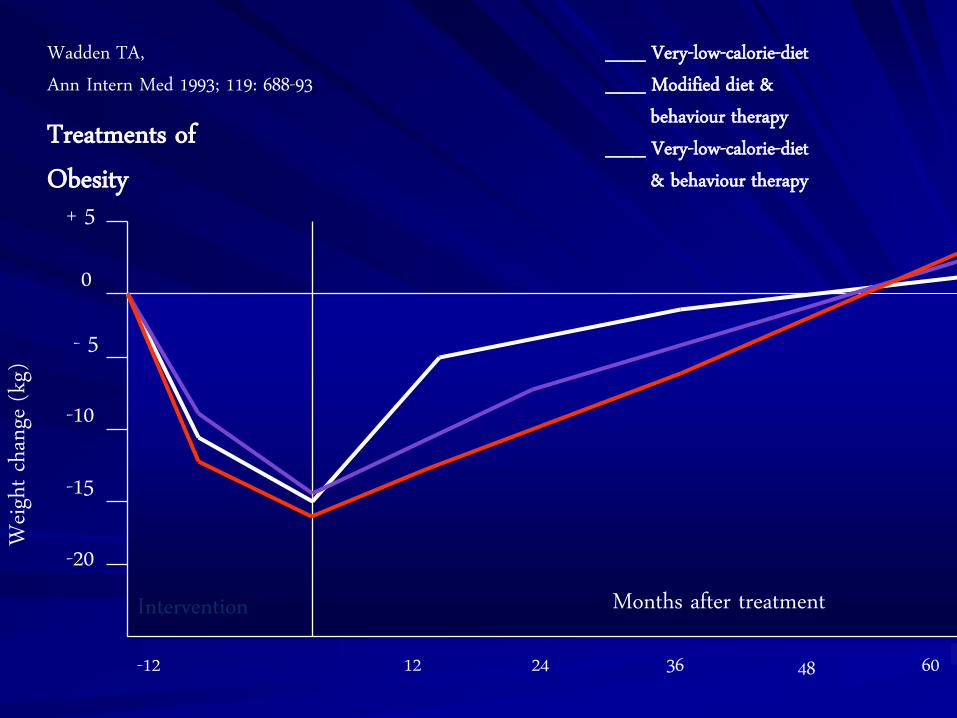
Treatments of Obesity
Wadden TA, Ann Intern Med 1993; 119: 688-93
Weig
ht cha
nge (
kg)
12 60483624
Months after treatment
- 5
-10
-15
-20
+ 5
0
___ Very-low-calorie-diet___ Modified diet &
behaviour therapy___ Very-low-calorie-diet
& behaviour therapy
-12
Intervention
Pharmacotherapy for obesity: a
quantitative analysis of four
decades of published
randomized clinical trials. Haddock CK et al. International Journal of Obesity (2002)
26, 262-273
No drug, or class of drug,demonstrated clear superiorityas an obesity medication.

Supportato da:NIH (National Institutes of Health)
Consensus Development Conference Statement, 1991
IFSO International Federation for the Surgery of Obesity www.obesity-online.com/IFSO
ASBS American Society for Bariatric Surgery
SAGES Society of American Gastrointestinal Endoscopic Surgeons
BMI 25 - 29,9 Overweight
BMI 30 - 34,9 Grade I Obesity
BMI 35 - 39,9 Grade II Obesity
