Embed Size (px)
Citation preview

Page 1 of 5
Meeting Title
Quality and Safety Committee
Date
20 December 2017 Agenda No
Report Title Quality Improvement Action Plan – November 2017
Lead Director/Manager
Professor Nancy Fontaine Chief Nurse Dr Andy Morris Chief Medical Officer
Report Author Sheila O’Sullivan – Clinical Lead for Compliance Action Required
Approve □ Discuss ■ Inform ■ Assure ■ Ratify □ Review □ Other □ (specify)
Executive Summary
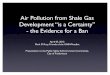
The purpose of this paper is to provide the Quality and Safety Committee with a summary of the CQC Quality Improvement Plan (QIP), specifically around the ‘must and should do’s’, detailing achievements in the month of November 2017. Progress on QIP: The BRAG assessment summary for overall progress against the desired KPI outcomes is as follows:
The progress on monthly ratings are: Blue: 19 actions Green: 2 actions Amber: 8 actions Red: 5 actions The five actions red rated areas are: Safeguarding adults training compliance for level 2 Life support training compliance Safeguarding children’s training compliance for level 3 Number of critical care step down delays Delays to ED handover from the ambulance service The outcome BRAG rating is based upon performance for each action over a three month period. To attain a blue BRAG rating the monthly target should have been achieved for a minimum of 3 consecutive months. This shows the
1314
10
67
54
3 3
5
0
23 3
6
11
1415
16
19
0
2
4
6
8
10
12
14
16
18
20
Progress
BRAG Assessment Summary For Overall Progress
Red
Amber
Green
Blue

Page 2 of 5
change has been embedded with sustained practice achieved. The progress achieved against each QIP outcomes is detailed in Appendix 1. Good progress has been made in month and the following actions are completed: 1. Care of gynaecology patients: the number of gynaecology patients not
admitted to the dedicated speciality ward has improved from 13% six months ago to 1.8% in November. 100% of nursing staff, both permanent and long term agency nurses who working in the speciality and have completed gynaecology competencies. This action has been signed off as completed.
2. Improve end of life care: The numbers of patients who are discharged to
their preferred place of death has improved from 67% six months ago to 100% in month. The target was 80% which has been achieved for 3 consecutive months.
3. Specialist Palliative Care Consultant: Our lead palliative care consultant
has completed Trust induction and is undertaking the agreed job plan.
Risks: a summary of the five areas where the performance has not been achieved in the month is listed below:
4. Safeguarding Adults Training Compliance: Level 1 training compliance was achieved at 93%. However Level 2 compliance: 76%, this is a 14% behind the trajectory plan.
Although this has improved steadily by 17% over the last six months. 5. Life Support Training Compliance: Basic Life Support (level 2) for adults and children is 67%, 23% below
monthly trajectory. Paediatric intermediate life support (pILS) training compliance is 79%, which
is 11% behind the trajectory. This was introduced in April 2017 and is steadily improving month on month.
6. Safeguarding Children’s training compliance Compliance for Safeguarding Children level 1 is 95%, Green RAG rated. Compliance for level 2 is 85% and Amber RAG rated. This has improved
steadily by 18% over the last six months Compliance for Level 3 is 76% and red RAG rated which is 14% below the
trajectory plan.
Mitigating actions for training topics: Safeguarding adults: Patients are kept safe as we have Matron and Clinical
Site Managers, available 24 hours a day, 365 days a year, to advise, support and participate in the safeguarding and MCA process on wards and with clinical teams.
There continues to be a focus on achieving the 90% compliance. Continuous focus through HCG performance reviews by the executive team
is completed.
7. Delay to discharges stepping down from critical care to ward areas: Patients delayed for >4 and < 24 hours has increased from 17 in October to
20 in month. The number of patients waiting for over 24 hours to step down to a ward has

