-
8/18/2019 Sian 1994
1/8
ORIGINAL ARTICLES
Alterations in Glutathone LevelsPadanson’s Disease andOther
Neurodegenerative Disorders AfKectmgBasal Gangha
in
Jeswinder Sian, BSc,” David T. Dexter, PhD,* Andrew J. Lees,
FRCP,? Susan Daniel, MRCPath,?Yves Agid, MD, P hD J France
Javoy-Agid, Ph D, I Peter Jenner, DSc,” and C. David Marsden,
FRSi
Reduced glutathione (GSH) and oxidized glutathione (GSSG) levels
were measured in various brain areas (substantianigra, putamen,
caudate nucleus, globus pallidus, and cerebral cortex) from
patients dying with Parkinson’s disease,progressive supranuclear
palsy, multiple-system atrophy, and Huntington’s disease and from
control subjects with noneuropathological changes in substantia
nigra. GSH levels were reduced in substantia nigra in Parkinson’s
diseasepatients (40 compared to contro l subjects) and GSSG levels
were marginally (27 ) but insignificantly elevated;there were no
changes in other brain areas. The only significant change in
multiple-system atrophy was an increaseof GSH (176 ) coupled with a
reduction of GSSG (60 ) in the globus pallidus. Th e only change in
progressivesupranuclear palsy was a reduced level of GSH in the
caudate nucleus (5 1 ). Th e only change in Huntington’s diseasewas
a reduction of GSSG in the caudate nucleus (50 ). Despite profound
nigral cell loss in the substantia nigra inParkinson’s disease,
multiple-system atrophy, and progressive supranuclear palsy, the
level of GSH in the substantianigra was significantly reduced only
in Parkinson’s disease. This suggests that the change in GSH in
Parkinson’sdisease is not solely due to nigral cell death, or
entirely explained by drug therapy, for multiple-system
atrophypatients were also treated with levodopa. The altered
GSH/GSSG ratio in the substantia nigra in Parkinson’s diseaseis
consistent with the concept of oxidative stress as a major
component in the pathogenesis of nigral cell death inParkinson’s
disease.
Sian J, Dexter DT, Lees AJ, Daniel S , Agid Y avoy-Agid F,
Jenner P, Marsden CD.Alterations in glutathione levels in
Parkinson’s disease and other neurodegenerative
disorders affecting basal ganglia. Ann Neurol
1994;36:348-355
The process underlying dopaminergic cell loss in thesubstantia
nigra (SN) in patients with Parkinson’s dis-ease (P D) is unknown.
Recent evidence from postmor-tem studies indicates that the
induction of oxidativestress may play a role. Thus, in the SN of
patientsdying with P D there are increased levels of total iron[ l
, 23, decreased ferritin levels [3], increased lipid per-oxidation
14, 53, and a reduced activity of complex Iof t he mitochondria1
respiratory chain [63. Free radicaltoxicity normally is prevented
by a range of antioxidant
vitamins and protective enzymes. Most of these appearto be
intact in the SN in PD. Thus, levels of catalaseand glutathione
peroxidase are normal or moderatelyreduced [7-93 while superoxide
dismutase activitymay be increased [lo]. Normal levels of ascorbic
acidand a-tocopherol are found in the SN in PD [2, 111.
Another important component protecting againstoxidative stress
is reduced glutathione (G SH ), whichmay be depleted in PD.
Glutathione plays a majorrole in the removal of peroxides, so
preventing theformation of more damaging oxygen radicals, such
asthe hydroxyl radical. Normally a high ratio of reducedG S H to
oxidized glutathione (GSS G) is maintained1123. Glutathione is also
important for the maintenanceof a-tocopherol and ascorbic acid in
the reduced state1133. A disappearance of total glutathione and
GSH
content in the SN of patients dying with PD was firstreported by
Perry and colleagues 1141.However, thesefindings were criticized [
l 5 ] because of the high pro-portion of GSSG reported in control
subjects and be-cause of the total absence of GSH in PD
patients.Nevertheless, the concept of altered glutathione
levels
From the “Parkinson’s Disease Society Experimental
ResearchLabo-ratories, Pharmacology Gr oup , Biom edical Sciences
Division, King’sCollege London, Lo ndon; Warkinson’s Disease
Society Brain Ban k,University Departmentof Clinical Neurology,
Instituteof Neurol-ogy, National Hospital, London, United Kingdom;
and tLaboratoirede Medicine Experimental, I N S E M U289, HBpital
de la Salpg-trii.re, Paris, France.
Received Jul 29, 1993, and in revised form Feb 14 and May
19,1994. Accepted for publication May 19, 1994.