BMI > 40 Grade III Morbid Obesity
BMI > 50 Grade IV Super Obesity
surg
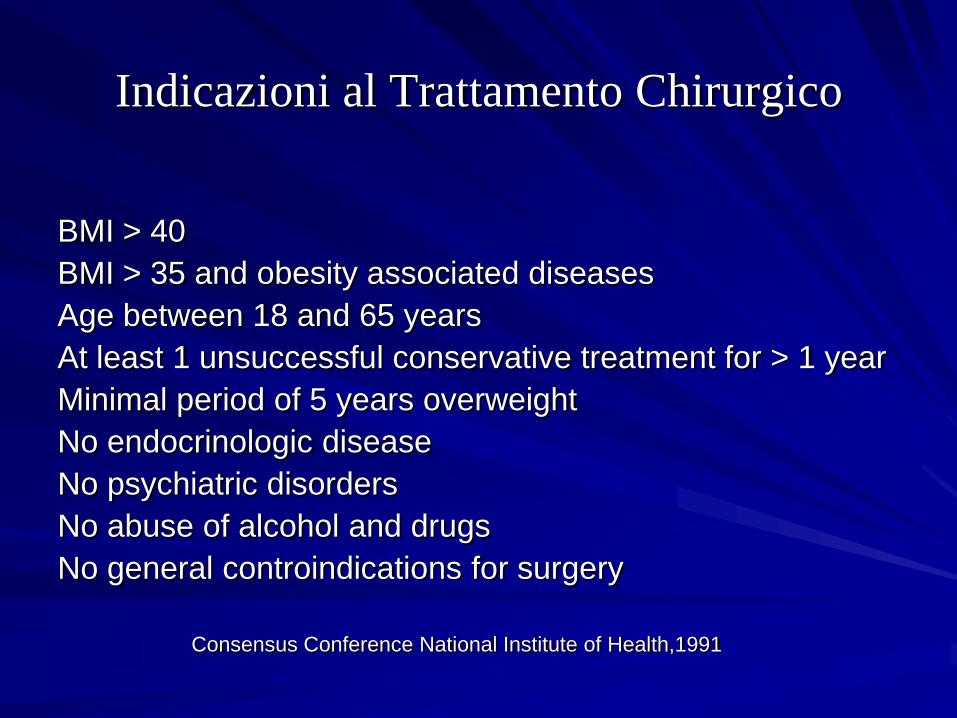
Indicazioni al Trattamento Chirurgico
BMI > 40
BMI > 35 and obesity associated diseases
Age between 18 and 65 years
At least 1 unsuccessful conservative treatment for > 1 year
Minimal period of 5 years overweight
No endocrinologic disease
No psychiatric disorders
No abuse of alcohol and drugs
No general controindications for surgery
Consensus Conference National Institute of Health,1991
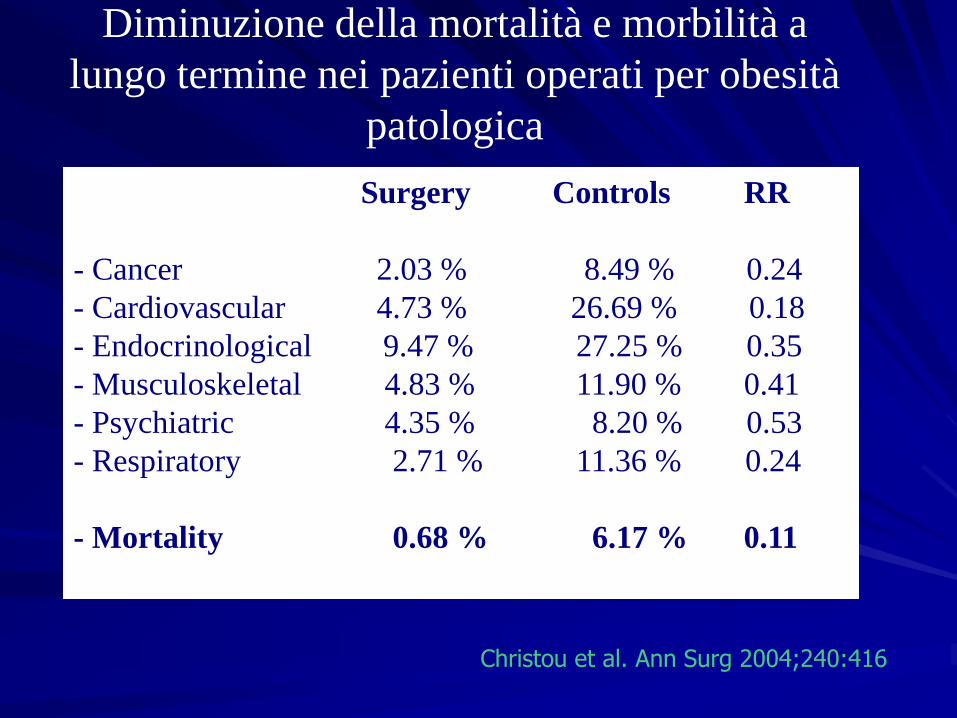
Surgery Controls RR
- Cancer 2.03 % 8.49 % 0.24
- Cardiovascular 4.73 % 26.69 % 0.18
- Endocrinological 9.47 % 27.25 % 0.35
- Musculoskeletal 4.83 % 11.90 % 0.41
- Psychiatric 4.35 % 8.20 % 0.53
- Respiratory 2.71 % 11.36 % 0.24
- Mortality 0.68 % 6.17 % 0.11
Diminuzione della mortalità e morbilità a
lungo termine nei pazienti operati per obesità
patologica
Christou et al. Ann Surg 2004;240:416
