Embed Size (px)
Citation preview

Respiration Physiology
陳雅雯 助理教授
ext. 2177

Vander’s Human PhysiologyThe Mechanisms of Body Function
References
Review of Medical PhysiologyGanong
Vander, sherman, & Luciano’s

Organization of the respiratory system

• Pulmonary: lung
• Alveolus: tiny air-containing sac, the site of gas exchange with blood, 300 million/adult.
• Airway: the tubes that air flows through from the external environment to the alveolus.
• Inspiration (inhalation), Expiration (exhalation).
• Respiratory cycle: Inspiration Expiration.
Respiratory cycle

Housing the vocal cords
Inspiration air
The walls of trachea and bronchus contain rings of cartilage, which give them their cyclindrical shape and support them.

Airways
no cartilage
alveolus appear
no alveolus and no gas exchange with the blood
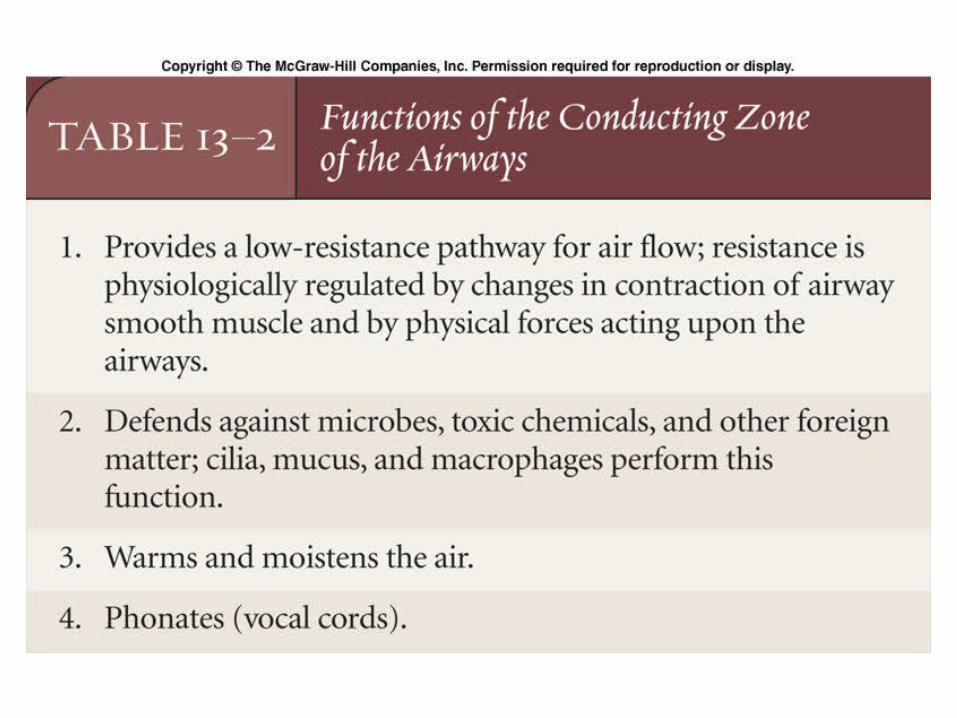
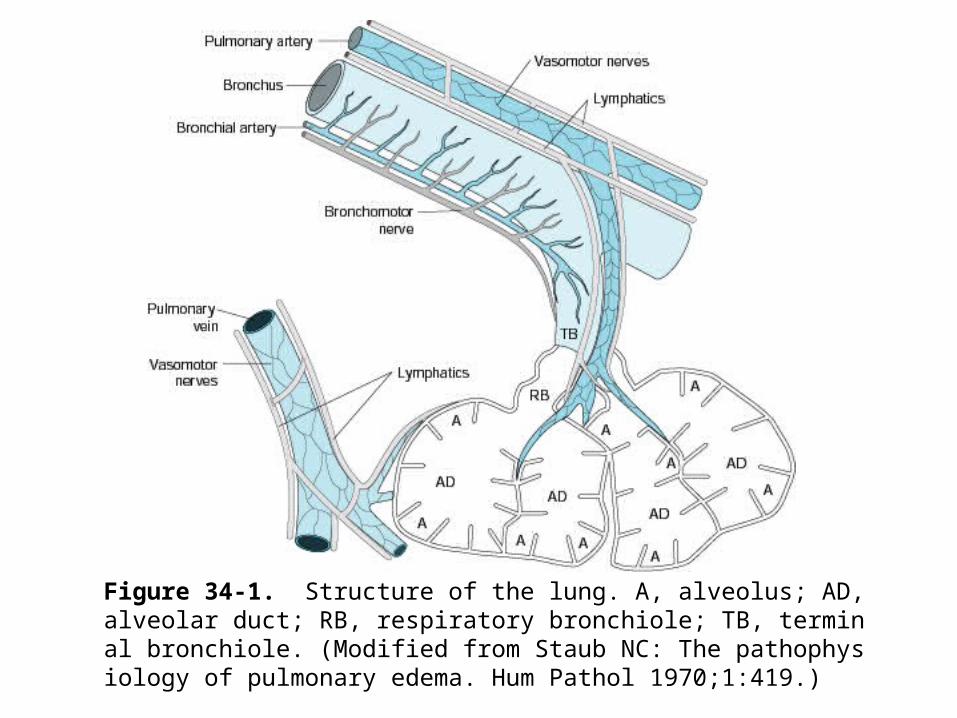
Figure 34-1. Structure of the lung. A, alveolus; AD, alveolar duct; RB, respiratory bronchiole; TB, terminal bronchiole. (Modified from Staub NC: The pathophysiology of pulmonary edema. Hum Pathol 1970;1:419.)

Alveolus


Alveolar wall
Contain interstitial fluid and connective tissues

The Lung: Scientific Foundations Second Edition 423-545, 1997
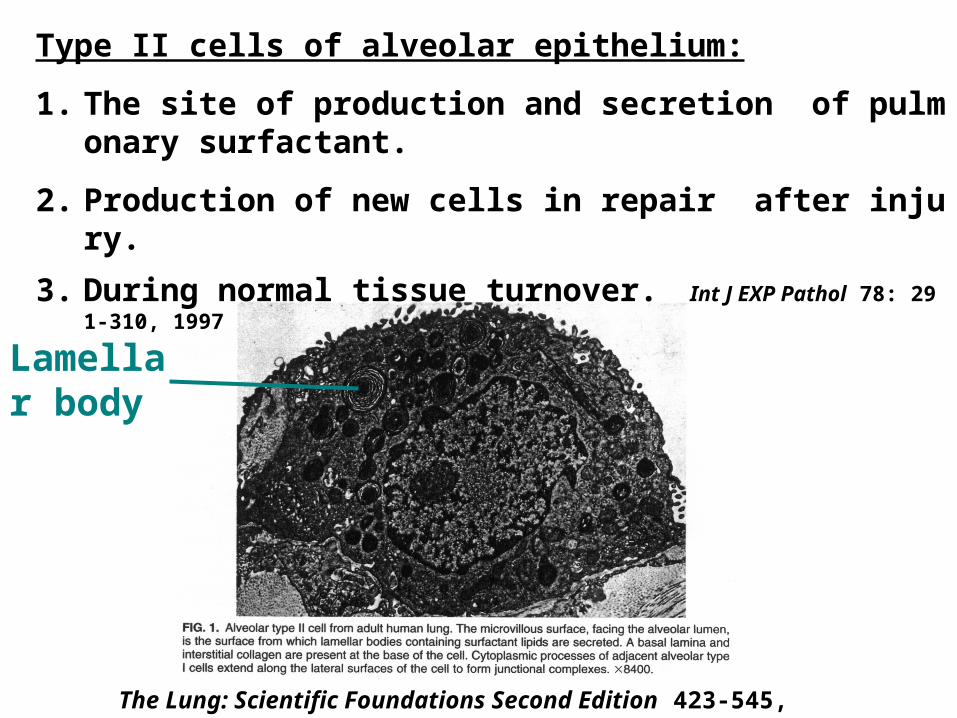
Type II cells of alveolar epithelium:
1. The site of production and secretion of pulmonary surfactant.
2. Production of new cells in repair after injury.
3. During normal tissue turnover. Int J EXP Pathol 78: 291-310, 1997
The Lung: Scientific Foundations Second Edition 423-545, 1997
Lamellar body

