Embed Size (px)
Citation preview

CASE REPORT
Successful treatment of small cell variant anaplastic large celllymphoma with allogeneic peripheral blood stem celltransplantation, and review of the literature
Rie Imamura • Fumihiko Mouri • Kei Nomura • Takayuki Nakamura • Eijiro Oku •
Satoshi Morishige • Yuka Takata • Ritsuko Seki • Koichi Osaki • Michitoshi Hashiguchi •
Koji Yoshimoto • Koichi Ohshima • Koji Nagafuji • Takashi Okamura
Received: 31 August 2012 / Revised: 4 December 2012 / Accepted: 4 December 2012 / Published online: 20 December 2012
� The Japanese Society of Hematology 2012
Abstract The small cell variant of anaplastic large cell
lymphoma (ALCL) presents in a nearly identical manner to
the more common ALK? primary ALCL, with the exception
that it is more frequently associated with leukemic involve-
ment, and the prognosis has been reported to be poor. We
report a 40-year-old Japanese male who was diagnosed with
small cell variant ALCL with peripheral blood involvement
stage IVB, age-adjusted international prognostic index 3.
Conventional cytogenetics of the bone marrow aspirate
specimen showed abnormal metaphases with the following
karyotype: 47, XY, ?X, t(2;5)(p23;q35). The patient was
treated with acute lymphoblastic leukemia-oriented intensive
chemotherapy. He underwent allogeneic peripheral blood
stem cell transplantation from his HLA-DR1 locus mismatch
sister. Prior to transplant, the patient had residual lymphad-
enopathy considered to be in partial remission. As of August
2012, the patient has achieved 18 months of continuous
complete remission (CCR), with a Karnofsky score of 100 %.
We have identified a total of seven cases of small cell variant
ALCL treated with allogeneic hematopoietic stem cell
transplantation (HSCT) in the literature. Of these, no relapse
was reported, and four patients were CCR more than 1 year.
Allogeneic HSCT appears to represent a promising treatment
option for small cell variant ALCL.
Keywords Anaplastic large cell lymphoma � Small cell
variant � ALK � Allogeneic � Transplantation
Introduction
Anaplastic large cell lymphoma (ALCL), a subgroup of
non-Hodgkin’s lymphoma with expression of CD30 (Ki-1),
was first described in 1985 by Stein et al. [1]. Anaplastic
lymphoma kinase (ALK) expression exists in approxi-
mately 60 % of ALCL cases [2]. Compared with the ALK-
negative cases, ALK-positive cases are usually character-
ized by younger age, an advanced stage, more systemic
symptoms, more extranodal involvement at presentation, a
good response to chemotherapy, and a good prognosis
[3, 4].
Among subentities of ALCL, small cell variant was first
reported by Kinney et al. [5] in 1993. The small cell variant
of ALCL presents nearly identically to the ALK-positive
primary ALCL, with the exception that leukemic involve-
ment has been more commonly described in the small cell
variant [6]. The prognosis of small cell variant of ALCL
has been reported to be poor [5, 7, 8].
Here, we report a case of small cell variant ALCL
successfully treated with allogeneic peripheral blood stem
cell transplantation, and review the literature on allogeneic
hematopoietic stem cell transplantation (HSCT) for small
cell variant ALCL.
