Embed Size (px)
Citation preview
Skeletal System
Chapter 7
Objectives
1. Iden/fy the different structures and fuc/ons of the Skeletal system.
2. Label a long bone and internal structures of bone.
3. Explain bone development and growth. 4. Apply knowledge of homeosta/c
mechanisms to explain the regula/on of blood calcium levels.

Introduction
• Bones are very ac/ve /ssues • Each bone is made up of several types of /ssues and is an organ
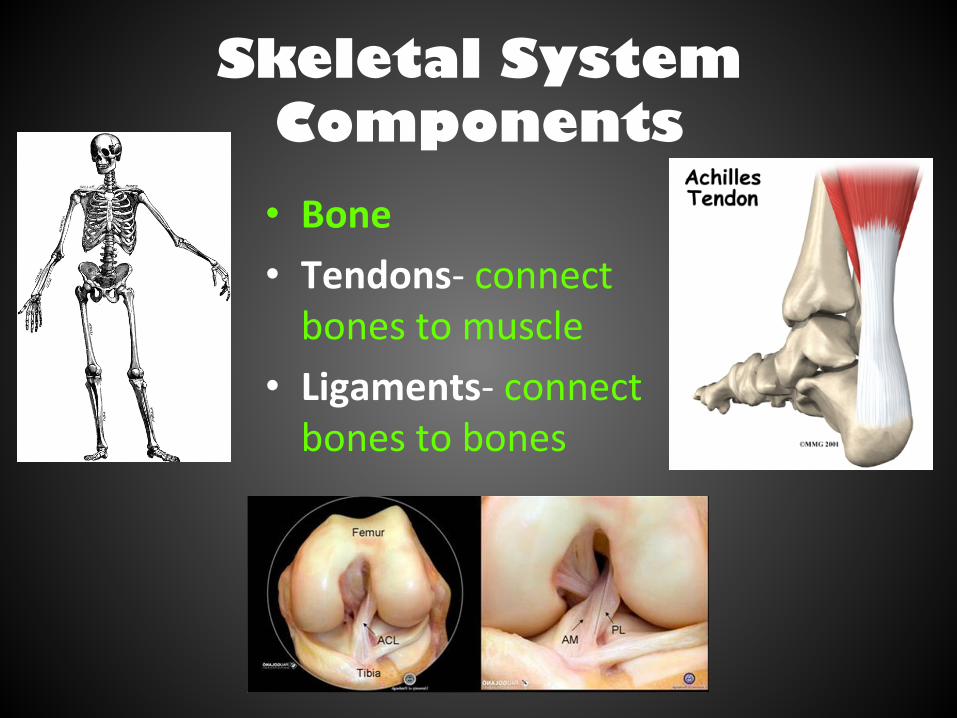
Skeletal System Components • Bone • Tendons-‐ connect bones to muscle
• Ligaments-‐ connect bones to bones

Functions
• Muscle aJachment • Protec/on • Contain blood-‐producing cells
• Storage of inorganic salts • Passageway for nerves & blood vessels
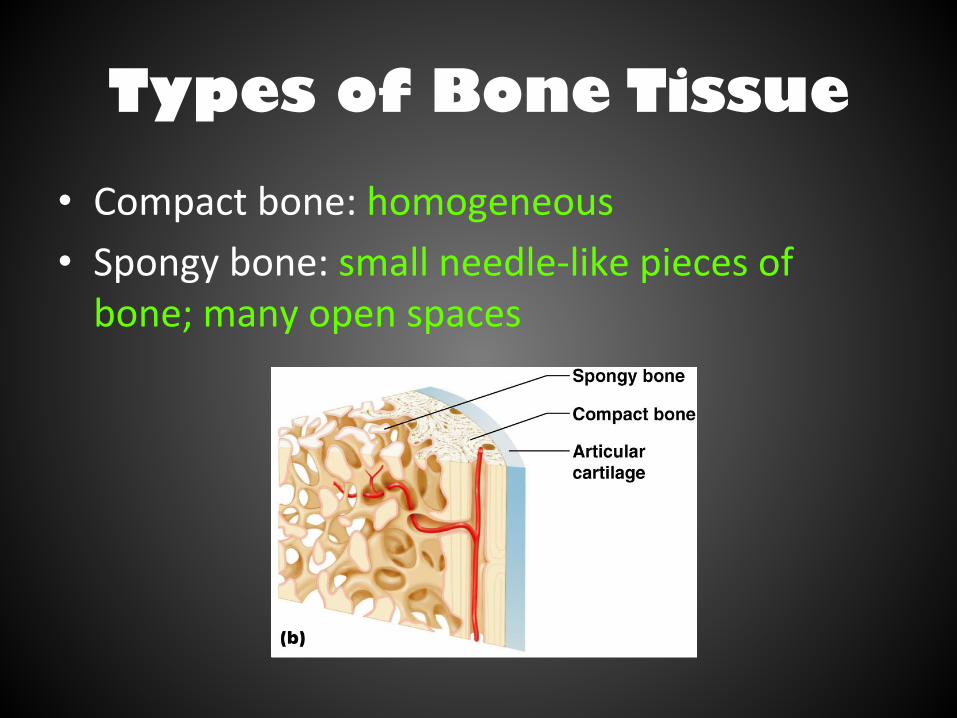
Types of Bone Tissue
• Compact bone: homogeneous • Spongy bone: small needle-‐like pieces of bone; many open spaces
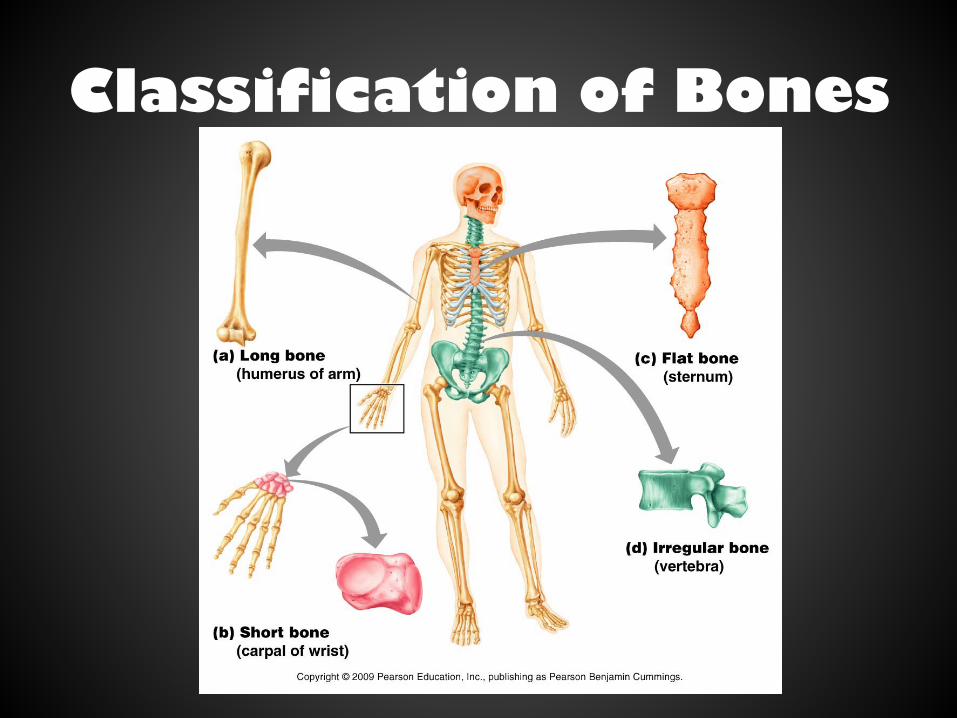
Classification of Bones
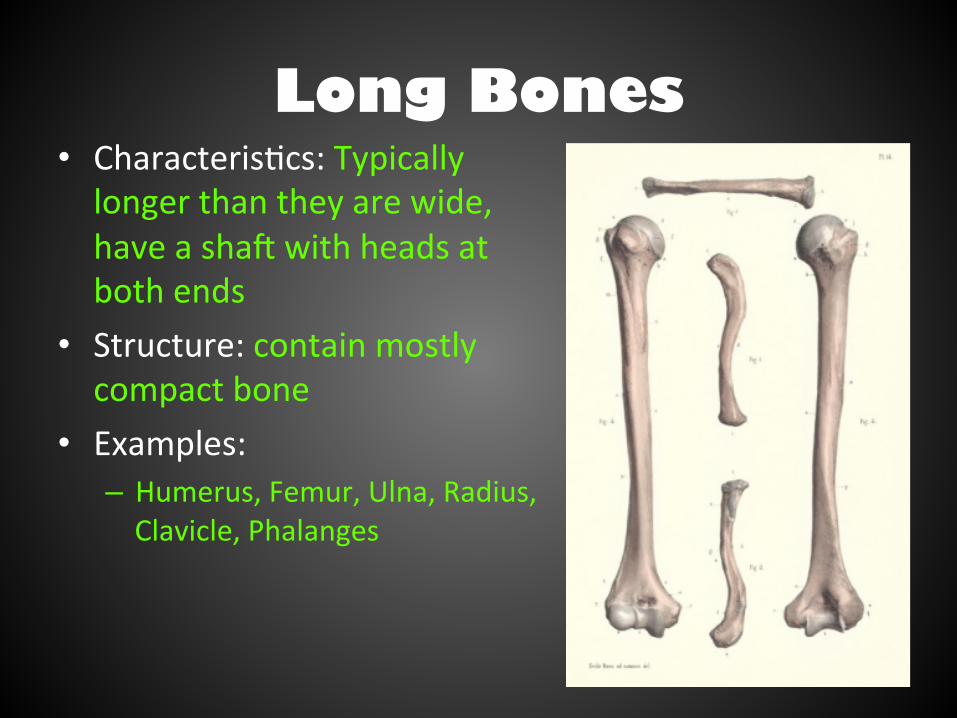
Long Bones • Characteris/cs: Typically longer than they are wide, have a shaQ with heads at both ends
• Structure: contain mostly compact bone
• Examples: – Humerus, Femur, Ulna, Radius, Clavicle, Phalanges
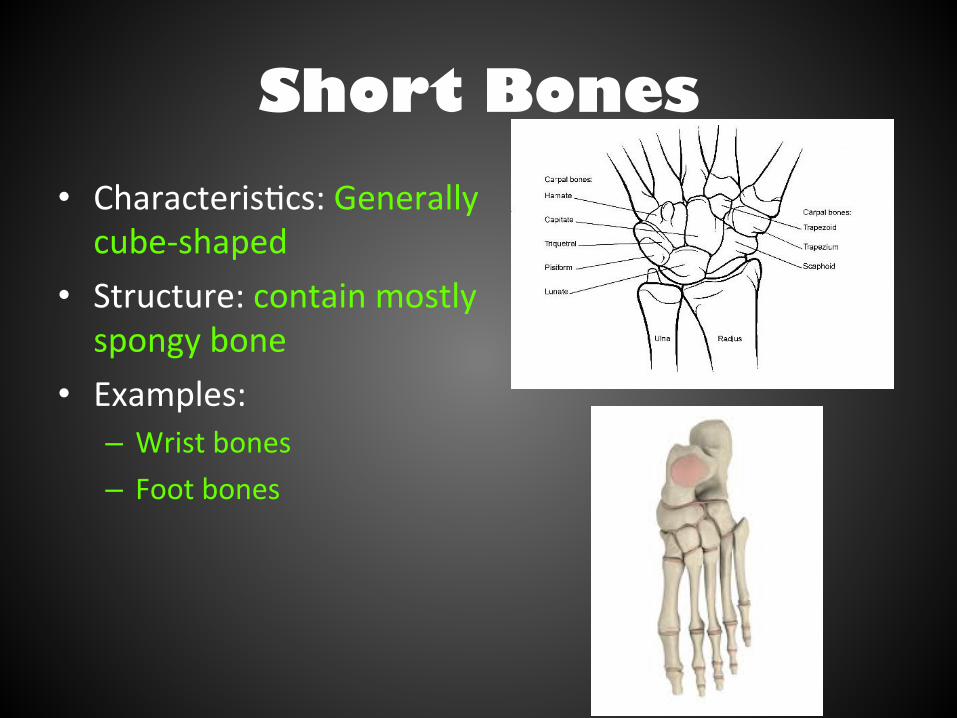
Short Bones • Characteris/cs: Generally cube-‐shaped
• Structure: contain mostly spongy bone
• Examples: – Wrist bones – Foot bones
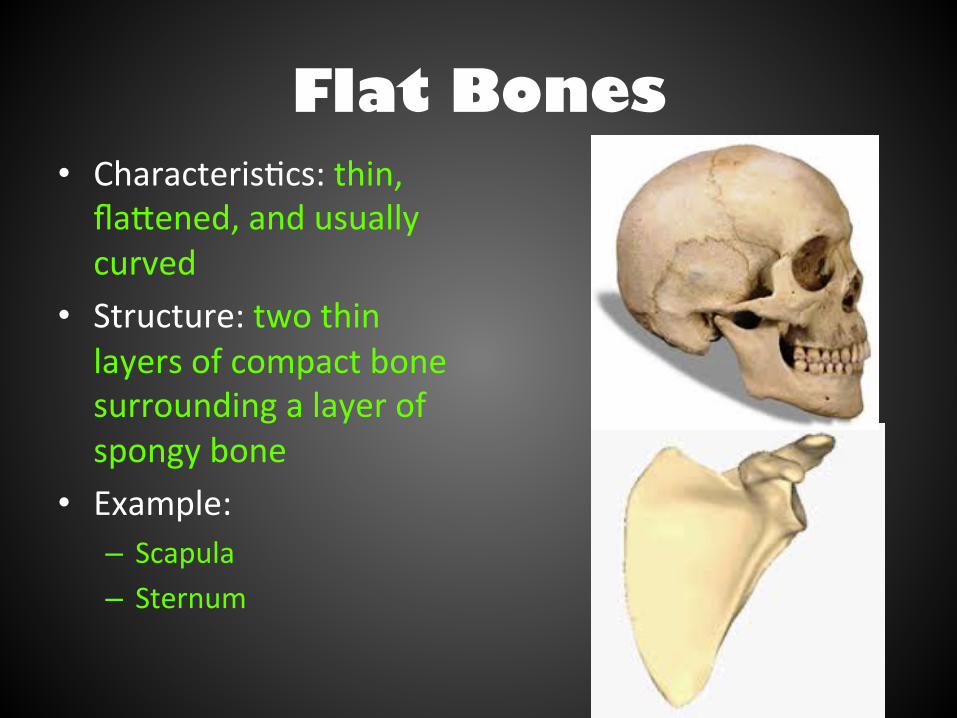
Flat Bones • Characteris/cs: thin, flaJened, and usually curved
• Structure: two thin layers of compact bone surrounding a layer of spongy bone
• Example: – Scapula – Sternum
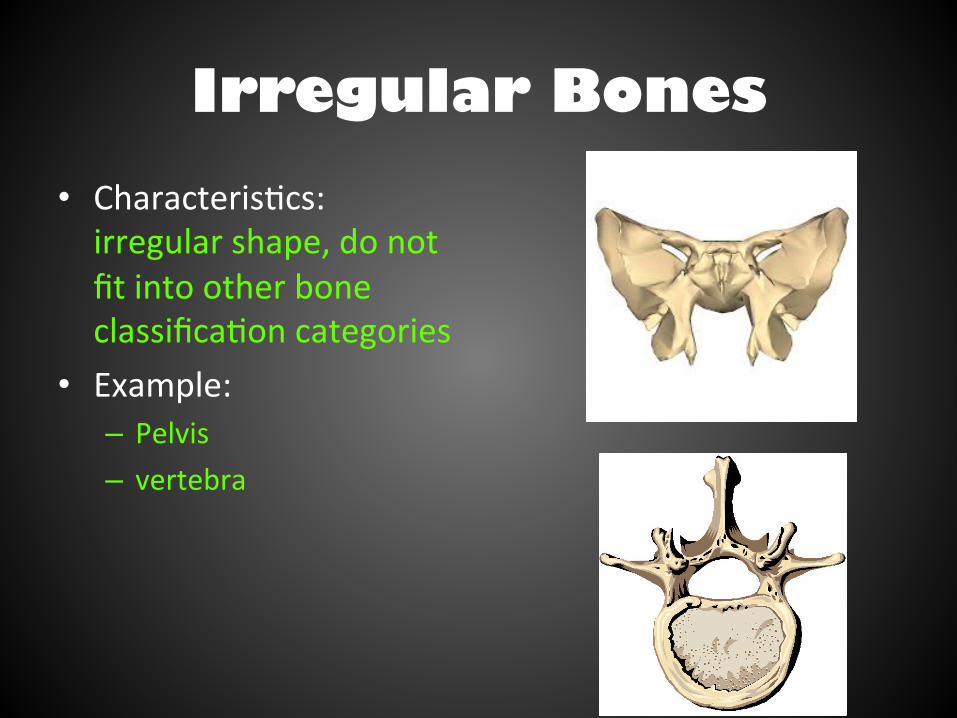
Irregular Bones • Characteris/cs: irregular shape, do not fit into other bone classifica/on categories
• Example: – Pelvis – vertebra
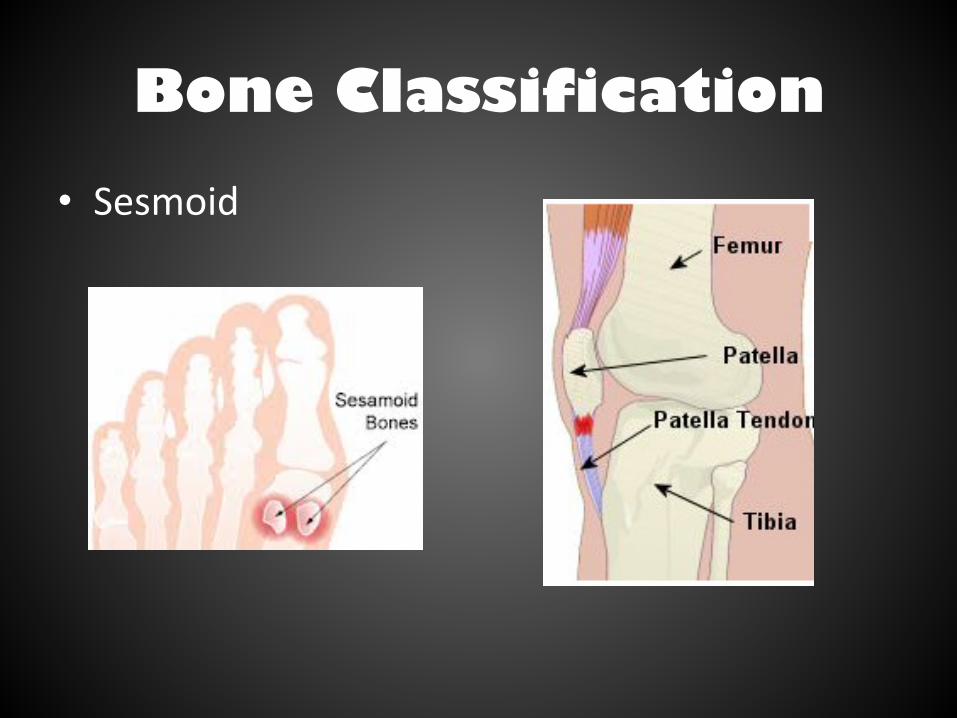
Bone Classification
• Sesmoid
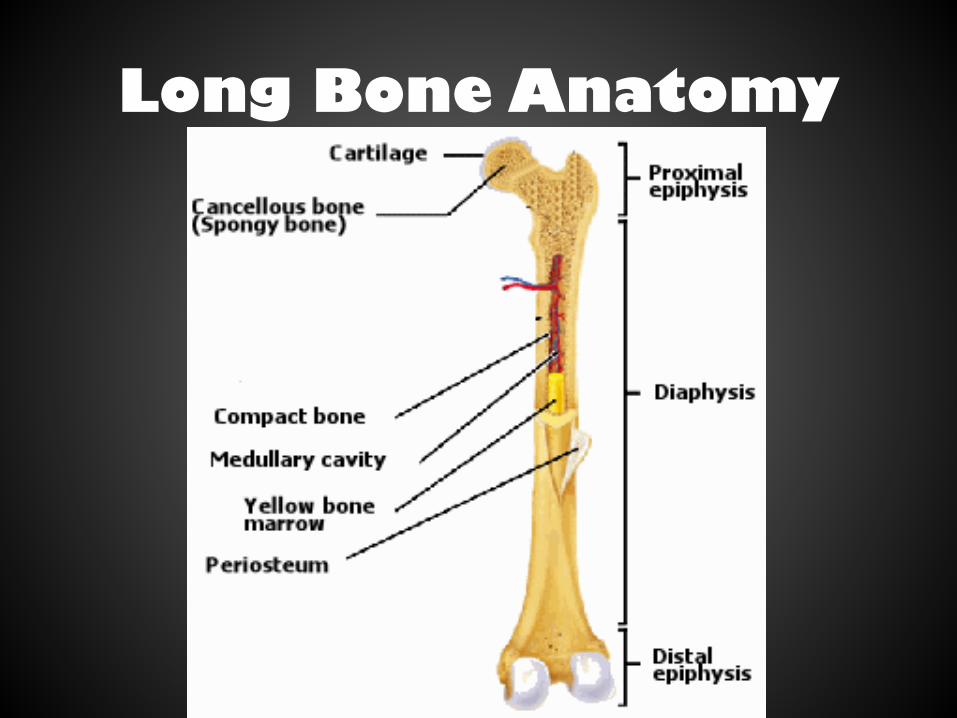
Long Bone Anatomy
Bone Structure • Bones differ in size and shape, yet are similar in several ways
• Parts of a long bone – Epiphysis – expanded ends of bones that form joints with adjacent bones
