Embed Size (px)
Citation preview
Bites and Stings

The most effective treatment to eliminate the lesions seen here:
A Topical steroidsB Oral antibioticsC Treatment of home for
fleasD 5% Permethrin cream to
all household membersE Oral antihistamines
Question 5
Think about distribution (exposure)Bites on face may be atypical
RedPruriticSoft and nontender
Intense, hemorrhagic reaction possibleFleas: some members of household “spared”
Clusters of 3Grass or sand mites: localized blisters
Bites and Stings
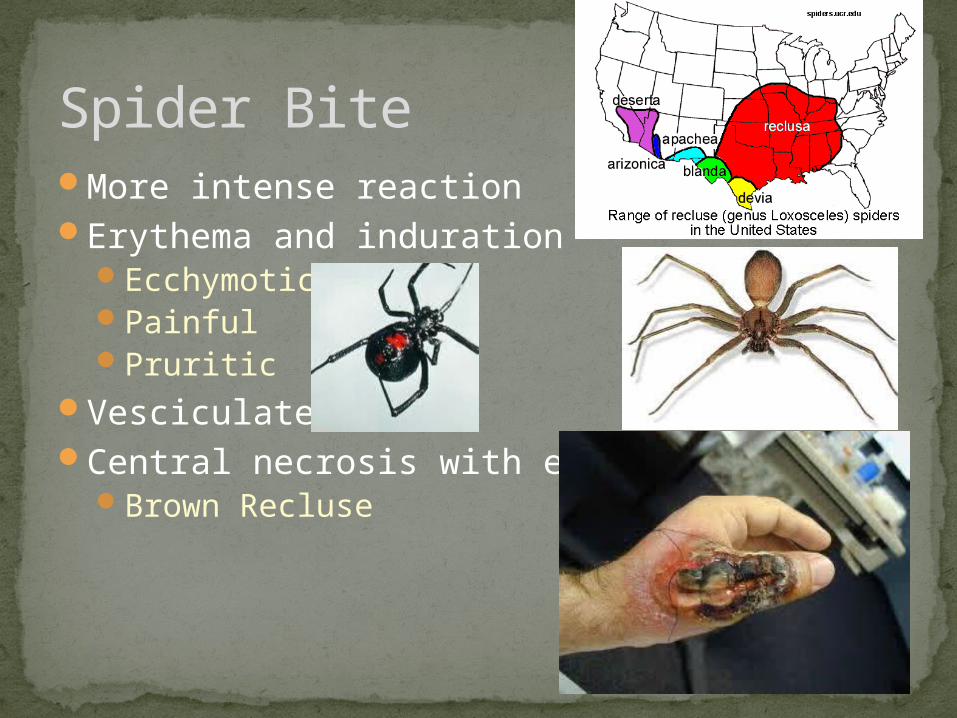
More intense reactionErythema and induration
EcchymoticPainfulPruritic
VesciculateCentral necrosis with eschar
Brown Recluse
Spider Bite
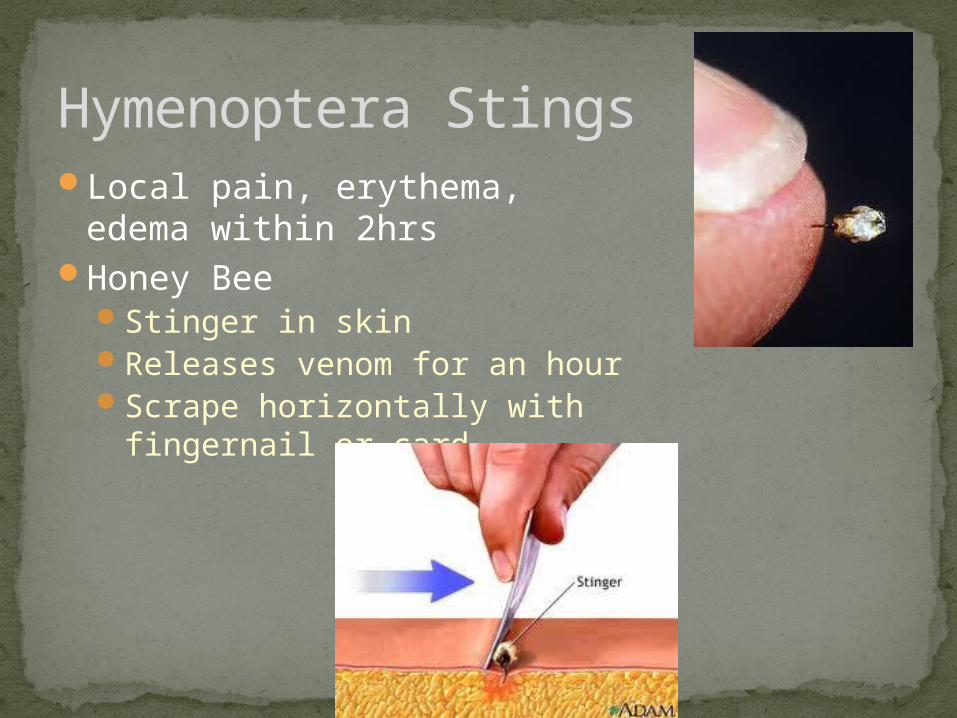
Local pain, erythema, edema within 2hrs
Honey BeeStinger in skinReleases venom for an hourScrape horizontally with
fingernail or card
Hymenoptera Stings
