Embed Size (px)
Citation preview

Renal ColicRenal ColicAmina Al-QaysiAmina Al-Qaysi

IntroductionIntroduction
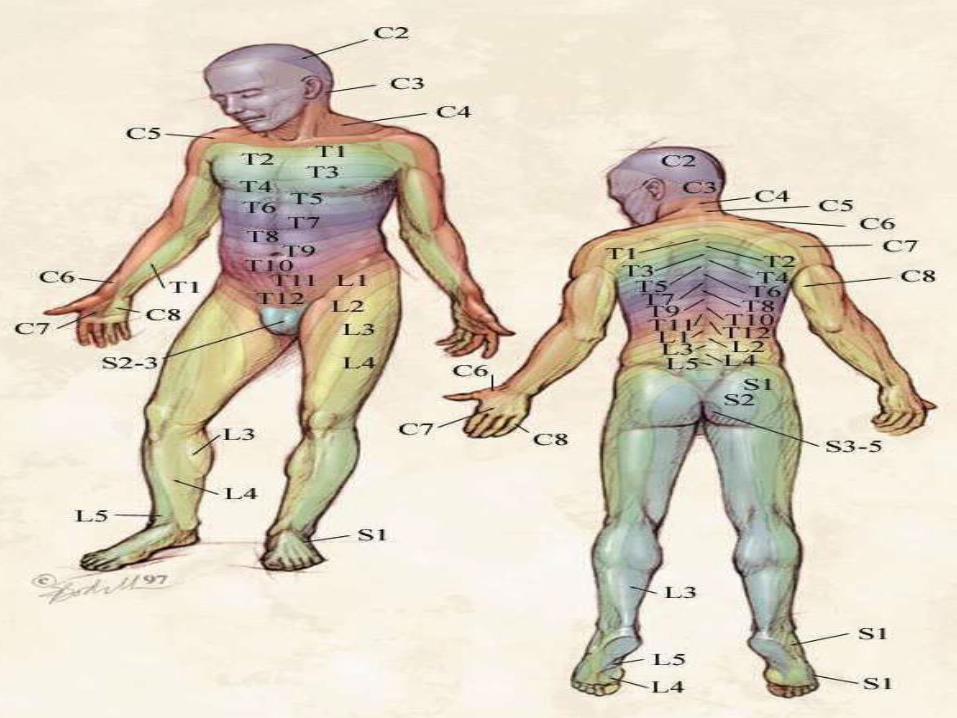
• T10-12, L1 roots innervate the renal capsule and ureter.
• Pain from these structures is felt in these dermatomes.
• Urinary tract & GIT share the same autonomic innervation, that’s why renal colic is usually associated with GI symptoms.

• Site:Site: Loin (space below 12th rib & iliac crest), Renal angle (between 12th rib & edge of erector spinae muscle).
• Radiation:Radiation: Towards the umbilicus.• Onset:Onset: Sudden.• Duration:Duration: variable.• Nature:Nature: Dull, aching pain .• Intensity:Intensity: Severe.
Renal ColicRenal Colic
• Course:Course: constant.• ProgressionProgression: progressive.
• Relieving & Exacerbating factors: Relieving & Exacerbating factors: patient tries changing his position in bed, or walking, but usually fails to relieve the pain. Relieved by analgesics.
• Associated Associated Hematuria, urinary frequency, dysuria, fever, sweating, nausea & vomiting.

Renal ColicRenal Colic

• Patient usually describesdescribes the pain by spreading his hand around his waist with his fingers covering the renal angle & his thumb above the anterior superior iliac spine.
• Acute Pyelonephritis and acute ureteral obstruction both causethis typical pain.

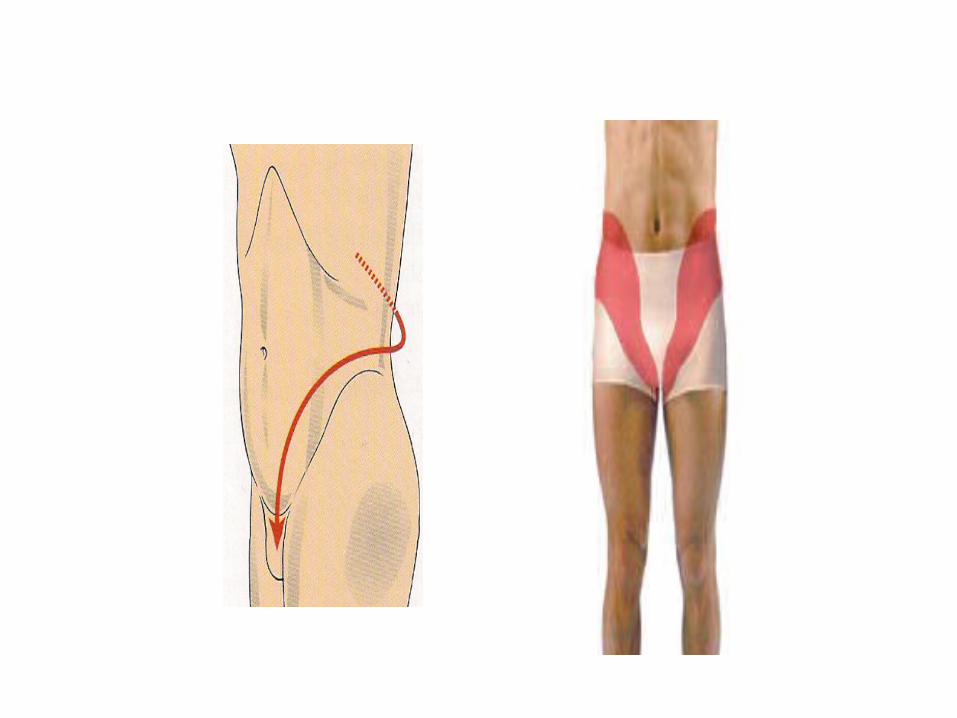
Ureteral ColicUreteral Colic• Site: Site: Originates at the costo-vertebral angle.• Radiation: Radiation: Lower quadrant of abdomen,
upper thigh and ipsilateral testicle or labium.• Onset:Onset: Sudden.• Duration:Duration: variable.• Nature: Nature: colicky, gripping.• Intensity:Intensity: Severe.

