Embed Size (px)
Citation preview

SusanEverson
portfolio

AnnualReports
design, layout, writing, editing, data presentation, infographics, prepress, project management

40 Key observations
42 First-year hospital admission rates among incident dialysis patients
46 Hospital admission rates among prevalent dialysis patients
50 Cardiovascular disease as the primary discharge diagnosis
52 Acute coronary syndrome (myocardial infarction & unstable angina)
54 Arrhythmia
56 Heart failure & cardiomyopathy
58 Fluid overload & pleural effusion
60 Stroke
62 Infection as the primary discharge diagnosis
64 Bacteremia & septicemia
66 Dialysis access infection, including peritonitis
68 Pneumonia & influenza
70 Intestinal infection with C. difficile
3MORTALITY
96 Key observations
98 First-year mortality in incident dialysis patients, by U.S. Census Division
102 Weekly mortality rates in incident dialysis patients
103 Daily mortality rates in incident dialysis patients
104 Expected remaining lifetimes in incident dialysis patients
105 Distribution of causes of death during the first year of dialysis
106 Cause-specific mortality in incident dialysis patients
107 Peritoneal dialysis in incident dialysis patients
108 Mortality in prevalent dialysis patients, by U.S. Census Division
112 Counts of prevalent patients & patient deaths
113 Mortality trends in prevalent dialysis patients, by stratum
4CARDIOVASCULAR
DISEASE
124 Rating from CMS methodology vs. rating based exclusively on SMR & SHR
126 Rating from CMS methodology vs. rating with 50 percent weight ascribed to SMR & SHR
128 Rating from CMS methodology vs. rating based exclusively on Kt/V & hypercalcemia metrics
130 Rating from CMS methodology vs. rating based exclusively on fistula & catheter metrics
132 Rating from CMS methodology vs. rating that reflects uncertainty in estimates of standardized outcome ratios
134 Rating based exclusively on Kt/V & hypercalcemia metrics vs. rating based exclusively on fistula & catheter metrics
136 Conclusions
5DIALYSIS CARE BENCHMARKS
124 Rating from CMS methodology vs. rating based exclusively on SMR & SHR
126 Rating from CMS methodology vs. rating with 50 percent weight ascribed to SMR & SHR
128 Rating from CMS methodology vs. rating based exclusively on Kt/V & hypercalcemia metrics
130 Rating from CMS methodology vs. rating based exclusively on fistula & catheter metrics
132 Rating from CMS methodology vs. rating that reflects uncertainty in estimates of standardized outcome ratios
134 Rating based exclusively on Kt/V & hypercalcemia metrics vs. rating based exclusively on fistula & catheter metrics
136 Conclusions
140 Analytical methods
chap
ter
on
e pa
tiEn
t pO
pula
tiO
nS
compared to prevalence estimates from other sources, including med-ical charts and administrative claims. Data here illustrate that, for several comorbid conditions, prevalence according to the Medical Evidence Report is 30–50 percent lower than prevalence according to the assess-ment of diagnosis codes in Medicare claims for medical services during the six months before dialysis initia-tion. Plausibly, under-reporting may vary by location and provider orga-nization. These comorbidity desig-nations are used for risk adjustment of several metrics of facility perfor-mance, including standardized mor-tality and hospitalization ratios, and the lack of consistent and compre-hensive reporting may bias metrics—leading, for example, to distortions in star ratings.
Ultimately, these data speak to a much broader issue: many aspects of regulatory oversight, including Dialysis Facility Compare, the Quality Incentive Program, and the 5-Star Quality Rating System, are influenced by the extent to which the Medical Evidence Report is accurately com-pleted, yet those who typically com-plete the form, including nephrolo-gists and nursing staff, have no direct
incentive to verify accurate comple-tion, let alone enough history with the patient to ascertain comorbidity more rigorously than through self-reporting.
The starting point for determining when to initiate dialysis treatment has been based on clinical symptoms and biochemistry. Several studies, how-ever, have shown no benefit in using biochemical criteria to justify starting dialysis at an earlier time. Data here show that the historical trend of rising estimated glomerular filtration rate (eGFR) at dialysis initiation has ceased in recent years. In contrast to the sta-ble landscape surrounding eGFR, the distribution of hemoglobin at dialysis initiation has changed markedly in recent years, with declines in mean hemoglobin due to more limited use of erythropoiesis-stimulating agents (ESAs) in non-dialysis-dependent chronic kidney disease patients.
We conclude this chapter with data regarding initial vascular access. The exceedingly common use of catheters at dialysis initiation is a major concern, and one that dialysis providers would like to address. However, these provid-ers do not treat patients prior to the onset of ESRD. Data from 2011 do indi-cate increased placement of maturing fistulas, but progress is modest.
Further changes must be tracked closely, as the structure of the ESRD Prospective Payment System forces providers to limit costs per treat-ment. Catheter use has been shown in many studies to increase the use of ESAs, likely as a result of increased risk of infectious complications, which themselves might engender hospi-talizations that necessarily result in missed outpatient dialysis treatments. Hopefully, these pressures lead pro-viders to work more closely with phy-sicians to reduce the use of catheters and, in particular, to remove catheters as soon as possible when their use has been acutely required.
10 ► counts of incident ESRD cases initiating on dialysis
in freestanding units
12 ► hemoglobin, estimated glomerular filtration rate, & vascular access at initiation
14 ► pneumonia & influenza
13
chap
ter
on
e Pa
tien
t Po
Pula
tio
ns
0 Annual counts of incident ESRD cases initiating on dialysis in freestanding facilities have increased by 3.1 percent per year in the Middle Atlantic, the second highest rate among all Census Divisions.
0 Leading the division has been New York, with a nearly 5 percent annual increase in counts of incident cases. More study is needed to assess within-state variation in incident count trends.
0 New Jersey trails New York only slightly, with a nearly 4 percent annual increases in counts of incident cases.
PA
NY
NJ
PA
NY
NJ
<325 (_x 138)
820-<1,5621,562-<2,6892,689+ (
_x 5,477)
text is white
325-<820
DiviSiOn 2 • miDDlE atlantic
0 Annual counts of incident ESRD patients initiating on dialysis in freestanding facilities have been stable in New England since 2004.
0 Counts in Massachusetts, the divisional leader in incident cases, have declined modestly. 0 Most dialysis facilities in Vermont are hospital-based, resulting in very few incident cases in
freestanding facilities. 0 “.” Zero values in this cell.
ME
NH
VT
MA
CTRI
<325 (_x 138)
820-<1,5621,562-<2,6892,689+ (
_x 5,477)
text is white
325-<820
DiviSiOn 1 • nEw EnglanD
0 The East North Central Division is complex, with major population centers (e.g., Chicago, Detroit, and Cincinnati), wide rural expanses (in Illinois, Indiana, and Wisconsin), and chal-lenging socioeconomics in the Ohio River Valley basin.
0 Annual counts of incident ESRD cases initiating on dialysis in freestanding facilities have increased by 2.2 percent per year in the East North Central Division, but trends have varied across states.
0 Counts have increased most rapidly in Indiana and Ohio, and most slowly in Michigan and Wisconsin.
WI
IL
IN
OH
MI
<325 (_x 138)
820-<1,5621,562-<2,6892,689+ (
_x 5,477)
text is white
325-<820
DiviSiOn 3 • EaSt nOrth cEntral
2004 2005 2006 2007 2008 2009 2010 2011 apc
All 2,894 3,011 3,033 2,934 2,990 3,056 2,916 2,927 0
Connecticut 763 806 835 815 837 897 850 822 1.2
Maine 193 233 215 158 188 176 136 159 -5.2
Mass. 1,415 1,436 1,454 1,415 1,413 1,424 1,408 1,417 -0.2
New Hamp. 232 261 286 279 271 284 272 245 0.6
Rhode Island 288 275 243 266 277 270 237 269 -1
Vermont . . . . . . 13 15 .
2004 2005 2006 2007 2008 2009 2010 2011 apc
All 9,687 9,966 10,430 10,811 11,079 11,646 11,548 11,965 3.1
New Jersey 1,973 2,061 2,204 2,179 2,187 2,375 2,400 2,689 3.8
New York 3,588 3,720 3,753 4,206 4,499 4,661 4,671 4,753 4.7
Pennsylvania 4,126 4,185 4,473 4,426 4,393 4,610 4,477 4,523 1.3
2004 2005 2006 2007 2008 2009 2010 2011 apc
All 13,431 14,210 14,596 14,686 14,975 15,438 15,987 15,629 2.2
Illinois 3,818 3,981 4,086 4,220 4,229 4,434 4,534 4,468 2.4
Indiana 1,791 2,013 2,165 2,212 2,275 2,240 2,274 2,362 3.2
Michigan 3,081 3,278 3,282 3,140 3,326 3,364 3,440 3,283 1.0
Ohio 3,727 3,941 3,954 4,123 4,094 4,328 4,648 4,405 2.7
Wisconsin 1,014 997 1,109 991 1,051 1,072 1,091 1,111 1.3
2.27 Counts of incident ESRD cases initiating on dialysis in freestanding facilities
15
ExEc
uti
vE S
um
mar
y
E X E C U T I V E S U M M A R YThe Peer Kidney Care Initiative is the result of collaboration among the Chief Medical Officers (cmOs) of thirteen dialysis provider organiza-tions in the United States, including all of the ten largest organizations, according to number of patients treated. The overarching emphases of Peer are on the ways by which provider organizations are addressing the challenges of mortality, morbidity, quality of life, and patient satisfaction, both collaboratively and within each provider organization, and on how provider organizations can learn from one another through examination of available data, all with the goal of advancing patient care. Objectivity is an important aim of Peer, with foci on the successes in the industry and on directions for improvement.
The first meeting of the CMOs was held in Chicago in March 2013, and organized by DaVita HealthCare Partners, Dialysis Clinic, Inc. (DCI), Fresenius Medical Care, and Renal Ventures Management, with Tom F. Parker III, MD, and Doug Johnson,MD, providing the initial structure.This was entirely a clinical meeting,attended by those involved daily inpatient care issues. Material waspresented on the morbidity asso-ciated with fluid overload and leftventricular hypertrophy, as well ason infectious complications, suddencardiac death, catheters for vascularaccess, and other topics affectingoutcomes. Members of the group
shared information on the differ-ent approaches used by each dialysis provider to address these and other clinical challenges.
The second meeting of the CMOs was held in Baltimore in March 2014. Participants described their efforts during the prior year and discussed new directions to further address fluid overload and congestive heart failure, infectious complications, sud-den cardiac death, dialysis bath com-position, and reduction of readmis-sion rates. The predominant feeling was that traditional quality measures are insufficient tools for achieving desired improvements. Members of the group began considering a
7
1PATIENT
POPULATIONS
20 Key observations
22 Identification of new patients in freestanding dialysis facilities
23 Rates of incident ESRD cases initiating on dialysis in freestanding facilities
24 Counts of incident ESRD cases initiating on dialysis in freestanding facilities
26 Pre-dialysis nephrology & cardiology care
28 Comparison of comorbid conditions, according to the ME Report & Medicare claims
32 Hemoglobin & estimated glomerular filtration rate at dialysis initiation
33 Vascular access at first outpatient dialysis session
6 Executive Summary
2HOSPITALIZATION
40 Key observations
42 First-year hospital admission rates among incident dialysis patients
46 Hospital admission rates among prevalent dialysis patients
50 Cardiovascular disease as the primary discharge diagnosis
52 Acute coronary syndrome (myocardial infarction & unstable angina)
54 Arrhythmia
56 Heart failure & cardiomyopathy
58 Fluid overload & pleural effusion
60 Stroke
62 Infection as the primary discharge diagnosis
64 Bacteremia & septicemia
66 Dialysis access infection, including peritonitis
68 Pneumonia & influenza
70 Intestinal infection with C. difficile
Financial support for the Peer Kidney Care Initiative is
provided by 13 participating dialysis provider organiza-
tions: American Renal Associates, Atlantic Dialysis
Management Services, Centers for Dialysis Care,
DaVita HealthCare Partners, Dialysis Clinic, Inc. (DCI), DSI
Renal, Fresenius Medical Care, Independent Dialysis
Foundation, Northwest Kidney Centers, Renal Ventures
Management, Satellite Healthcare, The Rogosin
Institute, and U.S. Renal Care.
In collaboration with the Chief Medical Officers of these
organizations, the Peer Kidney Care Initiative is operated by
the Chronic Disease Research Group, a division of the
Minneapolis Medical Research Foundation, in Minneapolis,
Minnesota. Allan Collins, MD, FACP, is the Executive Director
of Peer and Eric Weinhandl, MS, PhD candidate, is the Principal
Investigator. Allan Collins serves as a co-investigator
on Phase I and I I studies for DaVita Clinical Research. Eric Weinhandl reports no conflict
of interest. Graphic design work was provided by Susan
Everson, PhD, and Edward Constantini, MA. Analytic
support was provided by Craig Solid, PhD, Suying Li, PhD,
and David Gilberston, PhD.
Except for data regarding the 5-Star Quality Rating System, the data reported here have been supplied by the United
States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the
authors and in no way should be seen as an official policy or interpretation of the U.S.
government. The Peer Kidney Care Initiative has no affiliation
with the U.S. government.
pEEr
rEp
Ort
dia
lysi
s ca
re &
ou
tco
mes
in t
he
u.s
., 20
16
Tracking new cases of end-stage renal disease (ESrD) is challenging, because only patients who receive treatment for ESrD are reliably identified by the cmS ESrD Medical Evidence Report (form cmS-2728). Because there is no comprehensive registration system, patients with ESrD who choose not to initiate chronic dialysis are uncounted.
In this section we report on new ESRD patients in freestanding dialysis facili-ties, which provide the vast majority of dialysis treatments in the U.S. This does undercount the total number of new ESRD cases in the U.S., as we are not reporting new patients in hospital-based dialysis facilities (these patients pose an analytic challenge, with respect to the provision of inpa-tient versus outpatient dialysis, which we will address in the coming year) or new patients who immediately receive a kidney transplant. We begin with a flowchart that identifies this subset of new ESRD cases in 2011, and subsequently illustrate incident rates and counts, overall, by U.S. Census Division and by state. While incident rates have begun to decline, there is considerable geographic variation in the absolute burden of ESRD, with important implications for the capac-ity to deliver care.
Like the rates of hospitalization and mortality illustrated in subse-quent chapters, counts of new ESRD
patients vary in a cyclical manner, with the highest counts occurring in the winter and the lowest in the summer. This pattern was reported in Okinawa, Japan, in 1996 (Iseki et al, American Journal of Nephrology) and is clearly present in domestic data as well. As shown in trends by Census Division and state, the slowing of both rates and counts has been far from uniform across the country. Growth in counts continues, for example, in the Middle Atlantic Division, at 3.1 percent per year since 2004. Within the divi-sion, however, the corresponding rate of growth was 4.7 percent per year in New York, but only 1.3 percent per year in Pennsylvania.
Nephrologist care prior to dialy-sis initiation has been tracked for more than a decade through ques-tions in the Medical Evidence Report. Differences by Census Division are quite striking, with 80 percent of new patients in New England receiving pre-ESRD nephrologist care, compared to just 62 percent in the West South
Central Division. These geographic variations deserve greater attention from the physician community, as dialysis providers do not influence referral to a nephrologist prior to the start of dialysis treatment. The CKD education benefit, which became available to Medicare beneficiaries in January 2010, has been used by fewer than 2 percent of new ESRD patients (2013 USRDS ADR, page 117). This is a major concern, as poor preparation for ESRD has been reported to impact patient survival and access to home dialytic modalities. Interestingly, data from Medicare claims paint a more complex picture of nephrolo-gist care prior to dialysis initiation. Some patients appear to have seen a nephrologist only in the inpatient setting, and even in the outpatient setting, a substantial share of patients have only seen a nephrologist once or twice during the six months before dialysis initiation. These findings suggest that data from the Medical Evidence Report may overstate the progress that has been made.
The reporting of comorbidity at dialysis initiation has been a core part of the Medical Evidence Report since 1995. Several studies have noted under-reporting of comorbidity
INTRODUCTION
12
P E E R R E P O R T
D I A L Y S I S C A R E & O U T C O M E S I N T H E U N I T E D S T A T E S , 2 0 1 6
PEER KIDNEY CARE INITIATIVE
3
chap
ter
on
e pa
tiEn
t pO
pula
tiO
nS
C H A P T E R O N E
PATIENTPOPULATIONS 11
P E E R R E P O R T
D I A L Y S I S C A R E & O U T C O M E S I N T H E U N I T E D S T A T E S , 2 0 1 6
PEER KIDNEY CARE INITIATIVE
peer
rep
ort
dia
lysi
s ca
re &
ou
tco
mes
in t
he
u.s
., 20
16
0
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
2,000
4,000
6,000
8,000
10,000number of patients
Incident counts: by month
Incident counts: monthly average during the quarter
Incident counts: monthly average during the year
0
5,000
2004 2005 2006 2007 2008 2009 2010 2011
10,000
15,000
20,000
25,000
New England
Middle Atlantic
East North Central
West North Central
South Atlantic
East South Central
West South Central
Mountain
Pacific
number of patients
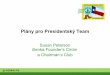
AverAge monthly counts of incident patients ini-tiating on dialysis in freestanding facilities rose steadily between 1996 and 2010, reaching a peak of more than 8,000 patients per month in 2009 and 2010. In 2011 the average monthly count actually declined, albeit by only slightly more than 1 percent. While it is uncertain whether this decline might represent an aberration due to recent economic weakness or portend a downturn in the inci-dence of Stage 5 CKD, the increasing age of the U.S. popu-lation, and the rising prevalence of diabetes, suggests the former is more likely.
Interestingly, average monthly counts of incident patients exhibit substantial seasonality, with those during the first quarter of recent years exceeding those during the third quarter by roughly 15 percent. This pattern may be due to broadly increased use of healthcare resources during the winter season, resulting in the detection of previously undiagnosed Stage 5 CKD. That more patients begin dialy-sis during the first quarter, a period marked by substantial risk of communicable disease, will be an ongoing challenge for dialysis providers. Mus acea doluptate quibusc iatemod unditas essum con perorem nIhil eatum explign
180%Increase in incident counts between 1996 & 2011
21,875Incident patients in the South Atlantic Census Division in 2011: the highest of all divisions
PATIENT POPULATIONShemoglobin, estimated glomerular filtration rate, & vascular access at initiation
2.25 Incident counts by month, quarter, & year
2.26 Incident counts by U.S. Census Division
14
Peer Kidney Care Initiative; design for 2016 Report
Susan Everson | portfolio | page 3