Case report
A 40-year-old Japanese male was admitted to our hospital
because of fever, lymphadenopathy, and elevated white
blood cell count without body weight loss or night sweat in
R. Imamura � F. Mouri � K. Nomura � T. Nakamura � E. Oku �S. Morishige � Y. Takata � R. Seki � K. Osaki �M. Hashiguchi � K. Yoshimoto � K. Nagafuji (&) � T. Okamura
Division of Hematology and Oncology,
Department of Medicine, Kurume University School
of Medicine, 67 Asahi-machi, Kurume 830-0011, Japan
e-mail: [email protected]
K. Ohshima
Department of Pathology, Kurume University School
of Medicine, 67 Asahi-machi, Kurume 830-0011, Japan
123
Int J Hematol (2013) 97:139–143
DOI 10.1007/s12185-012-1242-3

October 2010. His performance status was 2. Physical
examination revealed enlarged left cervical, bilateral axil-
lary, and bilateral inguinal lymphadenopathy with hepato-
splenomegaly. Imaging study revealed bilateral pleural
effusion. A complete blood count showed leukocytosis of
34.0 9 109/L with 31 % abnormal lymphoid cells consist-
ing of a mixture of small, markedly atypical lymphoid cells
and large lymphoma cells. These cells were basophilic and
had variations in size and nuclear shape, and some cells had
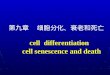
vacuolated cytoplasm (Fig. 1). The serum lactate dehy-
drogenase concentration was 1910 IU/l (normal range
119–229 IU/l), and the serum soluble interleukin-2 receptor
concentration was markedly elevated to 147015 U/ml
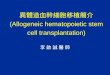
(normal range \466 U/ml). Bone marrow aspiration and
biopsy revealed hypercellular marrow with 10 % abnormal
lymphoid cells (Fig. 2a). Immunohistochemistry performed
on the bone marrow aspirate clot specimen showed that the
cells were positive for ALK-1, CD30, and EMA. The CD30
pattern of expression was membranous and paranuclear
(Fig. 2b). The pattern of ALK-1 was nuclear and cyto-
plasmic (Fig. 2c). Flow cytometric analysis showed
abnormal population of cells positive for CD2, cytoplasmic
CD3, CD4, CD7, CD25, CD30, and negative for CD8,
CD56, CD16, CD20, cytoplasmic CD79a, myeloperoxi-
dase, CD34, TdT. Conventional cytogenetics of the bone
marrow aspirate specimen showed 3 normal and 17
abnormal metaphases with the following karyotype: 47,
XY, ?X, t(2;5)(p23;q35). Fluorescence in situ hybridiza-
tion showed disruption of the ALK gene on 2p23. The
patient was diagnosed with ALK-positive ALCL small cell
variant with leukemic peripheral blood involvement, stage
IVB, with age-adjusted international prognostic index
(AA-IPI) 3. The patient received induction chemotherapy
for acute lymphoblastic leukemia (ALL). The patient
achieved hematologic complete remission with partial
remission (PR) status of lymphadenopathy, while menin-
geal invasion developed at the end of induction therapy. The
analysis of cerebrospinal fluid revealed increased
Fig. 1 Peripheral blood smear (91000) showing many small-/
intermediate-sized atypical lymphoid cells and large and atypical
lymphoid cells with basophilic and vacuolated cytoplasm
Fig. 2 a Bone marrow biopsy revealed hypercellular marrow with
10 % abnormal lymphoid cells (9400). b The large cells expressed
CD30 antigen in a cytoplasmic membrane and Golgi distribution
(9400). c The large cells expressed ALK in a cytoplasm and nucleus
distribution (9400)
140 R. Imamura et al.
123

concentration of protein (125 mg/dl) and cell numbers
(26 9 106/L) showing atypical cells consisted with lym-
phoma. Central nervous system (CNS) invasion was suc-
cessfully treated with intrathecal methotrexate in addition to
high-dose methotrexate and high-dose cytarabine. After
three courses of consolidation therapy, the patient under-
went allogeneic peripheral blood stem cell transplantation
from his HLA-DR 1 locus mismatch sister in February
2011. The interval from initial diagnosis to transplant was
5 months. Prior to transplant, the patient had residual
lymphadenopathy considered to be PR status while the bone
marrow examination revealed no residual lymphoma cells.
The patient then received a conditioning regimen con-
sisting of total body irradiation (12 Gy in 6 fractions on days
-8 to -6), etoposide (12.5 mg/kg on days -5 to -4), and
cyclophosphamide (60 mg/kg on days -3 to -2) [9]. The
numbers of infused cells and CD34 positive cells were
30.4 9 107/kg and 4.1 9 106/kg, respectively. Graft-ver-
sus-host disease (GVHD) prophylaxis consisted of intrave-
nous cyclosporin (3 mg/kg/day) beginning on day -1 and
short-term methotrexate on days 1 (10 mg/m2), 3 (7 mg/
m2), 6 (7 mg/m2), and 11 (7 mg/m2). Rapid engraftment was
obtained. A neutrophil count [0.5 9 109/L and a platelet
count [20 9 109/L were achieved on days 10 and 15,
respectively, and complete donor chimerism was observed
in a bone marrow sample on day 28. Grade II acute GVHD
that developed was successfully treated with 2 mg/kg of
methyl-prednisolone. CT scan on day 40 revealed complete
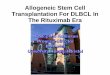
disappearance of lymphadenopathy. As of August 2012, the
patient had achieved 18 months of continuous complete
remission (CCR) with Karnofsky score of 100 % (Fig. 3).
