-
8/17/2019 PR siapa ya
1/18
1. PAS (Peripheral Anterior Synechia)
PAS is adhesions between the iris and posterior surface of the
cornea. ccc Today, peripheral
anterior synechiae are a well-recognized consequence of altered
anterior
chamber (AC) anatomy and anterior chamber inammation. !eripheral
anterior
synechiae can subsequently result in signi"cant morbidity as a
precipitant to
secondary angle-closure glaucoma.
http://emedicine.medscape.com/article/1206956-overviewhttp://emedicine.medscape.com/article/1206956-overview
-
8/17/2019 PR siapa ya
2/18
Pathophysiology
Peripheral anterior synechiae may form under the following 2
circumstances: a nonproliferative state or a
proliferative state.
Apposition of the iris against the trabecular meshwor as a
result of pupil bloc or a posterior pushing
mechanism without any inflammation can result in continuous
peripheral anterior synechiae. !hese
continuous peripheral anterior synechiae lead to "#ippering" of
the angle. Primary angle$closure glaucoma
and the various posterior pushing mechanisms are e%amples of
this process.
&n the presence of inflammation or cellular proliferation' a
membrane forms between the iris and the
trabecular meshwor' creating the peripheral anterior synechiae.
!his membrane contracts' resulting in
angle$closure glaucoma by an anterior pulling mechanism. %amples
of this process include the
fibrovascular membrane formed in neovascular glaucoma'
proliferating abnormal endothelial cells in the
iridocorneal endothelial (&) syndromes' epitheliali#ation of
the angle due to epithelial ingrowth' or inflammatory
trabecular and eratic precipitates in contact with an inflamed
iris. !hese processes can be
accentuated by iris swelling and protein transudation and
e%udation.
Physical
As a general principle' e%amination of the nonaffected eye in
unilateral presentations may prove to be
valuable in trying to discern between primary and secondary
etiologies of angle closure.
• *efraction: +yperopia is a ris factor for angle closure.
• ,onioscopy
o -eiss compression
-eiss compression should be performed to distinguish
appositional closure from
synechial closure in narrow$angle glaucoma.
Areas where an abrupt change in the angle from open to closed is
present suggest
the presence of peripheral anterior synechiae.
&f not visuali#ed directly' synechial presence can be
indicated by the lac of
displacement of the focal lines reflected from the posterior
surface of the cornea
and the anterior surface of the iris. hen peripheral anterior
synechiae are not
present' a displacement will be noted with compression
gonioscopy.
&t is imperative that the entire circumference of the angle
be e%amined for an
open' normal$looing angle and compared to the regions of
peripheral anterior
synechiae to estimate the filtration capabilities of the
eye.
-
8/17/2019 PR siapa ya
3/18
!he point of anterior attachment of peripheral anterior
synechiae should be noted
because peripheral anterior synechiae that obstruct the
central third of the
trabecular meshwor are more liely to result in increased
intraocular pressure.
!able 1. /escription of PAS on gonioscopy (0pen !able in a
new window)
• Prominent uveal meshwor (must be differentiated from
peripheral anterior synechiae)
o an be confused for peripheral anterior synechiae
o ore common and e%tensive in brown irides compared to blue
eyes
o +as a lacy and porous appearance through which angle
structures can be visuali#ed this
can be enhanced with transillumination
o A%enfeld and *ieger anomalies (anterior segment dysgenesis)
may have anterior
prominent uveal meshwor with an anterior displaced
Schwalbe line' which is not
believed to be true peripheral anterior synechiae.