• Course:Course: attacks, pain is less severe in between, but never disappears completely.
• ProgressionProgression: progressive.
• Relieving & Exacerbating factors: Relieving & Exacerbating factors: patient tries changing his position in bed, or walking, but usually fails to relieve the pain. Relieved by analgesics.
• Associated Associated Hematuria, urinary frequency, dysuria, fever, sweating, nausea & vomiting.
Ureteral ColicUreteral Colic• Typical of sudden ureteric distension &
associated distension of the renal pelvis.
• Most commonly due to calculi.
• Less commonly due to tumor, or blood clot.

• Ureteral colic caused by stone in the upper ureter may be associated with severe pain in the ipsilateral testicle; due to the common innervation of these structures (T11–12).
• Stone in the lower ureter may cause pain referred to the scrotal wall.
• Stones in mid-ureter on the right side, causes pain referred to McBurney’s point and may therefore simulate appendicitis.
• On left side it may resemble diverticulitis or other diseases of the descending or sigmoid colon (T12, L1).

On ExaminationOn Examination
• General examination: Agitated, in pain,
pallor, fever, tachycardia.
• Abdomen tense & rigid.
• Loin tenderness.
• Kidney enlargement.
InvestigationsInvestigationsLaboratoryLaboratory::• CBC, ESR.• Serum electrolytes.• Blood urea.• Renal Function Test.• Urinalysis, Urine culture & sensitivity.• 24 hours urine: calcium, phosphorus, uric
acid, oxalate, cystine, citrate.• Biochemical assessment of stone.

RadiologyRadiology::
• KUB: 90% of renal stones are radio-opaque.• Intravenous Urography (IVU): Filing defect,
delayed excretion of contrast, dilated ureter.• Ultrasound: stone visualization, acoustic
shadow, dilated ureter.• Non-enhanced spiral CT scan: most
accurate assessment, identify non-opaque stones.
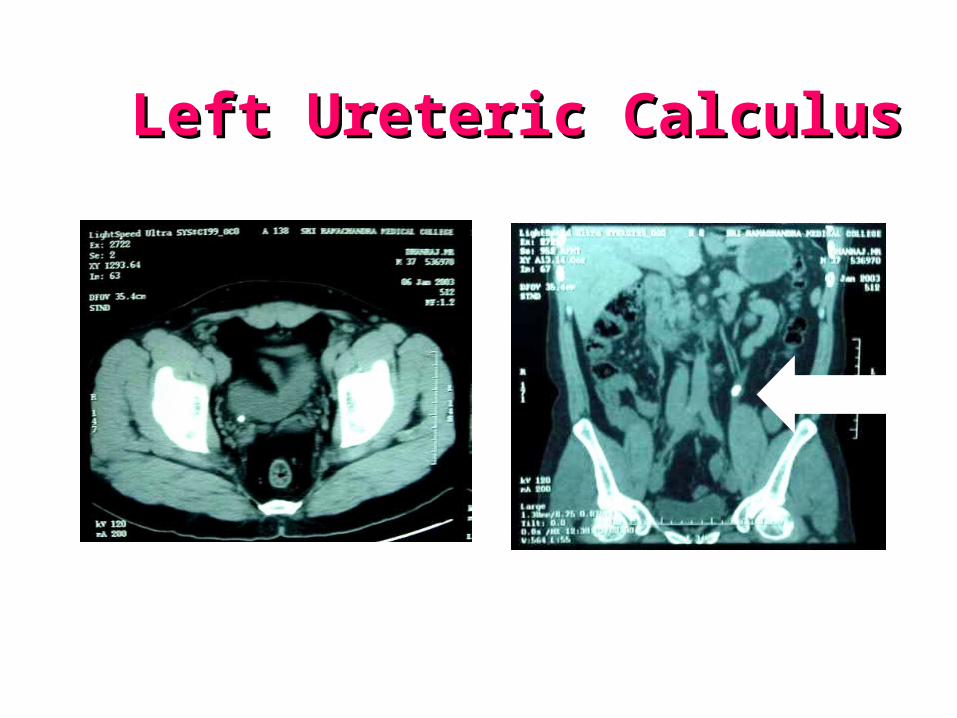
Left Ureteric CalculusLeft Ureteric Calculus
IVU Vs. CT scanIVU Vs. CT scan
IVUIVU::• More readily available.• Less irradiation.• Easy to interpret.• More economical.• Kidney function.
CT scanCT scan::• Quick.• No risk of contrast allergy.• High specificity.• Detailed anatomy.• Shows other pathology.

