Embed Size (px)
Citation preview

Sleep Medicine 14 (2013) 160–164
Contents lists available at SciVerse ScienceDirect
Sleep Medicine
journal homepage: www.elsevier .com/locate /s leep
Original Article
Obstructive sleep apnoea syndrome is associated with relative hypocortisolemiaand decreased hypothalamo–pituitary–adrenal axis response to 1 and 250 lg ACTHand glucagon stimulation tests
Zuleyha Karaca a, Sevda Ismailogullari b, Selda Korkmaz b, Ilkay Cakir a, Murat Aksu b,⇑, Recep Baydemir b,Fatih Tanriverdi a, Fahri Bayram a
a Erciyes University Medical School, Department of Endocrinology, Turkeyb Erciyes University Medical School, Department of Neurology, Turkey
a r t i c l e i n f o
Article history:Received 1 August 2012Received in revised form 5 October 2012Accepted 11 October 2012Available online 4 December 2012
Keywords:OSASHPA axisACTH stimulation testGlucagon stimulation testDexamethasone suppression testCortisol
1389-9457/$ - see front matter � 2012 Published byhttp://dx.doi.org/10.1016/j.sleep.2012.10.013
⇑ Corresponding author. Address: Erciyes Universityof Neurology, 38039 Kayseri, Turkey. Tel.: +90 352 207
E-mail address: [email protected] (M. Aksu).
a b s t r a c t
Objective: The investigations regarding the effect of obstructive sleep apnoea syndrome (OSAS) on hypo-thalamo–pituitary–adrenal (HPA) axis revealed conflicting results. We aimed to evaluate the effects ofOSAS on HPA-axis with dynamic tests.Methods: This study was carried out on 26 patients with OSAS and 15 subjects without OSAS which, weredefined according to the International Classification of Sleep Disorders. Patients were enrolled from eitherEndocrinology outpatient clinic or Neurology Sleep Center. Participants for the control group wereincluded from the patients admitting to Endocrinology Department with the complaint of obesity or vol-unteers from hospital staff. All the participants were evaluated by polysomnography (PSG) and dynamictests of HPA axis (dexamethasone suppression test, 1 and 250 lg ACTH and glucagon stimulation tests).Results: Serum basal and peak cortisol levels were found to be lower in OSAS patients when compared tothe control group during 1 lg ACTH and glucagon stimulation tests. When the area under curve (AUC) ofcortisol responses to dynamic stimulation tests were calculated according to trapezoid formula, patientswith OSAS were found to have lower values compared to control group. AUC responses of all threedynamic stimulation tests were found to be negatively correlated with AHI.Conclusion: OSAS is associated with relative hypocortisolemia in the morning with reduced responses to1 and 250 lg ACTH and glucagon stimulation tests.
� 2012 Published by Elsevier B.V.
1. Introduction
Obstructive sleep apnoea syndrome (OSAS) is a common healthproblem characterized by repetitive upper airway occlusionepisodes leading to apnoea and asphyxia. It typically occurs100–600 times per night and airway patency is reestablished byarousals from sleep [1]. The pathophysiology of OSAS is not wellunderstood, but obesity and male gender are important risk factors[2].
The effect of OSAS on hypothalamo pituitary adrenal (HPA) axishas aroused interest among scientists dealing with sleep medicine.The nocturnal hypoxia associated with repetitive arousals maylead to increased cortisol secretion in patients with OSAS. How-ever, many studies have failed to find differences in serum cortisollevels between patients with OSAS and healthy controls. Further-more, treatment of OSAS by the gold standard method continuous
Elsevier B.V.
Medical School, Department6600; fax: +90 352 4375273.
positive airway pressure (CPAP) has shown conflicting resultsregarding reduction in cortisol levels in OSAS patients and the re-moval of CPAP has not been shown to result in immediate cortisolincrease either [3–7].
