Embed Size (px)
Citation preview

Studio GARDEL: Implicazioni e Confronti
Gianni Di Perri
Clinica di Malattie Infettive Università degli Studi di Torino
Ospedale Amedeo di Savoia
Ospedale Amedeo di Savoia
Carlos Gardel - Da Wikipedia, l'enciclopedia libera. Tolosa
11/12/1890 - Medellin 24/06/1935. E’ stato un cantante, attore e compositore argentino, personaggio di spicco nella storia del Tango
19 centres in 6 countries
Argentina Mexico Spain Peru Brasil USA
The GARDEL Study
Phase 3, open-label, randomized-controlled, for non-inferiority 95% CI -12% + 12% NCT 01237444
LPV/RTV 400/100 mg +
3TC 150 mg bid vs
LPV/RTV 400/100 mg bid
+ 3TC 300 mg or FTc 200 mg co-
formulated with AZT or TDF or ABV QD or bid (Combivir® )
Background
• In the current era, achieving plasma viral load suppression below
the level of detection is no longer a difficult task.
• Current challenges include: tolerability, toxicities, user
friendliness, pill count, simplicity, applicability to different
populations (pregnant women, children, drug-users, elderly, etc)
and cost.
• Different strategies tested in naïve patients, including PI/r-
monotherapy, generally failed to show non-inferiority when
compared to standard triple-drug combinations.
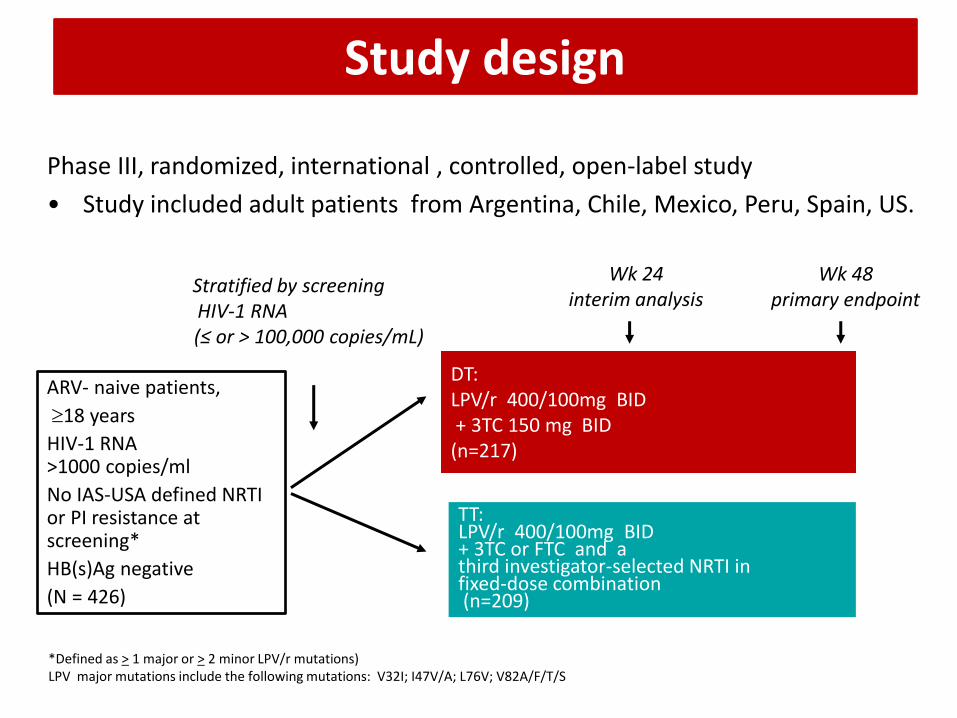
Study design
Phase III, randomized, international , controlled, open-label study
• Study included adult patients from Argentina, Chile, Mexico, Peru, Spain, US.
DT: LPV/r 400/100mg BID + 3TC 150 mg BID (n=217)
TT: LPV/r 400/100mg BID + 3TC or FTC and a third investigator-selected NRTI in fixed-dose combination (n=209)
ARV- naive patients,
18 years
HIV-1 RNA >1000 copies/ml
No IAS-USA defined NRTI or PI resistance at screening*
HB(s)Ag negative
(N = 426)
Stratified by screening HIV-1 RNA (≤ or > 100,000 copies/mL)
Wk 48 primary endpoint
*Defined as > 1 major or > 2 minor LPV/r mutations) LPV major mutations include the following mutations: V32I; I47V/A; L76V; V82A/F/T/S
Wk 24 interim analysis
Objectives • To compare the efficacy and safety of a dual therapy (DT)
