Embed Size (px)
Citation preview

Cuando el tiempo libre a la progresión es el objetivo
Agustí Barnadas
Servicio de Oncología Médica
Hospital de Sant Pau
Barcelona
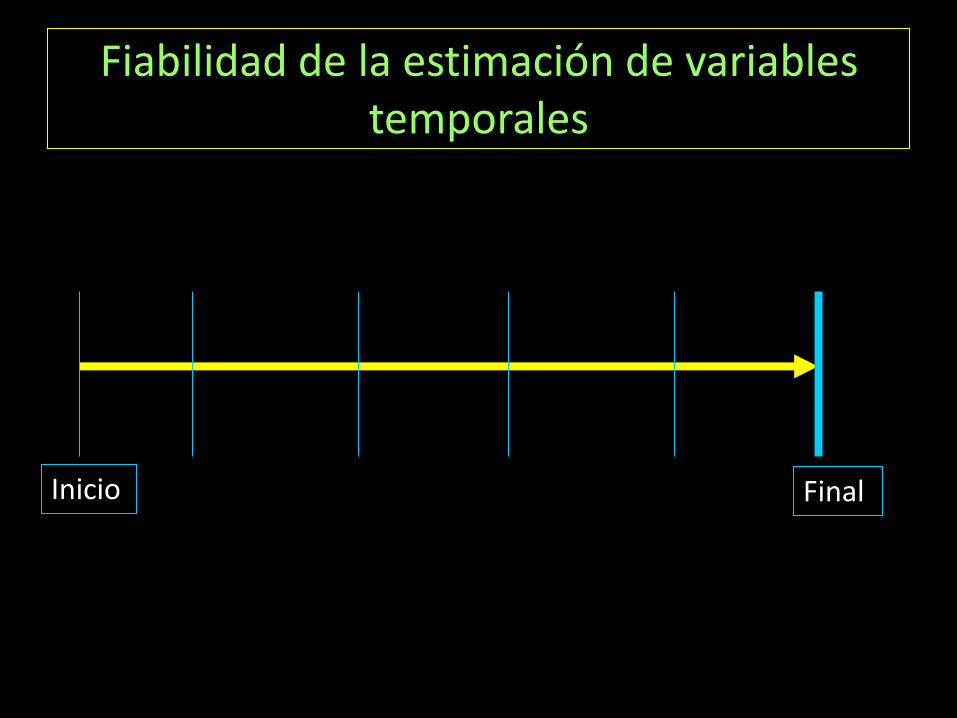
Fiabilidad de la estimación de variables temporales
Inicio Final
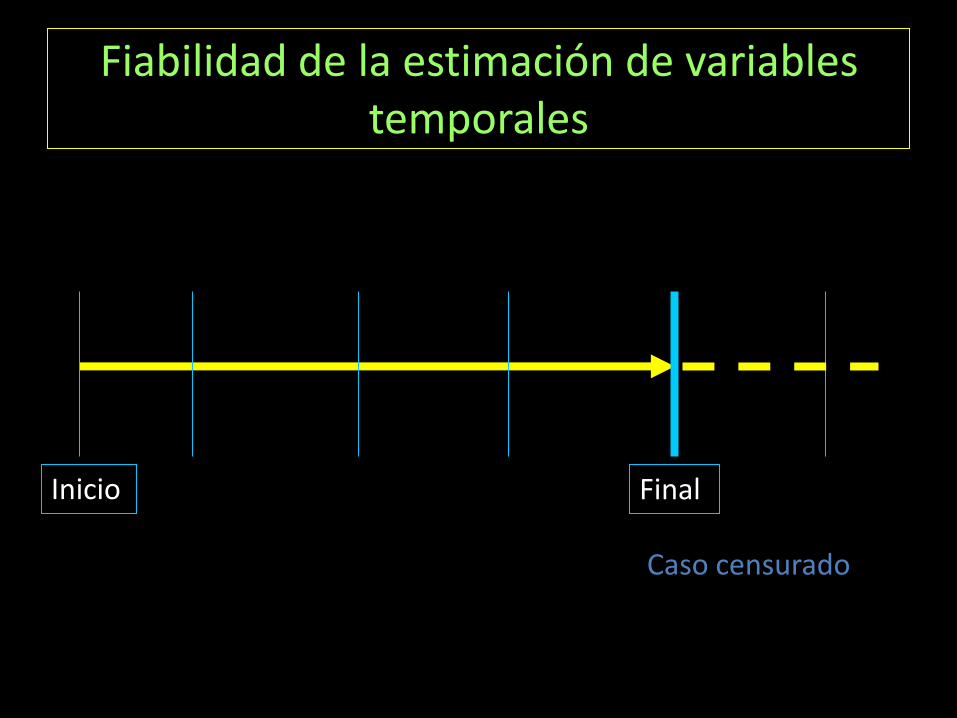
Fiabilidad de la estimación de variables temporales
Inicio Final
Caso censurado
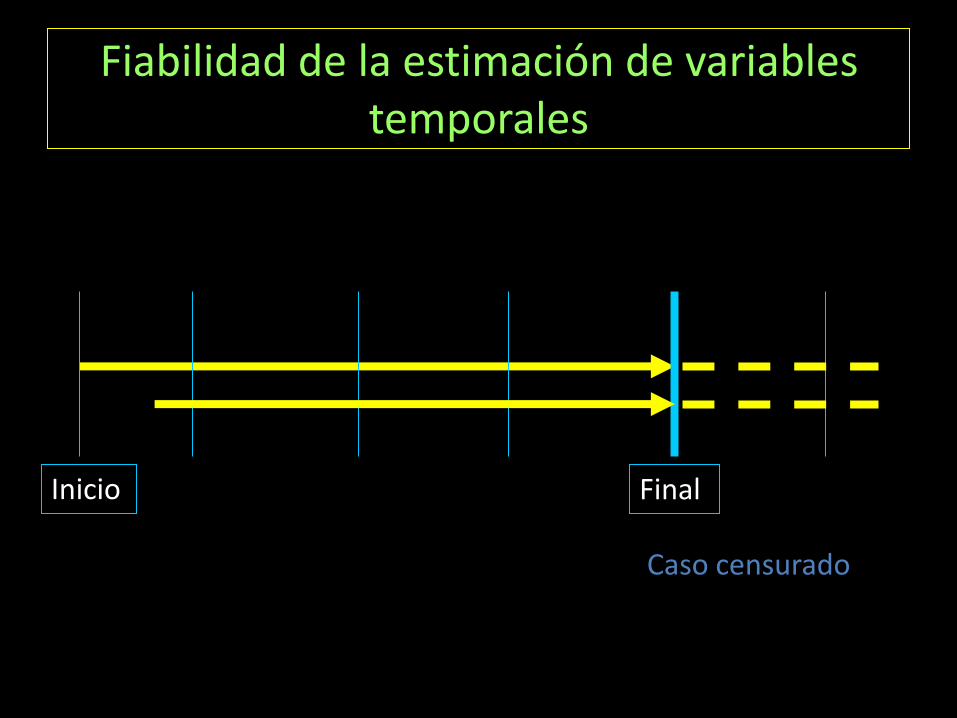
Fiabilidad de la estimación de variables temporales
Inicio Final
Caso censurado
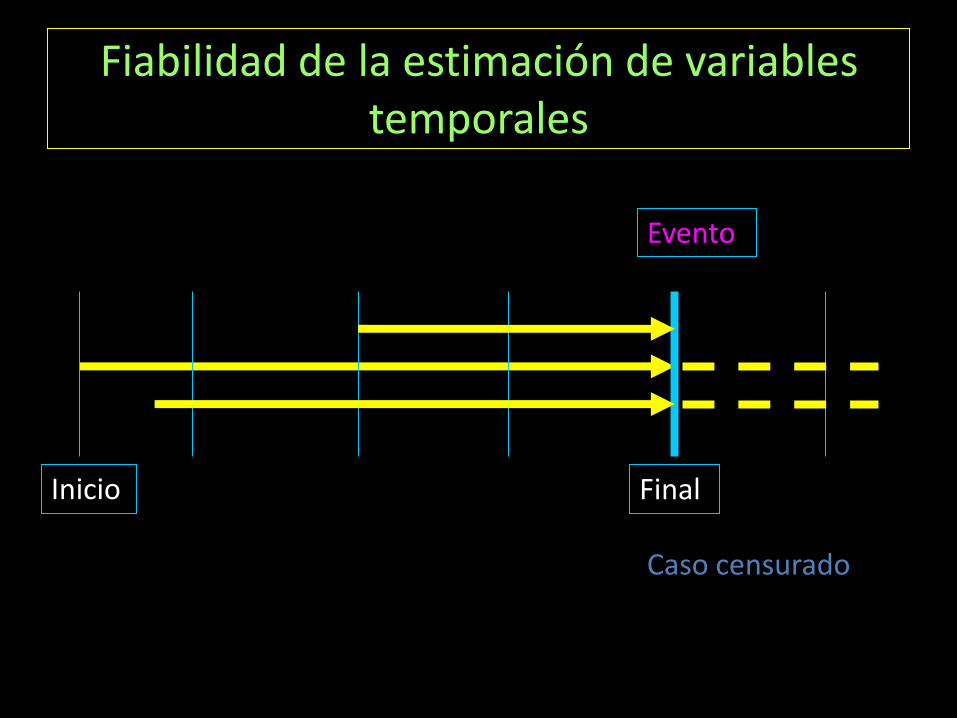
Fiabilidad de la estimación de variables temporales
Inicio Final
Caso censurado
Evento
Objetivos en los ensayos clínicos
• Objetivos centrados en el paciente – Calidad de vida – Supervivencia – Tolerancia/Seguridad
• Objetivos centrados en la enfermedad – Respuesta objetiva – Intervalo libre de enfermedad – Tiempo a la progresión – Valor del cambio de:
• CTCs • Marcadores tumorales: PSA, B-HCG
Objetivo centrado en el paciente: Supervivencia
• Reconocido como objetivo primario en una proporción importante de estudios de registro (“gold standard”)
• Definición: – Tiempo desde la aleatorización hasta la muerte
independientemente de su causa
• Corrección: Supervivencia específica de cáncer – Secundaria al tumor índice del estudio
– Secundaria a un segundo tumor de la misma estirpe
– Exclusión de muertes por otros tumores u otras causas
Supervivencia: limitaciones
• Efecto de los tratamientos administrados en una/varias líneas posteriores
• Necesita un mayor tiempo de observación
• Necesita de un gran número de pacientes para poder detectar diferencias
• Efecto de la historia natural de la enfermedad:
– Tumores con una progresión lenta
– Tumores con mayor agresividad
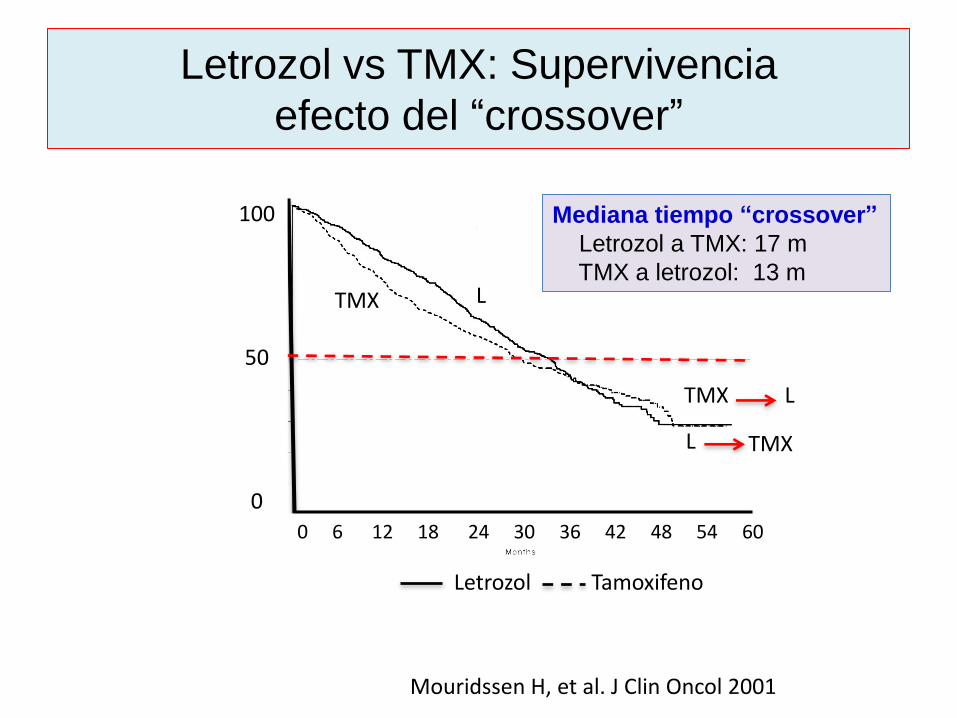
Letrozol vs TMX: Supervivencia
efecto del “crossover”
(19%) in the randomized letrozole arm compared with 132
deaths (29%) in the randomized tamoxifen arm (data not shown).