Serum or salivary morning cortisol levels were used for theinvestigation of HPA axis in many of the studies [8–12]. Moreextensive evaluation of circadian rhythm by measurement of corti-sol in every 30 minutes, revealed unchanged or increased cortisollevels during sleep without any change in 24 h mean cortisol levelsin patients with OSAS [7,13].
The response of HPA axis to challenge in OSAS patients has pre-viously been investigated with dexamethasone suppression andCRH stimulation tests. CRH administration was not shown to resultin different ACTH and cortisol responses in patients with OSAS [7],but OSAS was shown to be associated with less suppression of sal-ivary cortisol following dexamethasone administration comparedto obese subjects without OSAS. Although basal and late night sal-ivary cortisol levels were found to be similar in both groups [9].
The aim of the present study was to evaluate the HPA axis in pa-tients with OSAS and subjects without OSAS. Therefore, we used

Z. Karaca et al. / Sleep Medicine 14 (2013) 160–164 161
three well-defined dynamic stimulation tests of the HPA-axis (1and 250 lg ACTH and glucagon stimulation tests), which havenot previously been carried out in OSAS patients, at least accordingto our knowledge.
2. Materials and methods
2.1. Study participants and baseline tests
This study was carried out on 26 patients with OSAS and 15subjects without OSAS. OSAS was diagnosed according to the Inter-national Classification of Sleep Disorders 2. An apnoea-hypopnoeaindex (AHI) P 5 on PSG with at least one of the following: (i) unin-tentional sleep episodes during wakefulness, daytime sleepiness,unrefreshing sleep, fatigue or insomnia, (ii) the patient wakes withholding of breath, gasping or choking, (iii) the bed partner reportsloud snoring, breathing interruptions, or both during the patient’ssleep or (iv) AHI P 15 in the absence of another current sleep dis-order, medical or neurological disorder, medication or substanceuse [14]. We excluded all medical conditions (other thancontrolled hypertension), smoking more than 10 cigarettes/dayand any drug use (other than antihypertensives including angio-tensin converting enzyme inhibitors, angiotensin receptor blockersor calcium-channel blockers).
Serum fasting glucose and lipid levels were measured. Thyroidfunction tests, PRL, FSH, LH and estradiol levels in females and totaltestosterone in males were measured and found to be in the nor-mal ranges (data not shown).
2.2. Polysomnography
All the participants were evaluated with PSG recordings. A full-night PSG recording was performed using a computerized record-ing system (Grass Telefactor�, West Warwick, RI, USA) consistingof (1) sleep scoring through six channel electroencephalography(EEG) (EEG leads; F4-M1, C4-M1, O4-M1, F3-M2, C3-M2, O3-M2),two channel electrooculography (EOG), and one channel electro-myography (EMG); (2) respiration monitoring through a thermis-tor as well as a nasal pressure sensor for apnoea–hypopnoeadetection, piezo-crystal effort belts for thoraco-abdominal move-ment detection and a pulse-oximeter; (3) a two lead electrocardio-gram (ECG); and (4) bilateral tibial EMG and a body positiondetector.
All recordings were scored based on 30 second epochs accord-ing to the American Academy of Sleep Medicine (AASM) criteria[15]. Sleep stages were scored as W (wake), N1 (stage 1 sleep),N2 (stage 2 sleep), N3 (SWS), and R (REM sleep). Sleep parameterswere assessed based on the sleep recordings and included (1) sleepscoring data; total sleep time (TST; in minutes), sleep latency (SL;lightsout to first epoch of any sleep in minutes), percent sleep effi-ciency ([TST/total recording time] � 100), wake after sleep onset(WASO; stage W during total recording time, minus SL, in min-utes), percent of TST in each stage (time in each stage/TST), StageREM latency (sleep onset to first epoch of stage REM in minutes);(2) respiratory events; apnoea hypopnoea index (AHI; total num-ber of apnoeas and hypopnoeas � 60/TST). An obstructive apnoeawas defined as a drop in the peak thermal sensor excursion byP90% of baseline lasting at least 10 second accompanied by respi-ratory effort movement. An obstructive hypopnoea was defined asnasal pressure signal excursions drop by P30% of baseline withP4% desaturation from pre-event baseline, or P50% of baselinewith P3% desaturation from pre-event baseline or the event isassociated with arousal, associated with respiratory effort; (3)movement events; periodic leg movements of sleep (PLMS) index(PLMI; number of PLMS � 60/TST) according to the AASM criteria.