combination of LPV/r 400/100 mg BID+3TC 150 mg BID to a triple therapy (TT) with LPV/r 400/100 mg BID+3TC or FTC and a third investigator-selected NRTI in fixed-dose combination in ARV-naïve patients.
• Primary endpoint
% of patients with HIV-1 RNA< 50 copies/mL in an ITT-exposed analysis at 48 weeks (FDA-snapshot algorithm).*
• Secondary objectives
– % of patients with HIV-1 RNA< 400 copies/mL (ITT-e at 24 weeks by FDA-snapshot algorithm).
– Safety, tolerability and resistance
– Immunologic responses
* Alpha 0.05, power 80%, 2-sided 95% CI, 12% margin
0 24 36 48
Virological Efficacy (< 50 copies/mL):
1) “Snapshot Evaluation”
3) TLOVR2
2) TLOVR1
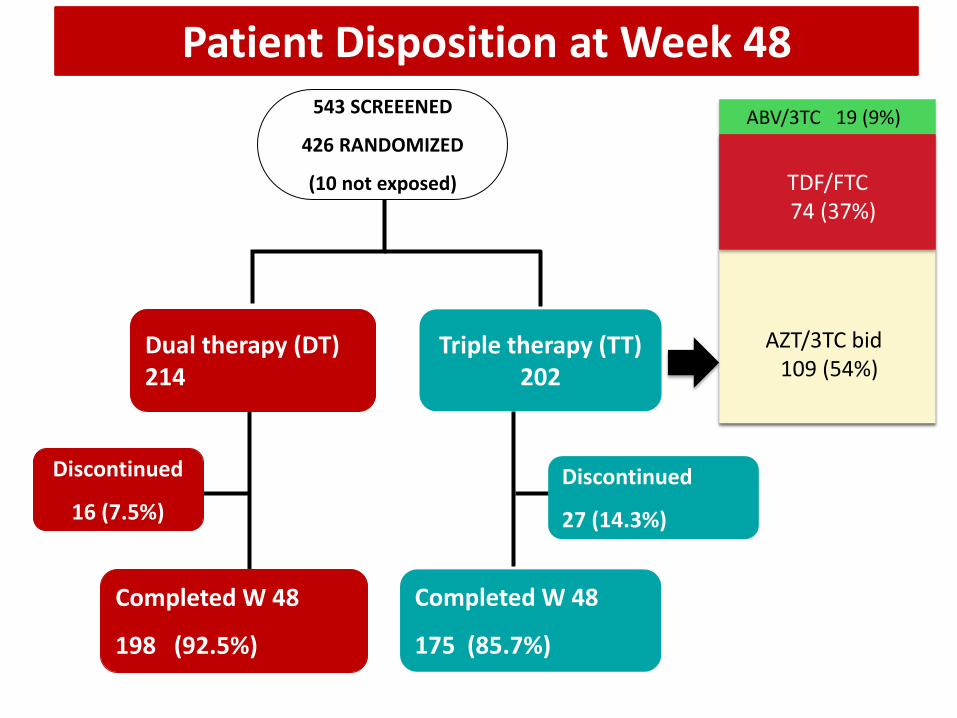
Patient Disposition at Week 48 543 SCREEENED
426 RANDOMIZED
(10 not exposed)
Completed W 48
198 (92.5%)
Completed W 48
175 (85.7%)
Discontinued
16 (7.5%)
Discontinued
27 (14.3%)
Dual therapy (DT) 214
Triple therapy (TT) 202
AZT/3TC bid 109 (54%)
TDF/FTC 74 (37%)
ABV/3TC 19 (9%)
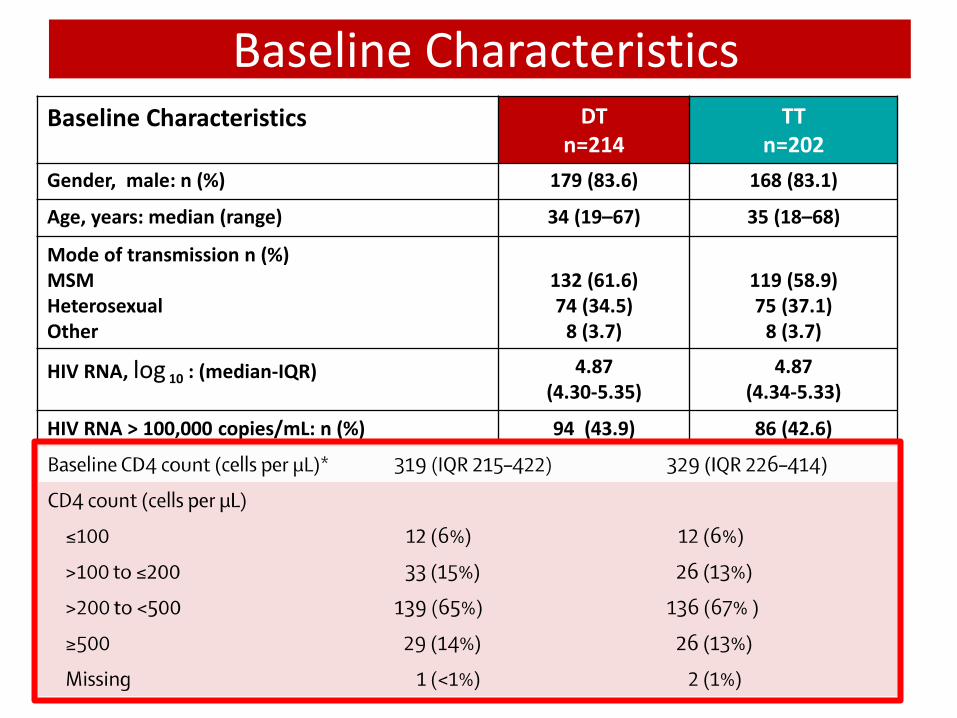
Baseline Characteristics Baseline Characteristics DT
n=214 TT
n=202
Gender, male: n (%) 179 (83.6) 168 (83.1)
Age, years: median (range) 34 (19–67) 35 (18–68)
Mode of transmission n (%) MSM Heterosexual Other
132 (61.6) 74 (34.5)
8 (3.7)
119 (58.9) 75 (37.1)
8 (3.7)
HIV RNA, log 10 : (median-IQR) 4.87 (4.30-5.35)
4.87 (4.34-5.33)
HIV RNA > 100,000 copies/mL: n (%) 94 (43.9) 86 (42.6)
CD4 count, cells/mm3:(median-IQR) 319 (215-422) 329 (226-414)
CD4 count ≤ 200 cells/mm3: n (%) 45 (21.1) 38 (18.8)
CDC stage 3 n (%) 6 (2.8) 6 (2.9)
Background NRTIs N/A ABC/3TC:19 TDF/FTC: 74
ZDV/3TC: 109
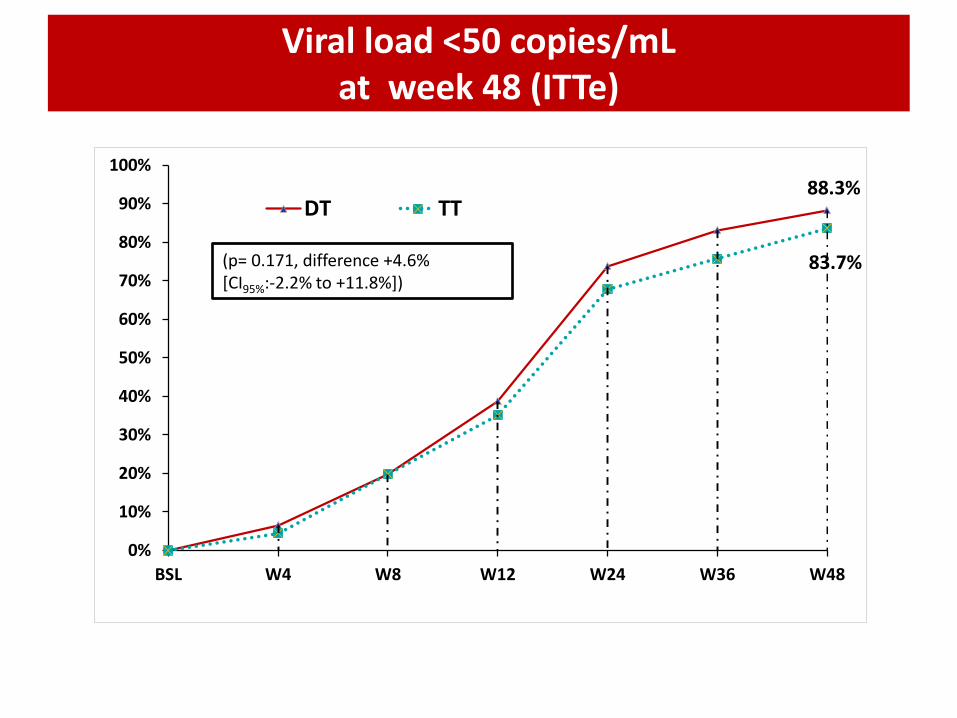
Viral load <50 copies/mL at week 48 (ITTe)
88.3%
83.7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
BSL W4 W8 W12 W24 W36 W48
DT TT
(p= 0.171, difference +4.6% [CI95%:-2.2% to +11.8%])
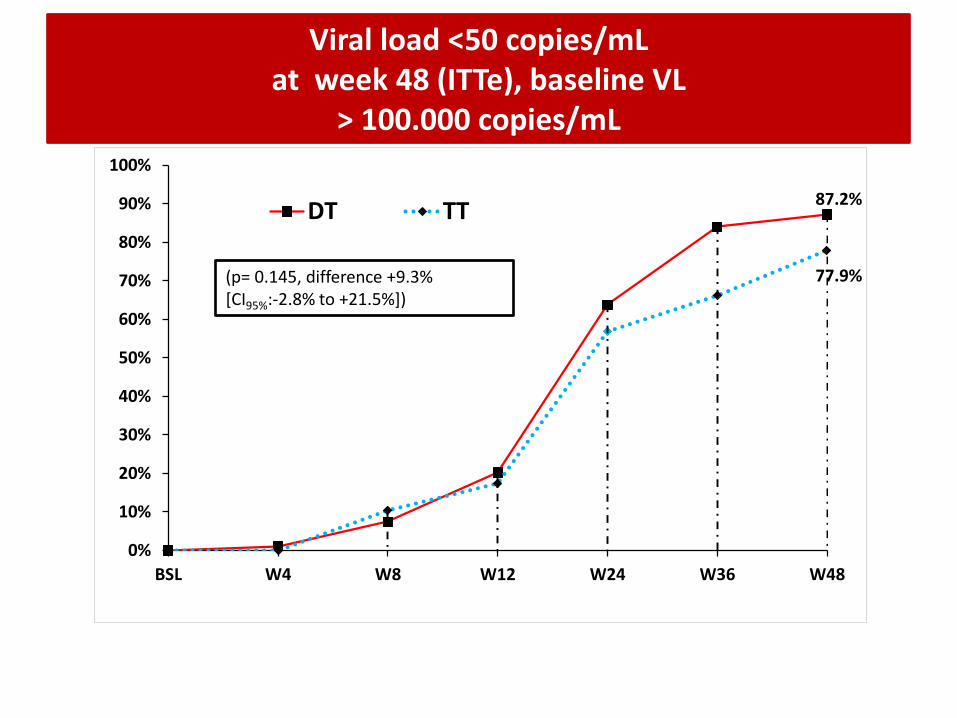
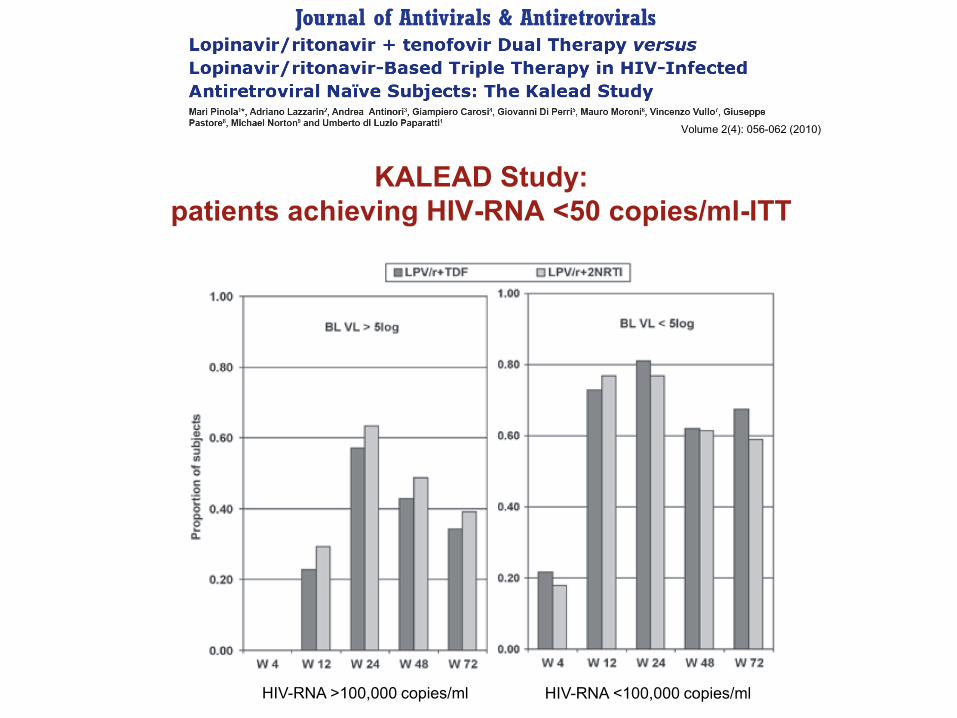
Viral load <50 copies/mL at week 48 (ITTe), baseline VL
> 100.000 copies/mL
87.2%
77.9%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