Discussion
In 1995, Shiota et al. [3] first reported that ALK-positive
ALCL patients have a better prognosis than those who are
ALK-negative, reporting 5-year overall survival (OS) of
79.8 versus 32.9 %. This observation was confirmed in 2
large series of ALCL patients [2, 10]. Thus, anthracycline-
based chemotherapy is recommended for the initial treat-
ment for ALK-positive ALCL patients. Good prognosis
patients (AA-IPI 0–1) had a 10-year OS of 94 % com-
pared with 41 % in patients with AA-IPI 2–3 [2]. Prog-
nosis is so good in this group of patients that autologous
HSCT should only be considered in case of relapse. ALCL
patients autografted at relapse have a 78–100 % 3-year OS
[11–13].
Small cell variant ALCL, first reported by Kinney et al.
[5] in 1993, is characterized by a mixture of small, medium-
sized, and large anaplastic cells positive for CD30 and ALK
[14]. Most patients are young at presentation, with a median
age of 14 years (range 4 months–40 years). Sites of
involvement frequently include peripheral blood, peripheral
lymph nodes, and skin. Most patients present with consti-
tutional symptoms, often with stage III/IV. The prognosis
of small cell variant ALCL has been reported to be poor
[5, 7, 8]. ALCL99 study analyzed 375 child patients with
ALK-positive ALCL. Among them, 22 patients (6 %) were
classified as small cell variant, and the hazard ratio for
failure was 4.7 (95 % CI 2.6–8.5) in patients with small
cell ALCL relative to the common type [15]. Indeed,
ALK-positive ALCL with leukemic involvement, most of
which cases are small cell variant, is reported to be a
0
500
1000
1500
2000Induction HD-
AraCHD-MTX
Abnormal cell 10.0% 0% 0% 0%
t(2;5) 85%46,XY 15%
Karyotype 46,XY 100%
46,XY 100%
XY-FISH XX 99.6%
IT MTX
Bone Marrow
TBI/VP16/CY
AllogeneicPBSCT
CSF cell count 26/µL 3/µL 0/µL
LDH
sIL2R147015 U/ml 755 U/ml 1522 U/ml 527 U/ml 765 U/ml 677 U/ml
LDH ( U/L )
HD-AraC
Oct.2010 Nov. Dec. Jan. 2011 Feb. Mar.
0%
IT MTX IT MTXFig. 3 Clinical course. HDhigh-dose, AraC cytarabine,
MTX methotrexate, CSFcerebrospinal fluid, TBI total
body irradiation, VP-16etoposide, CYcyclophosphamide, PBSCTperipheral blood stem cell
transplantation
Successful treatment of small cell variant ALCL 141
123

clinicopathologic entity with an unfavorable prognosis [8].
This proposal was supported by Nguyen et al. [16]. The
authors reviewed 21 cases of ALCL with leukemic pre-
sentation: of these, 18 were small cell variant, and 13 of
them died of the disease, usually within a few months, and
only one case had CCR after completion of chemotherapy.
Our patient was diagnosed with ALK-positive ALCL
small cell variant with leukemic peripheral blood
involvement, and was treated aggressively with ALL-
directed chemotherapy, resulting in PR status. Meningeal
infiltration was successfully treated with systemic and
intrathecal chemotherapy. Because of reported poor prog-
nosis of small cell variant ALCL with leukemic presenta-
tion, the patient was preceded to allogeneic PBSCT from
HLA-DR 1 locus mismatched related donor, and has since
been enjoying over 18 months CCR.
The role of allogeneic HSCT for ALCL has been eval-
uated in several reports. Berlin-Frankfurt-Munster group
reported 20 children and adolescents with high-risk relapsed
or refractory ALCL who underwent allogeneic HSCT, with
disease status at transplantation of 12 complete remission
(CR), 3 PR, 3 active disease, and 2 not evaluable. Three-
year event-free survival (EFS) was 75 ± 10 % [17].
Societe Francaise de Greffe de Moelle et de Therapie
Cellulaire reported a retrospective analysis including 27
adult ALCL patients who underwent allogeneic HSCT, with
disease status at transplantation of 10 CR, 6 PR, and 11
stable disease (SD)/progressive disease (PD). The 5-year
OS was 55 % (95 % CI 35–72 %) [18]. Dodero et al. [19]
reported 11 cases of reduced-intensity conditioning
allogeneic HSCT for relapsed ALCL, with 5-year OS 54 %
(95 % CI 23–70 %).
