Embed Size (px)
Citation preview

8/21/2019 Roelofs Et Al BDI 2013
http://slidepdf.com/reader/full/roelofs-et-al-bdi-2013 1/6
Norms for the Beck Depression Inventory (BDI-II)
in a Large Dutch Community Sample
Jeffrey Roelofs & Gerard van Breukelen &
L. Esther de Graaf & Aaron T. Beck & Arnoud Arntz &
Marcus J. H. Huibers
Published online: 31 July 2012# Springer Science+Business Media, LLC 2012
Abstract The Beck Depression Inventory (BDI-II) is a
widely used instrument that provides information about the
presence and severity of depressive symptoms. Although
the BDI-II is a psychometrically sound instrument, relative-ly little is known about norm scores. This study aimed to
develop reliable norms for the BDI-II in a Dutch community
sample. Gender, age, and education were hypothesized to
predict BDI-II scores. A total of 7,500 respondents from a
community sample in The Netherlands completed the BDI-
II. It was investigated by means of multiple regression
analysis whether distinct norms for genders, education lev-
els, and age group are appropriate. BDI-II scores depended
on gender and education level, but not on age. BDI-II norms
were computed based on the final regression model. These
BDI-II norms can be used for diagnostic purposes, clinical
decision making, or the evaluation of treatment effects.
Keywords BDI-II .
Beck DepressionInventory .
Depression .
Norming
Depression is one of the most common psychiatric disor-
ders. The epidemiological data suggest that prevalence rates
of depression range from 5 % to 17 % (Rihmer and Angst
2005), which underscores the importance of using reliable
and well-validated screening instruments. The measurement
of depressive symptoms was advanced by the development
of the Beck Depression Inventory (BDI: Beck et al. 1961).
The BDI was originally developed to detect, assess, and
monitor changes in depressive symptoms among individuals
in mental health care settings as well as primary care setting.
A second version of the inventory (BDI-II) was developed
to reflect revisions in the DSM-IV (APA 2000). The BDI-II
contains 21 items assessing symptoms and level of depres-
sion. Respondents are asked to choose one of four descrip-
tions that best fit how they have been feeling over the past
2 weeks. Each response is assigned a score ranging from
zero to three, indicating the severity of the symptom, with
total BDI-II scores ranging from 0 to 63. Although the BDI-
II is designed to provide information about the presence and
severity of depressive symptoms, it cannot by itself yield a
psychiatric diagnosis.
Despite the widespread research attention to examining
psychometric properties of the BDI-II, relatively few studies
have documented test norms. The revised manual describes
norm scores obtained by means of percentiles in 500 adult
psychiatric outpatients and a student sample of 120 college
students in Canada served as a control group (Beck et al.
1996b). This has led to interpretation guidelines of the BDI-
II in clinical samples with minimal depression (BDI-II range
0 – 13), mild depression (BDI-II range 14 – 19), moderate (BDI-
II range 20 – 28), and severe depression (BDI-II range 29 – 63).
J. Roelofs (*) : L. E. de Graaf : A. Arntz : M. J. H. Huibers
Department of Clinical Psychological Science,
Maastricht University,
P.O. Box 616, 6200 MD Maastricht, The Netherlands
e-mail: [email protected]
G. van Breukelen
Department of Methodology and Statistics, Maastricht University,
Maastricht, The Netherlands
L. E. de Graaf
Department of Medical Psychology and Psychotherapy,
Erasmus Medical Center,
Rotterdam, The Netherlands
A. T. Beck
Department of Psychiatry, University of Pennsylvania,
Philadelphia, PA, USA
A. Arntz
Netherlands Institute for Advanced Study in the Humanities
and Social Sciences,
Wassenaar, The Netherlands
M. J. H. Huibers
Department of Clinical Psychology, VU University Amsterdam,
Amsterdam, The Netherlands
J Psychopathol Behav Assess (2013) 35:93 – 98
DOI 10.1007/s10862-012-9309-2

8/21/2019 Roelofs Et Al BDI 2013
http://slidepdf.com/reader/full/roelofs-et-al-bdi-2013 2/6
Although these guidelines can assist the health care profes-
sional in determining the severity of depressive symptomatol-
ogy, it is recommended to determine norm scores in a variety
of non-clinical samples as well. The current study aimed to
establish norm scores in a large adult community sample.