Late onset edemaPeak 48-72hrsDelayed hypersensitivityPruritic, painful
TreatmentPaste of meat tenderizer and
waterSymptomatic treatment
Risk of anaphylaxisKnown historyMastocytosisEducation on avoidanceEpiPen
Hymenoptera Stings
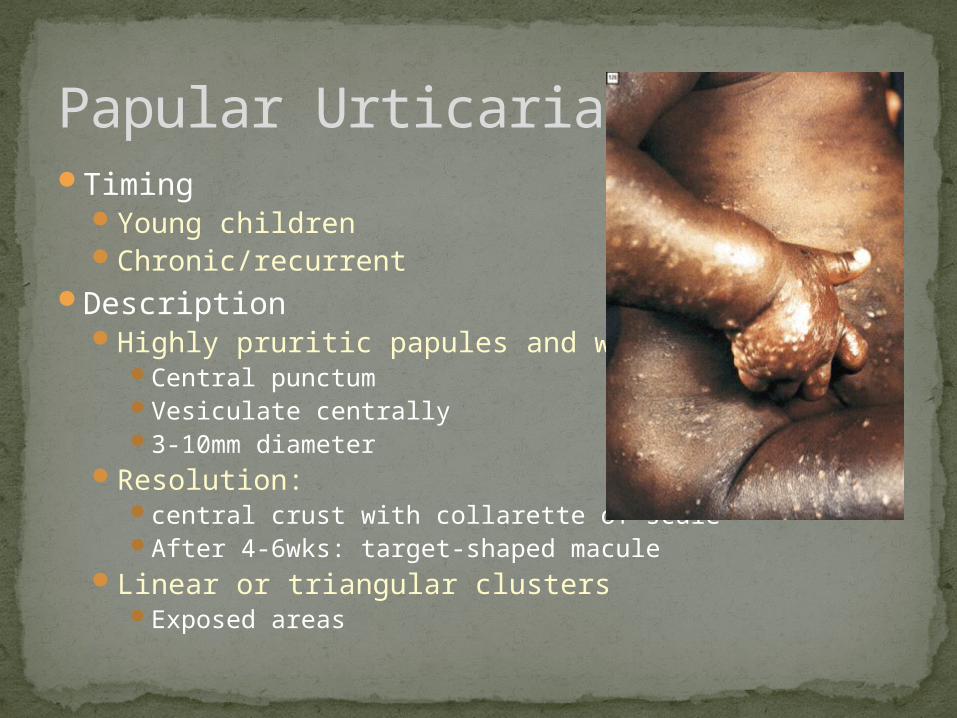
TimingYoung childrenChronic/recurrent
DescriptionHighly pruritic papules and wheals
Central punctumVesiculate centrally3-10mm diameter
Resolution: central crust with collarette of scaleAfter 4-6wks: target-shaped macule
Linear or triangular clustersExposed areas
Papular Urticaria
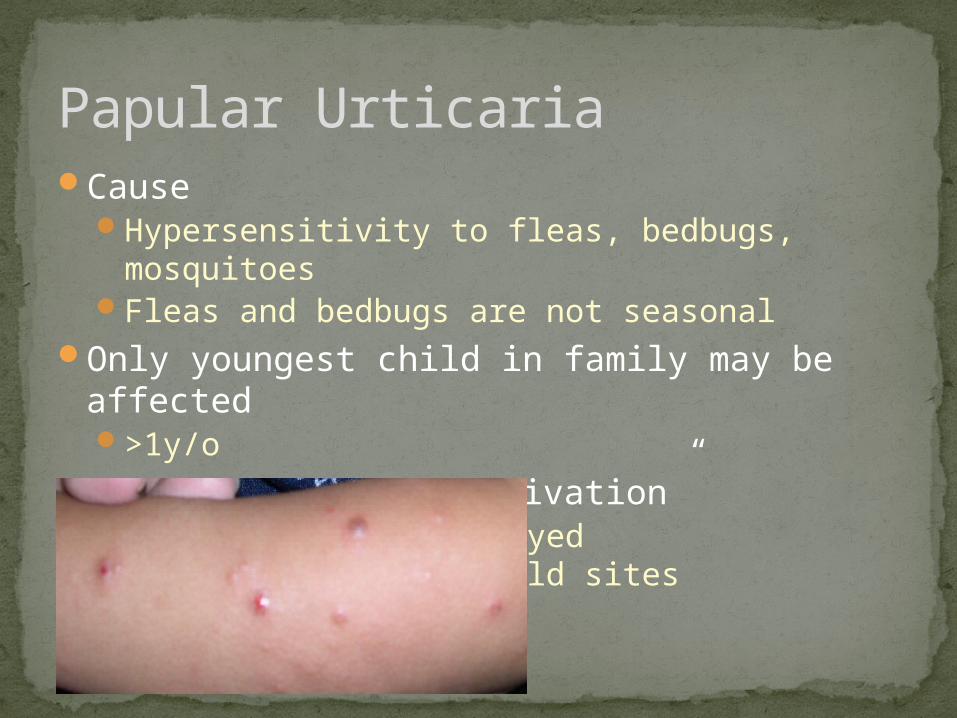
CauseHypersensitivity to fleas, bedbugs, mosquitoesFleas and bedbugs are not seasonal
Only youngest child in family may be affected>1y/o
May experience “reactivation”New bites incite delayed hypersensitivity at old
sites
Papular Urticaria
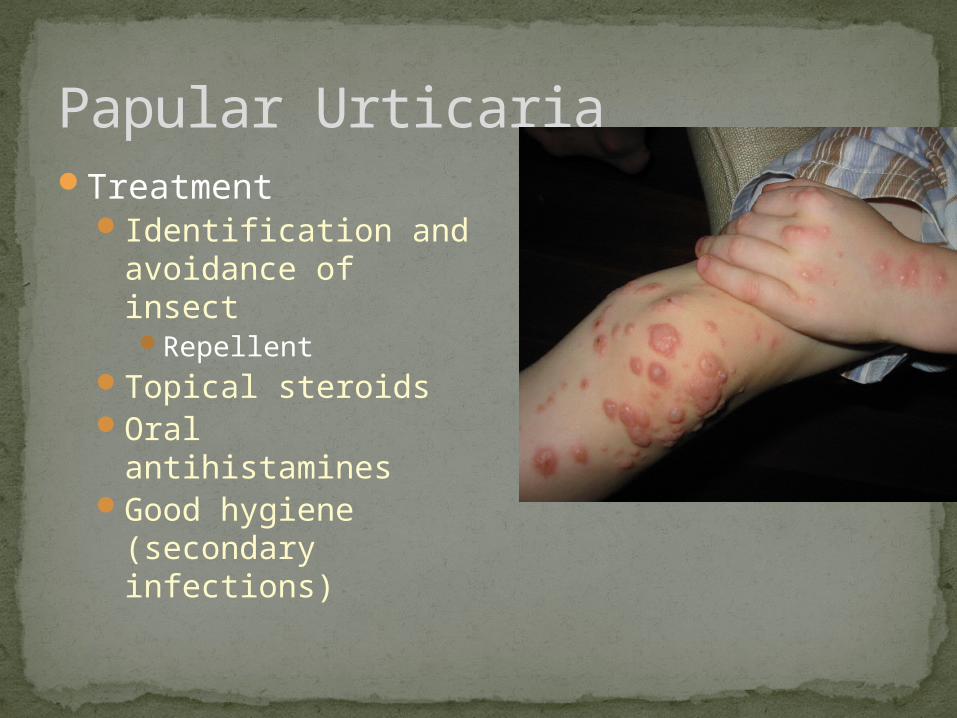