A map does not just chart, it unlocks and formulates meaning; it forms bridges between here and there, between disparate ideas that we did not know were previously connected.
Reif LarsenTHe SeleCteD WoRKS oF T.S. SpIVet
5
217
78 81 84 87 90 93 96 99 02 05 08 11N
umbe
r of p
atie
nts (
in th
ousa
nds)
0
50
100
150
200Hemodialysis (2011: 103,744)Peritoneal dialysis (7,438)Total dialysis (112,788)Transplant (2,855)
78 81 84 87 90 93 96 99 02 05 08 110
100
200
300
400Hemodialysis (2011: 395,656 )Peritoneal dialysis (31,684)Transplant (185,626)OPTN transplant wait list (90,474)
Incident Prevalent
page 217
nephrologist care, 30 percent began therapy with a maturing fistula and 50 percent had a mature fistula— a rate five times greater than that seen among non-referred patients.
The percentage of patients receiving an erythropoiesis stimulating agent (ESA) prior to initiation continues to change, from 33 percent in September, 2002 to 18.1 percent in 2011. This may reflect concern over potential adverse events when hemoglobin levels are targeted to a level above 11 g/dl. The mean hemoglobin at initiation of ESRD treatment also continues to change, and was 9.63 g/dl at the end of 2011. These changes place different demands on care after the initiation of dialysis. The current FDA rec-ommendations indicate that “In controlled trials, patients experienced greater risks for death, serious adverse cardio-vascular reactions, and stroke when administered eryth-ropoiesis-stimulating agents (ESAs) to target a hemoglo-bin level of greater than 11 g/dL.” “No trial has identified a hemoglobin target level, ESA dose, or dosing strategy that does not increase these risks.” The FDA recommends that clinicians “Use the lowest dose that will maintain a hemoglobin level sufficient to reduce the need for RBC transfusions.”
The percentage of dialysis patients beginning therapy with an estimated glomerular filtration rate (eGFR, calcu-lated with the CKD-EPI formula) above 15 ml/min/1.73 m2 fell in 2011, to 15.3 percent — still, however, almost three times higher than in 1996. It is not clear if the generally progressive increase has been the result of severe comor-bidity or of a simple numerical starting point based on the ability to calculate the eGFR. Concerns have recently been
raised about the usefulness of eGFR at ESRD initiation, as the lower serum creatinine used to calculate the rate may be impacted by low muscle mass in older, frail patients. Hopefully, symptoms and complications of uremia are still the primary indications for starting renal replacement therapy rather than a simple number, one which has been brought into question in recent years in controlled trials of early versus later dialysis initiation.
Biochemical data, collected on the Medical Evidence form since 2005, show that 57 percent of new patients in 2011 had an albumin less than the lower limit of normal, and the mean hemoglobin at initiation was9.7 g/dl. Total cholesterol was greater than 200 mg/dl in 16 percent of patients, while 28 percent had an LDL level greater than 100 mg/dl, and 56 percent had an HDL level less than 40 mg/dl. Among patients with diabetes, 29 percent had a hemoglobin A1c level greater than 7 percent.
Recent changes and new incentives in the bundled Prospective Payment System for dialysis patients, intro-duced in January, 2011, may alter several characteristics of the incident and prevalent populations. The mix of peritoneal dialysis and hemodialysis patients, for example, has clearly changed. It is unclear how the expansion of peritoneal dialysis will affect patient outcomes, and how the new incentives will impact the emerging daily home hemodialysis population; provider incentives for this therapy are less clear, particularly as related to training. A more detailed assessment of the bundled payment system is presented in Chapter Ten. • Figure 1.1; see page 430 for analytical methods. Incident & December 31 point prevalent ESRD patients; peritoneal dialysis consists of CAPD & CCPD.
Captain and crew, captain and crew,
Take me, oh take me to anywhere new.
Shel Silverstein“PIRAtE DREAmS”
1.1 Incident & prevalent patient counts (USRDS), by modality
vol 2
219
Num
ber o
f pat
ient
s (in
thou
sand
s)
0
10
20
30
40
50
81 84 87 90 93 96 99 02 05 08 11
Rate
per
mill
ion
popu
latio
n
0
500
1,000
1,500
2,000
0-19 20-44 45-64 65-74 75+
0-19 20-44 45-64 65-74 75+ All
Counts
Rates
Num
ber o
f pat
ient
s (in
thou
sand
s)
0
25
50
75
100
96 99 02 05 08 11
Rate
per
mill
ion
popu
latio
n
250
350
450
550
650
Counts
Rates
Non-Hispanic
Hispanic
Hispanic
Non-Hispanic
All
Num
ber o
f pat
ient
s (in
thou
sand
s)
0
20
40
60
80White Black/Af AmN AmAsian
81 84 87 90 93 96 99 02 05 08 11
Rate
per
mill
ion
popu
latio
n
0
300
600
900
1,200White Black/Af AmN AmAsian All
Counts
Rates
Num
ber o
f pat
ient
s (in
thou
sand
s)
0
10
20
30
40
50
81 84 87 90 93 96 99 02 05 08 11
Rate
per
mill
ion
popu
latio
n
0
50
100
150
200
Counts
Rates
DiabetesHypertensionGNCystic kidney
1.5 Incident counts & adjusted rates of ESRD, by race
1.7 Incident counts & adjusted rates of ESRD, by primary diagnosis
1.4 Incident counts & adjusted rates of ESRD, by age
1.6 Incident counts & adjusted rates of ESRD, by Hispanic ethnicity
Since 2000, the adjusted incident rate of ESRD has grown 7.1 percent for patients age 75 and older, to 1,707 per million population in 2011, while rates for those age 0–19 and 20–44 have increased 10.1 and 4.1 percent, respectively, to 15.6 and 127. Rates for patients age 45–64 and 65–74, in contrast, though rising slightly during the decade, are now 8.1–8.3 percent lower than in 2000, at 571 and 1,307 per million, respectively.
By race, rates for blacks/African Americans and Native Americans in 2011 were 940 and 453 per million population, respectively — 3.4 and 1.6 times greater than the rate of 280 found among whites. After rising in the middle of the decade, rates for both whites and Asians are now near the levels seen in 2000, while rates for blacks/African Americans and Native Americans are now 10.2 and 36 percent lower.
Fourteen percent of new ESRD patients in 2011 were Hispanic, up from 12.6 percent in 2007. While the rate of ESRD among Hispanics fell 3.0 percent between 2010 and 2011, to 518, it remains 1.5 times greater than that seen in the non-Hispanic population.
At 157 per million population in 2011, the rate of new ESRD cases due to dia-betes is 4.2 percent lower than in the previous year, and has now fallen back to a level not seen since 1998. The rate of ESRD due to hypertension, while down 4.9 percent in 2011, is 2.6 percent higher than the 2000 rate, at 101, while the rate of ESRD due to glomerulonephritis has fallen 29 percent, to 23 per million. • Figures 1.4–7; see page 430 for ana-lytical methods. Incident ESRD patients. Adj: gender/race (1.4), age/gender (1.5–6), age/gender/race (1.7); ref: 2010 ESRD patients.
vol 2
vol 2
vol 2
vol 2
incident counts & adjusted rates
17
Generalpopulation
(no CKD)
Generalpopulation
(no CKD)
All CKD
All CKD
ESRD
ESRD
$2,167
$417
$3,949
$613
$5,851
$422
CKD: 2011 No CKD: 2011
CHF 42.9%
CVA/TIA 26.7%
AMI 15.1%
None 38.7% None 61.7%
CHF 18.5%
CVA/TIA 20.3%
AMI 6.4%
CKD: $45.5 billionMedicare total: $249.8 billion
1% CKD + diabetes: $24.6 billionMedicare diabetes: $85.9 billion
CKD + CHF: $21.2 billionMedicare CHF: $54.7 billion
67% of CKD patients with CHF receive a BETA BLOCKER
52% of CKD patients with CHF receive an ACEI/ARB
58% of CKD patients with a stroke receive a STATIN
76% of CKD patients with AMIreceive a BETA BLOCKER
COSTS top three drug classes used by Part D enrollees with CKD
$394 million insulin
$302 million antiplatelet drugs
$264 millionstatins 20.0%
of total MedicarePart D drug costs in 2011
NET PART D COSTS FOR MEDICARE CKD PATIENTS IN 2011
$5.26BILLION
JANUARY 1, 2006: MEDICARE PART D GOES INTO EFFECTto help subsidize the costs of prescription drugs in Medicare bene� ciaries
Circle diagram: Figure 4.1Medication use: Table 4.bMedication costs: Figure 7.18Total Part D costs: Figure 5.9PPPY & OOP costs: Figure 5.10Costs of patient care: Figure 7.5–7
Costs of caring for patients with CKD in 2011(fee-for-service Medicare patients age 65 & older)
Overall, patIents wIth CKD account for 18% of total MedIcare expendItures
CKD patIents wIth dIabetes account for 29% of MedIcare dIabetes expendItures
CKD patIents wIth congestIve heart faIlure account for 39% of MedIcare CHF expendItures
Per person per year Medicare Part D costs, 2011
Per person per year out-of-pocket Part D costs, 2011
8.3%
6.3%
5.5%
CVD patients with CKD carry a larger burden of cardiovascular disease than those without CKD.
funding Production of this Annual Data Report (aDR) was solely funded through nIH contract HHSn 267 2007 15002c / no1-DK-7-5002 with the Min-neapolis Medical Research Foundation (mmRF). Most contributors to this report are employed by mmRF, with many of the physician investigators being employed by mmRF’s parent organization, Hennepin Healthcare System, Inc. mmRF has enacted conflict of interest (CoI) policies and practices governing the conduct of research within the USRDS and of other research not related to the USRDS. In addi-tion to internal controls, USRDS work is overseen by nIDDK Project Officers, the USRDS Steering Committee, and the USRDS External Expert Panel. Listed here are those who contributed to the 2013 aDR. Unless otherwise noted in parentheses, the contributor’s employer was mmRF or its parent organization, Hennepin Healthcare System, Inc.
chapter contributors directors & co-investigators Allan Collins, mD, FaCp, USRDS Director (entire aDR). Robert Foley, mB, mSc, USRDS Deputy Director (entire aDR). Blanche Chavers, mD (University of Minnesota School of Medicine; Vol 2, Ch 8). David Gilbertson, phD (entire aDR). Charles Herzog, mD (Vol 1, Ch 4; Vol 2, Ch 4). Kirsten Johansen, mD (University of California at San Francisco; Vol 2, Ch 9). Bertram Kasiske, mD (Vol 2, Ch 7). Nancy Kutner, phD (Emory University; Vol 2, Ch 9). Suying Li, phD (Vol 1, Ch 3; Vol 2, Précis & Chs 5 & 8; H & I tables). Jiannong Liu, phD (maps; Vol 2, Ch 10). Wendy St. Peter, PharmD, BCpS (Vol 1, Chs 5 & 7; Vol 2, Chs 6 & 11). Jon Snyder, phD (Vol 2, Ch 7). Craig Solid, phD (entire aDR). staff administrative staff » Beth Forrest, BBa (Vol 2, Hp2020, Ch 12). adr production » Delaney Berrini, BS (entire aDR), Edward Constantini, ma (entire aDR). Susan Everson, phD (entire aDR). biostatisticians » Haifeng Guo, mS (Vol 1, Ch 2; Vol 2, Hp2020, Chs 2, 8, & 10). Yan Hu, mS (Vol 1, Ch 4; Vol 2, Hp2020 & Ch 4). Allyson Kats, mS (Vol 1, Ch 1. B tables; Vol 2, Hp2020). Shuling Li, phD (Vol 1, Ch 4; Vol 2, Hp2020 & Ch 4). Julia Molony, mS (Vol 1, Chs 2 & 6). Tricia Roberts, mS (Vol 1, Ch 3; Vol 2, Précis & Chs 3, 5, & 8; G tables). Melissa Skeans, mS (Vol 2, Précis, Hp2020, Chs 1 & 7; e & F tables). Bryn Thompson, Ba (Vol 2, Ch 7; e tables). Eric Weinhandl, mS (Vol 1, Ch 5; Vol 2, Hp2020 & Chs 4 & 8). Hui Xiong, mS (maps). Akeem Yusuf, phD (Vol 1, Chs 5 & 7; Vol 2, Chs 6 & 11). David Zaun, mS (Vol 1, Ch 2; Vol 2, Chs 2 & 10). information systems & software development » for all chapters, with additional work as noted: Cheryl Arko, Ba. Shu-Cheng Chen, mS, mpH (Vol 2, Précis & Ch 1; D tables). Frank Daniels, BS. James Ebben, BS (Vol 1, Ch 2; Vol 2, Précis & Ch 10). Eric Frazier, BS (Vol 2, Précis, Hp2020, Chs 1, 2, & 8; a, B, C, m tables). Roger Johnson. C. Daniel Sheets, BS. Xinyue Wang, Ba/BS.
disclosures for potential conflicts of interest Allan Collins, Md, facP » Consultant/honoraria: Abbott Laboratories, Amgen, Keryx, NxStage, Takeda. Robert Foley, MB, Msc » Consultant/honoraria: 21st Services, Baxter, Keryx, Medtronic, Novartis, Vifor Pharma. David Gilbertson, Phd » Consultant/honoraria: DaVita Clinical Research, GlaxoSmithKline. Blanche Chavers, Md » Consultant/honoraria: Alexion. Charles Herzog, Md » Consultant/honoraria: Abbott, AbbVie, Affymax, Amgen, Fibro-gen, Keryx, Medtronic, UpToDate. Equity ownership: Boston Scientific, Cambridge Heart, Johnson & Johnson, Merck. Trustee: RoFaR. Kirsten Johansen, Md » Consultant/honoraria: Amgen. Bertram Kasiske, Md » Consultant/honoraria: Chugai, Janssen, Kidney Disease: Improving Global Outcomes (KDIGo), Litholink/LabCorp, Merck.
Also, mmRF as an institution has separate contracts to conduct other, independent research funded by the Agency for Healthcare Research and Quality (via subcontract with Johns Hopkins University), Affymax, Amgen, Concert, DaVita, Gilead, the Health Resources and Services Administration, Hennepin Healthcare System, Keryx, the National Institute on Aging/National Institutes of Health, the National Kidney Foundation, Novartis, NxStage, Ortho-McNeil-Janssen, Questcor, Takeda, and Zoll Medical Corporation.
This twenty-fifth annual report of the United States Renal Data System is produced by the USRDS Coordinating Center, operated under nIH contract HHSn 267 2007 15002c / no1-DK-7-5002 by the Minneapolis Medical Research Foundation. Suggested citation for this report U.S. Renal Data System, USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, mD, 2013. Publications based upon data reported here or supplied upon requ est must include this citation and the following notice The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. government.
4
216
218 incident counts & rates 220 incident rates & racial
differences 222 prevalent counts &
rates; modalities 224 incident & prevalent
modality 226 patient
characteristics 228 summary
2013USRDSannualdatareport
volume twoesrdincidence, prevalence, modalitiesintroduction
in 2011, the number of new patients starting therapy on hemodialysis declined 1.5 percent, the first decrease in more than three decades. The population initiating on peritoneal dialysis, in contrast, grew for the
third year in a row, and now accounts for 6.6 percent of patients with a known dialysis modality. This change is associated with the new bundled payment system, with its clear incentives for peritoneal dialysis. The number of total incident dialysis patients was 112,788, while 2,855 patients received a preemptive transplant as their first ESRD modality; a total of 115,643 patients thus began ESRD therapy in 2011 — a level below that of the two prior years.
The rate of new ESRD cases per million population, relatively stable since 2000, fell 3.8 percent in 2011, to 357. Growth in counts and rates has dropped across all age groups, though, as late reporting of cases can cause slight changes in the numbers, this finding needs to be confirmed in coming years.
The incidence of ESRD in the black/African American population has been declining for the last five years. The rate also continues to fall among Native Americans, reaching a level just 13.5 percent higher than that in the Asian population — the smallest difference in more than three decades. By cause, rates of incident ESRD have fallen across each of the major primary diagnoses: diabetes, hypertension, glomerulonephritis, and cystic diseases. Among those whose ESRD is caused by diabetes, however, racial disparities persist, particularly among younger blacks/African Americans.
The December 31, 2011 prevalent population included 430,273 patients on dialysis and 185,626 patients with a functioning kidney transplant, and the one-year growth of 3.4 percent — to 615,899 — was the smallest in 30 years. The rate of prevalent ESRD cases per million population reached 1,901, an increase of 1.3 percent from 2010, and also the slowest growth in the last three decades. The number of patients receiving home hemodialysis continued to grow, though at a slower pace in 2011.
Insurance coverage in the dialysis population continues to change, with more incident dialysis patients now covered by Medicare Advantage. Private insurance, in contrast, is dominant among patients who receive a preemp-tive kidney transplant. In the 2011 prevalent population, 84 percent of hemodialysis patients and 81 percent of those on peritoneal dialysis had some type of primary Medicare coverage, compared to just 53 percent of those with a transplant.
Since 2005, when new fields on the revised Medical Evidence form (2728) made it possible to analyze pre-ESRD treatment, there has been little improvement in the care patients receive prior to initiation of ther-apy. Forty-two percent of new ESRD patients in 2011, for example, had not seen a nephrologist prior to beginning therapy. And among these patients, 51 percent of those on hemodialysis began therapy with a cath-eter only, compared to 19 percent of those who had received more than a year of nephrology care. Among those with a year or more of pre-ESRD
2013 USRDS annUal
Data RepoRtVolUme one
Atlas of Chronic Kidney Disease in the United States
215 218
2013USRDSannualdatareport
volume twoesrd
81 84 87 90 93 96 99 02 05 08 11
Bars
: Rat
e pe
r mill
ion
popu
latio
n
0
100
200
300
400
Sym
bols
: one
-yea
r % c
hang
e
-5
0
5
10
15line: add’l adjustment for Hispanic ethnicity
10
16
16
17
11 21
3
6
7
8
91217/18
15
14
13
4
5
279.0 448.8310.3 337.3 366.9 408.8
incidence, prevalence, modalitiesincident counts �rates
In 2011, the adjusted incident rate of ESRD averaged 449 per million popu-lation in the upper quintile and was highest in areas of the Ohio Valley, and in portions of Texas and California. • Figure 1.3; see page 430 for analytical methods. Incident ESRD patients. Adj: age/gender/race/Hispanic ethnicity; ref: 2010 ESRD patients.
With an overall rate for incident dialysis patients of 349 per million population in 2011, rates by network range from 228 in Network 16 to 427 in Network 8. The distribu-tion of patients by race continues to vary widely across the country. Blacks/African Americans, for example, constitute just 6.4 percent of the new dialysis population in Network 16, but 54 percent of patients in Network 6. • Table 1.a; see page 430 for analytical methods. Incident dialysis patients, 2011. Adj: age/gender/race; ref: 2010 patients.
“.” Zero values in this cell.
After a 1.9 percent decrease in 2010, the incident rate of ESRD (adjusted for age, gender, and race) continued to decline, falling 3.8 percent in 2011 to 357 per million population. Since 2000, changes in the adjusted rate have shown little variation, but the 2011 adjusted rate is the lowest since 1998. Ethnicity was added to the Medical Evidence form in 1995. When adjusted
for Hispanic ethnicity, rates differ little from those adjusted for age, gender, and race alone. In 2005, for example, the incident rate including ethnicity was o.5 percent greater, and in 2011 it was 0.2 percent less, at 356.4 per mil-lion population compared to 357.1. • Figure 1.2; see page 430 for analytical methods. Incident ESRD patients. Adj: age/gender/race; ref: 2010 ESRD patients.
1.2 Adjusted incident rates of ESRD & annual percent change 1.3 Geographic variations in adj. inc. rates
of ESRD per million pop., 2011, by HSAvol 2
vol 2
vol 2
Network 1 Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, Vermont
Network 2 New YorkNetwork 3 New Jersey, Puerto Rico, Virgin IslandsNetwork 4 Delaware, Pennsylvania Network 5 Maryland, Virginia, Washington D.C., West VirginiaNetwork 6 Georgia, North Carolina, South Carolina Network 7 Florida Network 8 Alabama, Mississippi, Tennessee Network 9 Indiana, Kentucky, OhioNetwork 10 IllinoisNetwork 11 Michigan, Minnesota, North Dakota,
South Dakota, Wisconsin Network 12 Iowa, Kansas, Missouri, NebraskaNetwork 13 Arkansas, Louisiana, OklahomaNetwork 14 TexasNetwork 15 Arizona, Colorado, Nevada, New Mexico, Utah,
WyomingNetwork 16 Alaska, Idaho, Montana, Oregon, WashingtonNetwork 17 American Samoa, Northern California, Guam,
Hawaii Network 18 Southern California
1.a Patient demographics & adjusted rates, by ESRD network: incident dialysis patients, 2011
All % of Rate per Mean % % % % % % pts total million age DM White Af Am N Am Asian Hisp.1 3,628 3.2 246.2 65.2 40.5 81.0 15.1 0.2 3.6 8.82 6,727 6.0 334.9 63.9 41.0 59.5 32.4 0.3 6.1 13.73 5,035 4.5 397.2 64.9 50.1 70.3 25.5 0.1 3.9 37.34 5,118 4.5 369.7 65.1 42.4 73.8 24.4 0.1 1.6 3.95 6,492 5.8 383.0 62.2 39.7 48.9 46.0 0.2 3.0 3.26 9,571 8.5 386.8 60.9 42.3 43.1 54.4 0.6 1.5 2.47 7,447 6.6 382.2 64.2 41.5 65.8 31.7 0.2 2.0 15.68 6,159 5.5 427.5 61.2 42.8 51.0 48.1 0.3 0.6 0.59 8,780 7.8 385.0 64.0 44.9 75.0 23.7 0.1 0.9 1.910 4,862 4.3 365.4 63.7 39.6 63.5 31.2 0.1 3.3 10.711 7,054 6.3 308.1 63.7 39.5 72.2 22.0 3.0 2.5 3.512 4,322 3.8 303.2 63.6 38.8 76.5 19.7 0.7 1.3 3.313 4,506 4.0 392.6 61.1 44.8 53.2 41.2 4.3 1.1 2.614 9,600 8.5 368.5 60.2 53.4 73.0 24.2 0.2 2.4 41.815 5,389 4.8 266.0 61.7 50.8 76.6 9.0 9.0 4.8 24.916 3,260 2.9 227.9 62.4 43.7 81.1 6.4 3.9 8.3 8.417 5,445 4.8 330.4 62.0 50.9 58.4 11.9 0.7 28.1 21.118 9,371 8.3 388.7 62.4 50.0 72.3 13.8 0.5 12.7 42.4Unk 22 0.0 . 57.7 0.0 4.6 0.0 0.0 9.1 0.0All 112,788 100 348.8 62.7 44.7 65.4 28.0 1.2 4.7 15.0
16
2013USRDSannualdatareport
volume oneckd
0 100 200 300 400 500
Stage 1-2
Stage 3
Stage 4-5576
416
361Hospitalizations per1,000 patient years
0 20 40 60 80 100
.
109
64
65Stage 1-2
Stage 3
Stage 4-5
Deaths per 1,000patient years
Medicare patients age 65 and older are twice as likely to see a cardiologist as a nephrologist following any diagnosis for CKD. Among patients with a CKD diagnosis of Stage 3 or higher, approximately two-thirds see either a cardiologist or nephrologist in the year following the diagnosis.
Patients who see a primary care physician93% 93%
63%
31%
Patients who see a
cardiologist
Patients who see a
nephrologist
All CKD CKD code of 585.3 or hIgher
64%
57%
Hospitalization rates
All-cause rehospitalization Rehospitalization after all-cause index hospitalization
Rehospitalization after cardiovascular index hospitalization
Mortality rates
No CKD
Generalpopulation
(no CKD)
Generalpopulation
(no CKD)
Generalpopulation
(no CKD)
No CKDAll CKD
All CKD All CKD All CKDHemodialysis 585.1–2 585.1–2585.3 585.3585.4–5 585.4–5
All CKD
38% HIGHER 37% HIGHER
adjusted all-cause HOSPITALIZATION AND MORTALITY RATESare HIGHER IN CKD PATIENTS than in those without the disease
adjusted rates of REHOSPITALIZATION are also
HIGHER IN CKD PATIENTS than in those without the disease
307
17.4% 17.4% 17.8%
54423
24.1% 24.1% 24.8%24.0% 25.3%33.4% 22.5% 24.0%26.4% 26.8%
74
Physician care: Tables 2.g–hAcute kidney injury: Figures 6.3–4Hospitalization: Table 3.aMortality: Table 3.cRehospitalization: Figures 3.1 & 3.9–10
Acute kidney injury is highly associated with age, & rates of � rst AKI (per 1,000 patient years at risk) have increased
Patients rehospitalized within 30 days of a live hospital discharge (age 66 & older)
Truven Health ClInformatIcs MedIcare MarketScan DataMart 2001 2011 2001 2011 2001 201120-44 0.15 0.65 0.14 0.6545-54 0.47 1.82 0.45 1.8154-64 1.06 4.31 1.09 4.366-69 3.7 14.970-74 4.9 18.875-79 6.6 26.480-84 8.0 35.985+ 9.6 49.6
WhIte 5.7 25.8Black/Af Am 11.9 45.3
c onic kney diseasein tHe United states
USRDS Coordinating Center 701 Park Avenue Suite S2.100 Minneapolis, MN 55415 1.888.99USRDS www.usr
ds.o
rg
Uni
ted
Stat
es R
enal D
ata System 2013 Annual Data Report
Atlas of CKD & ESRD in the U.S.
2013 United States Renal Data System Annual Data Report
Susan Everson | portfolio | page 4

précis: an introduction to ESRD in the u.s. » 165
healthy people 2020 » 193recommended care among patients with AKI, diabetes, & CKD;
acei/arb treatment; esrd incidence; kidney failure due to diabetes; nephrologist care; vascular access; transplantation; mortality
1 incidence, prevalence, patient characteristics, & treatment modalities » 215
incident counts & rates; incident rates & racial differences; prevalent counts & rates; incident & prevalent modality; patient characteristics
2 clinical indicators & preventive care » 229anemia treatment; preventive care; vascular access
3 hospitalization » 237overall hospitalization; rehospitalization; admission rates by interdialytic interval
4 cardiovascular disease » 247sudden cardiac death in incident & prevalent dialysis patients; defibrillators & survival after a cardiac event; cardiovascular disease diagnostic testing in ESRD
patients; medication & survival in ESRD patients with cardiovascular disease
5 mortality » 259mortality & survival ; mortality in the general & ESRD populations; mortality rates by interdialytic interval
6 Part D prescription drug coverage in ESRD patients » 269Part D enrollment patterns; Part D coverage plans; overall costs of Part D enrollment;
coverage phase analyses for Part D enrollees; Part D prescription drug use & costs
7 transplantation » 283wait list; donation; transplant; outcomes; follow-up care;
Part D medications in kidney transplant recipients
8 pediatric esrd » 295ESRD diagnosis in the pediatric population; infections; vaccinations;
hospitalization & mortality; pediatric ESRD in the United States & Canada
9 rehabilitation/quality of life & nutrition special studies » 309 Comprehensive Dialysis Study; early awareness of peritoneal
dialysis & transplant as treatment options
10 esrd providers » 319provider growth; preventive care; treatment under the new dialysis
composite rate; standardized hospitalization & mortality ratios
11 costs of esrd » 329overall costs of ESRD & injectables; racial differences; matched & unmatched
dialysis populations; Medicare Part D costs; Medicare Part a, b, & d costs
12 international comparisons » 341worldwide view of the incidence of esrd; incidence of esrd;
prevalence of esrd; dialysis; transplantation
volume twoAtlas of End-Stage Renal Disease in the United States
7
list of ESRD figures & tables appearing each year » 152
ESRD program highlights » 154
overview of ESRD in the u.s. » 156
hospitalization & Part D use in the ESRD population » 158
introduction » 160
chapters » 165
reference tables: ESRD » 353
analytical methods » 421
USRDS products & services » 454
glossary » 460
CMS forms » 467
colophon » 476
data requests » 454
agreement for release of data » 463
merged dataset agreement for release of data » 465
All CKD inNHANES 2005-2010
eGFR <60 mls/min/1.73 m2 in NHANES 2005-2010
ACR ≥30 mg/g inNHANES 2005-2010
DM 9.3%
CKD 13.1%
CVD 8.5%DM 9.3%
CKD 6.3%
CVD 8.5%DM 9.3%
CKD 9.2%
CVD 8.5%
25
in the Medicare population, but has been shown to have high specificity, indicating individuals likely to have the disease. As identified from these codes within the 2010 prevalent popula-tion, CKD is recognized in 9.2 percent of older Medicare patients, and 1.4 percent of the younger employed population. When CKD patients newly identified during the year are included as well, CKD represents 11.9 percent of the Medicare population, and accounts for 27.5 percent of fee-for-service costs (see see Figure p.1 in the Volume Two Précis). When added to costs for ESRD patients, it appears that 35 percent of all Medicare expendi-tures are incurred by patients with a diagnosis of kidney disease.
Despite this high disease burden, the rate of progression to ESRD has been relatively stable over the last several years, sug-gesting that CKD patients are dying at a higher rate before they reach ESRD or that they are progressing to ESRD at a slower rate. The continuing decline in rates of death from cardiovascular disease (the major cause of mortality in the CKD population), along with improved treatment and control of hypertension and increased use of ACEIs/ARBs/renin inhibitors, suggest that progression of CKD to ESRD may indeed have slowed.
Care of CKD patients after diagnosis is challenging to assess. In the Medicare CKD population (age 65 and older), it appears that 93 percent see a primary care physician within a year of diagnosis, while 64 percent visit a cardiologist; only 31 percent, however, see a nephrologist. When restricted to patients with CKD of Stages 3–5 (based on diagnosis codes), these rates reach 93, 65, and 60 percent. Similar data are reported for the employed population. And as we show in Chapter Two, only one-third of patients with diabetes, and 5 percent of those with hypertension, receive a urine albumin test within a year, despite the fact that these measurements are recommended by the American Diabe-tes Association and the American Heart Association.
Rates of hospitalization, and of rehospitalization within 30 days, are progressively higher with advancing CKD. The issue of rehospitalization has received more attention for patients in the general population than for those with CKD, despite the fact that the rate for CKD patients is almost 40 percent higher. The rate accelerates as patients approach ESRD, reaching 43 percent in the month prior to ESRD initiation. These data show the sub-stantial burden of disease and needed care in the CKD popula-tion, burdens illustrated as well in our data on mortality and cardiovascular disease in CKD patients.
New figures show that, when compared to the general pop-ulation, Medicare Part D prescription drug use for those with CKD is dominated by diuretics, statins, beta blockers, ACEIs, and calcium channel blockers. Interestingly, thyroid replace-ment therapy is very common in the CKD population, a fact which has received little attention.
This year we again highlight data on acute kidney injury (AKI). In both the Medicare and employed populations, rates of AKI rise with age. Recurrent hospitalizations for AKI are com-mon, with rates reaching 28 percent for patients whose original AKI did not require dialysis, and 33 percent for those dialyzed during the original hospitalization; these numbers rise to 34 and 49 percent for blacks/African Americans. The rate of out-patient follow-up with a nephrologist in the year following AKI, however, is barely 20 percent.
Drug treatment changes considerably after an AKI event. The use of ACEIs/ARBs, for example, declines in the three months after discharge, but returns to the pre-AKI rate. It does not, however, exceed this initial rate, despite that fact that CKD has progressed. » Figure 1.1; see page 140 for analytical methods. NHANES participants 2005–2010, age 20 & older; eGFR calculated using CKD-EPI equation; urine albumin creatinine ratio (ACR).
1.1 Distribution of NHANES participants with diabetes,
congestive heart failure, & markers of CKD, 2005–2010vol 1
1988-1994 2005-20100
20
40
60
1988-1994 2005-2010 1988-1994 2005-2010
All CKD eGFR <60 ml/min ACR ≥30 mg/g
Perc
ent
0
10
20
30
40
50
1988-1994 2005-2010 1988-1994 2005-2010 1988-1994 2005-2010
All CKD eGFR <60 ml/min ACR ≥30 mg/g
Perc
ent
Perc
ent o
f pat
ient
s
0
20
40
60
80
100
1988-1994 2005-2010 1988-1994 2005-2010 1988-1994 2005-2010
All CKD eGFR <60 ml/min ACR ≥30 mg/g
0
20
40
60
1988-1994 2005-2010 1988-1994 2005-2010 1988-1994 2005-2010
All CKD eGFR <60 ml/min ACR ≥30 mg/g
Perc
ent
27
P
1.12 NHANES participants at
target blood pressure 1.13 NHANES participants within
LDL cholesterol target range
1.14 NHANES participants within
HDL cholesterol target range 1.15 NHANES participants with
glycohemoglobin <7%
vol 1 vol 1
vol 1 vol 1
Between 1988–1994 and 2005–2010, management of hyper-tension, hyperlipidemia, hyperglycemia, and diabetes in the NHANES cohorts improved, regardless of how CKD is defined — by eGFR or by ACR. » Figures 1.12–15; see page 140 for analytical methods. NHANES III (1988–1994) & 2005–2010 partici-pants age 20 & older; dialysis patients excluded from NHANES 2005–2010; eGFR calculated using CKD-EPI equation; urine albumin/creatinine ratio (ACR).
outcomes 432 adjusted hospitalization rate in white Medicare
ckd patients age 66 & older, 2010 (admissions per 1,000 patient years; Figure 3.3)Stage 1–2: 371 » Stage 3: 430 » Stage 4–5: 596
481 adjusted hospitalization rate in black/African American Medicare ckd patients age 66 & older, 2010 (admissions per 1,000 patient years; Figure 3.3)Stage 1–2: 395 » Stage 3: 470 » Stage 4–5: 598
78 adjusted mortality rate in white Medicare ckd patients age 66 & older, 2010 (deaths per 1,000 patient years; Table 3.c)Stage 1–2: 55 » Stage 3: 70 » Stage 4–5: 121
71 adjusted mortality rate in black/African American Medicare ckd patients age 66 & older, 2010 (deaths per 1,000 patient years; Table 3.c)Stage 1–2: 80 » Stage 3: 67 » Stage 4–5: 91
expenditures $4.5
billion
total net Part D payment for Medicare enrollees with ckd, 2010 (Figure 5.9)
$3,843 per person per year Medicare Part D costs for enrollees with ckd, 2010 (Figure 5.10)
$738 per person per year out-of-pocket Part D costs for enrollees with ckd, 2010 (Figure 5.1)
$41billion
total Medicare expenditures for ckd, 2010 (Figure 7.5)Non-Part D: $37.7 billion » Part D: $3.3 billion
$22.1billion
Medicare expenditures for patients with ckd & diabetes, 2010 (Figure 7.6)Non-Part D: $20.0 billion » Part D: $2.1 billion
$19.4billion
Medicare expenditures for patients with ckd & congestive heart failure, 2010 (Figure 7.7)Non-Part D: $18.1 billion » Part D: $1.4 billion
$22,323 per person per year expenditures for ckd patients in the general Medicare population, 2010 (includes Part D; Figure 7.8)non-DM/non-CHF: $15,607 » CKD + DM + CHF: $37,490
13
volume oneAtlas of Chronic Kidney Disease in the United States
6
précis: an introduction to CKD in the u.s. » 23
1 CKD in the general population » 41prevalence of CKD; comorbidity; awareness,
treatment, & control; predicting death
2 identification & care of patients with CKD » 51prevalence of recognized CKD; laboratory testing of patients at risk for CKD; probability & odds of a CKD diagnosis code; probability & odds of
seeing a physician after CKD diagnosis; prescription drug therapy
3 morbidity & mortality in patients with CKD » 65hospitalization rates in CKD & non-CKD patients;
rehospitalization ; mortality rates
4 cardiovascular disease in patients with CKD » 75diagnostic testing & cardiovascular mortality;
medication use & survival in patients with cvd
5 Part D prescription drug coverage in patients with ckd » 83Part D enrollment patterns in patients with CKD; Part D coverage
plans; overall costs of Part D enrollment; coverage phase analyses for Part D enrollees; Part D prescription drug use & costs
6 acute kidney injury » 97characteristics of patients with AKI; AKI hospitalization; patient care & outcomes
following AKI hospitalization; changes in CKD status following AKI hospitalization
7 costs of CKD » 109overall costs of chronic kidney disease; Medicare Part D
costs; PPPY Medicare Part D costs; drug utilization
guide to topics in the ADR » 8
list of CKD figures & tables appearing each year » 10
Volume One highlights » 12
overview of CKD in the u.s. » 14
introduction » 18
chapters » 23
reference tables: CKD » 119
analytical methods » 137
2012USRDSannualDataRepoRt
volumeCKD
24
Précis: an introduction to chronic kidney disease in the united states
1
introductionintroduction
For many years the World Health Organization has stressed that the primary threat to public health in this century lies in four major chronic diseases: dia-
betes, cardiovascular disease, chronic lung disease, and cancer. These conditions now account for the majority of deaths not only in high-income countries but in the middle- and now the low-income nations as well.
By reducing alcohol and tobacco use, controlling salt and calorie intake, and combating a sedentary lifestyle, these diseases are largely preventable. In Sep-tember, 2011, the United Nations held a summit on chronic diseases, looking at how member states can address their impact, and discussing the widespread problems of premature loss of life, loss of economic productivity, and financial stress on families, which can contribute to advancing poverty. For the first time, because of its impact on morbidity and mortality and its substantial cost to the healthcare system, chronic kidney disease was added to the list of major diseases.
All countries now recognize the substantial impact of an increasing popula-tion with kidney failure, people who face premature death if they do not receive dialysis or a kidney transplant. The reality is that many countries struggle with the costs of providing end-stage renal disease (ESRD) care, costs which place min-istries of finance at odds with ministries of health. The demand for transplant organs has led to the emergence of transplant tourism, with the buying and selling of organs. Some have expressed that a regulated market system would help fill this demand. Others suggest that prevention is a more sustainable approach, for with-out it the need will continue to grow, outpacing the pool of potential donors and increasing the known risks of the exploitation of poor populations at the expense of the wealthy. While the Istanbul Declaration on organ trafficking and transplant tourism has denounced the practice, the large number of patients across the globe who have advancing kidney disease continues to fuel demand.
The growing number of ESRD patients thus needs to be addressed in terms not only of its public health disease burden, but of its costs to the healthcare system, and of the high demand for replacement organs. And the overall prevention of kidney disease needs to be viewed in context of competing demands for resources, particularly in the difficult economic times currently faced around the world.
As shown in the Venn diagrams on the next page, 9.3 and 8.5 percent of patients in the general population had diabetes and cardiovascular disease, respectively, in 2010, while 13.1 percent had CKD, defined by an estimated GFR less than 60 ml/min/1.73 m2 or a urine albumin-to-creatinine ratio (ACR) of 30 mg/g or higher. Using only the eGFR, CKD prevalence was 6.3 percent; using only the ACR, it reached 9.2 percent — on a par with diabetes and cardiovascular disease. There is now substantial evidence that both eGFR and urine ACR are predictors of all-cause death, cardiovascular events, and ESRD (Lancet 2010).
With diabetes and hypertension known to be major risk factors for CKD, the awareness, treatment, and control of these conditions are crucial. NHANES data show that blood pressure control in the general population improved between 1988–1995 and 2005–2010, reaching almost 50 percent. LDL cholesterol control increased from 25 to 33 percent, while glycemic control rose from 31 to 48 percent overall, and from 37 to 58 percent in patients whose CKD is defined by an eGFR less than 60. These improvements in treatment and control may be contributing to the flat ESRD rate, despite the greater burden of diabetes in the general population.
While CKD has been characterized from population-level estimates in the NHANES data, much of the disease is silent and unrecognized, complicating any full assessment of its impact. We present data on CKD recognized through diag-nosis codes reported on claims — an approach which clearly underestimates CKD
The river was cut by the
world’s great flood and
runs over rocks from the
basement of time. On some
of those rocks are timeless
raindrops. Under the rocks
are the words, and some
of the words are theirs. I
am haunted by waters.
NoRmaN maCleaN,A River Runs Through It
26 CKD in the general population
28 identification & care of patients with CKD
30 hospitalization
32 cardiovascular disease
35 Part D prescription drug coverage
36 acute kidney injury
39 costs of chronic kidney disease
volume oneUSRDS Annual Data Report
Atlas of Chronic Kidney Diseasein the United States
national institutes of healthnational institute of diabetes & digestive & kidney diseases
division of kidney, urologic, & hematologic diseases
Grand Canyon National Park, Utah
an introduction to chronic kidney disease in the u.s.
23
USRDS Annual Data ReportAtlas of Chronic Kidney Disease
and End-Stage Renal Disease in the United States
NIH PUBLICATION NO.09-3176OCTOBER, 2012
2012 Annual D
ata Report
un
ited sta
tes r
en
al d
ata sy
stem
Diabetes Hypertension
eGFR<60 19.3% 8.6% 4.1%
10.9% 2.1%
ACR ≥30 29.9%
eGFR<60 12.9% ACR ≥30
14.8%
Cardiovascular disease
eGFR<60 27.9% ACR ≥30
24.3%
BMI ≥30 kg/m2
eGFR<60 7.4%
ACR ≥30 11.7%
Précis: an introduction to chronic kidney disease in the united states
2012USRDSannualDataRepoRt
volumeCKD
26
1
CKD in the general population
Between 1988–1994 and 2005–2010, the overall prevalence estimate for CKD — defined by an eGFR <60 ml/ min/1.73 m2 or an ACR ≥30 mg/g — rose from 12.3 to 14.0 percent. The larg-est relative increase, from 25.4 to 40.8 percent, was seen in those with cardiovascular disease. For eGFR <60, prevalence rose from 4.9 to 6.7 percent, with the largest increase in those age 40–59; for ACR ≥30 mg/g, the estimate rose from 8.8 to 9.4. » Table 1.a; see page 140 for analytical methods. NHANES III (1988–1994) & 2005–2010 participants age 20 & older; eGFR calculated using CKD-EPI equation; urine albumin creatinine ratio (ACR).
1.a Prevalence (%) of CKD in the NHANES population within
age, gender, race/ethnicity, & risk-factor categoriesvol 1
All CKD eGFR <60 ml/min/1.73m2 ACR ≥30 mg/g 1988–1994 2005–2010 1988–1994 2005–2010 1988–1994 2005–2010
20-39 5.1 5.7 0.1 0.2 5.0 5.740-59 8.4 9.1 1.3 2.2 7.7 7.660+ 32.2 35.0 19.5 24.1 18.3 18.4Male 10.2 12.1 4.1 5.6 7.4 8.6Female 14.2 15.8 5.6 7.7 10.2 10.2Non-Hispanic white 12.3 14.3 5.5 7.9 8.2 8.6Non-Hispanic Blk/Af Am 14.5 16.0 4.1 6.2 12.7 12.6Other 10.5 11.9 2.2 2.6 9.2 10.6Diabetes 43.1 40.1 15.6 19.3 36.3 29.9Self-reported diabetes 42.7 41.6 16.4 20.4 35.9 30.8Hypertension 22.2 23.2 10.4 12.9 15.4 14.8Self-reported hypertension 25.3 26.8 12.9 15.6 17.1 16.7CVD 25.4 40.8 14.5 27.9 16.6 24.3BMI ≥30 16.6 16.8 6.2 7.4 12.3 11.7All 12.3 14.0 4.9 6.7 8.8 9.4
1.11 Distribution of markers of CKD in NHANES participants with diabetes,
hypertension, cardiovascular disease, & obesity, 2005–2010vol 1Here we look at several subgroups
of NHANES 2005–2010 participants, showing the percentage in each popu-lation with an eGFR <60 m/min/1.73 m2 and an ACR ≥30 mg/g. Nearly 28 percent of participants with cardiovascular dis-ease (CVD) had an eGFR less than 60, compared to 19.3, 12.9, and 7.4 percent of those with diabetes, hypertension, and a high body mass index, respec-tively. Participants with diabetes were the most likely to have an ACR ≥30 mg/g, at 29.9 percent, compared to 24.3, 14.8, and 11.7 percent among those with CVD, hypertension, and a high BMI.
Nearly 11 percent of participants with CVD had both an eGFR <60 and an ACR ≥30, compared to 8.6 percent of those with diabetes and 4.1 and 2.1 percent, respectively, of those with hypertension and a high BMI. » Figure 1.11; see page 140 for analytical methods. NHANES III (1988–1994) & 2005–2010 participants age 20 & older; eGFR calculated using CKD-EPI equation; urine albumin creatinine ratio (ACR).
volume one highlights
patients 6.7% prevalence of egfr <60 in nhanes 2005–2010
participants (ckd-epi formula ; Table 1.a)among those with self-reported diabetes: 20.4% » among those with cardiovascular disease: 27.9%
9.4% prevalence of acr ≥30 in nhanes 2005–2010 participants (Table 1.a)among those with self-reported diabetes: 30.8% » among those with cardiovascular disease: 24.3%
9.2% prevalence of recognized ckd in Medicare patients age 65 & older, 2010 (Table 2.b & Figure 2.2)white: 8.8% » black/African American: 13.7%
patient care 85% hypertension among nhanes 2005–2010
participants with egfr <60 (ckd-epi formula; Table 1.b)
32% nhanes 2005–2010 participants with egfr <60 whose hypertension is treated & controlled (ckd-epi formula; Table 1.b)
81% hyperlipidemia among nhanes 2005–2010 participants with egfr <60 (Table 1.b)
27% nhanes 2005–2010 participants with egfr <60 whose hyperlipidemia is treated & controlled (Table 1.b)
42% nhanes 2005–2010 participants with diabetes & egfr <60 whose diabetes is uncontrolled (Table 1.b)
0.6 cumulative probability of a nephrologist visit at month 12 after a ckd diagnosis of 585.3 or higher, 2010: Medicare patients age 65+ (Table 2.h)
0.56 cumulative probability of a nephrologist visit at month 12 after a ckd diagnosis of 585.3 or higher, 2010: Marketscan patients age 50–64 (Table 2.h)
12
USRDS Coordinating Center 914 South 8th Street Suite S2.100 Minneapolis, MN 55404 1.888.99USRDS www.usrds.o
rg
2012 Annual Data ReportAtlas of Chronic Kidney Disease
and End-Stage Renal Disease in the United States
United States Renal Data System
2012 United States Renal Data System Annual Data Report
Susan Everson | portfolio | page 5

