-
8/19/2019 respirasi anak
1/13
2384 Part XXI ◆ Diseases of the Blood
Chapter 476
Hereditary Clotting
Factor Deficiencies(Bleeding Disorders)J. Paul Scott and
Veronica H. Flood
Hemophilia A (factor VIII deficiency) and hemophilia
B (factor IXdeficiency) are the most common and serious
congenital coagulationfactor deficiencies. Te clinical findings in
hemophilia A and hemo-philia B are virtually identical. Hemophilia
C is the bleeding disorderassociated with reduced levels of
factor XI (see Chapter 476.2). Reducedlevels of the contact
factors (factor XII, high-molecular-weight kinino-
gen, and prekallikrein) are associated with significant
prolongation ofactivated partial thromboplastin time (aP; also
referred to as PTT ),but are not associated with hemorrhage,
as discussed in Chapter 476.3.Other coagulation factor deficiencies
that are less common are brieflydiscussed in subsequent
subchapters.
476.1 Factor VIII or Factor IX Deficiency(Hemophilia A or
B)J. Paul Scott
Deficiencies of factors VIII and IX are the most common severe
inher-ited bleeding disorders. Recombinant factor VIII and factor
IX con-centrates are available to treat patients with hemophilia
and thereby
avoid the infectious risk of plasma-derived
transfusion-transmitteddiseases.
PATHOPHYSIOLOGY Factors VIII and IX participate in a
complex required for the activationof factor X. ogether with
phospholipid and calcium, they form the“tenase,” or factor
X–activating, complex. Figure 475-1 in Chapter 475shows the
clotting process as it occurs in the test tube, with factor Xbeing
activated by either the complex of factors VIII and IX or
thecomplex of tissue factor and factor VII. In vivo, the complex of
factorVIIa and tissue factor activates factor IX to initiate
clotting. In thelaboratory, prothrombin time (P) measures the
activation of factor Xby factor VII and is therefore normal in
patients with factor VIII orfactor IX deficiency.
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
2/13
Chapter 476 ◆ Hereditary Clotting Factor
Deficiencies (Bleeding Disorders) 238
specific mention. A patient may lose large volumes of blood into
tiliopsoas muscle, verging on hypovolemic shock, with only a
vagarea of referred pain in the groin. Te hip is held in a flexed,
internarotated position owing to irritation of the iliopsoas. Te
diagnosismade clinically from the inability to extend the hip but
must be cofirmed with ultrasonography or C (Fig. 476-1).
Life-threatenibleeding in the patient with hemophilia is caused by
bleeding into vistructures (central nervous system, upper airway)
or by exsanguintion (external trauma, gastrointestinal or iliopsoas
hemorrhagPrompt treatment with clotting factor concentrate for
these lithreatening hemorrhages is imperative. If head trauma is of
sufficie
concern to suggest radiologic evaluation, factor replacement
shouprecede radiologic evaluation. Simply put: “reat first, image
secondLife-threatening hemorrhages require replacement therapy to
achiea level equal to that of normal plasma (100 IU/dL, or
100%).
Patients with mild hemophilia who have factor VIII or factor
levels >5 IU/dL usually do not have spontaneous hemorrhages.
Teindividuals may experience prolonged bleeding aer dental
wosurgery, or injuries from moderate trauma and may not be
diagnosuntil they are older.
LABORATORY FINDINGS AND DIAGNOSISTe laboratory screening test
that is affected by a reduced level of factVIII or factor IX is P.
In severe hemophilia, the P value is usua2-3 times the upper limit
of normal. Results of the other screening teof the hemostatic
mechanism (platelet count, bleeding time, prothro
bin time, and thrombin time) are normal. Unless the patient has
inhibitor to factor VIII or IX, the mixing of normal plasma with
patieplasma results in correction of P value. Te specific assay for
factoVIII and IX will confirm the diagnosis of hemophilia. If
correctidoes not occur on mixing, an inhibitor may be present. In
25-35% patients with hemophilia who receive infusions of factor
VIII or factIX, a factor-specific antibody may develop. Tese
antibodies adirected against the active clotting site and are
termed inhibitors. such patients, the quantitative Bethesda
assay for inhibitors should performed to measure the antibody
titer.