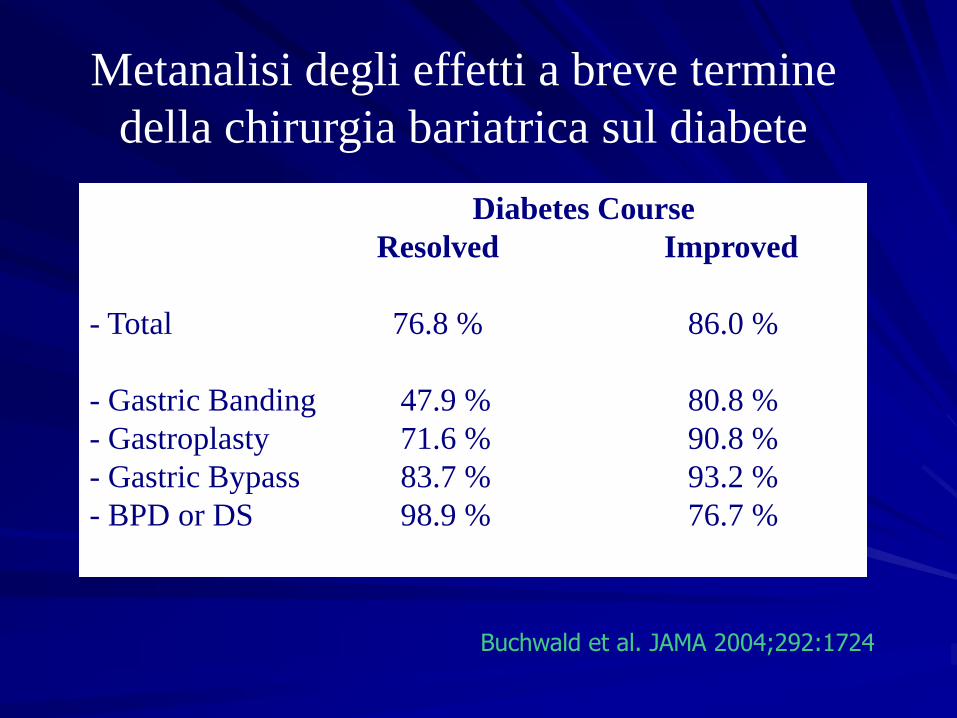
Diabetes Course
Resolved Improved
- Total 76.8 % 86.0 %
- Gastric Banding 47.9 % 80.8 %
- Gastroplasty 71.6 % 90.8 %
- Gastric Bypass 83.7 % 93.2 %
- BPD or DS 98.9 % 76.7 %
Metanalisi degli effetti a breve termine
della chirurgia bariatrica sul diabete
Buchwald et al. JAMA 2004;292:1724
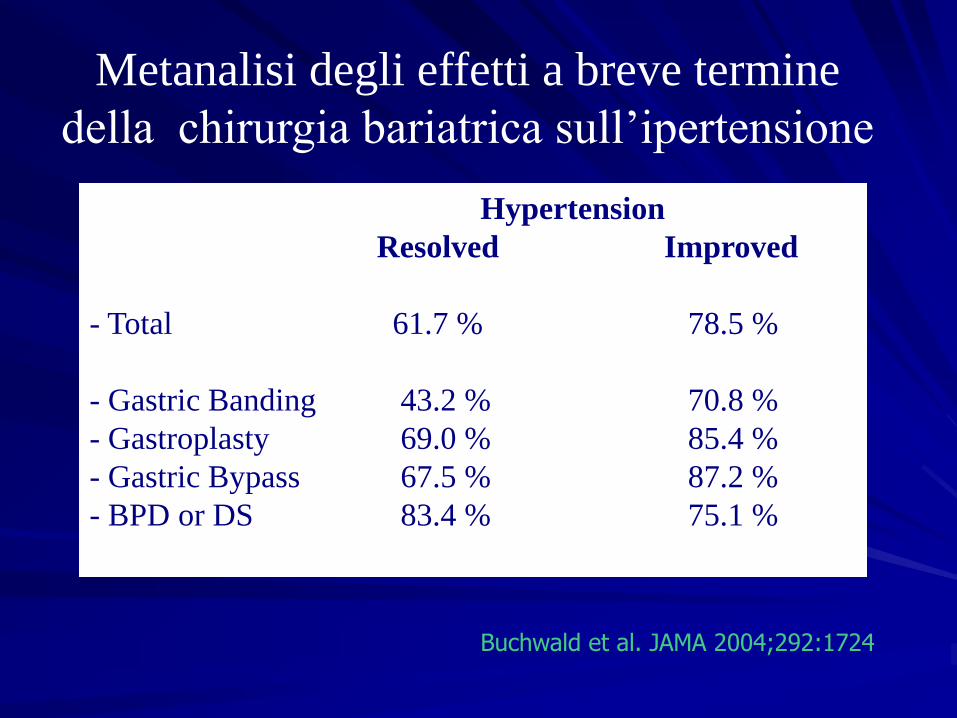
Hypertension
Resolved Improved
- Total 61.7 % 78.5 %
- Gastric Banding 43.2 % 70.8 %
- Gastroplasty 69.0 % 85.4 %
- Gastric Bypass 67.5 % 87.2 %
- BPD or DS 83.4 % 75.1 %
Metanalisi degli effetti a breve termine
della chirurgia bariatrica sull’ipertensione
Buchwald et al. JAMA 2004;292:1724
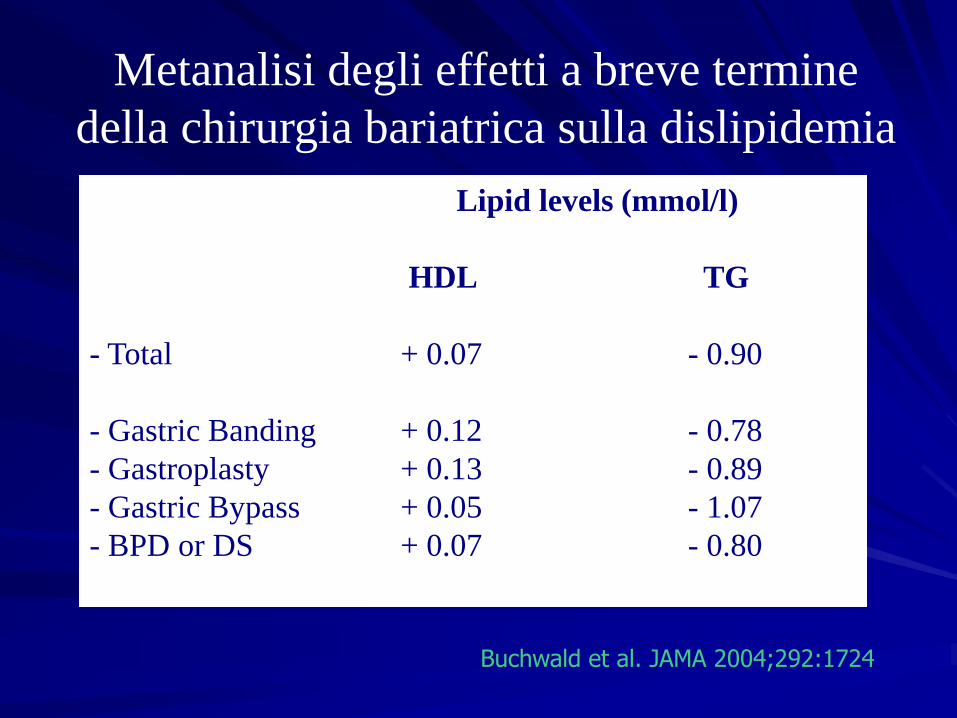
Lipid levels (mmol/l)
HDL TG
- Total + 0.07 - 0.90
- Gastric Banding + 0.12 - 0.78
- Gastroplasty + 0.13 - 0.89
- Gastric Bypass + 0.05 - 1.07
- BPD or DS + 0.07 - 0.80
Metanalisi degli effetti a breve termine