Address correspondence to p. Jenner, D S ~ , harmacology G ~ ~
~Biomedical Sciences Division, King,s College London, Manresa
Road, London sw3G ~ ~ ,K ,
348 Copyright 994 by the American Neurological Association
-
8/18/2019 Sian 1994
2/8
in PD is s u p p o r t e d b y a more recen t r epo r t by
Ried-e re r and co l l eagues (21 w h o s h o w e d t o ta l g lu t
a t h io n elevels to be r e d u c e d b y 50 , i n t h e SN. I t r
ema insu n c l e ar w h e t h e r a r e d u c t i o n i n GSH l eve
ls do es occu rin SN, w h e t h e r t h i s is speci f ic to PD, or
w h e t h e r itoccu r s i n other neu rodegene ra t i ve d i so
rde r s a f f ect i ngt h e SN. I t is a l so u n k n o w n w h e t
h e r a n y c h an g e i ng lu t a th ione i n SN i n PD occu r s
as a resul t
ofl e v o d o p a
t r ea tmen t .Cons equen t ly , w e have ana lyzed GSH a n d
GSSG
leve ls in a r a n g e of brain areas i n pa t i en t s with PD
a n din pa t i en t s w i th o the r degene ra t i ve d i so rde r
s , name lymul t i p l e - sys t em a t rophy MSA), prog re s s ive
sup ranu -clear palsy (PSP), and Hunt ing ton ’s d i s ea se(HD), a
n dc o m p a re d t h e m t o l ev e ls i nnormal individuals.
Materials and MethodsBrain tissue from patients dying with PD ,
PSP,or MSA andfrom con trol subjects dying of nonneurological
disorders was
obtained from the Brain Bank ofINSERM U28 9, HBpitalde la
[email protected],Paris, and the Parkinson’s Disease SocietyBrain Bank,
London. Tissue from patients dying withHDwas supplied by D r Gavin
Reynolds, De partme nt of Biomed-ical Science, Universityof
Sheffield.
Tissue PreparationIn London, at autopsy, brains were removed and
dividedmidsagittally. One-half of the brain was immediately
frozenat -20”C, transported on Cardiceto the Brain Bank, andfrozen
at 0°C until dissection. T he ot he r half of the brainwas placed
in 10% form ol saline solution for at least6 weeksprior to
neuropathological examination. In Paris, less than 2hours after
autopsy, the brainstem was first separated fromthe rest of the
brain. Subsequently, one hemisphere of thebrain was stored at 0°C
until dissection, while the ot he rhalf was used fo r
neuropathological examination.
T h e SN (total or zona compacta), putamen, caudate nu-cleus,
globus pallidus, and cerebral cortex (Brodm ann area10) were
dissected from frozen brain accordingto the tech-nique described by
D ext er and co authors 141. Samples fromeach brain area were
stored at - 0°C until the time of bio-
chemical analysis. Brain samples fr om patients with
neurolog-ical disease were assayed at the same time as samples
fromcont rol sub jects, which wer e matched as much as possiblefor
age and postm ortem delay.For som e sub jects, insufficientmaterial
was available for assaysto be undertaken in all re-gions of th e
individual brains. Th e num bers of samples stud-ied from each
brain area in each group are shown in Figures3 through 6. Whether
totalSN or zona compacta alon e was
utilized is stated in the legends of the individual
figures.Different control brains were used for comparison with
brains representing each of the neurodegenerative
diseasesstudied. This was undertaken to ensure appropriate
agematching and that postmortem handling, storage, and dissec-tion
were as similar as possible in each grou p. This was partic-ularly
important when brain material came from differentbrain banks and
every effort was madeto obtain matchedcontrol samples from the same
source of brain material.
Parkinson’s Disease GroupBrain tissue was obtained from 13
control subjects with noknown history of psychiatric or
neurological disorder and
16 P D p atients (Table 1). Histological diagnosis of P D
wasconfirmed in all the tissues utilized by the severe neuronalloss
in the SN pars compacta and the presence of Lewy bod-ies in
surviving cells. Th e control subjects and P D patientswere closely
matched for age and postmortem delay (timebetween death and removal
of brain). The caudate dopamineconten t was significantly lower in
the P D patients (1.02*0.25 pg/g m) compared to the control
subjects (2.84 0.40pg/gm; p < 0.05, Student’s test).
Multiple-System Atrophy GroupBrain tissue was obtained from10
control subjects withn oknown history of psychiatricor neurological
disorder and 7MSA subjects (Table 1. Pathological diagnosis of MS A
wasconfirmed by the presence of striatonigral degeneration
withmarked gliosis and cellloss in the SN, caudate nucleus,
andputamen. I n addition, there were pathological changes
thatvaried in severity involving the olivo pon tocere bellar
systemand preganglionic autonomic nuclei. Lewy bodies were
notobserved in any brain area from M SA patients. C ontrol
sub-jects and MSA patients were closely matched for age andpostm
ortem delay.