BSL W4 W8 W12 W24 W36 W48
DT TT
(p= 0.145, difference +9.3% [CI95%:-2.8% to +21.5%])
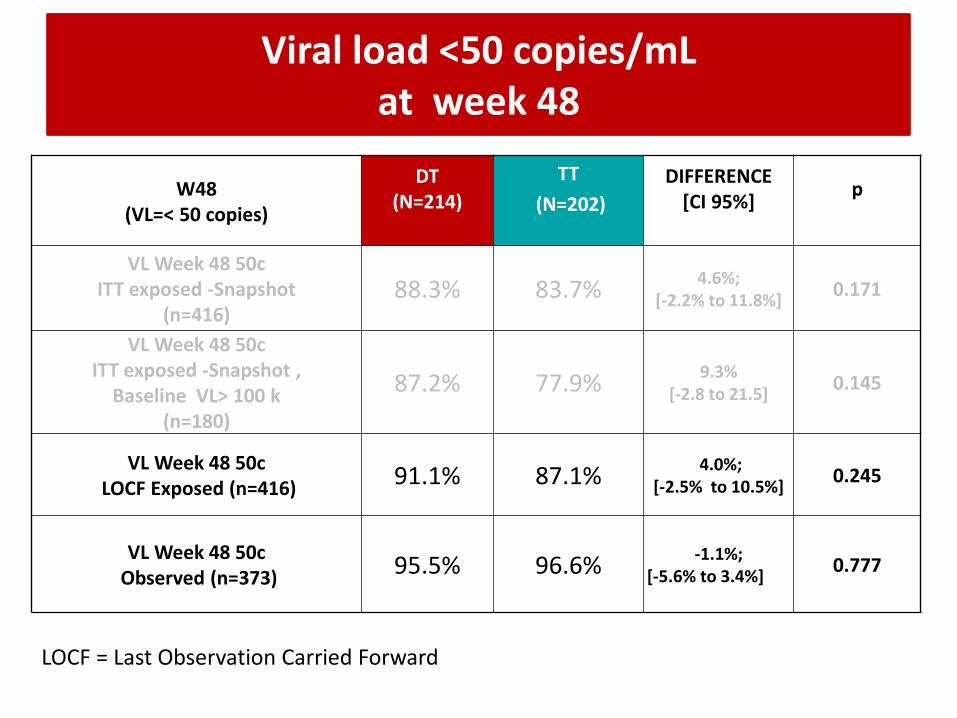
Viral load <50 copies/mL at week 48
W48 (VL=< 50 copies)
DT (N=214)
TT
(N=202)
DIFFERENCE [CI 95%]
p
VL Week 48 50c ITT exposed -Snapshot
(n=416) 88.3% 83.7%
4.6%; [-2.2% to 11.8%]
0.171
VL Week 48 50c ITT exposed -Snapshot ,
Baseline VL> 100 k (n=180)
87.2% 77.9% 9.3%
[-2.8 to 21.5] 0.145
VL Week 48 50c LOCF Exposed (n=416)
91.1% 87.1% 4.0%;
[-2.5% to 10.5%] 0.245
VL Week 48 50c Observed (n=373)
95.5%
96.6%
-1.1%; [-5.6% to 3.4%]
0.777
LOCF = Last Observation Carried Forward
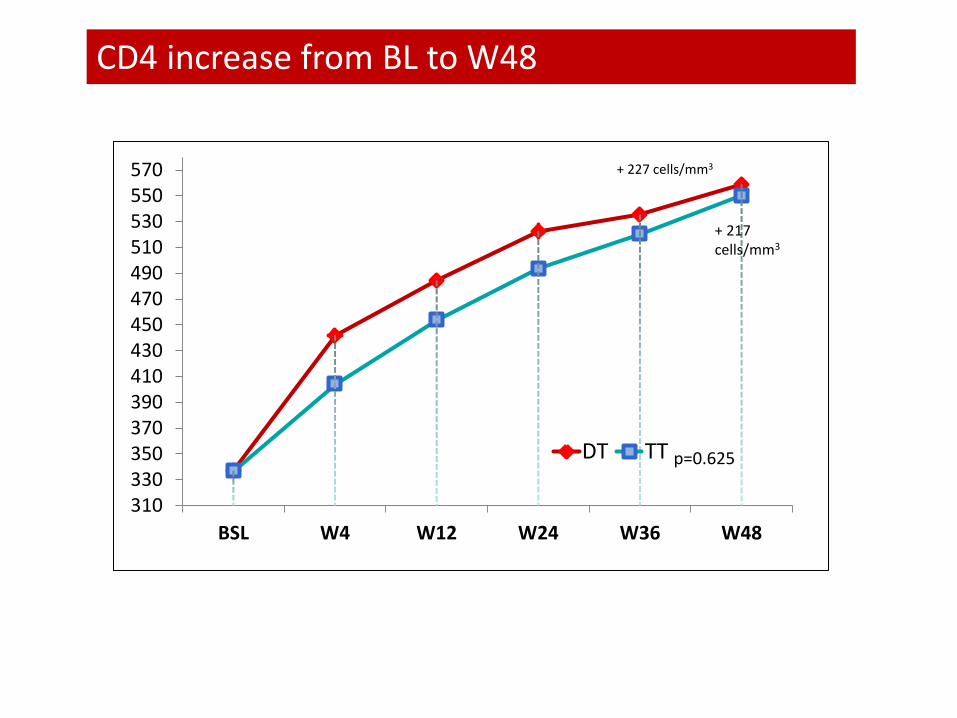
CD4 increase from BL to W48
310330350370390410430450470490510530550570
BSL W4 W12 W24 W36 W48
DT TT
+ 227 cells/mm3
+ 217 cells/mm3
p=0.625
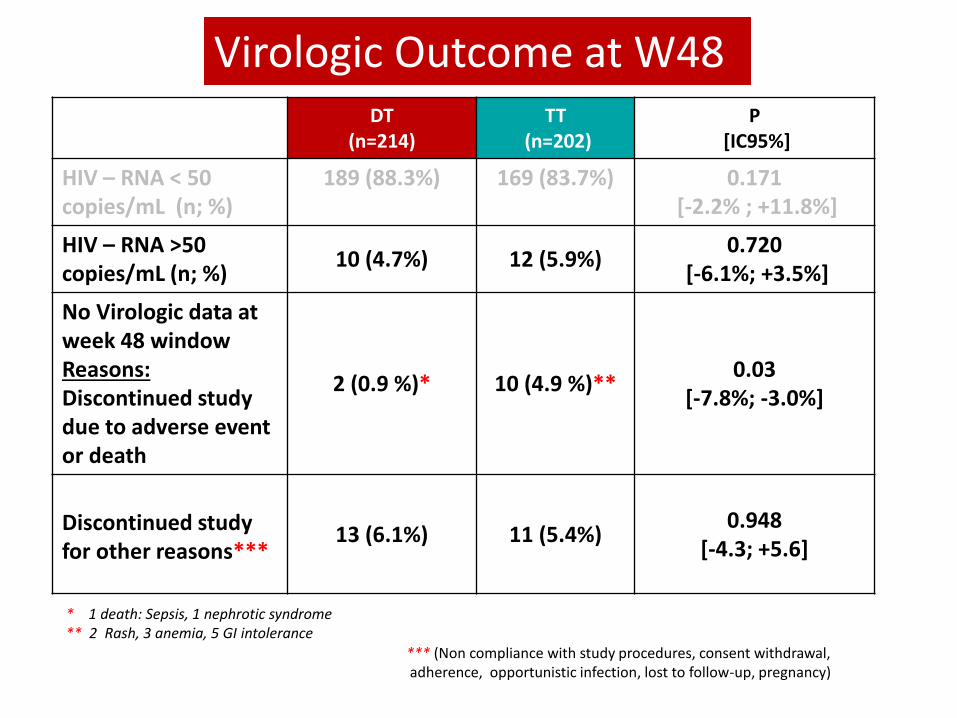
DT (n=214)
TT (n=202)
P [IC95%]
HIV – RNA < 50 copies/mL (n; %)
189 (88.3%) 169 (83.7%) 0.171 [-2.2% ; +11.8%]
HIV – RNA >50 copies/mL (n; %)
10 (4.7%) 12 (5.9%) 0.720
[-6.1%; +3.5%]
No Virologic data at week 48 window Reasons: Discontinued study due to adverse event or death
2 (0.9 %)* 10 (4.9 %)** 0.03
[-7.8%; -3.0%]
Discontinued study for other reasons***
13 (6.1%) 11 (5.4%) 0.948
[-4.3; +5.6]
Virologic Outcome at W48
*** (Non compliance with study procedures, consent withdrawal, adherence, opportunistic infection, lost to follow-up, pregnancy)
* 1 death: Sepsis, 1 nephrotic syndrome ** 2 Rash, 3 anemia, 5 GI intolerance
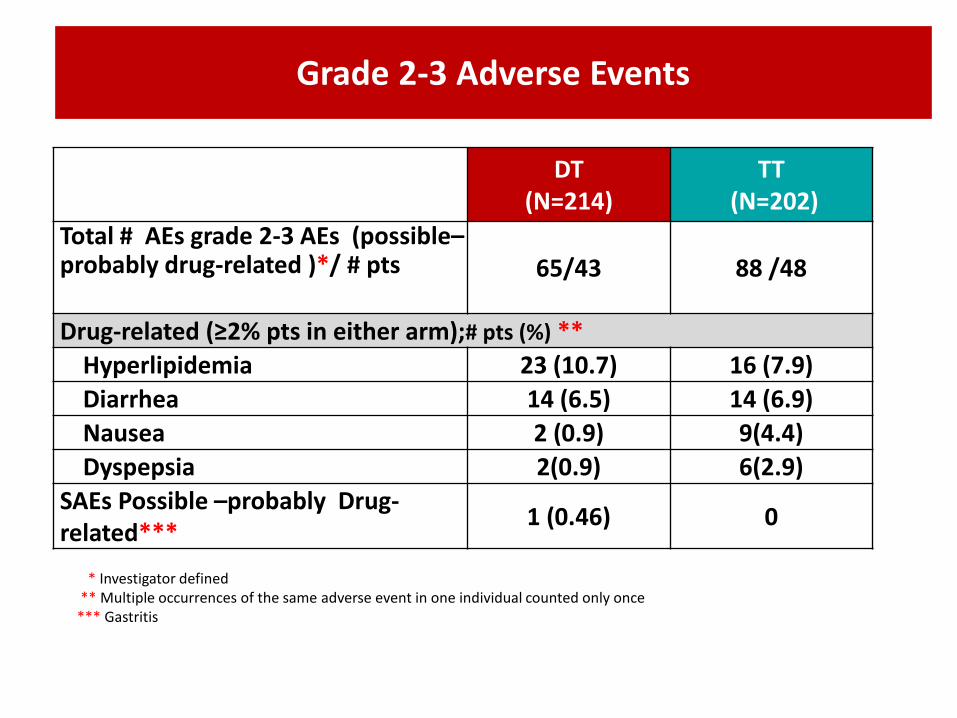
Grade 2-3 Adverse Events
DT (N=214)
TT (N=202)
Total # AEs grade 2-3 AEs (possible–probably drug-related )*/ # pts 65/43 88 /48
Drug-related (≥2% pts in either arm);# pts (%) **
Hyperlipidemia 23 (10.7) 16 (7.9)
Diarrhea 14 (6.5) 14 (6.9)
Nausea 2 (0.9) 9(4.4)
Dyspepsia 2(0.9) 6(2.9)
SAEs Possible –probably Drug-related***
1 (0.46) 0
* Investigator defined ** Multiple occurrences of the same adverse event in one individual counted only once *** Gastritis
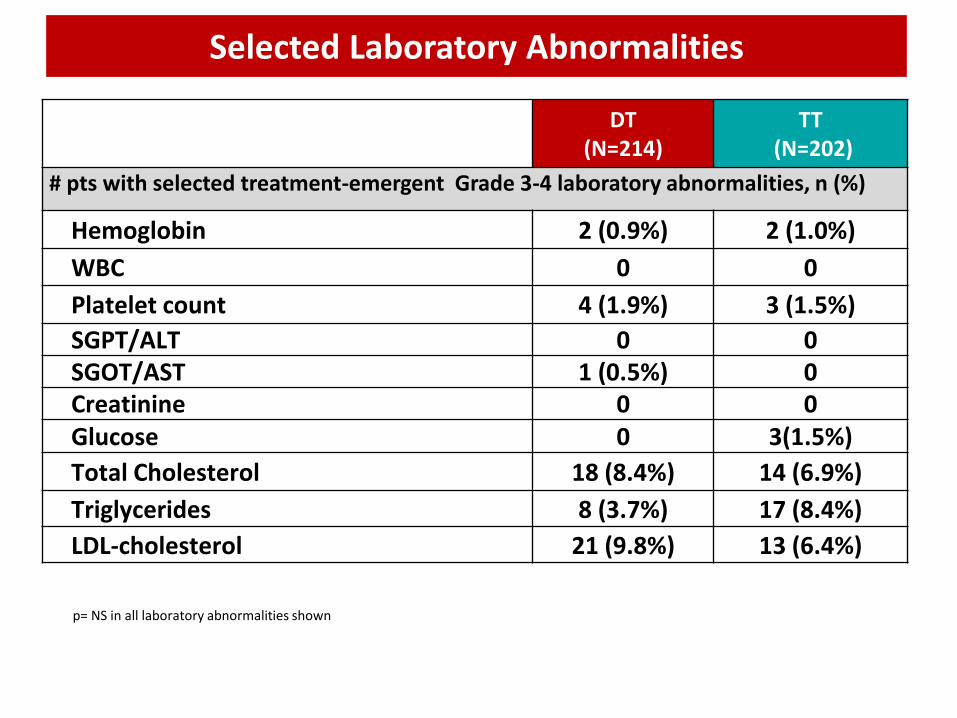
A DT (N=214)
TT (N=202)