The repeated log-rank tests indicated that all tests between 6 and
24 months were nominally statistically significant (ie, not ad-
justed for multiple tests), whereas the test at 30 months showed
a (nominal) strong trend in favor of the randomized letrozole arm
(Table 3).The two survival curves crossed at around 3 years
(clearly indicating nonproportional hazards; Fig 4), by which
time cross-overs were virtually complete.
Additional analyses were performed to explore whether the
evaluation of OS attributable to the first-line endocrine therapy
might be impaired by the cross-over to the other endocrine agent.
Median OS from initial randomization, censoring time to death at
cross-over, was 42 months (95% confidence interval [CI], 36
months to not estimable) for letrozole and 30 months (95% CI, 27
to 36 months) for tamoxifen. For the cross-over data, the numbers
of patients who progressed on first-line treatment and who crossed
over in each sequence are listed in Table 1. Of the patients who
crossed over, 63% crossing from letrozole first-line to tamoxifen
second-line died either during second-line therapy or, more usually,
during the follow-up period after their second progression. This
mortality rate was substantially higher than for patients crossing
from tamoxifen first-line to letrozole second-line (47%). Median OS
from the date of cross-over was 19 months (95% CI, 17 to 24
Fig 3. Forest plot of treatment compari-
sons for objective response rate by key
baseline covariates. Squares denote odds
ratios, drawn proportional to the number of
events, and lines represent 95% confidence
intervals. Odds ratios > 1 favor letrozole.
Fig 4. Overall survival (OS) at median
follow-up of 32 months, by randomized
treatment arm. Median OS was not signifi-
cantly different (overall log-rank, P .53).
There was a significant difference in favor of
the randomized letrozole arm between 6
and 20 months (Kolmogorov-Smirnov-type
test, P .003).
2105LETROZOLE VERSUS TAMOXIFEN IN BREAST CANCER
Letrozol Tamoxifeno
Mouridssen H, et al. J Clin Oncol 2001
TMX L
TMX
L
L
TMX
100
50
0 0 6 12 18 24 30 36 42 48 54 60
Mediana tiempo “crossover”
Letrozol a TMX: 17 m
TMX a letrozol: 13 m
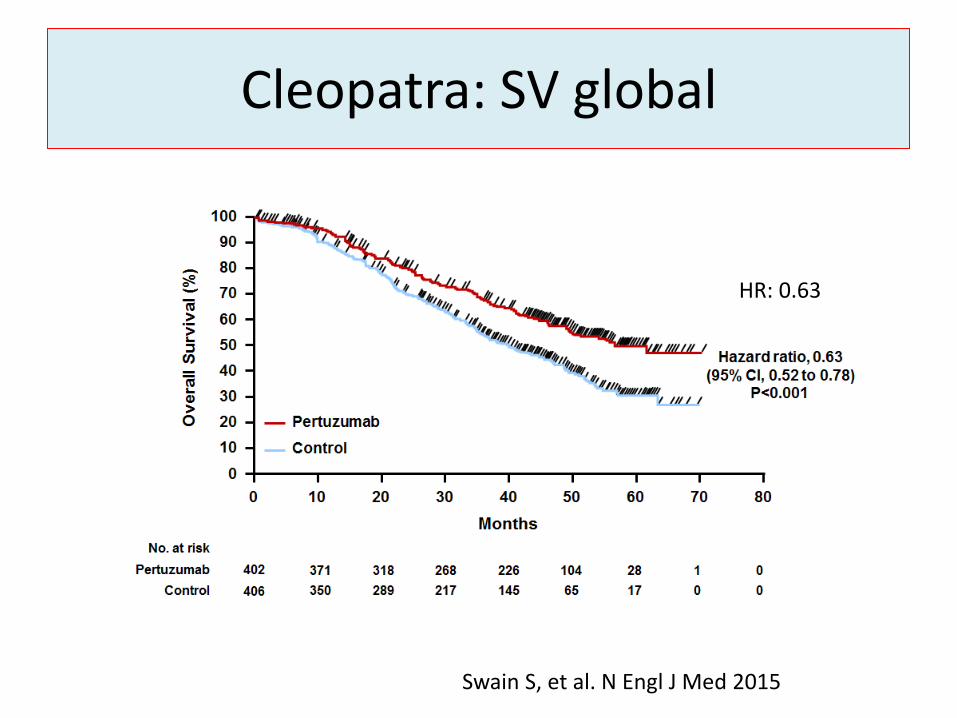
Cleopatra: SV global
HR: 0.63
Swain S, et al. N Engl J Med 2015
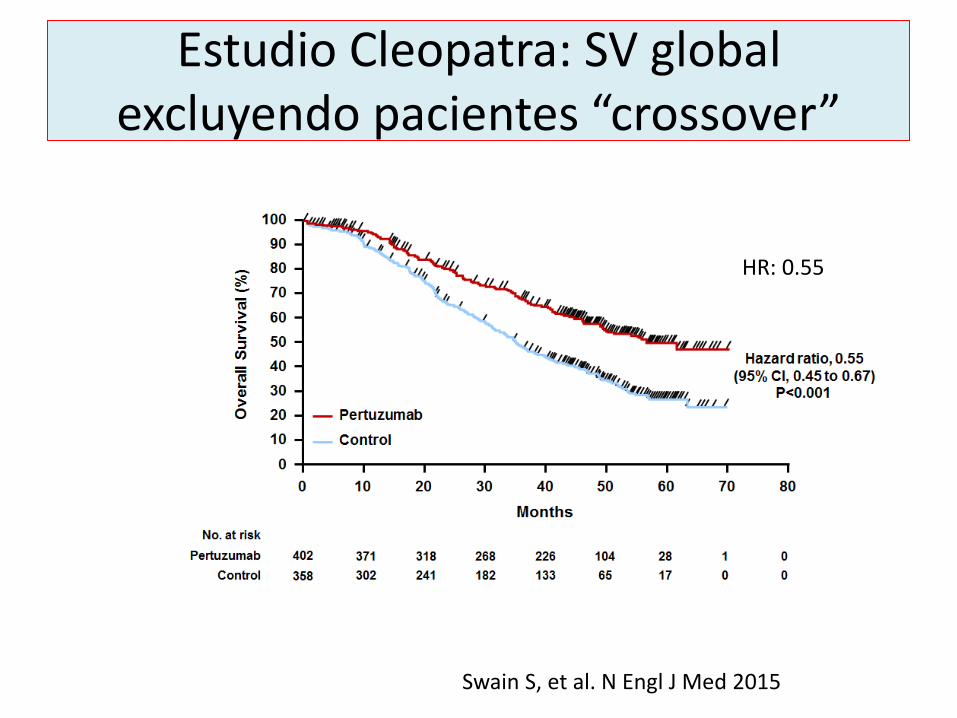
Estudio Cleopatra: SV global excluyendo pacientes “crossover”
Swain S, et al. N Engl J Med 2015
HR: 0.55
Objetivos en los ensayos clínicos
• Objetivos centrados en el paciente – Calidad de vida – Supervivencia – Tolerancia/Seguridad
• Objetivos centrados en la enfermedad – Respuesta objetiva – Intervalo libre de enfermedad – Tiempo a la progresión – Valor del cambio de:
• CTCs • ctDNA • Marcadores tumorales: PSA
• Variable que define el efecto de una única intervención
• Su resultado no depende de la actividad de un tratamiento posterior
• Retos: – Definición – Frecuencia en la medición de las lesiones diana/no
diana – Estimación subjetiva/objetiva – Comité independiente de valoración – ¿Son variables subrogadas?
Objetivos centrados en el tumor
Retos: definición DFS
• Tiempo entre la aleatorización hasta:
– la recaída del tumor local/distancia
– segundo tumor de la misma localización/otra
– o muerte por cualquier causa
• ¿Todos los estudios lo definen igual?