DIFFERENTIAL DIAGNOSISIn young infants with severe bleeding
manifestations, the differentdiagnosis includes severe
thrombocytopenia; severe platelet functi
Aer injury, the initial hemostatic event is formation of the
plateletplug, together with the generation of the fibrin clot that
prevents furtherhemorrhage. In hemophilia A or B, clot formation is
delayed and is notrobust. Inadequate thrombin generation leads to
failure to form atightly crosslinked fibrin clot to support the
platelet plug. Patients withhemophilia slowly form a so, friable
clot. When untreated bleedingoccurs in a closed space, such as a
joint, cessation of bleeding may bethe result of tamponade. With
open wounds, in which tamponadecannot occur, profuse bleeding may
result in significant blood loss. Teclot that is formed may be
friable, and rebleeding occurs during thephysiologic lysis of clots
or with minimal new trauma.
CLINICAL MANIFESTATIONSNeither factor VIII nor factor IX crosses
the placenta; bleeding symp-toms may be present from birth or may
occur in the fetus. Only 2% ofneonates with hemophilia sustain
intracranial hemorrhages, and 30%of male infants with hemophilia
bleed with circumcision. Tus, in theabsence of a positive family
history (hemophilia has a high rate ofspontaneous mutation),
hemophilia may go undiagnosed in thenewborn. Obvious symptoms such
as easy bruising, intramuscularhematomas, and hemarthroses begin
when the child begins to cruise.Bleeding from minor traumatic
lacerations of the mouth (a torn frenu-lum) may persist for hours
or days and may cause the parents to seekmedical evaluation. Even
in patients with severe hemophilia, only 90%have evidence of
increased bleeding by 1 yr of age. Although bleedingmay occur in
any area of the body, the hallmark of hemophilic bleeding
is hemarthrosis. Bleeding into the joints may be induced by
minortrauma; many hemarthroses are spontaneous. Te earliest joint
hemor-rhages appear most commonly in the ankle. In the older child
andadolescent, hemarthroses of the knees and elbows are also
common.Whereas the child’s early joint hemorrhages are recognized
only aermajor swelling and fluid accumulation in the joint space,
older childrenare frequently able to recognize bleeding before the
physician does.Tey complain of a warm, tingling sensation in the
joint as the firstsign of an early joint hemorrhage. Repeated
bleeding episodes into thesame joint in a patient with severe
hemophilia may become a “target” joint. Recurrent bleeding may
then become spontaneous because ofthe underlying pathologic changes
in the joint.
Although most muscular hemorrhages are clinically evident
owingto localized pain or swelling, bleeding into the iliopsoas
muscle requires
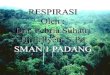
Figure 476-1 Massive hematoma into the iliopsoas muscle in
a patient with hemophilia B. A 38 yr old man with severe
deficiency of factor (hemophilia B) was admitted for right lower
abdominal pain of progressively increasing severity and tenderness.
He had had a common cold wsevere cough and loss of appetite for
approximately 1 wk. A, Abdominal radiograph shows presence of
the psoas sign on the right side and leshifted colon gas. B,
CT scan shows massive hematoma in the right iliopsoas muscle,
resulting in anterior translocation of the right
kidneC, Reconstructed 3-dimensional image shows more clearly
the kidney translocation and the extended, but intact, large
vessels. These are useffindings for the diagnostic procedures,
because progressive right lower abdominal pain may closely simulate
acute appendicitis. The hemorrhawas successfully managed by
replacement of factor IX for 1 wk without any recurrence. The
patient did not have any inhibitors to factor IX. (Fro
Miyazaki K, Higashihara M: Massive hemorrhage into the iliopsoas
muscle, Intern Med 44:158, 2005.)
A B C
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
3/13
2386 Part XXI ◆ Diseases of the Blood
Calculation of the dose of recombinant factor VIII (FVIII) or
recom-binant factor IX (FIX) is as follows:
Dose of rFVIII IU
desired rise in rFVIII Body weight kg
( )
% ( ) ( ) .= × × 0 5
Dose of rFIX IUdesired rise in plasma FIX Body weight kg
( )% ( ) ( ) .= × ×1 44
For factor VIII, the correction factor is based on the volume
ofdistribution of factor VIII. For factor IX, the correction factor
is basedon the volume of distribution and the observed rise in
plasma levelaer infusion of recombinant factor IX.
able 476-1 summarizes the treatment of some common types
ofhemorrhage in a patient with hemophilia.