Table I Characteristics o f Control Subjects and Parkinson’s
Disease (P D, and Multiple-System Atrophy( M S A )Patientsa
Contro l P D Contro l MSAPatient Details (n = 13) (n = 16) (n =
10) (n = 7 )
Age (yr) 73.5 2.9 77.1 * 1.8 68.3 5.7 63.4 3.0Sex
Female 1 4 1 2Male 12 12 7 5
Age at onset of disease (y r) 66 .8 -c 2.5 56.4 ? 2.8(59-7 )
(47- 72)
Duration of disease (yr ) 12.4-c 3.1 7.0 0.9
Levodop a dosage level at time of
Tim e between death and removal 15.6 2.2 13.4? 1.9 14.2 1.5 17.0
* 8.6
(5-24) (3-10)470 * 180 mglday 618 116 mglday
death (100- 1,000 mg) (330-1,100 mg)
of brain (hr)
‘Values are expressed as mean 5 standard error of mean. Rangesof
values are indicatedin parentheses.
Sian et al: Glutathione Levels in P D and O the r
Neurodegenerative D isorders 349
-
8/18/2019 Sian 1994
3/8
Table 2. Characteristics of Control Subjects and Progressizle
Supranuclear Palsy PSP) nd Huntington's Disease ( H D
)Patients"
Patient Details ( n = 15) ( n = 11) ( n = 10) (n = 10)
Age (yr) 80.3 ? 1.9 70.0 2.2h 50.1 ? 4.7 52.9 ? 3.5Sex
Control PSP Control HD
Female 9 6 1 3Male 6 5 9 7
Duration of disorder yr) N A 9.4 ? 1.9Time between death and
removal of brain (hr) 9.4 ? 1.8 11.8 t 1.9 36.0 ? 7.3 50.7 ?
10.7h
"Values are representedas mean standard erro rof mean.p <
0.03 as compared to control subjects, Student's t test.
N A = not available
Progressive Supranuclear Palsy GroupBrain tissue was obtained
from 15 control subjects with n oknown history of psychiatricor
neurological disorder and 11PSP patients (Ta ble 2). Pathological
diagnosis of PSP wasconlirmed by nerve cell loss in the S N ,
globus pallidus, andbrainstem nuclei, including the locus ceruleus
and superiorcolliculus, and th e presen ce of globos e
neurofibrillary tanglesin surviving neurons in the pallidum,
subthalamic nucleus,midbrain, and d entate nucleus. Contro l
subjects and PSP pa-tients were closely matched for postmortem
delay, but themean age of PSP patients was significantly lower than
that ofcontrol subjects.
Huntington Diseau GroupBrain tissue was obtained from 10 control
subjects withn oknown history of psychiatricor neurological
disorder and 10HD patients (Table 2) . Morphological diagnosisof HD
wasconfirmed by macroscopic atrophy with gliosis and markedneuronal
loss in the caudate nucleus and putamen. The timebetween death and
removal of the brain was longer for theHD patients than the control
subjects.
Measurement of GfututhioiieLevelsBrain tissue was homogenized
in6 volumes ice-cold 0.4 Mperchloric acid containing 0.1 mM
diethylenetriaminepen-taacetic acid using a microsonic probe. The
samples werecentrifuged at 4,000 rpm , 4°C for 1 5 minutes, and th
e super-natant was analyzed for GSSG and G S H con tent
immediatelyafter homogenization.
Measurement of Oxidized GfutathionrGSSG was measured by the
enzymatic recycling proceduredescribed by Tietze [ 16) and Slivka
and coauthors[ 15).
An aliquot (0.1 ml) of the tissue supernatant was addedto 1.35
ml of I1 mM N-ethylmaleimide (N EM ) in100 mMpotassium phosphate
buffer containing 5 mM ethylene-diaminetetraacetic acid, p H 7 .5 .
After a 20-minute incuba-tion period at room temperature, the
reaction mixture waspassed th roug h Sep-P ak C- 18 cartridges
(,Millipore, Wa tersAssociates, Watford, United Kingdom )to remove
unreactedNEM. Preliminary experiments showed 99.6% (n= 6) ofthe
unreacted NEM was retained by the cartridges.
Spectrophotom etric assays were performed using1.5 ml ofeluate
to which 0.4 mM 5,5 -dithiobis-(L-nitrobenzoic cid)
(DTN B) , 0 .17 mM N AD PH , and 16 kg /mlof GSSG reduc-
case were added. The final assay volume was 2.0 ml. Thereaction
was initiated by the addition of GSSG reductase.
Th e rate of reduction of DT N B to 5-thio-2-nitrobenzoate(T N
B) was measured at 412 nm using a Shimadzu double-beam
spectrophotometer at ambient temperature for 5 min-utes. A srandard
curve was constructed using known amounts
of synthetic GS SG (10-100 ng). Th e standard curves toGSS G w
ere l inear r = 0.994) ov er this concentration range.