della chirurgia bariatrica sulla dislipidemia
Buchwald et al. JAMA 2004;292:1724
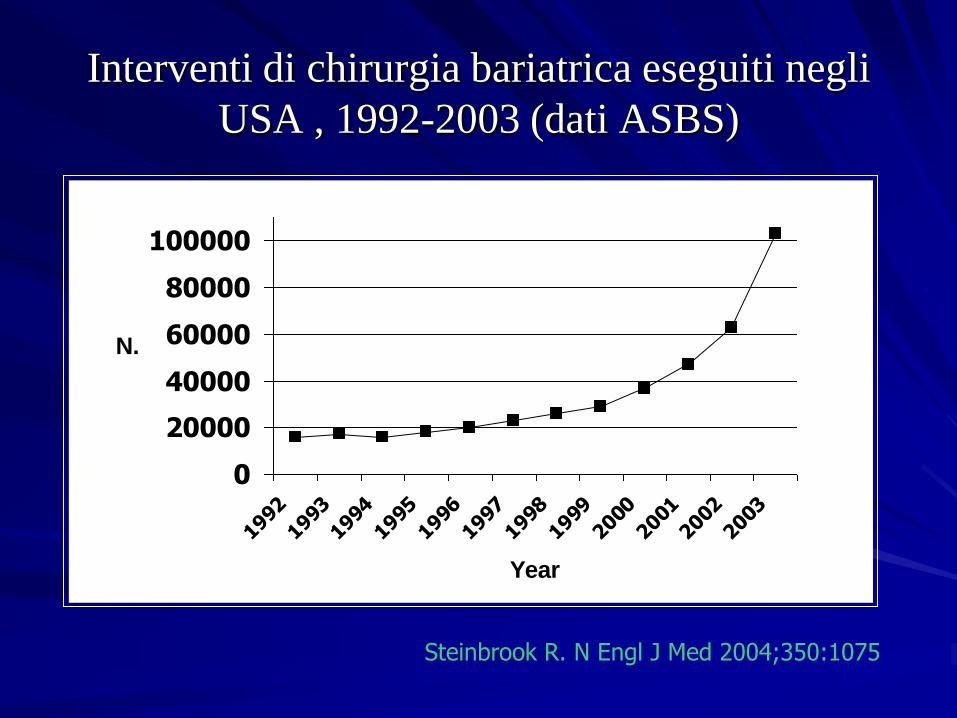
Interventi di chirurgia bariatrica eseguiti negli
USA , 1992-2003 (dati ASBS)
0
20000
40000
60000
80000
100000
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
Year
N.
Steinbrook R. N Engl J Med 2004;350:1075.
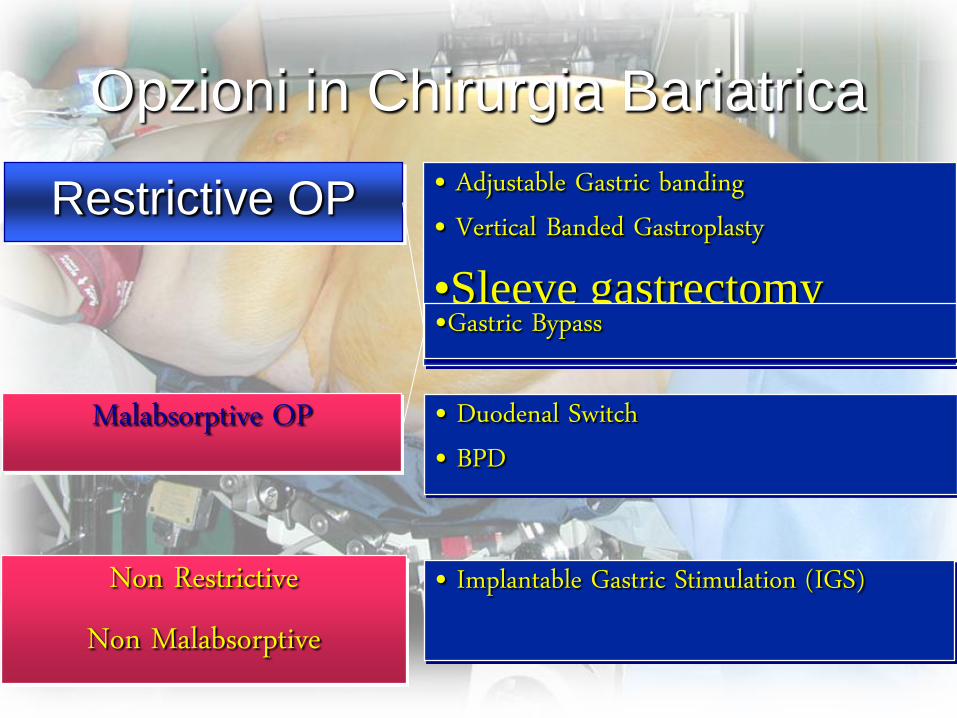
Opzioni in Chirurgia Bariatrica
• Duodenal Switch• BPD
• Adjustable Gastric banding• Vertical Banded Gastroplasty
•Sleeve gastrectomy
Restrictive OP
Malabsorptive OP
Non Restrictive Non Malabsorptive
• Implantable Gastric Stimulation (IGS)
•Gastric Bypass
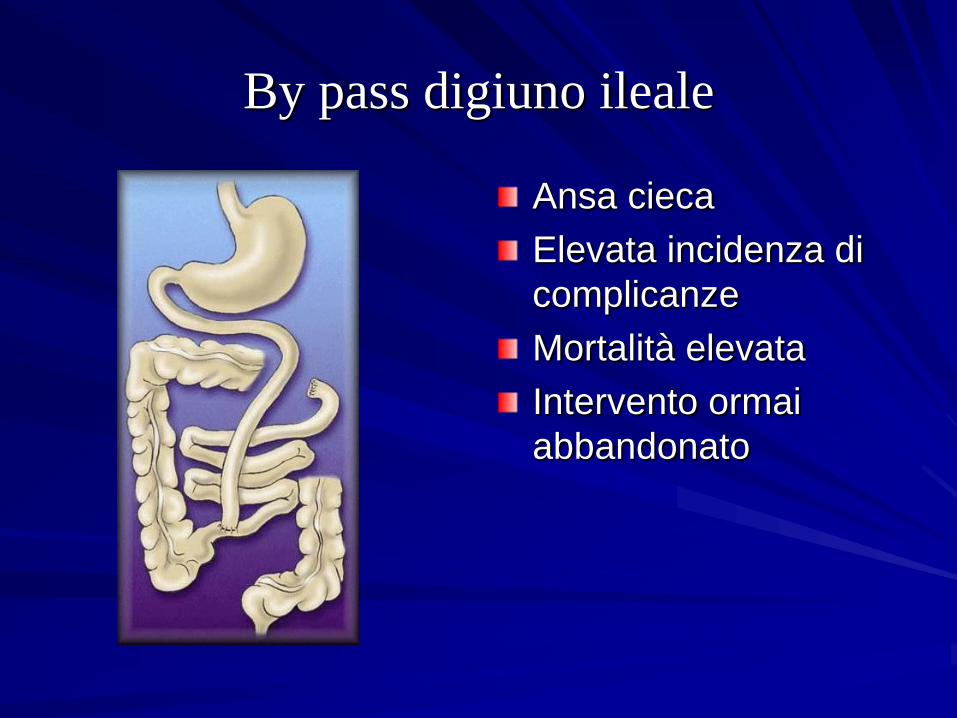
By pass digiuno ileale
Ansa cieca
Elevata incidenza di
complicanze
Mortalità elevata
Intervento ormai
abbandonato

By pass bilio intestinale
Intervento
malassorbitivo
Ansa anastomizzata
alla colecisti
Complicanze
metaboliche
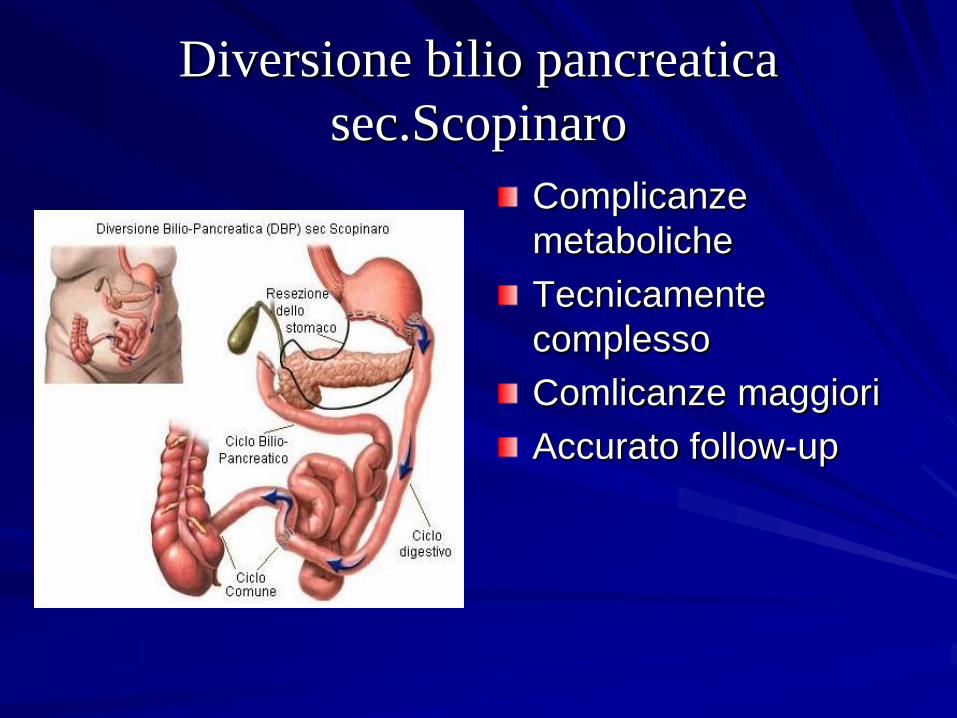
Diversione bilio pancreatica