The data were scored by a sleep medicine specialist who wasmasked to the status of subjects. Participants filled out the Ep-worth Sleepiness Scale (EPSS) and a score of equal or higher than10 was accepted as having sleepiness.
2.3. Dynamic tests evaluating HPA-axis
Overnight dexamethasone suppression test was performed inthe study-participants. 1 mg dexamethasone was given at 11 pmand serum cortisol was measured in the following morning at8 am.
Dynamic tests were performed at 8 am in the morning on differ-ent days after an overnight fast, leaving at least 48 h between tests.0.25 mg intravenous Tetracosactrin (1–24) (Synacthen, Novartis,Switzerland) was used for ACTH stimulation tests. 0.25 mg Tetrac-osactrin was mixed with 250 ml 0.9% NaCl solution and preservedat +4 �C for not more than a month and 1 lg ACTH was obtainedfrom this mixture. 1 and 250 lg ACTH stimulation tests were per-formed and blood samples for the measurement of cortisol wereobtained in the basal state and 30, 60, 90 and 120 minutes afterthe administration of 1 and 250 lg intravenous ACTH, respectively.
One mg glucagon (GlucaGen hypokit, Novo Nordisk, Denmark)was applied intramuscularly and blood samples were obtained inthe basal state and after 90, 120, 150, 180, 210 and 240 minutesfollowing administration of glucagon.
No adverse reactions were reported during ACTH or glucagonstimulation tests. Unfortunately, 250 lg ACTH stimulation testcould only be carried out in 16 patients and eight control subjectssince 0.25 mg intravenous Tetracosactrin (1–24) (Synacthen,Novartis, Switzerland) was unavailable for the others. The othertests were completed successfully in all participants.
2.4. Assays
Serum cortisol levels were measured by radioimmunoassay(RIA) method with DSL-2100 (Texas, USA) with an intraassay coef-ficient of variation: 8.4%, interassay coefficient of variation: 9.1%and sensitivity of 0.3 lg/dl.
Total cholesterol and HDL-cholesterol and triglyceride levelswere measured by enzymatic reactions (Beckman Coulter, SyncronLX20/LX20 pro) in the morning after an overnight fast. LDL-choles-terol was calculated according to the Friedewald formula.
This study was approved by Local Ethics Committee and thestudy participants signed the written informed consent.
2.5. Statistical analysis
All statistical analysis were done by Statistical Package for So-cial Sciences (SPSS for Windows, version 15; Chicago, IL). The re-sults are presented as mean ± standard deviation. Normaldistribution of the data were tested by Kolmogorov–Smirnov test.The correlations were tested with Pearson’s correlation analysis.Student t-test or Mann–Whitney U test were used as parametricand non-parametric tests for comparison of the groups, whereappropriate. Chi-square test was used for comparison of the cate-gorical variables. Analysis of covariance was used for comparisonof cortisol levels for BMI correction. p < 0.05 was considered as sta-tistically significant.
3. Results
The demographic characteristics of the patients are presented inTable 1. Patients with OSAS were found to be older than the controlsubjects. The sex distribution and body mass indices of the partic-ipants were similar in both groups. The groups did not show

Table 1Baseline characteristics of the participants.