# pts with selected treatment-emergent Grade 3-4 laboratory abnormalities, n (%)
Hemoglobin 2 (0.9%) 2 (1.0%)
WBC 0 0
Platelet count 4 (1.9%) 3 (1.5%)
SGPT/ALT 0 0 SGOT/AST 1 (0.5%) 0 Creatinine 0 0 Glucose 0 3(1.5%)
Total Cholesterol 18 (8.4%) 14 (6.9%)
Triglycerides 8 (3.7%) 17 (8.4%)
LDL-cholesterol 21 (9.8%) 13 (6.4%)
Selected Laboratory Abnormalities
p= NS in all laboratory abnormalities shown
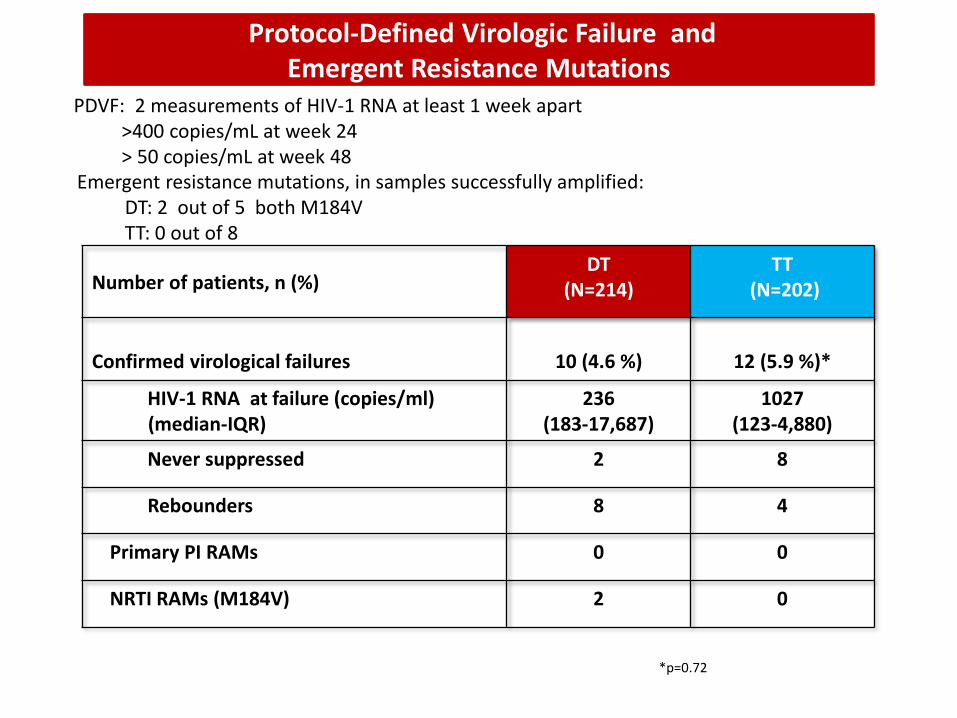
Protocol-Defined Virologic Failure and Emergent Resistance Mutations
Number of patients, n (%) DT
(N=214) TT
(N=202)
Confirmed virological failures
10 (4.6 %)
12 (5.9 %)*
HIV-1 RNA at failure (copies/ml) (median-IQR)
236 (183-17,687)
1027 (123-4,880)
Never suppressed 2 8
Rebounders 8 4
Primary PI RAMs 0 0
NRTI RAMs (M184V) 2 0
*p=0.72
PDVF: 2 measurements of HIV-1 RNA at least 1 week apart >400 copies/mL at week 24 > 50 copies/mL at week 48
Emergent resistance mutations, in samples successfully amplified: DT: 2 out of 5 both M184V TT: 0 out of 8
• Our results demonstrate that DT with LPV/r+3TC was non-inferior to triple therapy after 48 weeks of treatment, regardless of baseline viral load.
• The DT regimen showed fewer discontinuations due to safety and tolerability .
• Virologic failure, occurring at similarly low levels in both treatment arms, did not result in PI resistance development, preserving a wide range of drugs for 2nd line ARV therapy.
• These results suggest that a dual LPV/r+3TC regimen warrants further clinical research and consideration as a potential therapeutic option for ARV naïve subjects.
GARDEL: conclusions
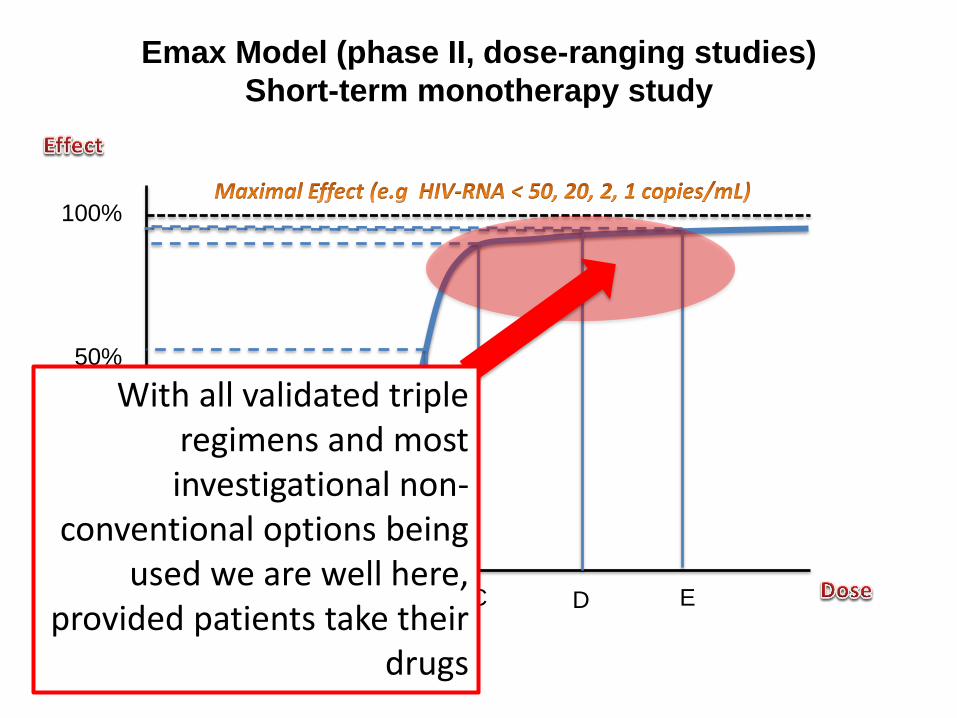
Emax Model (phase II, dose-ranging studies)
Short-term monotherapy study
100%
50%
20%
10%
0
A B C D E
With all validated triple regimens and most investigational non-
conventional options being used we are well here,
provided patients take their drugs

LDR: Razionale Soluzioni che permettano una maggiore personalizzazione della terapia offrendo vantaggi in termini clinici e/o economici senza riduzioni di efficacia.