sec.Scopinaro
Complicanze
metaboliche
Tecnicamente
complesso
Comlicanze maggiori
Accurato follow-up
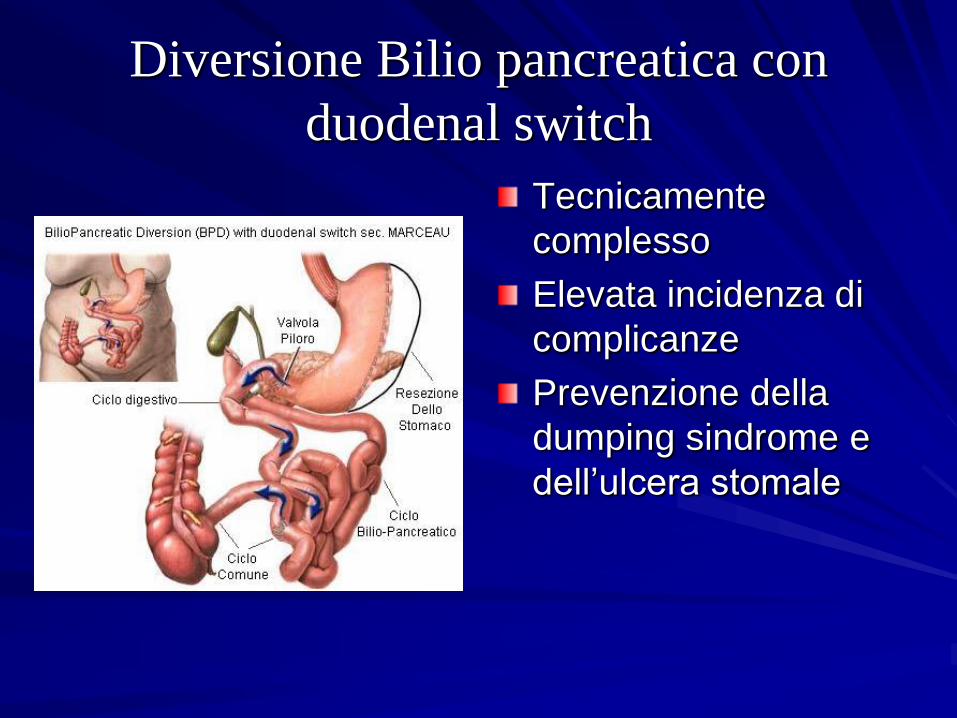
Diversione Bilio pancreatica con
duodenal switch
Tecnicamente
complesso
Elevata incidenza di
complicanze
Prevenzione della
dumping sindrome e
dell’ulcera stomale
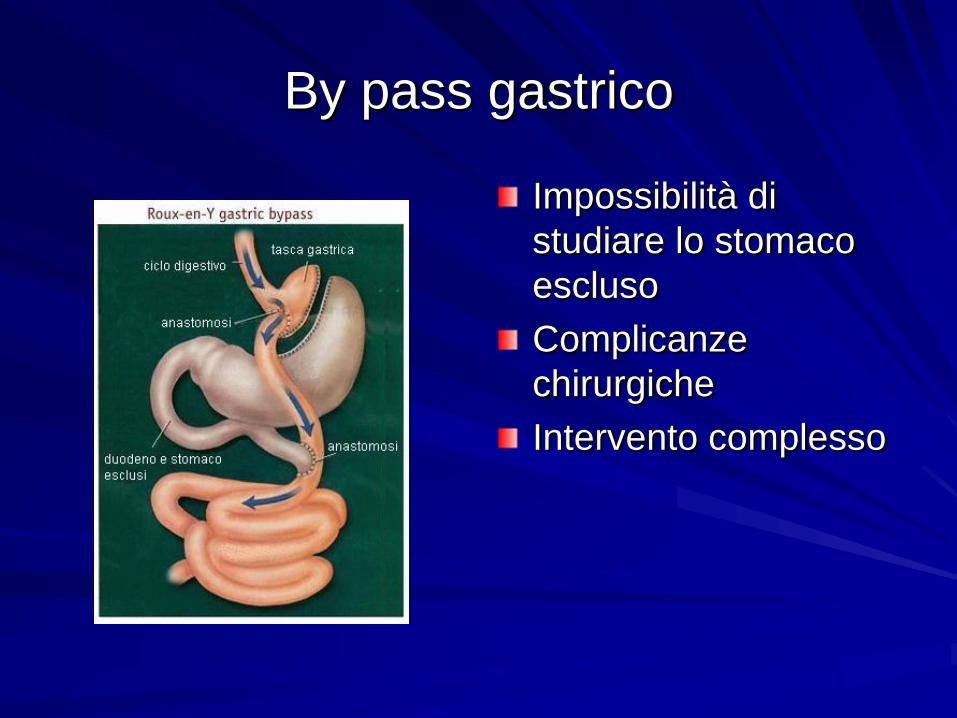
By pass gastrico
Impossibilità di
studiare lo stomaco
escluso
Complicanze
chirurgiche
Intervento complesso

Gastroplastica verticale sec. Mason
Parzialmente
reversibile
Compliance del
Paziente
Possibile deiscenza
della sutura gastrica
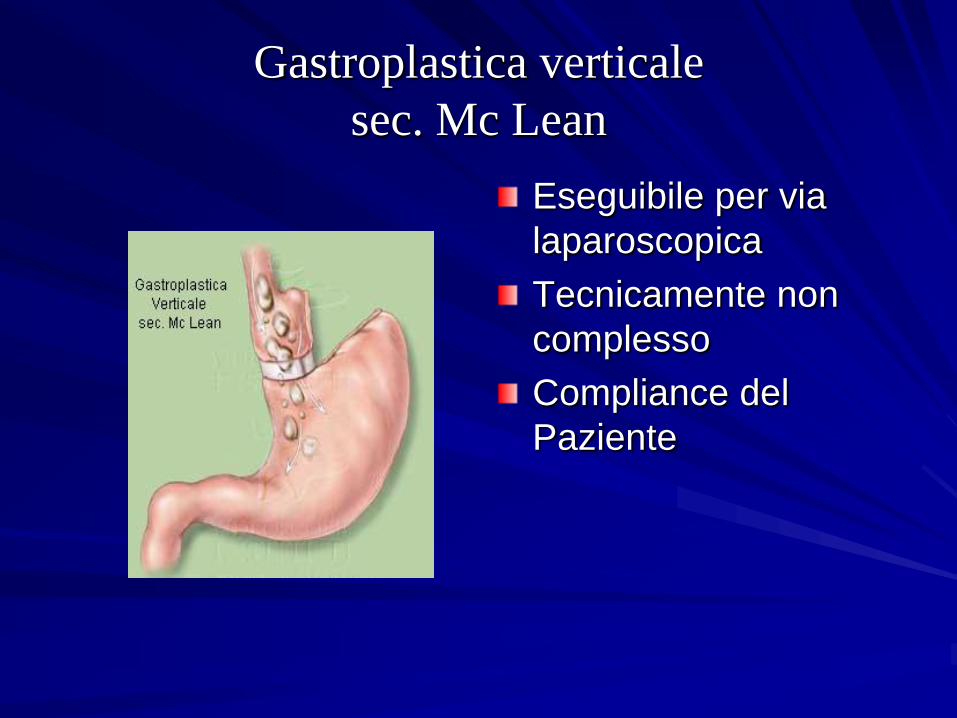
Gastroplastica verticale
sec. Mc Lean
Eseguibile per via
laparoscopica
Tecnicamente non
complesso
Compliance del
Paziente

Banding Gastrico
Semplice esecuzione
Reversibile
Complicanze:slippage
e dilatazione tasca
Buona compliance del
Paziente

Banding esofago-gastrico
Regolabile e
reversibile
Assenza di tasca