page133
page149
formed that year. Living donor donation rates appear to be
rebounding, while donations from deceased donors have
been stable. Risk factor monitoring among transplant
patients has improved, yet rates of influenza vaccinations
are still relatively low.
Highlighted data on pediatric ESRD patients show
that the number with cystic kidney disease has increased,
while there are fewer patients with glomerular disease.
Rates of hospitalization for pneumonia are greatest over-
all in patients younger than 10, and, in the hemodialy-
sis population, mortality is greatest in the first months
of therapy.
Dialysis providers continue to consolidate, with Frese-
nius Medical Care announcing the purchase of additional
units in July, 2011; the company thus maintains its position
as the largest provider of dialysis care in the United States.
Dialysis Clinic, Inc. continues to have the lowest standard-
ized hospitalization and mortality ratios among the large
providers, while, among the smaller providers, hospital-
based units have the highest standardized mortality ratios.
We conclude the Précis with data on the costs of ESRD
patient care, which rose very little in 2009. Costs per per-
son per year remain highest for hemodialysis patients, at
$82,285, compared to $61,588 and $29,983 for peritoneal
dialysis and transplant patients.» Figure p.1; see page 378 for analytical methods. Period prevalent
general (fee-for-service) Medicare patients. Diabetes, CKD, & congestive heart failure determined from claims, 1998–1999 & 2008–2009; costs are for calendar years 1999 & 2009.
p1ii Distribution of general (fee-for-service) Medicare patients & costs for CKD, CHF, diabetes, & ESRD, 1999 & 2009
General Medicare: population, 1999(n = 29,650,971; mean age 69.8)
General Medicare: costs, 1999($148 billion)
General Medicare: population, 2009(n = 31,156,428; mean age 69.2)
General Medicare: costs, 2009($289 billion)
DM 17.96%CHF 13.3%
CKD 3.6%
ESRD 0.99%
DM 32.6%CHF 38.3%
CKD 11.5%
ESRD 7.3%
DM 26.2%CHF 12.7%
CKD 10.4%
ESRD 1.3%
DM 41.97%CHF 36.3%
CKD 24.9%
ESRD 8.1%
vol 2esrd 88 92 96 00 04 08
Num
ber o
f pat
ient
s (in
thou
sand
s)
0
20
40
60
80
100
120
0
2
4
6
8
10
12
88 92 96 00 04 080
1
2
3
4
5
6
-4
0
4
8
12
16
20
88 92 96 00 04 080
1
2
3
4
-10
0
10
20
30
88 92 96 00 04 080
20
40
60
80
100
120
Sym
bols
: one
-yea
r % c
hang
e
0
2
4
6
8
10
12New patients Patients restarting dialysisPatients returning from tx Total pts starting/restarting
88 90 92 94 96 98 00 02 04 06 08
Num
ber o
f pat
ient
s (in
thou
sand
s)
0
50
100
150
200
250
300
350
400Prevalent dialysis (2009: 398,861)
Incident ESRD(116,395)
Prevalent transplant(172,553)
PrP R É C I S
page151
p2ii Counts of new & returning dialysis patients
p3ii Patient counts, by modality
In 2009, 116,395 new dialysis and transplant patients initiated ESRD therapy, for an adjusted rate per million population of 355. More than 571,000 patients were receiving treatment on December 31, 2009, for an adjusted rate of 1,738 per million population. Nearly 399,000 of these patients were being treated with dialysis, while 172,553 had a functioning graft; 90,118 ESRD patients died during the year. A total of 17,736 transplants were performed during 2009, including 6,388 from living donors. More than 34,000 patients were added to the transplant wait list, 85,539 were on the kidney-alone and kidney/pancreas wait lists at the end of 2009, and the median time on the list (for pediatric and adult patients combined) was 1.7 years.
With Medicare spending for ESRD at $29 billion, and non-Medicare spending at $13.5 billion, total ESRD costs in 2009 reached $42.5 billion. Medicare costs per per-son per year were more than $70,000 overall, ranging from $29,983 for transplant patients to $82,285 for those receiving hemodialysis therapy. » Table p.a; see page 378 for analytical methods. Dialysis & transplant patients, 2009.
The size of the prevalent dialysis popula-tion increased 4 percent in 2009, reaching 398,861, and is now 40 percent larger than in 2000. The size of the transplant popu-lation rose 4.2 percent, to reach 172,553 patients, while the number of incident patients rose 3.3 percent, to 116,395. These data suggest longer lifespans for preva-lent patients, ultimately influencing the steady growth of this population and the annual expenditures these patients incur. » Figure p.3. Incident & December 31 point prevalent ESRD patients.
The number of new dialysis patients rose 3.5 percent in 2009 — up from a 1.2 percent growth in 2008 — to 112,782. Just over 5,600 patients with graft fail-ure returned to dialysis from transplant, a one-year increase of 2.7 percent. The number of patients restarting dialysis increased 6.6 percent, to 3,492. Overall, the CMS Annual Facility Survey showed 121,880 patients starting or restarting dialysis in 2009, up 3.6 percent from 2008. » Figure p.2; see page 378 for analytical meth-ods. CMS Annual Facility Survey.
85 88 91 94 97 00 03 06 09 0
100
200
300
Among dialysis patients, the adjusted number of deaths per 1,000 patient years at risk has fallen 24% since 1985.
2711985
2072009
0 50 100 150 200 250 300
Dialysis
Transplant
Generalpopulation
Age 65 & older: adjusted deaths per 1,000 patient years at risk
48
75
313
ESRD: 402,000 patients $23.3 billion 1%
Hemodialysis $82,285
Peritoneal dialysis 61,588
Transplant 29,983
New patients All patientsNew patients All patients
Large dialysis organizations—those owning 20 or more units
Small dialysis organizations
Units based in hospitals
Independently owned units
3,330 units
438 units
806 units
927 units
1,000 patients
Large dialysis organizationsSmall dialysis organizations—
those owning 20−199 units
Units based in hospitals
Independently owned units
3,511units605 units
796 units
848 units
1,000 patients
Mortality
2%Transplant
92%Hemodialysis
65%HemodialysisWhile most hemodialysis occurs in a dialysis unit, use of home hemodialysis is rising. In Australia and New Zealand, 9–16% of dialysis patients receive therapy at home.
5%Peritoneal dialysis
Diabetes & hypertension; race: Table p.aPie charts: Figure 1.1, Table 12.cTransplant wait list: Figures 7.1 & 7.6
Mortality: Figures 5.4 & 5.2Unit ownership: Figure 10.1Costs: Figure p.1; Figure 11.7
6%Peritonealdialysis
30%Transplant
Renal replacement therapyMost new patients begin therapy on hemodialysis.
And in the entire ESRD population, 3 in 10 patients have a kidney transplant.
People are surviving longer on dialysis than in the past.
But mortality for dialysis patients is still far higher than in the general population.
Dialysis unit ownership
Costs of caring for patients with ESRD
total medicare spending
$289 billion
44% of new esrd cases have a primary diagnosis of diabetes28% have a primary diagnosis of hypertension
6 in 10 dialysis patients are treated in units owned by fresenius or davita
23,000 number of patients waiting for a kidney transplant in 1995
81,000 number waiting in 2009
2.3 yearsmedian time on transplant wait list
$42.5 billiontotal costs per year for esrd patient care
The rate of new esrd cases is 3.5 times higheramong african americans than among whites
1.3% of Medicare patients have esrd
They account for 8.1% of Medicare spending
Medicare spending per patient year, by type of renal replacement therapy
page139
chapterdetails
précis an introduction to esrd in the u.s. » 147
healthy people 2020 » 167recommended care among patients with aki, diabetes, and ckd; acei/arb treatment; esrd incidence; kidney failure due to diabetes; nephrologist care; vascular access; transplantation; mortality
1 incidence, prevalence, patient characteristics, and treatment modalities » 183incident counts and rates; prevalent counts and rates; incident and prevalent modality; patient care prior to initiation; anemia; laboratory values
2 clinical indicators and preventive care » 195anemia treatment; preventive care; vascular access; medicare part d use
3 hospitalization » 205overall hospitalization; rehospitalization; infectious hospitalization by major organ system; hospitalization in matched dialysis populations
4 cardiovascular disease » 217mortality; drug therapy
5 mortality » 225mortality; survival; mortality in the general and esrd populations
6 prescription drug coverage » 233medicare part d enrollment patterns; medicare part d coverage plans; overall costs of part d enrollment; coverage phase analyses for part d enrollees; medicare part d prescription drug use and costs
7 transplantation » 247wait list; donation; transplant; outcomes; follow-up care
8 pediatric esrd » 257esrd diagnosis in the pediatric population; infections; vaccinations; hospitalization; mortality
9 nutrition, rehabilitation/quality of life, and cardiovascular special studies » 267active/adipose: a cohort study to investigate the value of exercise in esrd/analyses designed to investigate the paradox of obesity and survival in esrd
10 esrd providers » 271provider growth; anemia treatment; preventive care; costs for intervention; standardized hospitalization and mortality ratios
11 costs of esrd » 281overall costs of esrd and injectables; racial differences; matched and unmatched dialysis populations; medicare part d costs
12 international comparisons » 291worldwide view of the incidence of esrd; incidence of esrd; prevalence of esrd; dialysis; transplantation
reference tables: esrd » 303
volume one ckdprécis » an introduction to ckd in the u.s. » 27
1 ckd in the general population » 37 strategies for
identifying ckd; comorbidity; awareness, treatment,
and control of disease conditions; mortality
2 identification and care of patients with ckd » 45 prevalence of
recognized ckd; laboratory testing of patients at risk for ckd;
probability and odds of a ckd diagnosis code; probability and odds of
seeing a physician post-ckd diagnosis; prescription drug therapy
3 morbidity and mortality in patients with ckd » 59 hospitalization rates
in ckd and non-ckd patients; infectious hospitalizations; mortality rates
4 cardiovascular disease in patients with ckd » 69
rates of cardiovascular disease; drug therapy
in patients with cardiovascular disease
5 prescription drug coverage » 77 medicare part d enrollment
patterns in patients with ckd; medicare part d coverage plans;
overall costs of part d enrollment; coverage phase analyses for
part d enrollees; medicare part d prescription drug use and costs
6 costs of ckd » 91 overall costs of ckd; components
of costs for ckd; medicare part d costs
reference tables: ckd » 101
page132
volume twoESRD
2011 USRDS ANNUAL DATA REPORT
volumetwoesrd
page148
précis » an introduction to esrd in the u.s.INTRODUCTION
Pr
INTRODUCTION
Peritoneal dialysis now accounts for 6–7 percent of the inci-
dent and prevalent dialysis populations, a level far lower
than the 12–18 percent in the 1980s and 1990s; there are
signs, however, that use of this therapy is growing. The
number of kidney transplants reached 17,736 in 2009, while
the prevalent transplant population increased 4.2 percent,
to 172,553, despite continued growth in the number of
patients on the transplant wait list. The median time on the
kidney-only and kidney-pancreas wait lists was 1.7 years.
In the rest of this Précis we highlight data from Volume
Two. We show, for instance, that rates of new ESRD cases
remain quite stable, at 355 per million population in 2009.
While ESRD due to diabetes has also been stable over the
last decade, at a rate of 154, ESRD caused by hypertension
has grown 10 percent. The prevalence of ESRD continues to
grow at a rate of 2 percent per year, reaching 1,738 in 2009.
Patients who see a nephrologist for more than 12
months before starting dialysis are the most likely to use
a fistula or internal graft at the first outpatient dialysis
treatment. Since nephrologists are central to discussions
with patients and families about ESRD treatment options,
greater pre-ESRD referral would help ensure increased use
of fistulas, which are associated with the lowest rates of
adverse events.
The treatment of anemia has changed during the last
four years, after changes in product labeling from the
FDA and in payment structures from CMS. Hemoglobin
levels at the initiation of dialysis have fallen below 10 g/dl,
a level not seen since December, 2000, while the percent-
age of patients using an erythropoiesis stimulating agent
(ESA) prior to initiation has also fallen — to 22 percent, a
level not seen since April, 1996. Hemoglobin levels at
six months following the start of ESRD therapy are now
lower than in 2001, yet the ESA dose is substantially higher.
Hemoglobin levels in the prevalent dialysis population
have decreased as well.
Hospitalizations continue to be an area of concern,
with admissions for infection in hemodialysis patients
43 percent higher than in 1993. New data on rehospitaliza-
tions show that rates are twice as high for ESRD patients
as in the general Medicare population. Mortality rates
continue to improve, though more slowly for the first year
of treatment than for the years following. Rates for ESRD
patients, however, are 2.0–2.5 times greater than for gen-
eral Medicare patients with cancer, diabetes, congestive
heart failure, or CVA/TIA.
This year we present new data on the Medicare Part D
prescription drug benefit, which started in 2006. ESRD and
non-ESRD CKD patients have higher Part D coverage with
the low income subsidy than do general Medicare patients
and, not surprisingly, out-of-pocket expenditures are
greatest for ESRD patients, at nearly $6,000 per year com-
pared to $1,985 in the general Medicare population and
$3,550 for those with a diagnosis of CKD.
The kidney transplant wait list continues to grow,
reaching 80,848 in 2009; 17,736 transplants were per-
The size of the ESRD population reached a new high in 2009, with 571,414 patients under treatment. The number
of patients returning from a failed transplant rose to 5,606, while the number restarting dialysis increased to 3,492.
150 trends in patient counts & spending
152 incidence, prevalence, modality, pre-esrd care
154 patient care
155 hospitalization
156 cardiovascular disease in patients with esrd
157 mortality
158 prescription drug coverage
160 transplantation
162 pediatric esrd
163 esrd providers
165 costs of esrd
united states renal data system
2011 USRDS ANNUALDATA REPORTvolume twoatlas of end-stage renal disease in the united states
NATIONAL INSTITUTES OF HEALTHNATIONAL INSTITUTE OF DIABETES & DIGESTIVE & KIDNEY DISEASESDIVISION OF KIDNEY, UROLOGIC, & HEMATOLOGIC DISEASES
page147
an introduction to end-stage renal disease in the united states
Sitting in the morning sunI’ll be sitting when the evening comesWatching the ships roll inAnd I watch ‘em roll away again
Otis Redding & Steve Cropper, “(Sittin’ on) the Dock of the Bay”
précis
2011 ANNUAL DATA REPORT
UNITED STATES RENAL DATA SYSTEM2011 ANNUAL DATA REPORT
atlas ofchronic kidney diseaseand end-stage renal disease in the united states
NIH PUBLICATION NO.09-3176
OCTOBER, 2011 United States Renal Data System
2011 USRDS ANNUAL DATA REPORT
volumetwoesrd
page150
précis » an introduction to esrd in the u.s.TRENDS IN PATIENT COUNTS & SPENDING
paii Summary statistics on reported ESRD therapy in the United States, by age, race, ethnicity, gender, & primary diagnosis, 2009
A Incident counts: include all known ESRD patients, regardless of any incomplete data on patient characteristics and of U.S. residency status.
B Includes only residents of the 50 states and Washington D.C. Rates are adjusted for age, race, and/or gender using the estimated July 1, 2005 U.S. resident population as the standard population. All rates are per million population. Rates by age are adjusted for race and gender. Rates by gender are adjusted for race and age. Rates by race are adjusted for age and gender. Rates by disease group and total adjusted rates are adjusted for age, gender, and race. Adjusted rates do not include patients with other or unknown race.
C Patients are classified as receiving dialysis or having a functioning transplant. Those whose treatment modality on December 31 is unknown are assumed to be receiving dialysis. Includes all Medicare and non-Medicare ESRD patients, and patients in the U.S. Territories and foreign countries.
D Deaths are not counted for patients whose age is unknown.
E Age is computed at the start of therapy for incidence, on December 31 for point prevalence, at the time of transplant for transplants, and on the date of death for death.
F Includes patients whose modality is unknown.
G Unadjusted total rates include all ESRD patients in the 50 states and Washington D.C.
H Total transplants as known to the USRDS; 57 transplants with unknown donor type excluded from counts.
I Adjustments using the Bureau of Labor Statistics inflationary adjustment and the CMS inflation adjustment for the medical component.
* Values for cells with ten or fewer patients are suppressed. “.” Zero patients in this cell.
IncidenceA December 31 point prevalence Kidney transplantsAdj. Adj. Deceased Living ESRD
Count % rateB CountC % rateB DialysisC % TxC % donor donor deathsD
0-19E 1,400 1.2 16 7,738 1.4 86 2,247 0.6 5,491 3.2 612 407 11520-44 14,300 12.3 131 100,031 17.5 924 55,904 14.0 44,127 25.6 2,982 2,296 4,63445-64 44,699 38.4 610 256,803 44.9 3,433 167,147 41.9 89,656 52.0 5,786 2,931 27,18965-74 26,998 23.2 1,407 116,607 20.4 6,066 89,802 22.5 26,805 15.5 1,699 676 23,93875+ 28,970 24.9 1,762 90,233 15.8 5,545 83,759 21.0 6,474 3.8 212 78 34,242Unknown 28 * * 0.0 . 0.0 White 76,377 65.6 277 347,268 60.8 1,279 223,178 56.0 124,090 71.9 6,602 4,680 60,708African American 32,314 27.8 976 180,685 31.6 5,284 147,290 36.9 33,395 19.4 3,535 843 24,799Native American 1,442 1.2 523 7,682 1.3 2,735 5,730 1.4 1,952 1.1 184 107 1,076Asian/Pacific Islander 5,647 4.9 403 30,365 5.3 2,101 19,679 4.9 10,686 6.2 830 707 3,092Other/unknown 615 0.5 5,414 0.9 2,984 0.7 2,430 1.4 140 51 443Hispanic 16,240 14.0 501 87,866 15.4 2,538 64,930 16.3 22,936 13.3 1,659 931 10,394Non-Hispanic 100,155 86.0 345 483,548 84.6 1,685 333,931 83.7 149,617 86.7 9,632 5,457 79,724Male 65,996 56.7 452 323,276 56.6 2,140 220,500 55.3 102,776 59.6 6,775 3,887 50,212Female 50,393 43.3 282 248,127 43.4 1,408 178,352 44.7 69,775 40.4 4,516 2,501 39,906Unknown * 11 * 0.0 * 0.0 .Diabetes 50,970 43.8 154 215,245 37.7 647 175,166 43.9 40,079 23.2 3,496 1,337 41,055Hypertension 32,688 28.1 101 140,498 24.6 429 113,173 28.4 27,325 15.8 2,340 999 25,490Glomerulonephritis 7,612 6.5 24 84,883 14.9 263 40,166 10.1 44,717 25.9 2,121 1,524 5,924Cystic kidney disease 2,662 2.3 8 27,254 4.8 83 10,664 2.7 16,590 9.6 866 702 1,522Urologic disease 1,590 1.4 5 13,108 2.3 41 7,271 1.8 5,837 3.4 252 180 1,538Other known cause 14,810 12.7 46 62,315 10.9 195 36,785 9.2 25,530 14.8 1,535 1,160 10,270Unknown cause 4,245 3.6 13 21,563 3.8 66 13,741 3.4 7,822 4.5 443 270 3,429Missing cause 1,818 1.6 4 6,548 1.1 13 1,895 0.5 4,653 2.7 238 216 890All 116,395 355.4 571,414 100.0 1,738 398,861F 172,553 11,291 6,388 90,118 Unadjusted rateG 371 1,810.6 Total transplantsH 17,736
Wait-list for kidney & kidney/pancreas transplantsNew Median
listings N, as of time on in 2009 12.31.09 list (yrs)0-17 769 775 0.8018-34 4,184 8,769 1.4835-49 9,482 23,295 1.7450-64 14,029 35,191 1.7165+ 5,641 14,508 1.72Male 20,420 48,163 1.63Female 13,685 34,375 1.77White 20,499 44,564 1.54African American 9,957 28,878 1.89Native American 406 983 1.72Asian/Pacific Islander 2,453 6,215 1.84Other/unknown 791 1,899 1.56Hispanic 5,713 15,183 1.79Non-Hispanic 28,393 67,356 1.66Diabetes 11,651 27,631 1.56Hypertension 7,001 18,693 1.77Glomerulonephritis 5,854 15,270 1.91Cystic kidney disease 2,449 5,262 1.54Urologic disease 571 1,491 2.17Other known cause 4,834 10,675 1.64Unknown cause 1,047 2,592 1.82Missing cause 699 925 0.97Blood type A 11,253 23,673 1.48B 4,992 13,382 1.81AB 1,343 2,433 1.28O 16,518 43,051 1.79PRA 0% 13,815 39,883 1.861-9 2,274 6,645 1.8410-79 3,928 13,490 2.0980+ 1,896 9,769 2.88Unknown 12,193 12,752 0.20Total 34,106 82,539 1.69
Medicare & non-Medicare spending*Medicare spending for ESRD, 2009(billions of dollars)
SAF paid claims (Part A & B) 25.112% incurred but not reported 0.50HMO-Medicare risk 3.13Organ acquisition 0.28
Total Medicare costs 29.03Non-Medicare spending for ESRD, 2009(billions of dollars)
EGHP (MSP) 2.99Patient obligations 4.84Non-Medicare patients 5.64
Total non-Medicare costs 13.47Total ESRD costs (billions), 2009 42.50Change in Medicare spending, 2008 to 2009
Total 6.77%Per patient year 5.63%
Adjusted for inflationI 6.1 to 2.4%Medicare spending per patient year, 2009
ESRD $70,216 Hemodialysis $82,285 Peritoneal dialysis $61,588 Transplant $29,983
* Does not include Medicare Part D.
80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09
80 84 88 92 96 00 04 080
20,000
40,000
60,000
80,000
100,000
120,000
80 84 88 92 96 00 04 080
100,000
200,000
300,000
400,000
500,000
600,000
New patients
Omnibus Budget Reconciliation Act (OMBA) includes Medicare Secondary Payor provision
Composite rate payment system for dialysis becomes e� ective; cyclosporine introduced
1972 Congress authorizes medical coverage of ESRD1978 Congress authorizes creation of ESRD networks
EPO receives FDA approval; USRDS
publishes � rst ADR
USRDS created
Center for Medicare & Medicaid Services (CMS) launches Fistula First initiative
New bundled prospective payment system for dialysis patients; implemented January 2011
U.S. Dept. of Health & Human Services develops Healthy People 2000 initiative
NIH begins National Kidney Disease Education Program (NKDEP)
United Network for Organ Sharing (UNOS) created
60,000 patients receive treatment for ESRD
Graphs: Figure 1.1Rates of new & existing patients: Figures 1.6 & 1.12Maps: Figures 1.4 & 1.10
571,00 patients receive treatment for ESRD
CMS adopts 26 new Clinical Performance Measures to
monitor the quality of care received by ESRD patients
UNOS begins to operate the Organ Procurement & Transplantation Network (OPTN)
National Kidney Foundation (NKF)
launches the Dialysis Outcomes Quality Initiative (KDOQI)
NKF publishes KDOQI guidelines; Health Care Financing Administration (HCFA) begins Hematocrit Measurement Audit program
enD-stAGe renAl dIseAse (ESRD)IN THE UNITED STATES
Total patientsMore than 116,000 people began treatment for end-stage renal disease (ESRD) in 2009.
U.S. patients newly diagnosed with ESRD
U.S. patients being treated for ESRD
per one million people in 2009
new patients
399
365
336
308
total patients
1,917
1,772
1,633
1,485
Nearly ten times more patients are now being treated for ESRD than in 1980.
19801 in 11,600
19801 in 3,450
20091 in 2,800
20091 in 575
2011 USRDS ANNUAL DATA REPORT
volumeoneesrd
page138
2011 United States Renal Data System Annual Data Report
Susan Everson | portfolio | page 6