OSAS patients n = 26 Control group n = 15 p Value
Age (years) 47 ± 8 37 ± 9 0.001Sex (female/male) 7/19 6/9 0.490BMI (kg/m2) 34.6 ± 7.5 31.6 ± 6.4 0.200AHI (n/h) 45 ± 26 4 ± 3 <0.001Min O2 saturation (%) 78 ± 10 88 ± 5 <0.001Sleep latency (min) 18.3 ± 14.9 10.7 ± 10.9 0.100Sleep efficacy (%) 83.5 ± 7.8 88.4 ± 10 0.090Sleep stages
N1 (%) 11 ± 5 10 ± 11 0.700N2 (%) 70 ± 11 62 ± 11 0.030N3 (SWS) (%) 9 ± 7 17 ± 7 0.006REM (%) 9 ± 6 11 ± 5 0.400
PLM index (mean ± standard error) 3.9 ± 1.6 0.4 ± 1.4 0.060Arousal index (n/h) 12.8 ± 8.2 median: 9.2 (4.3–32.6) 8.9 ± 10.8 median: 5.8 (2.3–39.1) 0.024Fasting glucose (mg/dl) 99 ± 12 84 ± 25 0.024Total cholesterol (mg/dl) 199 ± 35 195 ± 38 0.740LDL-cholesterol (mg/dl) 123 ± 31 125 ± 27 0.820Triglyceride (mg/dl) 165 ± 80 133 ± 58 0.760HDL-cholesterol (mg/dl) 42 ± 8 41 ± 11 0.190
PLM: periodic leg movement.
162 Z. Karaca et al. / Sleep Medicine 14 (2013) 160–164
statistically significant differences in means of number of smokers(15% and 20%, respectively in OSAS patients and control group) orhypertensive subjects (19% and 7%, respectively, in OSAS patientsand control group).
Apnoea–hypopnoea and arousal indices were found to be signif-icantly higher and minimum O2 saturation levels were significantlylower in patients with OSAS as expected. Fasting glucose levelswere found to be significantly higher in OSAS patients comparedto control subjects. Lipid levels were similar in both groups(Table 1).
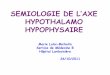
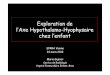
All OSAS patients and the control group had supressed cortisolresponse (<1.8 lg/dl) following dexamethasone administration.Serum basal and peak cortisol levels were found to be lower inOSAS patients when compared to the control group during 1 lgACTH and glucagon stimulation tests. Standard ACTH stimulationtest (performed on 16 OSAS patients and eight control subjects)did not reveal statistically significant difference between groupsin terms of both basal and peak cortisol responses. When the areaunder curve (AUC) of cortisol responses to dynamic stimulationtests were calculated according to trapezoid formula, patients withOSAS were found to have lower values compared to control group
Table 2Dexamethasone suppression, low-dose ACTH and glucagon stimulation tests.
Dynamic tests
Overnight DST Cortisol (lg/dl)Low-dose ACTH stimulation test Basal cortisol(lg/dl)
Peak cortisol response
AUC** of cortisol responses
Glucagon stimulation test Basal cortisol (lg/dl)
Peak cortisol response (lg/dl)
AUC** of cortisol responses
Standard-dose ACTH stimulation test⁄⁄ Basal cortisol (lg/dl)
Peak cortisol response (lg/dl)
AUC⁄⁄⁄ of cortisol responses
* Values in the second line are corrected for BMI.** AUC: area under curve was calculated from the trapezoid graph formed by cortisol r
(Table 2 and Figs. 1–3). Covariance analysis of BMI revealed similarstatistical results for basal and stimulated cortisol levels.
The correlation analyses revealed a positive correlation be-tween BMI and AHI (p = 0.041, r = 0.33) and a negative correlationbetween BMI and minimum O2 saturation (p = 0.001, r = �0.49),but not with arousal index or EPSS. Arousal index was found tobe positively correlated with total, LDL-cholesterol levels, LDL/HDL-cholesterol ratio, but not with triglyceride and HDL-choles-terol (p = 0.001, r = 0.56 and p = 0.003, r = 0.54 and p = 0.002,r = 0.54, respectively). AHI was found be positively correlated withtriglyceride and minimum O2 saturation was found to be positivelycorrelated with HDL-cholesterol (p = 0.035, r = 0.34 and p = 0.01,r = 0.42, respectively).