Page 3 of 5
decreased from 33 to 26 in month.
8. Delays in accepting handover from Ambulance Service: The current performance is delays of 30-60 minutes occur for 22% of
arrivals and delays of >60 minutes occur for 4.7% of patients.
Mitigating actions for improving flow through the Trust: A dedicated ED paramedic will accept handover from ambulance service
and care for patients in the queue. This will release the ambulance crew. All cases of a one hour delay will be discussed at Serious Incident Group
(SIG) meeting to determine if the patient was harmed. The CDU, MAU and SAU are now all open and performance should improve
as the areas comply and embed the standard operating procedures. All wards are to identify their golden hour patient who will be ready for early
morning discharge to the discharge lounge. This will allow flow then from assessment to ward beds and subsequently
ED to assessment beds. Early ward discharges should in turn improving the critical care step down
patients moving to a ward in a timely way.
8. Actions to support the Emergency Department: To support the emergency department team and the Trust, the COO and the
quality first team are working alongside the team to assist in delivery of the improvements required.
During November: - Utilise a Plan, Do, Study, Act (PDSA) approach to implementing the changes for quality improvement to the nurse led RAT role which continues.
Safety checklist pilot has ended and is now in use during December. Raising awareness and training continues for staff.
GP proforma for hospital assessment is on version 4 and implemented with one local GP practice who has agreed to adopt this for all referrals to the department. The CCGs in Essex & Herts will cascade this to all practices so the Trust is informed of patients condition and diagnostic investigations that were completed locally before referral to Trust.
Medical rotas have been reviewed with the Associate Medical Director and aligned with the known peak arrival times to ensure the medical staffing matches high demand periods.
Each speciality team received their performance data against the internal professional standard. The HCG is working with the executive team to identify actions to improve poor performance.
Plans for December: - Real time reporting of live in, through and out of the ED data will be launched by end of December. This should improve team’s proactive responses.
An automatic email or text messages will be sent when delays are beginning to occur.
CQC Planned Inspection 9. The CQC planned inspection of 6 core services was completed on 5th 6th
and 7th December 2017. 10. The summary of the high level feedback of preliminary findings received
stated:- The Trust felt different with a positive culture change Numerous examples of compassionate care. Concerns regarding out of date medicines on the ward areas was raised on
the first day and it was acknowledged the Trust took immediate action to resolve the issues.
11. Issues documented against each core service were:-

Page 4 of 5
Urgent and emergency care: recognised positive work in the ED but not all areas of the new build are open and new pathways are not fully functioning.
Medicine: Improvement in awareness of MCA and DOLs. Issues raised on Ray ward regarding management of an agitated patient
Surgery: Concerned about flow in day surgery when it closes at 20.00 hours as patients are taken back up to PACU. Children are recovered by non-paediatric intermediate life support (pILs) trained staff
Critical Care: Positive culture change was noticeable and improvements were noted. Mixed gender breaches were a concern but it was acknowledge we manage these.
Children and young people: - Matron manages Dolphin ward and it was recognised she is overstretched. Significant number of vacancies noted. Concerns rose about not having a dedicated transition team between children and adult services.
End of Life: Concerns about no planned equipment maintenance schedule for the mortuary (lift maintenance). Discussed a concern about our treatment escalation plan and that it does not allow for a full mental capacity act assessment to undertaken which can impact on DNACPR decision making.
Medicines management: Concerns were raised about the ambient room temperatures in the treatment room and that we do not monitor these.
Managing patients with mental health conditions: On the first day of the inspection CQC raised concerns about a patient who was given sedation in the ED and the inspector felt more frequent observations should have been recorded. The trusts rapid tranquilisation policy has been requested.
The letter received from the CQC is in Appendix 2 A measured and supportive approach by all inspectors is always required.
However concerns were raised about 2 of the inspection team. The first was raised by the CQC themselves where a fellow inspector was unhappy with the approach of a colleague in critical care. The inspector for pharmacy apologised to critical care staff on day two of the inspection. Concerns were raised by the CEO following the inspectors approach when assessing the ED. The CQC have accepted our concerns, apologised to our staff and assured us action will be undertaken.
The Trust will be making a formal response to the preliminary findings later this week ahead of he Well Led interviews.
The interviews for Well Led’ will be undertaken on 18 and 19 December 2017.
Recommendation The Committee are asked to discuss the information provided in this report as the risks identified will impact on the Trust at our next CQC inspection. In addition this report is discussed with our regulators at the Oversight Group meeting later this month.
Trust Strategic Objective
■ Our Patients: continue to improve the quality of care we provide our patients, improving our CQC rating and exiting special measures ■ Our People: support our people to deliver high quality care within a culture that improves, engagement, recruitment and retention and improvements in our staff survey results ■ Our Places: maintain the safety of and improve the quality and look of our places and work with our partners to develop an OBC for a new build, aligned with the development of a West Essex and East Hertfordshire Accountable Care ■ Our Performance: meet and achieve our performance targets, covering national and local operational, quality and workforce indicators ■ Our Pounds: manage our pounds effectively to achieve our agreed financial targets and control totals.
Risk Linked to all CQC Fundamental Standards

