Embed Size (px)
Citation preview

Digestive Endoscopy
(2003)
15
, 256–262
Blackwell Science, LtdOxford, UKDENDigestive Endoscopy0915-56352003 Blackwell Science Asia Pty LtdOctober 2003154256262Review
SURVEILLANCE FOR COLITIC CANCERK HATA ET AL.
Correspondence: Keisuke Hata, Department of Surgical Oncology,The University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655,Japan. Email: [email protected]
Received 3 February 2003; accepted 12 May 2003.
REVIEW
SURVEILLANCE COLONOSCOPY FOR COLITIC CANCER IN INFLAMMATORY BOWEL DISEASE
K
EISUKE
H
ATA
, T
OSHIAKI
W
ATANABE
AND
H
IROKAZU
N
AGAWA
Department of Surgical Oncology, The University of Tokyo, Tokyo, Japan
Patients with inflammatory bowel disease are known to be at increased risk for the development of colorectal cancer,especially those with long-standing extensive ulcerative colitis. Although some recommend prophylactic totalproctocolectomy for these high-risk patients, surveillance colonoscopy to detect ulcerative colitis-associated colorectalcancer is, instead, generally performed. Dysplasia has been considered to be a useful marker to detect colorectal cancer atsurveillance colonoscopy. High-grade dysplasia is a definite indication for total proctocolectomy, while management of low-grade dysplasia is still controversial. Patients with Crohn’s disease are also considered to be at higher risk for thedevelopment of colorectal cancer, although the risk may be lower than in extensive ulcerative colitis. Molecular biology-based surveillance and chemoprevention for ulcerative colitis-associated colorectal cancer are also reviewed.
Key words: colitic cancer, Crohn’s disease, dysplasia, surveillance, ulcerative colitis.
INTRODUCTION
The association between ulcerative colitis (UC) and colorec-tal cancer (CRC) was first reported by Crohn and Rosenbergin 1925.
1
Forty years later, Morson and Pang from St MarksHospital introduced the concept of surveillance by describinghow a precancerous lesion in the rectal flat mucosa maypredict UC-associated CRC.
2
This report prompted manysurveillance studies confirming the association between dys-plasia and UC-associated CRC.
Ulcerative colitis-associated CRC is different from spo-radic CRC in several ways. UC-associated CRC: (i) is morecommon in the younger generation;
3
(ii) is more frequentlylocated in the proximal colon;
3
(iii) is difficult to detect bybarium enema or even by colonoscopy due to its widespreadnature;
4
(iv) has mucinous and signet-ring histological fea-tures in approximately half of cases;
5
and (v) is geneticallydifferent from the adenoma-carcinoma sequence, and a dys-plasia-carcinoma sequence is postulated.
6
Fecal occult blood test (FOBT) and barium enema areuseful methods for sporadic CRC screening. However,FOBT is not useful for detecting UC-associated CRC, ashematochezia is a frequent symptom of UC. Barium enemais not useful either, because of its widespread nature.
In the 1960s and 1970s, several reports recommended pro-phylactic colectomy for patients with extensive UC of morethan 10 years duration, as the risk for the development ofCRC was considered to be high enough for such patients.
7–9
However, surveillance colonoscopy to detect UC-associatedCRC has been generally recommended instead of total proc-
tocolectomy, as surveillance colonoscopy has been reportedto be effective in detecting cancer or precancerous lesions,namely dysplasia.
10–12
PATHOLOGICAL CRITERIA FOR ULCERATIVE COLITIS-
ASSOCIATED DYSPLASIA
Since many reports have demonstrated that dysplasia is auseful marker of UC-associated CRC, the object of surveil-lance colonoscopy is to detect dysplasia, especially a dyspla-sia-associated lesion or mass (DALM).
13,14
In 1983, the IBDstudy group established a classification for UC-associateddysplasia.
15
According to this classification, dysplasia isdivided into high-grade dysplasia (HGD), low-grade dyspla-sia (LGD), indefinite (IND), and negative. IND is furtherclassified into three categories: probably negative, unknown,and probably positive. It was also emphasized in this reportthat inflammatory processes sometimes resulted in histolog-ical changes identical to those of dysplasia. Therefore, sur-veillance colonoscopy should preferably be performed in theremission state. The criteria for dysplasia itself have becomerelatively uniform since this classification was established.Rosenstock from the Cleveland Clinic reported that a majordiscrepancy was as low as 4%.
16
However, inter- and intraob-server variance is still seen in several studies.
11,17,18
Connellfrom St Marks Hospital reported that interobserver agree-ment between two experienced gastrointestinal pathologistswas 77.4%.
11
The Japanese criteria for dysplasia in which dysplasia wasclassified from UC-II to UC-IV were made according toRiddell’s criteria in 1995, and have been generally used inJapan, in addition to Riddell’s criteria.