AHI was found to be negatively correlated with peak cortisol re-sponse to glucagon stimulation test (p = 0.02, r = �0.38), but notwith other basal or peak cortisol levels. AHI was also found to benegatively correlated with AUC responses of all three dynamicstimulation tests (p = 0.008, r = �0.42; p = 0.007, r = �0.54 andp = 0.02, r = �0.36 for 1 and 250 lg ACTH, and glucagon stimula-tion tests, respectively). There were no correlations between arou-sal indices and basal cortisol levels and AUC responses of 1 lg
OSAS patients n = 26 Control group n = 15 p* Value
0.6 ± 0.3 0.5 ± 0.2 0.2606.3 ± 3.6 10.6 ± 4.3 0.0026.4 ± 0.8 10.4 ± 1.0 0.004
16.8 ± 5.6 21.5 ± 6.6 0.02117.1 ± 1.5 21.4 ± 1.2 0.042
1234 ± 339 1624 ± 418 0.0031253 ± 76 1607 ± 96 0.007
6.7 ± 3.5 11.2 ± 5.4 0.0036.6 ± 0.9 11.1 ± 1.1 0.004
12.7 ± 4.8 19.5 ± 6.5 <0.00112.7 ± 1.1 19.8 ± 1.4 <0.001
1474 ± 575 2233 ± 808 0.0011472 ± 135 2262 ± 176 0.001
9.7 ± 6.2 9.5 ± 6.4 0.80010.3 ± 1.6 8.4 ± 2.3 0.54431.2 ± 7.8 35.4 ± 2.8 0.17031.2 ± 1.7 35.4 ± 2.6 0.210
2362 ± 465 3027 ± 604 0.0072367 ± 136 3017 ± 201 0.019
esponses to dynamic stimulation tests.

00 30 60 90 120
5
10
15
20
25
30
35
40
minutes
cortisol control
OSAS
Fig. 1. Serum cortisol responses to 1 lg ACTH stimulation test.
05
10152025303540
minutes
cortisol
0 30 60 90 120
control OSAS
Fig. 2. Serum cortisol responses to 250 lg ACTH stimulation test.
00 90 120 150 180 210 240
510152025303540
minutes
cortisol control
OSAS
Fig. 3. Serum cortisol responses to glucagon stimulation test.
Z. Karaca et al. / Sleep Medicine 14 (2013) 160–164 163
ACTH and glucagon stimulation test. Arousal index was found to benegatively correlated with AUC of cortisol responses of 250 lgACTH stimulation test (p = 0.029, r = �54). EPSS did not show anycorrelation with basal or stimulated cortisol responses in OSASpatients.
Serum cortisol responds less than 20 lg/dl to standard-doseACTH, less than 12.5 lg/dl–1 lg ACTH and less than 9.5 lg/dl toglucagon stimulation tests were considered as adrenal insuffi-ciency [16]. Five patients had inadequate cortisol responses tomore than one dynamic stimulation tests. One patient had inade-quate cortisol response to all three tests. Four patients had inade-quate cortisol responses to 1 lg ACTH and glucagon stimulationtests, one patient had inadequate cortisol response to 250 lg ACTHand glucagon stimulation tests. Since none of the patients had
symptoms of adrenal insufficiency and all had a minimum cortisolresponse of 18 lg/dl–250 lg ACTH stimulation test, they were notrecommended to have glucocorticoid replacement therapy. All thecontrols had adequate cortisol responses to dynamic stimulationtests.