The traditional approach to deriving norm scores is split-
ting a group into subgroups based on relevant background
variables. A disadvantage of this approach is that the samplesize is reduced resulting in less reliable norms. A multiple
regression analysis approach to norming questionnaire data
overcomes this problem. This approach allows for exami-
nation of whether background variables (e.g., gender, age)
are important for calculating norm scores. Importantly, it is
possible to test for interactions between predictors. In the
case these interactions are significant, norms on the basis of
subgroups should be created, which boils down to the tra-
ditional approach to norming questionnaire data. The
strength of a multiple regression approach is thus that one
can examine whether it is necessary to provide norm data
separately for various background variables. For example,Van Breukelen and Vlaeyen (2005) found that pain coping
and cognitions were not predicted by gender, but by level of
education instead, suggesting that norm data do not have to
be given for males and females separately. Similarly, Van
der Elst et al. (2006) found that performance on the Concept
Shifting Test was influenced by age, gender, and level of
education, but not by any of their interactions. Consequent-
ly, the most stable and simple norming was obtained by
applying a regression model with age, gender and education
as predictors of test score, and applying that model to the
complete sample.
In the current study, we calculated norm scores of the
BDI-II in a large community sample of adults. Gender was
hypothesized to be a significant predictor of BDI-II scores
as prevalence rates of depression in females is generally
higher compared to males (Picinelli and Wilkinson 2000).
Evidence for a relation between age and symptoms of de-
pression is equivocal with studies finding positive associa-
tions (e.g., Glenn et al. 2001) a curvilinear relationship
(Steer et al. 1999), or no relationship (Beck et al. 1996b).
Age was therefore examined as both a linear and curvilinear
(quadratic) effect. There is also some evidence that educa-
tion level is (negatively) related to depressive symptoms
(Arnau et al. 2001) and education level was therefore hy-
pothesized to predict BDI-II scores as well. The aim of the
current study was to determine norm scores for the BDI-II
following a state-of-the-art methodology in a large commu-
nity sample. The effects of gender, age, education level and
the interaction effects of these predictors were examined to
determine whether norming should take place in the total
group or in subgroups. Norming of the BDI-II was done on
the total scale scores as factor analytic studies have yielded
variability in, and instability of, obtained factor solutions of
the BDI-II (Osman et al. 2008; Ward 2006). Moreover, the
BDI-II has been advanced as a general screening instrument
for depressive symptomatology in general, more than for
subfactors.
Method
Participants and Procedure
Data were collected as part of a large-scale community
screening program for the recruitment of individuals who
could participate in a randomized clinical trial on the effec-
tiveness of computerized cognitive behavioral therapy for
depression. A random selection of individuals in the general
population (age range: 18 – 65 years) received an invitation
letter to complete a screening questionnaire via the internet.
Six municipalities in the Southern part of the Netherlands
cooperated by providing names and addresses of their resi-
dents. More specifically, the municipalities provided a totalof 217.816 names and addresses and letters were sent to
these addresses with the request to participate in this study.
In the letter, no reference was made to research on the
treatment of depression but this information was provided
on the website where participants completed the BDI-II. In
the letter, it was emphasized that everyone could participate
even if one had no symptoms of depression. A total of 8,960
individuals responded but the first 1,460 individuals com-
pleted the BDI-primary care version and not the BDI-II.