– Ar/cular car/lage (hyaline car/lage) – covers the epiphysis
– Diaphysis – the shaQ of the bone – Periosteum – a tough layer of vascular connec/ve /ssue that covers the bone and is con/nuous with ligaments and tendons
Parts of a long bone • A bone’s shape makes possible its func/on • Bony processes or grooves indicate places of aJachment for muscles
• Compact bone makes up the wall of the diaphysis
• The epiphyses are filled with spongy bone to reduce the weight of the skeleton
• The diaphysis contains a hollow medullary cavity that is filled with marrow
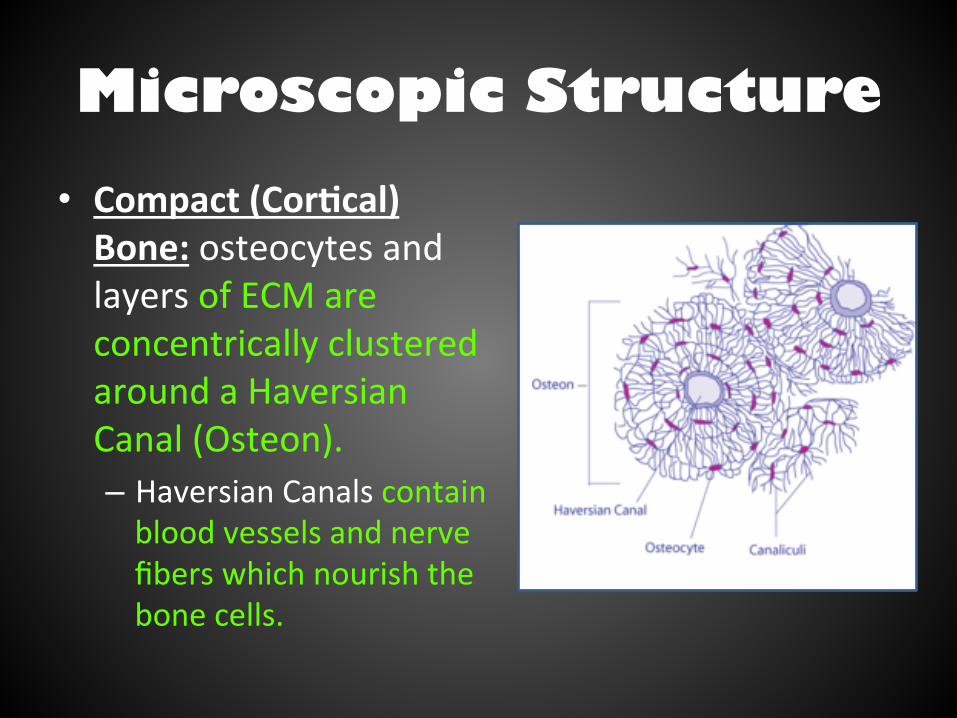
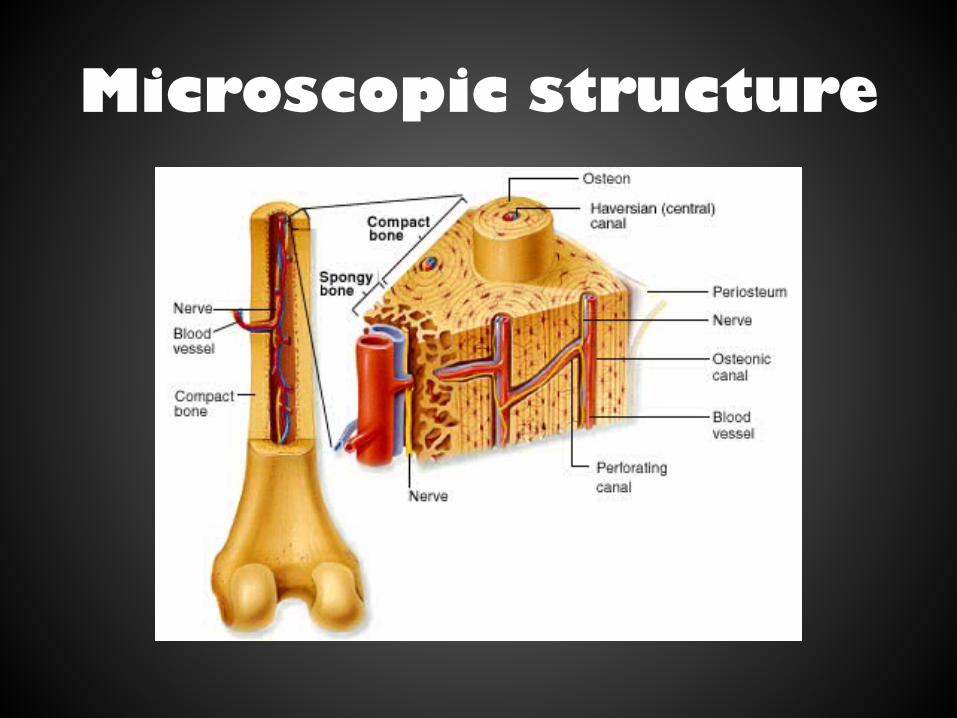
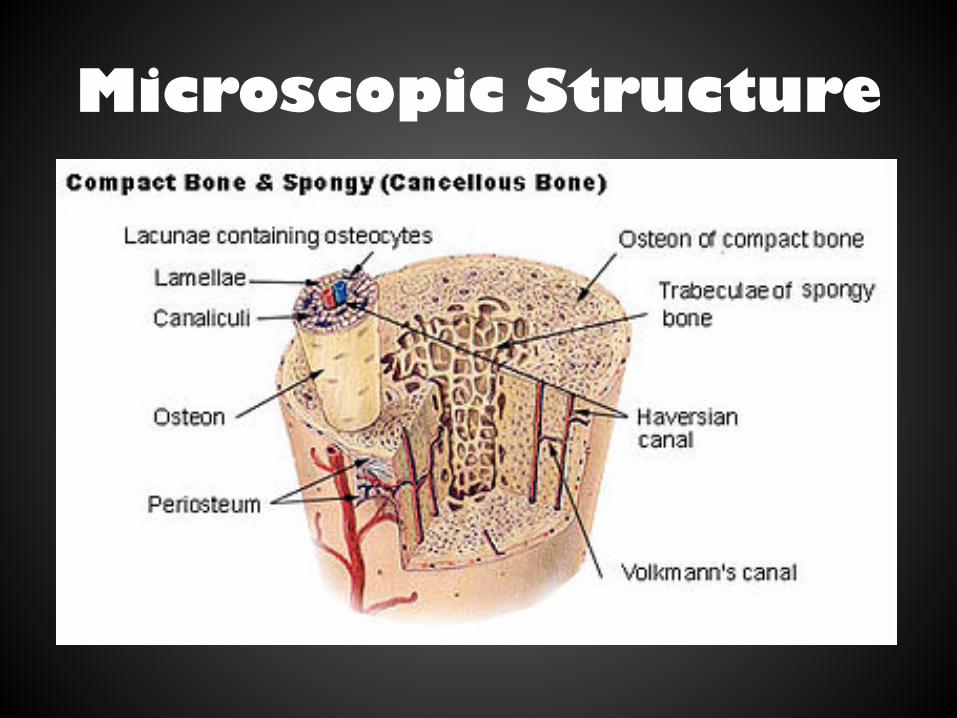
Microscopic Structure • Compact (Cor4cal) Bone: osteocytes and layers of ECM are concentrically clustered around a Haversian Canal (Osteon). – Haversian Canals contain blood vessels and nerve fibers which nourish the bone cells.
Microscopic structure
• Osteocytes – bone cells that are located within lacunae that lie in concentric circles around osteonic canals
• Intercellular material consists of collagen and inorganic salts
• In compact bone, osteocytes and intercellular material are organized into osteons that are cemented together.
Microscopic structure
• Osteonic canals contain blood vessels and nerve fibers and extend longitudinally through bone.
• Osteonic canals are interconnected by transverse perfora/on canals.
• Unlike compact bone, the osteocytes and intercellular material in spongy bone are not arranged around osteonic canals.
Microscopic structure
Microscopic Structure

Bone Growth and Development
• Osteoclasts – break down car/lage and bone • Osteoblasts – bone-‐building cells • Osteocytes – bone cells
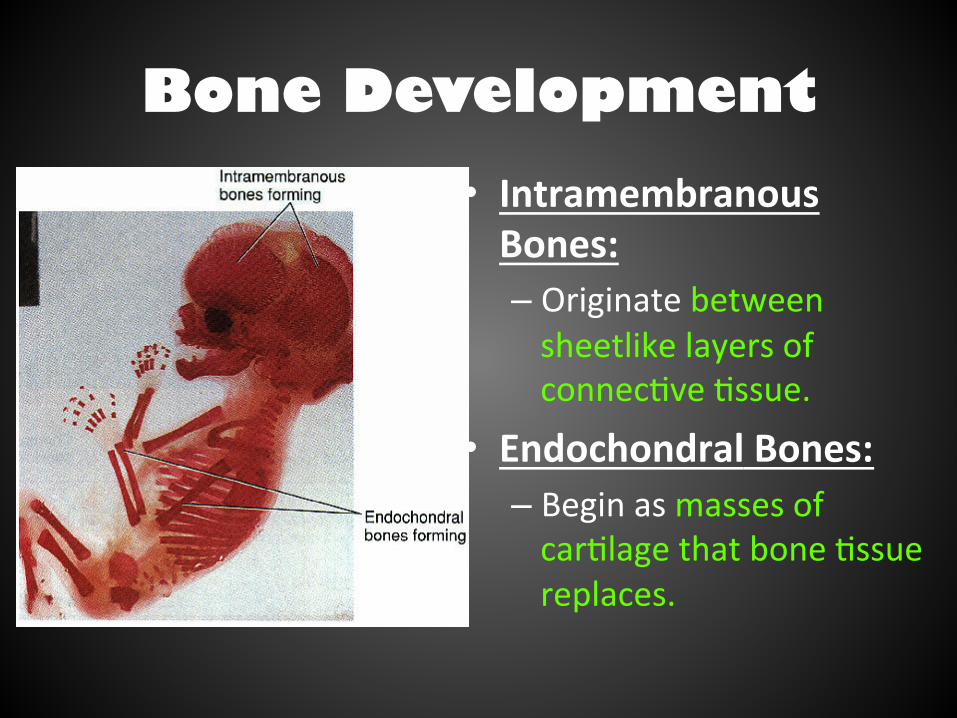
Bone Development • Intramembranous Bones: – Originate between sheetlike layers of connec/ve /ssue.
• Endochondral Bones: – Begin as masses of car/lage that bone /ssue replaces.
Bone Development • Intramembranous Ossifica4on:
1. Connec/ve /ssue appears at the sites of future bones. 2. Connec/ve /ssue cells differen/ate into osteoblasts. 3. Osteoblasts deposit bony material around themselves and form spongy bone. 4. Membranous /ssue cells give rise to the periosteum. 5. Osteoblasts inside the periosteum form compact bone.

Intramembranous Bones
Bone Development • Endochondral Ossifica4on (Condensed Version):
1. Car/lage breaks down in the center of the diaphysis. (primary ossifica/on center)
2. Periosteum forms around the developing dipahysis from connec/ve /ssue.
3. Blood vessels and osteoblasts from periosteum invade the car/lage and form spongy bone.
4. Epiphysis remain car/laginous and later secondary ossifica/on centers appear and form spongy bone.
5. Epiphyseal plate undergoes mitosis and produces new cells which enlarge , while calcium salts accumulate in the extracellular matrix, they calcify, and the car/lage cells die.
6. Osteoclasts secrete acid that dissolves part of the calcified matrix and osteoblasts deposit new bone /ssue in place of the calcified car/lage.
7. Bone con/nues to grow at the epiphyseal plate un/l adulthood.
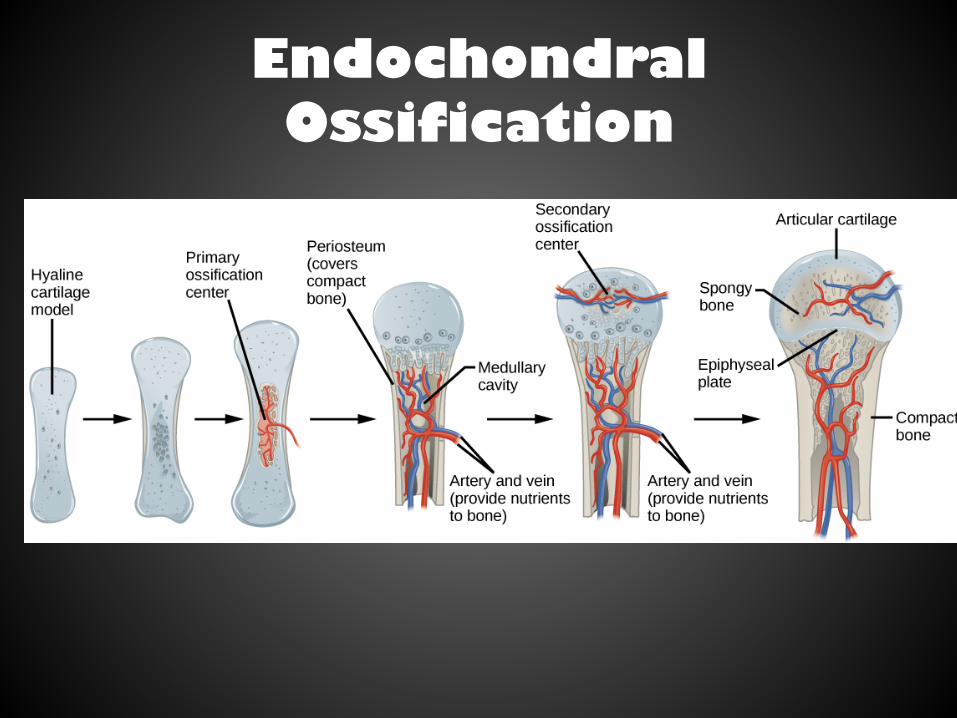
Endochondral Ossification
Objectives
• To explain the different func/ons of bone in detail.
• To apply your knowledge of homeostasis and nega/ve feedback loops to explain hormonal regula/on of bone calcium resorp/on and deposi/on.
Bone Functions
• Support and Protec/on – Bones give shape to the head, thorax, and limbs – The pelvis and lower limbs provide support for the body
– Bones of the skull protect the brain, ears and eyes • Movement – Muscles aJach to bones – Push and pull bones for movement
Bone Functions • Blood cell Forma/on – Two kinds of marrow occupy the medullary cavi/es of bone • Red marrow – forma/on of red blood cells, white blood cells and platelets
• Yellow marrow – stores fat
• Storage of Inorganic Salts – Bone stores inorganic mineral salts in the form of calcium phosphate
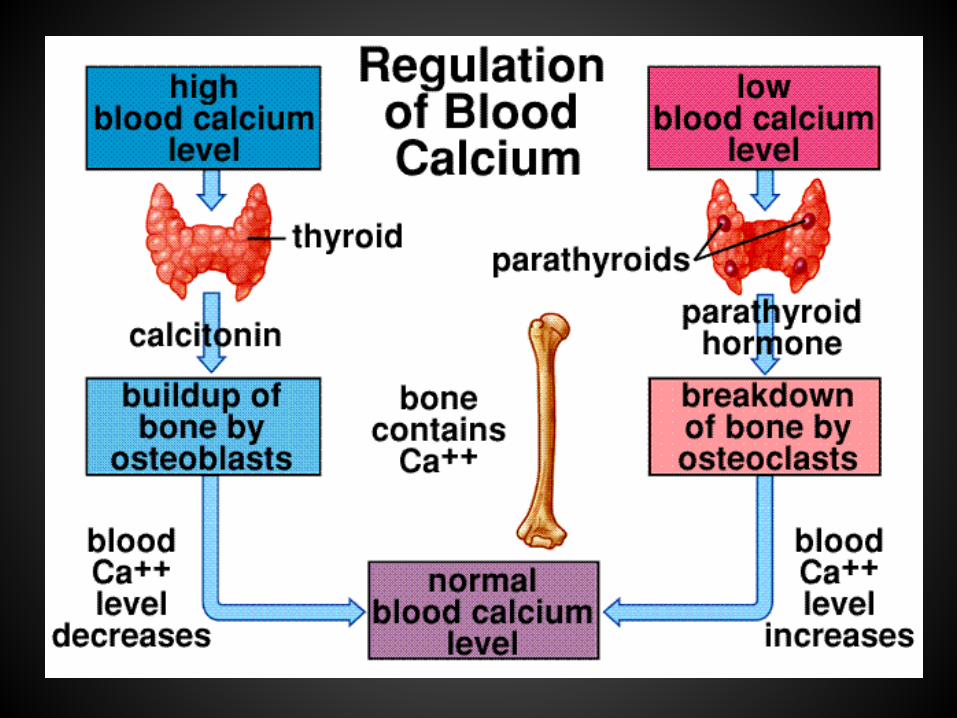
– Calcium in bone is a reservoir for body calcium • When blood levels of calcium are low, osteoclasts release calcium from bone.