Measurement of Redui-ed GlutathioneG S H was measured using a
minor modification of themethod described by Reed and coauthors
171. An aliquot(0.17 ml) of tissue supernatant was added to the
internalstandard (1 mM cysteic acid) and 0.88 M iodoacetic
acid.Excess sodium hydrogen carbonate was addedto precipitatesodium
perchlorate. The samples were incubated at roomtempe rature in the
dark for an hour. Subsequen tly, 0.5 mlof an alcoholic solution of
1.5% (vo l/vo l) 2,4-dinitro-fluorobenzene was added and the
samples were incubatedfor a further 4 hours. Th en diethyl
ether(1.0 ml) was addedto the samples, which were shaken and then
centrifuged at2,000 rpm, room temperature, for2 0 minutes. T he
aqueo usphase containing derivatized glutathione was separated
andanalyzed by high -perfo rman ce liquid chromatography(HPLC).
Aliquots (10 ILL) were injected onto a Spherisorb S-5amino OD S
column (25 x 4.6 m m, Phase Separations) andeluted with an ammonium
acetate gradient in glacial aceticacid, methanol, and water (p H
5.05; flow rate 1.00-1.25 mlimin at 2,70 0 psi). G S H levels were
measured using a Watersultraviolet de tector (m odel 441) a t a
wavelength of 3 65 nm.Chromatographic peaks were integrated by a
Waters 645data module. G S H derivatives were quantified in
relationtothe internal standard (cysteic acid).
StatisticsGSH and GSSG levels in each brain region from
controlsubjects and patients with PD , MSA, PSP,or HD were
com-pared using an unpaired two-tailed Student'st test.
ResultsGlutathione Leiiels in Control SubjectsA high GSHIGSSG
ratio (mean, 318: 1; range, 226-800: 1) was observed in control
subjects fromall the
groups examined for the present study. Therewas no
350 Annals of Neurology Vol 3 6 N o 3 September 1794
-
8/18/2019 Sian 1994
4/8
rp
t 0 a M ) M I S o w
Age < I N
B
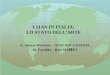
F i g I Linea r regression analys is fo r A ) educed
glutathione( G S H ) evels pniollgm wet weight) with age and ( B
)oxidizedglutathione GSSG) evels (pmollgm wet weight) with ageinthe
total substan tia nigra and pu tamen from control subjects.There
was n o correlation between gluta thione letleis and patientage
(regression coefficient< 0.01: n = 13-20),
obvious correlation betw een age and G S H or G SS Glevels in
the SN and putamen of control subjects (Fig1). Similarly, there was
no correlation between post-mortem delay (time berween death and
removal ofbrain) and GSH (Fig 2A) or GSSG (Fig 2 B ) contentin the
SN and putamen.
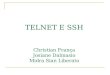
Glutathione Leuels in Parkin son's DiseaseTh ere was a
significant reduction in G S H in theSN( 4 0 % ) from all P D
patients cornparedto control sub-jects (P D: n = 16, 0.45 ? 0.03
+mol/gm wet weight;
control: n = 1 3 , 0.75 0.46; p < 0.01). This appliedto both
the SN pars compacta and to the totalSN (Fig3 A ) . G S H levels in
the cerebral cortex and putamenwere somewhat decreased com pared to
contro l values,but these changes did not reach statistical
significance.No alterations in G S H occu rred with o ther brain
areasstudied.
In contrast, GS SG levels (Fig3 B )were not altered inPD
patients compared to control subjects. Th e GS SGcontent in the SN
from all PD patients was insignifi-cantly increased by 27% (PD: n =
13, 0.00310.0004 pmol/gm wet weight; control: n = 12, 0.0024
0.0004, p = 0.17, not significant ENS]).
Ghtathione Letleis i n Multiple-System A trophyThe G SH con tent
of the lateral globus pallidus fromMSA patients was approximately
double(1969%) thatfound in control subjec ts (Fig4A). There was a
corre-sponding reduction (60 ) of the GSSG content in thelateral
glo bus pallidus inMSA patients (Fig4B ) .Therewere no significant
changesi n G S H or GSS G levels in
other brain areas examined.
Glutathione Leilels i n Progressive Supranuclear PalsyG S H
levels in PSP patients were reduce d in the cau-date nucleus ( 5 1
% ) (Fig 5A). There were no alter-ations in G S H content in the
cerebral cortex, putamen,or SN. GSSG content in PSP patients was
not alteredin any of the brain areas examined (Fig5B) . (Th ere
wasnot sufficient nigral tissue to measure GSSG levels.)
Glutathione Le?JeIs n Hun tingto n? DiseaseT he G S H conten t
in cerebral cortex, caudate nucleus,
and SN zona compacta from HD patients was not al-tered compared
to control values (Fig6A). Th ere wasa marked reduction in the GSS
G( 5 0 % )content in thecaudate nucleus fromHD patients comparedto
control
Fig 2 . Linear regression analysis fo r A) educed glutathione( G
S H ) leziels(pmollgm u'et weight)u i t h postmortem delay(time
between death and remcajalof brain) and (Bi oxidized glu-tathione
GSSG) hels (pmollgtn urt weight) with postmortemde ay (hours) iti
the total substantia nigra and putamen fromcontrol subjects. There
was no correlation between glutathionefezels and poslmortem delay
(regression coPfficient< 0.01n = 13-20).