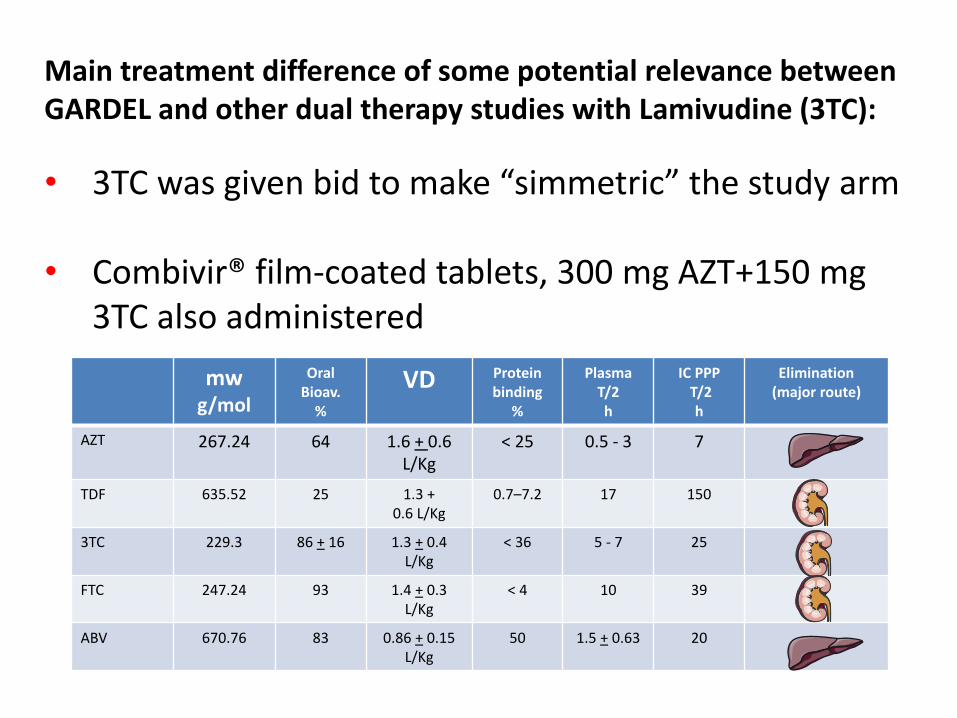
Main treatment difference of some potential relevance between GARDEL and other dual therapy studies with Lamivudine (3TC):
• 3TC was given bid to make “simmetric” the study arm
• Combivir® film-coated tablets, 300 mg AZT+150 mg 3TC also administered
mw g/mol
Oral Bioav.
%
VD Protein binding
%
Plasma T/2 h
IC PPP T/2
h
Elimination (major route)
AZT 267.24 64 1.6 + 0.6 L/Kg
< 25 0.5 - 3 7
TDF 635.52 25 1.3 + 0.6 L/Kg
0.7–7.2 17 150
3TC 229.3 86 + 16 1.3 + 0.4 L/Kg
< 36 5 - 7 25
FTC 247.24 93 1.4 + 0.3 L/Kg
< 4 10 39
ABV 670.76 83 0.86 + 0.15 L/Kg
50 1.5 + 0.63 20
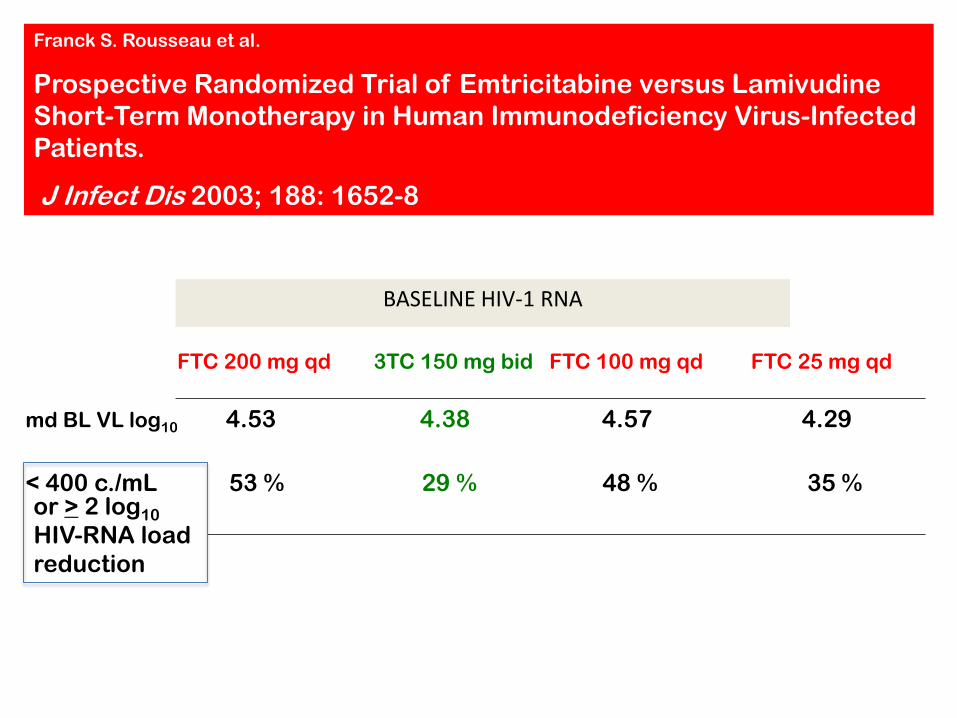
Franck S. Rousseau et al.
Prospective Randomized Trial of Emtricitabine versus Lamivudine
Short-Term Monotherapy in Human Immunodeficiency Virus-Infected
Patients.
J Infect Dis 2003; 188: 1652-8
BASELINE HIV-1 RNA
FTC 200 mg qd 3TC 150 mg bid FTC 100 mg qd FTC 25 mg qd
md BL VL log10 4.53 4.38 4.57 4.29
or > 2 log10
HIV-RNA load
reduction
< 400 c./mL 53 % 29 % 48 % 35 %
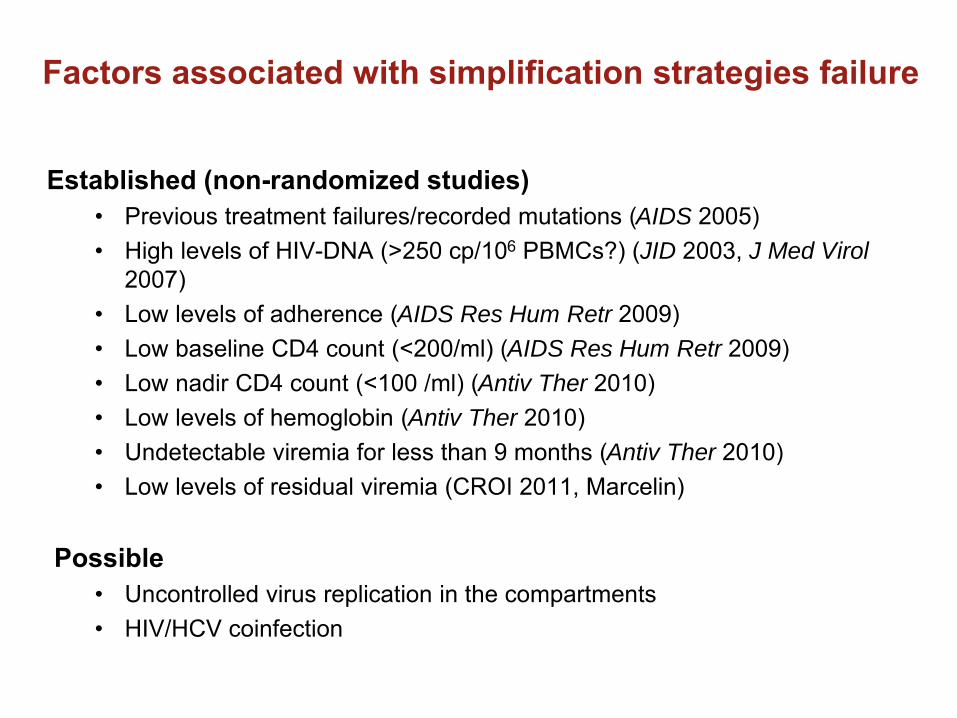
AIDS
JID J Med Virol
AIDS Res Hum Retr
AIDS Res Hum Retr
Antiv Ther
Antiv Ther
Antiv Ther
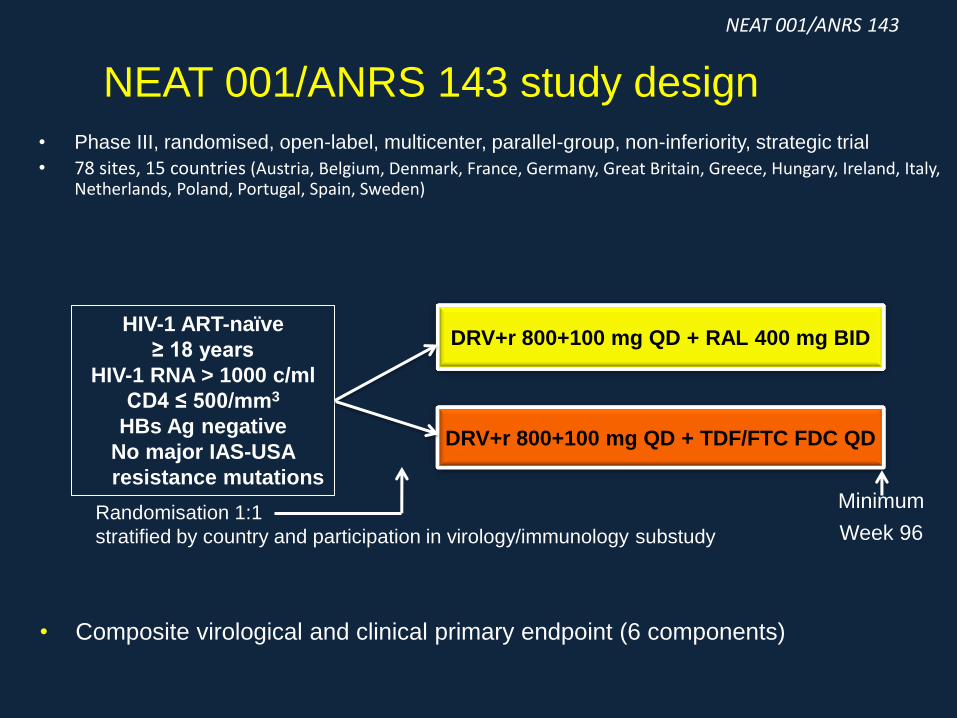
NEAT 001/ANRS 143 study design
• Phase III, randomised, open-label, multicenter, parallel-group, non-inferiority, strategic trial
• 78 sites, 15 countries (Austria, Belgium, Denmark, France, Germany, Great Britain, Greece, Hungary, Ireland, Italy, Netherlands, Poland, Portugal, Spain, Sweden)
DRV+r 800+100 mg QD + TDF/FTC FDC QD
DRV+r 800+100 mg QD + RAL 400 mg BID
Minimum
Week 96 Randomisation 1:1
stratified by country and participation in virology/immunology substudy
HIV-1 ART-naïve
≥ 18 years
HIV-1 RNA > 1000 c/ml
CD4 ≤ 500/mm3
HBs Ag negative
No major IAS-USA
resistance mutations
• Composite virological and clinical primary endpoint (6 components)
NEAT 001/ANRS 143
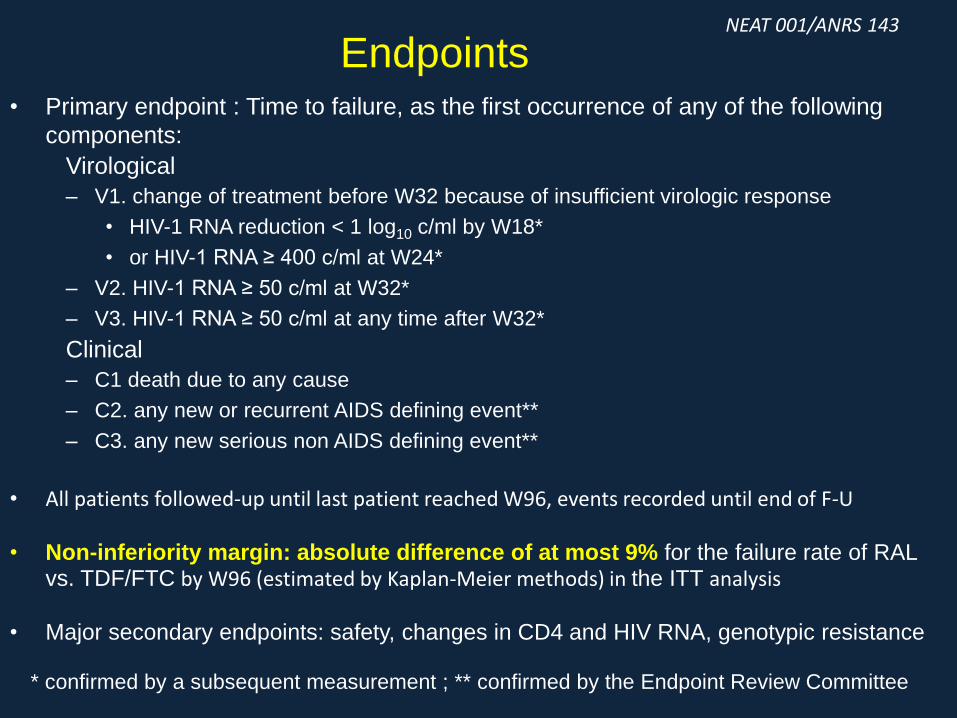
• Primary endpoint : Time to failure, as the first occurrence of any of the following
components:
Virological
– V1. change of treatment before W32 because of insufficient virologic response
• HIV-1 RNA reduction < 1 log10 c/ml by W18*
• or HIV-1 RNA ≥ 400 c/ml at W24*
– V2. HIV-1 RNA ≥ 50 c/ml at W32*
– V3. HIV-1 RNA ≥ 50 c/ml at any time after W32*
Clinical
– C1 death due to any cause
– C2. any new or recurrent AIDS defining event**