After these 1,460 respondents, the BDI-II was used instead
of the BDI-primary care version. A total number of 7,500
individuals completed the BDI-II. Participants were not
reimbursed for their efforts (see de Graaf et al. 2009). A
comparison of the demographic variables of the current
sample and the population in the Southern part of the Neth-
erlands (Statistics Netherlands, www.cbs.nl) did not reveal
any major discrepancies. The Ethical Committee of the
academic hospital Maastricht and Maastricht University ap-
proved the study protocol. In the description of the commu-
nity sample, 57.3 % was female ( N 04,300) and 42.7 % male
( N 03,200). Mean age was 43.3 years (SD 013.3 years,
range 18 – 65 years). Mean duration of depressive complaints
was 2.2 months (SD03.2). A total of 70.7 % had a paid job,
10 % were students, 8.2 % received a disablement insurance
benefit, 6.5 % were retired early, and 4.2 % had no work. A
total of 97 % of the total sample were Caucasian.
Instruments
Beck Depression Inventory
The Beck Depression Inventory-II (BDI-II; Beck et al.
1996b; Dutch version: Van der Does 2002) is a 21-item
94 J Psychopathol Behav Assess (2013) 35:93 – 98

8/21/2019 Roelofs Et Al BDI 2013
http://slidepdf.com/reader/full/roelofs-et-al-bdi-2013 3/6
self-report depression inventory designed to assess symp-
toms and level of depression. The questionnaire consists of
21 items comprising a list of four statements each about a
particular symptom of depression. Scores on the individual
items range from zero to three. The respondent has to
choose the statement that best represented his or her mood
during the last 2 weeks. Total scores can range between 0
and 63 with higher scores reflecting higher levels of depres-sion. Reliability and validity of the BDI-II have been sup-
ported (e.g., Osman et al. 2008; Van der Does 2002).
Demographic Variables
Demographic variables included gender, age, and education.
Regarding education, the highest completed level of training
was rated on an 8-point scale with 10no education,
20elementary school, 30lower technical and vocational
training, 40medium technical and vocational training,
50higher general secondary education, 60 pre-university ed-
ucation, 70 bachelor ’s degree, 80master ’s degree. Educationlevel was further categorized as follows: low education
(1,2,3: 14.7 %]), medium education (4,5,6: 50.4 %), and
high education (7,8: 35 %). Duration of depressive symp-
toms was rated on an 8-point scale with 10less than 1 month,
201 mo n th , 302 mo n th s , 403 mo n th s , 504 months,
605 months, 706 months, and 80more than 6 months.
Statistical Analyses
The Statistical Package for the Social Sciences (SPSS, ver-
sion 15.0) was used to perform regression analyses in order
to determine a parsimonious model for obtaining BDI-II
norms (see Van Breukelen and Vlaeyen 2005, for a detailed
description). Total BDI-II score was the dependent variable
in the regression analyses, and gender, age, education level,
and their interactions were the predictor variables. Dummy
coding was used for the categorical predictors gender
(females 0 0, males 0 1) and education level (low, medium,
high), with low education as reference group. Dummy cod-
ing involves the inclusion of a regression weight in the
model to represent the mean scale difference between the
reference category and each other category, adjusted for all
other predictors in the model. Linear and quadratic terms
were included for the quantitative predictor age, which was
centered to prevent collinearity between linear and quadratic
age terms.
The regression model was reduced in a stepwise fashion
by eliminating the least significant predictor, starting with
the interaction terms between the various predictors. Varia-
bles with a two-tailed p >.001 were excluded to prevent type
I error due to multiple testing. Note that with α0.001 two-
tailed, the present sample size of N 07,500 still gives a
power of 90 % to detect a correlation as small as .05, so
that the risk for type II error is negligible. For the final
model, residuals were plotted and analyzed to check the
assumptions of normality and homogeneity of residual var-
iance across the entire range of predicted scale scores and
the absence of outliers. Within the final model, a raw scale
score of an individual can be converted into a standardized
z-score by computing the predicted score Y (by means of
filling in the regression equation), computing the residualerror (subtracting predicted Y from observed Y), and finally,
dividing the residual error by the SD(e), which is the square
root of the MS(residual). If the residuals are normally dis-
tributed with the same variance, then z is normally distrib-
uted and the standard normal distribution can be used to
interpret z-values (e.g., Van Breukelen and Vlaeyen 2005).