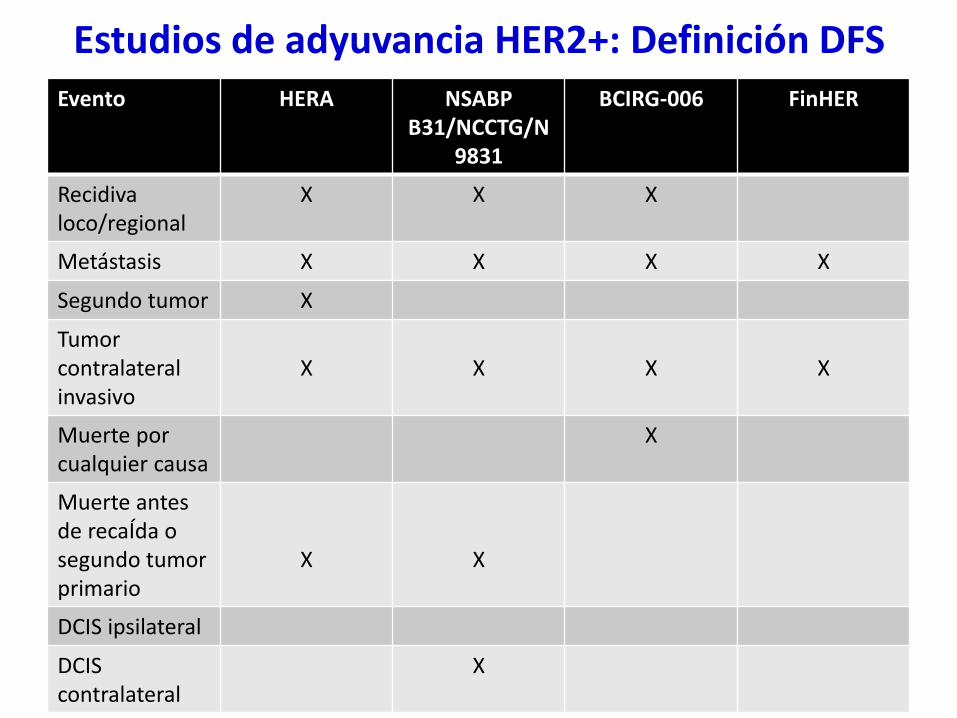
Estudios de adyuvancia HER2+: Definición DFS Evento HERA NSABP
B31/NCCTG/N9831
BCIRG-006 FinHER
Recidiva loco/regional
X X X
Metástasis X X X X
Segundo tumor X
Tumor contralateral invasivo
X
X
X
X
Muerte por cualquier causa
X
Muerte antes de recaÍda o segundo tumor primario
X
X
DCIS ipsilateral
DCIS contralateral
X
PFS/TTP
• Tiempo desde la aleatorización hasta la progresión o muerte – TTP: progresión pero excluye las muertes
• Retos: – Medición con la misma metodología: RECIST
• Incremento de al menos 20% suma de los diámetros de las lesiones diana
• Enfermedad voluminosa/indolente
– Frecuencia de las mediciones: 6/8/12 semanas – Papel de los comités centralizados de evaluación de
respuesta – Variables de confusión
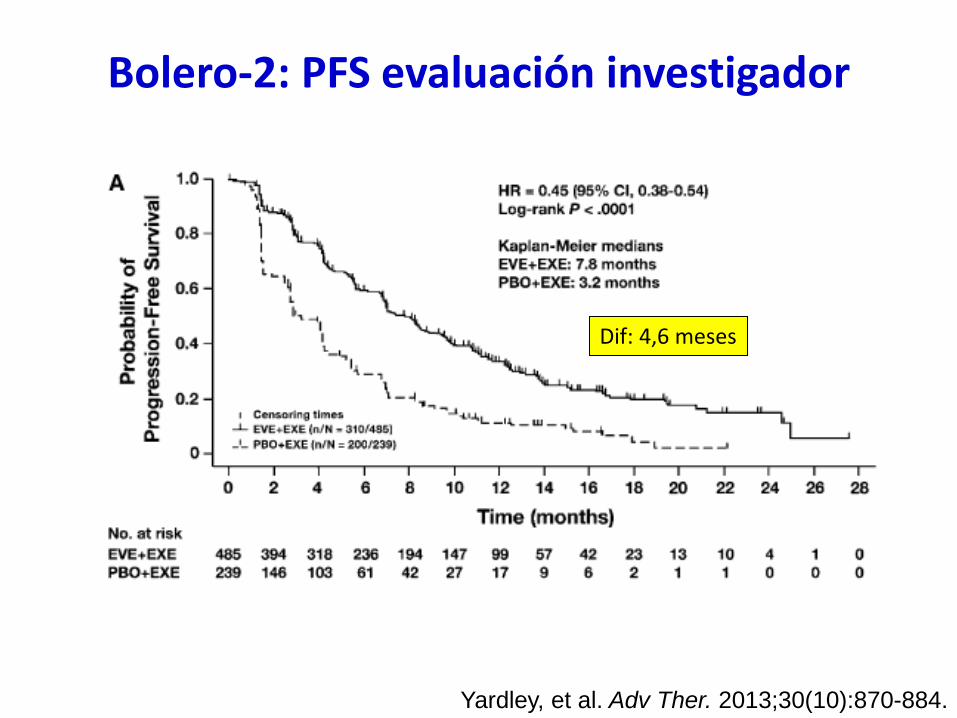
Bolero-2: PFS evaluación investigador
Yardley, et al. Adv Ther. 2013;30(10):870-884.
Dif: 4,6 meses
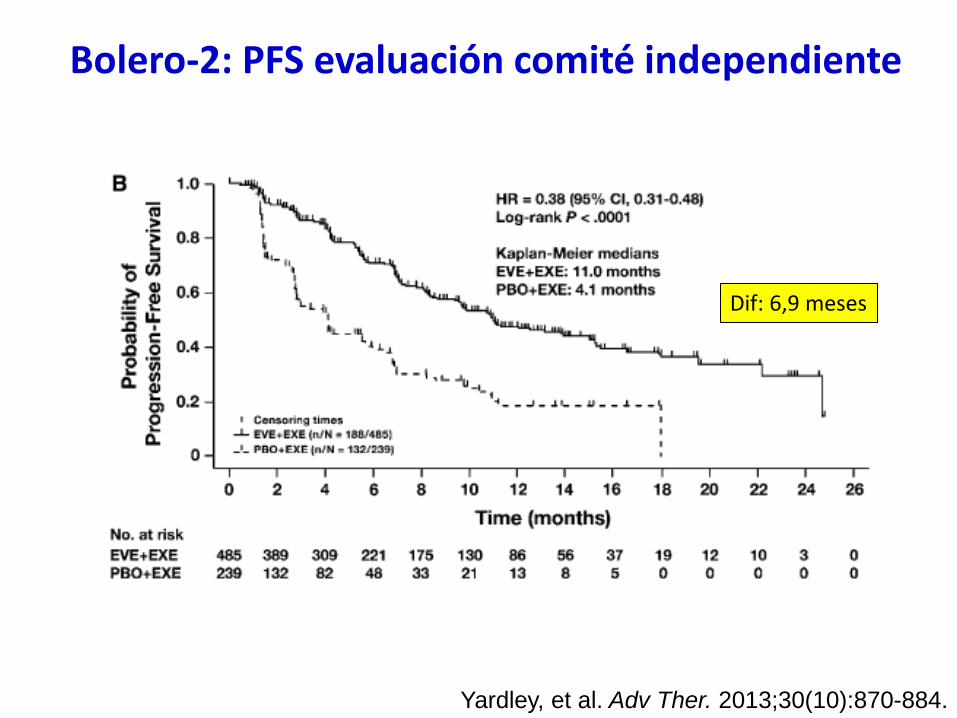
Bolero-2: PFS evaluación comité independiente
Yardley, et al. Adv Ther. 2013;30(10):870-884.
Dif: 6,9 meses
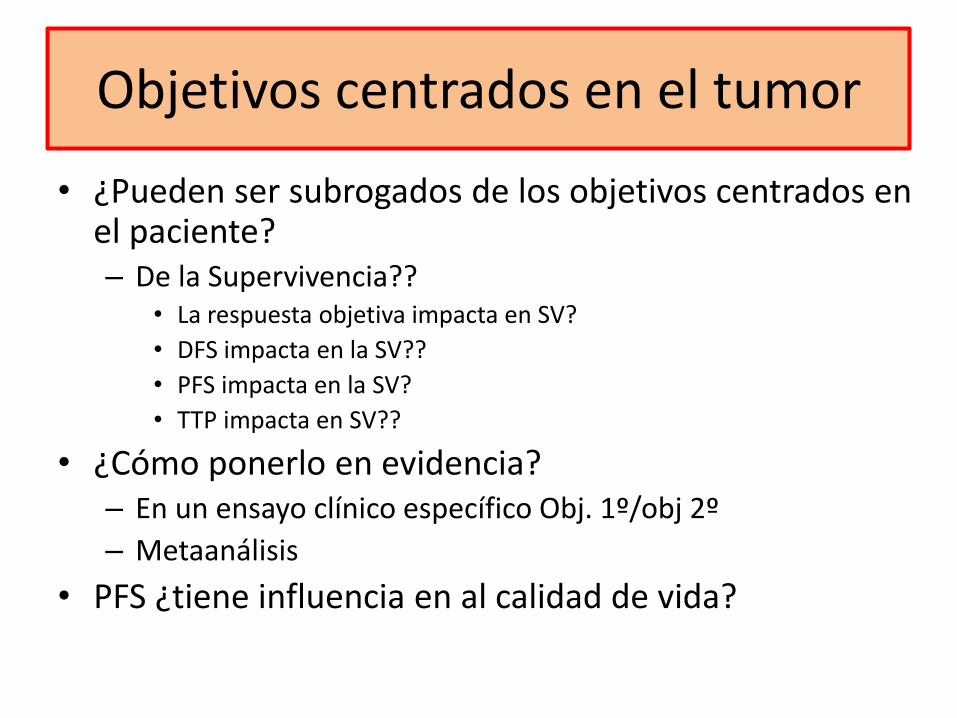
Objetivos centrados en el tumor
• ¿Pueden ser subrogados de los objetivos centrados en el paciente? – De la Supervivencia??
• La respuesta objetiva impacta en SV?
• DFS impacta en la SV??
• PFS impacta en la SV?
• TTP impacta en SV??