Uh\ha c g , ~\ < , ~ ? , . , l u > r = c ,11211
4 l'
-
8/18/2019 Sian 1994
5/8
k - 1 44erebral cortex -
Putamen IT)
Globus pallidus IL)
-_ _ IGlobus pallidus (MI
I r I0.0 0 2 0.4 0 6 0 8 1.0 1 1 1.4
GSH pmalr./p we1 weigh1 human braln
Cerebral cortex
Caudate nucleus
Putamen 1.1
------I
-lobus pallidus (L)
Globus pallidus IM)
+-I4+ubstantia nigra IT)
I
0.WO 0 002 0.004 a.m 0.008
GSSC prnalesip n e t weight human brain
Fig 3 . Lecels of ( top) reduced ,&tathione (GSH) (pmo llgm
wetweight, and (bottom) oxidized glutathione (GSSG) (pmollgrnwet
weight) i n Parkinson's disease(hatched bars)and age-matched
control (open bars)human autopsy brains. Values arerepresented as
mean standa rd error of mean. Asterisk indi-cates p < 0.01
compared with controls, Student's t test. Numberof saniph is shown
it2 each bar. T = total; L = lateral; M =medial: C = zana
cornpacta.
subjects (Fig 6B). (There was not sufficient tissue tomeasure
nigral GSSG levels.)
GSHIGSSGRatio in Szrbstantia Nigra i nParkinson's Disease and
Multiple-System AtrophyThe nigral GSH IGS SG rat io tendedto be
decreasedin both PD and MSA patients compared to controlsubjects
(Fig 7). Th e reduct ion of the GSH IGS SG ra-tio in P D patients
reached statistical significance p <0.05); that in MSA patients
only just failed to meetstatistical significance( p = 0.051). No
ratios could becalculated for PSP orHD patients since nigral
GSSGlevels could not be measured d ueto the limited
sampleavailable.
DiscussionMethodological h u e sWith the glutathione analysis
method of Slivka andcolleagues [ 151,a high G SH IG SS G ratio was
observedin the brains of all control subjects. This indicates
that
little autolytic loss of glutathione had taken place as aresult
of post mo rtem delay. Inde ed, in this study ther ewas no
correlation betw een glutathio ne levels and post-morte m delay in
control subjects. Th e great er part(>98 ) of total glutathione
was in the reduced form(GS H) , which is consistent with the normal
oxidativestate of the brain [12). Th e levels of G S H and GSS
G
found were in accordance with those previously re-ported [ 151.
The much higher levels of GSSG previ-ously repo rted by Perry and
coauthors[ 141 must havebeen due to postmo rtem delayor
methodological arti-facts. In the PSP group studied here, there was
a sig-nificant difference in age between disease brains andcontrol
brains. However, there was no correlation be-tween GSH or GSSG
levels and age in any groupstudied.
Alterations in Glutathione in the Substantia NigraT he pre sent
data indicate a selective reduc tionof G S H
in the SN of PD brains that occurs without a corre-
F i g 4. Lmels o ( t op ) reduced glu tathione (GSH) pmollgrn
wetweight) and (bottom) oxidized glutathione(GSSG) pmol lgmwet
weigh t) in multiple-system atrophy(hatched bars)and age-matched
control (open bars)human autopsy brains. Values arerepresented as
mean standard error of mean. Asterisk indicates p < 0.05
compared wi th controls. Stu de nti t test. The dzj-fereni-e or GSH
in the sub3,tantia nigra compared t o controlswas not significant (
p > 0.1 . Number of samples is shown ineach bar. L = lateral; M
= medial; T = total.
---II
Cerebral cortex
Globus pallidus M)
Globus pallidus 1,)E ---IFubstantia nigra
0.0 U.5 1.0 I s 2.0
csi i r rnocn/g wet urighl hunlan brain
Cerebral c o r t e x
3 4
__1utamen L )
Globus pallidus (M)
Globus pallidus IL)
Substantia nigra
352 Annals of Neurology Vol 36 N o 3 September 1994
-
8/18/2019 Sian 1994
6/8
I
--ICaudate nucleus
Putamen (T)
I C I ASubstantia nigra c )
0.0 0 5 1.0 1.1 2 0
CSH pmdru g wet w r i g h l human brain
~ .A
ICerebral cortex
Caudate nucleus
Putamen TI
Substant ia n i p C) N
0.WO 0.001 0 002 0.003 0.W4 0.001 0 006
CSSC pmolcsig wet weight human brain
B
F i g 5 Levels of (A) reduced glutathione ( G S H ) (ynioflgm
wetweighti and ( B )oxidized glutathione(GSSG)(ymollg m wetweighti
in progressive supranuclear palsy (stippled bars) andage-matched
control (op en bars) human autopsy brains. Valuesare represented as
mean tandard error of mean. Asterisk in-
dicates p < 0.05 compared w ith controls. Student\ t test.