If normality or homogeneity is seriously violated, percen-
tiles of the residuals can be used instead of z-values for
norming.
Results
Before addressing the main results, two remarks need to be
made. First, total BDI-II scores were not normally distrib-
uted with skewness and kurtosis outside the acceptable
range of −1 to +1. A square root-transformation of the
BDI-II total score was successful in ‘normalizing’ the total
scores to a reasonable extent (note that the residual of the
regression requires a normal distribution, not the dependent
variable itself). These square root-transformed BDI-II scores
were back-transformed into normal BDI-II scores after the
regression analyses in order to obtain norm data. Second,
mean BDI-II score was 10.6 (SD010.9; range 0 – 62) and the
BDI-II was reliable in terms of internal consistency with an
alpha of .95. Mean of the square root transformed BDI-II
scores was 2.77 (SD01.71; range 0 – 7.87).
Predictors of the BDI-II Score
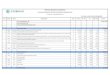
The final model containing significant predictors of the
BDI-II score consisted of gender and education level. None
of the interactions was significant, and after their deletion
from the model, age (linear and quadratic terms) did not
predict BDI-II total scores either. So norming can be per-
formed on the total sample, using gender and education
level as the only predictors. The final model is presented
in Table 1.
Model Checks
To apply the model for norming purposes, the model assump-
tions need careful checking as prediction of individual scores
depends even more on such assumptions than the regression
analysis does. More specifically, the use of (standardized)
J Psychopathol Behav Assess (2013) 35:93 – 98 95

8/21/2019 Roelofs Et Al BDI 2013
http://slidepdf.com/reader/full/roelofs-et-al-bdi-2013 4/6
residuals requires a normal distribution with homogeneous
variances of the residual. Normality was checked by means
of skewness and kurtosis and the Kolmogorov-Smirnov test.
Skewness and kurtosis were within the acceptable range of −1
to +1, but the Kolmogorov-Smirnov test revealed violation of
normality ( z 03.51, p <.001). However, note that theKolmogorov-Smirnov test gives significance even with minor
violation of normality in large samples like the present one. In
fact, the residual distribution looked quite normal in both
samples. As a further check, actual percentiles (5, 10, 25, 50,
75, 90, 95) of the standardized residuals were compared to the
corresponding percentiles of the standard normal distribution,
which revealed no deviation larger than .10 on the z -scale for
the standardized residuals. The homogeneity of variances was
tested by grouping patients into quartiles of the predicted scale
score and applying Levene’s test to the residuals. The homo-
geneity assumption was not violated ( p>.05) and the residual
standard deviation within each quartile did not deviate morethan 10 % from the overall residual standard deviation of the
scale. Thus, the overall residual standard deviation can be
used to compute z-scores.
Computing z-Scores
The model in Table 1 can be used to convert raw BDI-II
scores of any individual into a standardized residual or z-
score. The results are shown in the upper part of Table 2. To
illustrate how Tables 1 and 2 can be applied, consider a
woman, with medium education level and a BDI-II score of
25. Table 1 gives a predicted square root-transformed BDI-II
score of 3.51 (constant) −.25 (gender 00) −.55 (education
medium01) −1.03 (education high 0 0) 02.96. The residual
standard deviation is √ 2.7701.66. Thus, the z-score is equal
to (√ 25 – 2.96)/1.6601.23 according to Table 1.
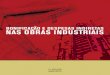
Finally, to further enhance user-friendliness of the present
norming, a norm table was derived (see upper part of Table 2).
Note that the norm scores depicted in Table 2 are estimated on
the basis of the full sample using the model in Table 1. The
following z-scores were chosen: −1.64, −.84, −.25, .25, .84,
and 1.64. As the residuals from which the z-scores were
computed had a normal distribution and the actual per-
centiles agreed very well with percentiles according to
the normal distribution, these z-scores correspond to the
traditional norming boundaries of 5th, 20th, 40th, 60th,
80th, and 95th percentile respectively. Raw BDI-II scores
corresponding to the boundaries were computed. Table 2 also
provides the formula for each subgroup by which one caneasily convert raw BDI-II scores into standardized scores.