Page 5 of 5
The risks are detailed within this report and Appendix 1
Legal/Regulatory This report details our progress against the Summary Quality Improvement Plan which was developed following the 2016 CQC inspection of compliance against the essential standards.
Previously Considered by
None Date N/A
Appendices Appendix 1 - Summary QIP for November 2017 Appendix 2 –Verbal feedback letter to Trust

Page 1 of 18
Appendix 1
Table 1 - Summary of the Quality Improvement Plan with Progress
Areas for improvement
KPI/ Trajectory Jan17
Feb 17
Mar17
Apr 17
Ma 17
Jun 17
Jul 17
Aug 17
Sep 17
Oct 17
Nov 17
Dec 17
Outcome BRAG
Progress November 2017 Risk
Our Patients
1.Timing of ward rounds and timely discharges
Standardise process for ward rounds to facilitate timely daytime discharges
Performance: discharges after 17.00 in %
KPI: (agreed 8/11) 8am to 10am: 33% 8am to 12md: 35% 8am to 5pm: 95% 5pm to 10pm: 5% Overnight 10pm to 8am: 0%
41 40 39 40 43 43 36 41
Performance: Against the newly agreed KPIs, the non-elective discharge timings were: 3% Discharged 8am to 10am, 11% between 8am to 12md, 54% from 8am to 17.00 41% of Discharges occur after 17.00 hours up to 12mn. 5%)Overnight discharges There were ward moves to put the assessment and short stay wards closer to the ED in month. These moves will help better patient flow long term.
RAG Prediction for next month: Red
What actions are we completing to bring about an improvement: Standard reviews daily (looking at all patients >7 days LOS). Wards to identify a golden patient who will be ready to go to the discharge lounge for 8am. Focus to get TTAs to pharmacy 24 hours before discharge. Daily report details discharges by time, the Deputy COO liaises regarding each night time discharge. Explanation/comment for RAG rating prediction: During December the embedding of the SOPs for MAU, SAU will be completed following the ward moves. Any increase in performance is not expected to be sustained over the month.
Workload and planning of workload to ensure timely discharge
0
10
20
30
40
50
60
70
% o
f P
atie
nts
Discharge Timings
% after17:00hrs
% before17:00 hrs
Overnight

Page 2 of 18
2.Reduce SSA breaches
Aiming for zero SSA breaches as part of national standard 0 – Green <10 – Amber >11 - Red Performance: No. of breaches
5 9 5 5 3 2 2 11 3 Performance: 3 mixed sex breaches in month
in HDU as a result of poor capacity. RAG Prediction for next month: Amber What actions are we completing to bring about an improvement: A 4 hour standard has been implemented internally for step-down patients in critical care to wards so all are placed by 7pm Explanation/comment for RAG rating prediction: Once the assessment and short stay areas function as per SOP then this should improve flow enabling discharge from critical care earlier each day and reducing occurrences of breaches.
Bed availability on the correct ward for patients stepping down from critical care
3.Response rates to call bells in ED
≥95% of patients satisfied with response to call
95
95
92
95
95
87
90
90 Performance: The performance in month is 90% and was impacted by the refurbishment work.
Pressure in the departme
5
9
5 5
32 2
11
3
0
2
4
6
8
10
12
Number o
f Patients
SSA Breaches
SSA Breaches
NationalTarget ‐ Zero
AmberCompliance< 10RedCompliance>10