ThediHerenc-e or GSH in substantia nigra compared t o controls
wasnot significant (p > 0.31. Number of samples is shown in
eachbar. T = total: C = compacta: N D = not determined.
Cerebral cortex
I C I L
Substantia nigra
Caudate nuclems
Substantia nigra - NI r [email protected] @.Wl 0.wz 0 m 0.wJ 0.w.F l l . I y
I
CSSD p m d c d g WCI weigh1 h u m a n brain
B
F i g 6 . Latiels of Ai reduced glutathione ( G S H ) ymol lgm
wetuiezght) an d IBi oxidized glutathione GSSG) ymollgmwetweight)
in Huntington's disease(stippled bars)and age-matched control (open
bars) human autopsy brains. AsteriskindicateJ p < 0.05 compared
with controls. Student's t test.Number of samples is shown iii each
bar. N D = not deter-mined; C = zona compacta.
sponding significant increase in GSSG content. Therewere no
other changes in glutathione content inPDbrains. However, the ratio
GSH/GSSG in theSN ofP D brains was altered in favor of the oxidized
formand in a manner consistent with the involvement ofoxidative
stress in nigral cell loss in PD. Th e present
findings are in agreement with a recent report fromRiederer and
colleagues which also showed a similardecrease of total glutathione
2 a nd G S H 1181 levelsin SN in PD.
T he m arked nigral depletion of GS H appearsto beselective to
PD , since it was not observed in the SNOf MSA7 psp' Or HD although
there was a
Fig 7 . Reduced-oxidized glutathione(GSHIGSSG)ratio i n
thesubstantia nigra o f Parkinson's disease (PD, n = 16) and
mul-
trend toward a reduction in and psp brains' Thisin GSH levels in
PD are
not a general consequenceof neurodegeneration what-
tiple-jystmi atrophy(MSA,compared t o age-matched contra( n =
10-13, open bars) hu-man autopsy brains. Values are represented as
mean
= 4 )patients (hatched bars)that the
Stan-ever the Cause, but are ~ ~ c hore evident in
thepathological process underlying PD. There are equiva-
lent degrees of cell loss, around 70%, in the lateral
dard error of mean. Asterisk indicates p < 0.05 for PD
com-pared wi th controls, Student? t test cfor M S Acompared to
controls. p = 0.051).
Sian et al: Glutathione Levels in P D and Oth er Ne urodegene
rative Disorders 353
-
8/18/2019 Sian 1994
7/8
ventral tier of the zona compacta of theSN in PD,MSA, and PSP
1191. Sup port for this conclusion come sfrom HD studies, where not
only were nigral levels ofG S H unchanged but also there were n o
alterations inGSH levels in the caudate nucleus despite the
markedpathology found in this brain area[201. T he change inG SH in
the SN in PD was unlikely to have been due
to L-dopa treatment. Patients with M SA also were tak-ing this
drug in larger doses on average, yet there wasa smaller and
insignificant fall in G S H c onte nt inMSAbrains. How ever, th ere
was a fall in the ratio of G S Hto GS SG both in P D and MSA brains
(although thatin MS A brains just failed to m ee t significance);
this iscompatible with oxidative stress in both conditions,sowe
cannot rule ou t a contribution from L-dopa therapy.
Alteratiom in Gbt athio ne in Other Brain RegionsThe re were som
e interesting changes in G S H andGSSG content in other areas in
MSA, PSP, andHD
brains, but these are difficult to interpret. The mostdramatic
occurred in the lateral globus pallidus in MSAbrains whe re the re
was an elevation of G S H levelscoupled to a reduction of GSSG
content. This areaof the globus pallidus is specifically affected
inMSA,showing a marked loss of myelinated fibers and gliosis[21].
This finding appears to signify an altered redoxstate that serves
to maintain glutathione in its reducedform 1121. Why this should
occur is not clear.
There was a reduction in GSH levels in the caudatenucleus in PSP
brains but no equivalent change inGSSG in this area. This changeis
similar to that ob-
served in the SN in P D brains, and may reflect thepresence of
oxidative stress. How ever , the striatum inPSP brains exhibits
only mild pathological changesC20). In HD brains there was a
reduction in GSSG inthe caudate nucleus bu t no change in G S H in
this area.T he reduction of GSSG in HD again is unexplained,but may
be secondary to the macroscopic atrophy andloss of the GABAergic
medium-sized spiny neuronsm.Possible Causes of Nigral Glutathione
Defcieniyin Parkinson? Disease
The decrease of GSH in PD might be the result ofdefective
synthesis, excessive metabolism, or abnormalutilization. Activity
of the rate-limiting synthetic en-zyme y-glutamylcysteine
synthetase in theSN in PDremains to be determin ed, as does the
enzyme mainlyresponsible for the translocation and breakdown ofboth
GSH and GSSG, namely y-glutamyltranspepti-dase. Th e abilityto form
mercapturate conjugates fromglutathion e appears unchanged since
glutathione trans-ferase activity in the SN in P D reportedly is
normal
Given the current concept of oxidative stress as a
contributory factor to nigral cell death in PD, changes
~ 2 2 3 .