Minima complicanze
lievi
Buona compliance del
Paziente
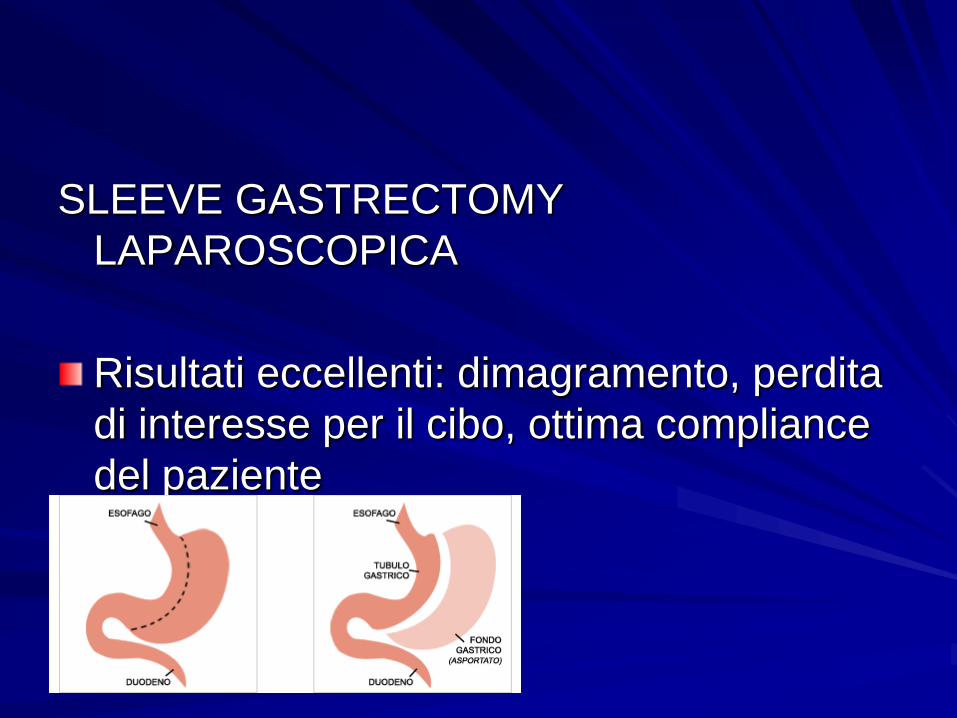
SLEEVE GASTRECTOMY
LAPAROSCOPICA
Risultati eccellenti: dimagramento, perdita
di interesse per il cibo, ottima compliance
del paziente
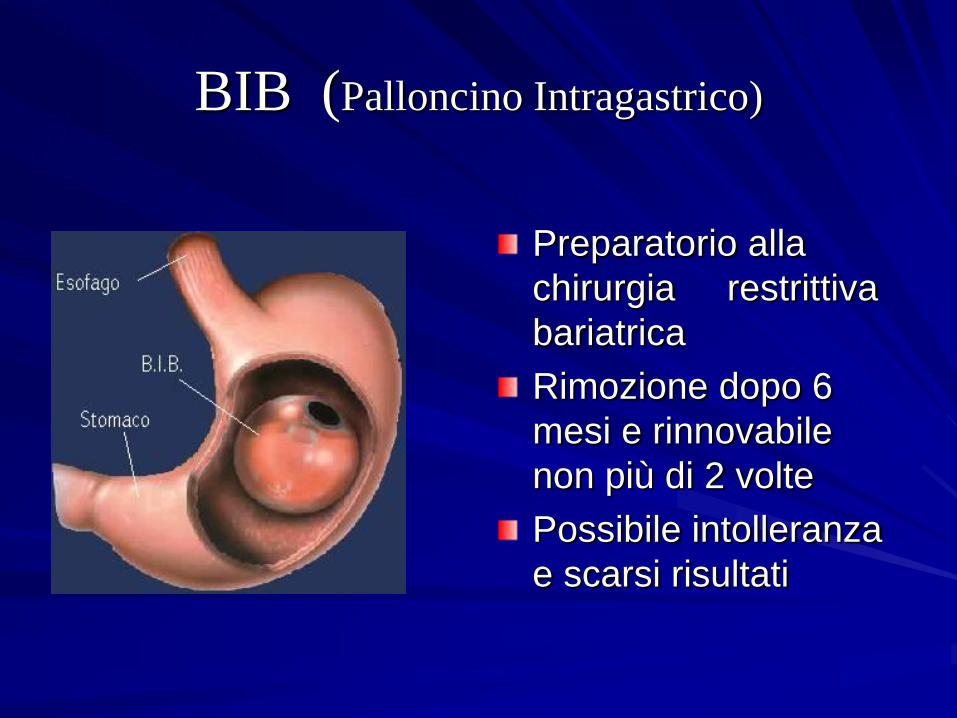
BIB (Palloncino Intragastrico)
Preparatorio alla
chirurgia restrittiva
bariatrica
Rimozione dopo 6
mesi e rinnovabile
non più di 2 volte
Possibile intolleranza
e scarsi risultati
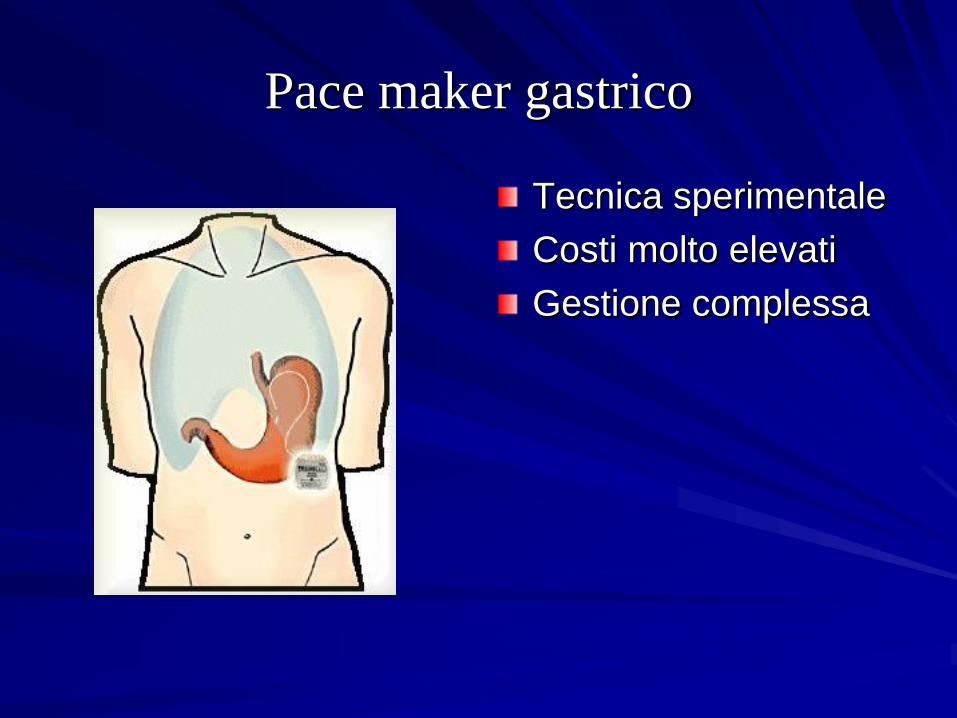
Pace maker gastrico
Tecnica sperimentale
Costi molto elevati
Gestione complessa
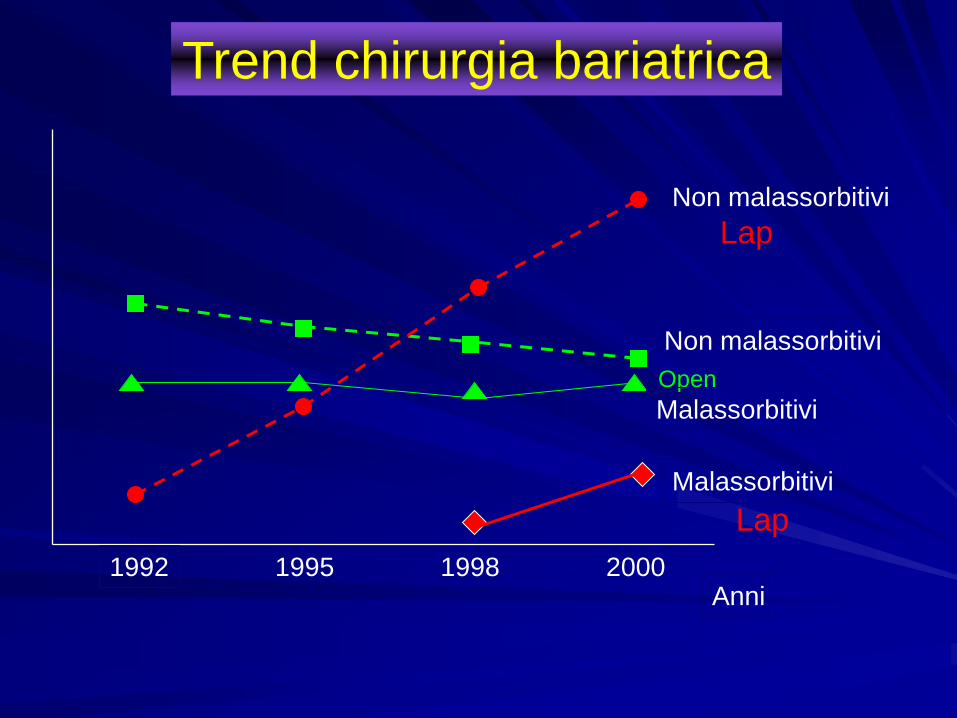
1992 1995 1998 2000Anni
Lap
Open
Non malassorbitivi
Malassorbitivi
Non malassorbitivi
Malassorbitivi
Lap
Trend chirurgia bariatrica
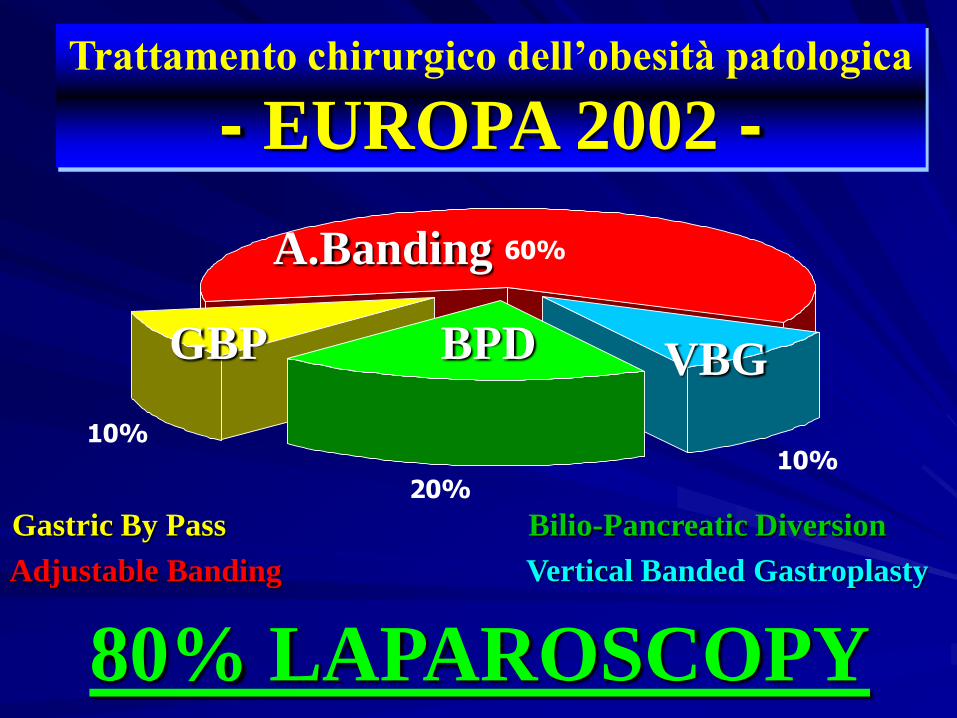
10%
20%10%
60%
Trattamento chirurgico dell’obesità patologica
- EUROPA 2002 -
80% LAPAROSCOPY
BPDGBP VBG
A.Banding
Gastric By Pass Bilio-Pancreatic Diversion