• Calcium is stored in bone under the influence of calcitonin when blood levels of calcium are high.
Hematopoiesis • Hematopoeiesis=Red blood cell forma/on • RBC’s form in the liver, spleen, and bone marrow – Red Marrow:
• Found in infants as well as in spongy bone of skull, ribs, sternum, clavicles, vertebrae, and hip bones of adults
• Produces red blood cells (erythrocytes), white blood cells (leukocytes), and platelets.
– Yellow Marrow: • In adults • Stores fat • *doesn’t produce RBC’s
Inorganic Salt Storage
• ECM of bone is rich in calcium • Calcium is required for muscle contrac/on, nerve impulse conduc/on, blood clohng, and other physiological processes.
• Our bodies must maintain a sufficient blood-‐calcium level using a homeosta/c mechanism.
Calcium Regulation

Low calcium levels
• Causes Parathyroid Hormone (PTH) to be released – PTH causes stored calcium in bone to be released – PTH causes calcium reabsorp/on in the kidney (not excreted in urine)
– PTH causes the synthesis of Vit. D. which increases Ca+ absorp/on in the small intes/nes.
High calcium levels
• Causes the release of calcitonin from the thyroid gland – Calcitonin Inhibits Ca2+ absorp/on by the intes/nes
– Inhibits osteoclast ac/vity in bones – Inhibits renal tubular cell reabsorp/on of Ca2+ allowing it to be excreted in the urine
Hypo vs. Hypercalcemia
• Hypocalcemia: can cause muscle s/ffness and seizures
• Hypercalcemia: too much calcium, causes kidney stones or even kidney failure, could cause heart problems

Bone Fractures
• Defini/on: break in a bone • Types of bone fractures – Closed (simple) fracture – break that does not penetrate the skin
– Open (compound) fracture – broken bone penetrates through the skin
• Treatment: reduc/on and immobiliza/on
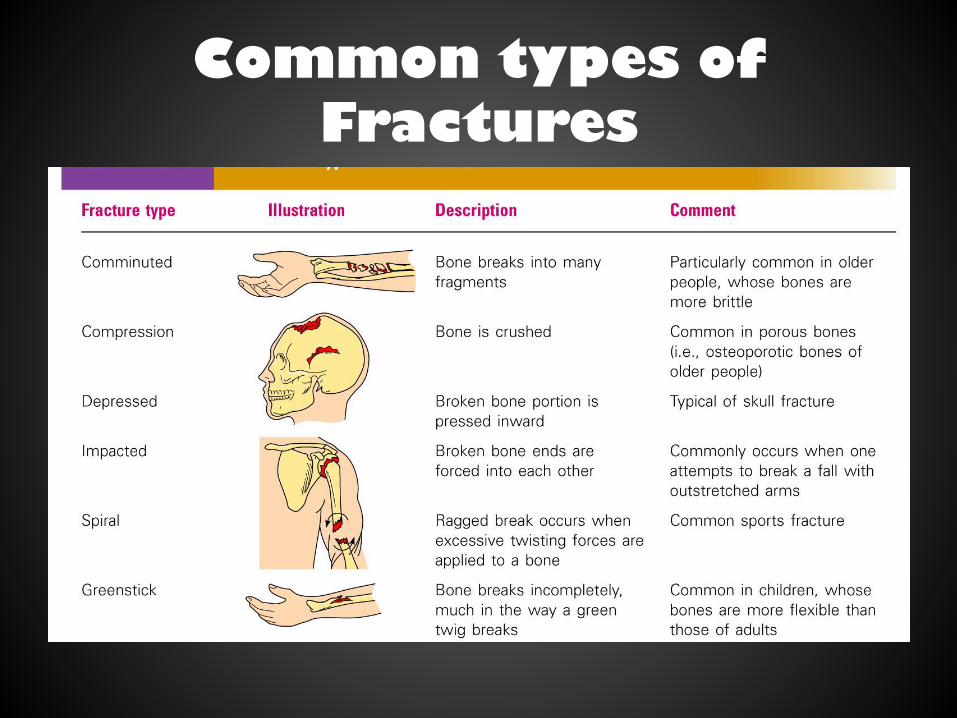
Common types of Fractures
Repair of Bone fractures
• Steps in repair of bone fractures 1. Hematoma: blood-‐filled swelling is formed 2. Fibrocar/lage callus: break is connected by
fibrocar/lage 3. Bony Callus: fibrocar/lage replaced by
spongy bone 4. Bone remodeling: permanent healing
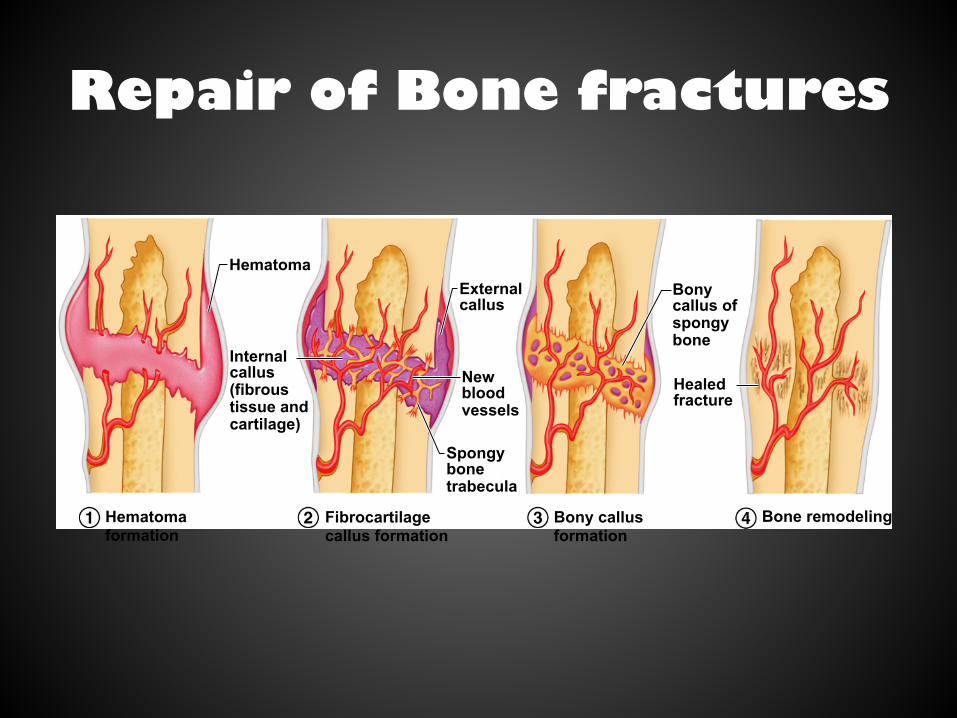
Repair of Bone fractures
Hematoma External callus
Bony callus of spongy bone
Healed fracture
New blood vessels
Internal callus (fibrous tissue and cartilage)
Spongy bone trabecula
Hematoma formation
Fibrocartilage callus formation
Bony callus formation
Bone remodeling
Curve of the Spine
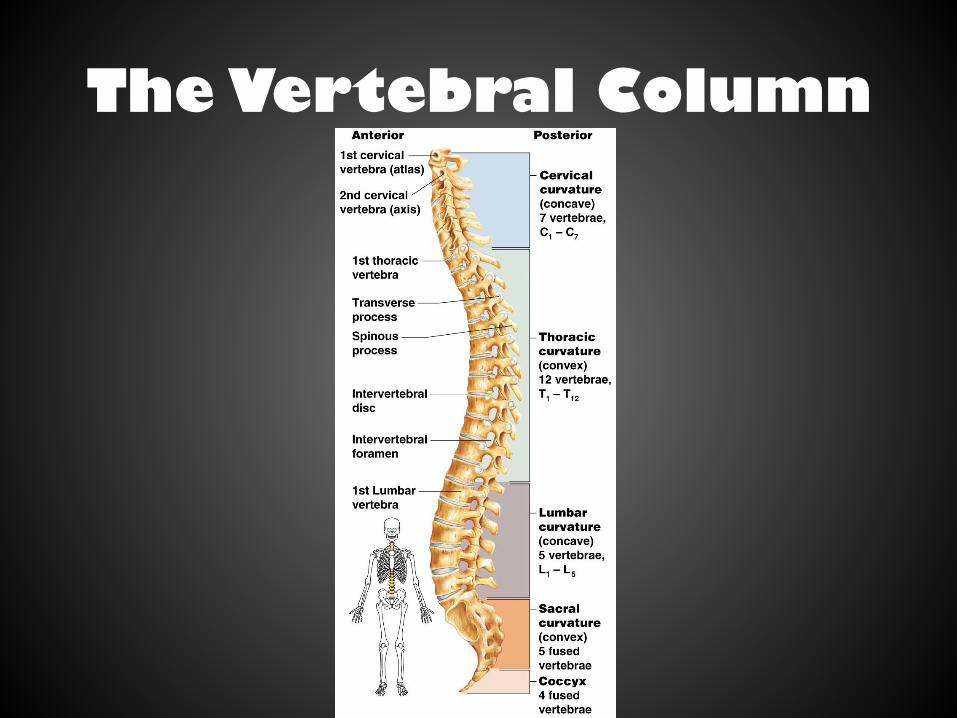
• The spine has a normal curvature • Primary curvatures: curvatures of the thoracic and sacral regions – Present from birth
• Secondary curvatures: spinal curvatures of the cervical and lumbar regions – Develop aQer birth
Skeletal changes throughout life
• Osteoporosis – Bone-‐thinning disease afflic/ng
• 50% of women over age 65 • 20% of men over age 70
– Disease makes bones fragile and bones can easily fracture
– Vertebral collapse results in kyphosis (also known as dowager’s hump)
– Estrogen aids in health and normal density of a female skelton
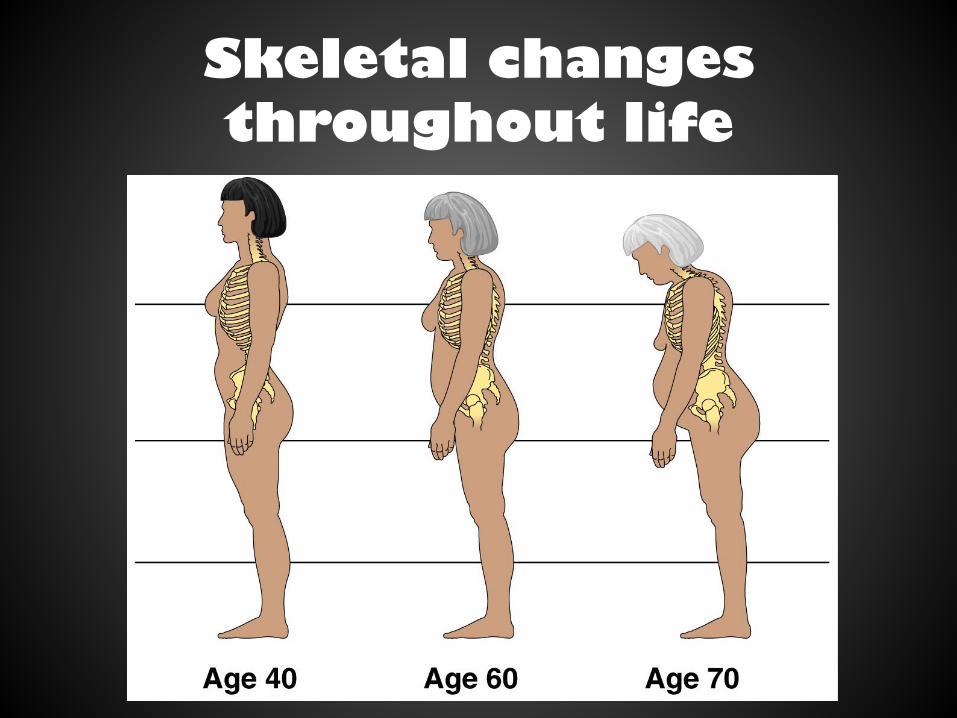
Skeletal changes throughout life

Skeletal changes throughout life
Objectives
• To Iden/fy the major bones of the skull. • To label the major features of the bones of the skull.