19
Intramucosal carci-noma was included in the category of HGD in this classifica-tion and was termed as UC-IV.

SURVEILLANCE FOR COLITIC CANCER 257
RISK FACTORS FOR ULCERATIVE COLITIS-ASSOCIATED COLORECTAL CANCER
Patients with UC are known to be at increased risk for thedevelopment of CRC. To perform more effective surveillanceand to maximize cost-effectiveness, it is important to identifyhigh-risk patients for the development of CRC in UC. Well-known risk factors for the development of UC-associatedCRC are the extent
20
and duration of disease.
21,22
Although some reports have stated that patients with left-sided colitis share the same risk as those with total colitis
10,23
a Swedish group performed a population-based study com-posed of 3117 UC patients and concluded that those withtotal colitis have a far higher risk for the development ofCRC than those with left-sided colitis. They reported that therelative risk for CRC is 1.7 for patients with ulcerative proc-titis, 2.8 for those with left-sided colitis, and 14.8 for pancoli-tis.
24
Disease progression should also be taken intoconsideration, as a considerable number of patients with lessextensive UC have experienced disease progression.
25,26
Lynch
et al.
reported two cases with UC-associated CRC whohad been diagnosed as having proctitis and were proven tohave total colitis in the resected specimens.
27
In order to re-evaluate the extent of disease, Connell
et al
. recommendedthat all patients with UC should undergo colonoscopy 8–10years from the onset.
11
Furthermore, it is of note that thedefinition of extent of disease varies between reports. Theborder between total colitis and left-sided colitis is taken tobe the splenic flexure,
21
the middle of the transverse colon
23
or the hepatic flexure.
11,12
Guidelines recommend thatpatients with total colitis and left-sided colitis should beentered in the surveillance program.
Duration of UC is another well-known risk factor for thedevelopment of UC-associated CRC. A recent meta-analysisestimated from 19 reports that the cumulative risk for UC-associated CRC was 2% at 10 years, 8% at 20 years, and 18%at 30 years.
28
Other reported but not established risk factors includeyounger onset of disease,
24,28
primary sclerosing cholangi-tis,
3,29
backwash ileitis,
30
family history of cancer
31,32
and dura-tion of diarrhea.
33
WHEN AND HOW FREQUENTLY SHOULD SURVEILLANCE COLONOSCOPY
BE PERFORMED?
Several guidelines recommend surveillance colonoscopy forhigh-risk patients (Table 1). Guidelines from the WorldHealth Organization (WHO)
34
and American Gastroentero-
logical Association
35
recommend that paitents with pancolitisundergo surveillance colonoscopy 8 years after the onset andthose with left-sided colitis 12–15 years after onset. Anotherguideline from Mount Sinai Hospital is more stringent, andrecommends that patients with either total colitis or left-sided colitis receive annual surveillance colonoscopy after 8–10 years of colitis.
36
As inflammation may cause regenerativechanges resembling dysplasia, surveillance colonoscopyshould be performed in the remission state.
The recommended interval of surveillance colonoscopyvaries depending on the reports or guidelines: annual or bian-nual. Nugent
et al
. reported that patients with no dysplasiadetected at the first surveillance colonoscopy might not needannual surveillance colonoscopy, as they had a lower chanceof having dysplasia or cancer.
10,17
However, this opinionseems rough and risky. Connell
et al
. reported that sevenpatients developed interval cancer although they had beenfree of dysplasia or cancer in any previous surveillancecolonoscopy. Furthermore, five of these were found to haveCRC in Dukes C stage 10–23 months after previous colonos-copy. These results suggest that the interval of surveillancecolonoscopy should be annual even for patients with no pre-vious dysplasia.
HOW TO SURVEY ULCERATIVE COLITIS-ASSOCIATED COLORECTAL CANCER
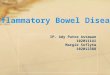
As described earlier, UC-associated CRC appears to be dif-ferent from sporadic CRC. It tends to be widespread, and issometimes difficult to recognize even by colonoscopy. Oneof the endoscopic markers for UC-associated CRC is DALM(Figs 1–4). Blackstone reported that seven out of 12 patientswith DALM were found to have invasive cancer, but onlyone out of 27 patients with flat dysplasia was found to haveCRC.
13
Woolrich reported that 12 of 13 patients with UC-associated CRC had dysplasia in the resected specimens.
37
However, flat dysplasia should not be disregarded, andbiopsy specimens should also be taken from endoscopicallyflat mucosa.
Table 1.
Recommended management of dysplasia
High-grade dysplasia ProctocolectomyLow-grade dysplasia with
DALMProctocolectomy
Flat low-grade dysplasia Surveillance colonoscopy within 3–6 months or proctocolectomy
If persistent and/or multifocal: proctocolectomy
Indefinite for dysplasia Surveillance colonoscopy within 3–6 months
DALM, dysplasia-associated lesion or mass.