page7
Volume One CKDchapter details 8introduction to volume one 12
précis an introduction to ckd in the united states 17
1 ckd in the general population 39
2 ckd identified in the claims data 53
3 care of patients with ckd 654 morbidity & mortality 775 cardiovascular disease in
patients with ckd 876 outcomes in the transition
zone in nursing home patients with ckd 99
7 the transition to esrd 1098 acute kidney injury 1219 costs of ckd 133reference tables 145
appendix a analytical methods (volume one) 164
appendix b usrds products & services 174
glossary 180index 185
data requests 174data release agreement 183
Volume Two ESRDchapter details 196information map 198program summary & retrospective 200introduction to volume two 202
précis An introduction to esrd in the united states 209
hp2010 healthy people 2010 2231 emerging issues 2392 incidence & prevalence 2533 patient characteristics 2674 treatment modalities 2775 clinical indicators & preventive health 2876 morbidity & mortality 3017 transplantation 3118 pediatric esrd 3259 special studies 33510 providers 35311 costs of esrd 36712 international comparisons 383reference tables 397
appendix a analytical methods (volume two) 462
appendix b usrds products & services 494
glossary 500cms forms 507index 521image credits 524colophon 526
data requests 494data release agreement 503international data collection form 505
page355
This year we include data on rates of hospitalization for vascular access infections, looking at differences by provider and region. Rates are more than three times higher in patients using a cath-eter at dialysis initiation rather than an internal access, are slightly lower in SDOs and hospital-based units, and are also lower in the western region of the country. These findings may reflect differences in infection prevention protocols, and should be assessed.
Hospitalizations for heart failure and/or fluid overload differ in the SDOs and other providers, particularly as related to the rate of extra dialysis procedures performed in patients with heart fail-ure. Within the large dialysis organizations, for example, Fresenius has higher rates of billed extra dialysis runs compared to DaVita and DCI. These variations need to be investigated to determine which practice patterns relate to lower rates of infectious complications.
As in past ADRs, we conclude the chapter with comparisons of mortality and hospitalization ratios by provider and geographic region; we also present outcomes across large and small dialy-sis organizations and hospital-based units. Hospitalization ratios are very similar across the large groups, though lower in DCI units. Ratios for SDOs are lowest in the Pacific region. And for hospital-based units, both mortality and hospitalization ratios are greatest in the East South Central, South Atlantic, and West South Central regions. These differences have narrowed compared to prior years, an important change. We will continue to assess these relative outcomes between providers, and examine them over time to determine areas for improvement.
provider growth; anemia treatment 356clinical monitoring; preventive care 358costs for interventions & preventive care 360vascular access & fluid overload hospitalizations 362standardized hospitalization & mortality ratios 364
101ii Distribution of patients, by unit affiliation, 2008
DCI (13K)
Fresenius(117K)
Large dialysis organizations (234,540 patients / 3,330 units) SDOs (33,084 / 438)
Hospital-based (39,759 / 806)
Independent (63,952 / 927)
Renal Advantage Inc.
Nat’l Renal Institutes
Renal Research Institute
American Renal Assoc.
Satellite Healthcare
Dialysis Corp. of America
Liberty dialysis Hawaii
Nat’l Renal Alliance
DaVita(104K patients)
03
08
03
08
03
08
03
08
03
08
03
08
03
08
03
08
03
08
03
08
Perc
ent o
f pat
ient
s
0
20
40
60
80
100
All F G* DV RCG** DCI NNA SDO Ind HB
<10 10-<12 12-<13 13+ g/dl
All F G* DV RCG** DCI NNA SDO Ind HB
Perc
ent o
f pat
ient
s
0
5
10
15
20
2003 2008
All F DV DCI SDOs Ind HB
Perc
ent o
f pat
ient
s
0
20
40
60
80
100
INFeD Ferrlecit Venofer
All F G* DV RCG** DCI NNA SDO Ind HB
Num
ber o
f mon
ths
with
IV ir
on
0
1
2
3
4
5
2003 2008
All F G* DV RCG** DCI NNA SDO Ind HB
Mea
n to
tal d
ose
(1,0
00s o
f uni
ts)
0.0
0.5
1.0
1.5
2.0
2.5
2003 2008
page357
105ii Distribution of prevalent, EPO-treated dialysis patients, by hemoglobin level & unit affiliation
106ii IV iron use in dialysis patients, by type of iron & unit affiliation, 2008
107ii Months with IV iron in the first six months of dialysis, by unit affiliation
108ii Mean total IV iron dose in the first six months of dialysis, by unit affiliation
109ii Dialysis patients with one or more transfusion events, by unit affiliation
treatment with iv iron Figures 10.6–8 illustrate IV iron use in the dialysis population. In 2008, one in four prevalent patients used Ferrlecit, while 61 percent were treated with Venofer; only 0.3 percent of dialysis patients received INFeD. These numbers vary considerably, however, by unit affiliation. In independent units and those owned by Fresenius, 37–42 percent of patients were treated with Ferrlecit; in DaVita and DCI units, in contrast, Ferrlecit was used by only 2–4 percent of the dialysis population, while 87 percent received Venofer.
In the first six months of dialysis, the number of months in which patients receive IV iron now ranges from 4.4 in Fresenius and hospital-based units to 4.8 in those owned by DCI. The mean total IV iron dose in this period increased 13.2 percent between 2003 and 2008 — from 1,973 units to 2,233 — and now ranges from 1,945 in hospital-based units to 2,274 in those owned by small dialysis organizations (SDOs). ∏ Fig-ures 10.6–8; see page 483 for analytical methods. Point prevalent dialysis patients (10.6); incident dialysis patients treated with EPO (10.7–8).
In 2008, 15.5 percent of prevalent dialysis patients re-ceived one or more tranfusions, only slightly higher than the 15.3 percent reported for 2003. By unit affili-ation, the percentage ranges from 13.8 in DaVita and DCI units to 17.1–17.6 in hospital-based and indepen-dent units. ∏ Figure 10.9; see page 483 for analytical meth-ods. Point prevalent dialysis patients.
In 2008, two in three prevalent, EPO-treated dialysis patients had a hemoglo-bin of 10–<12 g/dl, considerably higher than the 51 percent in 2007 (reported in the 2009 ADR), and perhaps a sign that providers are responding to studies showing the risks of higher hemoglobin levels. The percentage of patients with a level of 13 g/dl or above now ranges from 1.1 in DCI units to 3.3 in those that are hospital-based. ∏ Figure 10.5; see page 483 for analytical methods. Period prevalent dialysis patients.
pg 174 (vol 1), pg 494 (vol 2) agreement for re
lease
of data
pg 183
(vol 1
), pg
503 (
vol 2
)
CKD (vol 1): pg 164; ESRD (vol 2): pg 462 d
ata fi l
es av
ailab
le to
rese
arch
ers (
Appe
ndix
B)
ESRD (vol 2): p.19, 6.7, 8.19 Data analy
sis an
alytic
al m
etho
ds (
Appe
ndix
A)
ESRD (vol 2): p.17–18, Chapter 6, 8
.16–18
surv
ival C
KD (
vol
1):
5.6;
Chapter 6, 8.10–15 mortality CKD (
vol
1):,
1.18–
21,
4.16
–19;
Chapter 4, 5.7–8; ESRD (v
ol 2):
p.16
, 1.1–
14,
1.22–
24,
Outcomes hospitaliza
tion C
KD (
vol
1):
E N D - S T A G E R E N A L DI S
EA
SE
I N
T
HE
U
.S.
Diseases identifying CKD (vol 1): 1.a–4, 2.10–17 anemia ESRD (vol 2): 3.5–7, 5.2–9 cardiovascular disease
CKD (vol 1): 1.c–8, 3.15, Chapter 5; ESRD (vol 2): hp.5, 6.15, 9.2–14 diabetes CKD (vol 1):
Chapter 1, 2.12.b–18; ESRD (vol 2): hp.18–21, 2.7, 2.15, 5.10–13, 6.7, 10.13–15 acute kidney
injury (vol 1) Chapter 8 Medicare Part D CKD (vol 1): 9.12–17; ESRD (vol 2):
4.12–e, 5.24–40, 11.47–59 Costs CKD (vol 1): Chapter 9; ESRD (vol 2):
p.20–28, Chapter 11
T O P I C S O F P A R T I C U L A R I NT E R
EST
page11
2010 usrds annual data report
volumeoneckdpage6
at www.usrds.orgpdf files of the 2010 adr, booklet, & Researcher’s Guide ∏ PowerPoint slide files of all
adr figures & tables, & Excel files of the underlying data ∏ Excel files of the complete refer-ence tables ∏ render, our online query application for accessing usrds data ∏ An online ap-
plication for requesting data from the usrds ∏ A navigable index of adr figures & tables
new to this edition of the annual data report An expanded volume on chronic kidney disease ∏ A chapter on the transition to esrd in nursing home
patients, including information on cognitive function ∏ Data on use & costs of the Medicare Part D pre-scription drug benefit for both ckd & esrd patients ∏ An Emerging Issues chapter on hospital admissions
for infection ∏ A Special Studies chapter with data on prescription drug therapy in patients with heart disease, the association of bmi & heart failure, bariatric surgery, patients receiving information on transplant options at
the initiation of esrd therapy, & the use of nutritional therapies ∏ Comparative data on costs in the u.s. & Taiwan ∏ New data on the incidence of esrd in Asian & indigenous populations
2010 usrds annual data report
volumetwoesrdpage354
esrd providers10introduction
DCI; these organizations manage 3,330 units across the U.S. Smaller dialysis organizations (SDOs) treated 33,084 patients in 438 units, in-dependently owned units accounted for 63,952 patients in 927 units, and the remaining pa-tients were treated in hospital-based units.
Recent clinical trials have shown adverse outcomes when hemoglo-bin levels are targeted to 13 g/dl and above. The highest percentage of pa-tients with a hemoglobin of 10–<12 earlier occurred in units owned by Di-alysis Clinic, Inc. (DCI), but is now reported in units owned by Fresenius. Use of intravenous iron products to treat anemia varies across providers, with DaVita and DCI almost exclusively using Venofer, and Ferrlecit and Venofer used equally in Fresenius units. And the total months of IV iron therapy in the first six months of ESRD has now increased to 4.5, with the mean IV iron dose now at 2,233 mg; this dose is highest in DaVita units, at 2,332 mg, and lowest in hospital-based units, at 1,945 mg.
It is important that patients have adequate iron stores in order to maintain optimal hemoglobin levels. The percentage of patients receiving ferritin testing for three consecutive months after starting ESA therapy, however, is only 8.0 in DCI units, lower than that reported for other pro-viders. The new dialysis bundled payment system, taking effect in 2011, will incorporate all extra monthly tests into a single monthly payment, and its effect on the marked differences in testing rates across providers will be monitored closely by the USRDS in future ADRs.
This year we again assess preventive care services delivered by pro-viders. Glycemic control testing in diabetic patients, for example, differs across providers, with 63–64 percent of patients in Fresenius and DaVita units, and in the SDOs, receiving at least four glycosylated hemoglobin tests in a year, compared to 44–48 percent in DCI and hospital-based units. Rates of vaccinations, both for influenza and for pneumococcal pneumo-nia, have improved during the past several years.
Variations in Medicare payments across provider groups are con-siderable, particularly in the areas of erythropoiesis stimulating agents (ESAs), IV iron, and IV vitamin D. Laboratory costs, however, are fairly consistent, with the exception of DCI, for which costs are lower by nearly one-third compared to other providers. As these payments become fixed under the new payment bundle, it will be important to monitor the use of services to determine any changes in clinical performance.
The network of dialysis providers has
stabilized since the consolidation of
Gambro units into DaVita and RCG units
into Fresenius. At the end of 2008, 117,000
prevalent patients were being treated by
Fresenius, 104,000 by DaVita, and 13,000 by
national institutes of healthnational institute of diabetes & digestive & kidney diseasesdivision of kidney, urologic, & hematologic diseases
volumeoneatlas of chronic kidney
disease in the united states
united states renal data system2010 usrds annual data report
page353
chapterten
providersthat all things send forth love, inanimatethat all these loves have mingled in the airand set up a great clangorin the nodesheart of this sound, this deadly spirit lovea cosmos comes to birth
Diane Di Prima, “Ode to Elegance”
2010
Annual D
ata ReportU
nited States Renal Data System
United States Renal Data System2010 Annual Data Report
volume twoAtlas of End-Stage Renal Disease in the United States
ESRDvolum
e two
All All units F Fresenius G* DaVita/Gambro (Gambro
units were purchased by DaVita in October, 2005)
DV DaVita RCG** Renal Care Group (rcg units
purchased by Fresenius in 2006) DCI Dialysis Clinic, Inc. NNA National Nephrology AssociatesSDOs Small dialysis organizations
(defi ned as 20–99 dialysis units; unit classifi cation assigned by the usrds, W not used prior to 2005)
Ind Independent units HB Hospital-based units
Unit affi liation
ESRD network
All 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Perc
ent c
hang
e, 2
003
to 2
008
0
10
20
30
40
Units Patients
F G* DV RCG** DCI NNA SDOs Ind HB0
600
1,200
1,800Number of patients (in thousands)Number of units
F G* DV RCG** DCI NNA SDOs Ind HB0
40
80
12020032008
All G* RCG* NNA IndF DV DCI SDOs HB All G* RCG* NNA IndF DV DCI SDOs HB
Perc
ent o
f uni
ts
0
20
40
60
80
100 2003 2008
1 year 2 years 3-4 years 5+ years
2010 usrds annual data report
volumetwoesrdpage356
10esrd providersprovider growth; anemia treatment
102ii Percent change in the number of dialysis units & patients, 2003 to 2008, by ESRD network
103ii Dialysis unit & patient counts, by unit affiliation
104ii Dialysis unit distribution, by affiliation & time managed (time under chain ownership)
Between 2003 and 2008, the number of dialysis units grew 36–37 percent in Networks 9 and 14, and 28–29 percent in Networks 10, 15, and 16. In Networks 2 and 5, in contrast, the number of units rose less than 10 percent. The number of patients rose at least 25 percent in Networks 14, 15, 16, and 18. ∏ Figure 10.2; see page 483 for analytical methods. CMS Annual Facility Survey.
Dialysis unit and patient counts rose nearly 20 percent between 2003 and 2008. DaVita showed the largest growth — 163.9 percent in units and 138.3 percent in patients — in large part due to the purchase of Gambro in October, 2005. Hospital-based and in-dependent units experienced negative growth in both the number of units and the number of treated patients during the time period. ∏ Figure 10.3; see page 483 for analytical methods. CMS Annual Fa-cility Survey.
The percentage of units remaining under consistent owner-ship for five or more years fell from 70.6 in 2003 to 55.8 in 2008, a reflection of major unit purchases by DaVita and Fresenius in 2005 and 2006. It appears, however, that pur-chases of independent and hospital-based units by the large chains may be slowing. In 2003, for example, 57.9 percent of independent units were under the same ownership for five or more years, compared to 62.4 percent in 2008; in hospital-based units, 87.5 percent were owned for five or more years in 2003 compared to 90.9 percent in 2008. ∏ Figure 10.4; see page 483 for analytical methods. CMS Annual Facility Survey.
Chapters 4 & 7 laboratory values & testing CKD (vol 1): 1.d–9, 2.c–26, 3.9–16, 7.7–12; ESRD (vol 2): 3.b–13
(vol 2): 5.1 dialysis access ESRD
(vol 2): 3.1, 3.2–4, 5.17–23 transplantation (vol 2) p.6, hp.14–17,
physician care CKD
(vol 1): 3.2–8, 7.2–6; ESRD (vol 2): 3.2–a KDOQI guidelines ESRD
CKD
(vol 1): 1.e–13, 3.25–28 anemia treatment ESRD (vol 2): 3.5–7, 5.2–9
antibiotics ESRD (vol 2): 1.15–21, 1.25–33 awareness/treatment/control
(vol 1): 3.27–24, 5.a–5, 5.13–19, 7.13–a ESRD (vol2): 5.24–40
hp.21–h 5.10–16, 8.8–9, 10.13–18 drug therapy CKD
Treatment preventive care ESRD (vol 2):
INF
OR
MA
TIO
N I
N T
HE 2
0 1 0 AN N U A L D A TA R E P O R T:
AT
LA
S
OF
C
HR
ON
I C
K I D N E Y D I S E A S E &
Popu
lati
ons
NHAN
ES C
KD (v
ol 1)
: Cha
pter 1
new patie
nts CKD (vol 1): 2.2, 2.4–6, 2.10–13; ESRD
(vol
2): p
.a–4,
p.7,
hp.
2, Ch
apter
2, 4.
1, 4.a–
5, 8.1–
4 existin
g patients C
KD (vol 1): Chapter 1, 2.3,
2.7–
9, 2
.14–17
; ESR
D (v
ol 2)
: p.1–
3, p.7
, Chap
ter 2, 4.2,
4.b–8, 8.1, 8.5–7 CKD datasets
(vol
1) 2.
a ped
iatric
patie
nts ES
RD (v
ol 2): C
hapter 8 international comparisons;
CKD
(vo
l 1):
9.18
–23;
ESRD
(vol 2):
Chapter 12 Cognitive
func
tion
CKD
(vol
1): Chap
ter 6
2010 usrds annual data report
volumeoneckdpage10
USRDS Coordinating Center 914 South 8th
Stre
et S
uite
S20
6 M
inne
apol
is, M
N 5
5404
1.8
88.9
9USR
DS www.usrd
s.org
united states renal data system2010 annual data reportAtlas of chronic kidney disease & end-stage renal disease in the United States
brown: 469green: 7474
2010 United States Renal Data System Annual Data Report
Susan Everson | portfolio | page 7

On our website, www .usrds .org PDF files of the 2009 ADR & the Researcher’s Guide ¶ PowerPoint slide files of all ADR figures, & Excel files of the data underlying the graphs ¶ Excel files of the Reference Tables, including supplemental hos-pitalization & mortality tables with calculations per 1,000 patients, & Medicare-only tables ¶ RenDER, our online query application for accessing USRDS data ¶ An online application for requesting data from the USRDS ¶ A navigable index of ADR figures & tables New to this edition of the ADR An expanded volume on chronic kidney disease, with new chapters on the care of CKD patients, the transition to ESRD, and acute kidney injury ¶ A new chapter on renal function measures in the adolescent U .S . population ¶ Data on stroke in CKD and ESRD patients ¶ A Special Studies chapter that includes data from the Cardiovascular, Rehabilitation/Quality of Life, & Nutrition Special Studies Centers
Vol 2esRD
5
pg 175
Vol 2esrd
5
Précispg 191
2009 USRDS Annual D
ata Report 4
PrÉcis: A
n in
troduction
to ESR
D
two or more years, and adjusted first-year rates for hemodialysis patients now show three years of successive declines. The use of catheters is still an important issue here, as more than 80 percent of patients have a catheter at their first outpatient dialysis, and early morbidity from vascular access infections in the first months of dialysis is a concern (see Chapter One for data on infectious hospitalization rates in the first months of hemodialysis). ¶ Greater growth in general Medicare costs compared to those for eSrd — in 2006, 16.9 versus 4.9 percent — along with the inclusion, starting in 2006, of Part D in the total Medicare costs, have led to a decline in the percentage of the Medicare budget spent on eSrd, now at 5.8 percent. In absolute dollars, however, the program grew 6.1 percent in 2007. ¶ Costs for both diabetic and non-diabetic Medicare patients with eSrd continue to rise. The same is true for patients with employer group health plan (eGHP) coverage, though costs here are significantly higher. The average Medicare eSrd patient with diabetes now costs $72,461 per year, compared to $98,721 in the eGHP population.
¶ Figure p.1; see page 362 for analytical methods. Period prevalent general Medicare patients.
General Medicare: population, 1997(n = 32,070,486; mean age 69.4)
General Medicare: costs, 1997($165.8 billion)
General Medicare: population, 2007(n = 33,479,609; mean age 68.9)
General Medicare: costs, 2007($269.5 billion)
Diabetes 24.6% CVD 44.9%
CKD 8.8%
ESRD 1.2%
Diabetes 16.1% CVD 41.2%
CKD 3.3%
ESRD 0.85%
Diabetes 41.6% CVD 79.9%
CKD 24.6%
ESRD 7.3%
Diabetes 31.6% CVD 80.2%
CKD 12.4%
ESRD 6.1%
p1ii Distribution of general Medicare patients & costs for CKD, cardiovascular disease, diabetes, & ESRD, 1997 & 2007
89 93 97 01 05
Num
ber
of p
atie
nts
(in th
ou
san
ds)
0
20
40
60
80
100
120
0
2
4
6
8
10
12
89 93 97 01 050
1
2
3
4
5
6
-4
0
4
8
12
16
20
89 93 97 01 050
1
2
3
4
-10
0
10
20
30
89 93 97 01 050
20
40
60
80
100
120
Sym
bo
ls: o
ne-y
ear %
ch
ange
0
2
4
6
8
10
12New patients Patients returning from tx Patients restarting dialysis Total pts starting/restarting
88 90 92 94 96 98 00 02 04 06
Nu
mb
er o
f pat
ient
s (in
tho
usan
ds)
0
50
100
150
200
250
300
350
400Prevalent dialysis (2007: 368,544)
Incident ESRD(111,000)
Prevalent transplant (158,739)
2009 USRDS Annual D
ata Report
Vol 2esrd
5
Précispg 193
4 P
rÉcis: An
introdu
ction to E
SRD
Trends in patient counts &
spending
p2ii Counts of new & returning dialysis patients
p3ii Patient counts, by modality
In 2007, 111,000 new dialysis and transplant patients initiated eSrd ther-apy, for an adjusted rate per million population of 354 — a 2.1 percent decrease from the rate of 362 in 2006 (Figure p.4). More than 527,000
patients were receiving treatment on December 31, 2007, for an adjusted rate of 1,665 per million population — 2.0 percent higher than the 2006 rate of 1,632. Nearly 369,000 of these patients were being treated with dialysis, while 158,739 had a functioning transplant. A total of 17,513 transplants were performed dur-ing the year — 6,041 from living donors — and 87,812 eSrd patients died. Nearly 33,000 patients were added to the transplant wait list in 2007, and 73,555 were on the list at the end of the year; the median time on the list was 1.5 years.
With Medicare spending for eSrd at $23.9 billion, and non-Medicare spending at $11.4 billion, total eSrd costs in 2007 reached $35.3 billion. Medicare costs per person per year were nearly $62,000 overall, ranging from $24,572 for transplant patients to $73,008 for those receiving hemodialysis. ¶ Table p.a; see page 362 for analytical methods. Dialysis & transplant patients, 2007.
The number of new dialysis patients rose just 0.85 percent in 2007 — down from 3.6
percent in 2006 — to 107,644. Nearly 5,400 patients with graft failure re-turned to dialysis from transplant, a one-year decrease of 3.2 percent. The number of patients restarting dialysis, in contrast, grew 12.3 percent, to 3,031. Overall, the cMS Annual Facility Sur-vey showed 116,073 patients starting or restarting dialysis in 2007, up 0.9 percent from 2006. ¶ Figure p.2. CMS Annual Facility Survey.
The prevalent dialysis population grew 30 percent between 2000 and 2007, reaching nearly 370,000. The
transplant population increased 46 percent in this same period, and in 2007, with almost 159,000 patients, showed a one-year growth of 4.9 percent. The number of incident patients, in contrast, remained stable in 2007, at 111,000. These data suggest that the prevalent popu-lation is living longer, influencing both the growth of the treated eSrd population and the annual expenditures these patients incur. ¶ Figure p.3. Incident & December 31 point prevalent ESRD patients.
Volume OneCKD
4
Chapter details
Précis An introduction to chronic kidney disease in the United States: highlights from Volume One . . . . . . . . .17
Summary statistics & predictive models for CKD • Descriptive parameters; metabolic abnormalities • CKD claims; prescription drug therapy • Biochemical levels & control • Hospitalization & mortality • CKD claims & physician visits • A cute kidney injury
One Chronic kidney disease in the adult NHANes population . . . . . . . . . . . . . . . . .35
Strategies for identifying CKD • Comorbidity burden • Clinical & biochemical abnormalities • Awareness, treatment, & control of disease conditions • Predictive models for CKD; mortality
Two Renal function measures in the adolescent NHANes population . . . . . . . . . . . . . . . . .49
Characteristics of U .S . adolescents • Associations of abnormal GFR • Trends in renal function
Three Chronic kidney disease identified in the claims data . . . . . . . . . . . .59
Incidence & prevalence of CKD in the U .S . • CKD as defined by the new diagnosis codes • Comorbidity burden in patients with CKD • Defining CKD through laboratory data
Four Care of patients with chronic kidney disease . . . . .71
Identified CKD & physician follow-up • Laboratory evaluations prior to ESRD • Prescription drug therapy prior to ESRD • Biochemical levels & drug therapy prior to ESRD
Five Morbidity & mortality . . . .83Hospitalization rates in CKD & non-CKD patients • Infectious hospitalization rates • Mortality rates • Rates of stroke & mortality
Six Cardiovascular disease in patients with chronic kidney disease . . . . . . . . . . . . .95
CKD stage & cardiovascular disease • Geographic variations in CVD & procedure use • Survival, care, & costs of patients with CVD
Seven The transition to esRD . . . . . . . . . . . . . . . . . . 105
Patient care prior to ESRD • Laboratory testing prior to ESRD • Medication continuity in the transition to ESRD • Prescription drug therapy in the transition to ESRD • Dialysis access placement in the transition to ESRD
Eight Acute kidney injury . . . . 119Characteristics of patients with acute kidney injury • Overall rates of acute kidney injury • Patient care & outcomes following AKI hospitalization • Patient outcomes following AKI hospitalization
Nine Costs of chronic kidney disease . . . . . . . . . . . 131
Overall costs of chronic kidney disease • PPPM components of costs for CKD
5
pg 176
Chapter details . . . . . . . . . . . . . . . . . . . 8Introduction to Volume One . . . 12
Précis An introduction to CKD in the United States . . .17
One CKD in the adult NHANES population . . . . . . . .35
Two Renal function measures in the adolescent NHANES population . . . . . . . . . . . . . . . . . .49
Three CKD identified in the claims data . . . . . . . . . . .59
Four Care of patients with CKD . . . . . . . . . . . . . . . . . . . .71
Five Morbidity & mortality . . . . .83Six Cardiovascular disease
in patients with CKD . . . . . . . .95Seven The transition to ESRD . . 105Eight Acute kidney injury . . . . . 119Nine Costs of CKD . . . . . . . . . . . . 131
Appendix A: Analytical methods (Volume One) . . . . . . . . . . . . . . . 140
Appendix B: uSrDS products & services . . . . . . . . . . 152
Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . 158Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
Data requests . . . . . . . . . . . . . . . . . . . . . 152Data release agreement . . . . . . . . . . . 161
4Chapter details . . . . . . . . . . . . . . . . 177Frequently requested data
in the Reference Tables . . . 178Information map . . . . . . . . . . . . . . 179Program retrospective . . . . . . . . . 180Introduction to Volume Two . . 182
Précis An introduction to ESRD in the United States . . . . . . 189
HP2010 Healthy People 2010 . . 203One Emerging Issues . . . . . . . . . . 219Two Incidence & prevalence . . 231Three Patient
characteristics . . . . . . . . . . . . . 241Four Treatment modalities . . . 249Five Clinical indicators
& preventive health . . . . . . . 259Six Morbidity & mortality . . . . 269Seven Transplantation . . . . . . . . 281Eight Pediatric ESRD . . . . . . . . . . 295Nine Special Studies . . . . . . . . . . 307Ten Providers . . . . . . . . . . . . . . . . . 323Eleven Costs of ESRD . . . . . . . . . . 335Twelve International
comparisons . . . . . . . . . . . . . . 343
Appendix A: Analytical methods (Volume Two) . . . . . . . . . . . . . . . . 356
Appendix B: uSrDS products & services . . . . . . . . . . 388
Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . 394CMS forms . . . . . . . . . . . . . . . . . . . . . . . . . 401Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 415Image credits . . . . . . . . . . . . . . . . . . . . . . 418Colophon . . . . . . . . . . . . . . . . . . . . . . . . . . 420
Data requests . . . . . . . . . . . . . . . . . . . . . 388Data release agreement . . . . . . . . . . . 397International data
collection form . . . . . . . . . . . . . . . 399
Volume TwoESRD
Volume OneCKD
Volume ThreeReference Tables
A Incidence of reported ESRD . . . . . . . . . . . 429
B Prevalence of reported ESRD . . . . . . . . . . . 453
C Patient characteristics . . . . 487D Treatment modalities . . . . 507E Transplantation: process . . 539F Transplantation:
outcomes . . . . . . . . . . . . . . . 559G Morbidity &
hospitalization . . . . . . . . . . 593H Mortality &
causes of death . . . . . . . . . . 619I Patient survival . . . . . . . . . . 671J Provider characteristics . . . 717K Economic costs of ESRD . . 731L Vascular access . . . . . . . . . . 753M Census populations . . . . . . 779
5
pg 174
5Précispg 190
In 2005 the World Health Organization reported on the impact of chronic diseases in low, middle, and high income countries. The presentation focused on premature loss of life and on the economic impact of deaths during individuals’ most productive years. With the impact of chronic diseases in the United States long an area of concern, we summarize one perspective in the Venn diagrams on the next page, looking at diabetes, cardiovascular
disease (cVd), chronic kidney disease (cKd), and end-stage renal disease (eSrd). ¶ The growth of diabetes in the Medicare population — from 16.1 percent in 1997 to 24.6 percent in 2007 — is associated with a 32 percent increase in the proportion of Medicare costs consumed by patients with the disease. Cardiovascular disease, including hypertension, has long been an issue within the Medicare population. But while growth in the treated eSrd population has also long been reported, cKd has received little attention, despite the increased frequency of its diagnosis and the doubling of its associated costs. Taken together, expenditures for the care of patients who have cKd or eSrd now total 32 percent of the Medicare budget — up from 18.5 percent just ten years ago. The expanding size of the eSrd program, and projections that it will double in the next ten years (see Figure 2.1) suggest that the population at risk for kidney disease should be addressed with detection and prevention strategies to reduce the long-term burden of eSrd. ¶ The size of the eSrd population hit a new high in 2007, with 527,283 patients under treatment, while the number of new cases — precisely 111,000 — was almost exactly the same as in 2006. The number of patients starting dialysis, or returning to dialysis after a failed kidney transplant or the recovery of kidney function, reached 116,073, a 0.9 percent increase. Interestingly, the number returning from a failed transplant dropped to 5,398 from 5,578 in 2006. The number restarting dialysis, however, grew 12.3 percent, to a new high of 3,031. ¶ Peritoneal dialysis now accounts for 5–6 percent of the incident and prevalent dialysis populations, continuing to fall from peaks of 13 and 11 percent in the 1990s. The number of kidney transplants reached 17,513 in 2007, while the prevalent transplant population rose 3.6 percent, to 158,739, despite continued growth in the number of patients on the transplant wait list. The median time on the wait list was 678 days. ¶ In 2006, 41 percent of prevalent dialysis patients had a functioning fistula (see Figure hp.11), exceeding the 1997 KdoQi target of 40 percent, and leading to a new target of 66 percent. Fistula placement rates, however, appeared to peak in 2006, and in 2007 fell for the first time. The steep fall in graft placement rates appears to be slowing, while catheter placement rates continue to fall, reaching a level below that of 1991 and perhaps contributing to the recent decline in rates of hospitalization for vascular access infection (see Figure 6.4). ¶ Many patients receive no nephrologist care, dietary care, or treatment with erythropoietin stimulating agents (eSas) prior to beginning eSrd therapy. These findings sug-gest that planning for the transition to eSrd is poor, and that the Medicare cKd education benefit, included in the 2008 Medicare Improvements for Patients and Providers Act (MiPPa), needs to address the selection of patient modality and dialysis access, preemptive kidney transplantation, and cardiovascular risk factors. ¶ As of March, 2007, mean monthly hemoglobin levels have fallen below 12 g/dl. Seven percent of prevalent dialysis patients now have a mean monthly level less than 10 g/dl, and the percentage with a mean level above 13 g/dl has fallen slightly, to 16.7 percent. These changes may reflect concerns over high levels reported in clinical trials (cHoir and creaTe) in 2006, changes mandated by the Fda and cMS to eSa package inserts, and changes in eSa pay-ments by cMS when hemoglobin levels exceed 13 g/dl for three months. ¶ After rising steadily over several years, rates of hospitalization for infection again fell in 2007 — an important change in patient morbidity. Incident-based mortality rates continue to fall for those on eSrd treatment
Contents192 • Trends in patient counts & spending
194 • Trends in modalities
196 • Trends in quality of care
198 • Trends in hospitalization & mortality
200 • Trends in expenditures
202 • Summary
United States Renal Data System2009 Annual Data Report
Volume Two: Atlas of End-Stage Renal Disease in the United States
National Institutes of HealthNational Institute of Diabetes
& Digestive & Kidney DiseasesDivision of Kidney, Urologic,
& Hematologic Diseases
pr
Vol 2esrd
5
Précispg 189
The bodies of the elements are united and in them there is neither gravity nor lightness. Gravity and lightness are produced in the mixture of the elements.
Leonardo da Vinci
PrécisAn introduction to end-stage renal disease in the United States
United States Renal Data
System2009 Annual Data Report
Volume One
Atlas of Chronic Kidney Disease in the United States
5Précispg 192
paii Summary statistics on reported ESRD therapy in the United States, by age, race, ethnicity, gender, & primary diagnosis, 2007
IncidenceA December 31 point prevalence Kidney transplantsAdj. Adj. Deceased Living ESRD
Count % rateB CountC % rateB DialysisC % TxC % donor donor deathsD
0-19 1,304 1.2 15 7,596 1.4 85 2,200 0.6 5,396 3.4 564 365 10320-44 13,831 12.5 126 97,941 18.6 893 53,530 14.5 44,411 28.0 3,287 2,248 4,79345-64 42,184 38.0 611 234,190 44.4 3,283 152,216 41.3 81,974 51.6 5,816 2,822 26,20665-74 25,446 22.9 1,424 104,941 19.9 5,870 82,842 22.5 22,099 13.9 1,571 548 22,86875+ 28,234 25.4 1,735 82,615 15.7 5,124 77,756 21.1 4,859 3.1 208 58 33,842Unknown * . . . White 72,668 65.5 273 321,485 61.0 1,222 205,421 55.7 116,064 73.1 6,850 4,488 58,894African American 31,561 28.4 998 166,962 31.7 5,111 136,853 37.1 30,109 19.0 3,449 829 24,440Native American 1,254 1.1 495 7,067 1.3 2,713 5,364 1.5 1,703 1.1 148 93 953Asian/Pacific Islander 5,106 4.6 396 25,840 4.9 1,911 17,208 4.7 8,632 5.4 828 589 2,943Other/unknown 411 0.4 5,929 1.1 3,698 1.0 2,231 1.4 171 42 582Hispanic 15,057 13.6 508 77,680 14.7 2,408 57,604 15.6 20,076 12.6 1,689 785 9,573Non-Hispanic 95,943 86.4 342 449,603 85.3 1,613 310,940 84.4 138,663 87.4 9,757 5,256 78,239Male 62,239 56.1 445 296,585 56.2 2,038 202,171 54.9 94,414 59.5 7,078 3,650 48,046Female 48,758 43.9 284 230,688 43.8 1,357 166,369 45.1 64,319 40.5 4,368 2,391 39,766Unknown * * * * Diabetes 48,871 44.0 155 197,037 37.4 619 160,346 43.5 36,691 23.1 3,534 1,302 39,890Hypertension 30,657 27.6 99 127,935 24.3 407 103,488 28.1 24,447 15.4 2,406 854 24,883Glomerulonephritis 7,571 6.8 24 81,599 15.5 260 39,268 10.7 42,331 26.7 2,267 1,535 6,066Cystic kidney disease 2,633 2.4 9 24,828 4.7 79 9,889 2.7 14,939 9.4 878 697 1,498Urologic disease 1,554 1.4 5 13,139 2.5 42 7,444 2.0 5,695 3.6 251 172 1,768Other known cause 14,141 12.7 46 56,468 10.7 182 33,518 9.1 22,950 14.5 1,488 1,065 9,554Unknown cause 4,635 4.2 15 20,747 3.9 65 13,498 3.7 7,249 4.6 468 295 3,388Missing cause 938 0.8 2 5,530 1.0 12 1,093 0.3 4,437 2.8 154 121 765All 111,000 354 527,283 1,665 368,544 158,739 11,446 6,041 87,812 Unadjusted rateG 361 1,698 Total transplantsH 17,513
Wait-list for kidney & kidney/pancreas transplantsNew Median
listings N, as of time on in 2007 12.31.07 list (yrs)0-17 805 780 0.7518-34 4,049 8,247 1.4235-49 9,600 22,001 1.6050-64 13,444 30,751 1.5565+ 5,023 11,776 1.58Male 19,644 42,608 1.49Female 13,275 30,944 1.63White 19,711 39,405 1.39African American 9,612 25,954 1.76Native American 397 922 1.57Asian/Pacific Islander 2,404 5,394 1.59Other/unknown 797 1,880 1.54Hispanic 5,278 13,175 1.67Non-Hispanic 27,643 60,380 1.52Diabetes 10,940 23,879 1.40Hypertension 6,493 16,382 1.69Glomerulonephritis 5,980 14,403 1.75Cystic kidney disease 2,429 4,661 1.32Urologic disease 582 1,522 1.93Other known cause 4,873 9,595 1.45Unknown cause 1,101 2,401 1.65Missing cause 523 712 0.90Blood type A 10,845 20,957 1.33B 4,748 11,916 1.71AB 1,273 2,095 1.15O 16,055 38,587 1.65PRA 0% 19,823 41,756 1.431-9 3,190 6,612 1.3610-79 5,445 13,538 1.6480+ 2,638 9,381 2.38Unknown 1,825 2,268 1.09Total 32,921 73,555 1.54
Medicare & non-Medicare spendingMedicare spending for ESRD, 2007(billions of dollars)
SAF paid claims (Parts A & B) 21.062% incurred but not reported 0.42HMO-Medicare risk 2.14Organ acquisition 0.26
Total Medicare costs 23.88Non-Medicare spending for ESRD, 2007(billions of dollars)
EGHP (MSP) 2.43Patient obligations 4.29Non-Medicare patients 4.72
Total non-Medicare costs 11.44Total ESRD costs, 2007 35.32Change in Medicare spending, 2006 to 2007
Total 2.6Per patient year 0.4
Adjusted for inflation -2.3 to -3.8%Medicare spending per patient year, 2007
ESRD $61,768 Hemodialysis $73,008 Peritoneal dialysis $53,446 Transplant $24,572
A Incident counts: include all known ESRD patients, regardless of any incomplete data on patient characteristics and of U.S. residency status.
B Includes only residents of the 50 states and Washington D.C. Rates are adjusted for age, race, and/or gender using the estimated July 1, 2005 U.S. resident population as the standard population. All rates are per million population. Rates by age are adjusted for race and gender. Rates by gender are adjusted for race and age. Rates by race are adjusted for age and gender. Rates by disease group and total adjusted rates are adjusted for age, gender, and race. Adjusted rates do not include patients with other or unknown race.
C Patients are classified as receiving dialysis or having a functioning transplant. Those whose treatment modality on December 31 is unknown are assumed to be receiving dialysis. Includes all Medicare and non-Medicare ESRD patients, and patients in the U.S. Territories and foreign countries.
D Deaths are not counted for patients whose age is unknown.
E Age is computed at the start of therapy for incidence, on December 31 for point prevalence, at the time of transplant for transplants, and on the date of death for death.
F Includes patients whose modality is unknown.G Unadjusted total rates include all ESRD patients in
the 50 states and Washington D.C.H Total transplants as known to the USRDS; 26
transplants with unknown donor type excluded from counts.
I Adjustments using the CMS inflation adjustment for the medical component, and the Bureau of Labor Statistics inflationary adjustment.
* Values for cells with ten or fewer patients are suppressed. “.” Zero patients in this cell.
Volume OneCKD
4
Chapter details
Précis An introduction to chronic kidney disease in the United States: highlights from Volume One . . . . . . . . .17
Summary statistics & predictive models for CKD • Descriptive parameters; metabolic abnormalities • CKD claims; prescription drug therapy • Biochemical levels & control • Hospitalization & mortality • CKD claims & physician visits • A cute kidney injury
One Chronic kidney disease in the adult NHANes population . . . . . . . . . . . . . . . . .35
Strategies for identifying CKD • Comorbidity burden • Clinical & biochemical abnormalities • Awareness, treatment, & control of disease conditions • Predictive models for CKD; mortality
Two Renal function measures in the adolescent NHANes population . . . . . . . . . . . . . . . . .49
Characteristics of U .S . adolescents • Associations of abnormal GFR • Trends in renal function
Three Chronic kidney disease identified in the claims data . . . . . . . . . . . .59
Incidence & prevalence of CKD in the U .S . • CKD as defined by the new diagnosis codes • Comorbidity burden in patients with CKD • Defining CKD through laboratory data
Four Care of patients with chronic kidney disease . . . . .71
Identified CKD & physician follow-up • Laboratory evaluations prior to ESRD • Prescription drug therapy prior to ESRD • Biochemical levels & drug therapy prior to ESRD
Five Morbidity & mortality . . . .83Hospitalization rates in CKD & non-CKD patients • Infectious hospitalization rates • Mortality rates • Rates of stroke & mortality
Six Cardiovascular disease in patients with chronic kidney disease . . . . . . . . . . . . .95
CKD stage & cardiovascular disease • Geographic variations in CVD & procedure use • Survival, care, & costs of patients with CVD
Seven The transition to esRD . . . . . . . . . . . . . . . . . . 105
Patient care prior to ESRD • Laboratory testing prior to ESRD • Medication continuity in the transition to ESRD • Prescription drug therapy in the transition to ESRD • Dialysis access placement in the transition to ESRD
Eight Acute kidney injury . . . . 119Characteristics of patients with acute kidney injury • Overall rates of acute kidney injury • Patient care & outcomes following AKI hospitalization • Patient outcomes following AKI hospitalization
Nine Costs of chronic kidney disease . . . . . . . . . . . 131
Overall costs of chronic kidney disease • PPPM components of costs for CKD
5
pg 176
united states renal data system2009 Annual Data Report
Atlas of Chronic Kidney Disease& End-Stage Renal Disease
in the United States
USRDS Coordinating Center 914 South 8th Street Suite S206 Minneapolis, MN 55404 1.888.99USRDS www.usrds.org
2009 United States Renal Data System Annual Data Report
Susan Everson | portfolio | page 8