TreatmentIdentification and
avoidance of insectRepellent
Topical steroidsOral antihistaminesGood hygiene
(secondary infections)
Papular Urticaria
Infestations
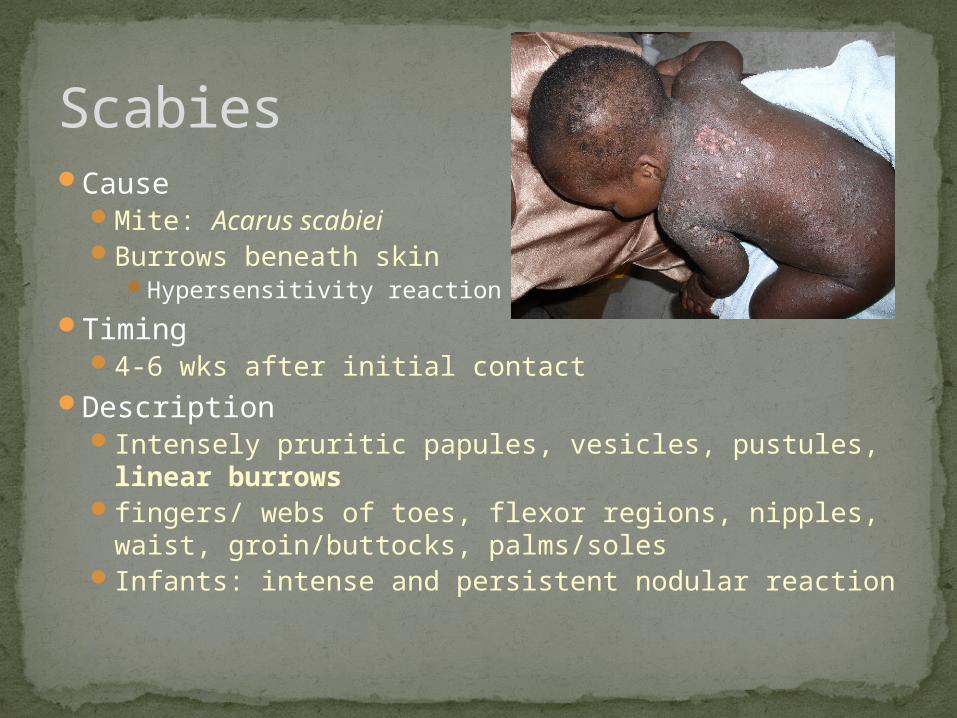
CauseMite: Acarus scabiei Burrows beneath skin
Hypersensitivity reaction
Timing4-6 wks after initial contact
DescriptionIntensely pruritic papules, vesicles, pustules,
linear burrowsfingers/ webs of toes, flexor regions, nipples,
waist, groin/buttocks, palms/solesInfants: intense and persistent nodular reaction
Scabies
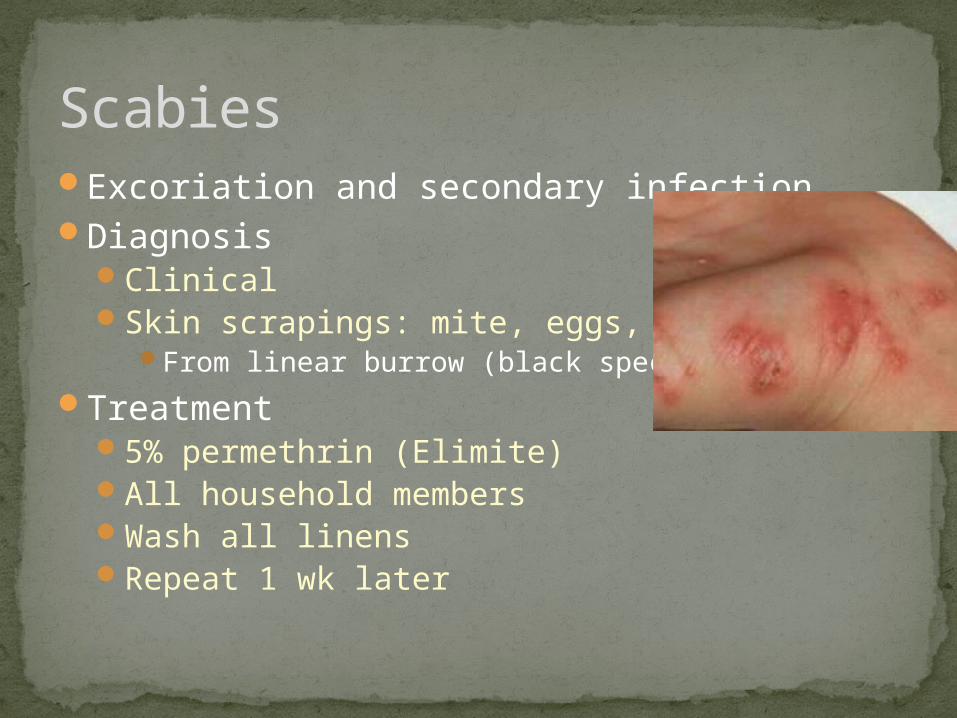
Excoriation and secondary infectionDiagnosis
ClinicalSkin scrapings: mite, eggs, feces
From linear burrow (black speck)
Treatment5% permethrin (Elimite)All household membersWash all linensRepeat 1 wk later
Scabies
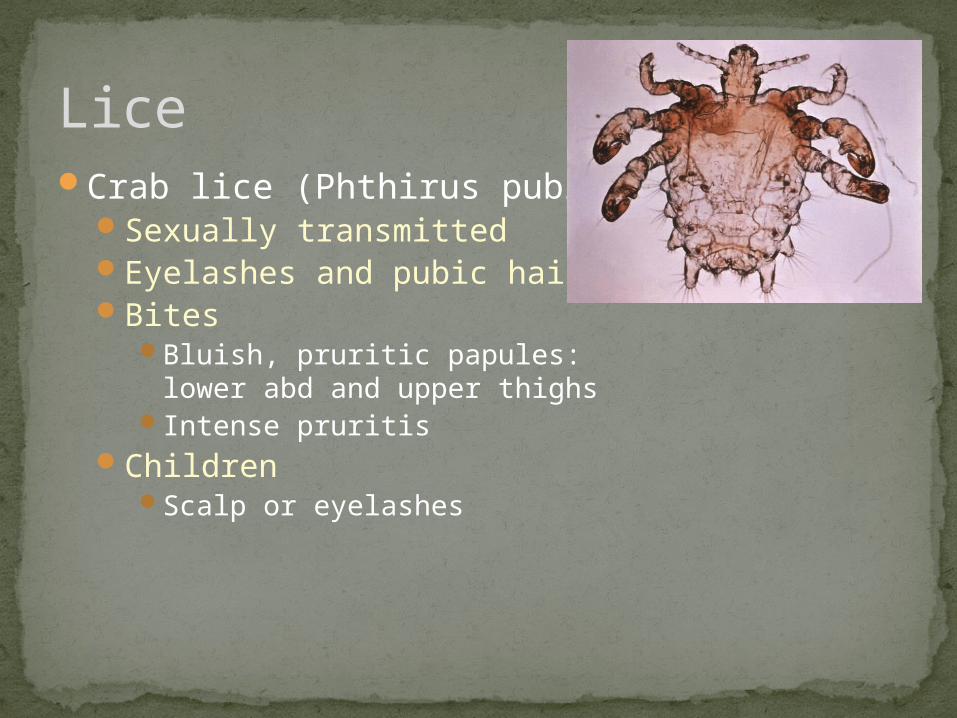
Crab lice (Phthirus pubis)Sexually transmittedEyelashes and pubic hairBites