• ¿Cómo ponerlo en evidencia? – En un ensayo clínico específico Obj. 1º/obj 2º
– Metaanálisis
• PFS ¿tiene influencia en al calidad de vida?
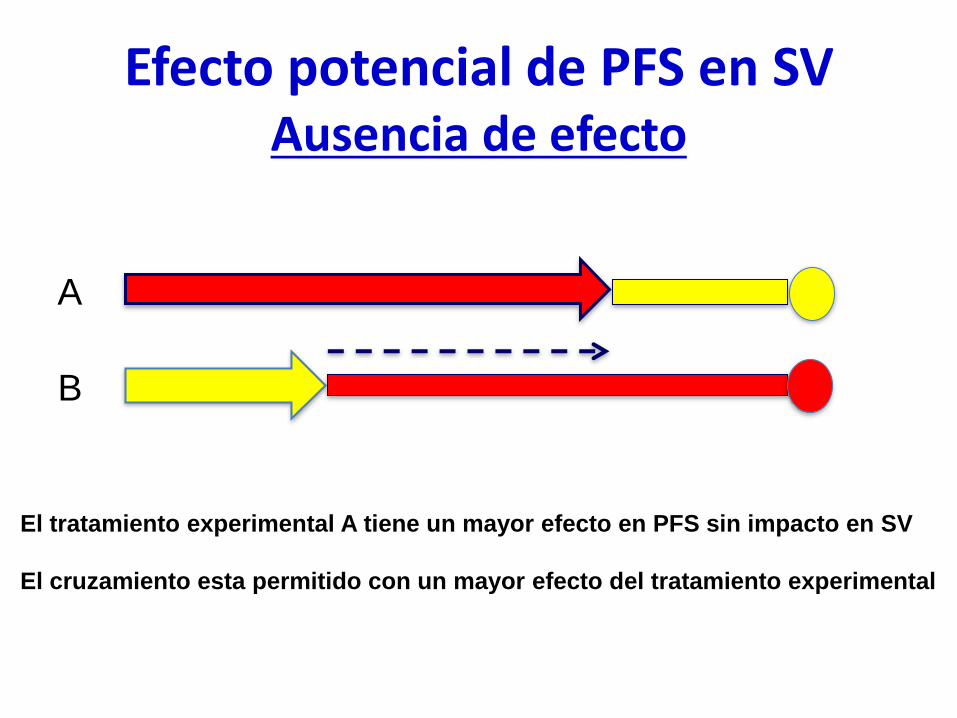
Efecto potencial de PFS en SV Ausencia de efecto
A
B
El tratamiento experimental A tiene un mayor efecto en PFS sin impacto en SV
El cruzamiento esta permitido con un mayor efecto del tratamiento experimental
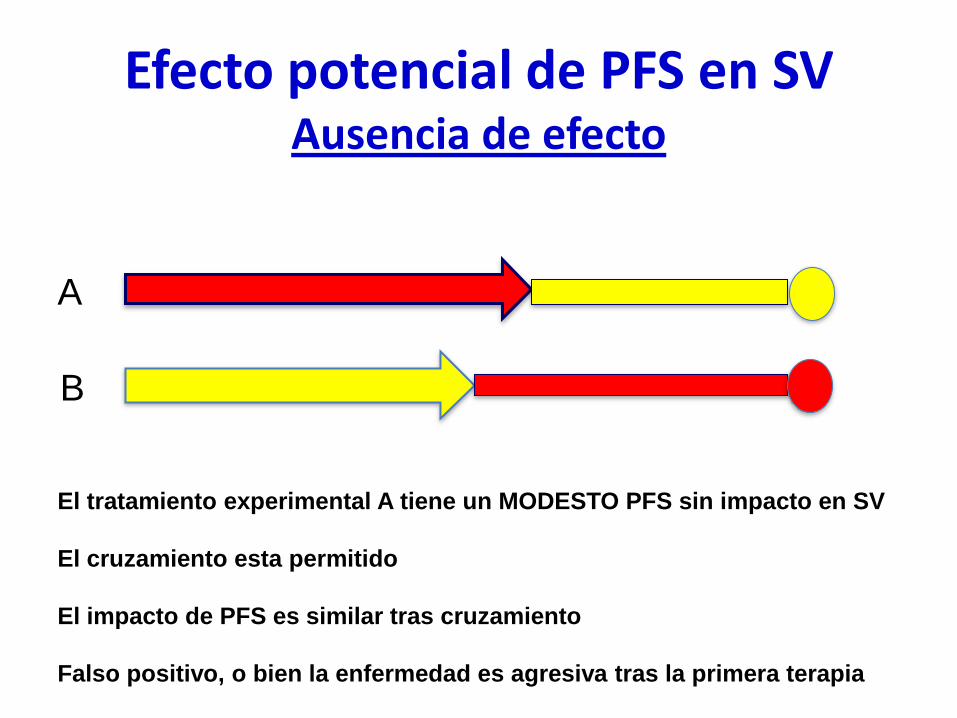
Efecto potencial de PFS en SV Ausencia de efecto
A
B
El tratamiento experimental A tiene un MODESTO PFS sin impacto en SV
El cruzamiento esta permitido
El impacto de PFS es similar tras cruzamiento
Falso positivo, o bien la enfermedad es agresiva tras la primera terapia
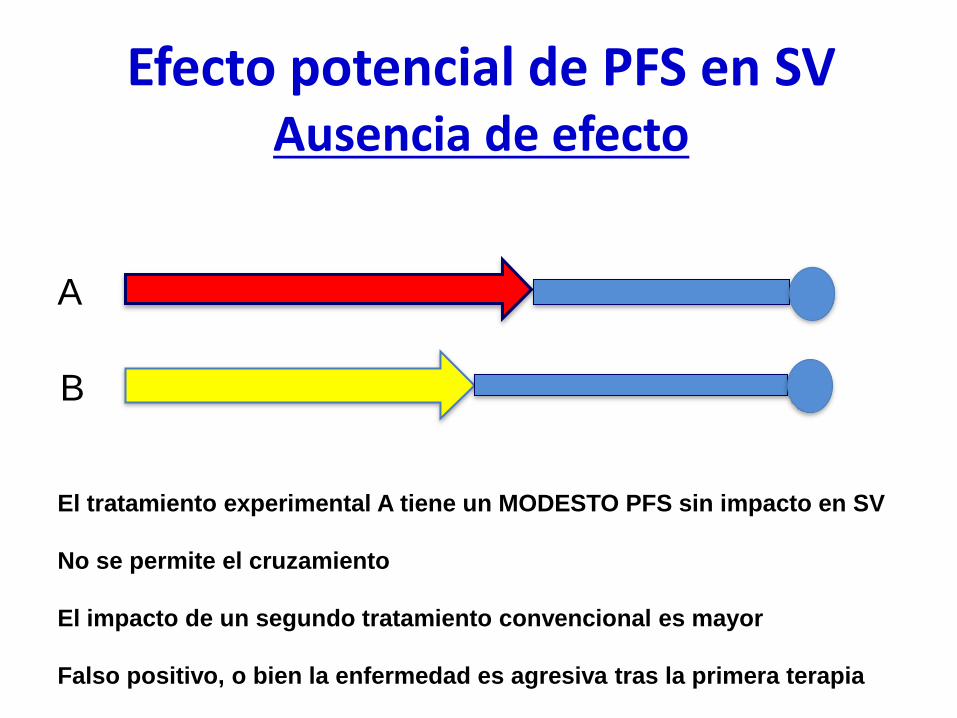
Efecto potencial de PFS en SV Ausencia de efecto
A
B
El tratamiento experimental A tiene un MODESTO PFS sin impacto en SV
No se permite el cruzamiento
El impacto de un segundo tratamiento convencional es mayor
Falso positivo, o bien la enfermedad es agresiva tras la primera terapia
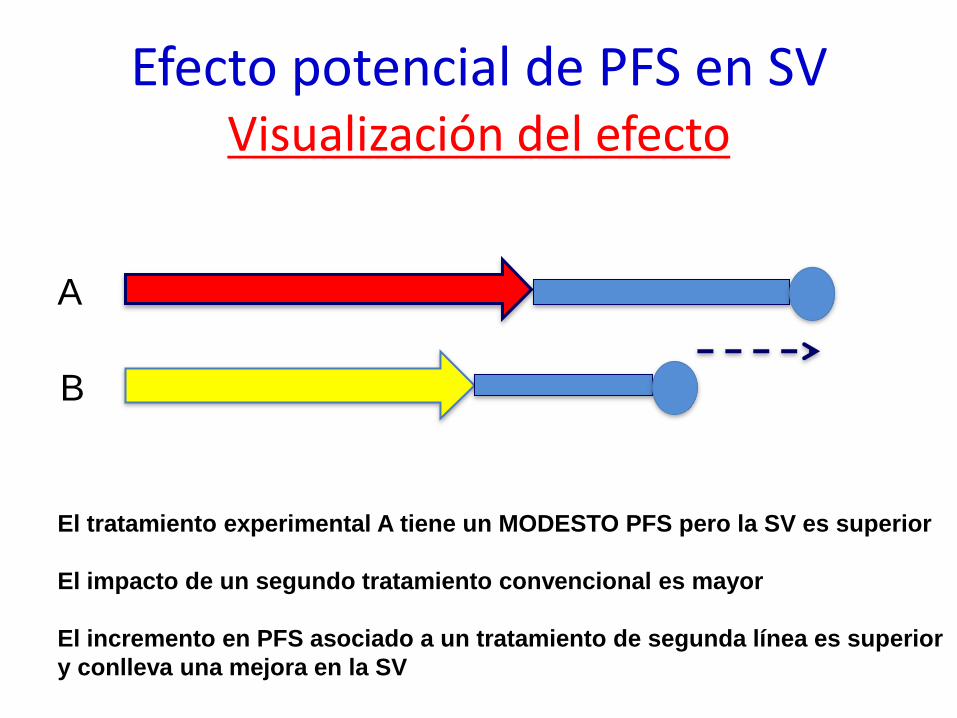
Efecto potencial de PFS en SV Visualización del efecto
A
B
El tratamiento experimental A tiene un MODESTO PFS pero la SV es superior
El impacto de un segundo tratamiento convencional es mayor
El incremento en PFS asociado a un tratamiento de segunda línea es superior
y conlleva una mejora en la SV
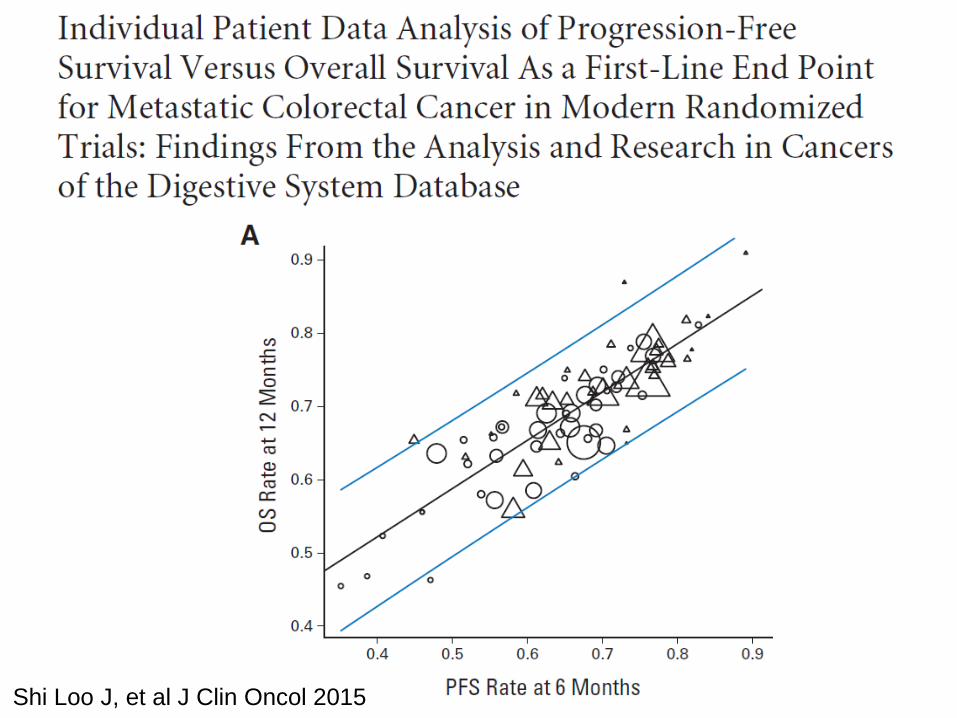
Shi Loo J, et al J Clin Oncol 2015
314 | JUNE 2010 | VOLUME 7 www.nature.com/ nrclinonc
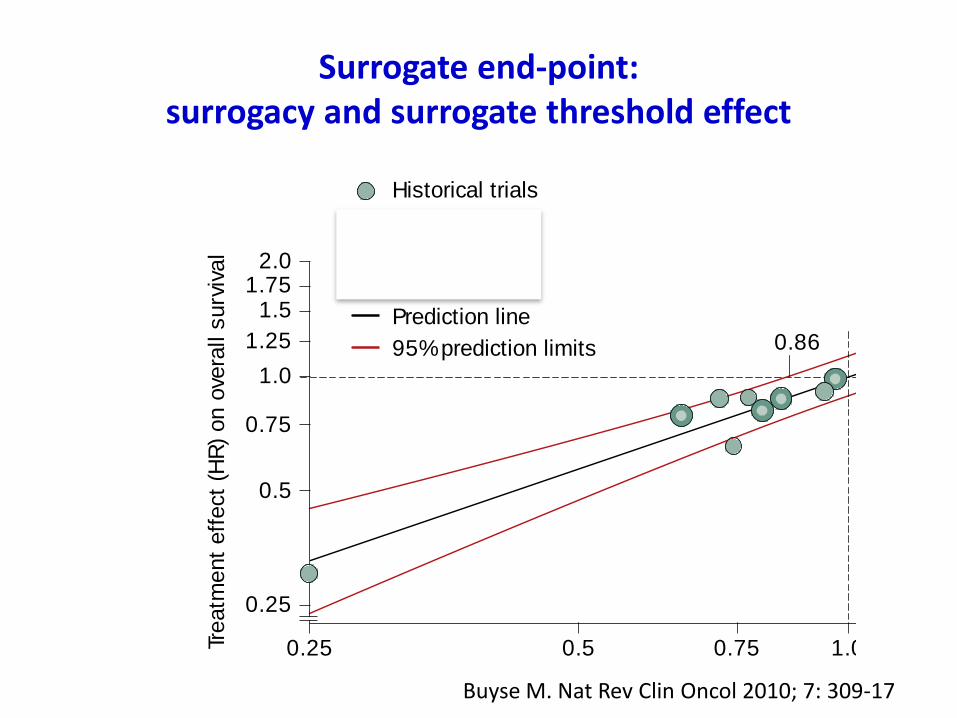
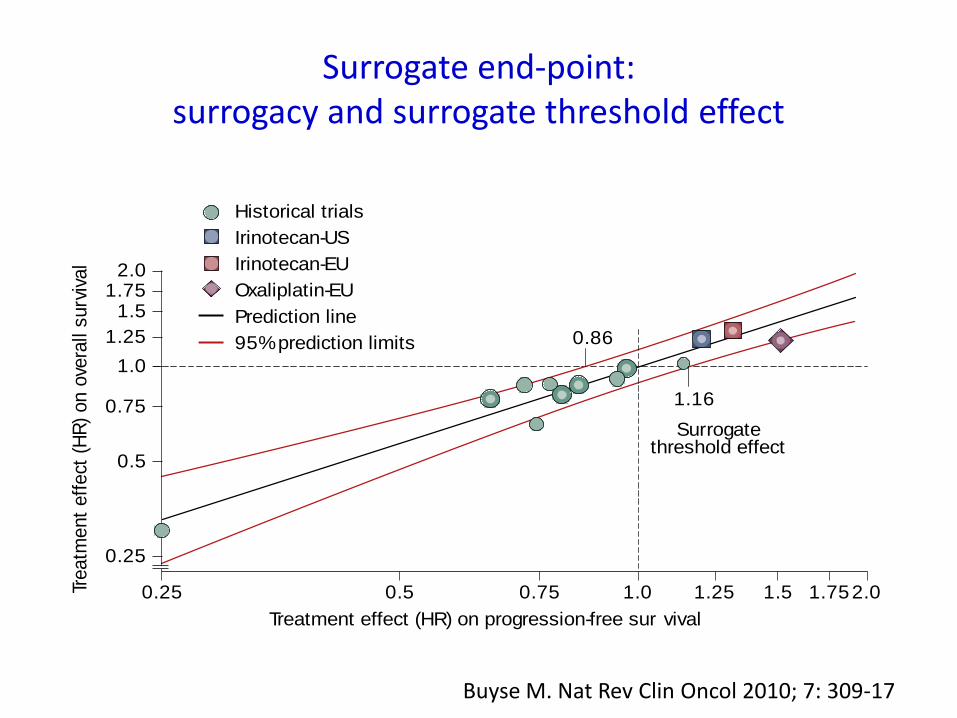
being correlated (‘tr ial-level’ surrogacy) (Figures 2
and 3).66 On the basis of a historical series of 10 random-
ized trials evaluating fluoropyrimidine-based treatment,
the surrogate threshold effect was equal to 0.86, or 0.77
after elimination of a highly influential trial, indicating
that if a new treatment reduced the hazard of tumor
progression by at least 23%, it would be very likely to
produce a benefit on survival (Figure 3).65
A major difficulty for the validation of surrogate end
points, however, arises from the fact that they are vali-
dated with respect to a specific treatment or set of treat-
ments. For a new treatment with a novel mechanism of
action, it is uncertain if the same surrogacy relationship is
applicable to that demonstrated for previous treatments.
For instance, in first-line trials in advanced colo rectal
cancer, PFS has not yet been demonstrated to be a surro-
gate for overall survival with respect to novel targeted
therapies such as bevacizumab (Avastin®, Genentech, San
Francisco, CA), panitumumab and cetuximab. The ques-
tion arises as to whether it is reasonable to assume that a
surrogacy that was demonstrated for prior therapeutics
can legitimately be treated as a surrogate in clinical assess-
ment of every new treatment that emerges. A further dif-
ficulty arises from the fact that treatment options evolve
with time. For instance, PFS was validated as a surrogate
for classical 5-fluorouracil-based chemotherapy in colo-
rectal cancer before the introduction of novel cyto toxics
and targeted therapies, which now provide a greater