ManagementManagement
• Bed rest.• Hydration.• Analgesia: Morphine I.M. (10-20 mg),
Pethidine I.M. (100 mg).• Anti-emetic.
• Further management according to the cause.
Renal Stones ManagementRenal Stones Management
• On this conservative regime 60% of all stones pass spontaneously.
• However 30% of stones do require surgical removal whilst the remaining 10% may be followed expectantly.

• >90% of kidney stones are treated by Extracorporeal Shock Wave Lithotripsy.
• For Staghorn calculi: Percutaneous Nephrolithotomy or conventional open surgery (Pyelolithotomy) are still indicated on occasion.
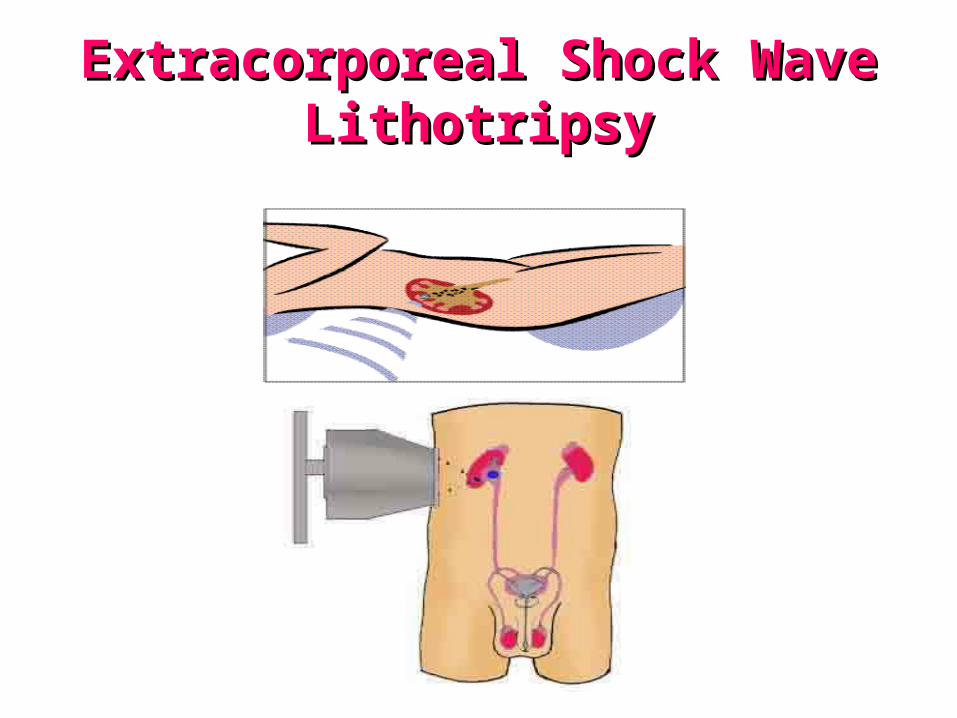
Extracorporeal Shock Wave Extracorporeal Shock Wave LithotripsyLithotripsy
Surgery indicated ifSurgery indicated if::
1.Large stone.2.Infection with severe obstruction.3.Failure of conservative measures.4.To correct anatomical abnormalities.

Ureteric Stones ManagementUreteric Stones Management
• 60% of all ureteric calculi will pass within a week to a month of onset of symptoms.
• Only 30% will require surgical removal.
• Most ureteric calculi are treated by ESWL.
• Push-bang treatment.
• Rigid or flexible Ureteroscopes can be used if ESWL fail.
• Stone fragmentation using laser, EHL and Ultrasound probes.
Surgery indicated ifSurgery indicated if::
1.Stone is too large to pass spontaneously (>7 mm).2.Causing obstruction & impairing renal function.3.Proximal infection combined with obstruction.

ReferencesReferences::1. Smith’s General Urology, 17th edition, Chapter 3,
Page 30-34.2. Davidsons’s principles & practice of medicine.3. Oxford handbook of urology.4. Bates’ guide to physical examination and history
taking, 10th edition, Chapter 11, Page 428-429.5. Textbook of medicine, Das.5. Browse’s introduction to the symptoms & signs of
surgical disease, Chapter 16, Page 435-436.6. Hutchinson’s clinical methods, 22nd edition, Chapter
14, Page 293.