Bluish, pruritic papules: lower abd and upper thighs
Intense pruritisChildren
Scalp or eyelashes
Lice
Body lice (pediculus humanus corporis)Bedding or clothingBites
Urticarial papulesWaist, neck, shoulders, axillae
Excoriations/ secondary infection
Lice
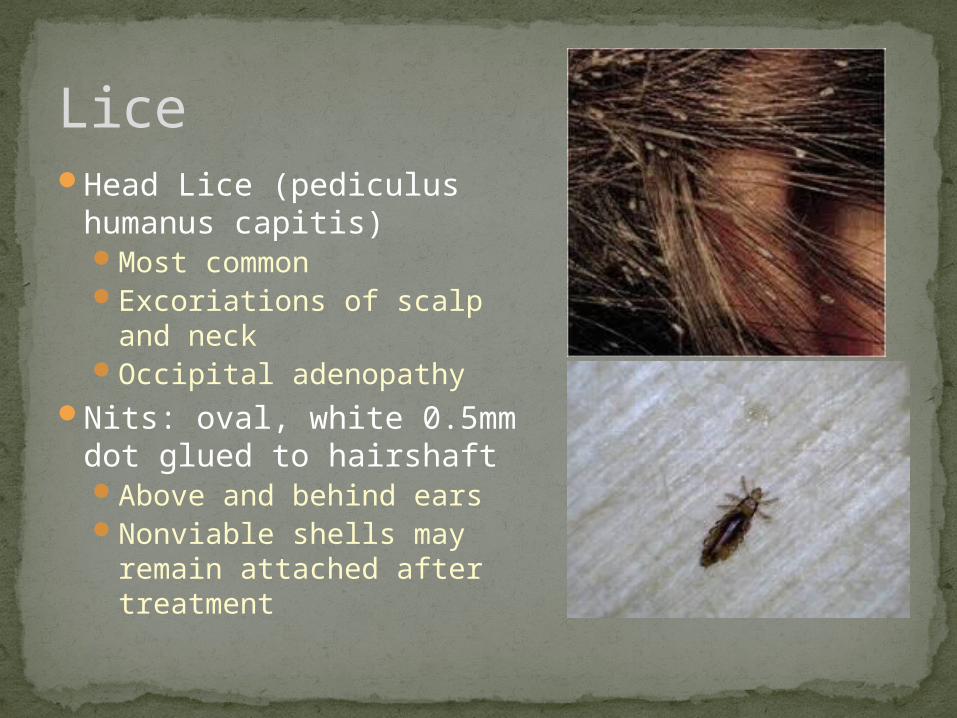
Head Lice (pediculus humanus capitis)Most commonExcoriations of scalp
and neckOccipital adenopathy
Nits: oval, white 0.5mm dot glued to hairshaftAbove and behind earsNonviable shells may
remain attached after treatment
Lice
Treatment:Pediculicide topically (all household members)
Permethrin creamMalathion lotion (second line…flammable)Lindane: contraindicated in young… neurotoxic
Cleaning of linens/clothingNits:Diluted vinegar rinseFine-toothed comb
Lice

Acne vulgarisDisorder of pilosebaceous apparatus
Cause: UnknownAbnormal follicular keratinizationDriven by androgensPropionibacterium acnes