Figure 34-13. Formation and metabolism of surfactant. Lamellar bodies (LB) are formed in type II alveolar epithelial cells and secreted by exocytosis. The released lamellar body material is converted to tubular myelin (TM), and the TM is probably the source of the phospholipid surface film (SF). Some surfactant is taken up by alveolar macrophages, but more is taken up by endocytosis in type II epithelial cells. N, nucleus; RER, rough endoplasmic reticulum; CB, composite body. (Reproduced, with permission, from Wright JR: Metabolism and turnover of lung surfactant. Am Rev Respir Dis 1987;136:426.)

(75 m2)

Components of thoracic wall: spinal column, ribs, sternum ,intercostal muscles and connective tissue.
Bronchus
Lung
Pleural sac
(intrapleural pressure, Pip)
Ventilation and lung mechanics

Bulk flow
F (flow)
= P (pressure)
R (resistance)
= (Palv-Patm)
R (resistance)

Alveolar pressure (Palv)
Atmospheric pressure (Patm)
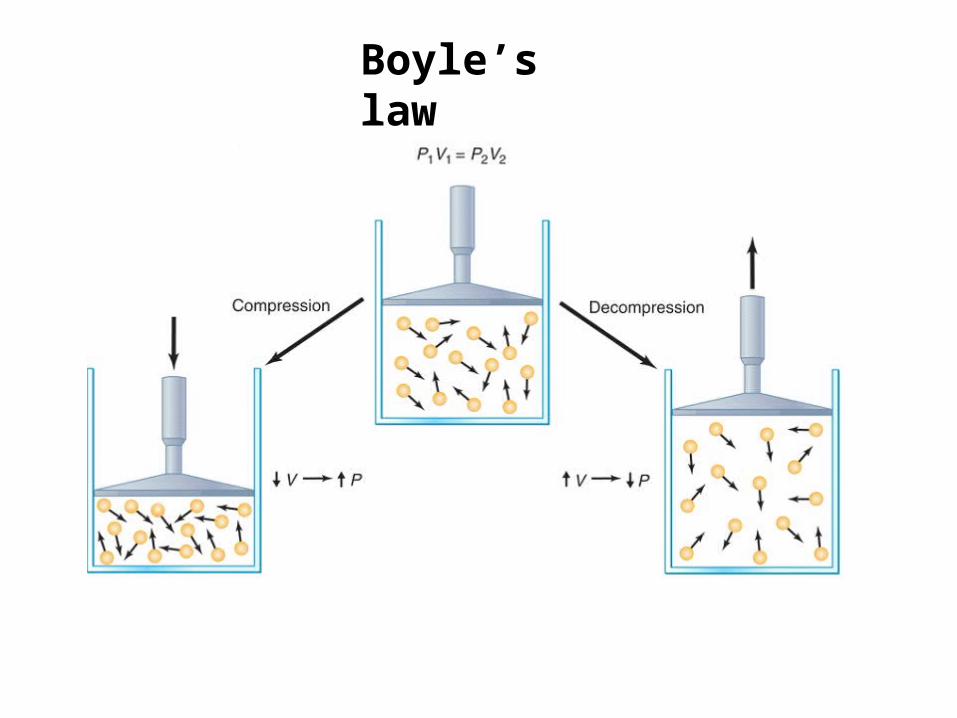
Boyle’s law

Lung volume depends on (1)transpulmonary pressure (Ptp)-between the inside and the outside of the lungs, (2)how stretchable the lungs are.

Rest: Palv=0, Patm=0, Pip= - 4 mmHg

How is a stable balance achieved between breaths .

Elastic recoil: the tendency of an elastic structure to oppose stretching or distortion.
(Rest)

Normal inspiration at restPhrenic nerves: diaphragm
Interscostals nerves: inspiratory intercostals muscles
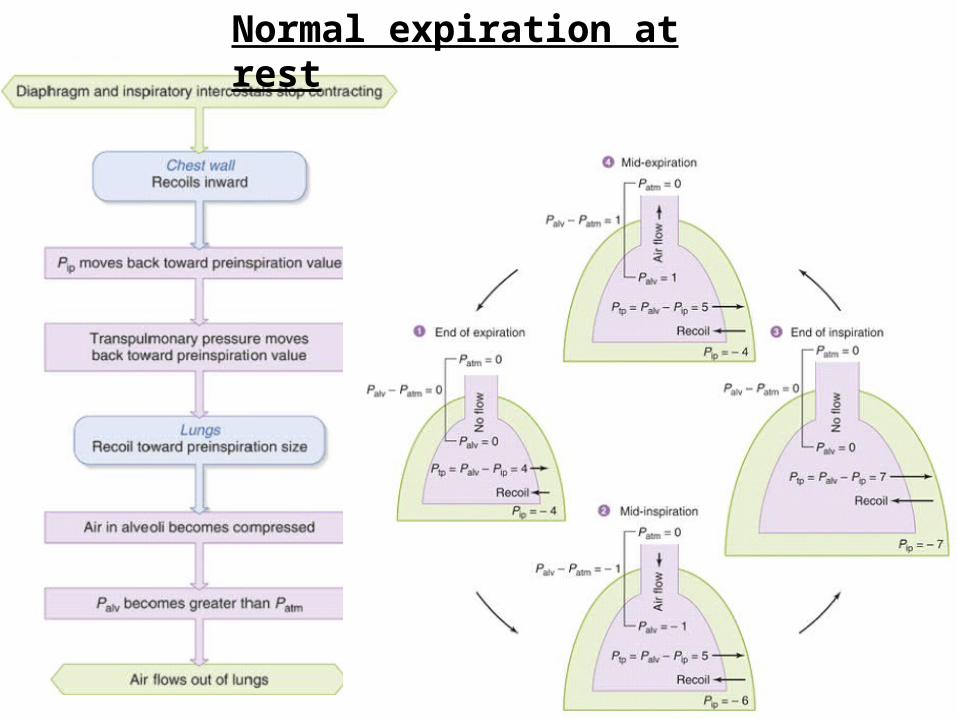
Normal expiration at rest

Lung compliance
There are two major determinants of lung compliance:
(1)Elastic connective tissues lung tissues
thickening compliance
(2) Surfactant surface tension
compliance


Interactive Respiratory Physiology
In fibrosis the lungs become stiff, making a large pressure necessary to maintain a moderate volume. Such lungs would be considered poorly compliant.
Lung fibrosis

Emphysema
Compliance of the lung in emphysema is significantly above normal; the lung becomes easy to distend but empties slowly.
Interactive Respiratory Physiology


Laplace law

Respiratory distress syndrome (RDS)
Newborn
(The lung filled with amniotic fluid)
Maternal blood
oxygen
Surfactant synthesizing cells immature
Low lung compliance

Respiratory distress syndrome (RDS) of the newborn
Premature infants.
The surfactant synthesizing cells may be
immature to function adequately.
Complete exhaustion, inability to breath,
lung collapse, death.
Therapy: mechanical ventilator, natural or
synthetic surfactant.