These data clearly show that allogeneic HSCT is an
effective therapy for advanced ALCL, suggesting a graft-
versus-ALCL effect. However, because of a lack of
detailed pathological information, we cannot identify cases
of small cell variant ALCL in these reports.
We have identified a total of 7 cases of small cell variant
ALCL treated with allogeneic HSCT, presented in Table 1
[8, 16, 20–22]. Disease status prior to transplantation was 1
1CR, 1 2CR, 2 1PR, 2 refractory. Among them, no relapse
was reported, and 4 patients were CCR more than 1 year.
Thus, allogeneic HSCT seems to be a promising treatment
option for small cell variant ALCL.
In conclusion, we report a small cell variant ALK-
positive ALCL adult patient with disease status 1PR suc-
cessfully treated with allogeneic HSCT. Because of lack of
more detailed information, there is a possibility that some
reports of allogeneic HSCT for ALCL might include cases
of small cell variant ALCL. More accumulation of case
records would help to evaluate the role of allogeneic HSCT
for small cell variant ALCL.
Conflict of interest None.
References
1. Stein H, Mason DY, Gerdes J, et al. The expression of the
Hodgkin’s disease associated antigen Ki-1 in reactive and neo-
plastic lymphoid tissue: evidence that Reed–Sternberg cells and
Table 1 Reported cases of allogeneic hematopoietic stem cell transplantation for small cell variant anaplastic large cell lymphoma
Patient Age/sex Primary location WBC count
(9109/L)
Lymphoma
cell in PB (%)
Disease status at
transplantation
Transplantation Follow-up References
1 18/F LN, skin, BM 15 54 2CR R-SCT CCR
18 months
7
2 20 months/F LN, BM, liver,
spleen
37.9 65 1 relapse R-SCT Died within
few months
7
3 6/F Lung, kidney, BM 204 51 Primary
refractory
Haplo-SCT CCR
17 months
15
4 16/M LN, lung, skin,
liver, spleen
NA NA 1CR U-BMT CCR
39 months
19
5 29/M LN, BM, liver,
spleen, pleura,
CNS
47.9 19 1PR U-BMT Died of
GVHD
1 month
20
6 23/F LN, BM, liver,
spleen, pleura,
skin
24.5 5.5 1 relapse HSCT Unknown 21
7 40/M LN, BM, liver,
spleen, pleura
34 31 1PR R-PBSCT CCR
18 months
This case
report
LN lymph node, BM bone marrow, CNS central nervous system, WBC white blood cell, PB peripheral blood, CR complete remission, PR partial
remission, R-SCT stem cell tranplatation from related donor, haplo-SCT SCT from haploidentical related donor, U-BMT bone marrow trans-
plantation from unrelated donor, HSCT hematopoietic stem cell transplantation, R-PBSCT peripheral blood stem cell transplantation from related
donor, CCR continuous complete remission, GVHD graft-versus-host disease
142 R. Imamura et al.
123

histiocytic malignancies are derived from activated lymphoid
cells. Blood. 1985;66:848–58.
2. Falini B, Pileri S, Zinzani PL, et al. ALK? lymphoma: clinico-
pathological findings and outcome. Blood. 1999;93:2697–706.
3. Shiota M, Nakamura S, Ichinohasama R, et al. Anaplastic large
cell lymphomas expressing the novel chimeric protein p80NPM/
ALK: a distinct clinicopathologic entity. Blood. 1995;86:
1954–60.
4. Savage KJ, Harris NL, Vose JM, et al. ALK- anaplastic large-
cell lymphoma is clinically and immunophenotypically different
from both ALK? ALCL and peripheral T-cell lymphoma, not
otherwise specified: report from the International Peripheral
T-Cell Lymphoma Project. Blood. 2008;111:5496–504.
5. Kinney MC, Collins RD, Greer JP, Whitlock JA, Sioutos N,
Kadin ME. A small-cell-predominant variant of primary Ki-1
(CD30)? T-cell lymphoma. Am J Surg Pathol. 1993;17:859–68.
6. Summers TA, Moncur JT. The small cell variant of anaplastic
large cell lymphoma. Arch Pathol Lab Med. 2010;134:1706–10.
7. Lesesve J-F, Buisine J, Gregoire M-J, et al. Leukaemic small cell
variant anaplastic large cell lymphoma during pregnancy. Clin
Lab Haematol. 2000;22:297–301.