Fig. 1.
Colonoscopy shows dysplasia-associated lesion or mass(DALM) in the sigmoid colon. Note that the border of the lesionis obscure.

258 K HATA
ET AL.
Flat dysplasia is very difficult to recognize considering thegranular changes of the background mucosa due to inflam-mation. Therefore, it is generally recommended to takebiopsy specimens from every 10 cm of the whole colorec-
tum.
34
However, a set of 10 biopsy specimens was theoreti-cally calculated to cover only 0.05% of the total surface areaof the whole colorectum.
16
Some, therefore, recommend tak-ing 33 biopsy specimens or one at every quadrant of a 10 cminterval, whichever is the greatest number, to obtain 90%confidence in detecting dysplasia.
38,39
However, feasibility islimited in clinical practice.
11
Until more effective methods areestablished, biopsy specimens from flat mucosa should betaken.
40
MANAGEMENT OF DYSPLASIA
Table 2 summarizes the recommended management ofpatients with dysplasia, although controversy exists. High-grade dysplasia is a definite indication for total proctocolec-tomy. Management of LGD is controversial, as the predictivevalue of LGD for CRC varies between reports.
41
Some authors believe that LGD is a useful marker todetect UC-associated CRC. A study from the USA statedthat 18% of patients with LGD later developed invasivecancer, and recommended careful follow up for thosepatients.
37
Another study from the USA reported that fourof 10 patients with LGD were found to have cancer, andanother two were found to have HGD in the colectomyspecimen.
10
Connell from St Marks Hospital reviewed theirseries and concluded that the 5-year cumulative probabilityof HGD or cancer for patients with LGD is as high as 54%and recommended that patients with persistent LGD should
Table 2.
Recommended starting point and interval of surveillence colonoscopy
Author Reference Year Starting point Interval
Winawer
et al.
34 1995 Pancolitis 8 yearsLeft-sided 12–15 years
1 or 2 years
Winawer
et al.
35 1997 Pancolitis 8 yearsLeft-sided 12–15 years
1 or 2 years
Kornbluth and Sachar 36 1997 8–10 years 1 year
Fig. 2.
Biopsy specimen of the lesion in Fig. 1 reveals low-grade dysplasia.
Fig. 3.
Colonoscopy shows dysplasia-associated lesion or mass(DALM) in the rectum. (Reproduced with permission fromNagasako K, Fujimori T, Hoshihara Y, Tabuchi M.
Atlas ofGastroenterologic Endoscopy.
Tokyo: Igaku-shoin Ltd, 1998;150: Fig 5-73b.
76
)
Fig. 4.
Biopsy specimen of the lesion in Fig. 3 reveals high-grade dysplasia.

SURVEILLANCE FOR COLITIC CANCER 259
undergo proctocolectomy.
11
Bernstein
et al.
reviewed 10 sur-veillance studies and reported that patients with LGD had a19% probability of having cancer at immediate colectomy,and asserted that the finding of definite dysplasia of anygrade is an indication for colectomy.
17
However, several authors doubt whether LGD is a usefulmarker for UC-associated CRC. Some LGD lesions havebeen reported to disappear at close follow-up colonoscopies.
4
Rosenstock
et al.
from the Cleveland Clinic reported thatonly one of 39 patients with LGD developed invasive carci-noma.
16
Axon concluded in his review that LGD has littleprognostic value.
40
A Swedish group reported that colectomydoes not appear to be justified in patients with LGD in flatmucosa, even if it is repeated, as no progression to HGD wasobserved during 10 years of follow up.
42
Guidelines fromWHO recommend that repeated surveillance colonoscopyshould be performed after 3–6 months for those with LGD,and total proctocolectomy is recommended if dysplasia ismultifocal, persistent or shows DALM.
34
Such discrepancy may result from a different ratio ofDALM to flat dysplasia. Blackstone reported that seven outof 12 patients with DALM were found to have invasive can-cer, but only one out of 27 patients with flat dysplasia wasfound to have CRC.
13
Another explanation for such dis-crepancy is that in some reports, sporadic adenoma isincluded in the category of LGD. These issues will bediscussed below.
SPORADIC ADENOMA OR DYSPLASIA IN ULCERATIVE COLITIS PATIENTS
As sporadic adenoma is not infrequent in the general popu-lation, patients with UC are expected to have sporadic ade-nomas incidentally. UC-associated CRC tends to bewidespread and to occur multifocally. Hence, total procto-colectomy is recommended for patients with dysplasia. Onthe other hand, it is feasible to resect sporadic adenoma oncolonoscopy.