TreatmentTopical retinoic acid, benzoyl peroxide, abxSevere: oral abx with topical agents
Acne
Other Lesions

The most reliable way to distinguish these lesions from other lesions frequently seen on the sole of the foot:
Question 6
A Black dots indicate corns that have received trauma
B Interruption of dermatoglyphics indicate plantar warts
C Superficial scaling indicates callus formationD Boggy texture indicates plantar warts
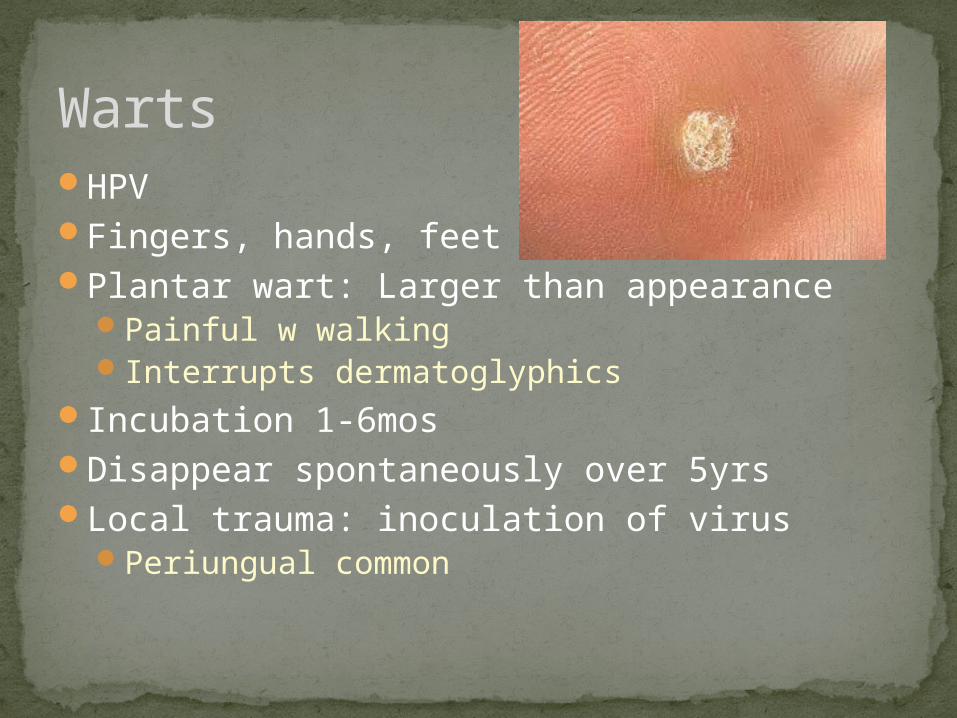
HPVFingers, hands, feetPlantar wart: Larger than appearance
Painful w walkingInterrupts dermatoglyphics
Incubation 1-6mosDisappear spontaneously over 5yrsLocal trauma: inoculation of virus
Periungual common
Warts
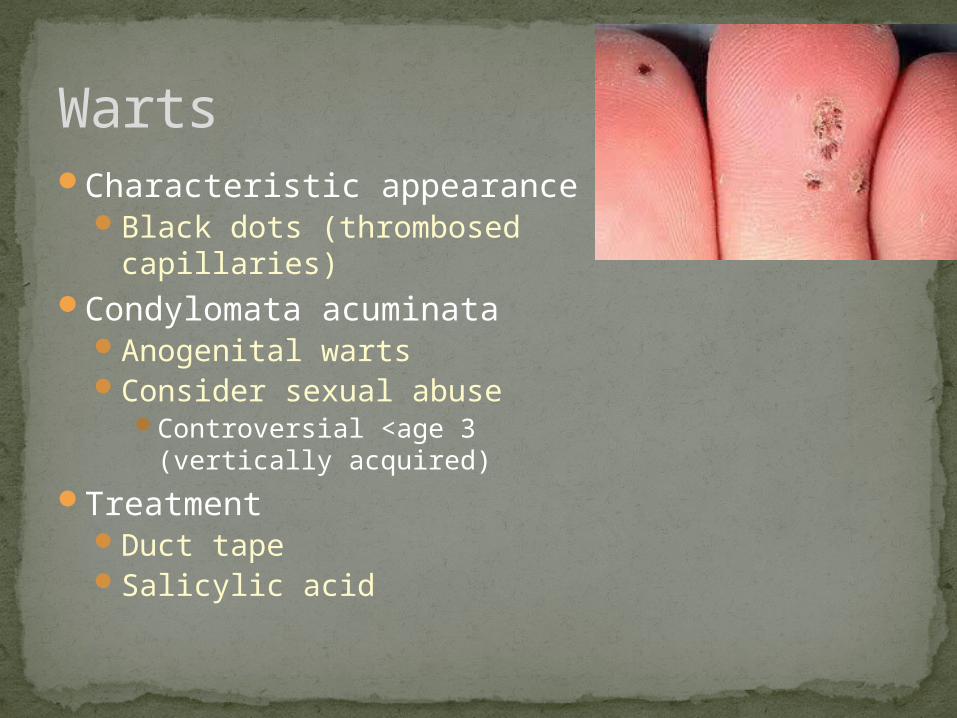
Characteristic appearanceBlack dots (thrombosed
capillaries)Condylomata acuminata
Anogenital wartsConsider sexual abuse