in GS H utilization throug h its oxidative-reductivepathway
might be relevant. However, there seems tobe no overall change in
tissue levels of glutathioneperoxidase activity in the SN in PD
[9]. Recently,however, a m arked elevation was found in
glutathioneperoxidase-containing glial cells in theSN from
par-kinsonian patients 1231. Under conditions of intense
oxidative stress, utilizationof GSH via glutathion e per-oxidase
leads to an irreversible loss of intracellularG S H [24 ] . Despite
the decreased GSH/GSSG ratioin the SN in PD, there was no absolute
increase inGSSG levels that might argue against the decrease inG S
H arising from oxidative stress. However, GS SG istransported from
cells under conditions of oxidativestress as protection against its
cytotoxic effects[25}.
T h e precise localization of altered G S H levels in theSN in P
D is not known. Since neurons only constituteapproximately 1% of
the total number of nigral cells,it is likely that the mark ed
nigral G S H depletion found
in PD occurs in nonneuronal populations such as glia.Inde ed,
histochemical studies have shown that G S H islocalized m ainly in
glial cells and t he neuropil{26-28).This raises fundamental
questions of the role playedby glial cells in the neuronal
degeneration inSN thatcharacterizes PD.
Relationship Between Depletionof GSH avzd OtherIndices of
Oxidutike Stress i n the Slrbstantia Nigr aThe deple tion of GS H
in theSN in P D adds to thegrowing list of biochemical changes
(increased lipidperoxidation, raised iron levels, inhibited
complexI
activity) that suggest oxidative stressas a componentof the
degene rative process[29]. Recently, we investi-gated t he same
biochemical param eters in subjects withincidental Lewy body
disease (pres ymp tomatic PD )1301. In the SN from these subjects,
there was noalteration in iron levels and no significant decrease
incomplex I activity but the levels of G S H w ere de-creased to
the same extent as in advanced PD [31].This suggests that the
reduction of GSH is the earliestindex of oxidative stressso far
uncovered and that onlysubsequently do alterations in iron m
etabolism a ndmi-tochondrial function become apparent.
Interestingly,
depletion of G S H in brain using an inhibitor
ofy-glutamylcysteine synthetase, namely buthionine sulfox-imine,
can itself lead to mitochondrial damage [ 12).
There may, however, be the opposite connectionberween the
depletion of GSH in the SN in P D andinhibition of complexI
activity. Thus, hepatocytes ex-posed to 1-methyl-4-phenylpyridinium
ion (MPP+and other mitochondrial toxins show a decrease inG S H
content with no corresponding rise in GS SG lev-els, resulting in a
fall in the GSHIGSSG ratio[32].This effect was attributed to a
combination of de-creased cellular metabolism and an efflux of GS H
from
the cells. So, even in incidental Lewy body disease
354 Annals of Neurology Vol 36 No 3 September 1994
-
8/18/2019 Sian 1994
8/8
there may be alterations in mitochondrial function thatremain to
be detected but that leadto GSH depletion.
This study was supported by the Medical Research Council and
theParkinson’s Disease Society and IN SERM .
References1. D exter D T, Carayon A, Javoy-Agid F, etal.
Alterations in the
levels of iron, ferritin and other trace metals in Parkinson’s
dis-ease and other neurodegenerative diseases affecting the
basalganglia. Brain 1991;114:1953-1975
2. Riederer P, Sofic E, Rausch W-D , et al. Transition m etals,
ferri-tin, glutathione and ascorbic acid in parkinsonian brains.J
Neu-rochem 1989;52:515-520
3. Dexter DT , Carayon A, Vidaillhet M, etal. Decreased
ferritinlevels in brain in Parkinson’s disease. J Ne uroc
hem1990;55:16-20
4. Dexter D T, Carter CJ, WellsFR, et al. Basal lipid
peroxidationin subsrantia nigra is increased in Parkinson’s
disease.J Neuro-
chem 1989;52:381-3895. Dexter DT. Holley AE, Flitter WE, etal.