349
outcomeshospitalization CKD (vol 1): 3.1–13; ESRD (vol 2): Chap-ter 3, 7.21–22, 8.7–9, 10.9–12
rehospitalization CKD (vol 1): 3.1, 3.8–13, 3.b; ESRD (vol 2): 3.14–20
mortality CKD vol 1): 3.1, 3.8–17, 3.c, 4.d; ESRD (vol 2): hp-14, 4.1, 4.7–11, Chapter 5, 7.17–18, 7.26, 8.10–12, 10.9–12
survival CKD (vol 1): 1.16, 4.2, 4.7–10; ESRD (vol 2): 4.4, 4.h, 4.28–31, 5.b, 8.13
standardized hospitalization & mortality ratios ESRD (vol 2): 10.9–12costsPart D CKD (vol 1): 5.9–11, 5,d, 7.9–18, 7.b; ESRD (vol 2): 6.9–12, 6.d, 6.16–18, 11.10–16
overall CKD (vol 1): Chapter 7; ESRD (vol 2): Chapter 11data analysisanalytical methods CKD (vol 1): pg 137; ESRD (vol 2): pg 421
data files available to researchers pg 454
agreements for release of data pg 465
ESRDVOL2ESRD
349
had an AV access either in use or maturing at the first out-patient dialysis treatment, up only slightly from 35.5 percent in 2007. In July, 2010, CMS began requiring the reporting of monthly data on vascular access use; as these data become available, the USRDS will examine prevalent access use and transitions in vascular access during the first months of dialysis.
The lack of progress in the use of catheters is a major concern, and may relate to the persistently high rates of hospitalization for infection (noted in Chapter Three). The CDC restarted its infection control survey in 2012 and 2013, collecting data on unit practices related to access prepa-ration for cannulation, on reuse practices, and on use of catheter antibiotic lock solutions. These practices will be assessed in the future to help guide targets for infection control and to reduce related complications. ◆ Figure 2.1; see page 431 for analytical methods.
1010
ESRDVOL2ESRD
Perc
ent o
f pat
ient
s
20
40
60
80
100
10-<11
12+
11-<129-<10
<9
92 94 96 98 00 02 04 06 08 10 12 0
92 94 96 98 00 02 04 06 08 10 12
Hem
oglo
bin
(g/l)
9
10
11
12
Mea
n m
onth
ly E
PO d
ose
(1,0
00 u
nits
)
2
6
10
14
EPO
Hemoglobin
Months after initiation
1 2 3 4 5 6
Hem
oglo
bin
(g/d
l)
9
10
11
12
13
1999 2003 2007 2011
00 01 02 03 04 05 06 07 08 09 10 11
Perc
ent o
f pat
ient
s
0
20
40
60
80
1000-<2 months 2-<4 4-<6 6+
Months after initiation
1 2 3 4 5 6
Mea
n w
kly
EPO
dos
e (in
1,0
00s)
6
8
10
12
1999 2003
2007 2011
Q2 Q3 Q4 Q2 Q3 Q4 Q22010 2011 2012
Perc
ent o
f pat
ient
s
0
1
2
3
4
5 All White Black/African American Other/unk.
349
2.9 Mean monthly hemoglobin & mean EPO dose per week: peritoneal dialysis patients
When compared to 2007 patients, those starting peritoneal dialysis in 2011 did so with lower hemoglobins one month post-initiation, at 10.9 and 10.2 g/dl, respectively. In 2011, mean hemoglobin levels at six months following initiation were 10.9 g/dl. The mean EPO dose per week was 10,482 units, compared to 10,542 in 2007.
In 2011, the proportion of peritoneal dialysis patients receiving IV iron in each of the first six months of dialysis was 11.6 percent, in contrast to 32 percent among hemodialysis patients.
The percentage of peritoneal patients receiving a transfusion has increased little since 2010, and in June of 2011 was slightly higher in whites compared to blacks/African Americans, at 3.1 and 3.0, respectively. ◆ Figures 2.10–13; see page 432 for analyt-ical methods. Incident peritoneal dialysis patients; for Figure 2.13, each month includes patients with a claim for peritoneal dialysis.
At the end of 2011, 66 percent of prevalent peritoneal dialysis patients had a mean monthly hemoglobin less than 11 g/dl, while 26 percent had hemoglobins that ranged from 11 g/dl to less than 12 g/dl . The mean EPO dose per week fell each month within the year, ending at 10,104 units in the month of December, while the mean hemoglobin at that time was 10.5 g/dl. ◆ Figures 2.8–9; see page 432 for analytical methods. Period prevalent peri-toneal dialysis patients.
vol 2 vol 2
vol 2 vol 2
vol 2
vol 2
2.8 Patient distribution, by mean monthly hemoglobin (g/dl): peritoneal dialysis patients
2.10 Mean monthly hemoglobin after peritoneal dialysis initiation, by year 2.12 Months with IV iron in the first six
months of PD (EPO-treated patients)2.11 Mean EPO dose per week after peritoneal dialysis initiation, by year
2.13 Peritoneal dialysis patients receiving transfusions, by race
349
chapter seven trends in transplantation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 .1
patients wait-listed or receiving a deceased donor transplant within one year of initiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 .2
likelihood of dying while awaiting transplant . . . . . . . . . . . . . . . . . 7 .8
cumulative incidence of transfusion in wait-listed patients, by PRA . . . 7 .9
donation rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 .10
deceased & living donor transplants . . . . . . . . . . . . . . . . . . . .7 .12, 7 .14
adj . transplant rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 .13, 7 .15
transplant outcomes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 .17–18
acute rejection within the first year post-transplant . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 .19
cardiac & infectious hospitalizations post-transplant . . . . . . . . . . . 7 .22
cumulative incidence of PTLD & diabetes . . . . . . . . . . . . . . . . 7 .23–24
adj . rate of outcomes after transplant . . . . . . . . . . . . . . . . . . . . . 7 .25
causes of death with function . . . . . . . . . . . . . . . . . . . . . . . . . . 7 .26
immunosuppression use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 .27
follow-up care & screening in the first 12 months post-transplant . . . 7 .28
medication use in the first six months post-transplant . . . . . . . . 7 .33–35
chapter eightdistribution of incident ESRD pediatric patients, by primary diagnosis . 8 .a
vaccination rates in pediatric patients . . . . . . . . . . . . . . . . . . . . 8 .5–6
adj . all-cause mortality rates in pediatric patients (from day one) . . . . 8 .10
adj . five-year survival in pediatric patients . . . . . . . . . . . . . . . . . . 8 .13
chapter tendistribution of patients, by unit affiliation . . . . . . . . . . . . . . . . . . 10 .1
dialysis unit & patient counts, by unit affiliation . . . . . . . . . . . . . . . 10 .3
preventive care in diabetic dialysis patients, by unit affiliation & number of tests . . . . . . . . . . . . . . . . . . . . .10 .4–6
all-cause standardized hospitalization & mortality ratios . . . . . . . 10 .9–12
chapter elevenESRD spending, by payer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 .1
costs of the Medicare & ESRD programs . . . . . . . . . . . . . . . . . . . .11 .2
estimated numbers of point prevalent ESRD patients . . . . . . . . . . . .11 .3
annual percent change in Medicare ESRD spending . . . . . . . . . . . .11 .4
total Medicare dollars spent on ESRD, by type of service . . . . . . . . . .11 .5
total Medicare ESRD expenditures overall & PPPY, by modality . . . . 11 .6–7
chapter twelvecomparison of unadj . ESRD incidence & prevalence worldwide . . . . .12 .1
geographic variations in the incidence of ESRD . . . . . . . . . . . . . . 12 .2
incidence of ESRD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12 .3, 12 .a
incident patients with ESRD due to diabetes . . . . . . . . . . . . . . . 12 .4–5
prevalence of ESRD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 .6, 12 .b
percent distribution of prevalent dialysis patients, by modality . . .12 .7, 12 .c
prevalent rates of functioning grafts . . . . . . . . . . . . . . . . . . . 12 .8, 12 .d
transplant rates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 .9, 12 .e
guide to topicsguide to topics
348
populationsnhanes CKD (vol 1): Chapter 1
new patients ESRD (vol 2): p.a, hp-8, hp-9, Chapter 1, 8.1–4
existing patients CKD (vol 1)1.a, 2.1–4, 2.a–b; ESRD (vol 2): p.a, Chapter 1
transplant patients ESRD (vol 2): Chapter 7
CKD datasets CKD (vol 1): 2.a–b, 2.2–4
pediatric patients ESRD (vol 2): Chapter 8
international comparisons ESRD (vol 2): Chapter 12
Part D prescription drug coverage CKD (vol 1): Chapter 5, 7.9–18, 7.a–b; ESRD (vol 2): Chapter 6, 7.29–35, 7.a–b, 11.10–16diseasesidentifying CKDCKD (vol 1): Chapters 1 & 2
anemia ESRD (vol 2): 1.23–24, 1.g
infections CKD (vol 1): 3.6, 3.13; ESRD (vol 2): 3.1, 3.a, 3.4–8, 5.3, 8.9, 8.12
cardiovascular disease CKD (vol 1): 3.5, 3.10, 3.13, Chapter 4; ESRD (vol 2): 3.1, 3.3, 3.a, 3.9–13, Chapter 4, 5.3
in the annual data reportdiabetes CKD (vol 1): Chapter 1; ESRD (vol 2): hp-9, 1.7–8, 1.15, 1.d–g
acute kidney injury CKD (vol 1): Chapter 6treatment preventive care & laboratory testing CKD (vol 1): Chapter 2; ESRD (vol 2): 1.f–g, 2.14–17, 2.a, 7.28, 8.5–6, 10.4–6
awareness, treatment, & control CKD (vol 1): 1.b
physician care & follow-up care CKD (vol 1): 2.c, 2.9–12, 2.g–i; ESRD (vol 2): hp-3, hp-4, hp-5, hp-10, 1.f, 1.22
drug therapy CKD (vol 1): 4.b, 4.3–5, 5.13–20; ESRD (vol 2): hp-5, 4.c, 4.12–17, 7.29–30, 7.32–35, 7.a–b, 8.14–17, 8.b–c
anemia treatment ESRD (vol 2): 1.23, 2.3, 2.5–7, 8.14–16, 10.7–8
vascular access ESRD (vol 2): hp-11, 2.18–20
transplantation ESRD (vol 2): hp-12, hp-13, Chapter 7
cardiovascular procedures CKD (vol 1): 4.a; ESRD (vol 2): 4.a, 4.2–3
ESRD PROVIDERS348
OVER THE PAST DECADE, improvements in ESRD care have been addressed by several organizations. Most notable is CMS’s assessment of provider performance through its Dialysis Facility Compare project (www.medicare.gov/dialysisfacilitycompare), which reports provider measures based on quality improvement targets and KDOQI published guidelines. The project is currently undergoing transition to a full web-based data entry sys-tem, which will include monthly laboratory data from providers. There have been challenges in implementing the system, but by the summer of 2013 most providers should be entering data. Until that time, some elements traditionally reported under the Clinical Performance Measures (CPM) program will not be up-to-date.
In Figure 2.1 we present data on KDOQI targets for dial-ysis therapy, vascular access, and clinical indicators, and look at other targets based on practice guidelines and safety issues. Dialysis adequacy has inched up slightly, with 95 percent of hemodialysis patients achieving a URR of ≥65 percent — a new high — and 87 percent of perito-neal dialysis patients achieving a Kt/V of ≥1.7. Forty-six and 51 percent, respectively, of diabetic ESRD patients received recommended glycemic control testing and lipid testing in 2011, while 65 percent of ESRD patients received an influenza vaccination.
Views of anemia treatment continue to evolve, as safety concerns about targeting hemoglobin levels above 11 g/dl have emerged from clinical trials. The new FDA label for ESAs, released in June, 2011, states “In controlled tri-als, patients experienced greater risks for death, serious adverse cardiovascular reactions, and stroke when admin-istered erythropoiesis-stimulating agents (ESAs) to target a hemoglobin level of greater than 11 g/dL.” The label also states that “No trial has identified a hemoglobin target level, ESA dose, or dosing strategy that does not increase these risks.” The FDA recommends that clinicians “Use the lowest dose that will maintain a hemoglobin level suffi-cient to reduce the need for RBC transfusions.” Based on new recommendations, these changes should reduce the risk of adverse cardiovascular events and strokes.
The new FDA recommendations and the concerns arising from clinical trials appear to be guiding clinical
practice. At six months after initiation in 2011, the mean hemoglobin level in patients is now lower than its peak seen in 1999. And the mean ESA dose used to achieve these levels is below that of 1999.
Data on iron dosing practices show that, in the first six months of dialysis treatment, more than 50 percent of patients receive monthly IV iron, a new high. Another 20 percent receive IV iron in five of the first six months of dialysis therapy.
Trends in the monthly percentage of patients receiving a transfusion have changed since 2010. Among hemodial-ysis patients, the transfusion rate, at 2.7–2.9 percent at the beginning of 2010, reached 3.3–3.8 percent in the first six months of 2012. Among peritoneal dialysis patients, the rate has increased from 2.3–2.9 to 3.0–3.9. Further anal-ysis will be needed into how these changes might affect dialysis patients on the waiting list for transplantation.
Comprehensive patient care has long been a focus of the ADR. Among diabetic patients, there has been a slight decline in the percentage of patients receiving recom-mended glycemic control testing and lipid testing, so that the overall rate of comprehensive diabetic monitoring has fallen from 17 percent in 2008–2009 to 14.4 percent in 2010–2011. It is not clear whether the new bundled pay-ment system has had an impact on this aspect of patient care, or whether this decrease will have a collateral effect on diabetes-specific hospitalizations.
Influenza vaccination rates have risen from 46 percent in 2001 to 65 percent in 2011 — still below the HP2020 target of 90 percent. The percentage of patients vacci-nated against pneumococcal pneumonia, peaking at 25.8 percent in 2008–2009 (reported in the 2012 ADR), has not improved, remaining at 25.6 percent in 2010–2011.
Vascular access has received increased attention since the release of data showing high catheter use at initiation and increasing rates of hospitalization due to infection in the first months of therapy. Unfortunately, the use of catheters at the start of ESRD remains high and relatively unchanged, at 81 percent. The CMS Fistula First program has worked to increase the use of arteriovenous (AV) fis-tulas, and to transition patients off dialysis catheters. Just 37 percent of 2011 incident hemodialysis patients, however,
introduction
ESRD PROVIDERS
348
ESRD PROVIDERS
Chapter Ten
ESRD PROVIDERS
Perc
ent o
f pat
ient
s
20
40
60
80
100
10-<11
12+
11-<129-<10
<9
92 94 96 98 00 02 04 06 08 10 12 0
92 94 96 98 00 02 04 06 08 10 12 5
10
15
20
Hem
oglo
bin
(g/d
l)
9
10
11
12
EPO
Hemoglobin
Mea
n m
onth
ly E
PO d
ose
(1,0
00 u
nits
)
Months after initiation
1 2 3 4 5 6
Hem
oglo
bin
(g/d
l)
8
9
10
11
12
13
1999 2003 2007 2011
00 01 02 03 04 05 06 07 08 09 10 11
Perc
ent o
f pat
ient
s
0
10
20
30
40
50
60 0-<2 months 2-<4 4-<6 6+
Months after initiation
1 2 3 4 5 6
Mea
n w
kly
EPO
dos
e (in
1,0
00s)
5
10
15
20
25
30
35 1999 2003 2007 2011
Q2 Q3 Q4 Q2 Q3 Q4 Q22010 2011 2012
Perc
ent o
f pat
ient
s
0
1
2
3
4
5
All White Black/African American Other/unk.
348
2.3 Mean monthly hemoglobin & mean EPO dose per week: hemodialysis patients
When compared to 2007, incident hemodialysis patients starting dialysis in 2011 did so with lower hemoglobins one month post-initiation, at 10.7 and 10.1 g/dl, respectively. In 2011, the mean hemoglobin level six months after initiation was slightly below 10.9 g/dl.
The mean EPO dose per week at six months after initiation was 15,213 units in 2011, compared to 20,506 units in 2007.
Between 2010 and 2011, the proportion of incident hemodi-alysis patients receiving IV iron in each of the first six months of dialysis showed a relative increase of 12 percentage points, to 52.1 percent.
The percentage of hemodialyis patients receiving a trans-fusion has increased little since 2010, and in June of 2011 was slightly higher in whites compared to blacks/African Americans, at 3.5 and 3.1 percent, respectively. ◆ Figures 2.4–7; see page 432 for analytical methods. Incident hemodialysis patients; for Figure 2.7, each month includes patients with a claim for hemodialysis.
At the end of 2011, 58 percent of prevalent hemodialysis patients had a mean monthly hemoglobin less than 11 g/dl, while 31 percent had hemoglobins that ranged from 11 g/dl to less than 12 g/dl. The mean EPO dose per week fell each month within the year, ending at 12,460 in the month of December, more than 3,600 units less than the average dose at the end of 2010; the mean hemoglobin at the end of 2011 was 10.7 g/dl. ◆ Figures 2.2–3; see page 431 for analytical methods. Period prevalent hemodialysis patients.
vol 2 vol 2
vol 2 vol 2
vol 2
vol 2
2.2 Patient distribution, by mean monthly hemoglobin (g/dl): hemodialysis patients
2.4 Mean monthly hemoglobin after hemodialysis initiation, by year 2.6 Months with IV iron in the first six
months of HD (EPO-treated patients) 2.5 Mean EPO dose per week after hemodialysis initiation, by year
2.7 Hemodialysis patients receiving transfusions, by race
treatment under the dialysis composite rate
esrd dataesrd data
348
appearing each year in the annual data report
précis distribution of general Medicare patients & costs for CKD, CHF, diabetes, & ESRD . . . . . . . . . .p .1
summary statistics on reported ESRD therapy in the U .S . . . . . . . . . . . . . . . . . . . . . . . . . . . p .a
counts of new & returning dialysis patients . . . . p .2
patient counts, by modality . . . . . . . . . . . . . . p .3
chapter one incident & prevalent counts, by modality . . . . . . . 1 .1
adj . rates of ESRD & annual change . . . . . . . 1 .2, 1 .10
geographic variations in adj . rates of ESRD . . . . . . . . . . . . . . . . . . . . . 1 .3, 1 .11
incident counts & adj . rates of ESRD . . . . . . . . 1 .4–7
prevalent counts & adj . rates of ESRD . . . . . . 1 .12–15
patient distribution, by modality & payer . . . 1 .17, 1 .19
access use at first outpatient hemodialysis, by pre-ESRD nephrology care . . . . . . . . . . . . . 1 .22
mean hemoglobin at initiation, by pre-ESRD ESA treatment . . . . . . . . . . . . . . 1 .23
variations in mean hemoglobin by HSA, 2011 . . . 1 .24
patient distribution at initiation, by eGFR . . . . . . 1 .25
patient demographics & adj . rates, by ESRD network . . . . . . . . . . . . . . . . . . . . 1 .a–c
counts & adj . rates of ESRD, by modality . . . . . 1 .d–e
pre-ESRD nephrologist care . . . . . . . . . . . . . . . 1 .f
patients initiating dialysis with laboratory values outside the normal limit . . . . . . . . . . . . 1 .g
chapter twopatient distribution, by mean monthly hemoglobin . . . . . . . . . . . . . . . . 2 .2, 2 .8
mean monthly hemoglobin & mean EPO dose per week . . . . . . . . . . . . 2 .3, 2 .9
mean monthly hemoglobin after initiation . . . . . . . . . . . . . . . . . . . . 2 .4, 2 .10
mean EPO dose per week after initiation . . . . 2 .5, 2 .11
IV iron in the first six months of dialysis . . . . 2 .6, 2 .12
transfusions . . . . . . . . . . . . . . . . . . . . . 2 .7, 2 .13
preventive care in ESRD patients with diabetes . . . . . . . . . . . . . . . . . . . . . 2 .14–17
vaccination rates . . . . . . . . . . . . . . . . . . . . . 2 .a
access use at initiation . . . . . . . . . . . . . . 2 .18–20
chapter threechange in adj . all-cause & cause-specific hospitalization rates, by modality . . . . . . . . . . . 3 .1
adj . admission rates & days, by modality . . . . . . .3 .2
all-cause & cause-specific hospitalization rates in hemodialysis patients . . . . . . . . . . . . . .3 .a
all-cause and cause-specific rehospitalization 30 days after live hospital discharge . . . . . . . . .3 .14–20
chapter five adj . mortality (from day 90), by modality & year of treatment . . . . . . . . . . . .3 .a
adj . mortality (from day one) in the first year of hemodialysis . . . . . . . . . . . . . . . . . . . . . . . .5 .3
adj . mortality in prevalent hemodialysis patients, by vintage . . . . . . . . . . . . . . . . . . . .5 .4
adj . five-year survival probabilities, from day one, in the incident ESRD population . . . . . 5 .b
mortality rates in the ESRD & general Medicare populations . . . . . . . . . . . . . . . . . . . . . . . . .5 .c
adj . mortality in the ESRD & general populations . . . . . . . . . . . . . . . . . 5 .5–6
chapter six sources of prescription drug coverage in Medicare enrollees . . . . . . . . . . . . . . . . . 6 .2–4
Part D non-LIS enrollees with gap coverage or no deductible, by modality . . . . . . . . . . . . . .6 .7
total estimated net Part D payment for enrollees . . . . . . . . . . . . . . . . . . . . . . . . 6 .9
PPPY Medicare & out-of-pocket Part D costs for enrollees . . . . . . . . . . . . . . . . . . . . . . . . . . 6 .9
12-month probability of reaching the coverage gap in Part D non-LIS enrollees . . . . . . 6 .e
Part D non-LIS enrollees who reach each coverage phase . . . . . . . . . . . . . . . . . . 6 .13
top 15 drugs used by Part D-enrolled dialysis patients, by net costs & drug class . . . . . . . . . . 6 .8
Design for 2014 United States Renal Data System Annual Data Report (not published)
atlas of chronic kidney disease in the united states
Volume OneVolume One
8 guide to topics in the adr 10 ckd figures & tables appearing each year 12 volume one highlights 14 infographics 18 ntroduction 23 chapters 119 reference tables: ckd 137 analytical methods
précis an introduction to ckd in the u.s. . . . . . . . . . . . . . 23 one ckd in the general population. . . . . . . . . . . . . . . . . 41 two identification & care of patients with ckd . . . . . . . . . . 51 three morbidity & mortality in patients with ckd . . . . . . . . . . . . 63 four cardiovascular disease in patients with ckd. . . . . . . . . . . 73 five Part D prescription drug coverage in patients with ckd . . . . . . . . . . . . . . . . . . . 83 six acute kidney injury . . . . . . . . . . . 95 seven costs of ckd. . . . . . . . . . . . . . . 107
348
atlas of end-stage renal disease in the united states
Volume TwoVolume Two
156 esrd figures & tables appearing each year 158 esrd program highlights 160 infographics 164 introduction 169 chapters 345 reference tables: esrd 421 analytical methods 454 usrds products & services 461 glossary 469 cms forms
454 data requests 465 agreements for release of data
précis an introduction to esrd in the u.s.. . . . . . . . . . . . 169healthy people 2020 . . . . . . . . . . . . . . 193 one incidence, prevalence, patient characteristics, modalities . . . 215 two clinical indicators & preventive care . . . . . . . . . . . 229 three hospitalization . . . . . . . . . . . . 237 four cardiovascular disease . . . . . . . 249 five mortality . . . . . . . . . . . . . . . . . 263 six part d prescription drug coverage in esrd patients . . . . . 271 seven transplantation. . . . . . . . . . . . 283 eight pediatric esrd . . . . . . . . . . . . . . 295 nine rehabilitation/quality of life & nutrition special studies . . . . 307 ten esrd providers . . . . . . . . . . . . . 315 eleven costs of esrd . . . . . . . . . . . . . . 325 twelve international comparisons . . . 333
349
Susan Everson | portfolio | page 9