Controversial <age 3 (vertically acquired)
TreatmentDuct tapeSalicylic acid
Warts
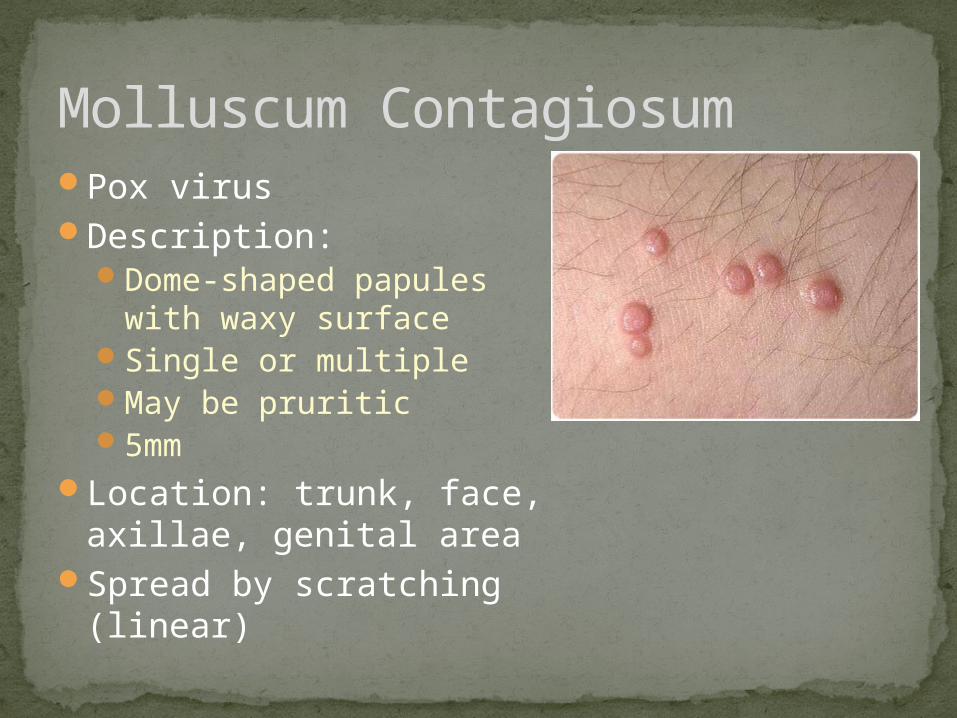
Pox virusDescription:
Dome-shaped papules with waxy surface
Single or multipleMay be pruritic5mm
Location: trunk, face, axillae, genital area
Spread by scratching (linear)
Molluscum Contagiosum
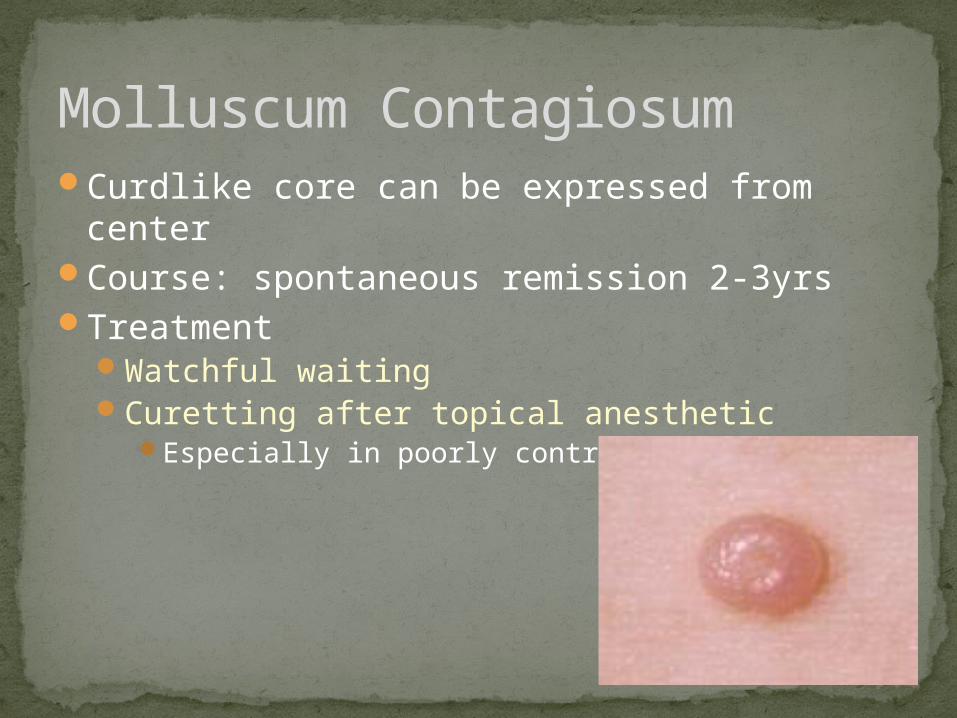
Curdlike core can be expressed from centerCourse: spontaneous remission 2-3yrsTreatment
Watchful waitingCuretting after topical anesthetic
Especially in poorly controlled eczema
Molluscum Contagiosum
Congenital Lesions
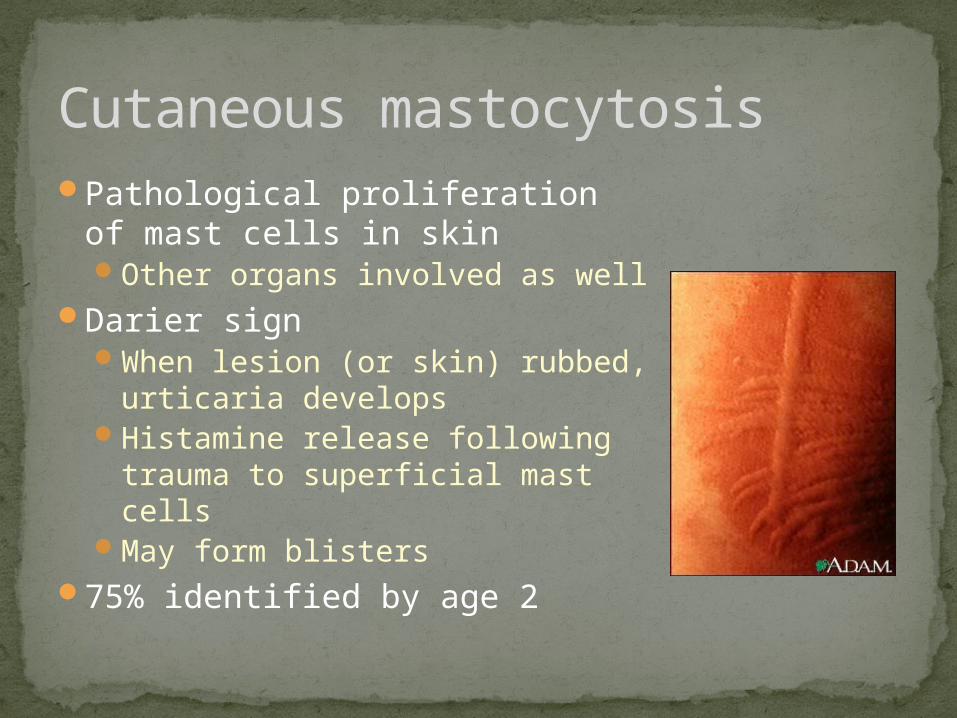
Pathological proliferation of mast cells in skinOther organs involved as well
Darier signWhen lesion (or skin) rubbed,
urticaria developsHistamine release following
trauma to superficial mast cellsMay form blisters
75% identified by age 2
Cutaneous mastocytosis