Page 3 of 18
bells on local audit Performance - %
Trajectory plan >95%: Green 85-94: Amber <85%: Red
RAG Prediction for next month: Green
What actions are we completing to bring about an improvement: Continuing with the regular reminders to the team Explanation/comment for RAG rating prediction: Continuing to complete the actions that worked in previous months.
nt and meeting patient needs
4.Centralise appointment booking
One booking system for electronic booking system for OPD by April 18
Electronic booking target planned of 80% by October 2017
Green: 80% Amber: >75 Red: <75
77 78 79 76 78 Performance: 78% There has been an improvement of 2% in the number of patients recorded as electronically booked during the month of November.
RAG Prediction for next month: Amber
What actions are we completing to bring about an improvement: Work will continue to validate the reporting to determine if we can extract more patients that should be excluded and monitor every referral that should be sent electronically.
The CCG is working very closely with the Trust to educate GP’s to refer by EBs only. we are waiting for agreement from the CCG that we can reject all paper referrals unless the pathway is excluded (for example Oral Surgery due to Dentists not being able to access eBs). Explanation/comment for RAG rating prediction: There is an expectation that the loss of activity over the Christmas and New Year holiday period will impact on the available capacity for January. This may prevent further improvement for EBS rates in December due
Not achieving our target of electronic patient booking
78
80
82
84
86
88
90
92
94
96
% o
f P
atie
nts
% of Patients Satisified with Call Bell Response Times
Performance ‐ %Trajectory:>95%
Trajectory85‐94%Trajectory<85%
74
75
76
77
78
79
80
81
Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17
Trust Perform
ance %
Centralised Appointment Booking
ElectronicBooking
PlannedTarget

Page 4 of 18
to forward booking into polled appointment slots.
5.Update Trust policies and guidelines
All Trust policies and guidelines to be up to date and evidence based
Performance: Trajectory is to approve 22 procedural documents per month
198
198
164
96
81
74
59
35
Performance: 165 policies (83%) are in date 35 policies (17%) are to be updated For all procedural documents we have 324 (85%) in date and 56 (15%) to be updated Total number of procedural documents approved in November was 32 against plan of 22. What actions are we completing to bring about an improvement: Trust policy group meets every two weeks and
RAG Prediction for next month: Green Plan to approve 22 procedural documents during the month. Explanation/comment for RAG rating prediction: We prioritised HCG policies to enable patient care. We are now focusing on corporate policies. Staff are asked to turn around the document to TPG within one week.
Out of date policies could impact on patient care
6.Gynaecology service improvement
i) ≥95% staff trained & competent in caring for i)gynaecology women i)
ii) ≥95% of ii) gynaecology
7.1
13
N/A
5
100
5.6
100
5.5
100
4.3
100
2.9
100
1.8
Performance: i) 100% of the substantive staff on our dedicated gynaecology ward (now on Nightingale ward) have completed the competencies. This includes the 3 long term agency staff. ii) The outlier position in month was 1.8% of ladies who were not placed on a gynaecology ward, this is 3 ladies. The Gynaecology
Patients not admitted to the gynaecology unit as result of high
118 116126
142165
198 198
164
9681 74
59
35
0
50
100
150
200
250
Number o
f Policies
Policies: Approved V Expired
ApprovedPolicies
ExpiredPolicies

Page 5 of 18
inpatients are allocated to the gynaecology wards
service will always move a lady outlying if their predicted LOS is >24 hours as the priority. The service has moved to its permanent location and is now on Nightingale ward There is an increase in bed numbers to 18. RAG Prediction for next month: Green What actions are we completing to bring about an improvement: i) Rolling RN adverts. ii) Daily reviews of gynaecology patient’s aiming to repatriate women to dedicated gynaecology ward if elsewhere and their LOS anticipated to be >24 hours. Explanation/comment for RAG rating prediction: High vacancy levels on the ward.
numbers of admissions against bed availability
7.Improvem-ents in end of life care
80% of EOL Patients discharged
to their preferred place of death by
31/10/2018
66.7 73.3 75 73.9 61.5 94 95 100 Performance: 100% of EOL patients discharged to their preferred place of death. This was 8 patients discharged home with SEPT support. Research shows that patients think it’s more of
Patient and family needs are not
8.5
7.1
13
56 5.5
4.4
2.91.8
0
2
4
6
8
10
12
14
Mar‐17
Apr‐17
May‐17
Jun‐17
Jul‐1
7
Aug‐17
Sep‐17
Oct‐17
Nov‐17
Dec‐17
Nu
mb
er o
f P
atie
nts
Gynae Patients On Dedicated Gynae Ward
% ofPatients onGynaewardTrojectory<5%