range of salvage therapies. Had such therapies been
available at an earlier stage in the evo lu tion of colorectal
cancer treatment, it is unlikely that the surrogacy of PFS
for overall survival would have been demonstrated for
5- fluorouracil-based chemotherapy.66
Indeed, as standards of care in clinical oncology evolve,
the difficulties of demonstrating surrogacy between
proximal end points and overall survival will inevit-
ably mount as the number of active treatment options
increase and survival is extended. A recent study in the
area of advanced breast cancer found that although tumor
response, PFS, disease control and time-to-disease pro-
gression were all associated with overall survival at an
individual-level, none had a sufficiently strong associ ation
at trial-level to qualify as a validated surrogate end point.67
An example of this situation was demon strated in a large
trial of bevacizumab in advanced breast cancer whereby
bevacizumab treatment was associated with a highly
signifi cant PFS benefit, but no overall survival benefit.68
These observations suggest that it might be difficult to
formally establish PFS as a surrogate for overall survival
in solid tumors for which several lines of treatment are
currently available, but this does not imply that PFS does
not have utility as an end point in its own right. Indeed,
PFS might be the only sensitive (and realistic) end point
for drug evaluation, given the availability of multiple
active therapeutic lines (all of which have the potential to
improve overall survival).69
Strict or pragmatic validat ion?The current shortage of validated predictive and surro-
gate biomarkers in oncology reflects not only the statisti-
cal challenges discussed in this article, but difficulties at
every stage of the discovery and evaluation process.70 The
US National Cancer Institute’s Early Detection Research
Network has proposed five distinct phases for the devel-
opment of biomarkers for early cancer detection.70,71 In
Table 3, we adapt these five phases to the development
of any biomarker, and outline the current status of
MammaPrint® with respect to these phases as an example.
One of the greatest challenges of validation is the lack of
availability of both high-quality biological samples and
standardized measures of response from all major trials,
whether the trials are run by government-funded agen-
cies or by industry. Regulatory authorities, such as the
European Medicines Agency (EMEA) and the FDA should
consider making stipulations to alleviate this problem
to their industry and academic partners. For example,
the generation of multi-trial tissue banks and databases
would accelerate the search for bio markers and provide
a resource for retrospective analysis. The Foundation for
the NIH Biomarkers Consortium in the USA represents a
welcome but modest step in this direction.72
Despite the difficulties involved, the next few years are
likely to see the accumulation of an increasing number of
biomarker candidates with varying degrees of statistical
Figure 2 | Progression-free survival (PFS) and overall survival (OS) in advanced
colorectal cancer.