Vertical Banded GastroplastyAdjustable Banding
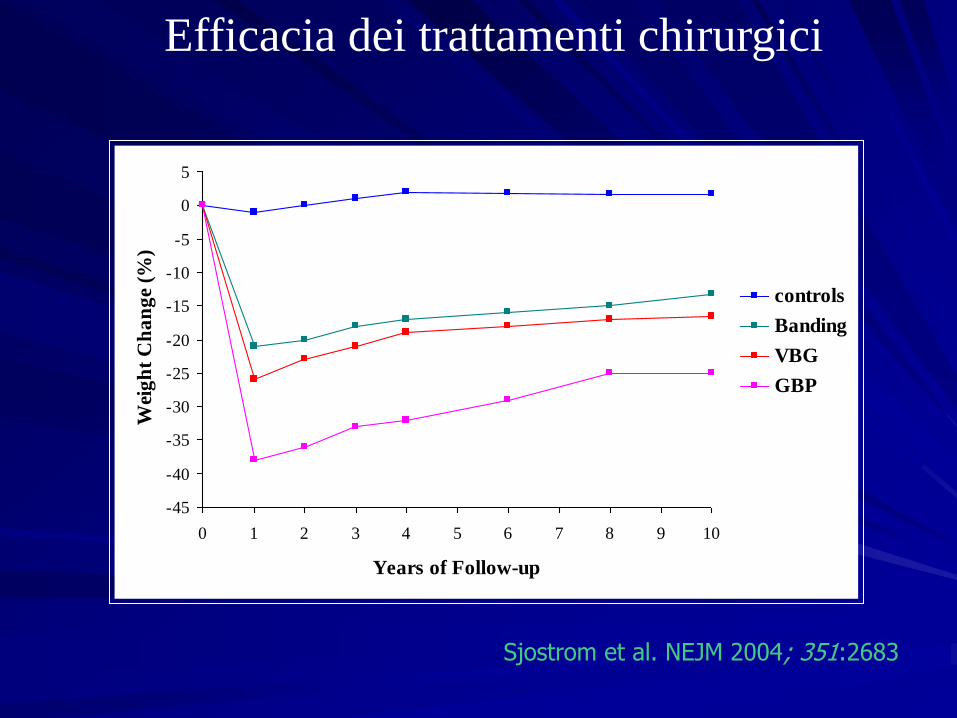
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
5
0 1 2 3 4 5 6 7 8 9 10
Years of Follow-up
Wei
gh
t C
ha
ng
e (%
)
controls
Banding
VBG
GBP
Efficacia dei trattamenti chirurgici
Sjostrom et al. NEJM 2004; 351:2683
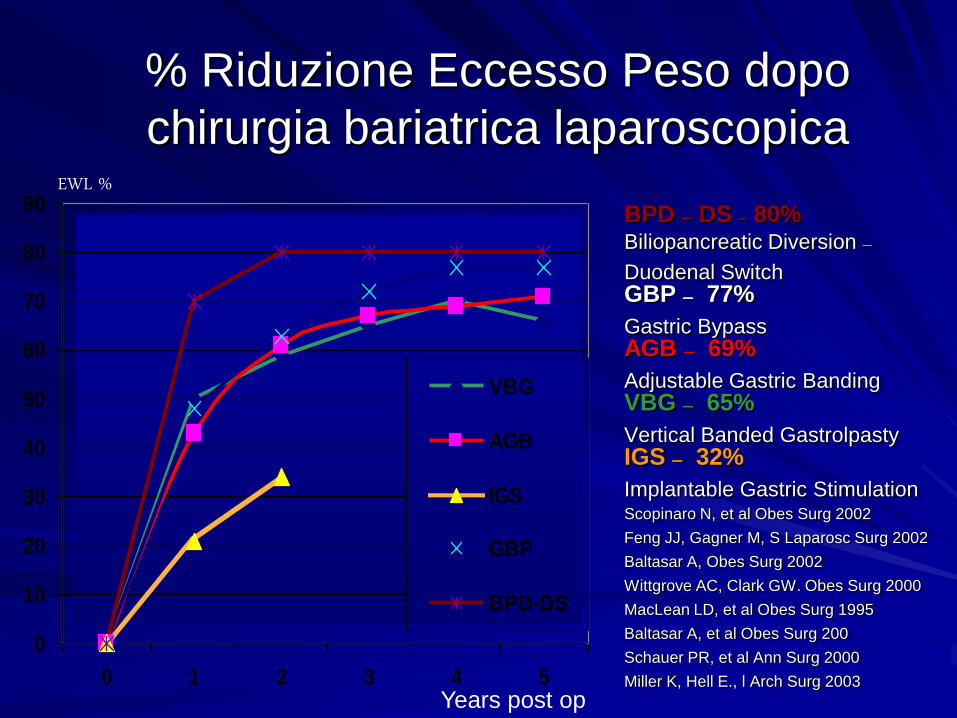
0
10
20
30
40
50
60
70
80
90
0 1 2 3 4 5
VBG
AGB
IGS
GBP
BPD-DS
EWL %
Years post op
% Riduzione Eccesso Peso dopo
chirurgia bariatrica laparoscopica
BPD – DS – 80%Biliopancreatic Diversion –Duodenal SwitchGBP – 77%
Gastric BypassAGB – 69%
Adjustable Gastric BandingVBG – 65%
Vertical Banded GastrolpastyIGS – 32%
Implantable Gastric StimulationScopinaro N, et al Obes Surg 2002
Feng JJ, Gagner M, S Laparosc Surg 2002
Baltasar A, Obes Surg 2002
Wittgrove AC, Clark GW. Obes Surg 2000
MacLean LD, et al Obes Surg 1995
Baltasar A, et al Obes Surg 200
Schauer PR, et al Ann Surg 2000