4. Discussion
Hypothalamo pituitary adrenal axis is thought to be disruptedin patients with OSAS. Not only hypoxia, but also sleep relatedalterations are likely to alter HPA-axis [17–19]. In this study, serumbasal cortisol levels and cortisol responses to dynamic stimulationtests evaluating HPA axis were found to be lower in OSAS patientsthan in healthy subjects without OSAS.
Although OSAS has been shown to be associated with increasedcortisol levels during the night [7]., morning cortisol levels werenot found to be different from healthy subjects in many studies[8–13]. Obesity was found to be associated with decreased salivaryand plasma cortisol levels, but no impact of OSAS could be demon-strated on cortisol levels [13]. Nocturnal awakenings were shownto be associated with pulsatile release of cortisol [18,20], whichis followed by temporary inhibition of cortisol secretion. Sleepmay inhibit the negative feedback inhibition of the HPA axis unlikewakefullness, which may increase negative feedback sensitivity[21]. The enhanced sensitivity of HPA axis to negative feedback ef-fect of cortisol may lead to decreased cortisol levels in the morning.In parallel to our findings, Schmoller et al. has shown that treat-ment of OSAS patients with CPAP decreased cortisol levels duringnight and increased prelunch cortisol levels. However, they couldnot demonstrate lower cortisol levels in patients with OSAS duringprelunch time since the study lacked a control group [5]. The ef-fects of OSAS on HPA axis is presumably more complex than it isthought to be.
Serum cortisol levels after overnight dexamethasone suppres-sion test did not reveal significant differences between patientswith OSAS and the control group in the present study, but the per-centage of suppression was found to be less in OSAS patients thanthe control group. In a previous study, OSAS was found to be asso-ciated with less suppression of salivary cortisol after dexametha-sone administration [9]. Therefore, response of HPA axis toexogenous dexamethasone may be partially blunted in OSAS pa-tients apart from the effect of obesity.
This study is the first comparing ACTH (with both 1 lg and250 lg ACTH) and glucagon stimulation tests in patients with OSASand the control subjects. Dynamic stimulation by all these tests re-vealed decreased cortisol responses in patients with OSAS. Sinceboth groups had similar BMIs and BMI corrected analysis revealedsimilar results, the relative hypocortisolemia is unlikely to be re-lated to obesity per se. The only difference between the groupswas the older age of the patients with OSAS. A meta-analysisregarding the effects of age on HPA axis revealed increased cortisolresponse to challenge with advancing age, which was more prom-inent in women [22]. The midnight cortisol levels were found to beincreased only after the age of 50 years associated with increasedREM sleep [23]. In a study we carried out in healthy individuals,neither basal nor stimulated cortisol levels in response to dynamicstimulation tests were found to be different in both age groups andgender [16]. So it is difficult to explain the relative hypocortisol-emia of OSAS patients by their older age.
The dynamics of CRH stimulation was previously studied in pa-tients with OSAS. An enhanced ACTH response to CRH was demon-strated in obese patients with or without OSAS compared tohealthy lean subjects, but serum cortisol responses did not differin three groups [7,11]. CRH hyposecretion was suspected to predis-pose the obese to sleep apnoea [7]. In a recent study, Lattova et al.

164 Z. Karaca et al. / Sleep Medicine 14 (2013) 160–164
could not demonstrate any difference in ACTH and cortisolresponses to post-dexamethasone CRH stimulation test [24]. Inthe present study, the impact of OSAS on HPA-axis was moreprominent than found in previous studies. We further found partialadrenal insufficiency at least in some patients.
The alteration of circadian rhythm [5,7] may result in decreasedmorning cortisol levels, causing, decreased total response of corti-sol to dynamic stimulation. Unfortunately, we could not confirmthis hypothesis since we were unable to evaluate the circadianrhythm of cortisol. Although it was found to be significant onlyfor AUC response of 250 lg ACTH stimulation, arousal index wasfound to be negatively correlated with basal and AUC cortisol re-sponses of dynamic stimulation tests. So, this supports the ideathat arousals during the night may lead to pulsatile increases incortisol levels followed by temporary inhibition of cortisol secre-tion [25], which may be responsible from this peculiar finding ofrelative morning hypocortisolemia and relatively low cortisol re-sponses to dynamic stimulation tests in OSAS patients. However,the increment in cortisol levels after stimulation tests were foundto be similar in both groups.