With the availability of recombinant replacement products,
prophy-laxis is the standard of care for most children with
severe hemophilia,to prevent spontaneous bleeding and early joint
deformities. In addi-tion to currently available recombinant
factors, products are beingdeveloped to increase the plasma
half-life and reduce the immunoge-nicity of hemostatic factors. A
study comparing prophylaxis withaggressive episodic treatment
provides evidence for the superiority ofprophylaxis in preventing
debilitating joint disease. If target jointsdevelop, “secondary”
prophylaxis is oen initiated.
With mild factor VIII hemophilia, the patient’s endogenously
pro-duced factor VIII can be released by the administration of
desmopres-
sin acetate. In patients with moderate or severe factor VIII
deficiency,the stored levels of factor VIII in the body are
inadequate, and desmo-pressin treatment is ineffective. Te risk of
exposing the patient withmild hemophilia to transfusion-transmitted
diseases and the cost ofrecombinant products warrant the use of
desmopressin, if it is effective.A concentrated intranasal form of
desmopressin acetate, not theenuresis or pituitary replacement
dose, can also be used to treatpatients with mild hemophilia A. Te
dose is 150 g (1 puff) for chil-dren weighing 50 kg. Most centers
administer a trial of desmopres-sin to determine the level of
factor VIII achieved aer its infusion.Desmopressin is not effective
in the treatment of factor IX–deficienthemophilia.
Preliminary trials of an adeno-associated virus vector
containing thefactor IX gene are underway with some encouraging
initial results.
PROPHYLAXISMany patients are now given lifelong prophylaxis to
prevent spontane-ous joint bleeding. Te National Hemophilia
Foundation recommendsthat prophylaxis be considered optimal therapy
for children withsevere hemophilia. Usually, such programs are
initiated with the first joint hemorrhage. Young children oen
require the insertion of acentral catheter to ensure venous access.
Such programs are expensivebut are highly effective in preventing
or greatly limiting the degree of joint pathology; however,
complications include central line infectionand thrombosis.
reatment is usually provided every 2-3 days to main-tain a
measurable plasma level of clotting factor (1-2%) when
assayed just before the next infusion (trough level). Whether
prophylaxisshould be continued into adulthood has not yet been
adequatelystudied. If moderate arthropathy develops, prevention of
future bleed-
ing will require higher plasma levels of clotting factors. In
the olderchild who is not given primary prophylaxis, secondary
prophylaxis isfrequently initiated if a target joint develops.
SUPPORTIVE CAREAlthough it is easy to tell parents that their
child should avoid trauma,this advice is not practical in active
children and adolescents. oddlersare active, are curious about
everything, and injure themselves easily.Effective measures include
anticipatory guidance, including the use ofcar seats, seatbelts,
and bike helmets, and the importance of avoidinghigh-risk
behaviors. Older boys should be counseled to avoid violentcontact
sports, but this issue is a challenge. Boys with severe hemo-philia
oen sustain hemorrhages in the absence of known trauma.Early
psychosocial intervention helps the family achieve a balance
disorders, such as Bernard-Soulier syndrome and Glanzmann
throm-basthenia; type 3 (severe) von Willebrand disease; and
vitamin K defi-ciency. Hemostatic screening tests should
differentiate these entitiesfrom hemophilia.
GENETICS AND CLASSIFICATIONHemophilia occurs in approximately 1
: 5,000 males, with 85% havingfactor VIII deficiency and 10-15%
having factor IX deficiency. Hemo-philia shows no apparent racial
predilection, appearing in all ethnicgroups. Te severity of
hemophilia is classified on the basis of thepatient’s baseline
level of factor VIII or factor IX, because factor levelsusually
correlate with the severity of bleeding symptoms. By definition,1
IU of each factor is defined as that amount in 1 mL of normal
plasmareferenced against a standard established by the World Health
Orga-nization (WHO); thus, 100 mL of normal plasma has 100 IU/dL
(100%activity) of each factor. For ease of discussion, henceforth
in thischapter, we use the term % activity to refer to
the percentage found innormal plasma (100% activity). Factor
concentrates are also referencedagainst an international WHO
standard, so treatment doses are usuallyreferred to in IU. Severe
hemophilia is characterized as having 5%, may go many years
before the conditionis diagnosed, and frequently require
significant trauma to cause bleed-
ing. Te hemostatic level for factor VIII is >30-40%, and for
factor IX,it is >25-30%. Te lower limit of levels for factors
VIII and IX in normalindividuals is approximately 50%.