8. Onciu M, Behm FG, Raimondi SC, et al. ALK-positive anaplastic
large cell lymphoma with leukemic peripheral blood involvement
is a clinicopathologic entity with an unfavorable prognosis.
Report of three cases and review of the literature. Am J Clin
Pathol. 2003;120:617–25.
9. Shigematsu A, Kondo T, Yamamoto S, et al. Excellent outcome
of allogeneic hematopoietic stem cell transplantation using a
conditioning regimen with medium-dose VP-16, cyclophospha-
mide and total-body irradiation for adult patients with acute
lymphoblastic leukemia. Biol Blood Marrow Transpl. 2008;
14:568–75.
10. Gascoyne RD, Aoun P, Wu D, et al. Prognostic significance of
anaplastic lymphoma kinase (ALK) protein expression in adults
with anaplastic large cell lymphoma. Blood. 1999;93:3913–21.
11. Blystad AK, Enblad G, Kvaloy S, et al. High-dose therapy with
autologous stem cell transplantation in patients with peripheral T
cell lymphomas. Bone Marrow Transpl. 2001;27:711–6.
12. Song KW, Mollee P, Keating A, Crump M. Autologous stem cell
transplant for relapsed and refractory peripheral T-cell lym-
phoma: variable outcome according to pathological subtype. Br J
Haematol. 2003;120:978–85.
13. Jagasia M, Morgan D, Goodman S, et al. Histology impacts the
outcome of peripheral T-cell lymphomas after high dose che-
motherapy and stem cell transplant. Leuk Lymphoma. 2004;45:
2261–7.
14. Stein H, Foss HD, Durkop H, et al. CD30(?) anaplastic large cell
lymphoma: a review of its histopathologic, genetic, and clinical
features. Blood. 2000;96:3681–95.
15. Lamant L, McCarthy K, d’Amore E, et al. Prognostic impact of
morphologic and phenotypic features of childhood ALK-positive
anaplastic large-cell lymphoma: results of the ALCL99 Study.
J Clin Oncol. 2011;29:4669–76.
16. Nguyen JT, Condron MR, Nguyen ND, De J, Medeiros LJ,
Padula A. Anaplastic large cell lymphoma in leukemic phase:
extraordinarily high white blood cell count. Pathol Int. 2009;
59:345–53.
17. Woessmann W, Peters C, Lenhard M, et al. Allogeneic haema-
topoietic stem cell transplantation in relapsed or refractory ana-
plastic large cell lymphoma of children and adolescents—a
Berlin-Frankfurt-Munster group report. Br J Haematol.
2006;133:176–82.
18. Le Gouill S, Milpied N, Buzyn A, et al. Graft-versus-lymphoma
effect for aggressive T-cell lymphomas in adults: a study by the
Societe Francaise de Greffe de Moelle et de Therapie Cellulaire.
J Clin Oncol. 2008;26:2264–71.
19. Dodero A, Spina F, Narni F, et al. Allogeneic transplantation
following a reduced-intensity conditioning regimen in relapsed/
refractory peripheral T-cell lymphomas: long-term remissions
and response to donor lymphocyte infusions support the role of a
graft-versus-lymphoma effect. Leukemia. 2012;26:520–6.
20. Bayle C, Charpentier A, Duchayne E, et al. Leukaemic presen-
tation of small cell variant anaplastic large cell lymphoma: report
of four cases. Br J Haematol. 1999;104:680–8.
21. Cesaro S, Pillon M, Visintin G, et al. Unrelated bone marrow
transplantation for high-risk anaplastic large cell lymphoma in
pediatric patients: a single center case series. Eur J Haematol.
2005;75:22–6.
22. Grewal JS, Smith LB, Winegarden JD 3rd, Krauss JC, Tworek
JA, Schnitzer B. Highly aggressive ALK-positive anaplastic large
cell lymphoma with a leukemic phase and multi-organ involve-
ment: a report of three cases and a review of the literature. Ann
Hematol. 2007;86:499–508.
Successful treatment of small cell variant ALCL 143
123










![Casusbespreking Tilburg - pathology.nl...2017/04/28 · Dropbox CytologyStuff.com- Gyn G Google ETZ- 8300-01 WV Screene... e:] Mantel Cel Lymfoom (MC... Google anaplastic large cell](https://img.pdfslide.tips/doc/110x75/60a92ad4247078370c3f1f2e/casusbespreking-tilburg-20170428-dropbox-cytologystuffcom-gyn-g-google.jpg)