10,13
The problem is that it is difficult to differen-tiate sporadic adenoma from dysplasia in a biopsy speci-men.
15,21
Indeed, sporadic adenoma and dysplasia have bothbeen treated as definite dysplasia in several studies.
12,42
Suzuki
et al
. recommended taking several biopsy speci-mens from the surrouding flat mucosa.
43
If those specimensare negative for dysplasia, endoscopic polypectomy may beadequate, followed by close surveillance colonoscopy. If pos-itive, total proctocolectomy should be considered. They alsoconcluded that patients with DALM were younger, hadlonger duration, and had more extensive disease than thosewith adenoma. The success of such management was con-firmed by several studies.
44,45
Engelsgjerd
et al.
and Rubin
etal.
successfully followed up 34 and 70 adenoma-like dysplas-tic polyps, respectively, after polypectomy.
MOLECULAR BIOLOGY-BASED AID FOR SURVEILLANCE
Inactivation of
p53
by mutation and loss of heterozygosity isa common event in UC-associated CRC and may be an ear-lier event than in sporadic CRC.
46–49
Recent studies havestated that the basal pattern of p53 expression is correlatedwith
p53
mutation.
50
Immunostaining for P53 protein is auseful and practically feasible way to detect dysplasia in clin-
ical practice in addition to hematoxylin and eosin staining.Brentnall
et al
. reported that p53 immunostaining might pre-cede dysplasia itself.
51
In contrast, Ilyas and Talbot conducteda longitudinal study consisting of 10 cases and reported thatp53 overexpression is a relatively late event.
52
Both studieswere too limited to draw a definite conclusion in terms of thenumber of cases. A Swedish group conducted cohort studiesconsisting of 95 patients and concluded that p53 overexpres-sion developed 8, 26 and 38 months before LGD, HGD andcancer, respectively.
53
Ki-67 antigen is known to be a marker of proliferatingcells.
54,55
The upper third of the crypts was stained with anti-Ki-67 antibody in dysplastic epithelium. A Ki-67 labelingindex is reported to be a useful marker for detecting dyspla-sia in UC. Shinozaki
et al
. reported that the positive predic-tive value was 96%, and that even proliferating activity mayprecede dysplasia as detected by H&E staining in somecases.
54
However, this technique cannot differentiate dysplas-tic from inflammatory changes.
A Swedish group performed an aneuploidy study frombiopsy specimens.
56
Aneuploidy correlated with dysplasia inthat study. Furthermore, aneuploidy preceded dysplasia intwo patients.
Several studies have focused on colonic lavage as an alter-native to colonoscopic surveillance, as it may be less invasiveand expensive. Aneuploidy can be recognized in colonic lav-age in patients with UC-associated dysplasia or cancer.
38,57
AUS group performed a prospective study in which fivepatients with aneuploidy who had never had dysplasia allprogressed to dysplasia within 2.5 years, while no patientswithout aneuploidy progressed to dysplasia.
P53
mutationcould be detected in colonic lavage in patients with long-standing UC, none of whom had dysplasia in serial biopsyspecimens, although false positives could not be fullyassessed due to insufficient follow up.
58
CANCER RISK FOR PATIENTS WITH CROHN’S DISEASE
Patients with Crohn’s disease (CD) are also reported to beat increased risk for CRC. CD-associated CRC is similar toUC-associated CRC in that it tends to be multifocal, dyspla-sia-associated and mucin productive.
5
A Swedish group performed a cohort study consisting of1655 patients with CD and 12 CRC were diagnosed.
59
In thatstudy, the relative risk for CRC in patients with Crohn’scolitis was 3.2 in those with ileocolitis, and 5.6 in those withcolonic involvement alone, while those with terminal ileitisalone had no increased risk. A study from Birmingham statedthat patients with extensive Crohn’s colitis had a 19-foldincrease in the risk of developing CRC. A US group per-formed a retrospective study consisting of 579 patients withCD, and seven CRC and four small bowel cancers werefound.
60
They concluded that the risk of CRC for patientswith CD was almost identical to that for those with left-sidedUC. Sachar reviewed those studies and recommended doing‘whatever to choose to do for patients with UC’.
61
Carcinomaarising in an anorectal fistula has also been reported inpatients with CD. Ky
et al.
reported seven cases and reviewed33 reported cases.
62
They concluded that diagnosis is verydifficult, but that examination under anesthesia, rectal ultra-sound examination and dynamic contrast-enhanced magnetic

260 K HATA
ET AL.
resonance imaging may help.
63
Treatment included surgicalexcision and/or chemoradiotherapy, especially for squamouscell carcinoma. Prognosis was poor due to the difficulty indiagnosis, and more than half of the reported patients diedof the disease.