Airway resistance
F= (Palv-Patm)/R
Physical factors
Neural factors
Chemical factors
Airway radii
Airway resistance
Transpulmonary pressure
Elastic connective tissues fiber
Physical factorsTranspulmonary pressure (Ptp)
1.which exerts a distending force on the
airway.
2.inspiration: Ptp, airway radius, airway
resistance, lung expand.Elastic connective tissues fiber
1. which link the outside of the airways to the
surrounding alveolar tissue.
2. lateral traction: which pull the airway open.

Neural factors
Neuroendocrine and paracrine factors:
Epinephrine
leukotrienes(-adrenergic
receptors)(members of eicosanoid family)
(airway smooth muscle)
Relaxation
Contraction


Forced expiratory volume in 1s (FEV1)
The person takes a maximal inspiration and then exhales maximally as fast as possible.
The important value is the fraction of the total forced vital capacity expired in 1s.
The normal individuals can expired approximately 80% of the vital capacity in 1s.
Obstructive lung disease
Airway resistance
A FEV1 that is less than 80% of the vital
capacity.
It is difficult to expire air rapidly through
the narrowed airway.

Restrictive lung disease
Normal airway resistance but impaired respiratory movement because of abnormalities in the lung tissue, the pleura, the chest wall, or the neuromuscular machinery.
A normal ratio of FEV1 to vital capacity.
Reduction of vital capacity.

Ventialtion
Minute ventialtion (VE)
Minute ventialtion = Tidal volume x Respiratory rate(ml/min)
(ml/breath)
(breaths/min)
(VE
)
(Vt) (f)
6000 ml/min = 500 ml/breath x 12 breath/min

Alveolar ventialtion (VA)
Alveolar ventilation (ml/mln)
Tidal volume
(ml/breath)
Dead space
(ml/breath)
Respiratory rate
(breaths/min)
= - x
(VA
)
(Vt) (f)(VD
)
4200 ml/min = (500 ml/breath – 150 ml/breath)
x 12 breaths/min


Dead space
Anatomic dead space: conducting airway, these airway do not permit gas exchange with the blood.
Alveolar dead space: some fresh inspired air is not used for gas exchange with blood even though it reachs the alveoli.
Physiologic dead space: the sum of anatomic dead space and alveolar dead space.This is as known as “wasted” ventilation.
Exchange of gases in alveoli and tissues
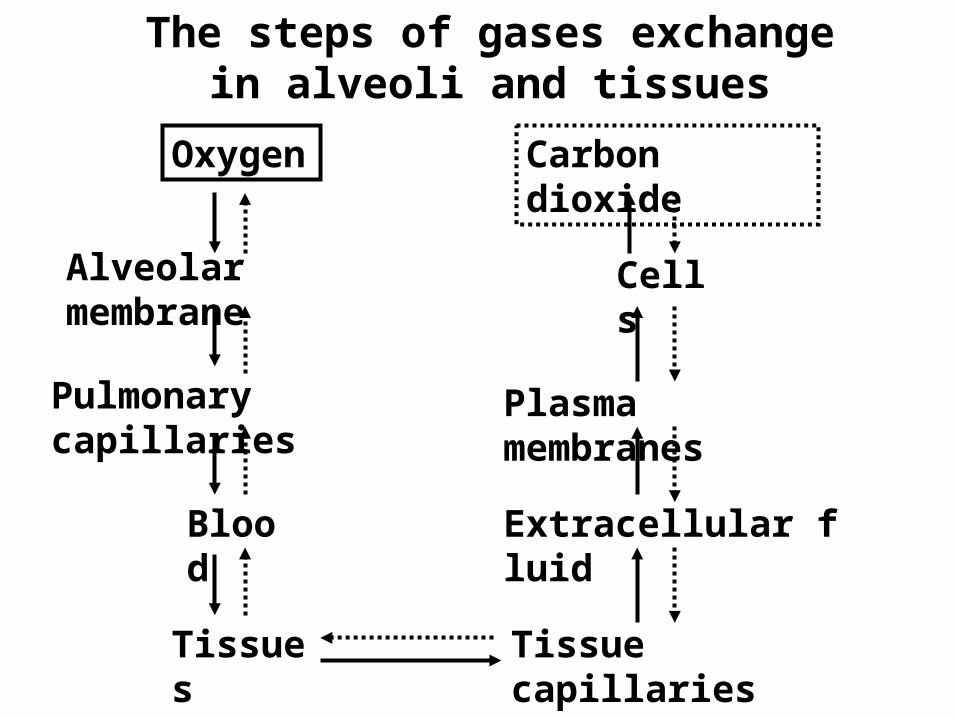
Oxygen
Alveolar membrane
Pulmonary capillaries
Blood
Tissues
Tissue capillaries
Extracellular fluid
Plasma membranes
Cells
Carbon dioxide
The steps of gases exchange in alveoli and tissues
Respiratory quotient (RQ)
The ratio of CO2 produced to O2 consumed.
For example, on a mixed diet, the RQ is approximately 0.8; that is, 8 molecules of CO2 are produced for every 10 molecules of O2 consumed,
RQ
Carbohydrate:1
Fat:0.7
Protein:0.8

(O2 consumption/min)
(CO2 production/min)
(21%x4L/min)

Partial pressure of gases As Dalton’s law states, in a mixture of
gases, the pressure each gas exert is independent of the pressure the other exert.
The individual pressures, termed partial pressure (P).
Partial pressure of oxygen: PO2
Partial pressure of carbon dioxide: PCO2
Net diffusion of a gas: high to low

Diffusion of gases in liquid Henry’s law states that the amount of gas
dissolved will be directly propotional to the partial pressure of the gas with which the liquid is in equilibrium.
PO2 of Gas phase> PO2
of liquid phase O2 dissolved in water
water
O2
Balance:
gas phase PO2 = liquid phase PO2
(alveolar)
(capillary)
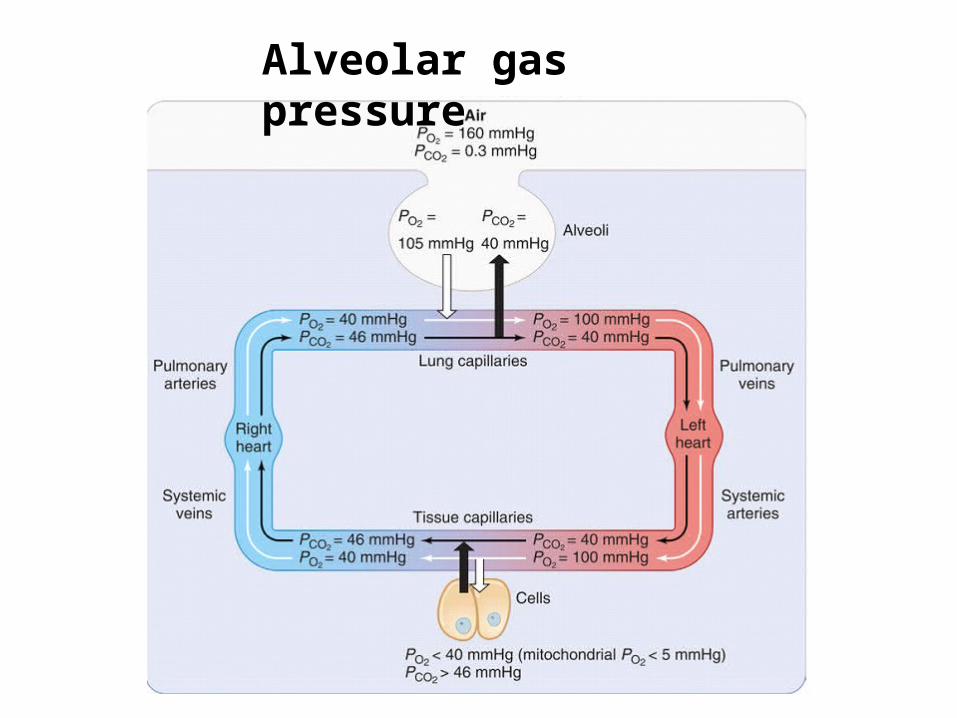
Alveolar gas pressure