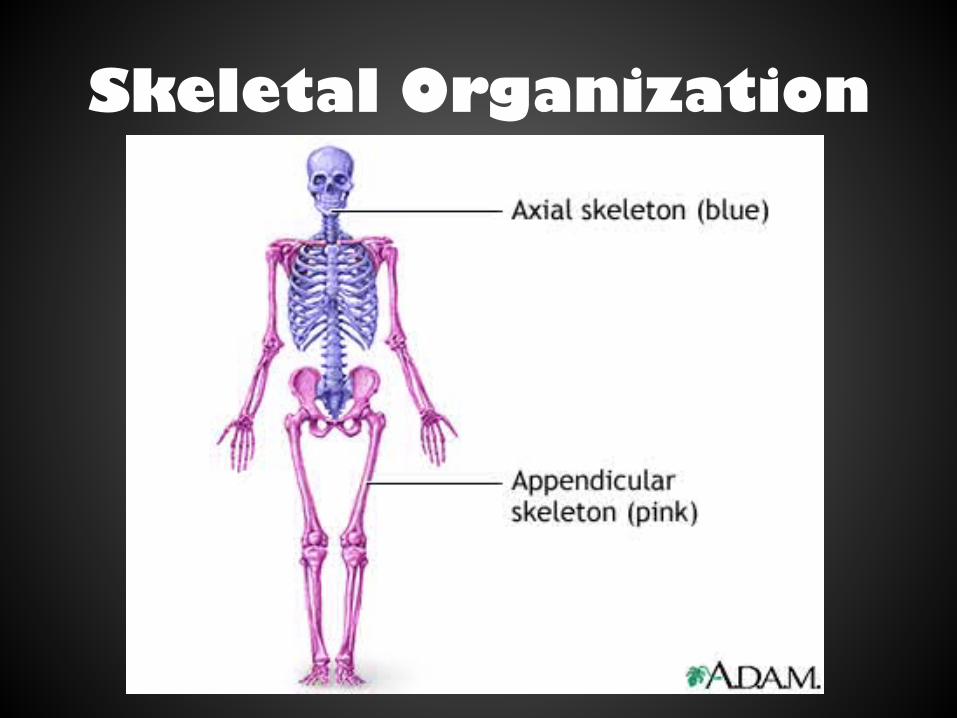
Skeletal Organization
• Axial Skeleton – Consists of the skull, hyoid bone, vertebral column and thorax (ribs and sternum)
• Appendicular Skeleton – Consists of the pectoral girdle (scapula and clavicle), upper limbs, pelvic girdle (coxal bones) and lower limbs
Skeletal Organization
The Skull!!
• Structure: made up of two sets of bones – Cranium – Facial bones
• Bones are joined by sutures
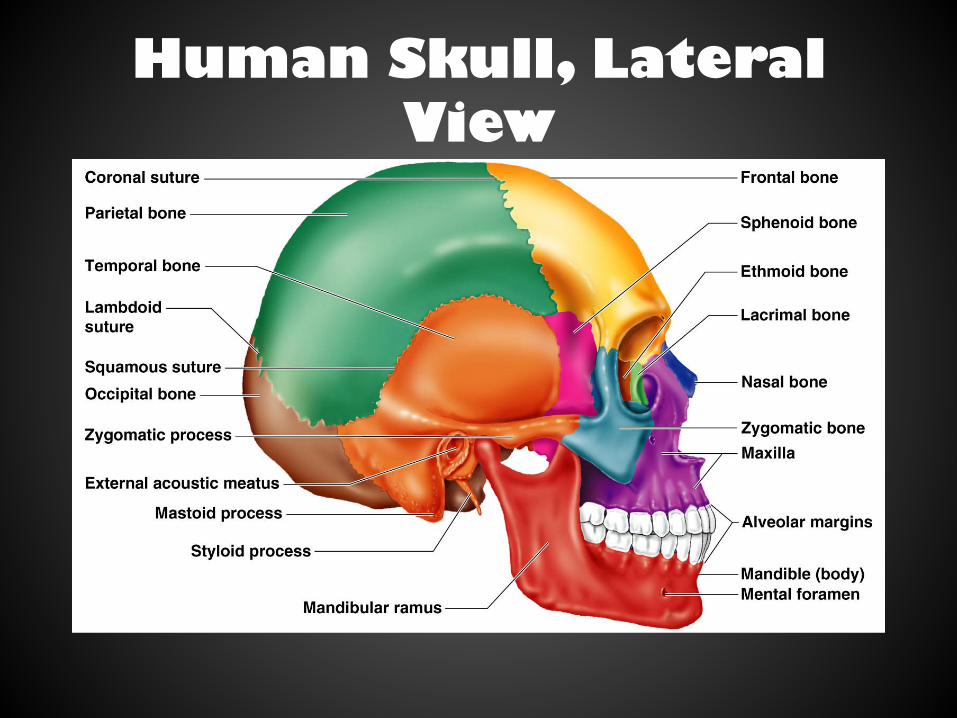
Human Skull, Lateral View
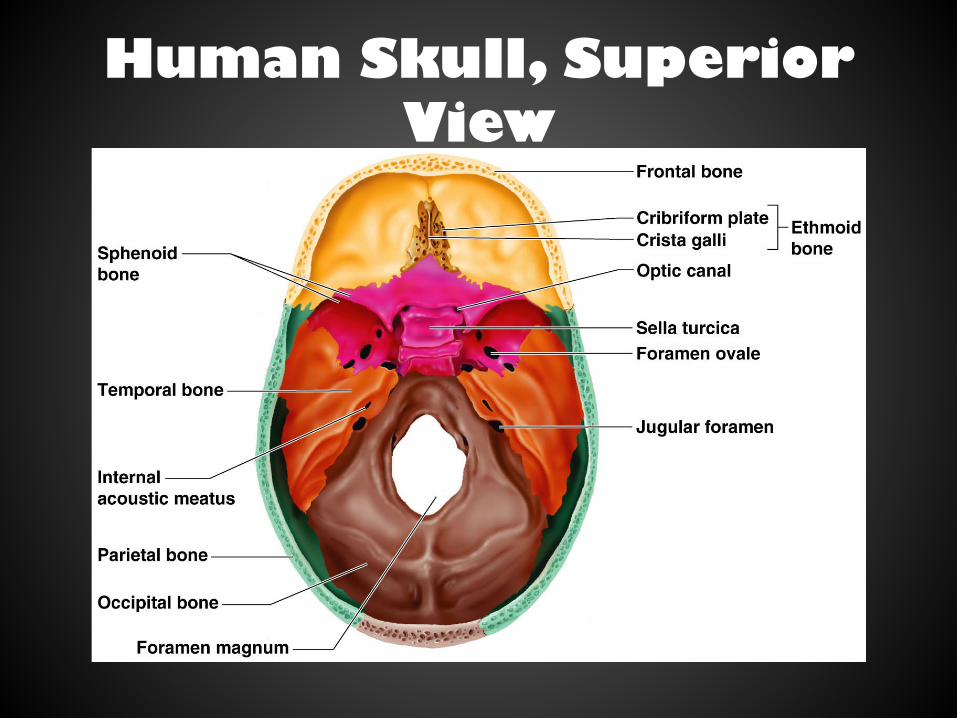
Human Skull, Superior View
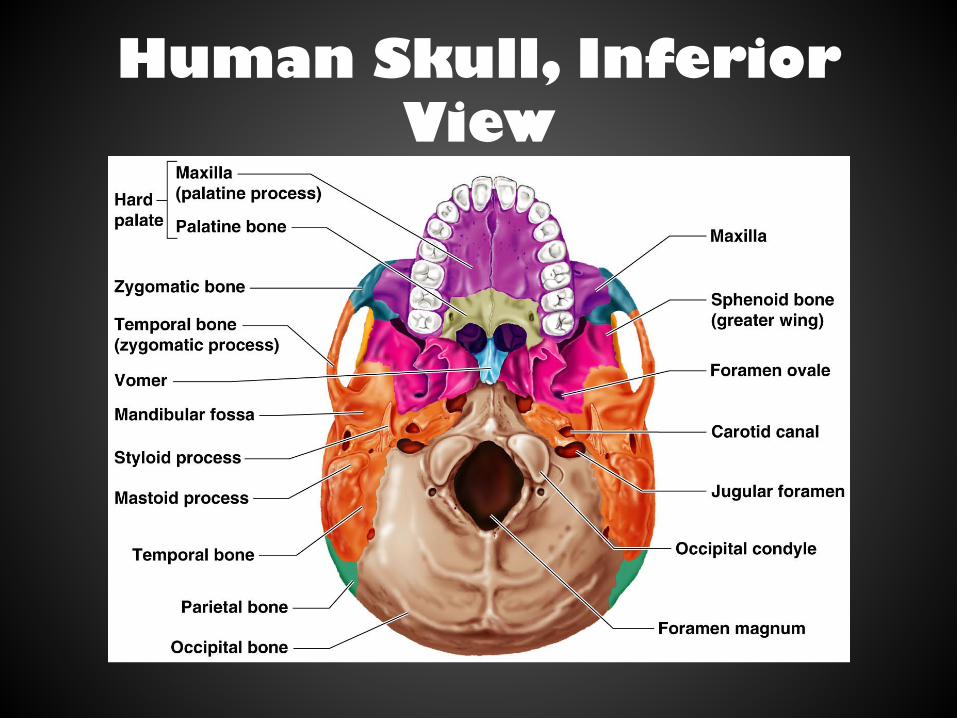
Human Skull, Inferior View
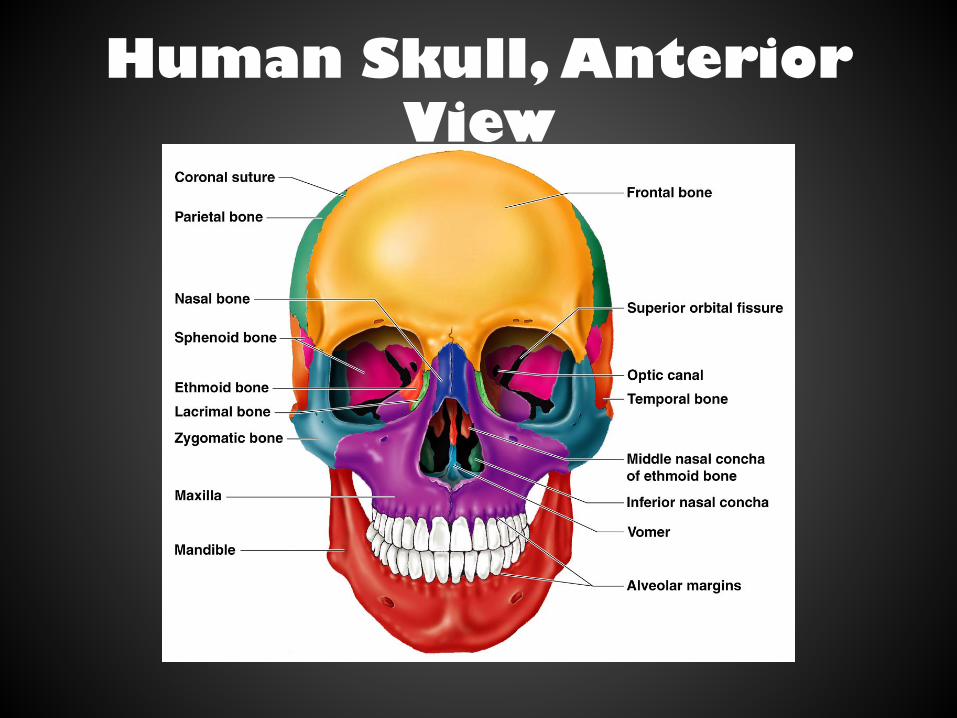
Human Skull, Anterior View
Paranasal Sinuses
• Structure: hollow por/ons of bones surrounding the nasal cavity
• Func/ons: – Lighten the skull – Amplify voice
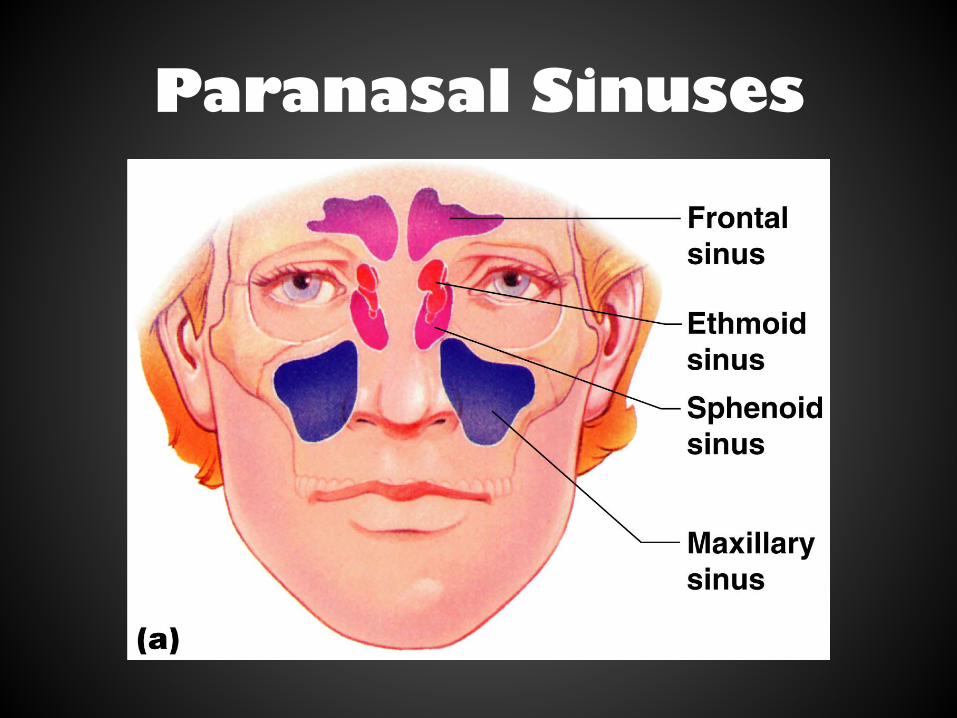
Paranasal Sinuses
The Vertebral Column
• Structure: 24 single vertebral bones separated by intervertebral discs – Cervical vertebrae: 7 in neck – Thoracic vertebrae: 12 in chest region – Lumbar vertebrae: 5 in lower back – Sacrum and coccyx: 9 fused vertebrae in gluteal region
The Vertebral Column
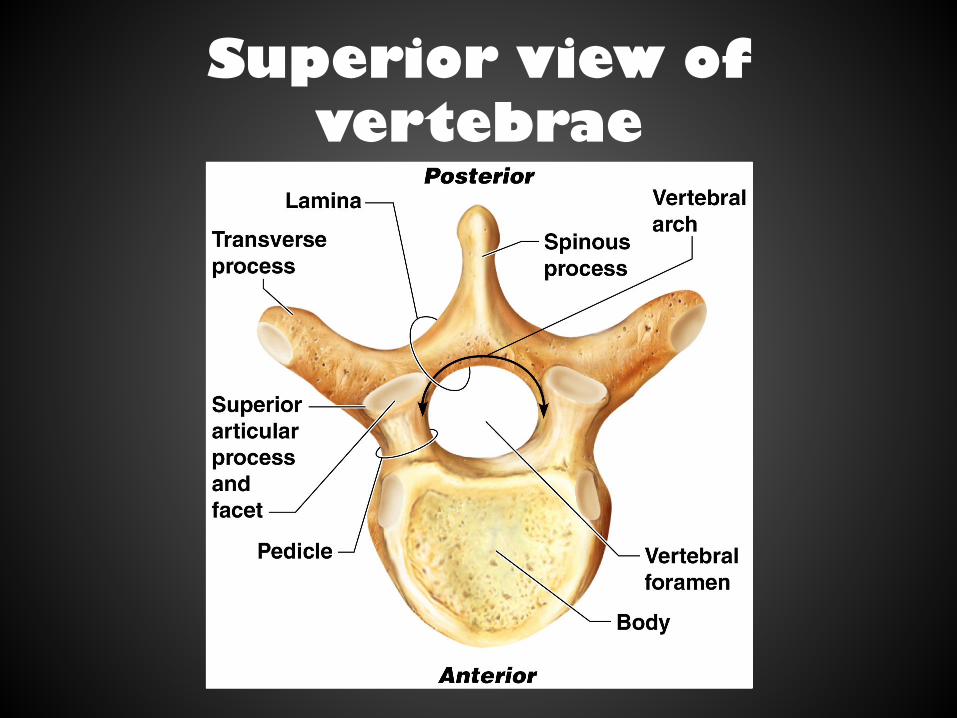
Superior view of vertebrae
Atlas and Axis
• Structure: most superior vertebrae – Atlas: C1 – Axis: C2
• Func/on: form joint connec/ng skull and spine; allow for movement of head

Regional characteristics of vertebrae
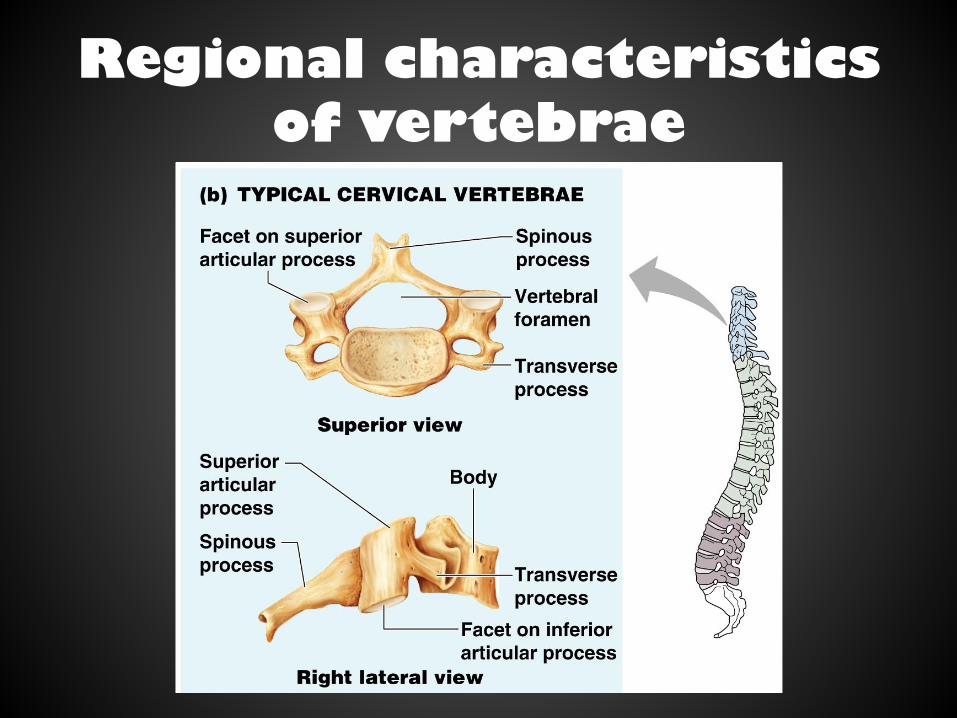
Regional characteristics of vertebrae
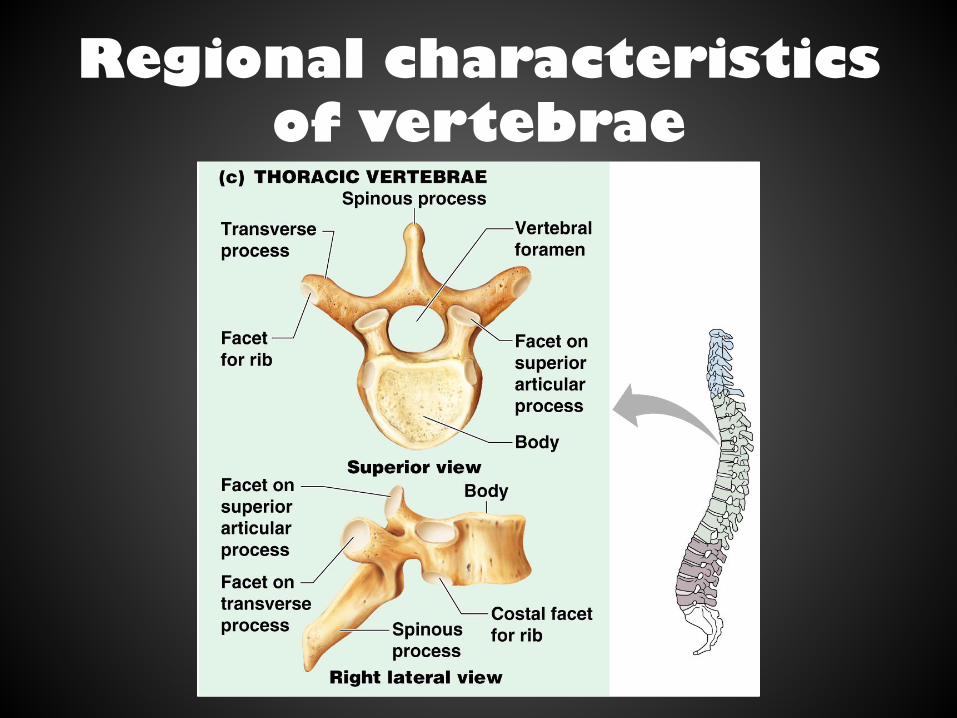