Figure 3 | Surrogate end point in advanced colorectal cancer: ‘trial level’ (effect)
surrogacy and surrogate threshold effect.
543210
0.0
0.25
Time (years)
5-FU + LV, PFS
5-FU/ raltitrexed, PFS
Irinotecan/ oxaliplatin, PFS
5-FU + LV, OS
5-FU/ raltitrexed, OS
Irinotecan/ oxaliplatin, OS
0.5
0.75
1.0
Ove
rall/pro
gre
ssio
n-fre
e s
urv
ival
1.751.51.251.00.5 0.750.25
0.25
0.75
0.5
Treatment effect (HR) on progression-free sur vival
Surrogatethreshold effect
Historical trials
Irinotecan-US
Prediction line
Irinotecan-EU
Oxaliplatin-EU
95% prediction limits
1.16
0.86
Treatm
ent
eff
ect
(HR
) on o
vera
ll s
urv
ival
1.0
1.25
1.75
2.0
1.5
2.0
REVIEWS
nrclinonc_43_JUN10.indd 314 12/5/10 14:51:56
© 20 Macmillan Publishers Limited. All rights reserved10
Buyse M. Nat Rev Clin Oncol 2010; 7: 309-17
Surrogate end-point: surrogacy and surrogate threshold effect
Surrogate end-point: surrogacy and surrogate threshold effect
314 | JUNE 2010 | VOLUME 7 www.nature.com/ nrclinonc
being correlated (‘tr ial-level’ surrogacy) (Figures 2
and 3).66 On the basis of a historical series of 10 random-
ized trials evaluating fluoropyrimidine-based treatment,
the surrogate threshold effect was equal to 0.86, or 0.77
after elimination of a highly influential trial, indicating
that if a new treatment reduced the hazard of tumor
progression by at least 23%, it would be very likely to
produce a benefit on survival (Figure 3).65
A major difficulty for the validation of surrogate end
points, however, arises from the fact that they are vali-
dated with respect to a specific treatment or set of treat-
ments. For a new treatment with a novel mechanism of
action, it is uncertain if the same surrogacy relationship is
applicable to that demonstrated for previous treatments.
For instance, in first-line trials in advanced colo rectal
cancer, PFS has not yet been demonstrated to be a surro-
gate for overall survival with respect to novel targeted
therapies such as bevacizumab (Avastin®, Genentech, San
Francisco, CA), panitumumab and cetuximab. The ques-
tion arises as to whether it is reasonable to assume that a
surrogacy that was demonstrated for prior therapeutics
can legitimately be treated as a surrogate in clinical assess-
ment of every new treatment that emerges. A further dif-
ficulty arises from the fact that treatment options evolve
with time. For instance, PFS was validated as a surrogate
for classical 5-fluorouracil-based chemotherapy in colo-
rectal cancer before the introduction of novel cyto toxics
and targeted therapies, which now provide a greater
range of salvage therapies. Had such therapies been
available at an earlier stage in the evo lu tion of colorectal
cancer treatment, it is unlikely that the surrogacy of PFS
for overall survival would have been demonstrated for
5- fluorouracil-based chemotherapy.66
Indeed, as standards of care in clinical oncology evolve,
the difficulties of demonstrating surrogacy between
proximal end points and overall survival will inevit-
ably mount as the number of active treatment options
increase and survival is extended. A recent study in the
area of advanced breast cancer found that although tumor
response, PFS, disease control and time-to-disease pro-
gression were all associated with overall survival at an
individual-level, none had a sufficiently strong associ ation
at trial-level to qualify as a validated surrogate end point.67
An example of this situation was demon strated in a large