The factors that determine the precise value
of alveolar PO2 are
(1) the PO2 of atomospheric air,
(2) the rate of alveolar ventilation,
(3) the rate of total body oxygen conusmption.
The factors that determine the precise value
of alveolar PCO2 are
(1) the rate of alveolar ventilation,
(2) the rate of total body oxygen conusmption.

The relationship of alveolar ventilation and partial pressure

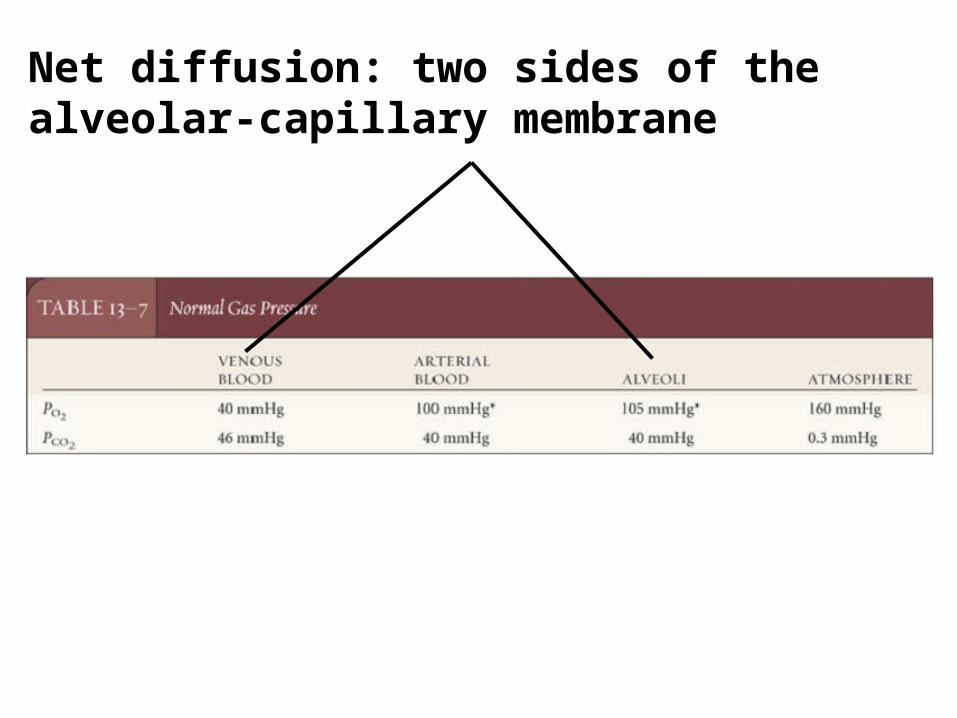
Net diffusion: two sides of the alveolar-capillary membrane

Lung infection Lung edema Diffuse interstitial fibrosis

Ventilation-perfusion inequality
Alveolar air flow (ventilation) and capillary blood flow (perfusion) mismatching.
The major effect is lower PO2 of the
systemic arterial blood.
Gravity effect: to increase the filling of blood vessels at the bottom of the lung.
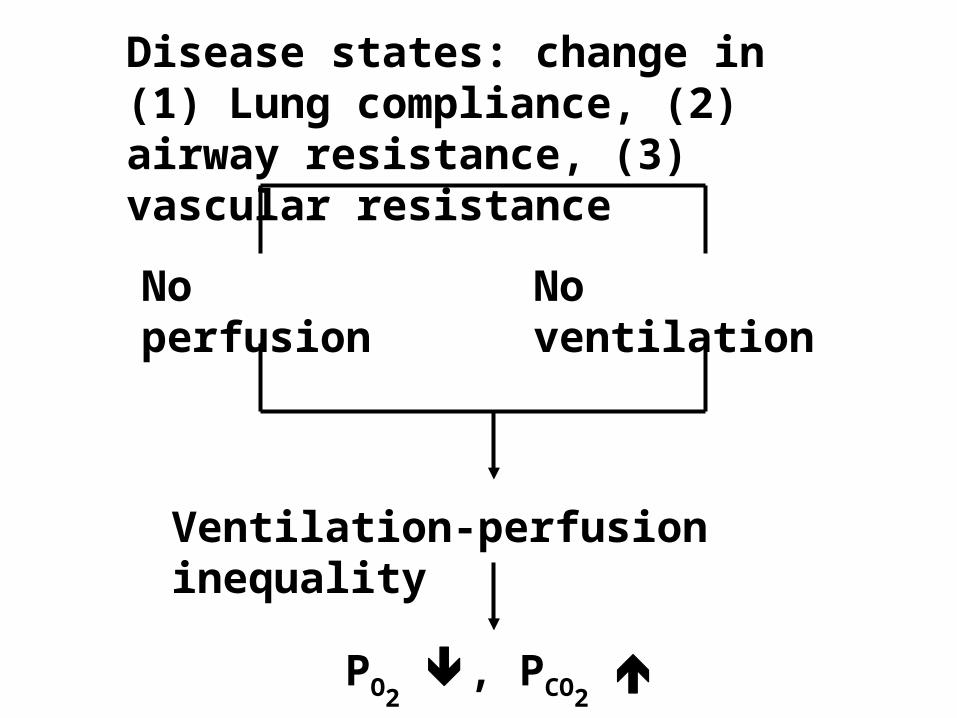
Disease states: change in (1) Lung compliance, (2) airway resistance, (3) vascular resistance
No perfusion
No ventilation
Ventilation-perfusion inequality
PO2 , PCO2