Regional characteristics of vertebrae
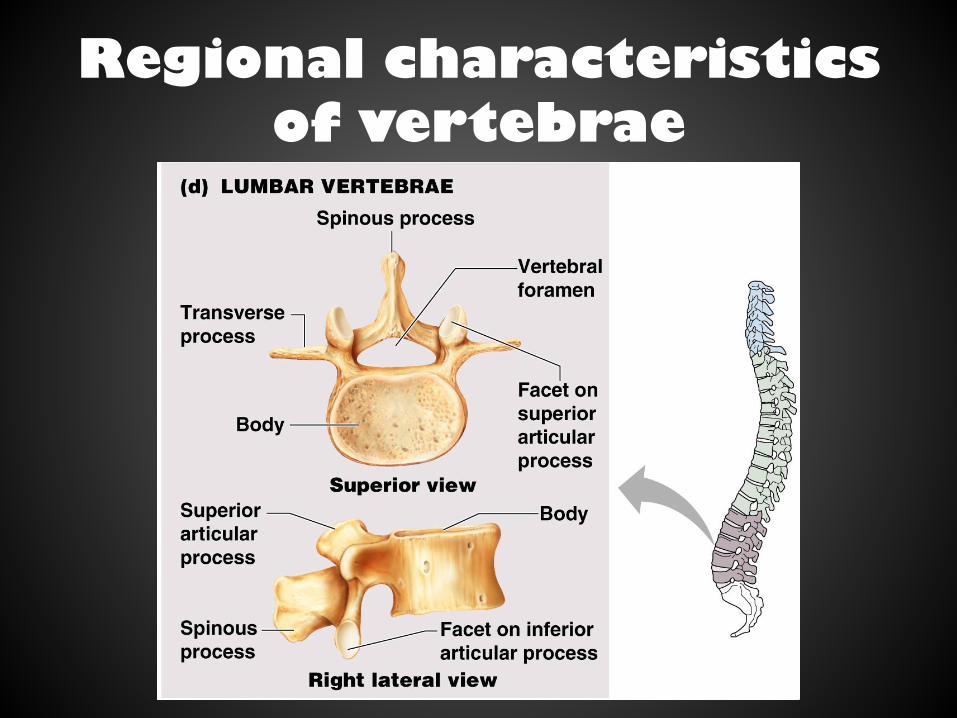
Regional characteristics of vertebrae
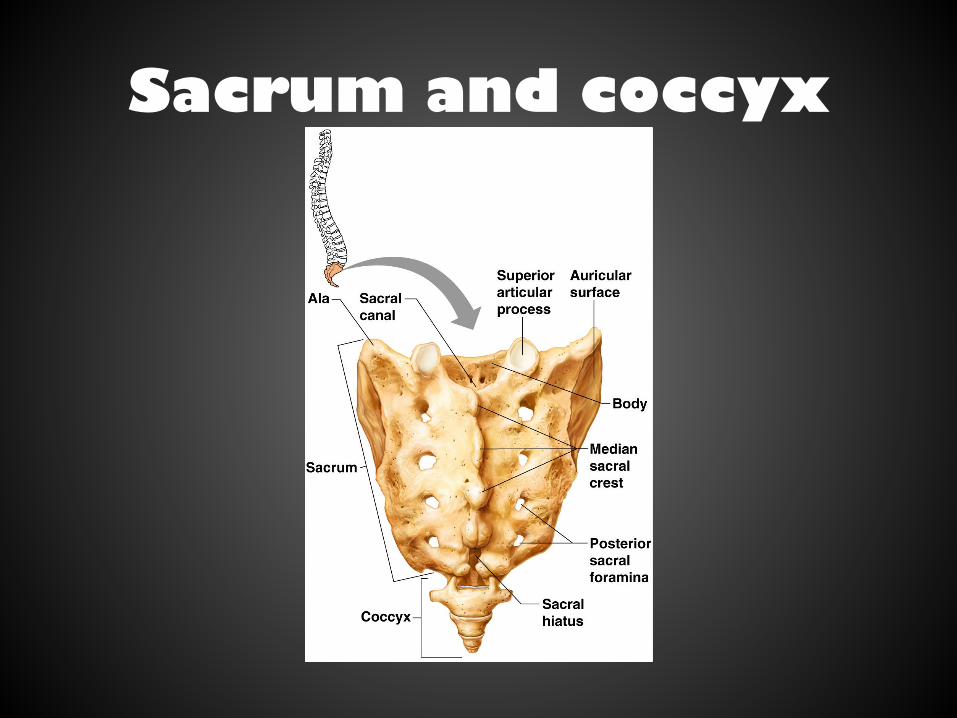
Sacrum and coccyx
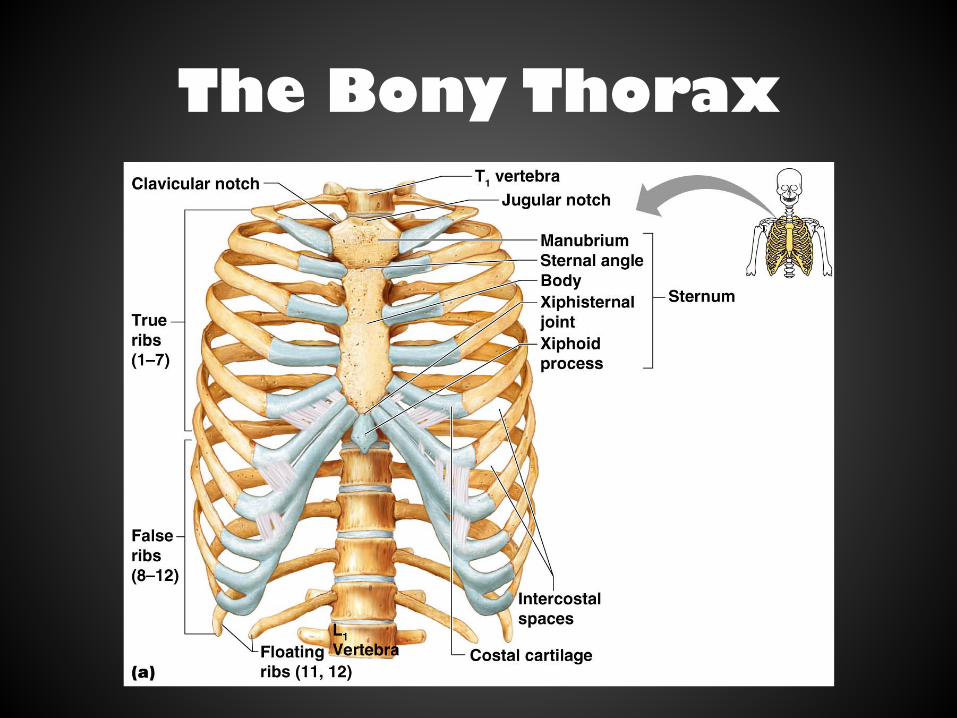
The Bony Thorax
• Structure: made of three parts 1. Sternum 2. Ribs • True ribs (pairs 1-‐7) • False ribs (pairs 8-‐12) • Floa/ng ribs (pairs 11-‐12)
3. Thoracic vertebrae • Func/on: forms a cage to protect major organs
The Bony Thorax
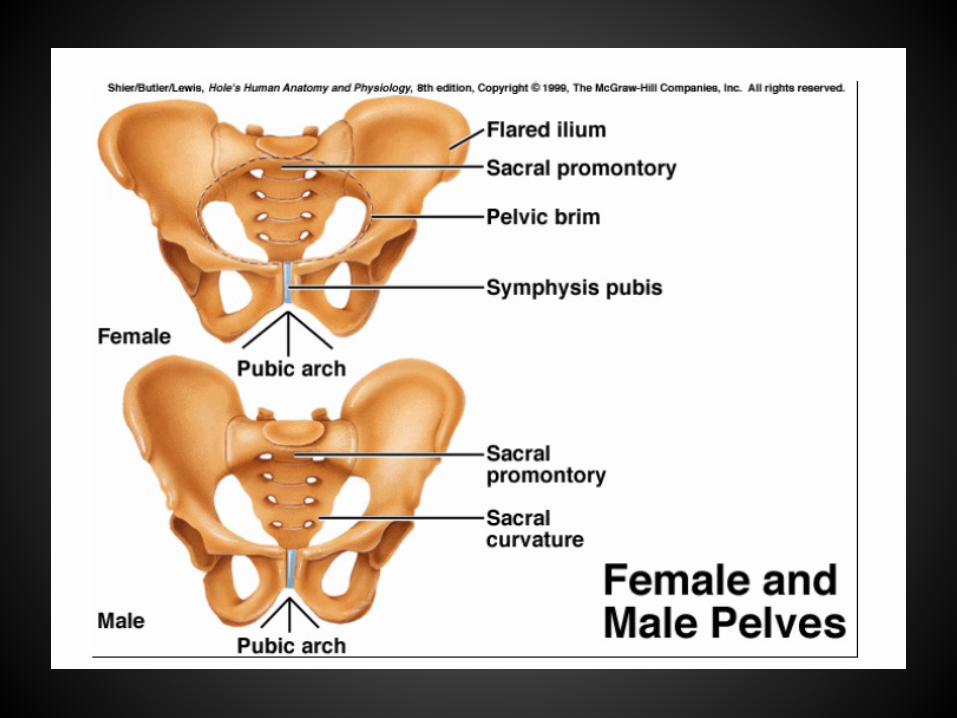
Male and Female Pelvis • Differences in male and female pelvis aid in childbirth – Female inlet is larger and more cicular – Female pelvis as a whole is shallower and the bones are lighter and thinner
– Female ilia flare more laterally – Female sacrum is shorter and less curved – Female ischial spines are shorter and further apart – Female pubic arch is more founded because the angle of the pubic arch is greater
Joints
• The func/onal junc/ons (ar/cula/ons) between bones
• Enable a wide variety of body movements • Can be classified according to the degree of movement possible: – Immovable – Slightly movable – Freely movable
Joints
• Can also be classified according to the type of /ssue that binds them together: – Fibrous – Car/laginous – Synovial

Fibrous Joints • Held together by dense connec/ve /ssue
• Immovable or only slightly moveable – Examples: • Sutures of the skull (immovable)
• Joint between the distal /bia and fibula (slightly movable)
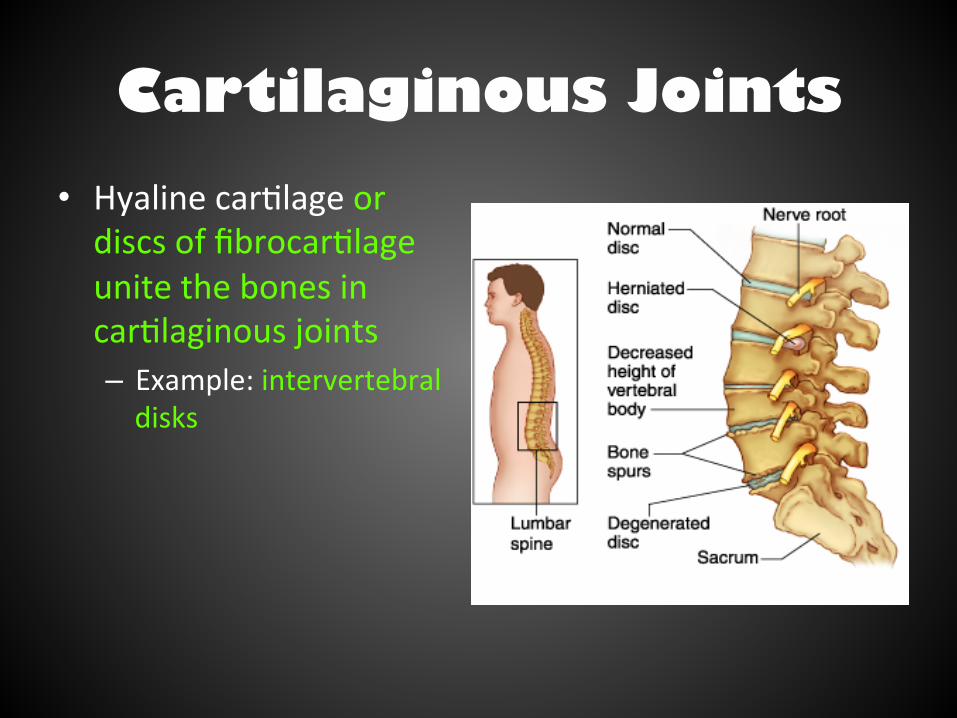