Other printed &digital material

iPad apps for the 2013, 2012, & 2011 USRDS Annual Data Reports
Susan Everson | portfolio | page 11
behold the threaden sails,Borne with the invisible and creeping wind,Draw the huge bottoms through the furrow’d sea,Breasting the lofty surge…
William Shakespeare Henry V
introduction
CKD in the general population
identification & care of patients with CKD
identification of CKD
hospitalization & mortality
cardiovascular disease
Part D drug coverage
acute kidney injury
costs of CKD
8 / 11
»
part D Drug Coverage
CarDiovasCular Disease: ContinueD
CHF
No CKD 50,637 57.3 61.6 15.7 23.8 1.2 49.2 5.4 All CKD 17,659 52.0 67.0 19.9 23.3 0.9 53.2 7.5 Stages 1–2 782 57.8 66.4 18.5 24.3 0.9 53.3 6.3 Stage 3 5,403 55.3 68.2 21.5 24.4 1.1 57.6 7.5 Stages 4–5 3,617 42.4 72.3 19.9 21.0 0.6 55.1 9.3AMI No CKD 3,581 64.5 76.9 48.3 12.6 1.1 68.8 6.0 All CKD 1,110 58.8 76.4 42.3 16.9 0.9 63.7 7.2 Stages 1–2 45 55.6 80.0 35.6 22.2 0.0 60.0 13.3 Stage 3 342 56.7 76.3 45.9 19.3 0.9 63.2 8.2 Stages 4–5 236 58.5 81.8 43.2 15.7 0.0 71.6 8.1PAD No CKD 62,503 49.0 45.0 16.8 12.3 0.5 48.3 2.0 All CKD 14,713 50.5 58.3 22.3 17.2 0.8 53.9 4.7 Stages 1–2 751 55.1 62.3 22.6 14.8 0.5 53.8 5.2 Stage 3 4,648 54.3 60.9 23.3 17.3 0.8 57.9 4.2 Stages 4–5 2,538 44.1 65.1 24.7 17.9 0.7 58.0 6.3CVA/TIA No CKD 41,016 51.6 46.3 22.8 14.6 0.8 55.6 2.1 All CKD 8,739 53.2 59.7 26.4 18.1 0.8 57.8 4.5 Stages 1–2 459 58.2 59.7 25.5 17.6 0.7 56.2 3.7 Stage 3 2,820 55.9 60.9 27.9 17.8 0.7 62.8 4.3 Stages 4–5 1,418 46.0 64.9 28.0 16.8 0.6 59.4 6.2AFIB No CKD 57,243 50.4 61.4 9.2 53.3 2.8 48.1 8.3 All CKD 12,432 50.1 66.5 14.2 48.7 1.8 51.7 12.8 Stages 1–2 598 56.7 66.2 14.7 49.7 2.5 57.0 11.9 Stage 3 4,005 52.7 67.3 13.9 50.4 2.1 56.4 13.2 Stages 4–5 2,180 42.3 69.6 15.0 47.5 1.4 51.7 16.1ICD/CRT-D No CKD 430 77.9 84.9 26.5 32.1 3.5 65.1 20.7 All CKD 178 64.0 88.2 26.4 35.4 2.2 62.9 18.5 Stages 1–2 13 53.8 84.6 30.8 46.2 0.0 69.2 7.7 Stage 3 66 65.2 87.9 28.8 31.8 4.5 66.7 13.6 Stages 4–5 31 58.1 87.1 29.0 32.3 0.0 48.4 38.7Revascularization: PCI No CKD 4,275 67.2 76.8 83.8 9.1 1.2 79.1 3.8 All CKD 767 62.8 78.4 79.0 14.5 1.7 72.9 5.7 Stages 1–2 43 76.7 76.7 79.1 16.3 0.0 72.1 7.0 Stage 3 298 62.1 81.5 80.5 14.4 2.7 73.5 5.0 Stages 4–5 130 46.9 75.4 76.2 17.7 0.0 77.7 10.0Revascularization: CABG No CKD 956 65.9 86.9 33.3 18.3 1.4 80.3 31.8 All CKD 142 63.4 85.9 33.1 23.9 2.1 81.0 31.0 Stages 1–2 10 70.0 90.0 20.0 30.0 0.0 80.0 50.0 Stage 3 60 63.3 86.7 28.3 28.3 3.3 85.0 30.0 Stages 4–5 13 61.5 92.3 23.1 30.8 0.0 84.6 23.1No cardiac event No CKD 390,635 44.8 29.8 5.0 2.4 0.0 45.2 0.2 All CKD 25,334 63.1 47.4 8.4 4.7 0.1 56.0 0.6 Stages 1–2 1,630 66.1 42.2 7.4 3.7 0.0 57.4 0.7 Stage 3 9,418 68.3 49.7 8.9 4.4 0.1 61.6 0.5 Stages 4–5 3,853 60.8 58.4 9.9 4.5 0.1 57.9 1.0
scroll to see more
4.b Cardiovascular disease & pharmacological interventions (row percent), by CKD status, 2011
Although prior publications have dem-onstrated a strong inverse relationship between the likelihood of cardioprotec-tive therapy use and advanced CKD stage, our overview of 2011 prevalent Medicare patients with Part D coverage provides some reassurance that this practice pat-tern has changed. While ACeI/ArB use in CHF patients does decline with advancing CKD, the same is not true of beta blocker therapy, which increases with CKD stage. The use of beta blocker therapy after AMI also demonstrates a change with respect to CKD. Despite earlier data indi-cating underutilization inversely related to eGFr, 76 percent of 2011 CKD patients with AMI — and a surprising 82 percent of those with Stage 4–5 CKD — received a beta blocker.
The treatment of AFIB presents a special clinical problem in CKD patients. In com-parisons of warfarin to newer oral antico-agulants in CKD patients, dabigatran was associated with the largest reduction in risk of ischemic stroke and apixaban with the greatest reduction in risk of serous hemorrhage (Hart et al, 2012). None of these trials, however, enrolled patients with estimated creatinine clearances of <25 ml/min. Despite the absence of clinical trial data, approval in the U.S. was given to newer oral anticoagulants — dabigatran, rivaroxaban, and apixaban — for preven-tion of ischemic stroke in non-valvular AFIB in patients with estimated creatinine clearances as low as 15. All three agents are approved for use in patients with CKD of Stage 3 or Stage 4, but not for those with Stage 5 CKD. In 2011, 2.4 percent of AFIB and with CKD of Stages 4–5 received dabi-gatran. Close attention will need to be paid to the expected increase in serious hemor-rhagic events associated with these agents in patients with advanced CKD, but avail-able data imply that newer oral anticoagu-lants are superior to warfarin in efficacy and safety. • Table 4.b. January 1 point prevalent patients with Medicare Parts A, b, & D enrollment & with a cardiovascular diag-nosis or procedure in 2011.
précisan introduction to chronic kidney disease in the United States
vol 1
ACEI/ Beta Clopid- Dabi- Amio- N ARB Blocker ogrel Warfarin gatran Statin darone
scroll for more text «ICD-9-CM
CODES
585.1 Chronic kidney disease, Stage 1 585.2 Chronic kidney disease,
Stage 2 (mild) 585.3 Chronic kidney disease,
Stage 3 (moderate) 585.4 Chronic kidney disease,
Stage 4 (severe) 585.5 Chronic kidney disease,
Stage 5 (excludes 585.6: Stage 5, requiring chronic dialysis.*)
CKD unspecified identified by multiple codes including 585.9, 250.4x, 403.9x, & others.
*In USRDS analyses, patients with ICD-9-CM code 585.6 & with no ESRD 2728 form or other indication of ESRD are considered to have code 585.5; see Appendix for details.CKD stage estimates are from a single measurement. For clinical case definition, abnormalities should be present ≥ 3 months.
volume one
Atlas of Chr� ic Kidney Diseasein the United � ates
volume one
Atlas of Chronic Kidney Diseasein the United � ates
National Institutes of HealthNational Institute of Diabetes & Digestive & Kidney DiseasesDivision of Kidney, Urologic, & Hematologic Diseases
volume one
Atlas of Chr� ic Kidney Diseasein the United � ates
volume one
Atlas of Chronic Kidney Diseasein the United � ates
National Institutes of HealthNational Institute of Diabetes & Digestive & Kidney DiseasesDivision of Kidney, Urologic, & Hematologic Diseases
navigation guide
view additional information
close a pop-up window
swipe left & right to view different chapters in the report
swipe up & down to read a chapternavigation tap screen
to see navigation tools
slide up to open a tab and down to close
tap to see additional figures and tables
tables of contents all titles are links to the chapters and sections they describe
«12
move through chapters in full screen or thumbnail view
return to the first page
return to the most recently viewed screen
view the chapter index
browse thumbnails
bookmark favorite chapters
introduction
incident counts & rates
incident rates & racial differences
prevalent counts & rates
incident & prevalent modality
patient characteristics
summary
Incidence, prevalence, patient characteristics, & modality
Here and there awareness is growing that man, far from being the overlord of all creation, is himself part of nature, subject to the same cosmic forces that control all other life. Man's future welfare and probably even his survival depend upon his learning to live in harmony, rather than in combat, with these forces.
Rachel Carson,"Essay on the Biological Sciences"
CHAPTER ONEINCIDENCE, PREVALENCE, PATIENT CHARACTERISTICS, & MODALITY
113 | 119
In 2010, the number of new patients starting therapy on hemodialysis declined for the first time in more than three decades. The population initiating on peritoneal dialysis, in contrast, grew for the second year in a row, and now accounts for 6.6 percent of patients with a known dialysis modality. This change may foreshadow those to come
under the new bundled payment system, with its clear incentives for this form of home dialysis. Total incident dialysis cases rose 0.27 percent in 2010, to 114,083, while 2,863 patients received a preemptive transplant as their first ESRD modality; a total of 116,946 patients began ESRD therapy in 2010.
The rate of new ESRD cases per million population, which has been relatively stable since 2000, fell 2.0 percent in 2010, to 348. Growth continues to be driven by a relatively linear increase in the number of patients age 45–64; growth in the population age 65 and older, in contrast, has slowed considerably, but a slight upturn is present among those age 65–74, which could reflect the emergence of the post-World War II baby boomers into retirement age.
The incidence of ESRD in the black/African American population has finally started to decline, overall and for ESRD due to diabetes. Among those age 20–39, however, differences between whites and blacks/African Americans continue to be dramatic, with rates among the latter up to 3.8 times greater. Rates are also considerably higher for blacks/African Americans age 60 and older than for their white counterparts, though the gap is beginning to narrow.
The December 31, 2010 prevalent population included 383992 patients on hemodialysis and 29,733 on peritoneal dialysis, as well as 179,361 with a functioning kidney transplant; the total treated ESRD population thus rose to 593,086 — growth of 4 percent from 2009, which is the smallest increase in 30 years. The rate of prevalent ESRD cases reached 1,752 per million population, an increase of 1.1 percent from 2009, and also the slowest growth in the last three decades.
Insurance coverage in the dialysis population continues to change, with more incident dialysis patients now covered by Medicare Advantage. Private insurance, in contrast, is dominant among patients who receive a preemptive kidney transplant. In the 2010 prevalent population, 84 percent of hemodialysis patients and 79 percent of those on peritoneal dialysis had some type of Medicare coverage, com-pared to just 65 percent of those with a transplant.
Nephrology care prior to ESRD continues to be a concern. Since the 2005 introduction of the new Medical Evidence form (2728), with fields addressing pre-ESRD care, there has been little progress made in this area (pre-ESRD data, however, should be interpreted with cau-tion because of the potential for misreporting). Forty-three percent of new ESRD patients in 2010, for example, had not seen a nephrologist prior to beginning therapy. And among these patients, 88 percent of those on hemodialysis began therapy with a catheter, compared to 54 percent of those who had received a year or more of nephrology care. Among those with a year or more of pre-ESRD nephrologist care, in contrast, 26 percent began therapy with a fistula — eight times higher than the rate among non-referred patients.
Data on patient care at the start of ESRD therapy show that the percentage of patients receiving an erythropoiesis stimulating agent (ESA) prior to initiation continues to decline, reaching just 20 percent in 2010 compared to one-third in the early part of the decade. This may reflect concern over potential adverse events when hemoglobin levels are targeted to a level above 12 g/dl. The mean hemoglobin at initiation of ESRD treatment is now 9.73 g/dl. These changes place different demands on care after the initiation of dialysis, and may alter the likelihood of a patient receiving a blood transfusion. The balance between cardiovascular risk with a hemoglobin greater than 12 g/dl and the risk of transfusion with lower hemoglobin levels needs to be addressed by patients and their physicians, particularly in the case of patients contemplating a kidney transplant, for whom sensitization from blood transfusions is to be avoided if at all possible.
The percentage of dialysis patients beginning therapy with an estimated glomerular filtration rate (eGFR, calculated with the CKD-EPI formula) above 15 ml/min/1.73 m2 continues to rise. It is not clear if this progressive increase is the result of severe comorbidity or a simple numerical starting point based on the ability to calculate the eGFR. Hopefully, symptoms and complications of uremia are still the primary indications for starting renal replacement therapy rather than a simple number, one which has been brought into question in recent years in controlled trials of early versus later dialysis initiation.
Biochemical data, collected on the Medical Evidence form since 2005, show that 57 percent of new patients in 2010 had an albumin less than the lower limit of normal, and 55 percent had a hemoglobin lower than 10 g/dl. Total cholesterol was greater than 200 mg/dl in 16 percent of patients, while 28 percent had an LDL level greater than 100 mg/dl, and 58 percent had an HDL level less than 40 mg/dl. Among patients with diabetes, 28 percent had a hemoglobin A1c level greater than 7 percent.
Recent changes and new incentives in the bundled prospective payment system for dialysis patients, introduced in January, 2011, may alter several characteristics of the incident and prevalent populations — particularly, due to cost incentives, the mix of peritoneal dialysis and hemodialysis patients. It is unclear how the expansion of peritoneal dialysis will affect patient outcomes, and how the new incentives will impact the emerging daily home hemodialysis population; provider incentives for this therapy are less clear, particularly as related to training. A more detailed assessment of the bundled payments is presented in Chapter Ten, and in future ADRs the USRDS will continue to assess the impact of this payment system on the ESRD population. » Figure 1.1. Incident & December 31 point prevalent ESRD patients.
scroll for more text
INCIDENT COUNTS & RATES
introduction
78 82 86 90 94 98 02 06 10
Num
ber o
f pat
ient
s (in
thou
sand
s)
0
50
100
150
200Hemodialysis (2010: 105,923)Peritoneal dialysis (7,703)Total dialysis (114,083)Transplant (2,863)
78 82 86 90 94 98 02 06 100
100
200
300
400Hemodialysis (2010: 383,992)Peritoneal dialysis (29,733)Transplant (179,361)OPTN transplant wait list (87,932)
Incident Prevalent
1.1 Incident & prevalent patient
counts (USRDS), by modalityvol 2
Science kills credulity and superstition, but to the well-balanced mind it enhances the feeling of
wonder, of veneration, and of kinship which we feel in the presence of the miraculous universe.
John Burroughs, Accepting the Universe
data sources
CKD in the general populationchapter one
identification and care of patients with CKD
chapter two
hospitalization and mortality in patients with CKD
chapter three
cardiovascular disease in patients with CKDchapter four
prescription drug coverage in CKD patientschapter five
acute kidney injurychapter six
costs of CKDchapter seven
reference tables
introduction
summary
Medicare Part D enrollment patterns
Medicare Part D coverage plansoverall costs of Part D enrollment
coverage phase analyses for Part D enrollees
Medicare Part D prescription drug use & costs
terms used in the Part D analyses
prescriptiondrug coverage in esrd patientsmedicare part d
There’s battle lines being drawnNobody’s right if everybody’s wrongYoung people speaking their mindsGetting so much resistance from behindI think it’s time we stop, hey, what’s that soundEverybody look what’s going down
Stephen Stills, “For What It’s Worth”
chapter six
CHAPTER 7
2 | 10
As of September, 2008, 26 million Medicare-enrolled elderly and
disabled people, as well as individuals with ESRD, were enrolled in
a Medicare Part D prescription-drug plan (PDP). Before 2006, these
patients obtained prescription drug coverage through various insur-
ance plans, state Medicaid programs, or pharmaceutical-assistance
programs, received samples from physicians, or paid out-of-pocket.
After 2006, however, the majority obtained Part D coverage. As
shown on the next page, 58–59 percent of elderly CKD and general
Medicare patients were enrolled in Part D in 2008, compared to 72,
61, and 53 percent of hemodialysis, peritoneal dialysis, and kidney
transplant patients.
The retiree drug subsidy, designed to encourage employers to
supply prescription coverage to Medicare-covered retirees that is
at least as valuable as the Medicare Part D standard plan, provides
employers with a tax-free rebate for 28 percent of retirees’ drug
costs. Other patients are enrolled in employer group health plans or
government/military plans (“creditable coverage”) which provide cov-
erage that is equivalent to or better than Part D.
The proportion of patients with no known source of drug cover-
age is highest in the peritoneal dialysis and transplant populations.
Given that many of these patients are employed, it is likely that some
have sources of prescription drug coverage not tracked by Medicare.
Prior to the start of the Medicare Part D program in 2006, patients
dually-enrolled in Medicare and Medicaid received prescription ben-
efits under state Medicaid programs. The Part D program, however,
offers a substantial low-income subsidy (LIS) benefit to enrollees with
limited assets and income, including those who are dually-enrolled.
The LIS provides full or partial waivers for many out-of-pocket cost-
sharing requirements, including premiums, deductibles, and copay-
ments, and provides full or partial coverage during the coverage gap
(“donut hole”). Compared to patients in the general Medicare popu-
lation, a higher proportion of dialysis, transplant, and elderly CKD
patients receive LIS benefits, and thus, in general, pay proportionally
lower out-of-pocket costs for their Part D prescriptions.
Part D does not cover every medication prescribed to Medicare
enrollees. Several drug categories — including over-the-counter
medications, barbiturates, benzodiazepines, anorexia and weight
loss or gain medications, prescription vitamins (except for prenatal
vitamins), and cough and cold medications — are excluded from the
Part D program by law.
The Medicare Part D program works in concert with Medicare
Part B, which covers medications administered in physician offices
(e.g. erythropoiesis stimulating agents (ESAs) in CKD patients), those
administered during hemodialysis (e.g. ESAs, intravenous vitamin D
and iron products, IV antibiotics, and resuscitative medications), and
most immunosuppressant medications required in the three-year
period following a Medicare-covered kidney transplant. Medicare-
covered transplant patients lose eligibility for Part B benefits after
three years, but, if they become Medicare-eligible due to age or dis-
ability, they again become eligible for Part B for immunosuppressant
coverage. Patients whose kidney transplant is not covered by Medi-
care, but who become Medicare-eligible due to age or disability, can
enroll in and receive their immunosuppressant medications through
Part D. Prescription drugs not covered for beneficiaries under Part B
may be covered by Part D, but coverage depends on whether the
drug is included on the plan formulary.
Part D benefits can be managed through a stand-alone PDP or
through a Medicare Advantage (MA) plan, which provides medical
as well as prescription benefits. The majority of dialysis and trans-
plant patients are covered through PDPs (as patients may not enroll
in Medicare Advantage after ESRD onset), but data in this chapter
encompass both types of plans. » Figure 6.1. Point prevalent Medicare enrollees alive on January 1,
2008.
scroll for more text
06
Gen Med HTN CVD DM CKD HD PD Tx
Perc
ent o
f pat
ient
s
0
20
40
60
80
100
General Medicare
Part D with LIS Part D without LIS
Retiree drug subsidy Other creditable coverageNo known coverage
ESRD
61 Sources of prescription drug
coverage in Medicare enrollees, 2008
CHAPTER 7
9 | 10
chapter six summary
patients enrolled in medicare part d, 2008general medicare » 59% (fig 6.4)
incident esrd » hemodialysis 64% » peritoneal dialysis 50% » transplant 30% (fig 6.4)
prevalent esrd » hemodialysis 72% » peritoneal dialysis 61% » transplant 53% (fig 6.5)
medicare part d enrollees with low income subsidy, 2008 » general medicare 38% » hemodialysis 74% » peritoneal dialysis 64% » transplant 64% (fig 6.7)
total estimated medicare part d net payment for enrollees, 2008 » hemodialysis $1.18 billion » peritoneal dialysis $78 million » transplant $284 million (fig 6.14)
per person per year medicare part d costs for enrollees, 2008medicare costs » hemodialysis $5,397 » peritoneal dialysis $5,537 » transplant $4,961 (fig 6.15)
out-of-pocket costs » hemodialysis $456 » peritoneal dialysis $646 » transplant $575 (fig 6.15)
per person per year medicare part d costs for enrollees, 2008patients with low income subsidy » hemodialysis $6,645 » peritoneal dialysis $7,334 » transplant $6,553 (fig 6.16)
patients with no low income subsidy » hemodialysis $2,028 » peritoneal dialysis $2,341 » transplant $2,083 (fig 6.16)
part d non-lis enrollees who reach the coverage gap, 2008at 12 months » general medicare 23% » hemodialysis 47% » peritoneal dialysis 48% » transplant 45% (fig 6.21)
part d non-lis enrollees who reach catastrophic coverage after reaching the coverage gap, 2008at 9 months » general medicare 13% » hemodialysis 24% » peritoneal dialysis 26% » transplant 25% (fig 6.22)
2011 iPad app chosen by Adobe Systems as a Customer Success Story, and highlighted on their Digital Publishing Suite Showcase
http://tinyurl.com/pz7akqv