Page 6 of 18
OCT 2017
>66%: Green 56-65: Amber <56%: Red Increasing
incrementally 1% per month
Performance - %
a priority to have their symptoms managed well, close to time of death then the location of death. This action has been signed off as achieved in month.
met if the patient is not discharged to their preferred place of death
8.Improvements in end of life care
Ceilings of care /treatment escalation plan to be documented in patient record by 31/12/17
Signed off as achieved in October.
9.Improved end of life care
Implement 7 day specialist palliative care team service by April 2018
Signed off as achieved: September
10. Improved record keeping in critical care
Improve record keeping to meet national standards in critical care
100 67 100 100 100
Signed off as achieved: August
11. Monitoring of fridge temperatures
Fridge compliance consistently above 98%
99 95.5 95 99.9 99.3 99.5 Signed off as achieved: August
73.9
61.5
94 92100
0
20
40
60
80
100
120
Jul‐17 Aug‐17 Sep‐17 Oct‐17 Nov‐17 Dec‐17
% o
f P
atie
nts
% of Patients Achieving Prefered Place of Death
% of PatientsAchievingPPD
ExpectedmonthlyTrojectory
AmberTrojectory
RedTrojectory

Page 7 of 18
12.Organise patient records to support pathways
Healthcare records to be accessible to facilitate seamless pathways for patients
Signed off as achieved: July
13.Checking emergency equipment
Resuscitation equipment above 98%
97 99.6 99.3 99.4 99.6
Signed off as achieved: July
14. Share the learning from complaints
Systematic learning to reach all staff
Signed off as achieved: August
15.Compliance with MCA
All patients who require MCA assessment to receive one
Signed off as achieved: August
MCA training is incorporated into the safeguarding adult updates for level 2 given to clinical staff
16. Learn from complaints /incidents re EOL care
Identify trends and learn from complaints and incidents related to end of life care
Signed off as achieved: June
17. Improve risk management arrangements
Implementation of robust risk management arrangements. Improving oversight and management of risk from ward to board
Signed off as achieved: June
The risk registers continue to be reviewed on a rotational basis at the monthly Risk meeting

Page 8 of 18
Our People
18. Safeguarding process for Adults
i) Stat-Man training L1 L2
ii) 100% of doctors & RN, band 6/7as
NIC to be competent in MCA
completion
October 2017 Green: ≥90%
Amber: ≥80-<90% Red: <80%
73
55
63
57
79
59
71
64
83
70
76
69
81
74
88
73
93
76
Ensuring Safety: 24 hours a day, 365 days a year we have senior nurses at Matron/ Clinical Site Manager grades available to advise, support and participate in the safeguarding and MCA process on wards, with teams who are managing safeguarding issues across the Trust
Performance: Compliance for Safeguarding Adults is: Level 1 - 93%, Level 1 is compliant with green RAG rating. Level 2 compliance is 76% and rated as red as it is 14% behind the trajectory plan.
RAG Prediction for next month: Red The monthly target for December is 90%
What actions are we completing to bring about an improvement: The face to face training sessions are booked each month to train additional staff. There continues to be a shortfall in attendance at the training against the number of places available.
The vacant safeguarding adults band 7 post will be interviewed on 20/12/17, 4 candidates have been shortlisted.
Explanation/comment for RAG rating prediction: The area below trajectory requires face to face training attendance. The gap has been in the high number of unfilled places on each training course. Given the target is 90% for next month and we generally have an uplift of 3-4% in month, we are unlikely to achieve a 4% uplift in month to achieve the amber target
Staff not booked or not attending
19. Life support training and
Training compliance October 2017
Green: ≥90%
61 65 65 69 72 74 71
68
67
Performance: Compliance for Level 2 BLS for adults & children is 67%, This is 23% below the monthly trajectory.
Staff not booked or not attending
0
10
20
30
40
50
60
70
80
90
100Compliance %
Safeguarding Adults Compliance
Level 1
Level 2
TargetGreen
TargetAmber
TargetRed