CRITICISM OF SURVEILLANCE COLONOSCOPY AND FUTURE PERSPECTIVES
Although many reports have confirmed that it is importantto perform surveillance colonoscopy, some doubt its effec-tiveness in terms of early detection, survival and cost.
17,27
Wehave performed surveillance colonoscopy for long-standingulcerative colitis since 1979. Patients with total colitis andleft-sided colitis of more than 7 years duration were recom-mended for endoscopic surveillance every year in our pro-gram. Matsuda
et al
. reported 10 patients with UCcomplicated with invasive cancer.
64
Five of them were iden-tified in surveillance colonoscopy, while the other five withsymptoms such as bowel obstruction or abdominal masswere referred without surveillance colonoscopy during thesame period. All the patients in the surveillance group arealive, while three of the five in the non-surveillance groupdied of the cancer. In contrast, Axon reviewed 12 studies ofcolonoscopic cancer surveillance and criticized its effective-ness.
40
In his review, 92 out of 1916 patients were found tohave cancer and only 52 (57%) were found in Dukes’ A orB. Patients with UC-associated CRC of Dukes A and Bshowed a good survival rate, while those of Dukes C had anextremely poor prognosis.
65
Furthermore, 476 colonoscopieswere needed to detect one UC-associated cancer. The cost-effectiveness of surveillance colonoscopy has remainedquestionable.
66,67
Recent advances in molecular biology will make surveil-lance better and more effective. Immunostaining for p27,
68
metallothionein,
69
carcinoembryonic antigen,
70
Gal-GalNAc
71
and nuclear matrix protein
72
have been investi-gated.
We should become more focused on primary preventionas well as on early detection (secondary prevention). Regular5-aminosalicylic acid intake may prevent patients with UCfrom developing CRC,
32
but a multivariate analysis by aSwedish group could not confirm this finding.
29
Folic acid mayalso have a preventive effect on UC-associated CRC carcino-genesis.
73 Cyclooxygenase-2 inhibitor is one such candidate,although it could cause a flare up of UC itself.74 Ursodiolseems to prevent UC-associated CRC complicated with pri-mary sclerosing cholangitis.75
CONCLUSION
Patients with inflammatory bowel disease (IBD) are at ahigher risk for the development of CRC. Although its effec-tiveness has not been established in terms of cost and sur-vival, surveillance colonoscopy should be performed forpatients with long-standing IBD until new methods areestablished. It is also important for patients as well as physi-cians to know that there are several limitations to surveil-lance colonoscopy. Further improvements in molecularbiology techniques and investigations of the effect of chemo-prevention are needed to improve the management of IBD-associated CRC.
REFERENCES
1. Crohn BB, Rosenberg H. Sigmoidoscopic picture of chroniculcerative colitis (non-specific). Am. J. Med. Sci. 1925; 170:220–8.
2. Morson BC, Pang LS. Rectal biopsy as an aid to cancercontrol in ulcerative colitis. Gut 1967; 8: 423–34.
3. Bansal P, Sonnenberg A. Risk factors of colorectal cancerin inflammatory bowel disease. Am. J. Gastroenterol. 1996;91: 44–8.
4. Collins RH, Feldman M, Fordtran JS. Colon cancer, dyspla-sia, and surveillance in patients with ulcerative colitis. Acritical review. N. Engl. J. Med. 1987; 316: 1654–8.
5. Choi PM, Zelig MP. Similarity of colorectal cancer inCrohn’s disease and ulcerative colitis: implications for car-cinogenesis and prevention. Gut 1994; 35: 950–4.
6. Fogt F, Vortmeyer AO, Goldman H, Giordano TJ, MerinoMJ, Zhuang Z. Comparison of genetic alterations in colonicadenoma and ulcerative colitis-associated dysplasia and car-cinoma. Hum. Pathol. 1998; 29: 131–6.
7. Dennis C, Karlsson KE. Cancer risk in ulcerative colitis:formidability per patient-year of late disease. Surgery 1961;50: 568–71.
8. MacDougall IPM. The cancer risk in ulcerative colitis. Lan-cet 1964; 2: 655–8.
9. Kewenter J, Ahlman H, Hulten L. Cancer risk in extensiveulcerative colitis. Ann. Surg. 1978; 188: 824–8.
10. Nugent FW, Haggitt RC, Gilpin PA. Cancer surveillance inulcerative colitis. Gastroenterology 1991; 100: 1241–8.
11. Connell WR, Lennard-Jones JE, Williams CB, Talbot IC,Price AB, Wilkinson KH. Factors affecting the outcome ofendoscopic surveillance for cancer in ulcerative colitis. Gas-troenterology 1994; 107: 934–44.