• ornea
o 3eratic precipitates would indicate an inflammatory
etiology.
o Polymorphous opacities at the /escemet membrane level suggest
posterior
polymorphous dystrophy (PP/).
o orneal guttata and4or edema are suggestive of handler
syndrome.
http://reftableshow%28%27layertablet852abe899%27%29/http://reftableshow%28%27layertablet852abe899%27%29/
-
8/17/2019 PR siapa ya
4/18
o ongenital corneal opacities or sclerocornea suggest a
congenital corneal defect (anterior
segment dysgenesis).
o Posterior embryoto%on
• Anterior chamber depth
o &f the peripheral depth in this region has a corneal
thicness of one fourth or less' the
possibility of angle closure e%ists (5on +erric law).
o /istinction should be made between peripheral and central
shallowing.
o Pupil bloc commonly results in greater peripheral shallowing
as compared to the central
anterior chamber.
o Posterior pushing mechanisms result in e6ual peripheral and
central shallowing.
• &ris
o &ris atrophy may suggest previous attacs of angle$closure
glaucoma' uveitis' or anterior
segment dysgenesis.
o 3oeppe and 7usacca nodules suggest iritis.
o &rregularity of the pupil may be secondary to trauma or
inflammation.
o 8ew vessels along the anterior iris stroma and ectropion
uveae suggest neovascular
glaucoma.
o ctropion uveae' corectopia' iris stretch holes' and nevi
suggest an iridocorneal
endothelial syndrome.
o Anterior bowing of the iris may imply an element of pupil bloc
or iris bomb9.
• ens
o ,lauomflecen suggests previous attacs of angle$closure
glaucoma.
o Pseudoe%foliation is associated with #onule la%ity' which can
result in forward
displacement of the lens.
o Posterior synechiae may lead to iris bomb9.
o &ntumescent lens may cause shallowing of the anterior
chamber.
• *etina
-
8/17/2019 PR siapa ya
5/18
o Any cause of vascular compromise (eg' diabetic retinopathy'
central retinal artery
occlusion ;*A0veitis
Pupil bloc
!rauma Primary angle$closure glaucoma
http://reftableshow%28%27layertablete18154a59%27%29/http://reftableshow%28%27layertablete18154a59%27%29/http://reftableshow%28%27layertablete18154a59%27%29/http://reftableshow%28%27layertablete18154a59%27%29/
-
8/17/2019 PR siapa ya
6/18
&nflammatory syndromes
&nfectious
ens related
Posterior synechiae resulting in iris
bomb9
Pseudophaic or aphaic pupil bloc
&ridoschisis
?lat anterior chamber Plateau iris
Posterior pushing
Postsurgical
!rauma
horoidal effusion
$Posterior uveitis
$*50
$8anophthalmos
$Post$pan retinal photocoagulation(P*P) or cryotherapy
Suprachoroidal hemorrhage
iliary bloc (malignant) glaucoma
(a6ueous misdirection)
-
8/17/2019 PR siapa ya
7/18
Posterior segment tumors
$*etinoblastoma
$horoidal melanoma or metastasis
&ris cyst or tumor
iliary body cyst' tumor' or effusion
ontracting retrolental tissue
$*etinopathy of prematurity
$Persistent hyperplastic primary vitreous
(P+P5)
Postscleral bucing surgery
Anterior lens sublu%ation (ectopia lentis)
ens intumescence (phacomorphic)
8eurofibromatosis
-
8/17/2019 PR siapa ya
8/18
Argon laser trabeculoplasty
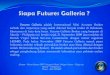
2. Anatomy of iliar 7ody
!he ciliary body is the site of a6ueous humor production and it
is totally involved in a6ueous
humor dynamics. !he ciliary body is the anterior portion of the
uveal tract' which is located
between the iris and the choroid. (figure 1)
Figure 1. +istology of human ciliary body (courtesy Prof. *uth
Santo)
0n cross$section' the ciliary body has the shape of a right
triangle' appro%imately @ mm in
length' where its ape% is contiguous with the choroid and the
base close to the iris. %ternally' it
attaches to the scleral spur creating a potential space' the
supraciliary space' between it and the
sclera. !he e%ternal surface forms the anterior insertion of the
uveal tract. !he internal surface of
the ciliary body comes in contact with the vitreous surface and
is continuous with the retina ;1
-
8/17/2019 PR siapa ya
9/18
!he pars plicata is contiguous with the iris posterior
surface and is appro%imately 2 mm in
length' B.D mm in width' and B.E$1 mm in height ;2'F
-
8/17/2019 PR siapa ya
10/18
supracoroidal lamina (fibers connecting choroid and sclera) as
far bac as the e6uator of the eye
;@
-
8/17/2019 PR siapa ya
11/18
!he maCor innervation is provided by ciliary nerve branches
(third cranial nerve$oculomotor)'
forming a rich parasympathetic ple%us. !here are also
sympathetic fibers originating from the
superior cervical ganglion which eep pace with arteries and
their branches.