98,914
53,935
1996 2011
and 20%higherin the Mountain&Pacific states
1996 2011
43.2
28.1
rate per 100,000 population
and were greatest in theEast South Central Division,
at 54.1
Of the112,453patients initiatingdialysis treatment
in 2011,91%eventually began
treatment in afreestanding
facility
Geographicvariations in
pre-esrdnephrologist care
deserve greater attention from the physician community, as dialysis providers do not influence referral to a nephrologist prior to the start of ESRD treatment
and the meanhemoglobinamong patients
with pre-dialysis esa use declined,
Between 2008 & 2011,the percentage of pre-esrd patients receiving anESA
during a nephrologist o�ce visit fell,
the esadoseper administration
during a visit fell 16.4%,from
16,167iuto19.1%
to13,157 from
10.2g/dl
to9.6
from27.7%
80%67%
In the New England Census Division,
in the U.S.as a whole
of patients saw a
nephrologistprior to starting dialysis,
compared to
In 2011,
patients did not see a
nephrologistprior to startingdialysis therapy
In 2011,
patients received an esa
during a nephrologyvisit prior to esrd
Between 2008 & 2011, the mean number of
nephrologyo�ce visits
during the 6 months
before starting dialysis fell9%
2%of new ESRD patients
used theckd education
benefit approved by Congress,and made available
to Medicare beneficiariesin January 2010*
Fewerthan
*usrds 2013 adr, page 117.
In 2011,
patients initiated hemodialysis
treatment with a
fistula
Among prevalent dialysis patients age 20–39,expected
remaininglifetimes
increased2to3years
between 2004and 2011
Mortality ratesare consistently
highestinnew england
andlowestin thepacific states
Infectionaccounts for a
growingpercentage
of deaths during thefirst yearafter dialysis
initiation
Infectionaccounts for10%
of deaths inmonth 10after dialysis initiation
Among incident patients,the proportion of deaths
caused bysudden cardiac death
is highestin thefirst monthof dialysis,
and declines to its lowestlevel during the
sixth month
Progress in reducingmortality is a core measure
of success for dialysis providers,and first-year mortality
in freestanding facilities has declined
consistently since 2004
1996 2003
per 100 patient years
2011
1996 2003 2011
27.8
30.6
26.022.4 22.5
18.2
Unadjustedmortality ratesamongincident
patientsare6.5%
lower thanin 1996 Unadjusted
mortality ratesamongprevalent
patientsare19%
lower thanin 1996
per 100 patient years
with-drawal
unknown other
infection
Month 1
Month 1 Month 3 Month 10
other cvdeath
with-drawal
unknown other
infection
Month 6
30.1%
Sudden cardiacdeath
down15%since
2003
down19%since
2003
Infection
21.1%othercv death
with-drawal
unknown other
other cvdeath
other cvdeath
with-drawal
unknown other
other cvdeath
with-drawal
unknown other
sudden cardiac
death
sudden cardiac
death
sudden cardiac
death6.3%10.4%
9.6%
suddencardiac death
accounted for3in10deaths among prevalent
dialysis patients in 2011
cardiovasculardeathaccounted
for4in10deaths amongprevalent dialysis
patients in 2011
There has beenlinear growth
in theprevalent
dialysis population
Counts of deathsbegan to turn away
from this lineartrend during the early 2000s,
a manifestationof improving
survival1996 20112003
Patientcounts
Patientdeaths
other
overalladmission
ratesper patient year
continueto fall
2.582003 2.36
2010
first-year
for twitter
22feweradmissions per100 patient years
2.012004 1.85
2011
prevalent
16feweradmissions per100 patient years
While hospitalization rates have fallen overall, there are
geographicvariations
in the degree of change acrossu.s. census divisions
50moreadmissions per 100 patient years
first-year
rates,2010
moun-tain & pacificdivisions
east north central & middle atlanticdivisions
In
states,hospitalizationrates have tended to
increasesince2003/2004
TheEast NorthCentralstates
have seen theleast
improvementin hospitalization rates
As a primary morbidity in the dialysispopulation,
provide a for provider efforts to improve
patient care & outcomesoverall
admissionrates
per patient year continue
to fall
2.012004 1.85
2011
prevalent
16feweradmissions per100 patient years
facilities receiving a
higher rating with alternate
method
facilities receiving a
lower rating with alternate
method
cms rating
facilities receiving a
higher rating with alternate
method
facilities receiving a
lower rating with alternate
method
cms rating
facilities receiving a
higher rating with alternate
method
facilities receiving a
lower rating with alternate
method
cms rating
61% 57%
15%
67%
25%
30%
55%
16%
60%47%
18%
56%
26%
21%
42%
20%
53% 47%
17%
58%
23%
27%
48%
17% 17% 17%
8%20%
8%
8%
16%
10%
29% 29%
13%
34%
15%
17%
33%
15%
cms rating vs rating based
exclusively on smr & shr
cms rating vsrating with 50% weight
to smr & shr
changes inStar Ratings
withalternate
approachesto defining quality
cms rating vs rating based exclusively on
Kt/V & hypercalcemia metrics
cms rating vs rating based exclusively on
fistula & catheter metrics
cms rating vs rating that reflects uncertainty in
estimates of standardized outcome ratios
2008 2009 2010 2011
2008 2009 2010 2011 2012
30% cardiovascular (overall)
22% infection (overall)
62% acute coronary syndrome
25% arrhythmia
46% heart failure & cardiomyopathy
71% pneumonia & influenza
27% intestinal infection with c. difficile
71% chronic pulmonary disease
36% dialysis access infection
Percent of month-to-month variation due to seasonal effects
orig lines
cardiovascular (overall)
infection (overall)
acute coronary syndrome
arrhythmia
heart failure & cardiomyopathy
intestinal infection with c. difficile
pneumonia& influenza
dialysis access infection, including peritonitis
In the prevalentdialysis population,hospitalization ratesfor many causespeak
in January,
February,& March
There has been clearprogress
across thecountry in reducing
hospital admissionsdue tocardiovascular
disease
There has been clearprogress
across thecountry in reducing
hospital admissionsdue to
In the prevalent dialysis population,hospitalization rates for many causes
peakin January,February,& March
In the prevalent dialysis population,hospitalization rates for many causes
peakinJanuary,February, & March
Dialysis access infections,in contrast,
peak inthe summer
since 2003/2004,overall
admissionsper patient year have
fallen
overall admissions
per patient year have
fallensince 2003/2004
admissionsforheart
failure have as well
admissionsforfluid
overload,however,are2.5times
higher than in 2003/2004
and admissionsfor infection
arehigheras well
admissionsforfluid
overloadare2.5times
higher than in 2003/2004
admissionsfor
havefallenas well
first-year prevalent
first-year prevalent
first-year prevalent
16.2% 14.4%
16.2% 14.4%
19% 23.5%
19% 23.5%
admissionsfor
havefallensince2003/2004
first-year prevalent
19% 23.5%
5% 0.8%
5% 0.8%
admissionsfor infection
haveincreased
since 2003/2004first-year prevalent
5% 0.8%
98,914
53,935
1996 2011
and 20%higherin the Mountain&Pacific states
1996 2011
43.2
28.1
rate per 100,000 population
and were greatest in theEast South Central Division,
at 54.1
Of the112,453patients initiatingdialysis treatment
in 2011,91%eventually began
treatment in afreestanding
facility
Geographicvariations in
pre-esrdnephrologist care
deserve greater attention from the physician community, as dialysis providers do not influence referral to a nephrologist prior to the start of ESRD treatment
and the meanhemoglobinamong patients
with pre-dialysis esa use declined,
Between 2008 & 2011,the percentage of pre-esrd patients receiving anESA
during a nephrologist o�ce visit fell,
the esadoseper administration
during a visit fell 16.4%,from
16,167iuto19.1%
to13,157 from
10.2g/dl
to9.6
from27.7%
80%67%
In the New England Census Division,
in the U.S.as a whole
of patients saw a
nephrologistprior to starting dialysis,
compared to
In 2011,
patients did not see a
nephrologistprior to startingdialysis therapy
In 2011,
patients received an esa
during a nephrologyvisit prior to esrd
Between 2008 & 2011, the mean number of
nephrologyo�ce visits
during the 6 months
before starting dialysis fell9%
2%of new ESRD patients
used theckd education
benefit approved by Congress,and made available
to Medicare beneficiariesin January 2010*
Fewerthan
*usrds 2013 adr, page 117.
In 2011,
patients initiated hemodialysis
treatment with a
fistula
Among prevalent dialysis patients age 20–39,expected
remaininglifetimes
increased2to3years
between 2004and 2011
Mortality ratesare consistently
highestinnew england
andlowestin thepacific states
Infectionaccounts for a
growingpercentage
of deaths during thefirst yearafter dialysis
initiation
Infectionaccounts for10%
of deaths inmonth 10after dialysis initiation
Among incident patients,the proportion of deaths
caused bysudden cardiac death
is highestin thefirst monthof dialysis,
and declines to its lowestlevel during the
sixth month
Progress in reducingmortality is a core measure
of success for dialysis providers,and first-year mortality
in freestanding facilities has declined
consistently since 2004
1996 2003
per 100 patient years
2011
1996 2003 2011
27.8
30.6
26.022.4 22.5
18.2
Unadjustedmortality ratesamongincident
patientsare6.5%
lower thanin 1996 Unadjusted
mortality ratesamongprevalent
patientsare19%
lower thanin 1996
per 100 patient years
with-drawal
unknown other
infection
Month 1
Month 1 Month 3 Month 10
other cvdeath
with-drawal
unknown other
infection
Month 6
30.1%
Sudden cardiacdeath
down15%since
2003
down19%since
2003
Infection
21.1%othercv death
with-drawal
unknown other
other cvdeath
other cvdeath
with-drawal
unknown other
other cvdeath
with-drawal
unknown other
sudden cardiac
death
sudden cardiac
death
sudden cardiac
death6.3%10.4%
9.6%
suddencardiac death
accounted for3in10deaths among prevalent
dialysis patients in 2011
cardiovasculardeathaccounted
for4in10deaths amongprevalent dialysis
patients in 2011
There has beenlinear growth
in theprevalent
dialysis population
Counts of deathsbegan to turn away
from this lineartrend during the early 2000s,
a manifestationof improving
survival1996 20112003
Patientcounts
Patientdeaths
other
Infographics/ data visualizationResearch and design
Susan Everson | portfolio | page 12

The contents of this article, graphics, images, and all other material (the “Content”), are for your private use and informational purposes only. If you have a medical emergency, do not rely on the Content to treat your condition; call your doctor or go to a hospital immediately. The Content is not intended to be professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health professional with any questions you may have regarding any medical concerns or conditions.
Beginning in 2003, more than 100,000 U.S. patients have begun chronic dialysis each year. Although dialysis is a life-saving treatment, death rates on dialysis have historically been much higher than in the general population.
WorldKidney DayMarch 12, 2015
Since 2003, however, dialysis patients have been living longer. One-year survival after dialysis initiation has improved for 8 consecutive years.
Dialysispatients
are livinglonger
0 2 4 6 8
20%
40%
60%
80%
100%
years
PATIENTSTART DATE
2011
2010
2009
2008
2007
2006
2005
2004
2003
0 2 4 6 8 0 2 4 6 8 0 2 4 6 8
compared to 74%
of those starting in 2003.
Age20–44
Age45–64
Age65–79
78% of patientsstarting dialysis
in 2011 survived
1 year,
Andsurvivalon dialysis has
improvedacross age
groups
Of patients startingdialysis in 2008,
46%survived
4 years,
comparedto39%
of those starting in 2003.
82% 59%47%77%
53%40%
3-year survival
3-year survival4-year survival
Dialysis patientsare livinglonger
World Kidney Day
The Peer Kidney Care Initiative (“Peer”) is a collaboration among 13 dialysis providers: American Renal Associates, Atlantic Dialysis Management Services, Centers for Dialysis Care, DaVita HealthCare Partners, Dialysis Clinic, Inc. (DCI), DSI Renal, Fresenius Medical Care, Independent Dialysis Foundation, Northwest Kidney Centers, Renal Ventures Management, Satellite Healthcare, The Rogosin Institute, and U.S. Renal Care.
The goal of Peer is to conduct and disseminate research that is important to all stakeholders in the dialysis community, including patients, physicians, provider organizations, payers, and state and federal governments. As a part of its outreach, Peer is dedicated to the translation of research findings to the clinical setting, with the aim of improving the quality of dialysis patient care.
Steadilyimprovingsurvival
among successive waves of new dialysis patients from 2004 to
2011 has resulted in
103,970years of
life gained
In patients who began dialysis in
2006 and 2007 and have been followed
into 2012, almost 40,000 years of life have been
gained, relative to the survival of counterparts beginning dialysis in 2003.
@peerkidney
peerkidney.org
Years0 5 10
2.9 additional years
2.7
2.9
3.3
2.4
1.7
1.2
1.0
0.7
0.5
0.5
0.4
0.2
0.3
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80-84
85+
ExpectedremaInInglIfetImes
after the startof dialysis have
increasedfor patients of all ages
ExpectedremaInIng
lIfetImesafter the startof dialysis have
increasedfor patients of all ages
2003 2011
Advances in dialysis technique, medication therapy, vaccinations, and vascular access care are all likely contributors to improved survival.
For patients beginning dialysis before age 40, lifetimes have increased by more than 2.5 years, while for patients beginning dialysis between ages 40 and 60, lifetimes have increased by more than 1 year.
U.S. dialysis providers are committed to the
continuous improvement of patient health and
well-being.
@peerkidney
peerkidney.org
The Peer Kidney Care Initiative (“Peer”) is a collaboration among 13 dialysis providers: American Renal Associates, Atlantic Dialysis Management Services, Centers for Dialysis Care, DaVita HealthCare Partners, Dialysis Clinic, Inc. (DCI), DSI Renal, Fresenius Medical Care, Independent Dialysis Foundation, Northwest Kidney Centers, Renal Ventures Management, Satellite Healthcare, The Rogosin Institute, and U.S. Renal Care.
The goal of Peer is to conduct and disseminate research that is important to all stakeholders in the dialysis community, including patients, physicians, provider organizations, payers, and state and federal governments. As a part of its outreach, Peer is dedicated to the translation of research findings to the clinical setting, with the aim of improving the quality of dialysis patient care.
Figures: Peer Kidney Care Initiative 2014 Report: Dialysis Care and Outcomes in the United States. Am J Kidney Dis. 2015;65(6). Pre-ESRD nephrologist care: United States Renal Data System, 2014 USRDS annual data report: Epidemiology of kidney disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2014. CDC recommendations: http://www.cdc.gov/dialysis/prevention-tools/core-interventions.html.
Rates of admission for dialysisaccess infection
have declined
These changes may reflect shifts in diagnosis coding
Data on admissions for any infection show that there has been
no progressin lowering the rate of
hospitalization for infection
At the same time, however, rates
of admission forbacteremia/septicemia
have been on the rise
Patients who receive at least one year of care from a nephrologist before starting dialysis are more likely to begin therapy with a fistula
14% of patientshospitalized for an access
infection are
rehospitalizedwithin 10 days
200443.9 admissions
per 100 patient years
201144.2
Therisk of access
infection is highest with a dialysis catheter, & lowestwith anarteriovenous fistula
1in3patients is readmitted
within
30DAYS
2004
2011
Dialysis access infection
The CDC’s Hemodialysis BSI Prevention Collaborative recommends the following interventions to prevent bloodstream infections in outpatient dialysis units:• monthly observations of opportunities for
hand hygiene, and the sharing of results with staff
• quarterly observations of vascular access care and adherence to aseptic technique
• staff training and competency evaluation
• patient education/engagement, with standardized training on preventing infections
• efforts to reduce catheter use and address barrriers to permanent vascular access placement
• use of chlorhexidine for skin antisepsis
• disinfection of catheter hubs
• application of antimicrobial ointment or povidone-iodine ointment to catheter exit sites during dressing changes
June 2015
The contents of this article, graphics, images, and all other material (the “Content”) are for your private use and informational purposes only. If you have a medical emergency, do not rely on the Content to treat your condition; call your doctor or go to a hospital immediately. The Content is not intended to be professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health professional with any questions you may have regarding any medical concerns or conditions.
Hospitalizations for dialysis access infection are lowest in the winter,
& peak in
the summer
Possible reasons for this peak include bacterial growth in
pools, lakes, and wells, and the impact of perspiration on bacterial growth.
2008 2009 2010 2011
July, August, September
January, February,
March
help patientsprevent
infectionthis summer &
Remind patientsto keep tap water and water from swimming pools, lakes, & rivers away from their access site
to keep the skin near their access clean between dialysis treatments
Dialysis access infection
These infections are of particular concern in the summer, when their rates rise
Access infections (including peritonitis) are a major cause of hospitalization for dialysis patients
The Healthy People program, operated by the Department of Health & Human Services, aims to improve the health of all Americans.
April 2015
The rate of new cases of end-stage renaldisease (ESRD) has been
3852003
3592012
344.3TARGET
In 2012,the rate
was 6.6%lowerthan in 2003
Progress has been made in several disadvantaged subgroups
Blacks/African Americans
15% 24% 17% 12%
American Indian/ Alaska Native Hispanic
HP2020 OBJECTIVE CKD-8Reduce the number of new cases
of ESRD per million population
TARGET
344.3
decliningHealthy People 2020
Healthy People 2020 (HP2020) was launched
in December of 2010. It centers on health-
related goals and objectives to be met
by the year 2020.
Significant progresshas been achieved in meeting goals related to
kidney disease
The contents of this article, graphics, images, and all other material (the “Content”) are for your private use and informational purposes only. If you have a medical emergency, do not rely on the Content to treat your condition; call your doctor or go to a hospital immediately. The Content is not intended to be professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health professional with any questions you may have regarding any medical concerns or conditions.
Healthy People 2020
The Peer Kidney Care Initiative (“Peer”) is a collaboration among 13 dialysis providers: American Renal Associates, Atlantic Dialysis Management Services, Centers for Dialysis Care, DaVita HealthCare Partners, Dialysis Clinic, Inc. (DCI), DSI Renal, Fresenius Medical Care, Independent Dialysis Foundation, Northwest Kidney Centers, Renal Ventures Management, Satellite Healthcare, The Rogosin Institute, and U.S. Renal Care.
The goal of Peer is to conduct and disseminate research that is important to all stakeholders in the dialysis community, including patients, physicians, provider organizations, payers, and state and federal governments. As a part of its outreach, Peer is dedicated to the translation of research findings to the clinical setting, with the aim of improving the quality of dialysis patient care.
Data obtained from the United States Renal Data System 2014 Annual Data Report (http://www.usrds.org/2014/view/v2_02.aspx). Revised HP2020 targets obtained from the HP2020 website, at https://www.healthypeople.gov/2020/topics-objectives/topic/chronic-kidney-disease.
More patients are receiving
at least one year of
nephrologist carebefore starting dialysis therapy
Less than 30% of black/African American & Hispanic patients receive the recommended care
Arteriovenous fistulas are associated with lower risks of vascular access infection & complications
25.7%2003
31.2%2003
33.1%2012
36.8%2012
CKD-10TARGET
29.8%
more patients are starting
dialysis with a fistula or maturing fistula as their
primary vascular access
CKD-11.3TARGET
34.5%
&
The death rate for dialysis patients is fallingOBJECTIVE CKD-14.1
Reduce thetotal death rate
TARGET
190.0per 1,000 patient
years at risk
OBJECTIVE CKD-14.3Reduce the
cardiovascular death rate
TARGET
80.9
OBJECTIVE CKD-14.2Reduce the death rate in the first 3 months of dialysis
TARGET
328.7
2372003
3872003
1162003
1812012
3122012
762012
The overalldeath rate
fell24%between
2003 & 2012
down19%
For many subgroups, death rates are well below the target
132 Asian135 Hispanic139 Black/African American144 American Indian /Alaskan Native
For white patients, the target has not yet been met
217
down35%
@peerkidney
peerkidney.org
May 2015
The contents of this article, graphics, images, and all other material (the “Content”) are for your private use and informational purposes only. If you have a medical emergency, do not rely on the Content to treat your condition; call your doctor or go to a hospital immediately. The Content is not intended to be professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health professional with any questions you may have regarding any medical concerns or conditions.
2004 2005 2006 2007 2008 2009 2010 2011
Adm
issi
ons
per 1
00 p
atie
nt y
ears
0
1
2
3
4
Months in the first year of dialysis
1 2 3 4 5 6 7 8 9 10 11 12
Adm
issi
ons
per 1
00 p
atie
nt y
ears
0
2
4
6
8
10
2003
2010
Adm
issi
ons
per 1
00 p
atie
nt y
ears
Admissions per 100
patient years
0
2
4
6
8
Months in the first year of dialysis
There is still, however,an increased risk of stroke in the first months of dialysis
and admissions for stroke in the first year
of dialysis therapy have declined1
There has been progress in lowering
the occurrence of stroke in dialysis
patients
In the prevalentpopulation, hospital
admissions forstroke fell
between 2004 & 2011
28%1
6.27.6
4.6
3.1
5.55.5
2 3 4 5 6
2003
2010
7 8 9 10 11 12
3.362004
2.432011
StrokeThe risk of stroke is considerably higher among dialysis patients than in the general population May is National Stroke
Awareness Month,encouraging everyone
to be aware of the impact of stroke, and to learn the warning signs
Among dialysis patients, ischemic stroke is approximately 4.5 times more common than hemorrhagic stroke2
Stroke
The Peer Kidney Care Initiative (“Peer”) is a collaboration among 13 dialysis providers: American Renal Associates, Atlantic Dialysis Management Services, Centers for Dialysis Care, DaVita HealthCare Partners, Dialysis Clinic, Inc. (DCI), DSI Renal, Fresenius Medical Care, Independent Dialysis Foundation, Northwest Kidney Centers, Renal Ventures Management, Satellite Healthcare, The Rogosin Institute, and U.S. Renal Care.
The goal of Peer is to conduct and disseminate research that is important to all stakeholders in the dialysis community, including patients, physicians, provider organizations, payers, and state and federal governments. As a part of its outreach, Peer is dedicated to the translation of research findings to the clinical setting, with the aim of improving the quality of dialysis patient care.
[1] Weinhandl E, Constantini E, Everson S, et al. Peer Kidney Care Initiative 2014 Report: Dialysis Care and Outcomes in the United States. Am J Kidney Dis. 2015;65(6):S1-S140. [2] Wetmore JB, Phadnis MA, Mahnken JD, et al. Race, ethnicity, and state-by-state geographic variation in hemorrhagic stroke in dialysis pa-tients. Clin J Am Soc Nephrol. 2014 Apr;9(4):756-63. [3] Wetmore JB, Ellerbeck EF, Mahnken JD, et al. Stroke and the “stroke belt” in dialysis: contribution of patient characteristics to ischemic stroke rate and its geographic variation. J Am Soc Nephrol. 2013 Dec;24(12):2053-61. [4] Shah M, Avgil Tsadok M, Jackevicius CA, et al. Warfarin use and the risk for stroke and bleeding in patients with atrial fibrillation undergoing dialysis. Circulation. 2014; 129:1196-1203. [5] Elliott MJ, Zimmerman D, Holden RM. Warfarin anticoagulation in hemodialysis patients: a systematic review of bleeding rates. Am J Kidney Dis. 2007; 50:433-440. [6] Chan KE, Edelman ER, Wenger JB, et al. Dabigatran and rivaroxaban use in atrial fibrillation patients on hemodialysis. Circulation. 2015;131:972-979. [7] Wetmore JB, Phadnis MA, Ellerbeck EF, et al. Relationship between stroke and mortality in dialysis patients. Clin J Am Soc Nephrol. 2015 Jan 7;10(1):80-9.
KNOW THE WARNING SIGNSRISK FACTORSHigh blood pressure
Cigarette smokingHigh blood cholesterol
Poor dietPhysical inactivity
& obesityfacedrooping
armweakness
speechdi�culty
time tocall 911
The rate of ischemic stroke in dialysis patients is highest in the southeastern states3
This “stroke belt” has been a focus of public health research since the 1960s
7
The risk of death is especially highright after a stroke,
& declinesthereafter7
36 mo24 mo12 mo6 mo3 mo1 mo7 days
Ad
just
ed h
azar
d r
atio
11.7
9.8
6.6
4.73.3
2.2 1.7
median life lost by a dialysis patient su�ering a stroke
@peerkidney
peerkidney.org
Published research offers no definitive conclusion about the efficacy of warfarin for stroke prevention in dialysis patients with atrial fibrillation. Most data, however, suggest that warfarin use does increase the risk of bleeding.4,5
New oral anticoagulants such as dabigatran, rivaroxaban, and apixaban have been tested in the general population, but the safety of these agents in dialysis patients is not entirely clear, based on an early report of observational data.6
The contents of this article, graphics, images, and all other material (the “Content”) are for your private use and informational purposes only. If you have a medical emergency, do not rely on the Content to treat your condition; call your doctor or go to a hospital immediately. The Content is not intended to be professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health professional with any questions you may have regarding any medical concerns or conditions.
July 2015
This rise in hospitalizations may be due in part to increased awareness by physicians.
More patients nowhave a monthly
hemoglobin level
<9 g/dl, which may promptdoctors to look for
causes of anemiaother than kidney
disease.
Admissions per 100
patient years1.82004
2004
2011
2.8%January
2010
2.32011
Among prevalentdialysis patients,hospital admissions
for GI bleeding have Increased,
and continue to vary across the country2
Middle Atlantic2.65
East North Central
2.8
Mountain1.45
Pacific1.9
U.S. 2.3
6.0%December
20123
In addition, the ESRD Prospective Payment System (introduced in 2011) includes an 18% greater
reimbursement*
for dialysis patients with GI bleeding,which may lead to greater vigilance on the part of doctors.*In the proposed changes to the PPS for 2016, this may change to 8%.
Gastrointestinalbleeding
GI bleeding is a significant cause of hospitalization & death for dialysis patients. Dialysis patients face a greatly
increased risk of GI bleeding. Their risk of an upper GI bleed, for example, is over 100 times higher than in the general population.1
@peerkidney
peerkidney.org
The Peer Kidney Care Initiative (“Peer”) is a collaboration among 13 dialysis providers: American Renal Associates, Atlantic Dialysis Management Services, Centers for Dialysis Care, DaVita HealthCare Partners, Dialysis Clinic, Inc. (DCI), DSI Renal, Fresenius Medical Care, Independent Dialysis Foundation, Northwest Kidney Centers, Renal Ventures Management, Satellite Healthcare, The Rogosin Institute, and U.S. Renal Care.
The goal of Peer is to conduct and disseminate research that is important to all stakeholders in the dialysis community, including patients, physicians, provider organizations, payers, and state and federal governments. As a part of its outreach, Peer is dedicated to the translation of research findings to the clinical setting, with the aim of improving the quality of dialysis patient care.
1Yang J-Y, et al. Trends in acute nonvariceal upper gastrointestinal bleeding in dialysis patients. J Am Soc Nephrol. 2012 Mar;23(3):495-506. 2Weinhandl E, et al. Peer Kidney Care Initiative 2014 Report: Dialysis Care and Outcomes in the United States. Am J Kidney Dis. 2015;65(6). 3United States Renal Data System, 2014 USRDS annual data report: Epidemiology of kidney disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2014. 4Song YR, et al. Proton-pump inhibitors for prevention of upper gastrointestinal bleeding in patients undergoing dialysis. World J Gastroenterol. 2015 Apr 28;21(16):4919-24.
85-90% of dialysis patients
with an upper GI bleedare hospitalized,compared to
60% in the generalMedicarepopulation1
1in3was readmitted to the hospital
within30DAYS2
Among hemodialysis patients hospitalized
for GI bleeding in 2011,
Gastrointestinal bleeding
Dialysis patients facean increased risk of GI
bleeding, in part becauseof their frequent
exposure to anti-coagulants.
Other risk factors include older age, disability, and cardiovascular disease.
platelet dysfunction for upper GI bleeds
peptic ulcer disease, Helicobacter pylori (H. pylori), and gastritis
Common clinical conditions associated with GI bleeding
for lower GI bleeds angiodysplasia, polyps, ischemic colitis, cancer, inflammatory bowel disease, colonic ulcers, and diverticular disease
The use of proton pump inhibitors has been associated with a lower risk of upper GI bleeding.4(QT interval prolongation risk should be monitored.)
Monthly fliers for the Peer Kidney Care InitiativeResearch, design, layout, writing, graphics
Susan Everson | portfolio | page 13

Corporate rebranding: logo and stationery design
cdrgCHRONIC DISEASE RESEARCH GROUP
Susan Everson | portfolio | page 14
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
set 2 set 3 set 4set 1
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
612.123.4567 | [email protected] | www.cdrg.org
701 park avenue | suite s2.100 | minneapolis mn 55415
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
701 park avenue | suite s2.100minneapolis mn 55415
www.cdrg.org
allan collins, md, facpDIRECTOR
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
cdrgCHRONIC DISEASE RESEARCH GROUP
set 2 set 3 set 4set 1
cdrgCHRONIC DISEASE RESEARCH GROUP
914 south 8th st. | suite s2.100 | minneapolis mn | 55404 | 612.873.6200 | www.cdrg.org
for photoshop
for photoshop

Corporate rebranding: website (www.cdrg.org)Design, content, writing
Susan Everson | portfolio | page 15

