Embed Size (px)
Citation preview

CONTENTS
Case Report
127輔仁醫學期刊 第 16卷 第 3期 2018
Superior mesenteric artery syndrome: an unusual cause of intestinal obstruction
Ta-Pin Lee1,*, Wen-Chih Huang2,3
ABSTRACT
Superior mesenteric artery (SMA) syndrome is a condition arising from the compres-sion of the duodenum between the SMA and the aorta and subsequently causing bowel obstruction. Its initial management is usually conservative with nutritional support. Surgical intervention is indicated when conservative management fails. We report a case with SMA syndrome and episodes of intestinal obstruction, which was successfully treated by duodeno-jejunostomy.
Keywords: superior mesenteric artery syndrome, superior mesenteric artery, intestinal obstruction
1 Department of Radiology, Wei-Gong Memorial Hospital, Miaoli, Taiwan2 Department of Anatomic Pathology, Far Eastern Memorial Hospital, New Taipei, Taiwan3 College of Nursing, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan* Corresponding author: Ta-Pin Lee E-mail: [email protected]
INTRODUCTION
The SMA syndrome is a rare cause of intes-tinal obstruction. It is characterized by extrinsic compression of the third portion of the duodenum by narrowing of the aortomesenteric angle that is primarily attributed to loss of the intervening mesenteric fat [1]. This unusual illness was first re-ported by Von Rokitanski and has been known as Wilkie Syndrome, the author who published the largest series of cases in 1927 [2]. It usually oc-curs in thin and young females, and often caused by weight loss due to harsh dieting or a eating dis-
order. Because the symptoms can include nausea and early satiety, it is important and necessary to take a recent history, especially of weight loss. The final diagnosis rests on abdominal comput-ed tomography, which confirms a decrease of an angle between the superior mesenteric artery and the abdominal aorta. We believe this article would be helpful for the education of the young medical staff.
CASE REPORT
This 24-year-old woman presented with inter-mittent dull pain in the lower abdomen for about
DOI 10.3966/181020932018091603003

CONTENTS
Fu-Jen Journal of Medicine Vol.16 No.3 2018128
Ta-Pin Lee Wen-Chih Huang
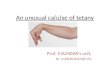
three months. She was slim, her body weight was 42 kilograms, and she denied significant weight loss, major illness or trauma before com-ing for consult. She had visited the local hospital and diagnostic laparotomy yielded inconclusive findings. The symptom persisted and eventually progressed to frequent episodes of diffuse abdomi-nal discomfort, especially in the epigastric region. Postprandial discomfort was also reported. Nausea and vomiting were usually presented two hours af-ter meals. Physical examination revealed epigastric tenderness. Upper gastrointestinal panendoscopy disclosed superficial gastritis. Upper gastrointes-tinal radiography with a barium meal ingestion showed compression of the third portion of du-odenum with delay in contrast passage (Figure 1). Subsequent abdominal computed tomogra-phy demonstrated compression at the third part of the duodenum and an acute angle (13 degrees) be-tween the superior mesenteric artery and the aorta, suggesting SMA syndrome (Figures 2 and 3). To-tal parenteral nutrition was given in the interim for nutrition support. The abdominal discom-fort remained despite the treatment, and surgical intervention was indicated. An open duodenojeju-nostomy was carried out thereafter. Her physical condition improved gradually after the operation and she was discharged without any complication.
DISCUSSION
The cause of superior mesenteric artery syndrome is stark weight loss due to various condi-tions such as malignancy, bariatric surgery, trauma, chronic infections, severe burns, etc. Young and thin females like our subject, are also predisposed to the illness. Reduction in the mesenteric fat tissue
Figure 3. Sagittal reformatted abdominal computed to-mography showed an angle of 13 degrees between the superior mesenteric artery and the aorta.
Figure 1. Upper gastrointestinal radiography with a bari-um meal ingestion shows abrupt cutoff of the third portion of the duodenum.
Figure 2. Axial abdominal computed tomography demon-strated duodenal compression at the third portion between the aorta and the superior mes-enteric artery (arrow).