12. Lennard-Jones JE, Melville DM, Morson BC, Ritchie JK,Williams CB. Precancer and cancer in extensive ulcerativecolitis: findings among 401 patients over 22 years. Gut 1990;31: 800–6.
13. Blackstone MO, Riddell RH, Rogers BH, Levin B. Dyspla-sia-associated lesion or mass (DALM) detected by colonos-copy in long-standing ulcerative colitis: an indication forcolectomy. Gastroenterology 1981; 80: 366–74.
14. Butt JH, Konishi F, Morson BC, Lennard-Jones JE,Ritchie JK. Macroscopic lesions in dysplasia and carci-noma complicating ulcerative colitis. Dig. Dis. Sci. 1983;28: 18–26.
15. Riddell RH, Goldman H, Ransohoff DF et al. Dysplasia ininflammatory bowel disease: standardized classification withprovisional clinical applications. Hum. Pathol. 1983; 14: 931–68.
16. Rosenstock E, Farmer RG, Petras R, Sivak MV, Rankin GB,Sullivan BH. Surveillance for colonic carcinoma in ulcer-ative colitis. Gastroenterology 1985; 89: 1342–6.
17. Bernstein CN, Shanahan F, Weinstein WM. Are we tellingpatients the truth about surveillance colonoscopy in ulcer-ative colitis? Lancet 1994; 343: 71–4.
18. Eaden J, Abrams K, McKay H, Denley H, Mayberry J.Inter-observer variation between general and specialistgastrointestinal pathologists when grading dysplasia inulcerative colitis. J. Pathol. 2001; 194: 152–7.
19. Konishi F, Wakasa H, Kino I, Watanabe H, Nagura H, MutoT. Histological classification of the neoplastic changes aris-ing in ulcerative colitis: a new proposal in Japan. J. Gastro-enterol. 1995; 30: 20–4.
20. Greenstein AJ, Sachar DB, Smith H et al. Cancer in univer-sal and left-sided ulcerative colitis: factors determining risk.Gastroenterology 1979; 77: 290–4.
21. Leidenius M, Kellokumpu I, Husa A, Riihela M, SipponenP. Dysplasia and carcinoma in longstanding ulcerative coli-

SURVEILLANCE FOR COLITIC CANCER 261
tis: an endoscopic and histological surveillance programme.Gut 1991; 32: 1521–5.
22. Gyde SN, Prior P, Allan RN et al. Colorectal cancer inulcerative colitis: a cohort study of primary referrals fromthree centres. Gut 1988; 29: 206–17.
23. Sugita A, Sachar DB, Bodian C, Ribeiro MB, Aufses AH,Greenstein AJ. Colorectal cancer in ulcerative colitis. Influ-ence of anatomical extent and age at onset on colitis-cancerinterval. Gut 1991; 32: 167–9.
24. Ekbom A, Helmick C, Zack M, Adami HO. Ulcerative coli-tis and colorectal cancer. A population-based study. N. Eng.J. Med. 1990; 323: 1228–33.
25. Farmer RG, Easley KA, Rankin GB. Clinical patterns, nat-ural history, and progression of ulcerative colitis. A long-term follow-up of 1116 patients. Dig. Dis. Sci. 1993; 38: 1137–46.
26. Leijonmarck CE, Lofberg R, Ost A, Hellers G. Long-termresults of ileorectal anastomosis in ulcerative colitis in Stock-holm County. Dis. Colon Rectum 1990; 33: 195–200.
27. Lynch DA, Lobo AJ, Sobala GM, Dixon MF, Axon AT.Failure of colonoscopic surveillance in ulcerative colitis. Gut1993; 34: 1075–80.
28. Eaden JA, Abrams KR, Mayberry JF. The risk of colorectalcancer in ulcerative colitis: a meta-analysis. Gut 2001; 48:526–35.
29. Lindberg BU, Broome U, Persson B. Proximal colorectaldysplasia or cancer in ulcerative colitis. The impact of pri-mary sclerosing cholangitis and sulfasalazine: results from a20-year surveillance study. Dis. Colon Rectum 2001; 44: 77–85.
30. Heuschen UA, Hinz U, Allemeyer EH et al. Backwash ileitisis strongly associated with colorectal carcinoma in ulcerativecolitis. Gastroenterology 2001; 120: 841–7.
31. Matsuda K, Watanabe T, Shinozaki M et al. Ulcerative colitispatients with a family history of colorectal cancer should besubjected to close and careful surveillance. Jpn J. Clin.Oncol. 1999; 29: 448–51.
32. Eaden J, Abrams K, Ekbom A, Jackson E, Mayberry J.Colorectal cancer prevention in ulcerative colitis: a case-control study. Aliment. Pharmacol. Ther. 2000; 14: 145–53.
33. Shinozaki M, Muto T, Suzuki K et al. Chronic active diseasereflects cancer risk in ulcreative colitis. Jpn J. Cancer Res.1999; 90: 1066–70.