Te genes for factors VIII and IX are carried near the terminus
ofthe long arm of the X chromosome and are therefore X-linked
traits.Te majority of patients with hemophilia have reduced
clotting factorprotein; 5-10% of those with hemophilia A and 40-50%
of those withhemophilia B make a dysfunctional protein.
Approximately 45-50% ofpatients with severe hemophilia A have the
same mutation, in whichthere is an internal inversion within the
factor VIII gene that results inproduction of no protein. Tis
mutation can be detected in the bloodof patients or carriers and in
the amniotic fluid by molecular techniques.African-Americans oen
have a different factor VIII haplotype, andthis difference may be
the reason that African-Americans have higherinhibitor formation
(see later). Because of the multiple genetic causes
of either factor VIII or factor IX deficiency, most cases of
hemophiliaare classified according to the amount of factor VIII or
factor IX clottingactivity. In the newborn, factor VIII values may
be artificially elevatedbecause of the acute-phase response
elicited by the birth process. Tisartificial elevation may cause a
mildly affected patient to have normalor near-normal levels of
factor VIII. Patients with severe hemophiliado not have detectable
levels of factor VIII. In contrast, factor IX levelsare
physiologically low in the newborn. If severe hemophilia is
presentin the family, an undetectable level of factor IX is
diagnostic of severehemophilia B. In some patients with mild factor
IX deficiency, the pres-ence of hemophilia can be confirmed only
aer several weeks of life.
Trough lyonization of the X chromosome, some female
carriers ofhemophilia A or B have sufficient reduction of
factor VIII or factor IXto produce mild bleeding disorders. Levels
of these factors should bedetermined in all known or potential
carriers to assess the need for
treatment in the event of surgery or clinical bleeding.Because
factor VIII is carried in plasma by von Willebrand factor,the ratio
of factor VIII to von Willebrand factor is sometimes used
todiagnose carriers of hemophilia. When possible, specific genetic
muta-tions should be identified in the propositus and used to test
otherfamily members who are at risk of either having hemophilia or
beingcarriers.
TREATMENTEarly, appropriate therapy is the hallmark of excellent
hemophilia care.When mild to moderate bleeding occurs, values of
factor VIII or factorIX must be raised to hemostatic levels, in the
35-50% range. For life-threatening or major hemorrhages, the dose
should aim to achievelevels of 100% activity.
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
4/13
-
8/19/2019 respirasi anak
5/13
2388 Part XXI ◆ Diseases of the Blood
increase the plasma concentration by 2%. Tus, infusion of plasma
at10-15 mL/kg will result in a plasma level of 20-30%, which is
usuallysufficient to control moderate hemorrhage. Frequent
infusions ofplasma would be necessary to achieve higher levels of
factor XI.Because the half-life of factor XI is usually ≥48 hr,
maintaining ade-quate levels of factor XI commonly is not
difficult.
Chronic joint bleeding is rarely a problem in factor XI
deficiency,and for most patients, the deficiency is a concern only
at the time ofmajor surgery unless there is a second underlying
hemostatic defect(e.g., von Willebrand disease).
Bibliography is available at Expert Consult.
476.3 Deficiencies of the Contact Factors(Nonbleeding
Disorders)J. Paul Scott
Deficiency of the “contact factors” (factor XII, prekallikrein,
and high-molecular-weight kininogen) causes prolonged P but no
bleedingsymptoms. Because these contact factors function at the
step of initia-tion of the intrinsic clotting system by the reagent
used to determineP, the P is markedly prolonged when these factors
are absent.Tus, there is the paradoxical situation in which P is
extremely
prolonged with no evidence of clinical bleeding. It is important
thatindividuals with these findings be well informed about the
meaning oftheir clotting factor deficiency because they do not need
treatment,even for major surgery.
476.4 Factor VII DeficiencyJ. Paul Scott
Factor VII deficiency is a rare autosomal bleeding disorder that
isusually detected only in the homozygous state. Severity of
bleeding varies from mild to severe with hemarthroses,
spontaneous intracra-nial hemorrhage, and mucocutaneous bleeding,
especially nosebleedsand menorrhagia. Patients with this deficiency
have markedly pro-
longed P but normal P. Factor VII assays show a marked
reductionin factor VII. Because the plasma half-life of factor VII
is 2-4 hr,therapy with FFP is difficult and is oen complicated by
fluid overload.A commercial concentrate of recombinant factor VIIa
is effective intreating patients with factor VII deficiency.
Bibliography is available at Expert Consult.