– C3. any new serious non AIDS defining event**
• All patients followed-up until last patient reached W96, events recorded until end of F-U
• Non-inferiority margin: absolute difference of at most 9% for the failure rate of RAL vs. TDF/FTC by W96 (estimated by Kaplan-Meier methods) in the ITT analysis
• Major secondary endpoints: safety, changes in CD4 and HIV RNA, genotypic resistance
Endpoints
* confirmed by a subsequent measurement ; ** confirmed by the Endpoint Review Committee
NEAT 001/ANRS 143
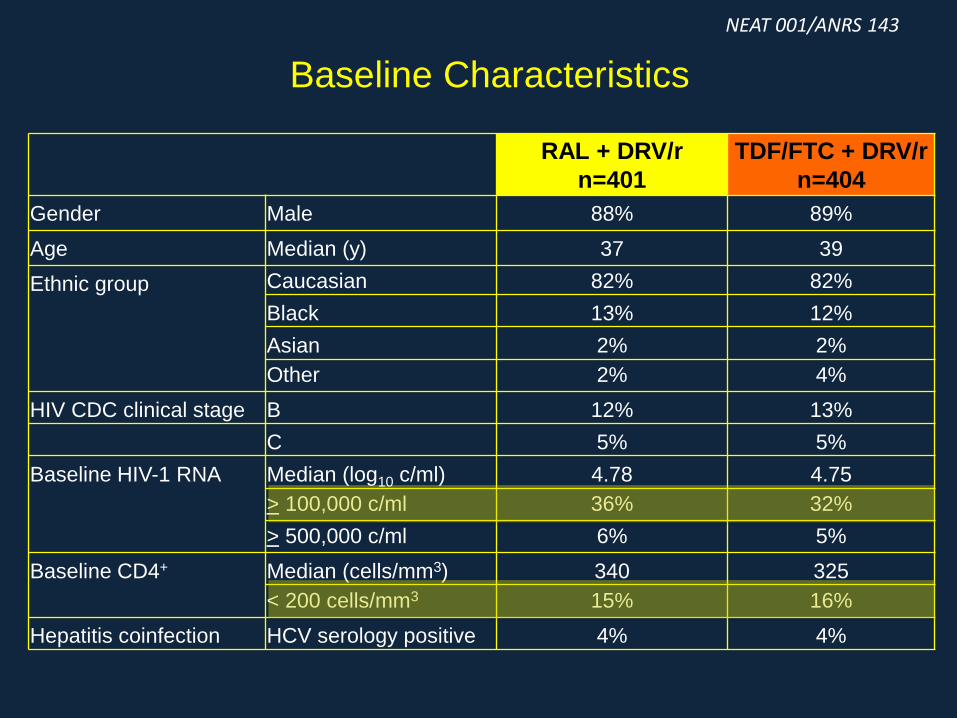
Baseline Characteristics
RAL + DRV/r
n=401
TDF/FTC + DRV/r
n=404
Gender Male 88% 89%
Age Median (y) 37 39
Ethnic group Caucasian 82% 82%
Black 13% 12%
Asian 2% 2%
Other 2% 4%
HIV CDC clinical stage B 12% 13%
C 5% 5%
Baseline HIV-1 RNA Median (log10 c/ml) 4.78 4.75
> 100,000 c/ml 36% 32%
> 500,000 c/ml 6% 5%
Baseline CD4+ Median (cells/mm3) 340 325
< 200 cells/mm3 15% 16%
Hepatitis coinfection HCV serology positive 4% 4%
NEAT 001/ANRS 143
0
0 4 8 12 18 24 32 48 64 80 96
401
404
385
389
377
385
382
387
376
388
356
374
RAL + DRV/r
TDF/FTC + DRV/r
20
40
60
80
100
Weeks
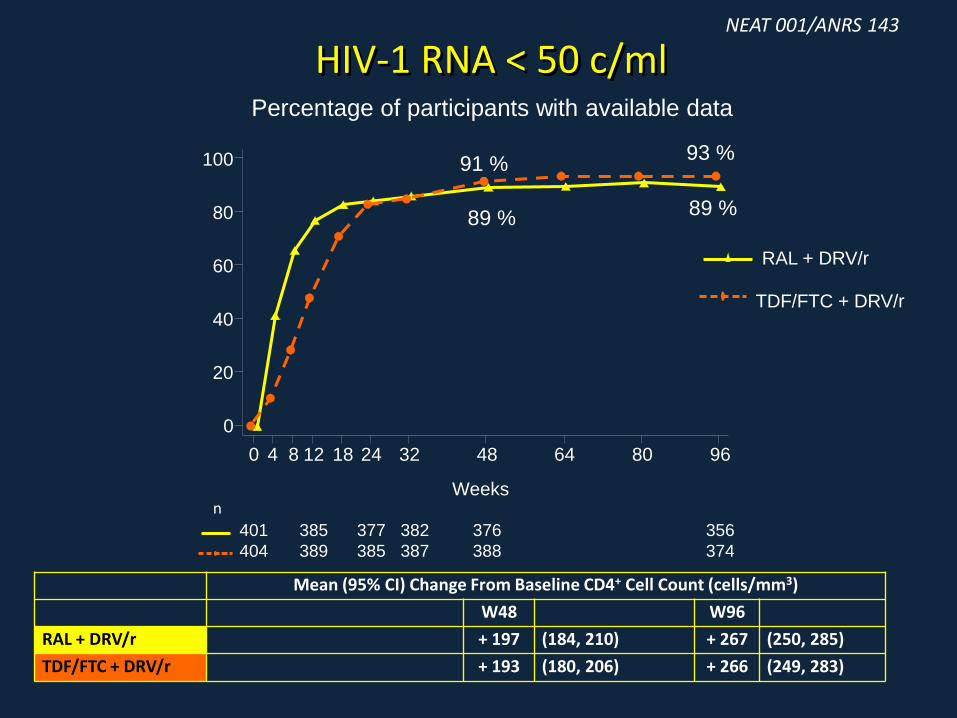
Percentage of participants with available data
89 %
91 % 93 %
89 %
HIV-1 RNA < 50 c/ml
n
Mean (95% CI) Change From Baseline CD4+ Cell Count (cells/mm3)
W48 W96
RAL + DRV/r + 197 (184, 210) + 267 (250, 285)
TDF/FTC + DRV/r + 193 (180, 206) + 266 (249, 283)
NEAT 001/ANRS 143
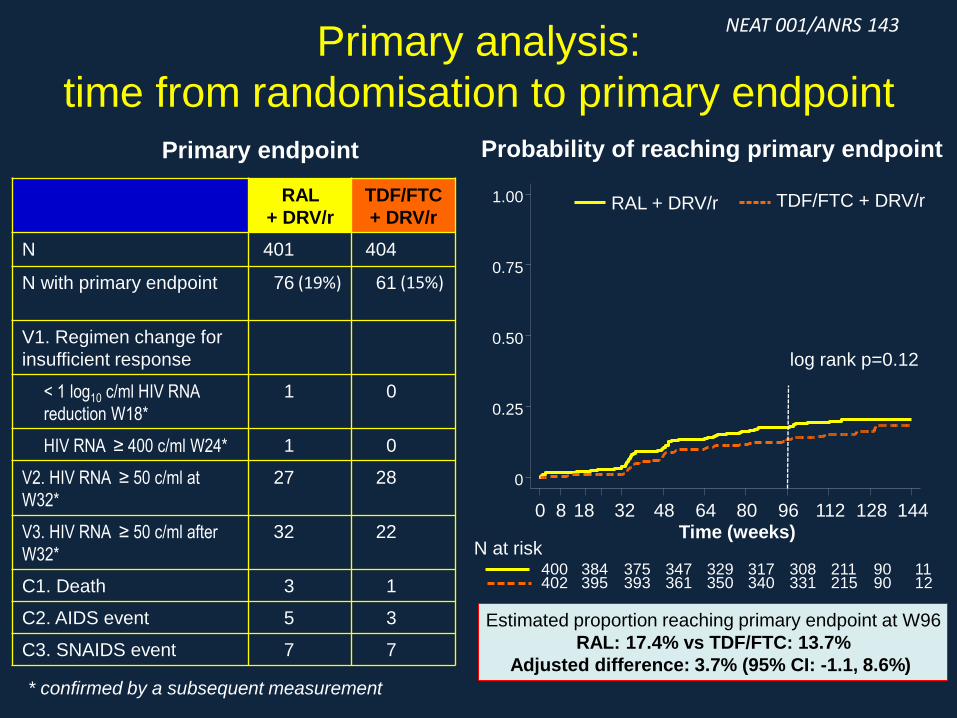
Primary analysis:
time from randomisation to primary endpoint
Primary endpoint
* confirmed by a subsequent measurement
Estimated proportion reaching primary endpoint at W96
RAL: 17.4% vs TDF/FTC: 13.7%
Adjusted difference: 3.7% (95% CI: -1.1, 8.6%)
log rank p=0.12
0
0.25
0.50
0.75
1.00
Probability of reaching primary endpoint
402 395 393 361 350 340 331 215 90 12 400 384 375 347 329 317 308 211 90 11
0 8 18 32 48 64 80 96 112 128 144 Time (weeks)
RAL + DRV/r TDF/FTC + DRV/r
N at risk
NEAT 001/ANRS 143
RAL
+ DRV/r
TDF/FTC
+ DRV/r
N 401 404
N with primary endpoint 76 (19%) 61 (15%)
V1. Regimen change for
insufficient response
< 1 log10 c/ml HIV RNA
reduction W18*
1 0
HIV RNA ≥ 400 c/ml W24* 1 0
V2. HIV RNA ≥ 50 c/ml at
W32*
27 28
V3. HIV RNA ≥ 50 c/ml after
W32*
32 22
C1. Death 3 1
C2. AIDS event 5 3
C3. SNAIDS event 7 7
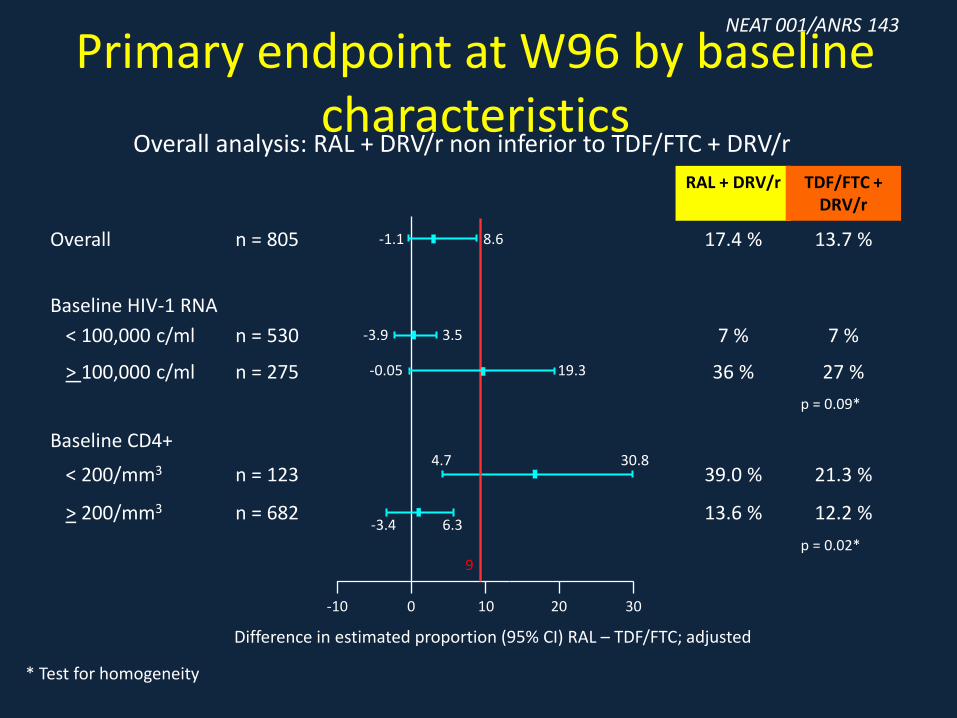
Overall analysis: RAL + DRV/r non inferior to TDF/FTC + DRV/r