34. Winawer SJ, St John DJ, Bond JH et al. Prevention of col-orectal cancer: guidelines based on new data. WHO Collab-orating Center for the Prevention of Colorectal Cancer.Bull. World Health Org. 1995; 73: 7–10.
35. Winawer SJ, Fletcher RH, Miller L et al. Colorectal cancerscreening: clinical guidelines and rationale. Gastroenterol-ogy 1997; 112: 594–642.
36. Kornbluth A, Sachar DB. Ulcerative colitis practice guide-lines in adults. American College of Gastroenterology, Prac-tice Parameters Committee. Am. J. Gastroenterol. 1997; 92:204–11.
37. Woolrich AJ, DaSilva MD, Korelitz BI. Surveillance in theroutine management of ulcerative colitis: the predictivevalue of low-grade dysplasia. Gastroenterology 1992; 103:431–8.
38. Rubin CE, Haggitt RC, Burmer GC et al. DNA aneuploidyin colonic biopsies predicts future development of dysplasiain ulcerative colitis. Gastroenterology 1992; 103: 1611–20.
39. Farrell RJ, Peppercorn MA. Ulcerative colitis. Lancet 2002;359: 331–40.
40. Axon AT. Cancer surveillance in ulcerative colitis—a timefor reappraisal. Gut 1994; 35: 587–9.
41. Ullman TA, Loftus EV, Kakar S, Burgart LJ, Sandborn WJ,Tremaine WJ. The fate of low grade dysplasia in ulcerativecolitis. Am. J. Gastroenterol. 2002; 97: 922–7.
42. Befrits R, Ljung T, Jaramillo E, Rubio C. Low-grade dyspla-sia in extensive, long-standing inflammatory bowel disease:a follow-up study. Dis. Colon Rectum 2002; 45: 615–20.
43. Suzuki K, Muto T, Shinozaki M, Yokoyama T, Matsuda K,Masaki T. Differential diagnosis of dysplasia-associatedlesion or mass and coincidental adenoma in ulcerative coli-tis. Dis. Colon Rectum 1998; 41: 322–7.
44. Engelsgjerd M, Farraye FA, Odze RD. Polypectomy may beadequate treatment for adenoma-like dysplastic lesions inchronic ulcerative colitis. Gastroenterology 1999; 117: 1288–94; 1488–91.
45. Rubin PH, Friedman S, Harpaz N et al. Colonoscopicpolypectomy in chronic colitis: conservative managementafter endoscopic resection of dysplastic polyps. Gastroenter-ology 1999; 117: 1295–300.
46. Yin J, Harpaz N, Tong Y et al. p53 point mutations in dys-plastic and cancerous ulcerative colitis lesions. Gastroenter-ology 1993; 104: 1633–9.
47. Holzmann K, Klump B, Borchard F et al. Comparative anal-ysis of histology, DNA content, p53 and Ki-ras mutations incolectomy specimens with long-standing ulcerative colitis.Int. J. Cancer 1998; 76: 1–6.
48. Kern SE, Redston M, Seymour AB et al. Molecular geneticprofiles of colitis-associated neoplasms. Gastroenterology1994; 107: 420–8.
49. Burmer GC, Rabinovitch PS, Haggitt RC et al. Neoplasticprogression in ulcerative colitis: histology, DNA content,and loss of a p53 allele. Gastroenterology 1992; 103: 1602–10.
50. Noffsinger AE, Belli JM, Miller MA, Fenoglio-Preiser CM.A unique basal pattern of p53 expression in ulcerative colitisis associated with mutation in the p53 gene. Histopathology2001; 39: 482–92.
51. Brentnall TA, Crispin DA, Rabinovitch PS et al. Mutationsin the p53 gene: an early marker of neoplastic progressionin ulcerative colitis. Gastroenterology 1994; 107: 369–78.
52. Ilyas M & Talbot IC. p53 expression in ulcerative colitis: alongitudinal study. Gut 1995; 37: 802–4.
53. Lashner BA, Shapiro BD, Husain A, Goldblum JR. Evalu-ation of the usefulness of testing for p53 mutations in col-orectal cancer surveillance for ulcerative colitis. Am. J.Gastroenterol. 1999; 94: 456–62.
54. Shinozaki M, Watanabe T, Kubota Y, Sawada T, Nagawa H,Muto T. High proliferative activity is associated with dyspla-sia in ulcerative colitis. Dis. Colon Rectum 2000; 43: S34–9.
55. Sjoqvist U, Ost A, Lofberg R. Increased expression of pro-liferative Ki-67 nuclear antigen is correlated with dysplasticcolorectal epithelium in ulcerative colitis. Int. J. ColorectalDis. 1999; 14: 107–13.