476.5 Factor X DeficiencyJ. Paul Scott
Factor X deficiency is a rare (estimated 1/1,000,000) autosomal
disor-der with variable severity. Mild deficiency results in
mucocutaneous
and posttraumatic bleeding, whereas severe deficiency results in
spon-taneous hemarthroses and intracranial hemorrhages. Factor X
defi-ciency is the result of either a quantitative deficiency or a
dysfunctionalmolecule. A reduced factor X level is associated with
prolongation ofboth P and P. In patients with hereditary factor X
deficiency, factorX levels can be increased with use of either FFP
or prothrombincomplex concentrate. Te half-life of factor X is
approximately 30 hr,and its volume of distribution is similar to
that of factor IX. Tus,1 unit/kg will increase the plasma level of
factor X by 1%.
Although it is rarely a problem in pediatric patients, systemic
amy-loidosis may be associated with factor X deficiency,
owing to theadsorption of factor X on the amyloid protein. In the
setting of amy-loidosis, transfusion therapy oen is not successful
because of the rapidclearance of factor X.
off-label (i.e., in a use not approved by the FDA), as an
alternate therapyfor patients with high inhibitor titers in whom
immune tolerance pro-grams have failed. Some centers first begin
with prednisone with orwithout cyclophosphamide; others add
cyclosporine if there is a poorresponse. If desensitization fails,
bleeding episodes are treated witheither recombinant factor VIIa or
activated prothrombin complex con-centrates (factor VIII inhibitor
bypassing activity). Te use of theseproducts bypasses the inhibitor
in many instances but may increase therisk of thrombosis. Some
patients with low titers of inhibitor can betreated with high-dose
factor VIII during a bleeding episode. Patientswith inhibitors
require referral to a center that cares for many suchpatients and
has a comprehensive hemophilia program.
In the past, plasma-derived treatment products transmitted
hepatitisB and C as well as HIV to large numbers of patients with
hemophilia.In the era of recombinant products, the risk of
acquiring such infec-tions should be minimal, but patients should
receive appropriateimmunizations against hepatitis B. Tose who are
exposed to bloodproducts should be monitored for
transfusion-related infections.Reports have also identified the
transmission of variant Creutzfeldt-Jakob disease to patients
receiving therapeutic plasma and may warrantstudy of patients with
hemophilia for prion transmission from plasma-derived factor
concentrates.
COMPREHENSIVE CAREPatients with hemophilia are best managed
through comprehensive
hemophilia care centers. Such centers are dedicated to patient
andfamily education as well as to the prevention and/or treatment
of thecomplications of hemophilia, including chronic joint disease
andinhibitor development as well as infection, such as hepatitis B
and Cor HIV. Such centers involve a team of physicians, nurses,
orthopedists,physical therapists, and psychosocial workers, among
others. Educa-tion remains crucial in hemophilia care, because
patients who arereceiving prophylaxis may be less “experienced” in
recognizing bleed-ing episodes than affected children from previous
eras.
Bibliography is available at Expert Consult.
476.2 Factor XI Deficiency (Hemophilia C)
J. Paul Scott
Factor XI deficiency is an autosomal deficiency associated with
mildto moderate bleeding symptoms. It is frequently encountered in
Ash-kenazi Jews but has been found in many other ethnic groups. In
Israel,1-3/1,000 individuals are homozygous for this
deficiency.
Te bleeding tendency is not as severe as in factor VIII or
factor IXdeficiency. Te bleeding associated with factor XI
deficiency is notcorrelated with the amount of factor XI. Some
patients with severedeficiency may have minimal or no symptoms at
the time of majorsurgery. Because factor XI augments thrombin
generation and leadsto activation of the fibrinolytic inhibitor
thrombin-activatable fibrino-lysis inhibitor, surgical bleeding is
more prominent in sites of highfibrinolytic activity like the oral
cavity. Unless the patient previouslyhad surgery without bleeding,
replacement therapy should be con-
sidered and given preoperatively, depending on the nature of the
sur-gical procedure. No approved concentrate of factor XI is
available inthe United States; therefore, the physician must use
fresh-frozenplasma (FFP).