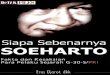
Figure 3. +istology of human ciliary epithelia
Ultrastructure of the ciliary processes
ach ciliary process is composed of a central stroma and
capillaries' covered by a double layer
of epithelium. (?&,>* F).!he ciliary process capillaries
occupy the center of each process ;1B
-
8/17/2019 PR siapa ya
12/18
!he pigmented epithelium is the outer layer' and the cuboidal
cells contain numerous melanin
granules in their cytoplasm. !his layer is separated from the
stroma by an atypical basement
membrane' a continuation of 7ruchJs membrane which contains
collagen and elastic fibers ;1D
-
8/17/2019 PR siapa ya
13/18
the conventional or canalicular system' and accounts for EF to
K@G of a6ueous outflow of normal
human eyes ;21'22
-
8/17/2019 PR siapa ya
14/18
and conCunctival veins. !he trabecular meshwor consists of
connective tissue surrounded by
endothelium. &n a meridional section' it has a triangular
shape' with the ape% at SchwalbeNs line
and the base at the scleral spur.
!he meshwor consists of a stac of flattened' interconnected'
perforated sheets' which run from
SchwalbeNs line to the scleral spur. !his tissue may be divided
into three portions: a) uveal
meshwor' b) corneoscleral meshwor and c) Cu%tacanalicular
tissue@. 7y gonioscopy' the
trabecular meshwor can be separated into two portions: an
anterior (named non$pigmented)
and a posterior (pigmented).
!he inner layers of the trabecular meshwor can be observed in
the anterior chamber angle and
are referred to as the uveal meshwor. !his portion is adCacent
to the a6ueous humor' is arranged
in bands or rope$lie trabeculae' and e%tends from the iris root
and ciliary body to the peripheral
cornea. !hese strands are a normal variant and are called by a
variety names such as iris process'
pectinated fibers' uveal trabeculae' ciliary fibers' and
uveocorneal fibers. !he deeper layers of the
uveoscleral meshwor are more flattened sheets with wide
perforations.
!he outer layers' the corneoscleral meshwor' consist of E to 1D
perforated sheets. !he
corneoscleral trabecular sheets insert into the scleral sulcus
and spur. !hese sheets are not
visible gonioscopically. !he perforations are elliptical and
become progressively smaller from
the uveal meshwor to the deep layers of the corneoscleral
meshwor ;2E
-
8/17/2019 PR siapa ya
15/18
Cunctions and have microfilaments' including actin
filaments and intermediate filaments
(vimentin and desmin) ;FB
-
8/17/2019 PR siapa ya
16/18
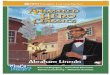
posterior chamber to anterior chamber ( seclusio
pupillae). !hus' the a6ueous collects
behind the iris and pushes it anteriorly (leading to
‘iris-bombe’ formation) . !his is
usually followed by a rise in intraocular pressure.
3. Total posterior synechiae due to plastering of total
posterior surface of iris with the
anterior capsule of lens are rarely formed in acute plastic type
of uveitis. !hese result
in deepening anterior chamber.
-
8/17/2019 PR siapa ya
17/18
-
8/17/2019 PR siapa ya
18/18