lncreased levels of
lipid hyd roperoxides, bu t no evidence for increased free
radicalformation, in the parkinsonian substantia nigra. Mov
Disord1994;9:92-97
6. Schapira AHV , Cooper JM, DexterDT, e t al.
Mitochondrialcomplex I deficiency in Park inson’s disease.J
Neurochem 1990;54 323-82 7
7. Kish SJ, Moriro C, Hornykiewicz 0 Glutathione
peroxidaseactivity in Parkinson’s disease brain. Neurosci
Lett1985;58:
8. Ambani IM, Van Woert M H, Murphy S. Brain peroxidase
andcatalase in Parkinson’s disease. Arch N eur ol 1975;3 2: 114-1 1
8
9. Marttila RJ, Lorentz H, Rinne UK. Oxygen toxicity
protect-
ing enzym es in Parkinson ’s disease: increase of
superoxidedismutase-like activity in the substantia nigra and basal
nucleus.J Neurol Sci 1988;86:321-331
10. Saggu H, CookseyJ Dexte r DT, e t al. A selective increase
inparticulate superoxide dismutase activity in parkinsonian
sub-stanria nigra.J Neurochem 1989;53:692-697
11. Dexter D T, Ward RJ, Wells FR, et al. a-Tocopherol levels
inbrain are not altered in Parkinson’s disease. A nn Ne urol
1992;32:591-593
12. Meister A, Anderson ME. Glutathione. Annu Rev
Biochem1983;52:711-760
13. MarrenssonJ, ames EKL, Meister A. H igh affinity transport
ofglutathione is a part of a multicom partment system essential
formitochondrial function. Proc Natl Acad Sci USA 1990;87:7185-7
189
14. Perry TL, Godin DV , Han sen S. Parkinson’s disease: a
disorder
343-346
due to nigral glutathione deficiency Neurosci Lett 1 982;33:
15. Slivka A, Spina MB , Coh en G . Reduced and oxidised
glutarhi-one in human and monkey brain. Neurosci Lett
1987;74:112-118
16. Tietze F. Enzymatic method for quantitative determination
ofnanogram amountsof total and oxidised glutathione. A nal Bio-chem
1969;27:502-522
17. Reed DJ, Babson JR, Beatty PW, etal. High performance
liquidchromatography analysis of nanom ole levels of glutathione ,
glu-tarhione disulphide and related thiols and disulphides. Anal
Bio-chem 1980;106:55-62
18. Sofic E, Lange KW, Jellinger K, et al. Reduced and
oxidisedglutathione in the substantia nigra of patients with
Parkinson’sdisease. Neurosci Lett 1992;142:128-130
19. Fearnley JM , Lees AJ. Ageing and Parkinson’s disease:
subsran-ria nigra regional selectivity. Brain
1991;119:2283-2301
20. Gib b WR G. N europathology of th e subsrantia nigra. Eu rJ
N eu-rol 1991;3 (suppl):48-59
2 1. Fearnley JM , Lees AJ. Striatonigral degeneration. B
rain1990;
22. Perry TL, Yong VW. Idiopath ic Parkinson’s disease,
progressiv esupranuclear palsy and glutathione m etabolism in the
substantia
nigra of patients. Neurosci Lett 1986;67:269-27423. Dauvier P,
Hirsch EC, Zhang P, etal. Glutathione peroxidase,
glial cells and P arkinson’s disease. Neuroscie nce
1093;52:1-624. UhligS, Wendel A. The physiological co nsequences of
glutathi-
one variations. Life Sci 1992;5: 1083-109425. Griffiths O W ,
Meister A. Origin and turnover of mitochondrial
glutathione. Proc Natl Acad Sci USA 1985;82:4668-467226.
Abramovitz M, H om ma H , IshigakiS, e t al. Characterization
and localization of glutathione-S -rransferase in rat brain
andbinding of hormones, neurotransmitters and drugs.J Neuro-chem
1988;50:50-57
27. Slivka A, Mytilineou C, Coh enG . Hiscochemical
evaluationofglutathione in brain. BrainRes 1987;409:275-284
28. Philbert MA, Beiswanger CM, Waters DK, etal. Cellular
and
regional distribution of reduced glutathione in the nervous
sys-tem of the rat: histochemical localisation by mercury orange
andophthaldialdehyde-induced histo-fluorescence. Toxicol
ApplPharmacol 1991;107:2 13-227
29. Jenn er P, Dexter D T, SianJ, et al. Oxidative stress as a
causeof nigral cell death in Parkinson’s disease and incidental
Lewybody disease. Ann Neurol 1992;35:S82-S87
30. Gi bb W RG , Lees AJ. The relevance of Lcwy bodyto the
parho-genesis of idiopathic Parkinson’s disease. J Neu rol N
eurosurgPsychiatry 1988;5 1:745-752
31, Dexter DT, Sian J, Rose S, et al. lndices of oxidative
stressin individuals with incident al Lewy body disease. Ann N eu
rol
32. Mithofer K, Sandy MS, Smith M T, et al. Mitochondrial
poisonscause de pletion of reduc ed glutathione in isolated
hepatocyres.Arch Biochem Biophys 1992;295:132-136
305-310
113: 1823- 1842
1994;35~38-44
S i a n e t al: G l u t a t h i o n e Levels i n PD a n d O t h
e r N e u r o d e g e n e r a t i v e D i s o r d e r s 355