BDI-II scores that, in terms of their standardized residual, lie
below the 80th ( z 0.84) percentile are considered normal
depression scores, whereas scores between the 80th and
95th ( z 01.64) percentile are elevated depression scores.
BDI-II scores above the 95th percentile are high depres-
sion scores. Back to the example, the woman with a BDI-II
score of 25 has a z-score of 1.23, which is indicative of an
elevated depression score. 1
Discussion
The aim of the present study was to develop reliable and
representative norms for the BDI-II in a large-scale Dutch
community sample. Using multiple regression, predictors
for BDI-II total scores were identified (i.e., gender, educa-
tion level) and, after some model checks, norm scores were
calculated.
Predictors for BDI-II Norm Scores
As hypothesized, gender was a significant predictor of BDI-
II total scores, with females having somewhat higher BDI-IIscores than males. These findings are in line with prevalence
rates in depression being higher in females than in males
(Picinelli and Wilkinson 2000) and with research findings
showing that females have higher scores than males (Arnau
et al. 2001; Beck et al. 1996b; Coelho et al. 2002; Kojima et
al. 2002; Kumar et al. 2002; Steer et al. 1997, 1998, 1999),
but contradict other studies reporting no significant gender
differences on the BDI-II (Beck et al. 1996a ; Dozois et al.
1998; O’Hara et al. 1998; Penley et al. 2003; Schulenberg
and Yutrzenka 2001; Steer and Clark 1997; Steer et al.
2000). Age did not correlate with the BDI-II total scores
(i.e., no linear or quadratic age effects). These findings addto research showing little relationship between the BDI-II
scores and age in samples of outpatients or college students
(Beck et al. 1996b; Kojima et al. 2002; Penley et al. 2003;
Steer et al. 1997), but are not in line with studies reporting
1 As an ancillary analysis, we determined the BDI-II norm scores for a
model with no predictors to allow for a comparison of an individual
BDI-II score with the total sample. Table 2 presents the BDI-II norm
scores for that model.
Table 1 Regression model for predictors of the (square root) BDI-II
scores
N 07,500, R20.05, MSresidual02.77
Predictor B SE of B p (two-tailed)
Constant 3.51 .050 <.001
Gender −.25 .039 <.001
Medium education −.55 .055 <.001
High education −1.03 .058 <.001
Gender was coded 0 for females and 1 for males. Low education was
the reference groups. Square root depression scores (BDI-II) range
roughly between 0 and 8
96 J Psychopathol Behav Assess (2013) 35:93 – 98

8/21/2019 Roelofs Et Al BDI 2013
http://slidepdf.com/reader/full/roelofs-et-al-bdi-2013 5/6
that depression is more likely with increasing age (Glenn et
al. 2001) or that severity of self-reported depression
scores gradually increases from 18 to 38 years of age
and then decrease to age 82 years (Steer et al. 1999),
suggesting a quadratic age effect. Note, however, that
the current study included individuals aged between 18and 65 so that a quadratic age effect should be visible.
It might be that a quadratic age effect disappears when
controlling for the effects of gender and education level
as was done in the current study. For education level,
higher BDI-II scores were found to relate to lower
education levels, which is in line with our hypothesis
and with previous research (Arnau et al. 2001).
