Embed Size (px)
Citation preview

Int. J. Oral Maxillofac. Surg. 1986: IS: 349-351
(Key words: cysticerosis, oral; mucous membrane. oral; surgery. oral and maxillofacial)
Oral cysticercosis
A. K. SHARMA, R. S. MISRA, A. MUKHERJEE, V. RAMESH AND R. K. JAIN
Department ofDermatology, Institute of Pathology-ItlM'R, Safdarjang Hospital, New Delhi, India
ABSTRACT - A 35-year-old Indian male with nodules in the tongue, lowerlip and subcutaneous tissues and convulsions of recent onset is presented.Surgical excision of the nodules confirmed the clinical diagnosis of cysticercosis and relieved the lingual discomfort. This is the 26th case of oralcysticercosis being reported.
(Acceptedfor publication 7 February 1985)
Cysticercosis, a helminthic disease commonly seen in India, Latin America, EasternEurope and Southern Africa, results fromextraintestinal encystation of the larvalform of Taenia solium. Normally this parasite completes the larval phase of its lifecycle in the pig and is then transmitted toman through eating undercooked and contaminated pork, where it develops into theadult tape worm in the intestine. The wormsagain shed gravid segments laden with eggsin the stool which reinfect pigs. Accidentalingestion of the egg by man through fecalcontamination of fingers or food or regurgitation of eggs from the intestine leads to thepresence of eggs in the stomach where theresultant embryos penetrate the mucosa andare dispersed by the blood stream leadingto cysticercosis. The usual organs showingparasitic infestation are the subcutaneoustissues, skeletal muscles and brain. The oralcavity is a distinctly unusual site for thesecysts and till now only 25 cases of oralcysticercosis have been reported', We are
reporting here a case of cysticercosis withinvolvement of tongue and lip.
Case reportA 3$-year-old non-vegetarian male presentedwith multiple small nodules all over the body forabout 7years. The first nodule was noticed on thelower lip. This was followed by the appearance ofmultiple lesions scattered over the limbs, trunkand also the tongue. 2 months after the onset ofdisease, the patient began to have generalisedconvulsions and till now has had 15-20 such fits.He did not have any history of any neurologicaldisorder prior to this. There was also no historyof gastrointestinal upsets or of passing tapeworms or worm segments in the feaces.
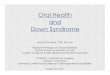
Examination of the skin revealed numerous,discrete, non-tender, firm, subcutaneous nodulesof varying sizes ranging from 0.5 ern to 2.5 emsall over the body including scalp and palms, withsparing of the soles. Some of the lesions in themuscles of the lower limbs and along the tendonsover the forearms were fairly deep-seated. Oralexamination showed similar nodules on thetongue which were easier felt than seen (Fig. 1)and a solitary nodule on the inner surface of the

350 SHARMA ET AL.
Fig. 1. Clinical photograph of tongue showingsmooth nodules on upper surface.
lower lip. Detailed clinical neurological examination did not reveal any abnormality.
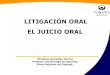
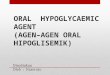
Complete blood counts were within normallimits, except for an absolute eosinophil count of423/dl. Stool examination performed on 3 consecutive days showed no eggs or worm segments.Lateral and anteroposterior skull X-rays andwhole body skeletal survey did not show anycalcified nodules. Electroencephalogram was alsonormal. Surgical removal of the cysts in thetongue was carried out under local anaesthesiaand 6 cysts ranging in diameter from 0.6 to 0.9em (Fig. 2) in diameter were excised. Each cysthad a translucent cyst wall and contained about0.3 ml of pale fluid. Cut section showed a smallyellowish spot on the inner lining. Histopathological examination revealed that the cysts wereenclosed by a thick fibrous capsule with heavyinflammatory inliltrate around it. The outermostlayer of the cyst was formed by a cellular hyalinematerial and internal to this the duct-like invaginated segments of the larval body were seen (Fig.3).
Fig. 2. Gross photograph of the 6 smooth walledcysts excised from the tongue.
Fig. 3. Photomicrograph showing cysticercus eellulosae in the tongue. The fibrotic and inflammatory cyst wall is seen to the left of the photograph.H & Ex80.
DiscussionCysticercosis presents with multiorgan infestations, giving rise to varied symptoms.The present case had oral and subcutaneousnodules and convulsions. Though cysticercosis is commonly encountered in India,oral lesions are rarely seen. In a large seriesof 450 cases, DIXON & LIPSCOMB2 detectedlingual involvement in only 8 cases (1.8%).The frequent lodgement of the larva in skeletal muscles with rare involvement of thetongue is intriguing. No explanation for thisobservation has been given. It is interestingto note that in tongue lesions in lepromatous leprosy, a systemic bacterial disease,absence of bacilli in the lingual muscle fibres, was attributed to the high muscularactivity and metabolic rate of the tonguemuscle'. We suggest that a similar mechanism might be mitigating against the lodgement and development of the cysticercuscellulosae in the tongue. It may further bementioned that in pigs, the tongue is a preferential organ of involvement.
The occurrence of convulsions followingappearance of nodules in this case in theabsence of any other progressive neurological disease strongly indicates cerebral involvement due to cysticercosis. In the studymentioned earlier', convulsions were seen in

ORAL CYSTICEROSIS 351
92% of cases while 76% cases had convulsions as the first symptom. In a study of631 cases ofepilepsy from India', cysticercosis was found to be the cause in 14 (2.2%)cases.
All of DIXON & LIPSCO~IB'S2 8 cases oflingual cysticercosis had cerebral involvement also . Similar muitiorgan involvementin cases of oral cysticercosis has been seenin earlier studies's,
The presence of the cyst interferes withthe movement of the tongue, causing discomfort during speaking, eating, etc. Medical treatment is of no use and surgical excision of the cysts as was done in the presentcase remains the only way ofconfirming thediagnosis and giving relief to the patient.The report further emphasizes the need toconsider cysticercosis along with othercauses of cystic lesions of the tongue, particularly in areas with a high incidence ofthis condition.
References1. BEDI T. R., PANDIII, R. K. & BHUTANI L. K.:
A case of cysticercus cellulosae involving theoral cavity.Jnr . Jr. Dermat. 1974: 13: 188-189.
2. DIXON H. B. F. & Lrrscoxa F. M.: Cysticercosis. all analysis and follo w up of 450 cases.Privy Council, Med. Res. Council, SpecialReport SeriesNo : 299. Her Majesty's Stationary Office, London 1961.
3. LUSTMANN J. & COPELYN M. (1981): Oralcysticercosis: review of literature and reportof 2 cases. 1111. J. Oral Surg, 1981: 10:371-375.
4. MANI, A. J., RAMESII, C. K., AHUJA, G. K. &MANI, K. S.: Cerebral cysticercosis presentingas epilepsy. Neurology India 1974: 22: 30-34.
5. MUKHERJEE A., GIRDHAR B. K. & DESIKANK. V.: Histopathology of tongue lesions inleprosy. Leprosy Re~'ielV 1980: 50: 37-43.
6. TIMOSCA G. & GAVRILITA L.: Cysticercosis ofthe maxillo facial region. A clinico pathologicstudy of 5 cases. Oral Surgery 1974: 37:390-400.
Address:
R. S. Misra.Department of Dermatology.Safdarjang Hospital,New Delhi - I/O 029India