Cartilaginous Joints • Hyaline car/lage or discs of fibrocar/lage unite the bones in car/laginous joints – Example: intervertebral disks
Synovial Joints • Makes up most joints of the skeletal • More complex than fibrous or car/laginous joints
• Ar/cular ends of bone in a synovial joint are covered with hyaline car/lage
• Ar/cula/ng surfaces within the joint are lubricated with synovial fluid
• Are classified (and named) based on the shapes of their parts and the movements they permit
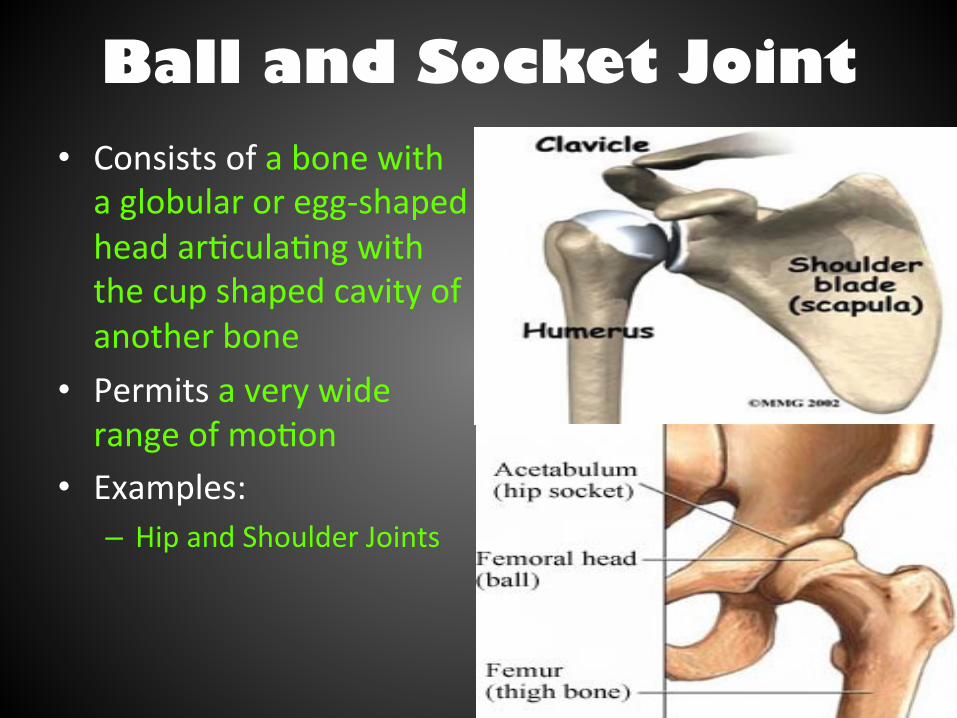
Ball and Socket Joint • Consists of a bone with a globular or egg-‐shaped head ar/cula/ng with the cup shaped cavity of another bone
• Permits a very wide range of mo/on
• Examples: – Hip and Shoulder Joints
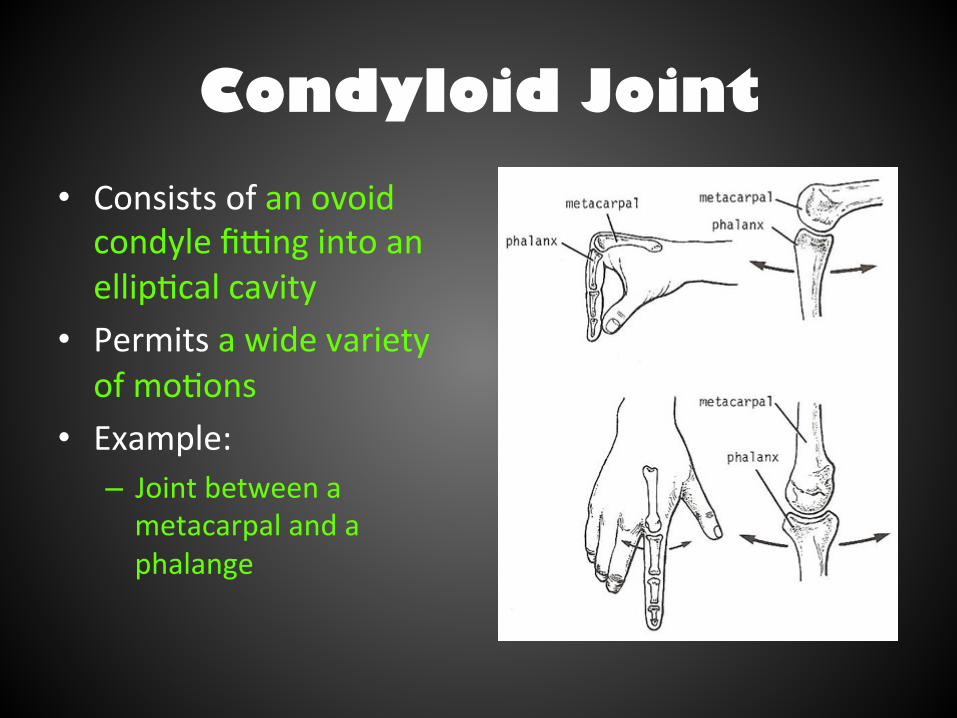
Condyloid Joint • Consists of an ovoid condyle fihng into an ellip/cal cavity
• Permits a wide variety of mo/ons
• Example: – Joint between a metacarpal and a phalange
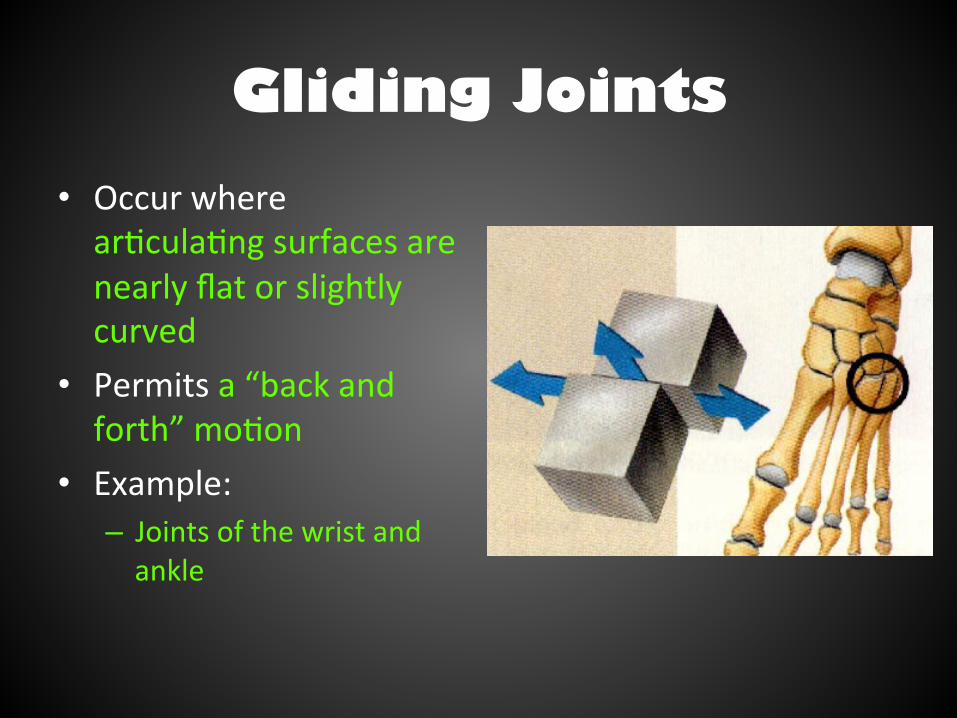
Gliding Joints • Occur where ar/cula/ng surfaces are nearly flat or slightly curved
• Permits a “back and forth” mo/on
• Example: – Joints of the wrist and ankle
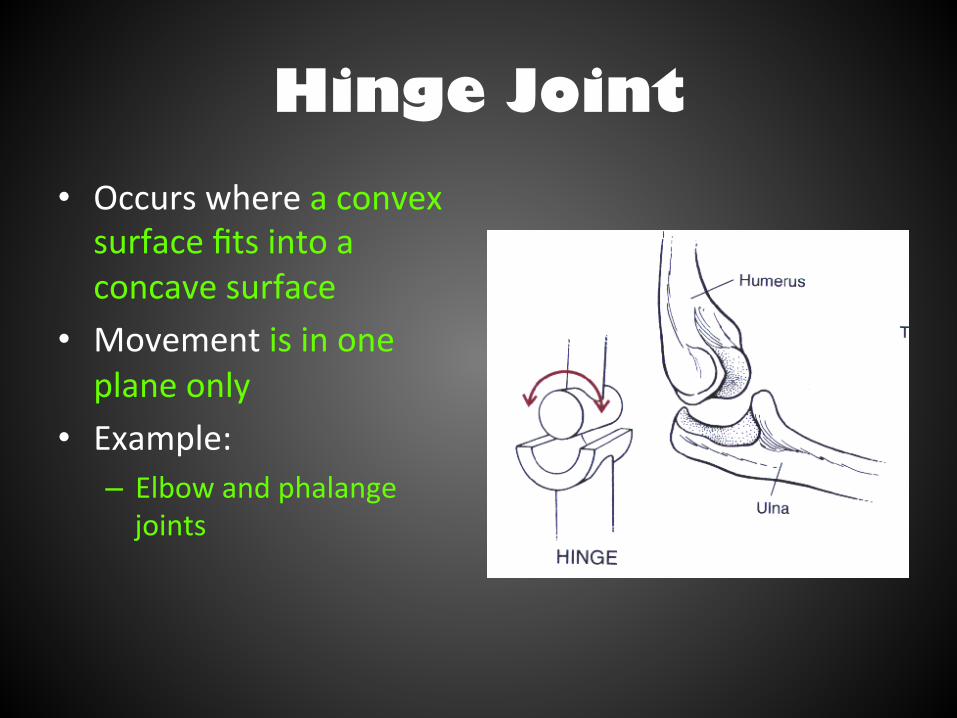
Hinge Joint • Occurs where a convex surface fits into a concave surface
• Movement is in one plane only
• Example: – Elbow and phalange joints
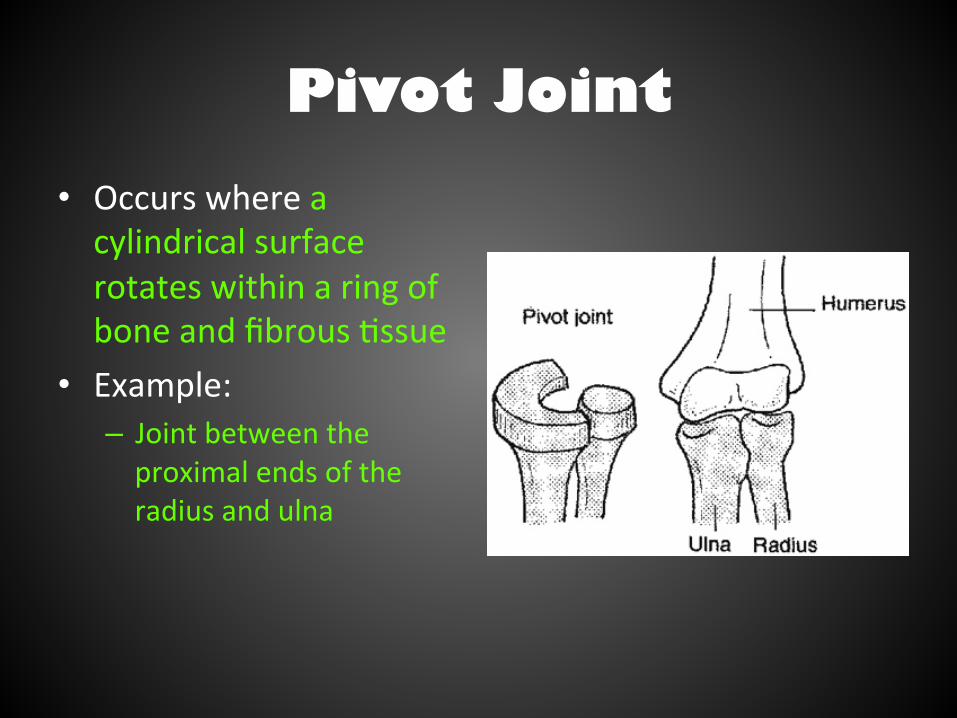
Pivot Joint • Occurs where a cylindrical surface rotates within a ring of bone and fibrous /ssue
• Example: – Joint between the proximal ends of the radius and ulna