Implications
With respect to the norm data, the interpretation of raw
BDI scores depends on gender and education level. Z -
scores computed from the residuals of the present re-
gression of (square root) scores of BDI-II on these
variables, can provide a more objective picture of the
meaningfulness of depressive symptoms in adults. That
is, z -scores can be helpful to identify the severity of the
problems and also to evaluate treatment success. How-
ever, the results should be cautiously interpreted in
terms of what BDI-II scores may have (preventive)
treatment implications. In this respect, a number of
cutoff scores for the BDI-II have been identified ranging
from 14 to 18 in different samples (Sprinkle et al. 2002;
Arnau et al. 2001; Dutton et al. 2004). The choice of a
particular cutoff point depends in part on the purpose
for using the test. If the purpose is to detect the max-
imum number of persons with depression, then the cut-
score threshold must be lowered to minimize false neg-
atives. If it is important to obtain as pure a group of
pers ons wi th de pres sion as poss ib le , th e cut- score
should be raised to reduce the number of false positives.
Thus, the norm data are indicative of where a person with a
certain BDI-II score lies in terms of z -scores compared to the
best possible reference group but the norm data cannot be used
for determining thresholds for a certain intervention. That is, a
score of 29 (cutoff for severe depression according to Beck et
al. 1996b) on the BDI-II corresponds to different z -scores
depending on gender and education level, but it does not
indicate that the personal burden is also different. Further-more, a decision to offer treatment should never be based on a
BDI-II score alone, but should be decided upon a diagnostic
evaluation. In clinical practice, much more is needed for an
informed decision: only the severity of the depressive symp-
tomatology will not do, and additional data regarding comor-
bidity, functioning, motivation for trea tment is neede d.
Normative data merely position a respondent in the normal
population.
Strengths and Limitations of the Current Study
The results of the current study advance the BDI-II as screen-
ing instrument for depression and provide reliable and repre-
sentative norms for an adult community sample. It is a strength
of the BDI-II that it takes only 5 – 10 min to fill in and its
reliability is good. Another strength of the study is that a large
sample of adults was involved, deriving from different educa-
tion levels, which enhances the generalization. A number of
limitations of the present study need to be addressed. First,
norm data obtained in the current study were found for the
Dutch version of the BDI-II. It should be borne in mind that
norming is culture and translation bound. As a consequence,
the present norms are not generalizable to other language
versions of the BDI or to populations stemming from other
countries. It is quite likely that respondents from other
countries or cultures respond differently to self-report ques-
tionnaires. Second, the current study used an in internet-based
approach to completing the BDI-II (see also Schulenberg and
Yutrzenka 2001). Paper-and-pencil and web-based administra-
tions appear to yield equivalent results at least for the Child
Depression Inventory (see Roelofs et al. 2010). Third, it is
possible that selection bias might have occurred. Although
there was no reference to research on the treatment of
Table 2 Norms of the BDI-II total score in a community sample breakdown by gender and education level
5th
Percentile
( z 0−1.64)
20th
Percentile
( z 0−.84)
40th
Percentile
( z 0−.25)
60th
Percentile
( z 0 .25)
80th
Percentile
( z 0.84)
95th
Percentile
( z 01.64)
Formula for computing
z scores in (sub)groups:
Males Low education 0 3 8 14 22 36 z ¼ p BDI scoreð Þ 3:26ð Þ 1:66=
Medium education 0 2 5 10 17 30 z ¼ p BDI scoreð Þ 2:71ð Þ 1:66=
High education 0 1 3 7 13 25 z
¼ p BDI scoreð Þ
2:23
ð Þ 1
:66
=Females Low education 0 4 10 15 24 39 z ¼ p BDI scoreð Þ 3:51ð Þ 1:66=
Medium education 0 2 6 11 19 32 z ¼ p BDI scoreð Þ 2:96ð Þ 1:66=
High education 0 1 4 7 15 27 z ¼ p BDI scoreð Þ 2:48ð Þ 1:66=
Total sample 0 2 6 11 18 32 z ¼ p BDI scoreð Þ 2:77ð Þ 1:71=
J Psychopathol Behav Assess (2013) 35:93 – 98 97

8/21/2019 Roelofs Et Al BDI 2013
http://slidepdf.com/reader/full/roelofs-et-al-bdi-2013 6/6
depression in the recruitment letters that were sent and all
individuals, even those without depressive symptoms, were
encouraged to participate, one cannot rule out that those with
higher levels of depressive complaints were more likely to
participate, as indicated by the mean duration of depressive
symptoms, which was about 2 months. Finally, practitioners
should keep in mind that self-report inventories are subject to
response bias (Beck et al. 1996b; Hunt et al. 2003). Someindividuals may magnify symptoms, and other may minimize
them. Therefore, determination of the presence and severity of
depression will require additional exploration. Despite these
limitations, the current study contributes to the usefulness of
the BDI-II by providing norm scores that can assist researchers
and clinicians in assessing depression severity with the BDI-II.