We were unable to demonstrate any correlation of basal orstimulated cortisol responses with EPSS. AHI was found to be neg-atively correlated with AUC responses of all three dynamic stimu-lation tests. So, as the disease severity increased serum cortisolresponses decreased.
The feedback effect of cortisol on paraventricular nucleus (PVN)and pituitary is inhibitory or excitatory depending on the activatedreceptor type and location within the brain. Low doses of glucocor-ticoids decrease wakefullness and increase SWS by mineralocorti-coid receptor (MR) mediated PVN inhibition via hippocampus. Incontrast, high doses of glucocorticoids, such as in times of stress,act on glucocorticoid receptor (GR)s in amygdala and exert a posi-tive feed-back effect on CRH and as a result, increase wakefullnessand decrease SWS [25]. So there may be minor increments in cor-tisol levels during the night due to hypoxia and sleep arousals, butthis may act as low-dose exogenous glucocorticoids leading to in-creased negative feedback effect. However, it is difficult to be cer-tain if the relative hypocortisolemia in OSAS patientsdemonstrated in the present study is a result of short or long-termsuppression of HPA axis or both.
The lipid profile did not reveal significant differences in patientswith or without OSAS, but arousal index was found to be positivelycorrelated with atherogenic lipid profile (increased total, LDL-cho-lesterol and LDL-HDL cholesterol ratio. This is in accordance withprevious findings [20].
In conclusion, OSAS is associated with relative hypocortisolemiain the morning with reduced responses to dynamic stimulationtests of 1 and 250 lg ACTH and glucagon.
Conflict of Interest
The ICMJE Uniform Disclosure Form for Potential Conflicts ofInterest associated with this article can be viewed by clicking onthe following link: http://dx.doi.org/10.1016/j.sleep.2012.10.013.
Acknowledgement
Grant support: by Erciyes University Council of Scientific Inves-tigations (project code: TSA-08-452).
References
[1] Flemons WW, Remmers JE. The diagnosis of sleep apnea: questionnaires andhome studies. Sleep 1996;9:S243–7.
[2] Bixler EO, Vgontzas AN, Ten Have T, Tyson K, Kales A. Effects of age on sleepapnea in men: I. Prevalence and severity. Am J Respir Crit Care Med1998;157:144–8.
[3] Henley DE, Russell GM, Douthwaite JA, et al. Hypothalamic–pituitary–adrenalaxis activation in obstructive sleep apnea: the effect of continuous positiveairway pressure therapy. J Clin Endocrinol Metab 2009;94:4234–42.
[4] Nakamura T, Chin K, Shimizu K, et al. Acute effect of nasal continuous positiveairway pressure therapy on the systemic immunity of patients withobstructive sleep apnea syndrome. Sleep 2001;24:545–53.
[5] Schmoller A, Eberhardt F, Jauch-Chara K, et al. Continuous positive airwaypressure therapy decreases evening cortisol concentrations in patients withsevere obstructive sleep apnea. Metabolism 2009;58:848–53.
[6] Tomfohr LM, Edwards KM, Dimsdale JE. Is obstructive sleep apnea associatedwith cortisol levels? a systematic review of the research evidence. Sleep MedRev 2012;16:243–9.
[7] Vgontzas AN, Pejovic S, Zoumakis E, et al. Hypothalamic–pituitary–adrenalaxis activity in obese men with and without sleep apnea: effects of continuouspositive airway pressure therapy. J Clin Endocrinol Metab 2007;92:4199–207.
[8] Barcelo A, Barbe F, De la PM, et al. Insulin resistance and daytime sleepiness inpatients with sleep apnoea. Thorax 2008;63:946–50.