Local control of ventilation-perfusion matching
Transport of oxygen in blood

Normal arterial PO2 100
mmHg
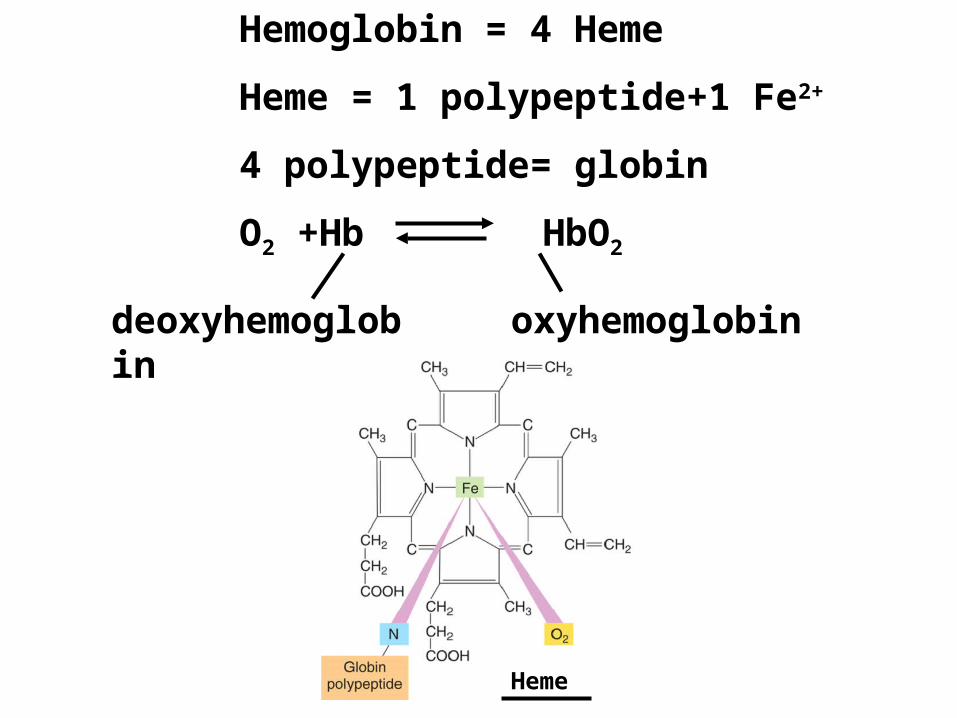
Hemoglobin = 4 Heme
Heme = 1 polypeptide+1 Fe2+
4 polypeptide= globin
O2 +Hb HbO2
deoxyhemoglobin
oxyhemoglobin
Heme

Percent hemoglobin (Hb) saturation
O2 bound to Hb
Maximal capacity of Hb to bind O2
X 100
=
Oxygen-carrying capacity of blood
The factors determined the percent hemoglobin saturation are PO2
and the amount of Hb.

What is the effect of PO2 on
hemoglobin saturation ?

Oxygen-hemoglobin dissociation curveThe law of mass action:
Blood PO2 oxygen-Hb combination

Effect of added hemoglobin on oxygen distribution
The oxygen bound to Hb dose not contribute directly to the PO2
of the blood; only dissolved oxygen does so.

Oxygen movement in the lung
PO2=40 mmHg
PO2=105
mmHg
Plasma PO2
oxygenerythrocyte
erythrocyte PO2
HbO2 formation

Oxygen movement in the tissues

Carbon monoxide
colorless, odorless gas
A product of incomplete combustion of hydrocarbons, such as gasoline.
It is about 200 times of high affinity for the oxygen binding sites in hemoglobin.
oxygen combined with Hb in lung capillary.
Shift the oxygen-hemoglobin dissociation curve to left.
unloading of oxygen from Hb in the tissues.
Factors influence the degree of hemoglobin saturation
Blood PO2
Blood PCO2
H+ concentration
Temperature
2,3-diphosphoglycerate (DPG), [also as
known as 2,3-Bisphosphoglycerate (BPG)]
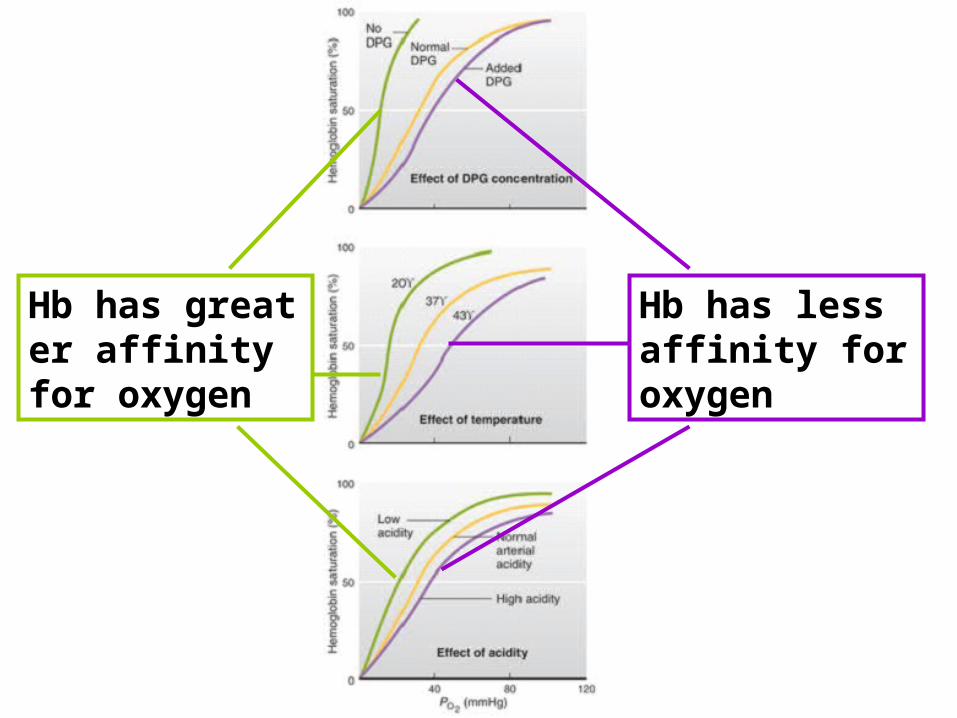
Hb has less affinity for oxygen
Hb has greater affinity for oxygen

Transport of carbondioxide (cell to blood)
Dissolved
Interstitial fluid
Dissolved
Dissolved
10%
30%
60%
(Carbonic anhydrase)
Chloride shift

Total blood carbon dioxide
The sum of
(1) Dissolved carbon dioxide (plasma and RBC)
(2) Bicarbonate (HCO3-)
(3) Carbon dioxide in carbamino hemoglobin
(HbCO2)

Transport of carbondioxide (blood to alveolus)
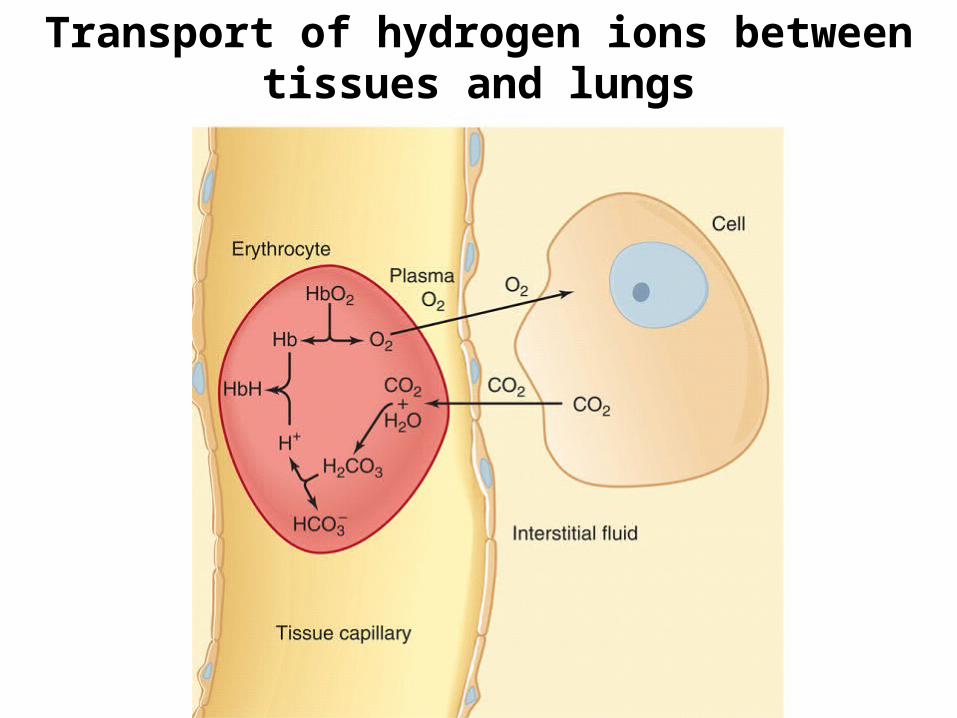
Transport of hydrogen ions between tissues and lungs