trial of bevacizumab in advanced breast cancer whereby
bevacizumab treatment was associated with a highly
signifi cant PFS benefit, but no overall survival benefit.68
These observations suggest that it might be difficult to
formally establish PFS as a surrogate for overall survival
in solid tumors for which several lines of treatment are
currently available, but this does not imply that PFS does
not have utility as an end point in its own right. Indeed,
PFS might be the only sensitive (and realistic) end point
for drug evaluation, given the availability of multiple
active therapeutic lines (all of which have the potential to
improve overall survival).69
Strict or pragmatic validat ion?The current shortage of validated predictive and surro-
gate biomarkers in oncology reflects not only the statisti-
cal challenges discussed in this article, but difficulties at
every stage of the discovery and evaluation process.70 The
US National Cancer Institute’s Early Detection Research
Network has proposed five distinct phases for the devel-
opment of biomarkers for early cancer detection.70,71 In
Table 3, we adapt these five phases to the development
of any biomarker, and outline the current status of
MammaPrint® with respect to these phases as an example.
One of the greatest challenges of validation is the lack of
availability of both high-quality biological samples and
standardized measures of response from all major trials,
whether the trials are run by government-funded agen-
cies or by industry. Regulatory authorities, such as the
European Medicines Agency (EMEA) and the FDA should
consider making stipulations to alleviate this problem
to their industry and academic partners. For example,
the generation of multi-trial tissue banks and databases
would accelerate the search for bio markers and provide
a resource for retrospective analysis. The Foundation for
the NIH Biomarkers Consortium in the USA represents a
welcome but modest step in this direction.72
Despite the difficulties involved, the next few years are
likely to see the accumulation of an increasing number of
biomarker candidates with varying degrees of statistical
Figure 2 | Progression-free survival (PFS) and overall survival (OS) in advanced
colorectal cancer.
Figure 3 | Surrogate end point in advanced colorectal cancer: ‘trial level’ (effect)
surrogacy and surrogate threshold effect.
543210
0.0
0.25
Time (years)
5-FU + LV, PFS
5-FU/ raltitrexed, PFS
Irinotecan/ oxaliplatin, PFS
5-FU + LV, OS
5-FU/ raltitrexed, OS
Irinotecan/ oxaliplatin, OS
0.5
0.75
1.0
Ove
rall/
pro
gre
ssio
n-fre
e s
urv
ival
1.751.51.251.00.5 0.750.25
0.25
0.75
0.5
Treatment effect (HR) on progression-free sur vival
Surrogatethreshold effect
Historical trials
Irinotecan-US
Prediction line
Irinotecan-EU
Oxaliplatin-EU
95% prediction limits
1.16
0.86
Treatm
ent
eff
ect
(H
R)
on o
vera
ll surv
ival
1.0
1.25
1.75
2.0
1.5
2.0
REVIEWS
nrclinonc_43_JUN10.indd 314 12/5/10 14:51:56
© 20 Macmillan Publishers Limited. All rights reserved10
Buyse M. Nat Rev Clin Oncol 2010; 7: 309-17
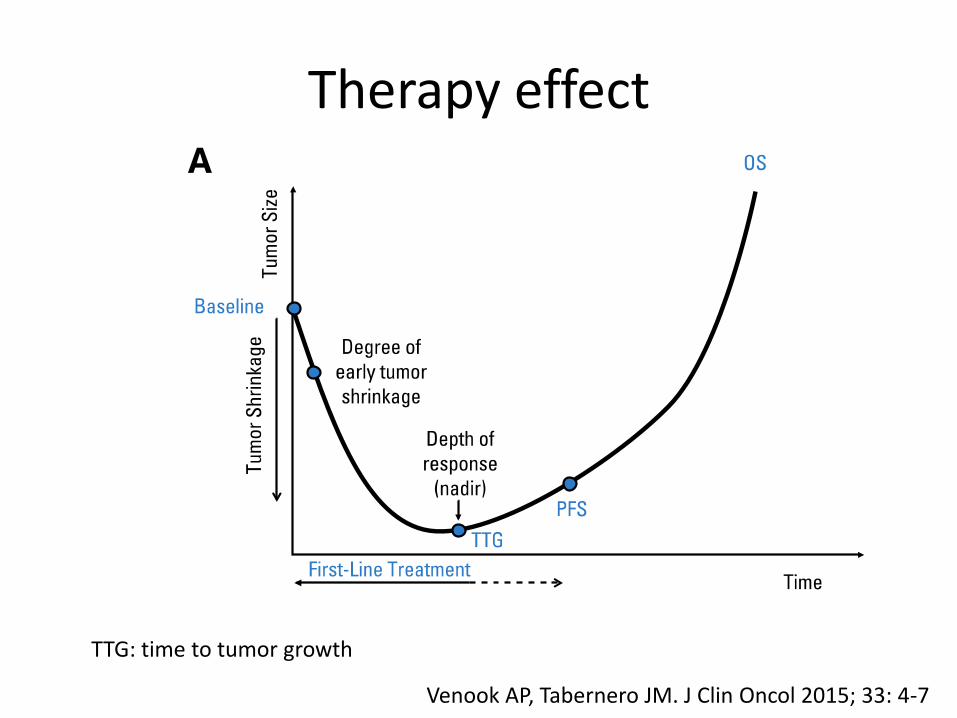
Therapy effect
TTG: time to tumor growth
Venook AP, Tabernero JM. J Clin Oncol 2015; 33: 4-7
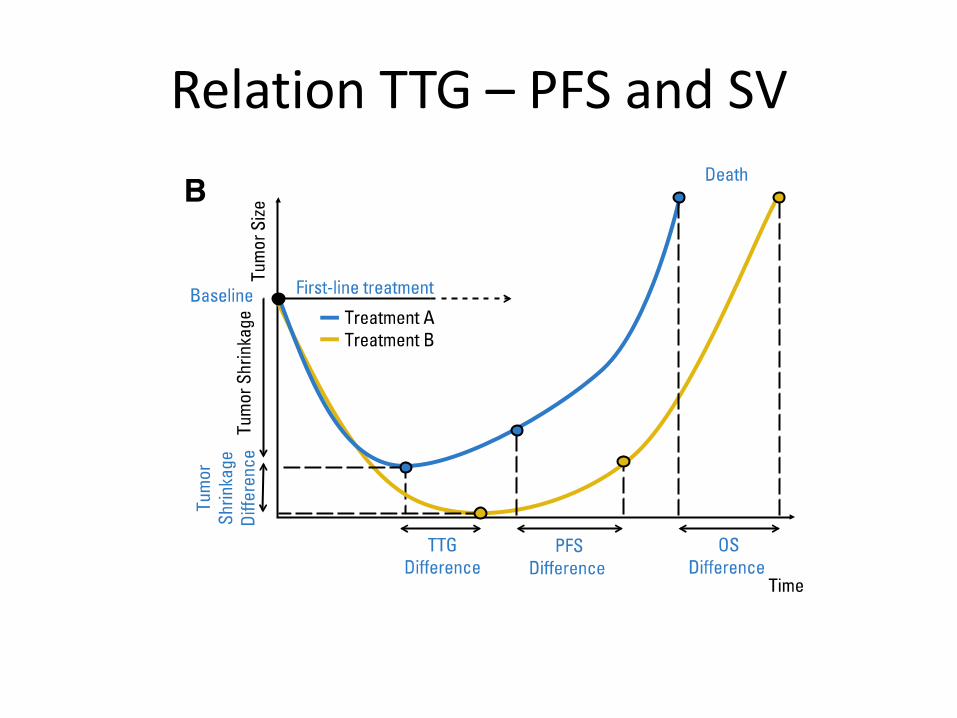
Relation TTG – PFS and SV
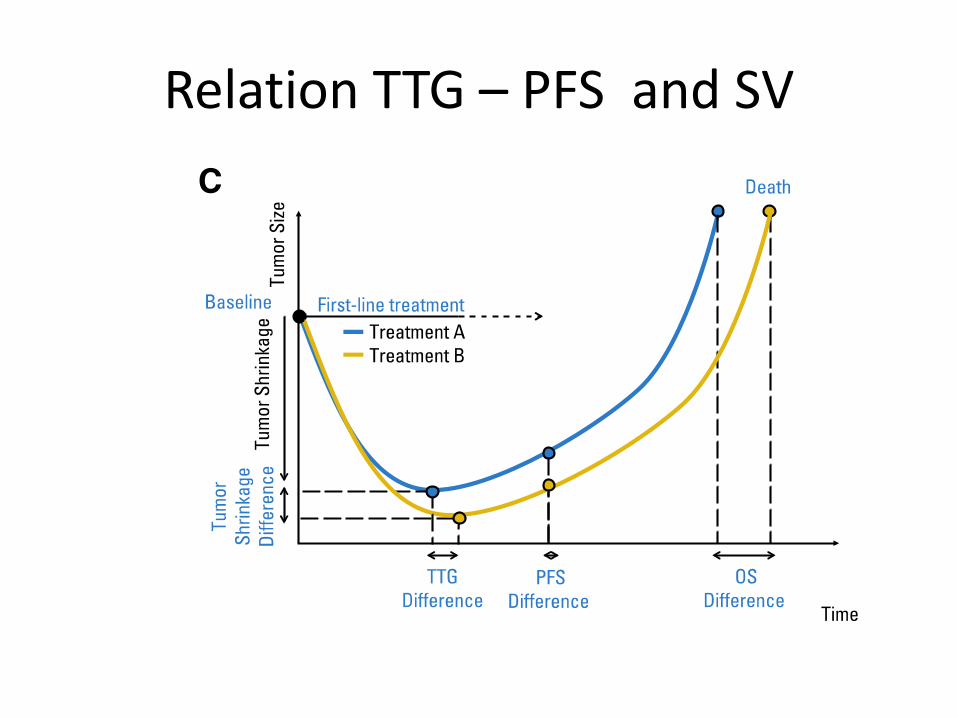
Relation TTG – PFS and SV
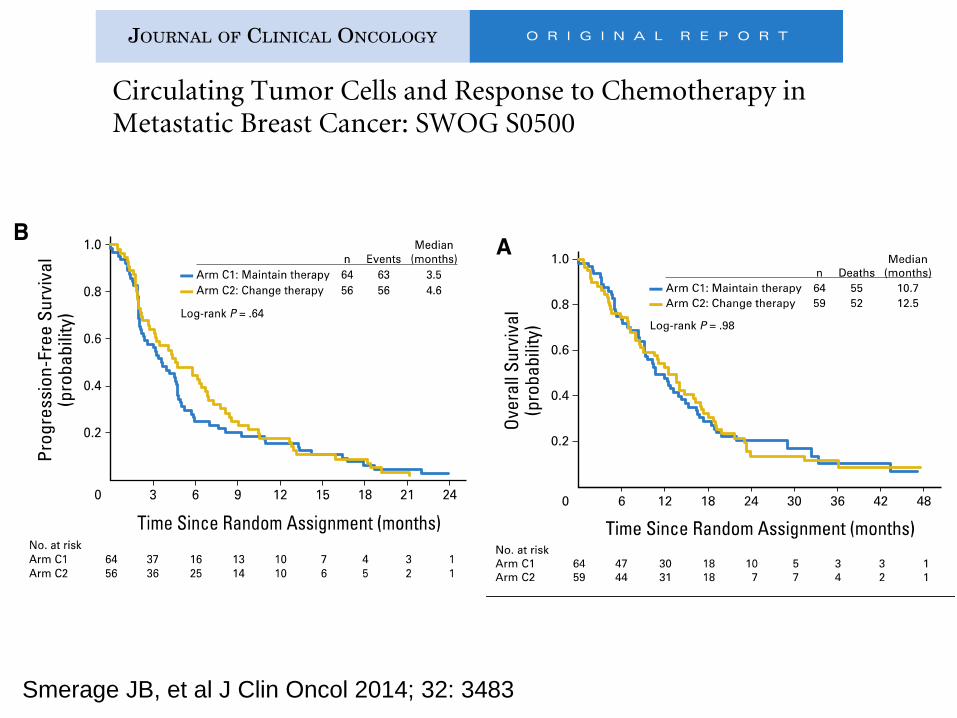
Smerage JB, et al J Clin Oncol 2014; 32: 3483
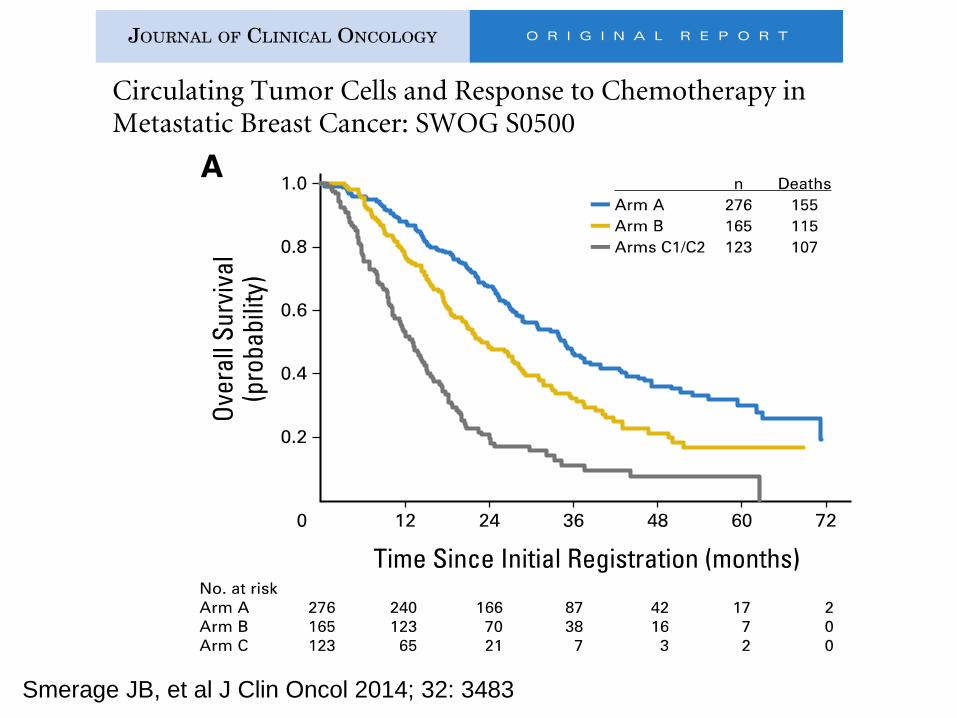
Smerage JB, et al J Clin Oncol 2014; 32: 3483