Primary endpoint at W96 by baseline characteristics
n = 805
n = 530
n = 275
n = 123
n = 682
Overall
< 100,000 c/ml
> 100,000 c/ml
< 200/mm3
> 200/mm3
Baseline HIV-1 RNA
Baseline CD4+
17.4 %
7 %
36 %
39.0 %
13.6 %
13.7 %
7 %
27 %
21.3 %
12.2 %
RAL + DRV/r TDF/FTC + DRV/r
10 0 -10 20 30
9
Difference in estimated proportion (95% CI) RAL – TDF/FTC; adjusted
* Test for homogeneity
p = 0.09*
p = 0.02*
-1.1 8.6
-3.9 3.5
-0.05 19.3
4.7 30.8
-3.4 6.3
NEAT 001/ANRS 143
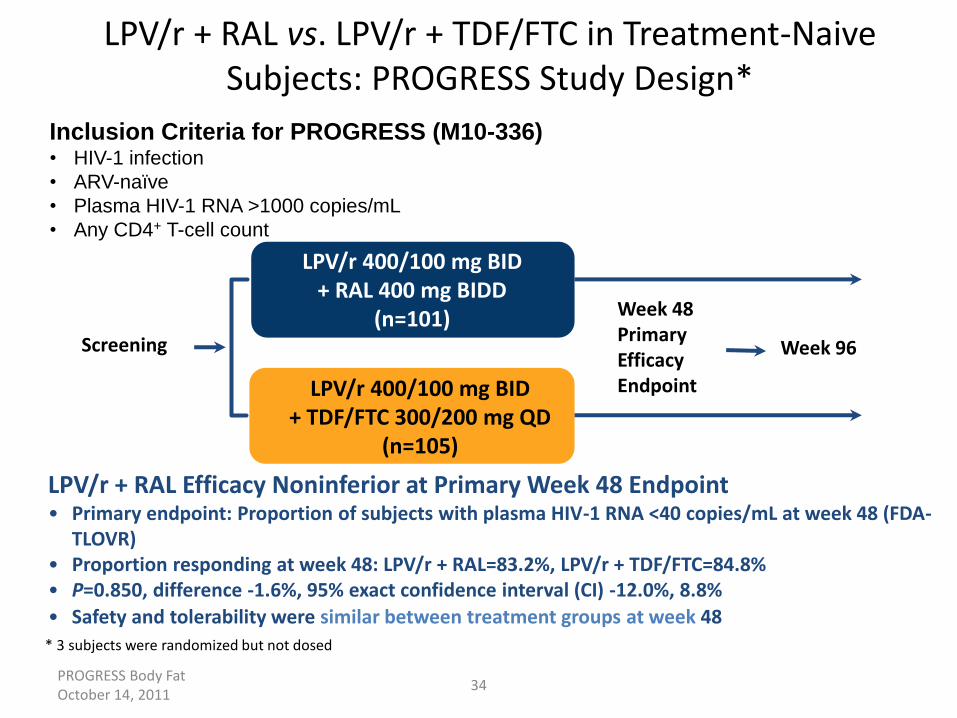
PROGRESS Body Fat October 14, 2011
34
LPV/r + RAL vs. LPV/r + TDF/FTC in Treatment-Naive Subjects: PROGRESS Study Design*
LPV/r + RAL Efficacy Noninferior at Primary Week 48 Endpoint • Primary endpoint: Proportion of subjects with plasma HIV-1 RNA <40 copies/mL at week 48 (FDA-
TLOVR) • Proportion responding at week 48: LPV/r + RAL=83.2%, LPV/r + TDF/FTC=84.8% • P=0.850, difference -1.6%, 95% exact confidence interval (CI) -12.0%, 8.8%
• Safety and tolerability were similar between treatment groups at week 48
LPV/r 400/100 mg BID + TDF/FTC 300/200 mg QD
(n=105)
Inclusion Criteria for PROGRESS (M10-336) • HIV-1 infection
• ARV-naïve
• Plasma HIV-1 RNA >1000 copies/mL
• Any CD4+ T-cell count
Screening Week 96
Week 48 Primary Efficacy Endpoint
* 3 subjects were randomized but not dosed
LPV/r 400/100 mg BID + RAL 400 mg BIDD
(n=101)
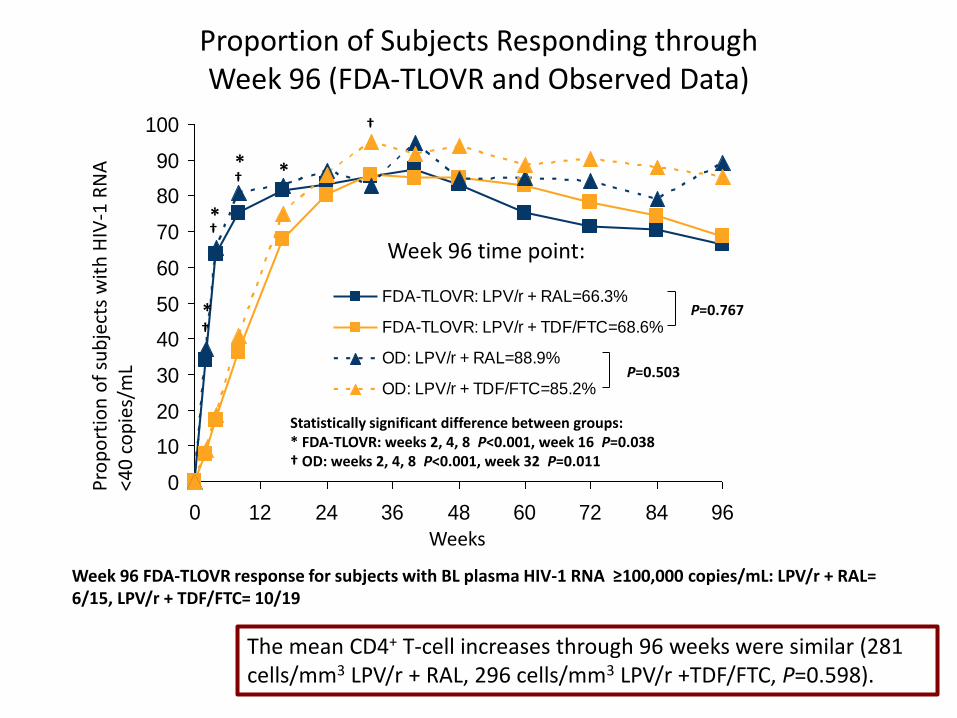
Proportion of Subjects Responding through Week 96 (FDA-TLOVR and Observed Data)
Pro
po
rtio
n o
f su
bje
cts
wit
h H
IV-1
RN
A
<40
co
pie
s/m
L
0
10
20
30
40
50
60
70
80
90
100
0 12 24 36 48 60 72 84 96
FDA-TLOVR: LPV/r + RAL=66.3%
FDA-TLOVR: LPV/r + TDF/FTC=68.6%
OD: LPV/r + RAL=88.9%
OD: LPV/r + TDF/FTC=85.2%
Week 96 time point:
Statistically significant difference between groups: * FDA-TLOVR: weeks 2, 4, 8 P<0.001, week 16 P=0.038 † OD: weeks 2, 4, 8 P<0.001, week 32 P=0.011
*
*
* *
†
†
†
†
P=0.767
P=0.503
Weeks
The mean CD4+ T-cell increases through 96 weeks were similar (281 cells/mm3 LPV/r + RAL, 296 cells/mm3 LPV/r +TDF/FTC, P=0.598).
Week 96 FDA-TLOVR response for subjects with BL plasma HIV-1 RNA ≥100,000 copies/mL: LPV/r + RAL= 6/15, LPV/r + TDF/FTC= 10/19
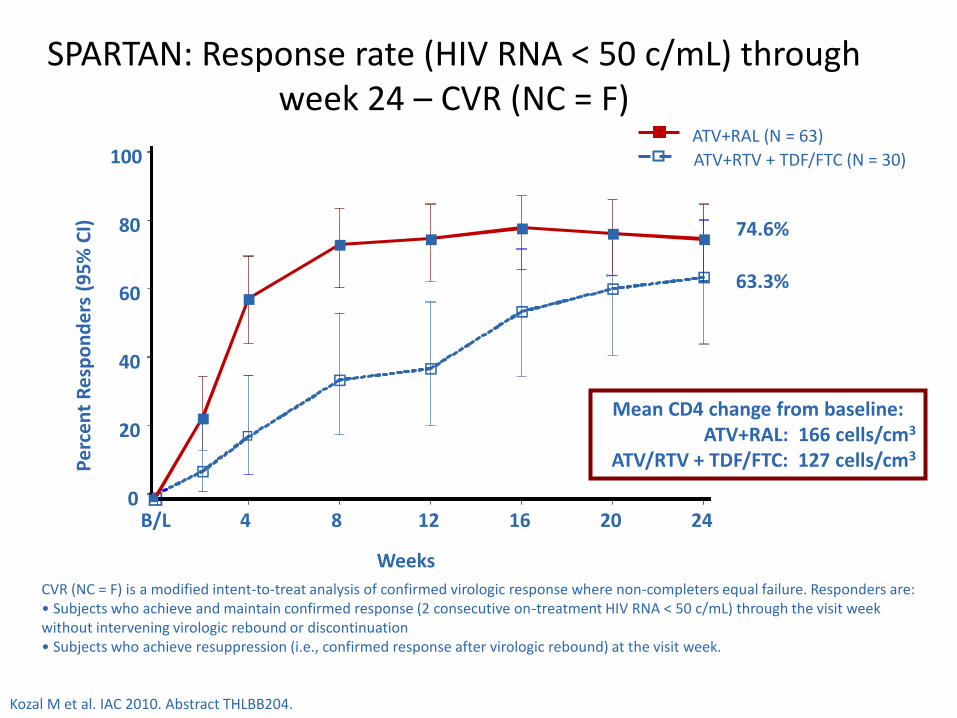
SPARTAN: Response rate (HIV RNA < 50 c/mL) through week 24 – CVR (NC = F)