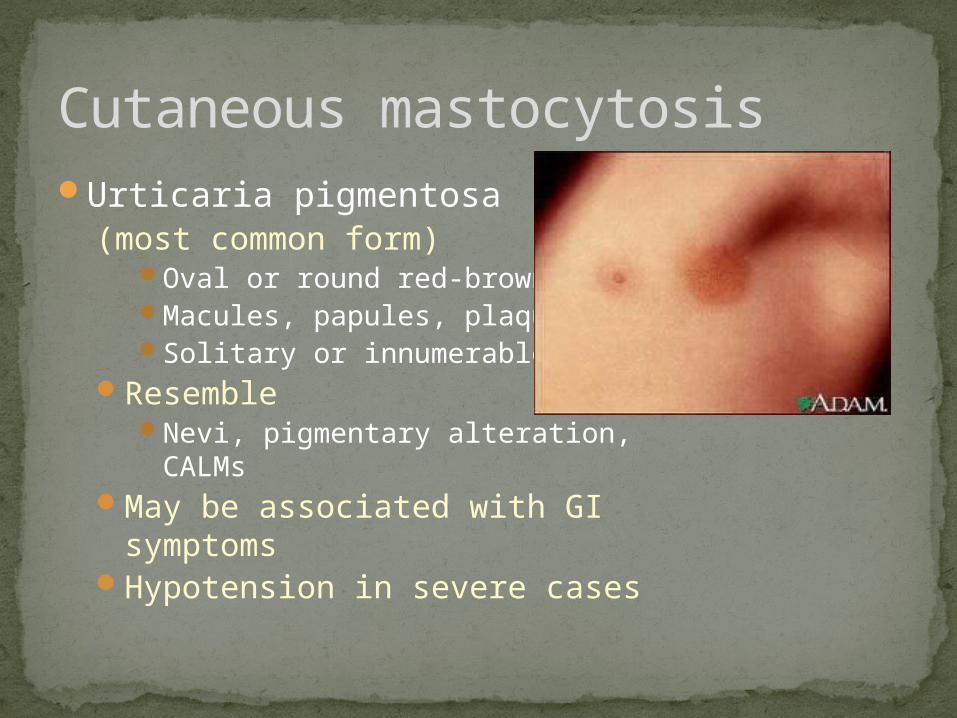
Urticaria pigmentosa (most common form)
Oval or round red-brownMacules, papules, plaquesSolitary or innumerable
ResembleNevi, pigmentary alteration,
CALMsMay be associated with GI
symptomsHypotension in severe cases
Cutaneous mastocytosis
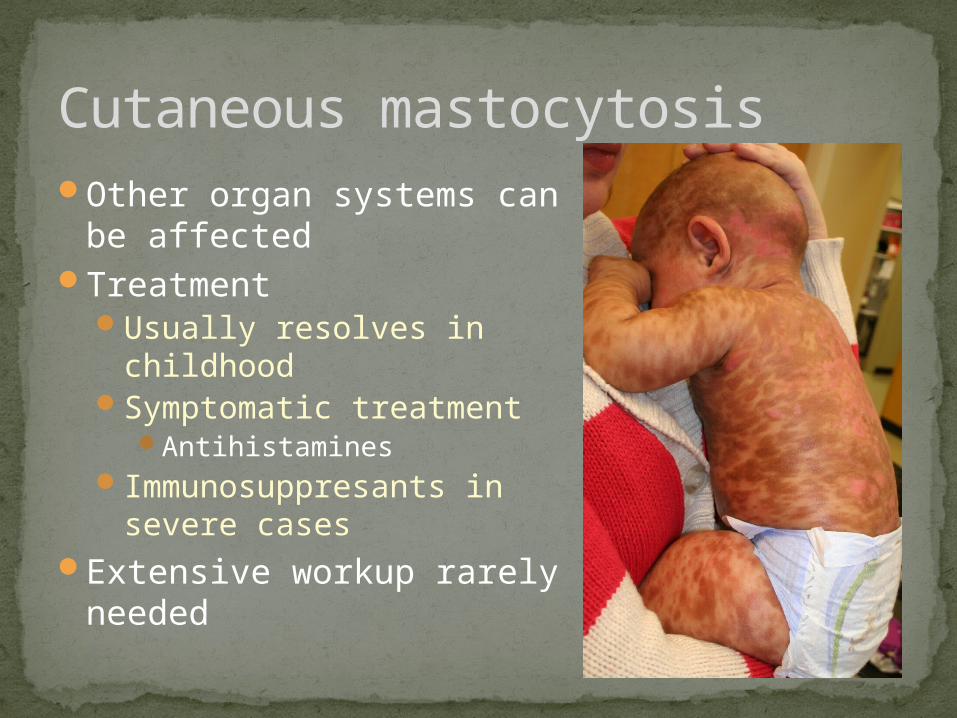
Other organ systems can be affected
TreatmentUsually resolves in childhoodSymptomatic treatment
AntihistaminesImmunosuppresants in
severe casesExtensive workup rarely
needed
Cutaneous mastocytosis
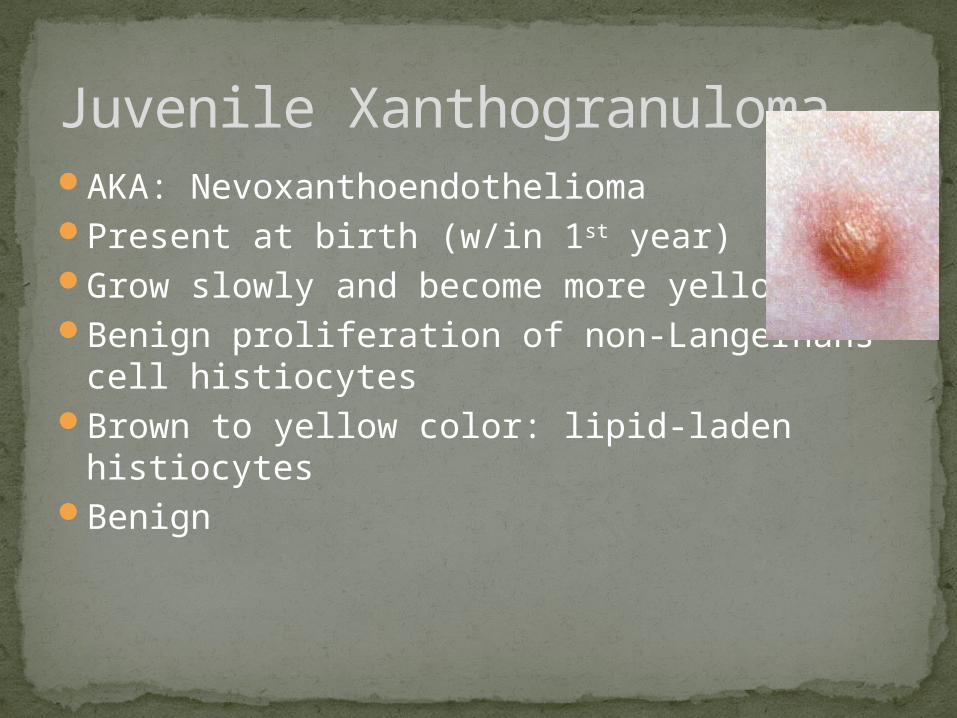
AKA: NevoxanthoendotheliomaPresent at birth (w/in 1st year)Grow slowly and become more yellowBenign proliferation of non-Langerhans cell
histiocytesBrown to yellow color: lipid-laden histiocytesBenign
Juvenile Xanthogranuloma
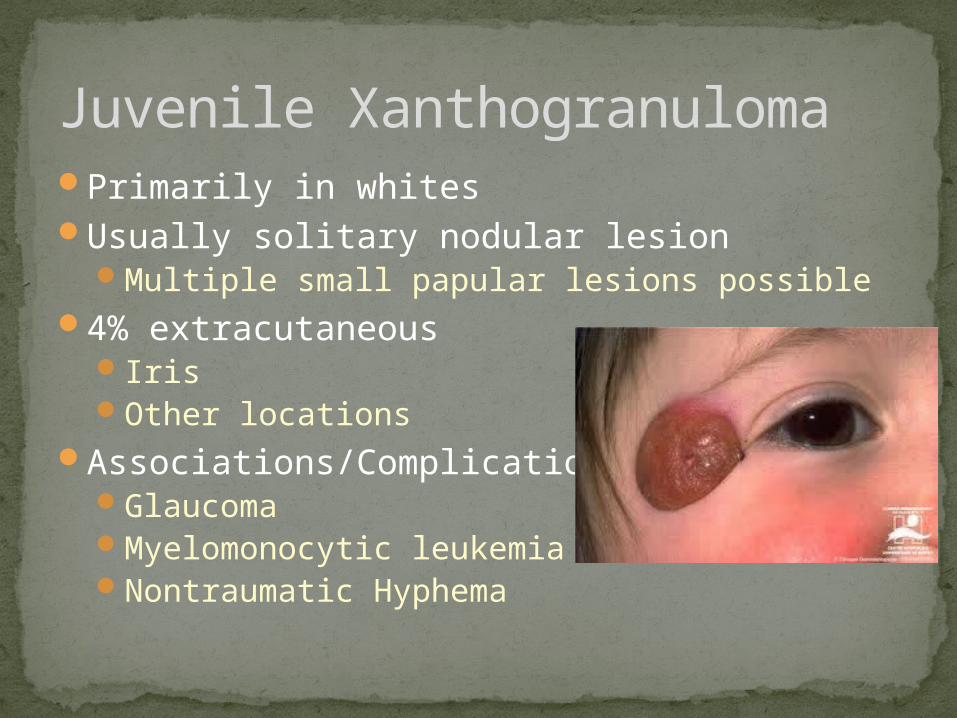
Primarily in whitesUsually solitary nodular lesion