Hyperventilation and hypoventilation
Hyperventialtionrespiratory alkalosis:
arterial (1) PCO2 (2) H+
Hypoventialtionrespiratory acidosis:
arterial (1) PCO2 (2) H+


Nitric oxide (NO)
Lung
Blood
HbO2 HbNO
Peripheral tissues
Hb+O2 Hb+NO
NO:
(1) Vasodilator agent
(2) A treatment for persistent pulmonary hypertension in new born children

Control of respiration
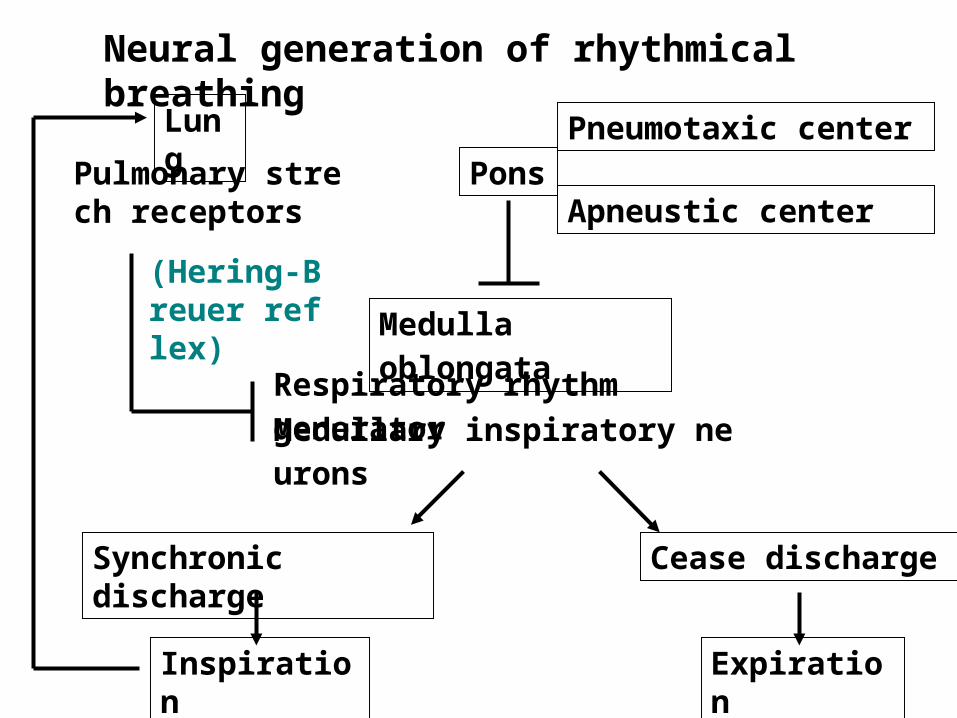
Neural generation of rhythmical breathing
Pons
Medulla oblongata
Pneumotaxic center
Apneustic center
Respiratory rhythm generator Medullary inspiratory neurons
Synchronic discharge
Cease discharge
Inspiration Expiration
LungPulmonary strec
h receptors
(Hering-Breuer reflex)

Control of ventilation by PO2
, PCO2, and H+
concentration

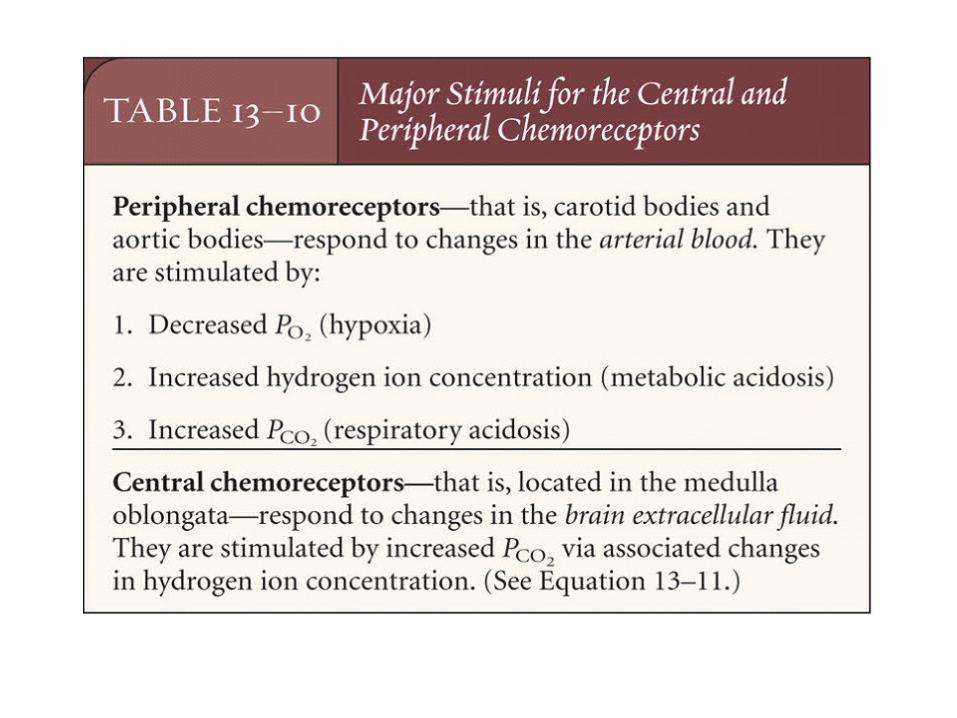
Peripheral chemoreceptors
Peripheral chemoreceptors provide excitatory synaptic input to the medullary inspiratory neurons.