CVR (NC = F) is a modified intent-to-treat analysis of confirmed virologic response where non-completers equal failure. Responders are: • Subjects who achieve and maintain confirmed response (2 consecutive on-treatment HIV RNA < 50 c/mL) through the visit week without intervening virologic rebound or discontinuation • Subjects who achieve resuppression (i.e., confirmed response after virologic rebound) at the visit week.
o
Weeks
o
o
n 0
20
40
60
80
100
B/L 4 8 12 16 20 24
n
n
n n n
n n
o
o o
o
o
Pe
rce
nt
Re
spo
nd
ers
(9
5%
CI)
74.6%
63.3%
Mean CD4 change from baseline: ATV+RAL: 166 cells/cm3
ATV/RTV + TDF/FTC: 127 cells/cm3
ATV+RTV + TDF/FTC (N = 30)
ATV+RAL (N = 63)
Kozal M et al. IAC 2010. Abstract THLBB204.
IMPLICAZIONI
• I risultati dello studio GARDEL rafforzano l’opinione che, in presenza di elevati / ottimali livelli di aderenza, il desiderato risultato immunovirologico sia ottenibile anche con l’impiego di regimi non convenzionali, ovvero caratterizzati da un minore numero di farmaci
• Lo studio GARDEL conferma, con coordinate di valutazione decisamente superiori, e con risultati di vertice, il valore di LPV/r bid nelle strategie LDR
• Lo studio GARDEL genera una ragionevole curiosità sull’ipotetico esito di precedenti tentativi infruttuosi (e.g. MonarK) nel caso anzichè esser basati sulla monoterapia con LPV/r si fossero dotati del 3TC bid
• Benchè una tale strategia fin dall’inizio possa trovare un’accoglienza limitata, quando
proiettata in un maggiormente prudente schema di induzione – mantenimento, ha il potenziale di modificare l’opinione di un buon numero di scettici a proposito delle opzioni LDR
• Il rispetto di determinati valori relativi a parametri individuali già determinati in precedenti studi di LDR costituisce un’ulteriore nota di riferimento prudenziale

Acknowledgments
THE UNIVERSITY
of LIVERPOOL
TORINO:
Stefano Bonora
Antonio D’Avolio
Mauro Sciandra
Lorena Baietto
Cristina Tettoni
Sabrina Audagnotto
Letizia Marinaro
Margherita Bracchi
Laura Trentini
Andrea Calcagno
Marco Simiele
Anna Lucchini
Filippo Lipani
Roberto Bertucci
Agostino Maiello
Bernardino Salassa
Francesco G. De Rosa
Chiara Montrucchio
Chiara Alcantarini
Chiara Cardellino
Paolo Bigliano
Lucio Boglione
Micol Ferrara
Ilaria Motta
Nicole Pagani
Francesca Patti
Amedeo De Nicolò
LIVERPOOL:
David Back
Saye Khoo
Andy Owen
Marco Siccardi
LONDON:
Marta Boffito
Anton Pozniak
ROMA:
Andrea Antinori
Emanuele Nicastri
Giuseppe Ippolito