Multiple small papular lesions possible4% extracutaneous
IrisOther locations
Associations/ComplicationsGlaucomaMyelomonocytic leukemiaNontraumatic Hyphema
Juvenile Xanthogranuloma

No specific gene defectNF-1Urticaria pigmentosaNiemann-Pick
TreatmentWatchful waiting
Resolve 5y/oSurgical excisionSteroids +/- chemo
Juvenile Xanthogranuloma
Abnormal immunityT-Cells, NeutrophilsHigh IgE and eosinophils
Chromosome q4ADVariable expressivity
Job Syndrome
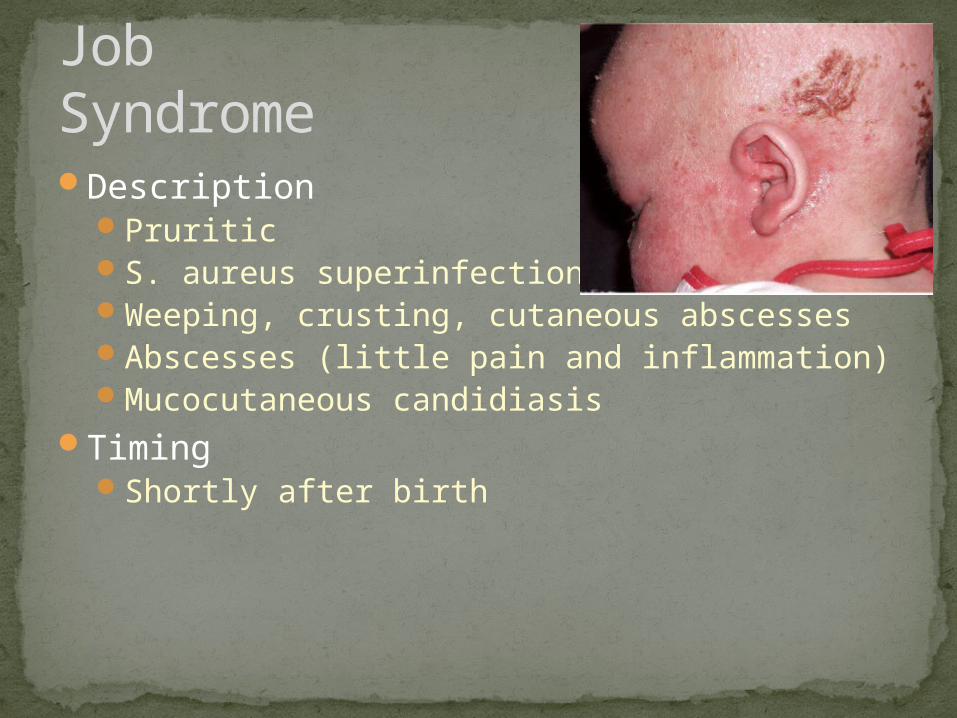
DescriptionPruriticS. aureus superinfectionWeeping, crusting, cutaneous abscessesAbscesses (little pain and inflammation)Mucocutaneous candidiasis
TimingShortly after birth
Job Syndrome
CourseRecurrent focal bacterial
infectionsDecreased bone density
with multiple fracturesLittle pain
With age: scoliosis and coarsening of facial features
TreatmentControl infections
Job Syndrome





























