-
PENATALAKSANAAN HIPERTENSI
TERKINI :
FOKUS PADA JNC 8
WACHID PUTRANTO
Divisi Ginjal Hipertensi
Fakultas Kedokteran UNS/RS.Dr. Moewardi
Surakarta
-
Suatu keadaan klinis dimana tekanan darah seseorang lebih tinggi
daripada tekanan darah normal
Epidemiologi :
Jumlah penderita hipertensi di seluruh dunia :
1 milyar
USA : 65 juta
Indonesia ? : belum ada data resmi
Conlin PR, Int J Clin Pract 2005; 59(2):214-24
-
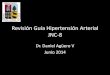
Franklin, S.S., J Hypertens 1999; 17 (suppl 5): S29-S36
0
10
20
30
40
50
60
70
18-29 30-39 40-49 50-59 60-69 70-79 80+
SBP > 140 mm Hg DBP > 90 mm Hg
age (yrs)
pre
vale
nce
of
hyp
ert
en
sio
n (
%)
4 11
21
44
54
64 65
Prevalensi Hipertensi
-
Hypertension complication
Damages depend on:
How high of the blood pressures
How long the uncontrolled and
untreated high blood
presure
Target Organ damage!! Eyes retinopathy
Kidneys renal failure
Brain stroke
Heart ischaemic heart disease
left ventricular hypertrophy heart failure
Peripheral arterial disease
-
Blood Pressure Reduction Of 2 mmHg Reduces The Risk Of CV Events
by 710%
Meta-analysis of 61 prospective, observational studies
1 million adults
12.7 million person-years
Lewington et al. Lancet 2002;360:190313
2 mmHg decrease in mean SBP
10% reduction in risk of stroke mortality
7% reduction in risk of ischaemic heart disease mortality
-
HYPERTENSION GUIDELINES
ASH/ISH
-
CLASSIFICATION HYPERTENSION
BP SBP DBP
Normal
-
Topic JNC 7 2014 Hypertension Guidelin
Methodology Non systematic literature review by Critical
questions and review criteria defined by expert expert committee
including a range panel with input from methodology team of study
design Initial systematic review by methodologist restricted to
Recommendation based on consensus RCT evidence Subsequent review of
RCT evidence and recommendations by the panel according to a
standardized protocol Definitions Defined hypertension and
prehypertension Definision of hypertension and prehypertension not
addressed, but tresholds for pharmacologic treatment were defined
Treatments Separate treatmen goals defined for Similar treatment
goals defined for all hypertensive Goals uncomplicated hypertension
and for populations except when evidence review supports subsets
with various comorbid condition different goals for a particular
subpopulation Lifestyle Recommended lifestyle modifications
Lifestyle recommendations recommended by endorsing Recommendation
based on literature review and expert the evidence based
recommendations of the Lyfestyle opinion Work Group Drug therapy
Recommended 5 classes to be considered Recommended selection among
4 specific medications as initial therapy for most patients without
classes ( ACEI or ARB, CCB or Diuretics) and doses based compelling
indication for another class on RCT evidence Specified particular
antihypertensive Recommended specific medication classes based on
medication classes for patients with evidence review for racial,
CKD, and diuretics sub group compelling
indication,ie,diabetes,CKD,heart Panel created a table of drugs and
doses used in the failure,myocardial infarction,stroke,high outcome
trials CVD risk
-
Included a comprehensive table oral Antihypertensive drugs
including names and usual dose ranges Scope of topics Addressed
multiple issues ( blood pressure Evidence review of RCTS addressed
a limited measurements methods,patients evaluation number of
questions,those judge by the panel components,secondary
hypertension, to be of highest priority adherence to
regimens,resistant hypertension, and hypertension in special
populations) based on literature review and expert opinion Review
process Reviewed by the National High Blood pressure Reviewed by
experts including those affiliated Prior to Education Program
Coordinating Committee, with professional and public organizations
and Publication a coalition of 39 major professional,public, and
federal agencies; no official sponsorship by any voluntary
organizations and 7 federal agencies organization should be
inferred
-
The Process
Literature review 1/1/1966 12/31/2009
Inclusion Criteria (1) HTN (2) 2000 participants (3) multisenter
(4) Kriteria inklusi/eksklusi.