Page 9 of 18
Paediatric Life Support Training
Amber: ≥80-<90% Red: <80%
Performance - %
The paediatric Intermediate life support training compliance is 79%; this is 11% behind the trajectory. This is steadily improving month on month.
RAG Prediction for next month – Red/Amber The monthly target for December 90%
What actions are we completing to bring about an improvement: Training plan in place and staff are allocated to their training? Sufficient places are planned for the month.
Explanation/comment for RAG rating prediction: Resuscitation Lead has confirmed sufficient sessions have been planned to ensure the target can be delivered. The gap has been in the high number of unfilled places on each training course. Given the target is 90% for next month, generally the uplift per month is a maximum of 3-5%. We are unlikely to achieve a 13% uplift in one month to achieve the amber target.
20. Safeguarding processes for Children – Stat man training compliance
Performance: %: L1 L2 L3
Stat / Man training compliance from
October 2017 Green: ≥90%
Amber: ≥80-<90%
78
66
**
70
57
81
72
67
81
72
76
78
85
67
67
77
78
75
82
80
75
88
83
70
95
85
76
Performance: Compliance for Safeguarding Children is: Level 1 - 95% Level 2 - 85% Level 3 – 76% The monthly planned trajectory was 90%. The compliances for levels 1 training achieves a Green RAG rating. Level 2 compliance achieves an amber
Staff not booked or not attending
6165 65
69 72 74 71 68
0
10
20
30
40
50
60
70
80
90
100
Mar‐17
Apr‐17
May‐17
Jun‐17
Jul‐1
7
Aug‐17
Sep‐17
Oct‐17
Nov‐17
Dec‐17
Co
mp
lian
ce %
Life Support Training Compliance
Performance ‐%
Target Green: ≥83%
Target Amber:75‐82%
Target Red:<75%

Page 10 of 18
Red: <80%
compliance rating. Safeguarding level 3 is 14% below the plan.
RAG Prediction for next month: Red The monthly target for November is 90%
What actions are we completing to bring about an improvement: The named nurse has contacted all staff requiring level 3 training to ensure they are booked onto sessions. The line manager is contacted by the named nurse for any staff member that does not attend their booked training. Explanation/comment for RAG rating prediction: The area below trajectory requires face to face training attendance. Given the level 3 training generally has uplift per month of a maximum of 7%. We will probably not achieve 4% uplift in one month to achieve the amber target with the Christmas holiday period.
21. Staffing levels in Resuscitation ED
Two nurses allocated to the resuscitation room at all times
Compliance: Green: ≥99% Amber: 89-98%
90 92 92 90 92 83 87 89 Performance: 89% of shifts had 2 RNs in resuscitation room. In event there is not two qualified nurses to work in resuscitation room, the second person allocated will supported closely by a senior RN, to be a runner, present intermittently to give drugs, be available for procedures etc. The clinical acuity of patients is reviewed regularly to ensure we deploy staff to ensure patient safety. Staff aware how to
Ensuring safety for patients in the resuscitation area and the relentless workload
81 8178
67
75 75
70
76
40
50
60
70
80
90
100
Apr‐17
May‐17
Jun‐17
Jul‐1
7
Aug‐17
Sep‐17
Oct‐17
Nov‐17
Dec‐17
Compliance %
Safeguarding Children Compliance
Level 1
Level 2
Level 3
TargetGreen
TargetAmber
TargetRed

Page 11 of 18
Red: <88%
escalate concerns to shift leader.
RAG Prediction for next month: Amber
What actions are we completing to bring about an improvement: Unable to always have 2 nurses in the resuscitation room due to staffing gaps. If 2 RNs cannot be placed there we will put 1 RN and a second staff member will be a final year student nurse or one of our Trust paramedic crew. Explanation/comment for RAG rating prediction: As result of staffing gaps we are unlikely to achieve this
75
80
85
90
95
100
105
% o
f S
hif
ts w
ith
2 R
N in
Res
usc
Resuscitation Room Staffing Levels
Performance ‐ %
Trojectory Target: ≥99%
AmberTrojectory: 89‐98%Red Trojectory:<88%

Page 12 of 18
22. Improved RN staffing
Incremental reduction of RN vacancy rates, ≤10% by 2020
Position against Trajectory: % Sep 17: < 22%
N/A N/A 23 24.7 24.9 24.9 23.9 22.9
Performance: RN vacancy is reduced to 22.9%, (200 WTE), Midwives positive balance, HCSW: 5.4% (30 WTE posts, AHP 3.68% (9.41 posts) The Trust has appointed 6.8 registered and 2 pre-registered nurse and midwifery starters in November, with 5.0 WTE assigned to the wards. In November there were 9 (headcount) nursing and midwifery leavers, with 2.0WTE leaving the adult inpatient wards. November data shows the Trust recruiting only 0.28 WTE more than left in month, the fourth successive month of positive balance.
Progress Against Outcome: Registered nurse staffing remains a considerable risk for the organisation and on all local risk registers. RAG Prediction for next month: Amber The planned starters in month are: RN/M: Confirmed 7, predicted 2 HCSW: confirmed 8, predicted 1, AHP: 0 December shows a potential negative balance. The rolling 12 month position shows there is a net gain of 23.37 WTE R N&M.
What actions are we completing to bring about an improvement: To maintain safety meetings: Thrice daily staffing meetings with ADON, CSM, and Matrons to review staffing across the Trust. Significant progress in utilising SafeCare in determining evidence based staff redeployment according to patient acuity and dependency. Non-nursing staff such as the ward co-ordinator, ward clerks and ward assistants are taken into consideration.
Progress Against Outcome: Registered nurse staffing remains a considerable risk for the organisation and is on all local risk registers. RAG Prediction for next month: Amber for registered nurses Trust wide.
Safe delivery of care and possible gaps in staffing or high use of temporary staff