[9] Carneiro G, Togeiro SM, Hayashi LF, et al. Effect of continuous positive airwaypressure therapy on hypothalamic–pituitary–adrenal axis function and 24-hblood pressure profile in obese men with obstructive sleep apnea syndrome.Am J Physiol Endocrinol Metab 2008;295:E380–4.
[10] Lam JC, Yan CS, Lai AY, et al. Determinants of daytime blood pressure inrelation to obstructive sleep apnea in men. Lung 2009;187:291–8.
[11] Lanfranco F, Gianotti L, Pivetti S, et al. Obese patients with obstructive sleepapnoea syndrome show a peculiar alteration of the corticotroph but not of thethyrotroph and lactotroph function. Clin Endocrinol 2004;60:41–8.
[12] Panaree B, Chantana M, Wasana S, Chairat N. Effects of obstructive sleep apneaon serum brain-derived neurotrophic factor protein, cortisol, and lipid levels.Sleep Breath 2011;15:649–56.
[13] Dadoun F, Darmon P, Achard V, et al. Effect of sleep apnea syndrome on thecircadian profile of cortisol in obese men. Am J Physiol Endocrinol Metab2007;293:E466–74.
[14] Sateia MJ, editor. International classification of sleep disorders: diagnostic andcoding manual. Westchester (IL): American Academy of Sleep Medicine; 2005.
[15] Iber C, Ancoli-Israel S, Chesson A, Quan SF. American Academy of SleepMedicine. The AASM manual for the scoring of sleep and associated events:rules, terminology and technical specifications. 1st ed. Westchester(IL): American Academy of Sleep Medicine; 2007.
[16] Karaca Z, Lale A, Tanriverdi F, Kula M, Unluhizarci K, Kelestimur F. Thecomparison of low and standard dose ACTH and glucagon stimulation tests inthe evaluation of hypothalamo–pituitary–adrenal axis in healthy adults.Pituitary 2011;14:134–40.
[17] Basu M, Sawhney RC, Kumar S, Pal K, Prasad R, Selvamurthy W. Hypothalamic–pituitary–adrenal axis following glucocorticoid prophylaxis against acutemountain sickness. Horm Metab Res 2002;34:318–24.
[18] Follenius M, Brandenberger G, Bandesapt JJ, Libert JP, Ehrhart J. Nocturnalcortisol release in relation to sleep structure. Sleep 1992;15:21–7.
[19] Raff H, Tzankoff SP, Fitzgerald RS. ACTH and cortisol responses to hypoxia indogs. J Appl Physiol 1981;51:1257–60.
[20] Ekstedt M, Akerstedt T, Soderstrom M. Microarousals during sleep areassociated with increased levels of lipids, cortisol, and blood pressure.Psychosom Med 2004;66:925–31.
[21] Spath-Schwalbe E, Gofferje M, Kern W, Born J, Fehm HL. Sleep disruption altersnocturnal ACTH and cortisol secretory patterns. Biol Psychiatr1991;29:575–84.
[22] Otte C, Hart S, Neylan TC, Marmar CR, Yaffe K, Mohr DC. A meta-analysis ofcortisol response to challenge in human aging: importance of gender.Psychoneuroendocrinology 2005;30:80–91.
[23] Van Cauter E, Leproult R, Plat L. Age-related changes in slow wave sleep andREM sleep and relationship with growth hormone and cortisol levels inhealthy men. JAMA 2000;284:861–8.
[24] Lattova Z, Keckeis M, Maurovich-Horvat E, et al. The stress hormone system invarious sleep disorders. J Psychiatr Res 2011;45:1223–8.
[25] Buckley TM, Schatzberg AF. On the interactions of the hypothalamic–pituitary–adrenal (HPA) axis and sleep: normal HPA axis activity andcircadian rhythm, exemplary sleep disorders. J Clin Endocrinol Metab2005;90:3106–14.