(Under the PCO2=40 mmHg
condition)
The effect on ventilation of breathing low-oxygen mixtures.
Control by PO2
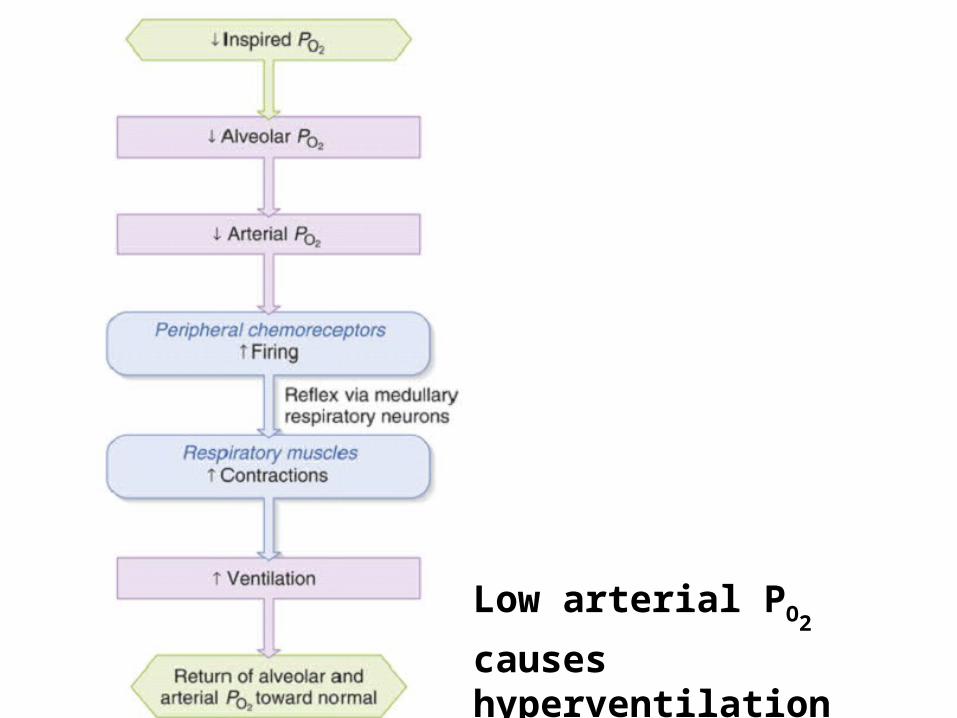
Low arterial PO2 causes
hyperventilation
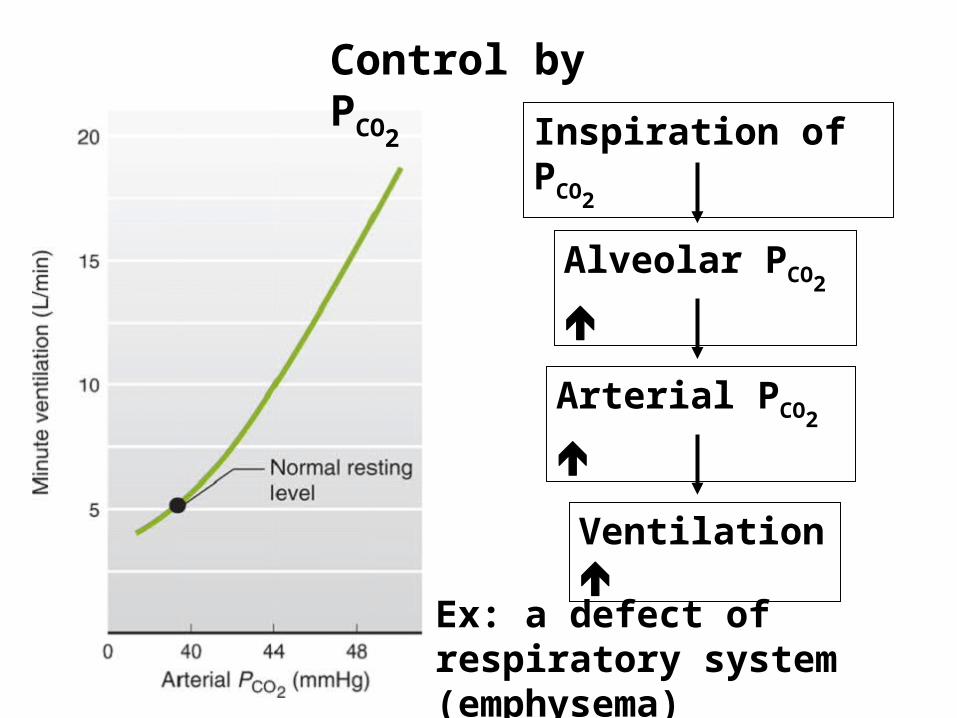
Control by PCO2 Inspiration of
PCO2
Alveolar PCO2
Arterial PCO2
Ventilation
Ex: a defect of respiratory system (emphysema)

Pathways by which increased arterials PCO2 stimulates
ventilation.
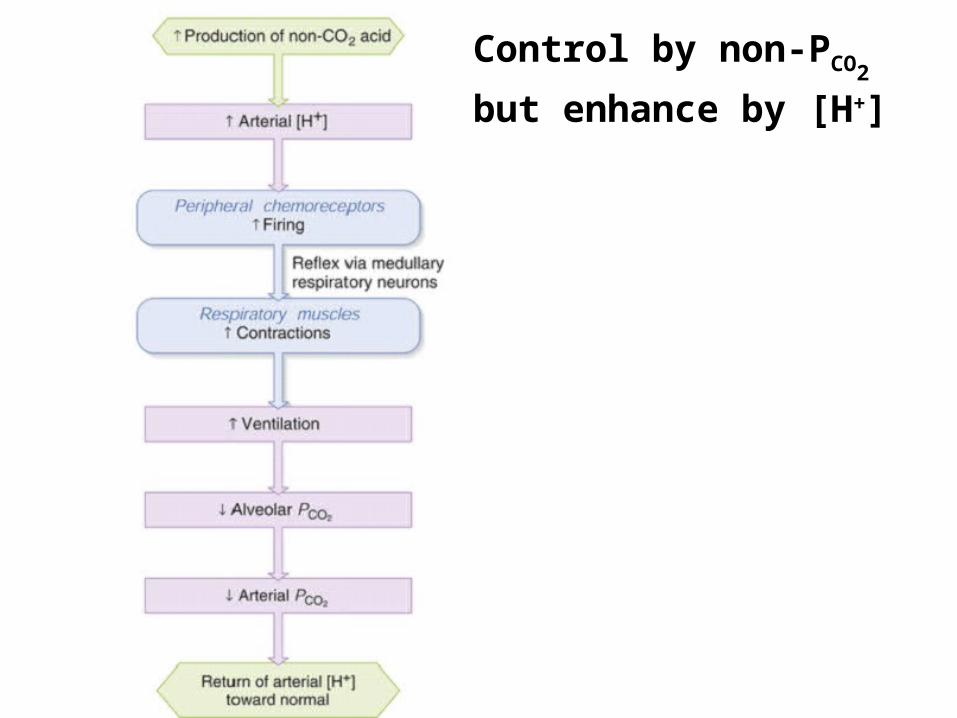
Control by [H+]