Page 13 of 18
What actions are we completing to bring about an improvement: Recruitment plan: the Trust attends job fairs, has open days and has focused advertisement campaigns. There are rolling adverts for band 5 and HCA. We are aiming to continue to improve our relationship with our students as our band 5s of the future. Key recruitment events planned for December include Herts University Open Day for both adult and paediatric nursing, along with ED holding an interview day on the 9th December
Retention plan: The Trust continues participating in the national Retention Support Programme launched by NHS Improvement in July 2017. The Trusts retention plan which outlines the key measures that the Trust is initiating to address the issues of staff retention has been updated. We have extended the Preceptorship programme to 18 months to support staff. The itchy feet programme is now embedded and a number of staff has made contact.
23. Mandatory
Stat / Man training compliances by
72 62 67 69 72 74 77 80
84
Performance: Compliance is 84%. This is 6% below the planned trajectory. There continues
Staff not booked
20.5
21
21.5
22
22.5
23
23.5
24
24.5
25
25.5
Vacan
cy ra
te ‐%
RN Vacancy
Green<22%
Performance

Page 14 of 18
Training October 2017
Green: ≥90% Amber: ≥80-<90% Red: <80%
to be unfilled places on training sessions each week
During November the training team met with the healthcare groups and corporate teams to reduce the data mismatch between the central and locally held records.
RAG Prediction for next month: Amber The monthly target for November is 90%
What actions are we completing to bring about an improvement: Improvement is expected as staff have their level 1 training booklet. We know staff are signing off their training using this. Explanation/comment for RAG rating prediction: We generally have an uplift per month of 2-5%
or not attending
24. Improved appraisals for
Appraisal compliance of ≥90%
70 72 74 75 74 77 80
81 86
Performance: Appraisal compliance for (non -medical staff) was 86%; this is 4% behind
Staff feel valued if
6267 69 72 74 77 80
84
0
10
20
30
40
50
60
70
80
90
100
Apr‐17
May‐17
Jun‐17
Jul‐1
7
Aug‐17
Sep‐17
Oct‐17
Nov‐17
Dec‐17
Co
mp
lian
ce%
Stat:Man Training Compliance
Stat/ManTrainingComplianceTarget Green
Target Amber
Target Red

Page 15 of 18
non-medical staff
by October 2017. Green: ≥90% Amber: ≥80-<90% Red: <80%
trajectory. A deep dive to review compliance undertaken for our HCGs and corporate teams.
RAG Prediction for next month: Amber. The monthly trajectory target for December remains 90% What actions are we completing to bring about an improvement: Clear reports are provided to all teams with targeted emails to the leadership team, highlighting areas below trajectory? Deep dive meetings with HCG and corporate teams to align local and central data. Reminder prompts sent to all individual staff. Continued offer of training including in local departments. 1 to 1 support offered to managers who have a discrepancy between central and local data. Explanation for the RAG prediction: Despite highlighting the requirement for improvement in appraisal completion and a high focus on appraisal, recent months have produced only a typical 3% improvement month on month. Given the upcoming bank holidays it is unlikely we will reach the 90% target before January.
appraisal and they develop
25. Improvements in end of life care
Achieve full time substantive consultant
Implement 7 day SPCT cover by June 2018
AG AG
Performance: The EOL /Specialist Palliative Care consultant Dr Jane Hegarty has completed Trust induction and is now undertaking the EOL/specialist palliative care role since mid-November This action has been signed off as achieved
26. Ratify and embed Fit and Proper persons Process
100% compliance
with FPP process
Signed off as achieved: August
72 74 75 74 77 80 8186
0
10
20
30
40
50
60
70
80
90
100
% A
chie
ved
Appraisal (non-medical staff)
Performance ‐%
MonthlyTarget
Amber Target
Red Trojectory