9 Recommendations
-
A
C
B
N
D
E
-
Recommendation
Strength of Recommendation
Recommendation 1 Populasi berusia 60 yrs,mulai terapi
farmakologi SBP150 mmHg, DBP90 mmHg
Grade A
HYVET, Sys-Eur, SHEP, JATOS, VALISH, CARDIO-SIS
Corollary Recommendation Populasi usia 60 yrs, jika terapi
farmakologi mengakibatkan penurunan TD lebih rendah (
-
Recommendation
Strength of Recommendation
Recommendation 3 Populasi usia
-
Recommendation
Strength of Recommendation
Recommendation 6 Pada populasi non black , termasuk dg DM,
initial anti HTN treatment : a thiazide type diuretic, CCB, ACEI or
ARB
Grade B
VA-cooperative, HDFP, SHEP
Recommendation 7 Populasi kulit hitam, termasuk dg DM, initial
anti HT: thiazide-type diuretic or CCB
Grade B ( No DM)
Grade C ( DM)
ALLHAT
Recommendation 8 Populasi usia 18 dg CKD dan HTN, initial (or
add on) anti HTN : ACEI or ARB utk memperbaiki kidney outcomes.
Tanpa melihat ras atau status DM
Grade B
IDNT, AASK
-
Recommendation Strength of Recommendation
Recommendation 9 Tujuan treatment HTN adalah untik mencapai
dan
mempertahankan target BP Jika target BP tidak tercapai dlm 1 bl,
naikkan dosis
atau tambahkan 2nd 1 obat dr rekomendasi 6 (thiazide-type
diuretic, CCB, ACEI, or ARB)
Jika target BP tidak tercapai dg 2 obat, tambah dan titrasi obat
3rd . Do not use an ACEI and an ARB together
Jika target BP tidak dapat tercapai dg obat-obat pada
recommendasi 6 krn kontraindikasi atau butuh >3 obat, obat
antiHT dari kelas lain bias digunakan.
Referral kepada hypertension specialist jika BP tidak tercapai
atau untuk management komplikasi.
Grade E
-
Strategies to Dose Antihypertensive Drugs
Strategies Description Details
A Mulai 1 obat naikan sp dosis maksimum,kemudian tambahkan obat
ke-2
Jika target BP blm tercapai naikkan dosis obat 1 sp dosis
maksimum sblm menambahkan obat ke-2 dan ke-3.
B Mulai 1 obat kemudian tambahkan obat ke-2 sblm dosis
maksimum
Tambahkan obat ke-2 sblm obat 1 mencapai dosis maks.Jk Target BP
blm tercapai,tambahkan obat ke-3 dan titrasi sp dosis maks.
C Mulai dengan 2 obat (separate or single combination)
Mulai dg 2 obat Bbrp committee merekomendasi: 2 obat SBP >160
dan/atau DBP
>100, atau SBP >20 mmHg diatas target dan/atau DBP >10
mmHg
Jika target BP tdk tercapai (2 drugs), tambahkan obat ke-3 dan
titrasi.
-
Lifestyle Modification
-
JNC 8
-
JNC 7
-
Guideline Population Goal BP Initial drugs
2014 HT Guideline
General 60 y General
-
Guideline Population Goal BP Initial drugs
ADA DM
-
Important Variables For HTN Recommendations
BP NICE ESC/ESH ASH/ISH AHA/ACC/CDC
JNC 7 JNC 8
Definition HTN
140/90 and
daytime ABPM
135/85
140/90 140/90 140/90 Pre HT 120-139 or 80-89 Stg 1 HT
140-159 or 90-99
Stg 2 HT 160 or 100
Not addressed
Drug th/ in low risk pts after non pharm th/
160/100 or daytime ABPM 150/95
140/90 140/90 140/90 140/90
-
NICE ESH/ESC ASH/ISH AHA/ACC/CDC
JNC 7 JNC 8
Diuretic Chorthali-done (CTD)
Indapami- de (IND)
Thiazides (THZ), CTD ND
THZ CTD IND
THZ THZ THZ CTD IDP
Initiate th/ with 2 drugs
Not mentio-
ned
Pts w/ markedly
elevated BP
160/90 160/100 160/100 Not mentioned
BP target
-
Under JNC 8, in all cases, targets BP should be reached within a
month of starting treatment either by increasing the dose or by
using a combination drugs
In patients 60 yrs who do not have DM or CKD, the goal BP level
is
-
Under the JNC 8 guidelines, patients would receive a dosage
adjustment and combinations of the 4 first-line & later line
therapies ACEI/ARB, CCB, and thiazide-type diuretic
The JNC 8 does not recommend -blockers and -blockers as 1st
therapy due to 1 trial that showed a higher rate of CV events with
use of B compared with use of an ARB, and another trial in which B
resulted in inferior CV outcomes compared with use of a
diuretic
JNC 8 also recommend lifestyle interventions include use of the
DASH eating plan, weight loss, reduction in sodium intake to
-
When initiating therapy, patients of African descent without CKD
should use CCBs and thiazides instead of ACE inhibitors
ACE inhibitors and ARBs should not be used in the same patient
simultaneously