Saddle Joint • Forms where ar/cula/ng surfaces have both concave and convex areas
• Permits a wide range of movements
• Example: – The metacarpal of the thumb
Inflammatory Disorders of the Joints
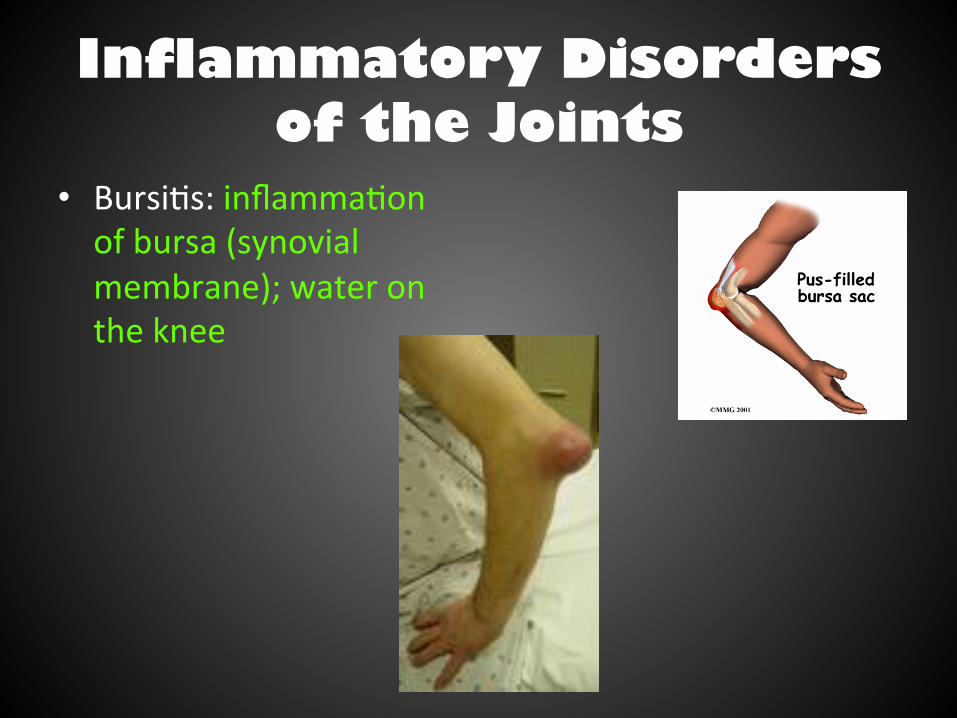
• Bursi/s: inflamma/on of bursa (synovial membrane); water on the knee
Inflammatory Disorders of the Joints
• Sprain – Ligaments or tendons reinforcing joint are damaged by excessive stretching or are torn away from bone
– Slow to heal because of poor blood supply • Disloca/on – When a bone is forced out of normal posi/on in the joint cavity
Inflammatory Disorders of the Joints
• Arthri/s – Most widespread, crippling disease in the U.S. – 1 in 7 Americans suffer with it – Ini/al symptoms: Pain, s/ffness, and swelling of the joint
– Acute and Chronic forms of Arthri/s

Inflammatory Disorders of the Joints
• Acute Arthri/s – Result from bacterial invasion – Treated with an/bio/c – Synovial membrane thickens and fluid produc/on decreases, leading to increased fric/on and pain
Inflammatory Disorders of the Joints
• Chronic Arthri/s – Osteoarthri/s
• Most common form • Degenera/ve condi/on, usually affects the aged • Wear and tear affects • Can cause bone spurs which restrict joint movement
– Rheumatoid arthri/s • Occurs between 40-‐50 years of, but can occur at any age • Affects more women than men • Many joints affected at the same /me and usually in symmetrical manner (leQ elbow then right elbow)
• Marked by remission (goes away) and flare ups (comes back) • Autoimmune disease – body aJacks its own /ssues
– Gouty arthri/s