Acknowledgments We would like to express our gratitude to Annie
Hendriks, Greet Kellens, and Sylvia Gerhards, who assisted with data
collection, and to Rosanne Janssen, who developed the infrastructure
for online data collection. Municipalities Eijsden, Meerssen, Sittard-
Geleen, Valkenburg, and Maastricht sponsored the study. Competing
interests: the authors have no competing interests.
References
American Psychiatric Association. (2000). DSM-IV-TR: diagnostics
and statistical manual of mental disorders-Text revision (4th
ed.). Washington, D.C.: American Psychiatric Association.
Arnau, R. C., Meagher, M. W., Norris, M. P., & Bramson, R. (2001).
Psychometric evaluation of the Beck Depression Inventory-II with
primary care medical patients. Health Psychology, 20, 112 – 119.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J.
(1961). An inventory for measuring depression. Archives of Gen-
eral Psychiatry, 4, 561 –
571.Beck, A. T., Steer, R. A., Ball, R., & Ranieri, W. F. (1996a). Compar-
ison of Beck Depression Inventories-IA and – II in psychiatric
outpatients. Journal of Personality Assessment, 67 , 588 – 597.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996b). Beck Depression
Inventory (2nd ed.). San Antonio: The Psychological Corporation.
Coelho, R., Martins, A., & Barros, H. (2002). Clinical profiles relating
gender and depressive symptoms among adolescents ascertained
by the Beck Depression Inventory II. European Psychiatry, 17 ,
222 – 226.
De Graaf, L. E., Gerhards, S. A. H., Arntz, A., Riper, H., Metsemakers,
J. F. M., Evers, S. M. A. A., et al. (2009). Clinical effectiveness of
online computerised cognitive-behavioural therapy without sup-
port for depression in primary care: randomised trial. The British
Journal of Psychiatry, 195, 73 – 80.
Dozois, D. J. A., Dobson, K. S., & Ahnberg, J. L. (1998). A psycho-metric evaluation of the Beck Depression Inventory-II. Psycho-
logical Assessment, 10, 83 – 89.
Dutton, G. R., Grothe, K. B., Jones, G. N., Whitehead, D., Kendra, K.,
& Brantley, P. J. (2004). Use of the Beck Depression Inventory-II
with African American primary care patients. General Hospital
Psychiatry, 26 , 437 – 442.
Glenn, M. B., O’ Neil-Pirozzi, T., Goldstein, R., Burke, D., & Jacob, L.
(2001). Depression amongst outpatients with traumatic brain in-
jury. Brain Injury, 15, 811 – 818.
Hunt, M., Auriemma, J., & Cashara, A. C. (2003). Self-report bias and
underreporting of depression on the BDI-II. Journal of Personality
Assessment, 80, 26 – 30.
Kojima, M., Furukawa, T. A., Takahashi, H., Kawai, M., Negaya, T., &
Tokudome, S. (2002). Cross-cultural validation of the Beck Depres-
sion Inventory-II in Japan. Psychiatry Research, 110, 291 – 299.
Kumar, G., Steer, R. A., Teitelman, K. B., & Villacis, L. (2002).
Effectiveness of Beck Depression Inventory-II subscales in
screening for major depressive disorders in adolescent psychiatric
inpatients. Assessment, 9, 164 – 170.