Bleeding during minor surgery can be controlled with local
pressure.Patients undergoing dental extractions can be monitored
closely andmay benefit from treatment with fibrinolytic inhibitors
like aminoca-proic acid, with plasma replacement therapy used only
if hemorrhageoccurs. In a patient with homozygous deficiency of
factor XI, P isoen longer than it is in patients with either severe
factor VIII or factorIX deficiency. Te paradox of fewer clinical
symptoms in combinationwith longer P is surprising, but it occurs
because factor VIIa canactivate factor IX in vivo. Te deficiency of
factor XI can be confirmedby specific factor XI assays. Plasma
infusions of 1 IU/kg usually
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
6/13
Chapter 476 ◆ Hereditary Clotting Factor
Deficiencies (Bleeding Disorders) 2388.e
BibliographyBerntorp E, Halimeh S, Gringeri A, et al: Management
of bleeding disorders in
children, Haemophilia 18(Suppl 2):15–23, 2012.Berntorp E,
Shapiro AD: Modern haemophilia care,
Lancet 379:1447–1454,
2012.Branchford BR, Monahan PE, Di Paola J: New developments in
the treatment of
pediatric hemophilia and bleeding disorders, Curr Opin
Pediatr 25:23–30,2013.
Broderick CR, Herbert RD, Latimer J, et al: Association between
physical activityand risk of bleeding in children with
hemophilia, JAMA 308:1452–1458, 2012.
Coppola A, agliaferri A, Di Capua M, et al: Prophylaxis in
children withhemophilia: evidence-based achievements, old and new
challenges, Seminromb Hemost 38(1):79–94, 2012.
DiMichele DM: Inhibitors in childhood hemophilia A: genetic and
treatment-related risk factors for development and eradication,
Pediatr Blood Cancer 60(Suppl 1):S30–S33, 2013.
Fijnvandraat K, Cnossen MH, Leebeck FWG, et al: Diagnosis and
management ofhaemophilia, BMJ 344:36–40, 2012.
Gouw SC, van der Bom JG, Ljung R, et al: Factor VIII products
and inhibitordevelopment in severe hemophilia A, N Engl J
Med 368:231–238, 2013.
Hay CRM, Brown S, Collins PW, et al: Te diagnosis and management
of factorVII and IX inhibitors: a guideline from the United Kingdom
haemophilia centredoctors organization, Br J
Haematol 133:591–605, 2006.
Kruse-Jarres R: Current controversies in the formation and
treatment ofalloantibodies to factor VIII in congenital hemophilia
A, Hematology 407–412,2011.
Kulkarni R, Soucie JM, Lusher J, et al: Site of initial bleeding
episodes, mode ofdelivery and age of diagnosis in babies with
haemophilia diagnosed before theage of 2 years: a report from Te
Centers for Disease Control and Prevention’s
(CDC) Universal Data Collection (UDC) project, Haemophilia
15:1281–12902009.
Leissinger C, Gringeri A, Antmen B, et al: Anti-inhibitor
coagulant complexprophylaxis in hemophilia with inhibitors, N Engl
J Med 365:1684–1692,2011.
Ljung R: Hemophilia and prophylaxis, Pediatr Blood
Cancer 60(Suppl 1):S23–S262013.
Ljung RC, Knobe K: How to manage invasive procedures in children
withhaemophilia, Br J Haematol 157(5):519–528, 2012.
Manco-Johnson MJ, Abshire C, Shapiro AD, et al: Prophylaxis
versus episodictreatment to prevent joint disease in boys with
severe hemophilia, N Engl J M357:535–544, 2007.
Manco-Johnson MJ: Collision sports and risk of bleeding in
children withhemophilia, JAMA 308:1480–1481, 2012.
Montgomery RR, Cox Gill J, Di Paola J: Hemophilia and von
Willebrand diseaseIn Orkin SH, Nathan DG, Ginsberg D, et al,
editors: Nathan and Oski’shematology of infancy and
childhood , ed 7, Philadelphia, 2009, SaundersElsevier, pp
1487–1524.
Nathwani AC, uddenham EGD, Rangarajan S, et al:
Adenovirus-associated viru vector-mediated gene transfer in
hemophilia B, N Engl J Med 365:2357–2365,2011.
Ross C, Goldenberg NA, Hund D, et al: Athletic participation in
severehemophilia: bleeding and joint outcomes in children on
prophylaxis, Pediatri124:1267–1272, 2009.
Witmer CM, Huang YS, Lynch K, et al: Off-label recombinant
factor VIIa use anthrombosis in children: a multi-center cohort
study, J Pediatr 158:820–825,2011.
Zimmerman B, Valentino LA: Hemophilia: in review, Pediatr
Rev 34:289–294,2011.