Respiratory acidosis: ventilation PCO2
[H+]
Respiratory alkalosis: ventilation PCO2
[H+]
Metabolic acidosis: [H+]
Metabolic alkalosis: [H+]
Elimination of PCO2
effect
The peripheral chemoreceptors play the major role in altering ventilation.
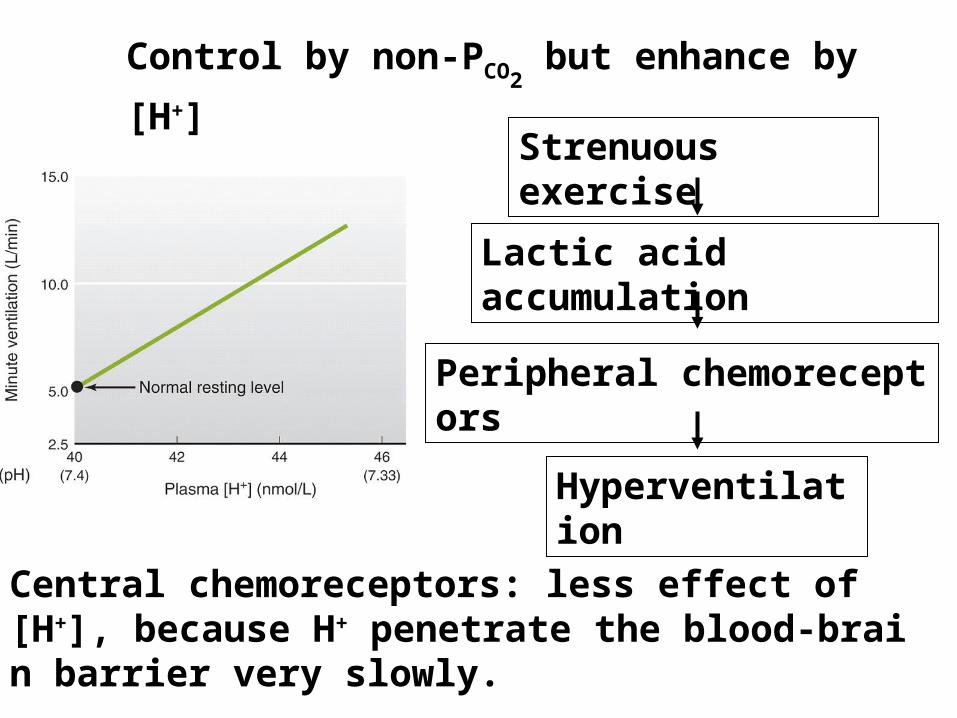
Control by non-PCO2 but enhance by
[H+]Strenuous exercise
Lactic acid accumulation
Peripheral chemoreceptors
Hyperventilation
Central chemoreceptors: less effect of [H+], because H+ penetrate the blood-brain barrier very slowly.
Control by non-PCO2
but enhance by [H+]
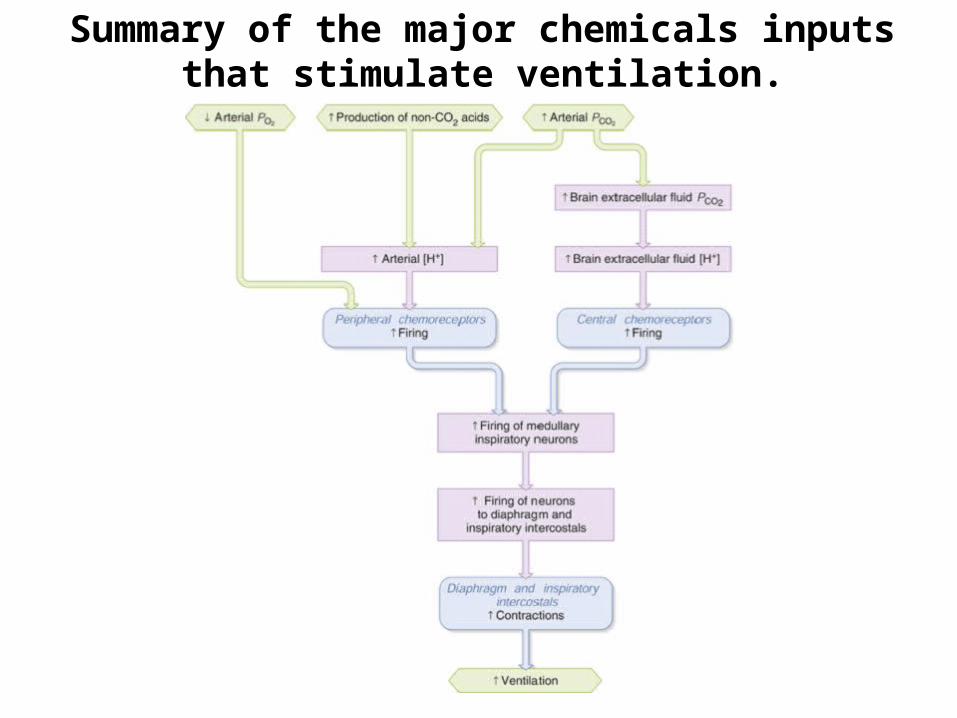
Summary of the major chemicals inputs that stimulate ventilation.

The effect of exercise on ventilation, arterial gas pressure and hydrogen ion
concentration.
Hyperventilation in strenuous exercise
Lactic acid accumulation
The roles of other factors stimulate ventilation Reflex input from mechanoreceptors in joints and muscles
Body temperature
Inputs to the respiratory neurons via branches form axons descending from the brain to motor neurons supplying the excising muscles
In the plasma epinephrine concentration
In the plasma potassium concentration
A conditioned (learned) response mediated by neural input to the respiratory centers.
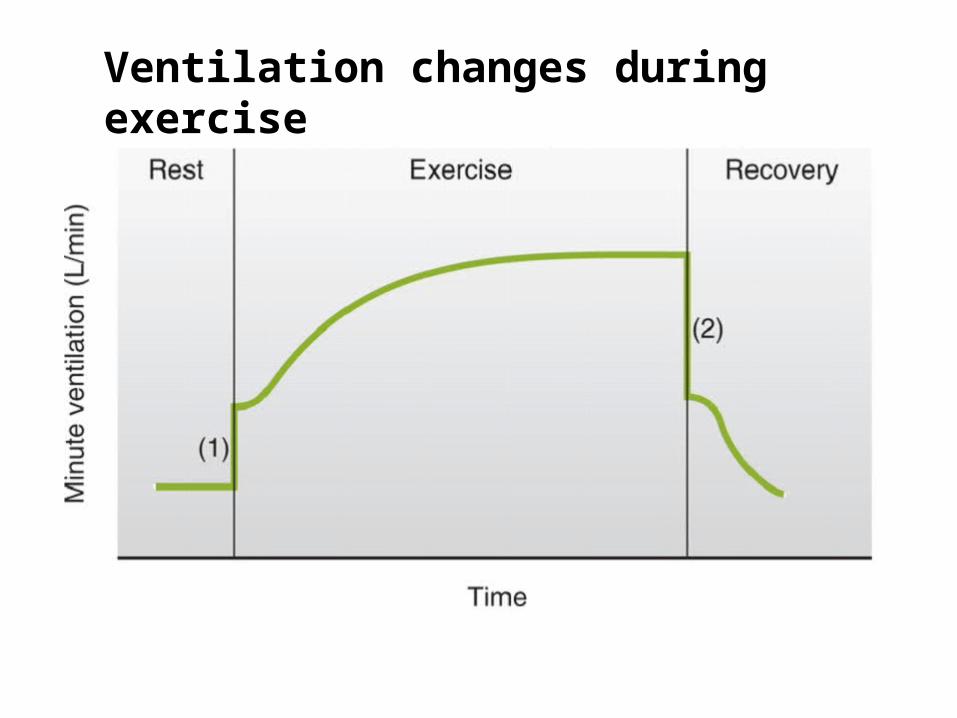
Ventilation changes during exercise
Other ventilatory responses
Protective reflexes: cough and sneeze reflexes
Voluntary control of breathing
Reflexs from J receptors: J receptors exist in the capillary wall or the interstitium

Hypoxia: a deficiency of oxygen at tissue level
Hypoxic hypoxia (hypoxemia) arterial PO2
Anemic or carbonmonoxide hypoxia inadequate numbers of RBC
Ischemic hypoxia (hypoperfusion hypoxia) blood flow to the tissues is too low
Histotoxic hypoxia toxicant interfere the cell’s metabolic machinery


~END~