O’Hara, M., Sprinkle, S. D., & Ricci, N. A. (1998). Beck Depression
Inventory-II: college population study. Psychological Reports, 82,
1395 – 1401.
Osman, A., Barrios, F. X., Gutierrez, P. M., Williams, J. E., & Bailey, J.
(2008). Psychometric properties of the Beck Depression
Inventory-II in nonclinical adolescent samples. Journal of Clinical
Psychology, 64, 83 – 102.
Penley, J. A., Wiebe, J. S., & Nwosu, A. (2003). Psychometric prop-
erties of the Spanish Beck Depression Inventory-II in a medical
sample. Psychological Assessment, 15, 569 – 577.
Picinelli, M., & Wilkinson, G. (2000). Gender differences in depres-
sion. The British Journal of Psychiatry, 177 , 486 – 492.
Rihmer, Z., & Angst, J. (2005). Mood disorders: epidemiology. In B. J.
Sadock & V. A. Sadock (Eds.), Kaplan & Sadock ’ s comprehensive
textbook of psychiatry (pp. 1575 – 1581). Philadelphia: Lippincott,
Williams, & Wilkins.
Roelofs, J., Braet, C., Rood, L., Timbremont, B., van Vlierberghe, L.,
Goossens, L., et al. (2010). Norms and screening utility of the
Dutch/Flemish version of the Children’s Depression Inventory
(CDI) in clinical and non-clinical youth. Psychological Assess-
ment, 22, 866 – 878.
Schulenberg, S. E., & Yutrzenka, B. A. (2001). Equivalence of com-
puter ized and conventional versions of the Beck Depres sion
Inventory-II (BDI-II). Current Psychology, 20, 216 – 230.
Sprinkle, S. D., Lurie, D., Insko, S. L., Atkinson, G., Jones, G. L.,
Logan, A. R., et al. (2002). Criterion validity, severity cut scores,
and test-retest reliability of the Beck Depression Inventory-II in a
university counselling center sample. Journal of Counseling Psy-
chology, 49, 381 – 385.
Steer, R. A., & Clark, D. A. (1997). Psychometric characteristics of the
Beck Depression Inventory-II with college students. Measure-
ment and Evaluation in Counseling and Development, 30, 128 –
136.
Steer, R. A., Ball, R., Ranieri, W. F., & Beck, A. T. (1997). Further
evidence for the construct validity of the Beck Depression
Inventory-II with psychiatric outpatients. Psychological Reports,
80, 443 – 446.
Steer, R. A., Kumar, G., Ranieri, W. F., & Beck, A. T. (1998). Use of
the Beck Depression Inventory-II with adolescent psychiatric out-
patients. Journal of Psychopathology and Behavioral Assessment,
20, 127 – 137.
Steer, R. A., Ball, R., Ranieri, W. F., & Beck, A. T. (1999). Dimensions
of the Beck Depression Inventory-II in clinically depressed out-
patients. Journal of Clinical Psychology, 55, 117 – 128.
Steer, R. A., Rismiller, D. J., & Beck, A. T. (2000). Use of the Beck
Depression Inventory-II with depressed geriatric inpatients. Be-
haviour Research and Therapy, 38, 311 –
318.Van Breukelen, G. J. P., & Vlaeyen, J. W. S. (2005). Norming clinical
questionnaires with multiple regression: the pain cognitions list.
Psychological Assessment, 17 , 336 – 344.
Van der Does, A. J. W. (2002). Handleiding bij de Nederlandse versie
van Beck Depression Inventory — second edition (BDI-II- NL).
Amsterdam: Harcourt.
Van der Elst, W., Van Boxtel, M. P. J., Van Breukelen, G. J. P., & Jolles,
J. (2006). The concept shifting test: adult normative data. Psycho-
logical Assessment, 18, 424 – 432.
Ward, L. C. (2006). Comparison of factor structure models for the
Beck Depression Inventory-II. Psychological Assessment, 18,
81 – 88.
98 J Psychopathol Behav Assess (2013) 35:93 – 98