Miller K, Hell E., l Arch Surg 2003
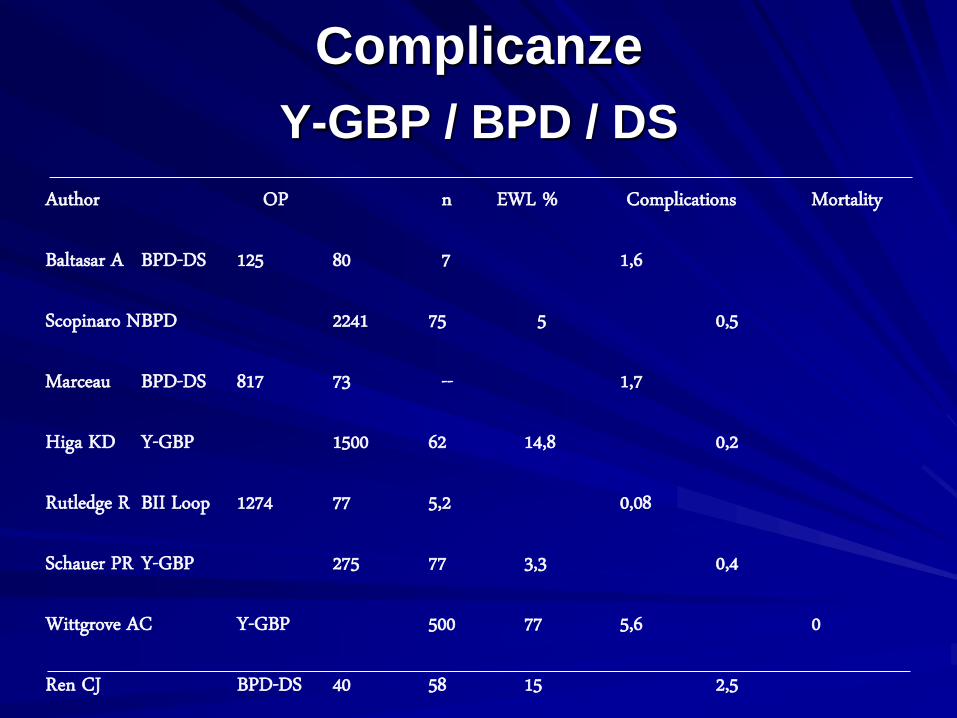
Author OP n EWL % Complications Mortality
Baltasar A BPD-DS 125 80 7 1,6
Scopinaro NBPD 2241 75 5 0,5
Marceau BPD-DS 817 73 -- 1,7
Higa KD Y-GBP 1500 62 14,8 0,2
Rutledge R BII Loop 1274 77 5,2 0,08
Schauer PR Y-GBP 275 77 3,3 0,4
Wittgrove AC Y-GBP 500 77 5,6 0
Ren CJ BPD-DS 40 58 15 2,5
Complicanze
Y-GBP / BPD / DS
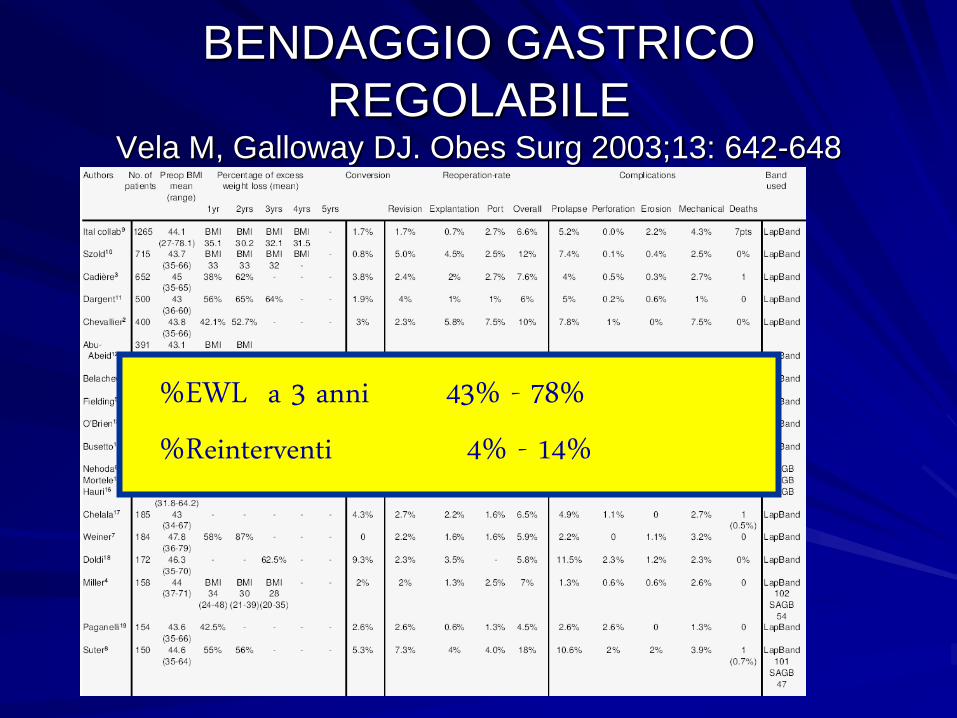
BENDAGGIO GASTRICO
REGOLABILEVela M, Galloway DJ. Obes Surg 2003;13: 642-648
%EWL a 3 anni 43% - 78%%Reinterventi 4% - 14%
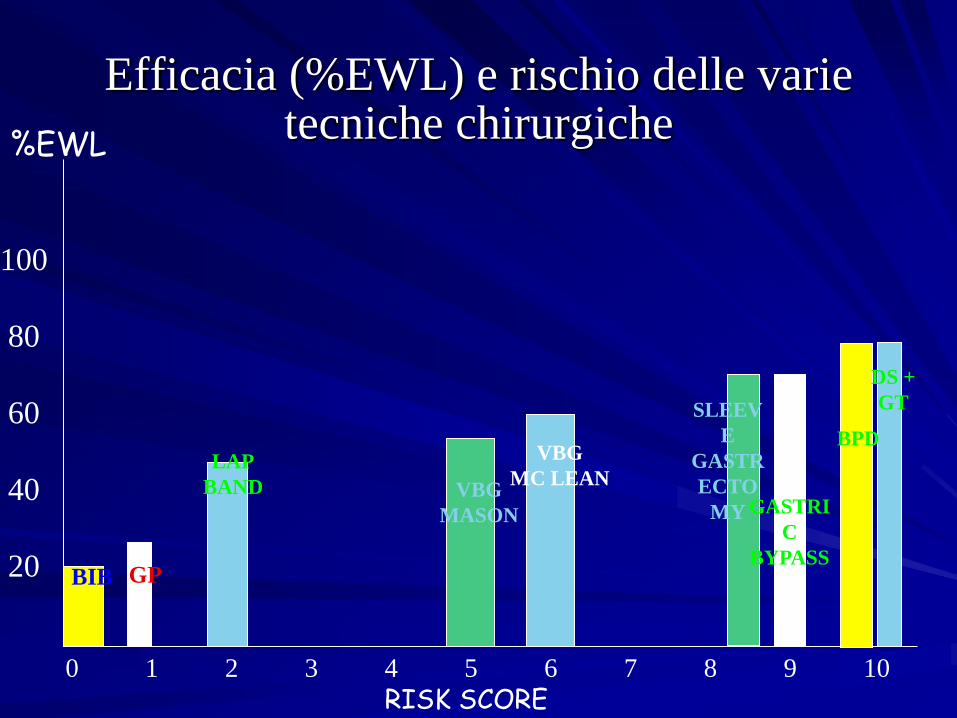
Efficacia (%EWL) e rischio delle varie tecniche chirurgiche
0 1 2 3 4 5 6 7 8 9 10
RISK SCORE
100
80
60
40
20
%EWL
BIB GP
LAP
BAND VBG
MASON
VBG
MC LEAN
SLEEV
E
GASTR
ECTO
MY GASTRI
C
BYPASS
BPD
DS +
GT

Surgery reduces weight but does not cure obesity
.... lifelong therapy
Obesity is a chronic
multifactorial disease requiering
treatment (WHO)