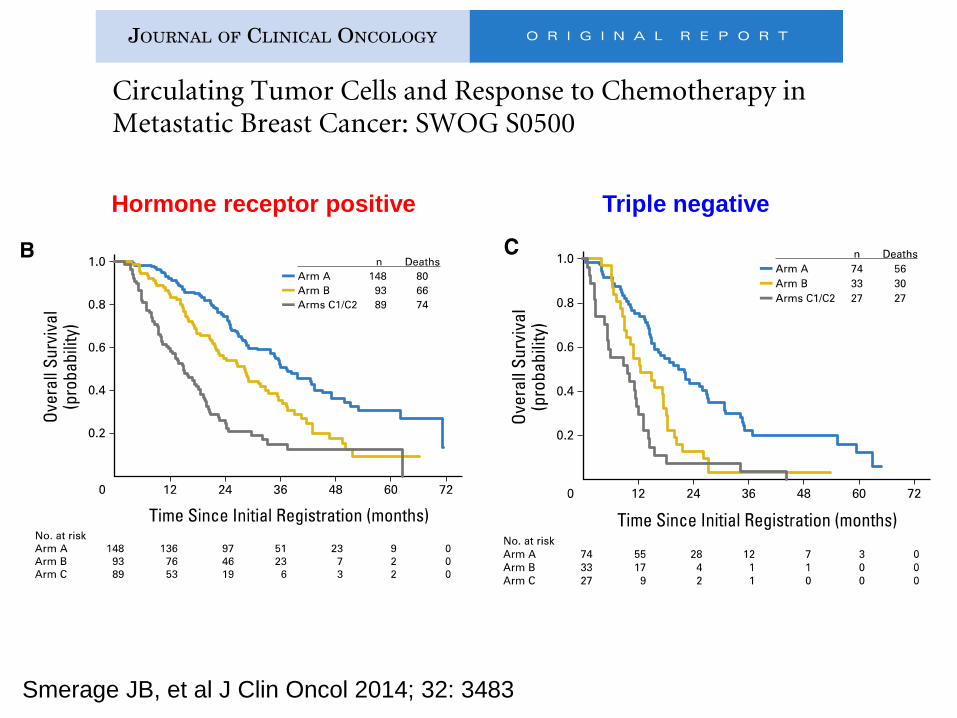
Hormone receptor positive Triple negative
Smerage JB, et al J Clin Oncol 2014; 32: 3483
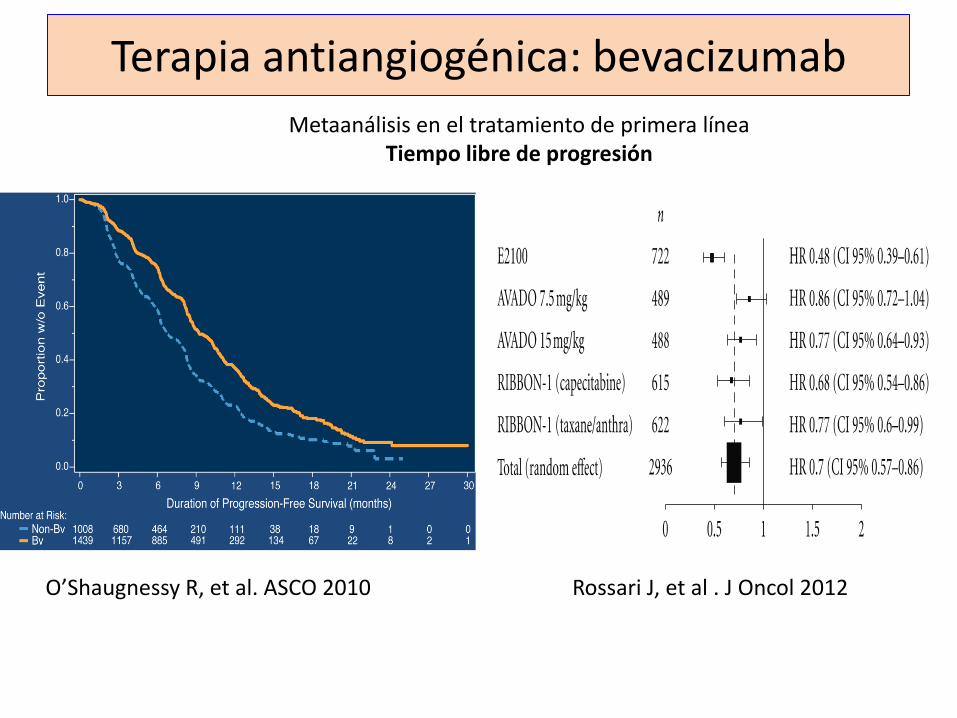
Terapia antiangiogénica: bevacizumab
O’Shaugnessy R, et al. ASCO 2010 Rossari J, et al . J Oncol 2012
Metaanálisis en el tratamiento de primera línea Tiempo libre de progresión
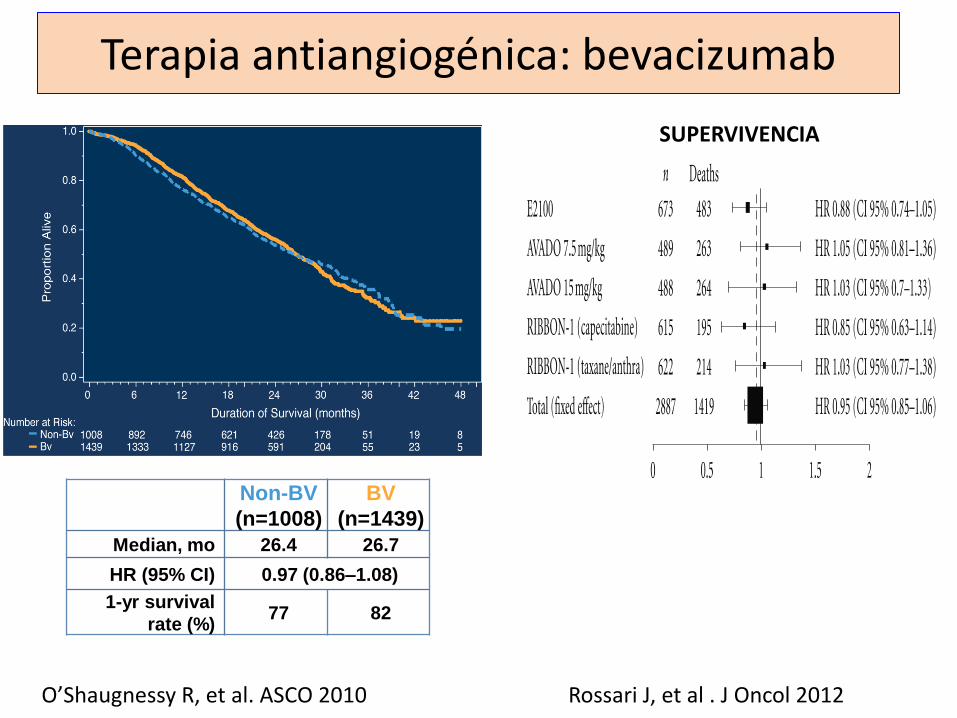
Non-BV
(n=1008)
BV
(n=1439)
Median, mo 26.4 26.7
HR (95% CI) 0.97 (0.86–1.08)
1-yr survival
rate (%) 77 82
Terapia antiangiogénica: bevacizumab
O’Shaugnessy R, et al. ASCO 2010 Rossari J, et al . J Oncol 2012
SUPERVIVENCIA
“Despite the reduced ability to predict overall survival in modern trials, we feel that PFS
remains an appropriate end point for first-line superiority trials in advanced disease”
Quian S, De Gramont A, et al. J Clin Oncol 2015; 33: 22-28

Definición y objetivos
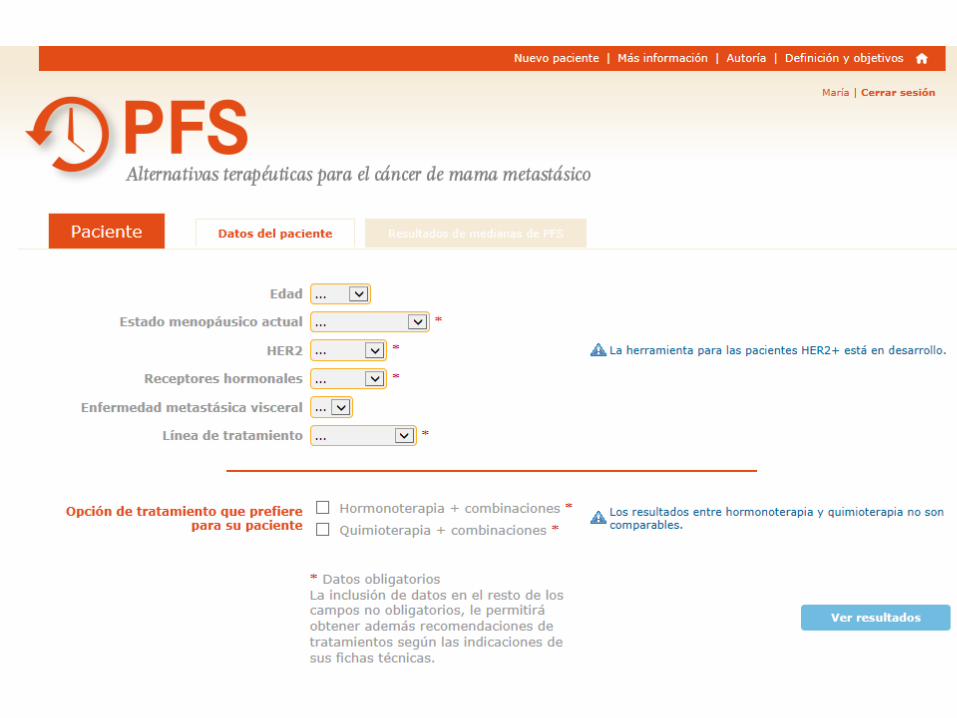
PFS online: herramienta de ayuda al clínico para visualizar el beneficio que aportan diferentes estrategias de tratamiento para la enfermedad avanzada
Se fundamenta en la evidencia disponible a partir de los resultados de los estudios fase III y metaanálisis
Incorpora información adicional con: Descripción de la población de los estudios seleccionados
Enlace con las referencias bibliográficas
Las fichas técnicas de los fármacos: EMA/AEMPs
Selección bibliográfica
Bases de datos: PubMed y Google Scholar.
Palabras clave: • Por ejemplo, para inhibidores de aromatasa: ("advanced breast cancer"
OR "advanced breast carcinoma") AND ("endocrine therapy" OR "tamoxifen") AND ("aromatase inhibitor" OR "anastrozole" OR "letrozole" OR "exemestane").
Filtros: • Tipo de artículo: “clinical trial” y “meta-analysis”.
• From 1999 (dado el tiempo transcurrido desde la introducción de los inhibidores de aromatasa).
Búsqueda manual de artículos clave.
Selección de los artículos de referencia
Extracción y validación de la información de cada artículo
• Cálculo de las medianas PFS: se utiliza el modelo paramétrico de Weibull
S(t)=exp(-α.tγ ) • La mediana de PFS se calcula a partir de los parámetros del
modelo
Med=(log(2) /α)1/γ
• El modelo permite incorporar las HR entre tratamientos asumiendo el principio de riesgos proporcionales
S2(t)=S1(t)HR = exp(-α.tγ )HR
Fundamentos estadísticos
Variables consideradas
Edad.
Estado menopáusico.
HER2 y receptores hormonales.
Afectación visceral.
Tratamientos previos administrados.
Intervalo hasta metástasis.
Indicaciones de ficha técnica.
Opción de tratamiento preferida por el clínico para cada paciente.

Trabajo desarrollado (siguiendo las indicaciones aprobadas por AEMPs)
Terapia endocrina 1ª , 2ª línea
Quimioterapia 1ª, 2ª línea
Terapia antiangiogénica
“En construcción”: • Primera línea terapia anti-HER2
• Segunda línea terapia anti-HER2
Próximos objetivos
• Acceso en: http://www.pfsonline.es
• Estudio de validación prospectivo: REGISTREM

Comité científico Agustí Barnadas Molins Teresa Ramón y Cajal César A. Rodríguez Sánchez
Comité Asesor Isabel Álvarez López Lourdes Calvo Martínez Eva Carrasco Ana Lluch Hernández Miguel Martín Jiménez Miguel Ángel Seguí Palmer
GEICAM Roser Trilla
Agradecimientos
NPGI María José Jerez Paula Peral
Metodología Jesús Herranz Xavier Mas
Novartis Marion Chalumeau Ariela Beliera Cristina Puig






















![MARCADORES TUMORALES[1].ppt](https://img.pdfslide.tips/doc/110x75/55cf884655034664618f3227/marcadores-tumorales1ppt.jpg)