56. Lofberg R, Brostrom O, Karlen P, Tribukait B, Ost A.Colonoscopic surveillance in long-standing total ulcerativecolitis—a 15-year follow-up study. Gastroenterology 1990;99: 1021–31.
57. Suzuki K, Muto T, Masaki T, Morioka Y. Microspectropho-tometric DNA analysis in ulcerative colitis with special ref-erence to its application in diagnosis of carcinoma anddysplasia. Gut 1990; 31: 1266–70.
58. Lang SM, Stratakis DF, Heinzlmann M, Heldwein W,Wiebecke B, Loeschke K. Molecular screening of patientswith long standing extensive ulcerative colitis: detection ofp53 and Ki-ras mutations by single strand conformationpolymorphism analysis and differential hybridisation incolonic lavage fluid. Gut 1999; 44: 822–5.
59. Ekbom A, Helmick C, Zack M, Adami HO. Increased riskof large-bowel cancer in Crohn’s disease with colonicinvolvement. Lancet 1990; 336: 357–9.
60. Greenstein AJ, Sachar DB, Smith H, Janowitz HD, AufsesAH Jr. A comparison of cancer risk in Crohn’s disease andulcerative colitis. Cancer 1981; 48: 2742–5.

262 K HATA ET AL.
61. Sachar DB. Cancer in Chrohn’s disease: dispelling themyths. Gut 1994; 35: 1507–8
62. Ky A, Sohn N, Weinstein MA, Korelitz BI. Carcinoma aris-ing in anorectal fistulas of Crohn’s disease. Dis. Colon Rec-tum 1998; 41: 992–6.
63. Spencer JA, Ward J, Beckingham IJ, Adams C, AmbroseNS. Dynamic contrast-enhanced MR imaging of perianalfistulas. AJR Am. J. Roentgenol. 1996; 167: 735–41.
64. Matsuda K, Yokoyama T, Suzuki K, Watanabe T, Masaki T,Muto T. Precancerous lesion in inflammatory bowel disease.Clin. Gastroenterol. 1998; 13: 761–70.
65. Heimann TM, Oh SC, Martinelli G et al. Colorectal carci-noma associated with ulcerative colitis: a study of prognosticindicators. Am. J. Surg. 1992; 164: 13–17.
66. Vemulapalli R, Lance P. Cancer surveillance in ulcerativecolitis: more of the same or progress? Gastroenterology 1994;107: 1196–9.
67. Jonsson B, Ahsgren L, Andersson LO, Stenling R, RutegardJ. Colorectal cancer surveillance in patients with ulcerativecolitis. Br. J. Surg. 1994; 81: 689–91.
68. Walsh S, Murphy M, Silverman M et al. p27 expression ininflammatory bowel disease-associated neoplasia. Furtherevidence of a unique molecular pathogenesis. Am. J. Pathol.1999; 155: 1511–18.
69. Bruewer M, Schmid KW, Krieglstein CF, Senninger N,Schuermann G. Metallothionein: early marker in the car-
cinogenesis of ulcerative colitis-associated colorectal carci-noma. World J. Surg. 2002; 26: 726–31.
70. Thor A, Itzkowitz SH, Schlom J, Kim YS, Hanauer S.Tumor-associated glycoprotein (TAG-72) expression inulcerative colitis. Int. J. Cancer 1989; 43: 810–15.
71. Said IT, Shamsuddin AM, Sherief MA, Taleb SG, Aref WF,Kumar D. Comparison of different techniques for detectionof Gal-GalNAc, an early marker of colonic neoplasia. Histol.Histopathol. 1999; 14: 351–7.
72. Izzo RS, Pellecchia C. Dysplasia expresses altered nuclearmatrix protein composition in human ulcerative colitis. Bio-chem. Mol. Biol. Int. 1996; 40: 521–6.
73. Lashner BA, Provencher KS, Seidner DL, Knesebeck A,Brzezinski A. The effect of folic acid supplementation on therisk for cancer or dysplasia in ulcerative colitis. Gastroenter-ology 1997; 112: 29–32.
74. Agoff SN, Brentnall TA, Crispin DA et al. The role ofcyclooxygenase 2 in ulcerative colitis-associated neoplasia.Am. J. Pathol. 2000; 157: 737–45.
75. Tung BY, Emond MJ, Haggitt RC et al. Ursodiol use isassociated with lower prevalence of colonic neoplasia inpatients with ulcerative colitis and primary sclerosing cho-langitis. Ann. Intern. Med. 2001; 134: 89–95.
76. Nagasako K, Fujimori T, Hoshihara Y, Tabuchi M. Atlas ofGastroenterologic Endoscopy. Tokyo: Igaku-shoin Ltd, 1998;150.