A HISTORY OF DIALYSIS
1860 18801870 1890 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010
1861 Thomas Graham coins the word “dialysis,” from the Greek “dia,” meaning through, and “lysis,” to loosen. He also creates the Hoop dialyzer, tying parchment around a hoop floating in water. Into this hoop dialyzer he places solutions of colloids and crystalloids, and demonstrates that only crystalloids pass through the membrane.
1855 German physiologist Adolph Fick uses membranes made from collodion, which allow diffusion of small particles, and proposes the quantitative laws of diffusion.
1854 Scottish chemist Thomas Graham presents a paper entitled “On Osmotic Force,” describing the principles of solute transport across a semipermeable membrane. Having founded the study of colloids, he is widely regarded as the father of colloidal chemistry.
1923 German physician Heinrich Necheles develops a “sandwich” technique to increase the surface area of a dialyzer membrane in relation to blood volume, ultimately increasing dialysis efficiency.
1914 Charles von Hess and Hugh McGuigan, at Northwestern University, improve the efficiency of the vividiffusion apparatus by creating pulsatile flow through the celloidin tubes, thus inhibiting clotting. They also introduce the use of a turbulant flow dialysis fluid around the dialyzing tubes, a principle still used in modern dialysis.
1913 At Johns Hopkins University, John Able, Leonard Rowntree, and BB Turner devise a vividiffusion apparatus they call an “artificial kidney,” which consists of a series of tubes made of celloidin contained in a glass jacket filled with saline or artificial serum. They describe a method “by which the blood of a living animal may be submitted to dialysis outside the body and again returned to the natural circulation.”
1956 Dr. Frank Parsons installs a Kolff-Brigham rotating drum dialysis machine in the Leeds’ General Infirmary, establishing the first artificial kidney unit in the UK. With development help from Willem Kolff, the first pre-sterilized, disposable coil dialyzer is made commercially available by Baxter Laboratories.
1952 During the Korean war, Colonel Paul Techan reports use of the Kolff-Bringham Drum Kidney for treating severely injured troops.
1948 Using stainless steel, researchers at Peter Bent Brigham Hospital in Boston develop the Kolff-Brigham rotating drum kidney. At Mount Sinai Hospital in New York, Drs. Alfred Fishman and Irving Kroop use a a Kolff machine to perform the first human dialysis in the United States.
1947 Swedish physician Nils Alwall develops the first dialyzer with controllable ultrafiltration, creating the first truly practical device for hemodialysis.
1946 At Case Western Reserve University in Ohio, Leonard Skeggs and Jack Leonards develop a large-surface multichannel dialyzer using two sheets of membrane sandwiched between two rubber pads, reducing blood volume and assuring a uniform distribution of blood accross the membrane.
1945 Canadian surgeon Gordon Murray designs a static coil dialyzer, with cellophane tubing wound around a steel frame, and is credited with the first successful use of an artificial kidney machine in North America.
1943–1945 In the Netherlands, Willem Kolff constructs the first modern drum dialyzer. In 1945, a 67 year-old woman in a uremic coma becomes the first patient successfully treated with the Kolff dialyzer.
1962 The first outpatient dialysis unit opens in Seattle.
1960 Norwegian Fredrik Kiil modifies a Skeggs-Leonard dialyzer and develops the Kiil parallel-plate dialyzer, increasing solute clearance efficiency.
1993 The Renal Physicians Association publishes “Clinical Practice Guidelines on Adequacy of Hemodialysis,” defining acceptable methods for measuring hemodialysis adequacy (urea kinetic modeling) and a minimum acceptable level of hemodialysis dose (Kt/V=1.2, or a urea reduction ratio of 65%).
1980s High-efficiency therapies (hemodialysis, hemofiltration, hemo-diafiltration, and high-flux dialysis) are introduced, yielding shortened dialysis times. Ultrafiltration control systems are incorporated into hemodialysis delivery systems allowing precise fluid removal and safe use use of hemodialyzers with high ultrafiltration coefficients.
1985 Drs. Frank Gotch and John Sargent present a mathematical description of urea kinetics (Kt/V), establishing the measurement as an important marker of clinical outcomes.
1981 The National Cooperative Dialysis Study (NCDS) establishes that average urea concentration and protein catabolic rate (PCR) are important factors in determining morbidity and mortality in hemodialysis patients, and that a higher dialysis dose results in reduced morbidity.
1964 Richard Stewart and colleagues at Dow Chemical Company develop the first capillary dialyzer, with hollow fiber membranes made from deacetylated cellulose di-acetate.
1896 Mathieu Jaboulay and Eugene Briau (Lyon, France) and John Murphy (Chicago) use experimental techniques for repair or anastomosis of blood vessels, laying the foundation for dialysis vascular access.
1902 French surgeon and biologist Alexis Carrel publishes on the three-point end-to-end and side-to-side blood vessel anastomosis techniques.
1916 Working under WH Howell at Johns Hopkins University, medical student Jay McLean isolates heparin from canine liver cells. Howell coins the term “heparin” two years later.
1935 The first human trials of heparin begin in May, 1935. By 1937 it is clear that heparin is a safe, easily-available, and effective blood anticoagulant.
1947 At Michael Reese Hospital in Chicago, MR Malinow and W Korzon pioneer methods of fluid removal from the blood of uremic animals using negative pressure.
1949 Swedish physician Nils Allwall conducts experiments on vascular access using rubber tubing and a glass cannula device to connect an artery and vein, but results are unsuccessful.
1960 In Seattle, Belding Scribner, Wayne Quinton, and David Dillard advance the arteriovenous shunt, using silastic tubes fitted with Teflon tips. This shunt provides continuous circulation of the blood when the patient is not attached to the machine, effectively eliminating clotting, providing ready access for repeated long-term hemodialysis, and opening the door to chronic renal replacement therapy.
1961 In London, Stanley Shaldon introduces the temporary femoral vein catheter for use in acute and chronic dialysis.
1966 Brescia, Cimino, Appel, and Hurwich describe a native arteriovenous fistula for chronic vascular access, generally created by an end-to-side vein-to-artery anastomosis. A mature native AV fistula is by far the safest and longest lasting vascular access for hemodialysis.
1973 T Buselmeier and colleagues introduce a new subcutaneous shunt.
Hemodialysis
Peritoneal dialysis
Related developments
Milestones in dialysis policy1972 Congress passes the Social Security Amendments of 1972, authorizing Medicare coverage of the End-Stage Renal Disease (ESRD) program in patients younger than 65. 1973 The ESRD program launches on July 1. 1978 Congress authorizes creation of the ESRD networks. 1981 The Omnibus Budget Reconciliation Act (OMBA) includes a Medicare Secondary Payor provision. 1983 The composite rate payment system for dialysis be-comes effective; cyclosporine is introduced. 1988 The United States Renal Data System is established. 1989 Erythropoietin (EPO) receives FDA approval. 1990 The United States Department of Health & Human Services develops the Healthy People 2000 initiative. 1995 The National Kidney Foundation (NKF) launches the Dialy-sis Outcomes Quality Initiative (KDOQI). 1997 The NKF publishes KDOQI guidelines; the Health Care Financing Administration (HCFA) begins the Hematocrit Measure-ment Audit program. 2001 The National Institutes of Health begin the National Kidney Disease Education Pro-gram (NKDEP). 2004 The Center for Medicare and Med-icaid Services (CMS) launches the Fistula First initiative, aimed at increasing the use of arteriovenous fistulas in hemodialysis patients. 2006 CMS adopts 26 new Clinical Performance Measures to monitor the quality of care re-ceived by ESRD patients. 2011 The new bundled Prospec-tive Payment System for dialysis patients is implemented.
Dialyzer typesCoil dialyzer The first single use hemodialyzer. Early designs used a tubular mem-brane supported by a fibrous mesh wound around a central core. Use of the coil dialyzer gradually declined as more efficient hemodialyzer designs evolved. Single uSe flat Plate dialyzer Dialyzers of this type consist of membrane sheets sup-ported on either side by rigid plastic plates. During the early 1960s, these types of dialyzers (Kiil) were considered non-disposable, with only the membrane and blood ports requiring replacement. The Gambro-Alwall diayzer was the first commerically produced device of this type exhibiting a greatly reduced physical size. Hollow fiber dialyzer Present designs of the hollow fiber hemodialyzer can be traced back to experimental designs in the early 1960s from the Cordis Dow Chemical Company, consisting of regenerated cellulosic hollow fibers. Until 1975, these were the only commercially available fibers for use in hemodialyzers. Since 1975, more refined hol-low fiber dialyzers using modified cellulosic and synthetic membranes have become available. HigH flux dialyzer Dialyzers of this type are the newest generation of the hollow fiber dialyzers, constructed of synthetic membranes that offer larger pore sizes for increased middle molecule clearance and higher ultrafiltration coef-ficients, and said to be more biocompatible than their low-flux counterparts.
1744–1745 Christopher Warrick and the Reverend Stephan Hales introduce peritoneal lavage for the treatment of severe ascites. 1877 German investigator G Wegner reports on animal experiments involving the perfusion of the abdominal cavity with cold saline, and determines the absorption rates of various solutions from the peri-toneum. 1894 English physiologist EH Starling and cohorts confirm the work of Wegner and describe the fluid removal characteristics of the peritoneum. 1923 Georg Ganter performs the first clinical application of peritoneal dialysis. 1930s Peritoneal dialysis remains relatively unknown as a treatment for uremia, with clinicians lacking knowlege about its efficiency and procedural issues such as optimal flows and perfusion fluid concentrations. 1946 Boston physicians Howard Frank, Arnold Seligman, and Jacob Fine report a successful application of peritoneal irrigation on a patient with severe uremia. 1959 Intermittent peritoneal dialysis gradually be-comes a safe and standardized technique thanks to the pioneering work of groups headed by PD Doolan and MH Maxwell. 1959 The first case of chronic, irreversible renal failure is successfully treated with intermittent peritoneal dialysis (IPD). 1962 ST Boen and colleagues introduce the automatic cycling machine, making periodic peritoneal dialysis far more dependable. 1964–1966 Semiautomatic peritoneal dialysis cycler machines are used to treat patients. Boen publishes the first textbook on PD for use in clinical medicine. 1965 Recirculation peritoneal dialysis is introduced. 1968 The Tenckhoff in-dwelling catheter, which allows long-term access to the abdominal cavity, is introduced. 1972 Closed loop, reverse osmosis automatic peritoneal dialysis machines are introduced. 1976 J Moncrief and R Popovich propose the kinetics of continuous ambulatory peritoneal dialysis (CAPD). 1978 Reciprocating, fresh fluid semicontinuous PD is introduced, aimed at improving peritoneal clearance. 1981 JA Diaz Buxo and FF Adams introduce continuous cyclic peritoneal dialysis (CCPD).
blood
dialysate
drum dialyzer static coil dialyzer parallel plate dialyzer
hollow fiber dialyzer
Scottish chemist Thomas Graham presents a paper “On Osmotic Force,” describing the principles of solute transport across a semipermeable membrane. Having founded the study of colloids, he is widely regarded as the father of colloidal chemistry.
Belding Scribner, Wayne Quinton, and David Dillard advance the arteriovenous shunt, using silastic tubes fitted with Teflon tips. This shunt provides continuous circulation of the blood when the patient is not attached to the machine, effectively eliminating clotting, providing ready access for repeated long-term hemodialysis, and opening the door to chronic renal replacement therapy.
The first outpatient dialysis unit opens in Seattle, brought to fruition by Belding Scribner and James Haviland, President of the King County Medical Society. The Seattle Artificial Kidney Center later becomes the Northwest Kidney Centers.
Michael Brescia, James Cimino, and Keith Appel first describe their native arteriovenous fistula for chronic vascular access, generally created by an end-to-side vein-to-artery anastomosis. A mature native A-V fistula is by far the safest and longest lasting vascular access for hemodialysis.
Mathieu Jaboulay and Eugene Briau (Lyon, France) and John Murphy (Chicago) use experimental techniques for repair or anastomosis of blood vessels, laying the foundation for dialysis vascualr access.
Stanley Shaldon introduces the femoral vein catheter for use in acute and chronic dialysis followed by the Uldall subclavian catheter and single and double lumen jugular vein catheters.
Alexis Carrel publishes the three-point end-to-end- and side-to-side anastomosis techniques, a milestone and still used today.
The Buselmeier Shunt is intro-duced, and becomes the pre-ferred access for pediatric dial-ysis.
Nils Allwall conducts experiments on vascular access using rubber tub-ing and a glass cannula device to connect an artery and vein, but results are un-successful.
During the Korean war, Colonel Paul Techan reports use of the Kolff-Bringham Drum Kidney for treating severely injured troops.
Dr. Frank Parsons installs a Kolff-Brigham rotating drum dialysis machine in the Leeds’ General Infirmary establishing the first artificial kidney unit in the UK.
With development help from Willem Kolff, the first pre-sterilized, disposable coil dialyzer is made commercially available by Baxter Laboratories, followed by the introduction of the
“Twin Coil System.”
Norwegian Fredrik Kiil modifies a Skeggs-Leonard dialyzer and develops the Kiil parallel-plate dialyzer. This uses fewer “stacked” blood compartments but has a larger surface area, thus increasing its efficiency for solute clearance. The Kiil dialyzer can be broken down and reassembled, and does not require the use of a blood pump.
Richard Stewart and colleagues at Dow Chemical Company develop the first capillary dialyzer, with hollow fiber membranes made from deacetylated cellulose di-acetate. During the next three years, Dow develops the manufacturing technology to mass produce the hollow fiber dialyzer.
In Minneapolis, Minnesota, the Regional Kidney Disease Program is established by Dr Fred L. Shapiro.
Milestones in dialysis policy1972 Congress passes the Social Security Amendments of 1972, authorizing Medicare coverage of the End-Stage Renal Disease (ESRD) program in patients younger than 65. 1973 The ESRD program launches on July 1. 1978 Congress authorizes creation of the ESRD networks. 1981 The Omnibus Budget Reconciliation Act (OMBA) includes a Medicare Secondary Payor provision. 1983 The composite rate payment system for dialysis becomes effective; cyclosporine is introduced. 1988 The United States Renal Data System is established. 1989 Erythropoietin
(EPO) receives FDA approval. 1990 The United States Department of Health & Human Services develops the Healthy People 2000 initiative. 1995 The National Kidney Foundation (NKF) launches the Dialysis Outcomes
Quality Initiative (KDOQI). 1997 The NKF publishes KDOQI guidelines; the Health Care Financing Administration (HCFA) begins the Hematocrit Measurement Audit program. 2001 The National Institutes of Health begin the National Kidney Disease Education Program (NKDEP). 2004 The Center for Medicare and Medicaid Services (CMS) launches the
Fistula First initiative, aimed at increasing the use of arteriovenous fistulas in hemodialysis patients. 2006 CMS adopts 26 new Clinical Performance Measures to monitor the quality of care received by ESRD patients. 2011 The new bundled Prospective Payment System for dialysis patients is implemented.
Dialyzer typesCOIL DIALYZER The first single use hemodialyzer construct-
ed. Early designs used a tubular membrane supported by a fibrous mesh wound around a central core. The early coils had
serious performance limitations that were gradually overcome through refinements in the design. Use of the coil dialyzer grad-
ually declined, however, as more efficient hemodialyzer designs evolved.
SINGLE USE FLAT PLATE DIALYZER Dialyzers of this type consist of membrane sheets cupported on either side by rigid plastic plates.
During the early 1960s, these types of dialyzers (Kiil) were considered non-disposable with only the membrane and blood ports requiring
replacement. The Gambro-Alwall diayzer was the first commerically produced device of this type exhibiting a greatly reduced physical size.-
Use of these types of devices diminished following the introduction of the hollow fiber dialyzer.
HOLLOW FIBER DIALYZER Present designs of the hollow fiber hemodia-lyzer can be traced back to experimental designs in the early 1960s from the
Cordis Dow Chemical Company, consisting of regenerated cellulosic hollow fibers. Until 1975, these were the only commercially available fibers for use in
hemodialyzers. Since 1975, more refined hollow fiber dialyzers using modified cellulosic and synthetic membranes have become available.
HIGH FLUX DIALYZER Dialyzers of this type are the newest generation of the hollow fiber dialyzers and are constructed of synthetic type membranes that offer
larger pore sizes for increased middle molecule clearance and higher ultrafiltration coefficients. These types of dialyzers are said to be more biocompatible than their
l0w-flux counterparts.
Heinrich Necheles develops a “sandwich” technique to increase a dialyzer membrane’s surface area in relation to blood volume, ultimately increasing dialysis efficiency.
German physiologist Adolph Fick uses membranes made from collodion, which allow diffusion of smaller particles and proposes the quantitative laws of diffusion.
Thomas Graham coins the word “dialysis”—from the Greek “dia,” meaning through, and “lysis,” to loosen. He also creates the Hoop dialyzer, by tying parchment around a hoop floating in water. Into this hoop dialyzer he places solutions of colloids and crystalloids, and demonstrates that only crystalloids pass through the membrane.
John Able, Leonard Rowntree, and BB Turner devise a vividiffusion apparatus named the “artificial kidney” consisting of a series of tubes made of celloiden contained in a glass jacket filled with saline or artificial serum. They describe a method “by which the blood of a living animal may be submitted to dialysis outside the body and again returned to the natural circulation.”
CL von Hess and H McGuigan improve the efficiency of the vividiffusion apparatus by creating pulsatile flow through the celloiden tubes, thus inhibiting clotting. They also introduce the use of a turbulant flow dialysis fluid around the dialyzing tubes, a principle still used in modern dialysis.
Working under WH Howell at Johns Hopkins University, medical student Jay McLean isolates heparin from canine liver cells. Howell coins the term “heparin” two years later.
Swedish professor Nils Alwall develops the first dialyzer with controllable ultrafiltration, creating the first truly practical device for hemodialysis.
Using stainless steel, researchers at Peter Bent Brigham Hospital in Boston develop the Kolff-Brigham rotating drum kidney, furthering Kolff’s original machine. Between 1954 and 1962, machines were shipped to more than 20 hospitals around the world.
At Mount Sinai Hospital in New York, and using a Kolff machine, Drs. Alfred Fishman and Irving Kroop perform the first human dialysis in the United States.
At Case Western Reserve University in Ohio, Leonard Skeggs and Jack Leonards begin development of a large surface multichannel dialyzer using two sheets of membrane sandwiched between two rubber pads which reduced reduced blood volume and assured a uniform distribution of blood accross the membrane.
At Michael Reese Hos-pital in Chicago, Ma-linow and Korson pio-neer methods of fluid removal from the blood of uremic animals using negative pressure.
Gordon Murray designs a static coil dialyzer which consists of cellophane tubing wound around a steel frame, and is credited with the first successful use of an artificial kidney machine in North America.
The first human trials of heparin begins in May, 1935. By 1937 it is clear that heparin is a safe, easily-available, and effective blood anticoagulant.
1854
1960
1962
1966
1896
196419
02
1973
1949
1952
1956
1960
1964
1968
1923
1855
1861
1913
1914
1916
1943
–194
519
4719
48
1946
1947
1945
1935
In the Netherlands, Willem Kolff constructs the first modern drum dialyzer, which remains the standard for the next decade. In 1945, a 67 year-old woman in a uremic coma becomes the first patient successfully treated with the Kolff dialyzer.
A History of Dialysis
HEMODIALYSIS
PERITONEAL DIALYSIS
TITLE...
1744–1745 Christopher Warrick and the Reverend Stephan Hales introduce peritoneal lavage for the treatment of severe ascites.
1877 German investigator G Wegner reports on animal experiments involving the perfusion of the abdominal cavity with cold saline and determines the absorption rates of various solutions from the peritoneum.
1959 Intermittent peritoneal dialysis gradually becomes a safe and standardized technique thanks to the pioneering work of groups headed by PD Doolan and MH Maxwell.
1959 The first case of chronic, irreversible renal failure is successfully treated with intermittent peritoneal dialysis.
1962 ST Boen and colleagues introduce the automatic cycling machine, making periodic peritoneal dialysis far more dependable.
1964–1966 Semiautomatic peritoneal dialysis cycler machines are used to treat patients.
1965 Recirculation peritoneal dialysis is introduced.
1972 Closed loop, reverse osmosis automatic peritoneal dialysis machines are introduced.
1978 Reciprocating, fresh fluid semicontinuous PD is introduced, aimed at improving peritoneal clearance.
J Moncrief and R Popovich publish articles on continuous ambulatory peritoneal dialysis (CAPD).1981 JA Diaz Buxo and FF Adams introduce continuous cyclic peritoneal dialysis (CCPD).
1968 The Tenckhoff in-dwelling catheter, which allows longterm access to the abdominal cavity, is introduced.
1894 English physiologist EH Starling and cohorts confirm the work of Wegner and describe the fluid removal characteristics of the peritoneum.
1923 Georg Ganter performs the first clinical application of peritoneal dialysis.
1930s Peritoneal dialysis remains relatively unknown as a treatment for uremia, with clinicians lacking knowlege about its efficiency and procedural issues such as optimal flows and perfusion fluid concentrations.
1946 Boston physicians Howard Frank, Arnold Seligman, and Jacob Fine report a successful application of peritoneal irrigation on a patient with severe uremia.
blood
dialysate
1860
1860
1880
1880
1870
1870
1890
1890
1900
1900
1910
1910
1920
1920
1930
1930
1940
1940
1950
1950
1960
1960
1970
1970
1980
1980
1990
1990
2000
2000
2010
2010Timeline of the history of dialysis Research, writing, design, layout (one version for inclusion in printed report, one for framing)
Susan Everson | portfolio | page 16

USRDS Coordinating Center Technical Proposal
NIH-NIDDK-06-01
USRDS Investigative Team
We shall not cease from explorationAnd the end of all our exploringWill be to arrive where we startedAnd know the place for the first time
Thomas Stearns Eliot, “Four Quartets”
I find the great thing in this world is not so much where we stand, as in what direction we are moving: To reach the port of heaven, we must sail sometimes with the wind and sometimes against it — but we must sail, and not drift, nor lie at anchor.
John Galsworthy, “Erranty”
Our compass points to the improved care of patients living with kidney disease. We strive to capture the wind, & with full sail set forth toward the port we seek.
With this in mind, we offer our proposal to continue our work as the Coordinating Center of the United States Renal Data System.
USRDS Coordinating Center Technical Proposal
NIH-NIDDK-06-01
USRDS Investigative Team
Minneapolis MedicalResearch Foundation
Proposal for the Coordinating Centerof the United States Renal Data System (USRDS),RFP Number NIH-NIDDK-06-01
Technical Proposal
USRDS Coordinating Center Technical Proposal
NIH-NIDDK-06-01
USRDS Investigative Team
Fulfilling the objectives of the USRDS 1 Executive summary 1 Introduction to the objectives of the USRDS 2 Objective A: Characterize the ESRD patient population 3 Objective B: Describe the prevalence & incidence rates
of kidney diseases that lead to ESRD 3 Objective C: Investigate the relationships among modalities, diseases,
& patient groups 4 Objective D: Support investigator-initiated research 4 Two-hour requests 5 Greater than two-hour requests 5 Merged data requests 5 Investigator-initiated research files 5 Objective E: Provide datasets to support special studies research by the SSCs 6 Objective F: Identify problems & opportunities for focused investigation 7 Objective G: Design & implement data studies & special data collection studies
to help improve ESRD patient health 8 Objective H: Conduct cost-effectiveness & other economic studies of ESRD 8 Accomplishments of the current Coordinating Center
Qualifications of the proposed Coordinating Center 10 Introduction 10 Relationship of the investigators 11 Experience of the current USRDS analytical team 11 Proposed USRDS Principal Investigator/Project Director 12 Biostatistical investigators 13 Investigators at HCMC & at the University of Minnesota
(Departments of Internal Medicine & Pediatrics, & the School of Public Health) 13 HCMC data management team 14 Conclusion 15 Figure 1: Affiliation agreement, investigational teams, institutional relationship
USRDS Coordinating Center Technical Proposal
Use or disclosure of data contained on this page is subject to the restriction on the cover sheet of this proposal.
NIH-NIDDK-06-01 Ful� lling the objectives of the USRDS
USRDS Investigative Team 1
Ful� lling the objectivesof the USRDS
■ Executive summary
The United States Renal Data System constitutes the most comprehensive database of end-stage renal disease—and now of chronic kidney disease as well—in the world, serving a major public health role by documenting patients with these diseases and advancing their treatment. Under NIH direction, the USRDS has produced major studies addressing changes in disease rates, defining pre-ESRD care, developing methods to define the recognized CKD population, assessing prescription drug therapy, determining the frequency and quality of preventive care and risk factor monitoring, defining care by large ESRD providers, and assessing outcomes.
In the last seven years, under the direction of investigators from the Minneapolis Medical Research Foundation (MMRF), the USRDS has implemented substantial changes in the registry’s focus, addressing Healthy People 2010 objectives while also de� ning the potential growth of the renal program and its implication for the U.S. healthcare system. In the 2005 Annual Data Report (ADR), for instance, the Coordinating Center (CC) demonstrated the multiplying e� ects of kidney disease, illustrating how its interaction with diabetes and cardio-vascular disease impacts the healthcare budget in the U.S. and around the world. � e CC has also played a central role in working with the Special Studies Centers (SSCs), addressing � eld operations for data collections, providing database and technical support, and de� ning the strengths and weaknesses in past and future plans for such studies.
Our proposal to continue serving as the CC advances the high standards set by the previ-ous contractor and by ourselves. We describe advanced disease rate mapping to depict varia-tions in care, enhanced data access, major new initiatives in preventive care, documentation of the recognized CKD population, an expanded Internet website with dynamic and real-time data access, and our extensive attention to data quality and consistency, and provide a criti-cal assessment of analytical methods. And we present an outstanding group of investigators. We propose new approaches to expand and disseminate USRDS information from the ADR, journal publications, presentations, and government-requested information, using enhanced web applications. Our administrative approach will continue to expand documentation of the operational elements of the USRDS and enhance the open access to USRDS activities, meth-ods, and systems under the direction of the NIH, the oversight committees, and the ESRD community.
■ Introduction to the objectives
of the USRDS
The original five goals of the USRDS have this year been expanded to eight, broadly defining the major functions of the registry. In its first ten years, the USRDS focused on descriptive characteristics of the ESRD population and on comparative event rates. In the last seven years,
USRDS Coordinating Center Technical Proposal
Use or disclosure of data contained on this page is subject to the restriction on the cover sheet of this proposal.
NIH-NIDDK-06-01 Ful� lling the objectives of the USRDS
USRDS Investigative Team 2
our investigative team has broadened the scope of the USRDS to address clinical care, improve access to data, expand disease mapping of variations in care and events, develop the pre-ESRD and CKD databases, and advance the administrative operations. Our proposal illustrates our commitment to expand and further this work, including, for example, investigations into dis-parities in care within the kidney disease population.
■ Objective A Characterize the
ESRD patient population
In our work as the CC of the USRDS we have addressed this goal in great detail, paying increased attention to the major causes of ESRD and to trends in disease rates by age, gender, and race. We have also introduced geo-mapping of the data, further developing advanced statistical methods to illustrate geographic differences in disease rates and patterns of care. Additional information on the level of counties and Metropolitan Statistical Areas (MSAs) is needed to provide detail on high concentrations of disease.
� e declining incident rates of ESRD seen in most populations, for example, are not present in younger African Americans. � is trend may be more pronounced in certain geographic areas, and merits investigation, as does the care these populations receive. To address these issues, we propose to use the extensive geomapping techniques developed by the CC to more closely examine regions with a high frequency of disease, such as the southern states and inner cit-ies on the East Coast. � e increasing burden of diabetes in the general population is a related concern, particularly since it disproportionally a� ects a number of racial and ethnic groups. A more detailed investigation is needed of the growth in diabetes overall and as it relates to ESRD incident rates and access to care.
� e new CMS 2728 form (the Medical Evidence form for ESRD enrollment), which was revised in 2004 and implemented the following spring, added data � elds on patient access to care. � e form now collects information on pre-ESRD care by a nephrologist and kidney dietician, on treatment with exogenous erythropoietin, and on the type of � rst outpatient vascular access. Each of these elements further illustrates the care given in the pre-ESRD period, and may pro-vide insight into racial disparities in incident rates. � e details we have outlined under Task Two identify ways to consolidate these data and enhance these comparisons.
In our proposal we also describe new epidemiologic cohorts which will characterize the disease burden in incident and prevalent patients. � ese cohort descriptions will provide expanded information on comorbidity and complications, and will be used to study pre-existing con-ditions associated with future outcomes. We propose to address the care, comorbidity, and access to care among working adults in employer group health plan (EGHP) populations as well as in elderly Medicare patients, working to determine the di� erences which may in� uence early mortality and morbidity.
Recent years have seen a dramatic consolidation in dialysis providers, with two large chains now treating more than 60 percent of the dialysis population. Smaller provider groups con-tinue to consolidate as well, reducing the number of independent providers. Hospital-based operations still treat approximately one in � ve dialysis patients, yet use widely diverse prac-tices. � ese changes in the provider community need to be addressed on a geographic basis to determine how consolidation may have a� ected care. Some data, for instance, suggest that large dialysis organizations treat fewer patients with home dialysis than do hospital-based operations. To illustrate access to alternative dialysis therapies, and to evaluations for the transplant wait-list and for transplantation itself, these � ndings need to be explored.
We also address the expanded demand for data, particularly on disparities in access to care, through enhancements to RenDER, our web-based on-line data query system. � e basic sys-tem currently addresses incidence, prevalence, and mortality. To help enhance public health oversight of the care system, we will further develop the system’s provision of geomapped data, allowing users to drill down to various cities and MSAs.
USRDS Coordinating Center Technical Proposal
Use or disclosure of data contained on this page is subject to the restriction on the cover sheet of this proposal.
NIH-NIDDK-06-01 Ful� lling the objectives of the USRDS
USRDS Investigative Team 3
■ Objective B Describe the
prevalence & incidence rates
of kidney diseases that lead to ESRD
In the Annual Data Report (ADR) the CC has developed special sections addressing diseases beyond diabetes and hypertension. These rare conditions include Alport’s disease, polycys-tic kidney disease, Fabry’s disease, multiple myeloma, and other inflammatory diseases. New treatments have been developed for some of these rare diseases, such as the enzyme replace-ment therapy now used to treat Fabry’s. Patient outcomes have received little attention, but should be assessed in depth, and the USRDS database contains the largest amount of data on these cases collected in one place. Immunologic disorders such as systemic lupus erythemato-sus, Wegener’s granulomatosis, and ANCA-positive vasculitis, with their associated complica-tions, are also rare but important diseases to track over time.
Most attention related to ESRD incidence has centered on the concept that kidneys progres-sively lose function over time. Emerging data, however, suggest that many patients su� er epi-sodes of acute kidney failure prior to the start of ESRD treatment. Some data suggest that acute kidney failure in a hospital setting may re� ect undiagnosed CKD manifesting itself dur-ing an acute medical complication. � e recent increase in hospitalizations which list acute kidney failure as a complication or primary cause of stay suggests that this event merits greater attention, with analyses to determine how patients are followed and their potential to progress to ESRD.
It is important to track the comorbidity of patients entering ESRD treatment, as their com-plexity in� uences subsequent survival time under ESRD care. � e CC has created methods to identify this comorbidity, addressing patterns of hospitalizations and associated medical con-ditions in Medicare patients age 65 and older, and evaluating the services they receive in the two years prior to starting ESRD care. � is approach has provided signi� cant information on the older population, but little on those younger than 65. Now that CC’s ESRD database con-tains six years of Medstat data, however, we can also begin to examine data on EGHP patients, who are primarily younger than 65, looking back from the date of ESRD or regular dialysis services to determine the level of comorbidity carried in the past. � ese di� erent approaches should be advanced to assess long-term trends in adjusted ESRD incidence, prevalence, and mortality.
Comorbidity in the prevalent population is a particularly challenging issue, since data are not collected on a sample of ESRD or dialysis patients over time. � e CC has developed methods (incorporating the approach of Hebert et al.) for assessing an individual’s comorbidity using medical claims for services. We have also performed a more comprehensive validation study, which should help address the complexity of the existing population and its outcomes. To assess care and risk factor interventions, however, it would be very helpful to have biochemical data on both the incident and prevalent populations. CMS, with support from the ESRD networks and large dialysis organizations, is considering obtaining monthly biochemical data on the dialysis population to assess the e� ectiveness of medical interventions. � ese data would be very impor-tant, since classic outcome studies—assessing, for example, associations of mortality with the use of intravenous vitamin D—would be enhanced with access to data on calcium, phosphorus, and parathyroid hormone levels. So that the e� ectiveness of risk factor interventions and their associated outcomes may be addressed, these biochemical data need to be made available.
■ Objective C Investigate the
relationships among modalities,
diseases, & patient groups
The USRDS ADR has documented significant changes in the use of ESRD treatment modali-ties. The use of peritoneal dialysis in incident patients, for example, has declined steadily, so that the prevalent peritoneal dialysis population is down to 25,000 from a high of 35,000 just a decade ago. While these changes may reflect new perceptions about the therapy and its long-term complications, little is known about why utilization rates for the major dialytic modali-ties have changed so dramatically.
Considerable attention has recently been paid to daily home or in-center hemodialysis as a method to increase the total delivered therapy, and to thereby improve control of � uid over-load and other complications. Since there is no registration system for the di� erent types of
Grant proposal for the United States Renal Data SystemLayout, typesetting, editing, project management
Susan Everson | portfolio | page 17