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
7/13
2388.e2 Chapter 476 ◆ Hereditary
Clotting Factor Deficiencies (Bleeding Disorders)
BibliographyNathwani AC, Reiss UM, uddenham EGD, et al:
Long-term safety and efficacy of
factor IX gene therapy in hemophilia B, N Engl J
Med 371:1994–2004, 2014.Seligsohn U: Factor XI in
haemostasis and thrombosis: past, present and future,
romb Haemost 98:84–89, 2007.
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
8/13
Chapter 476 ◆ Hereditary Clotting Factor
Deficiencies (Bleeding Disorders) 2388.e
BibliographyMariani G, Dolce A, Batorova A, et al: Recombinant,
activated factor VII for
surgery in factor VII deficiency: a prospective evaluation-the
surgical SER, Br J Haematol 152(3):340–346,
2011.
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
9/13
Chapter 476 ◆ Hereditary Clotting Factor
Deficiencies (Bleeding Disorders) 238
able fibrinogen level is diagnostic. In addition to the
quantitative deciency of fibrinogen, a number of dysfunctional
fibrinogens have bereported (dysfibrinogenemia). Rarely patients
with dysfibrinogeemia present with thrombosis. A human fibrinogen
concentratecommercially available for therapy of bleeding episodes
in afibrinogeemic patients. Because the plasma half-life of
fibrinogen is 2-4 daytreatment with either FFP or cryoprecipitate
is also effective. Themostatic level of fibrinogen is >60 mg/dL.
Each bag of cryopreciptate contains 100-150 mg of fibrinogen. Some
clinical assays for fibrogen are inhibited by high doses of
heparin. Tus, a markedly prolongthrombin time associated with a low
fibrinogen level should be evalated with determination of reptilase
time. Prolonged reptilase timconfirms that functional levels of
fibrinogen are low and that heparis not present.
476.10 Factor XIII Deficiency(Fibrin-Stabilizing Factor
orTransglutaminase Deficiency)J. Paul Scott
Because factor XIII is responsible for the crosslinking of
fibrin stabilize the fibrin clot, symptoms of delayed hemorrhage
are secon
ary to instability of the clot. ypically, patients have trauma 1
day anthen have a bruise or hematoma the next day. Clinical
symptominclude mild bruising, delayed separation of the umbilical
stumbeyond 4 wk in neonates, poor wound healing, and recurrent
spotaneous abortions in women. Rare kindreds with XIII deficiency
whemarthroses and intracranial hemorrhage have been describeResults
of the usual screening tests for hemostasis are normal patients
with factor XIII deficiency. Screening tests for factor Xdeficiency
are based on the observation that there is increased solubity of
the clot because of the failure of crosslinking. Te normal
clremains insoluble in the presence of 5M urea, whereas in a
patiewith XIII deficiency, the clot dissolves. More specific assays
for factXIII are immunologic. Te half-life of factor XIII is 5-7
days and themostatic level is 2-3% activity. Tere is a
heat-treated, lyophilizconcentrate of coagulation factor XIII
available to treat bleeding ep
sodes or for prophylaxis.
Bibliography is available at Expert Consult.
476.11 Antiplasmin or PlasminogenActivator Inhibitor
DeficiencyJ. Paul Scott
Deficiency of either antiplasmin or plasminogen activator
inhibitboth of which are antifibrinolytic proteins, results in
increased plasmgeneration and premature lysis of fibrin clots.
Affected patients haa mild bleeding disorder characterized by
mucocutaneous bleedibut rarely have joint hemorrhages. Because
results of the usual hem
static tests are normal, further work-up of a patient with a
positibleeding history should include euglobulin clot lysis time
(if availablwhich measures fibrinolytic activity and yields a
shortened result the presence of these deficiencies. Specific
assays for α2-antiplasmand plasminogen activator inhibitor are
available. Bleeding episodare treated with FFP; bleeding in the
oral cavity may respond to amnocaproic acid.
Bibliography is available at Expert Consult.
476.6 Prothrombin (Factor II) DeficiencyJ. Paul
Scott
Prothrombin deficiency is caused either by a markedly reduced
pro-thrombin level (hypoprothrombinemia) or by functionally
abnormalprothrombin (dysprothrombinemia). Laboratory testing in
homozy-gous patients shows prolonged P and P. Factor II, or
prothrombin,assays show a markedly reduced prothrombin level.
Mucocutaneousbleeding in infancy and posttraumatic bleeding later
are common.Patients are treated with either FFP or, rarely,
prothrombin complexconcentrates. In prothrombin deficiency, FFP is
useful, because thehalf-life of prothrombin is 3.5 days.