Page 16 of 18
27. Supervisory time for nursing leads
All nursing leads enabled to carry out their role utilising supervisory time
Signed off as achieved: July
28. Critical care improvement in MDT working/ MM
Create a cohesive MDT approach. Review the process for M & M
Action: Signed off in April
29. Appraisals for Doctors
Appraisal rate to remain at ≥95%
Action Signed off in April
Our Performance
30. Reduce number of delayed discharges for critical care
Achieve timely discharge, reduce delays to the wards Delays 4 - 24 hours Delays >24 hours
AG AG 26 10
15 27
16 27
19 19
27 22
17 22
10 23
17 33
20 26
Performance: The number of discharges delayed for >4 hours/< 24 hours has increased to 20 in month. The number of discharges delayed for > 24 hours has decreased to 26.
RAG Prediction for next month: Red What actions are we completing to bring about an improvement: The actions we have been completing for the last two months will be continuing as they are the right actions. CC team identify patients for discharge each day and attend the patient placement meeting to request a bed. Critical care step down patients are treated with equal access as ED for bed allocation. A 4 hour standard has been implemented internally for step-down patients and all step downs to take place by 7pm. Explanation/comment for RAG rating prediction: Once the assessment and short stay areas function as per SOP then this should improve flow enabling discharge from critical care earlier each day.
Ward capacity to take patients ready for step down
impacts on new admissions
26
15 1619
27
17
10
1720
10
27 27
1922 22 23
33
26
0
5
10
15
20
25
30
35
Mar‐17
Apr‐17
May‐17
Jun‐17
Jul‐1
7
Aug‐17
Sep‐17
Oct‐17
Nov‐17
Dec‐17
Nu
mb
er o
f P
atie
nts
exp
erie
nci
ng
d
elay
Critical Care Step Down Delays
Delays for>4/<24hrs
Delays>24hrs

Page 17 of 18
31. ED handover from the ambulance service
Improve timely handover from ambulance to Trust. Reducing 30 min Reducing >60 minute delays
19
4.6
19.3
5.7
23
7
17
5.5
1.4
4.3
17.5
4.5
24
7
22
4.7
Performance: Ambulance Handover performance has improved during the month. The compliance was < 15 mins: 26% (trajectory plan 45%) >15 <30 mins: 47% (trajectory plan 41%) 30-60 mins: 22% (trajectory plan 12%) > 60+ mins: 4.7% (trajectory plan 1.8%)
The ED team are being supported daily by the COO and Quality First team and during part of October and for the next few months.
RAG Prediction for next month - Red
What actions are we completing to bring about an improvement: A recovery action plan is in place for improved performance supported by HCG and Quality First.
The reconfigured ED and bed base is now in place.
Explanation/comment for RAG rating prediction: There has been sustained high attendances in the department effecting flow of patients through the trust
Patients having a delay in handover and keeping ambulance staff for too long in our ED
32. Future sustainability of maternity services
Ensure capacity meets anticipated service demand
Performance: Work has commenced on building the new theatres and is expected to be completed by end January with theatres in use by early February.
RAG Prediction for next month - Green
What actions are we completing to bring about an improvement: Work is underway
Explanation/comment for RAG rating prediction: Theatres should be in use during February 2018.
Engagement
0
5
10
15
20
25
30
Del
ays
as a
%
Ambulance Handover Delays
30‐60 mindelays
>60 mindelays

Page 18 of 18
33. Reduce number of cancelled operations
Ensure maximum theatre utilisation
0 0 1 0
Action Signed off in July
Our Places
34. Mortuary refurbishment
Compliance with HTA requirements
G G G B
Action Signed off in April
Our Pounds
No Actions
Outcome BRAG scoring system
Rating is based upon performance for each action assessed over a three month period. The initial decision making takes place between the action lead and clinical lead for compliance, reviewing the last three months performance and
the RAG prediction for the coming month. Each BRAG score is then signed off with the lead executive, Chief Nurse and the Clinical Lead for Compliance To attain a blue BRAG rating the monthly target should have been achieved for a minimum of 3 consecutive months. This shows the change has
been embedded with sustained practice achieved.