CONTENTS
輔仁醫學期刊 第 16卷 第 3期 2018 129
Superior mesenteric artery syndrome: an unusual cause of intestinal obstruction
surrounding the duodenum ensues, and results in shortening the distance and reducing the angle be-tween the SMA and the aorta. Other predisposing factors may be congenital, such as a short Treitz’ ligament, high insertion of the duodenum at the Treitz’ ligament, and abnormal low origin of the SMA. Anatomical changes caused by surgical pro-cedures such as scoliosis correction surgery and esophagectomy can also induce SMA syndrome [3,4].
According to a document reported by V. Bi-ank et al., the most frequent symptoms include abdominal pain, vomiting, nausea, early satiety and anorexia [5]. The condition is generally thought of as a diagnosis of exclusion. Patients might experi-ence relief when lying prone, as opposed to supine where gravity contributes to the duodenal com-pression. According to the patient’s symptoms, the clinician should be aware of the diagnosis due to the great similarity of symptoms with other more common gastrointestinal diseases, such as peptic ulcer, cholecystitis, pancreatitis, mesenteric isch-emia. Our patient received upper gastrointestinal panendoscopy and excluded peptic ulcer disease.
The condition of obstruction can progress and result in compression of the inferior vena cava and aorta. Subsequent decreases in cardiac output and distal ischemia may cause lactic acidosis, metabol-ic derangement, and even death [6].
Plain radiograph may show evidence of proxi-mal obstruction such as massive gastric distention. Upper gastrointestinal series may show compres-sion of the third portion of duodenum, as in our case, with delay in contrast passage. The diagnosis mainly depends on abdominal computed tomogra-phy, which confirms the loss of an angle between the superior mesenteric artery and the abdominal
aorta to less than 20 degrees. The distance between the two vessels is also less than 6mm (the normal distance is 8–12 mm) [7]. The patient’s angle be-tween the superior mesenteric artery and the aorta was 13 degrees, which meets the diagnostic criteria of SMA syndrome.
Conservative management is recommend-ed first with initial gastrointestinal decompression, correction of electrolyte abnormalities and nutri-tional support for weight regain and growth of the fat pad between the SMA and aorta. For those
unable to attain adequate caloric intake by mouth, nasojejunal tube feedings placed past the obstruction can be applied. Nasojejunal feeding is thought to offer a more durable alternative without the accompanying surgical morbidity [8].
Total parenteral nutrition is also an option if nasojejunal feedings remain inadequate. However, enteral feeding tubes remain more favorable be-cause they enable a better response to nutritional therapy.
Surgery is indicated for failed conservative management and for patients with chronic and refractory symptoms. The three main surgical pro-posals are the Strong operation, gastrojejunostomy and duodenojejunostomy. Duodenojejunostomy has demonstrated greater effectiveness in solv-ing symptoms, and the laparoscopic approach has being adopted as a viable alternative with the ad-vancement of minimally invasive surgery [9]. Recently, the use of robotics in the SMA syndrome surgery has gained popularity. This advanced technology provides surgical movement with great precision under a three-dimensional view of the surgical field [10].
In conclusion, SMA syndrome is rare and may mimic symptoms of acute or chronic upper intes-

CONTENTS
Fu-Jen Journal of Medicine Vol.16 No.3 2018130
Ta-Pin Lee Wen-Chih Huang
tinal obstruction. The patients are usually young and thin in body type. It should be also suspected for those experiencing significant body weight loss in short period of time. The initial management is conservative with decompression and nutritional support. Surgical duodenojejunostomy is indicated when conservative management fails.
REFERENCES
[1]. Welsch T, Büchler MW, Kienle P. Recall-ing superior mesenteric artery syndrome. Dig Surg 2007; 24(3): 149-156.
[2]. Wilkie DP. Chronic duodenal ileus. Br J Surg 1921;9: 204.
[3]. Merrett ND, Wilson RB, Cosman P, Biankin AV. Superior mesenteric artery syndrome: diagnosis and treatment strategies. J Gastroin-test Surg 2009; 13(2): 287-292.
[4]. Lippl F, Hannig C, Weiss W, Allescher HD, Classen M, Kurjak M. Superior mesen-teric artery syndrome: diagnosis and treatment from the gastroenterologist's view. J Gastro-enterol 2002; 37(8): 640-643.
[5]. Biank V, Werlin S. Superior mesenteric artery
syndrome in children: a 20-year experience. Pediatr Gastroenterol Nutr 2006; 42(5): 522-525.
[6]. Malbrain ML, Cheatham ML, Kirkpat-rick A, et al. Results from the international conference of experts on intra-abdominal hypertension and abdominal compartment syndrome. I. Definitions. Intensive Care Med 2006; 32(11): 1722-1732.
[7]. Derrick JR, Fadhli HA. Surgical anatomy of the superior mesenteric artery. Am Surg 1965; 31: 545-547.
[8]. Chan DK, Mak KS, Cheah YL. Successful nutritional therapy for superior mesenter-ic artery syndrome. Singapore Med J 2012; 53(11): e233-236 .
[9]. Munene G, Knab M, Parag B. Laparoscopic duodenojejunostomy for superior mesenteric artery syndrome. Am. Surg 2010; 76(3): 321-324.
[10]. Ayloo SM, Masrur MA, Bianco FM, Giulianot-ti PC. Robotic roux-en-Y duodenojejunostomy for superiormesenteric artery syndrome: opera-tive technique. J Laparoendosc Adv Surg Tech A 2011; 21(9): 841-844.

CONTENTS
輔仁醫學期刊 第 16卷 第 3期 2018 131
Superior mesenteric artery syndrome: an unusual cause of intestinal obstruction
上腸系膜動脈症候群:罕見的腸阻塞病因
李達彬 1,*,黃文志 2,3
中文摘要
上腸系膜動脈症候群(superior mesenteric artery syndrome)是上腸系膜動脈和主動脈之間的十二指腸遭受擠壓而引起的腸阻塞的病症。其處理通常以保守性治療及營
養支持為優先考量,而當保守性治療失敗後才考慮手術。我們提供一則上腸系膜動脈
症候群及腸阻塞的病例報告,其後成功接受十二指腸空腸吻合術(duodenojejunostomy)治療。
關鍵字:上腸系膜動脈症候群;上腸系膜動脈;腸阻塞
1 為恭紀念醫院放射科2 亞東紀念醫院解剖病理科3 國立台北護理健康大學護理學院
收稿日期:2017年 06月 07日 接受日期:2018年 03月 12日* 通訊作者:李達彬 電子信箱:[email protected]

CONTENTS
Fu-Jen Journal of Medicine Vol.16 No.3 2018132
Ta-Pin Lee Wen-Chih Huang