Administration of 1 IU/kg of pro-thrombin will increase the plasma
activity by 1%.
Bibliography is available at Expert Consult.
476.7 Factor V DeficiencyJ. Paul Scott
Deficiency of factor V is an autosomal recessive, mild to
moderatebleeding disorder that has also been termed
parahemophilia. Hem-arthroses occur rarely; mucocutaneous
bleeding and hematomas
are the most common symptoms. Severe menorrhagia is a
frequentsymptom in women. Laboratory evaluation shows prolonged
Pand P. Specific assays for factor V show a reduction in factor
Vlevels. FFP is the only currently available therapeutic product
thatcontains factor V. Factor V is lost rapidly from stored FFP.
Patientswith severe factor V deficiency are treated with infusions
of FFP at10 mL/kg every 12 hr. Rarely, a patient with a negative
family historyof bleeding has an acquired antibody to factor V.
Oen, such a patientdoes not bleed because the factor V in platelets
prevents excessivebleeding.
Bibliography is available at Expert Consult.
476.8 Combined Deficiencyof Factors V and VIIIJ. Paul
Scott
Combined deficiency of factors V and VIII occurs secondary to
theabsence of an intracellular transport protein that is
responsible fortransporting factors V and VIII from the endoplasmic
reticulum to theGolgi compartments. Tis explains the paradoxical
deficiency of 2factors, one encoded on chromosome 1 and the other
on the X chro-mosome. Bleeding symptoms are oen milder than for
hemophilia Aand are treated with FFP to replace both factors V and
VIII.
476.9 Fibrinogen (Factor I) Deficiency
J. Paul Scott
Congenital afibrinogenemia is a rare autosomal recessive
disorder inwhich there is an absence of fibrinogen. Patients with
this disorder donot bleed as frequently as patients with hemophilia
and rarely havehemarthroses. Affected patients may present in the
neonatal periodwith gastrointestinal hemorrhage or hematomas aer
vaginal delivery.In addition to marked prolongation of P and P,
thrombin time isprolonged. In the absence of consumptive
coagulopathy, an unmeasur-
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
10/13
Chapter 476 ◆ Hereditary Clotting Factor
Deficiencies (Bleeding Disorders) 2389.e
BibliographyLancellotti S, De Cristofaro R: Congenital
prothrombin deficiency, Semin romb
Hemost 35:367–381, 2009.
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
11/13
2389.e2 Chapter 476 ◆ Hereditary
Clotting Factor Deficiencies (Bleeding Disorders)
BibliographyAsselta R, Peyvandi F: Factor V deficiency, Semin
romb Hemost 35:382–389,
2009.
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
12/13
Chapter 476 ◆ Hereditary Clotting Factor
Deficiencies (Bleeding Disorders) 2389.e
BibliographyDreyfus M, Barrois D, Borg JY, et al: Successful
long-term replacement therapy
with FXIII concentrate (Fibrogammin(®)P) for severe congenital
factor XIIIdeficiency: a prospective multicentre study, J romb
Haemost 9(6):1264–1266,2011.
Greenberg CS, Sane DC, Lai S: Factor XIII and fibrin
stabilization. In ColmanRW, Marder VJ, Clowes AW, et al, editors:
Hemostasis and thrombosis: basic
principles and clinical practice, ed 5, Philadelphia,
2006, Lippincott Williams &Wilkins, pp 317–334.
Downloaded from ClinicalKey.com at Universitas Hasanuddin on
March 17, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/19/2019 respirasi anak
13/13
2389.e4 Chapter 476 ◆ Hereditary
Clotting Factor Deficiencies (Bleeding Disorders)
BibliographyAgren A, Wiman B, Schulman S: Laboratory evidence of
hyperfibrinolysis in
association with low plasminogen activator inhibitor type 1
activity, BloodCoagul Fibrinolysis 18:657–660, 2007.
Bauer KA: Rare coagulation factor abnormalities. In Orkin SH,
Nathan DG,Ginsberg D, et al, editors: Nathan and Oski’s hematology
of infancy andchildhood , ed 7, Philadelphia, 2009, Saunders
Elsevier, pp 1525–1532.
Carpenter SL, Mathew P: Alpha2-antiplasmin and its deficiency:
fibrinolysis out ofbalance, Haemophilia 14:1250–1254,
2008.