Embed Size (px)
Citation preview
RESEARCH ARTICLE
The presence of the gadolinium-based
contrast agent depositions in the brain and
symptoms of gadolinium neurotoxicity - A
systematic review
Cyprian Olchowy1*, Kamil Cebulski2, Mateusz Łasecki1, Radosław Chaber3,
Anna Olchowy2, Krzysztof Kałwak4, Urszula Zaleska-Dorobisz1
1 Department of General and Pediatric Radiology, Wroclaw Medical University, Wrocław, Poland,
2 Radiology Students’ Scientific Club, Wrocław Medical University, Wroclaw, Poland Department of General
and Pediatric Radiology, Wroclaw Medical University, Wroclaw, Poland, 3 Division of Hematology, Cancer
Prevention and Propaedeutics of Rare Diseases, Faculty of Medicine, University of Rzeszow, Rzeszow,
Poland, 4 Department of Pediatric Hematology, Oncology and BMT, Wroclaw Medical University, Wrocław,
Poland
Abstract
Background and purpose
Gadolinium based contrast agents (GBCAs) are widely used in magnetic resonance
imaging, but recently, high signal intensity in the cerebellum structures was reported after
repeated administrations of contrast- enhanced magnetic resonance images. The aim of
this systematic review was to investigate the association between increased signal inten-
sity in the dentate nucleus and globus pallidus in the brain and repeated administrations
of GBCAs. Additionally, we focused on possible short- and long-term consequences of
gadolinium use in those patients.
Methods
Systematic review of retrospective investigations in PubMed and Medline was performed in
July 2016. Primary outcomes included the presence of increased signal intensity within the
dentate nucleus and globus pallidus on unenhanced T1-weighted MR images in patients fol-
lowing administrations of GBCAs. Two independent reviewers were responsible for search
and data extraction.
Results
25 publications satisfied inclusion criteria (19 magnetic resonance images analyses, 3 case
reports; 3 autopsy studies). Magnetic resonance images of 1247 patients with increased sig-
nal intensity on unenhanced T1-weighted MR images were analyzed as well as tissue speci-
mens from 27 patients. Signal intensity correlated positively with the exposure to GBCAs
and was greater after serial administrations of linear nonionic than cyclic contrast agents.
Gadolinium was detected in all tissue examinations.
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 1 / 14
a1111111111
a1111111111
a1111111111
a1111111111
a1111111111
OPENACCESS
Citation: Olchowy C, Cebulski K, Łasecki M, Chaber
R, Olchowy A, Kałwak K, et al. (2017) The presence
of the gadolinium-based contrast agent depositions
in the brain and symptoms of gadolinium
neurotoxicity - A systematic review. PLoS ONE 12
(2): e0171704. doi:10.1371/journal.pone.0171704
Editor: Subhra Mohapatra, University of South
Florida, UNITED STATES
Received: August 7, 2016
Accepted: January 23, 2017
Published: February 10, 2017
Copyright: © 2017 Olchowy et al. This is an open
access article distributed under the terms of the
Creative Commons Attribution License, which
permits unrestricted use, distribution, and
reproduction in any medium, provided the original
author and source are credited.
Data Availability Statement: All relevant data are
within the manuscript.
Funding: The authors received no specific funding
for this work.
Competing interests: The authors have declared
that no competing interests exist.
Conclusions
High signal intensity in the dentate nucleus and globus pallidus on unenhanced T1-weighted
magnetic resonance images were associated with previous administration of GBCAs. Sig-
nal intensity correlated negatively with stability of contrast agents. Clinical significance of
gadolinium deposition in the brain remains unclear. There is a strong need for further
research to identify type of gadolinium deposited in the brain as well as to gather knowledge
about long-term consequences.
Introduction
Magnetic resonance imaging (MRI) is one of the fastest developing noninvasive diagnostic
modalities in medicine. It employs innovative techniques and the newest discoveries, which
are safe and effective, but even so it is difficult to avoid pitfalls especially regarding long-term
consequences. The safety of gadolinium is now the most frequently discussed topic. This rare
paramagnetic metal is widely used in diagnostic imaging due to its high magnetic moment
and relatively long magnetic relaxation time. High toxicity of free gadolinium was eliminated
by closing free Gd3+ions in organic chelates. [1] Gadolinium based contrast agents (GBCAs)
are widely used in medicine since 1988, after Magnevist (Bayer Healthcare Pharmaceuticals)
gained the U.S. Food and Drug Administration approval. In 2014 unfortunately, Kanda et al.
observed connection between previous gadolinium administrations and high signal intensity
in the dentate nucleus and globus pallidus in the human brain independent of renal function.
[2] This discovery has drawn attention to the safety of contrast enhanced MRI. The impact of
gadolinium on human health remains unknown, although efforts are made to understand the
mechanisms of gadolinium toxicity which can help to find therapeutic and preventive solu-
tions for patients presenting signs and symptoms of gadolinium accumulation.[3]
Aim of the review
To shed more light on recent controversies regarding the use of GBCAs for MRI, we per-
formed a systematic review of the current literature with the aim to investigate the association
between increased signal intensity in the dentate nucleus and globus pallidus in the brain of
patients with a history of GBCA administrations. Additionally, we focused on possible short-
and long-term consequences of gadolinium use.
Search strategy
This study was done according to the guidelines of systematic reviews PRISMA. [4] We per-
formed a systematic search of PubMed and Medline databases for studies on MRI of the brain,
which assessed signal intensity of the dentate nucleus and globus pallidus performed in patients
following MRI examinations with GBCAs. The search was carried out in July 2016. The search
terms were gadolinium AND (dentate nucleus OR globus pallidus) and their combinations.
Additionally, we supplemented the electronic searches by hand searching the bibliographies of
relevant articles. Titles and abstracts were screened by two authors in order to exclude dupli-
cates and articles that did not meet the inclusion criteria. All other studies were retrieved for
full-text assessment performed by two researchers. Any discrepancies between the two review-
ers were resolved by consensus, with a third reviewer consulted when necessary.
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 2 / 14
Inclusion and exclusion criteria
Original studies, which investigated signal intensity in dentate nucleus and globus pallidus
examined in patients who had undergone repeated GBCA-enhanced magnetic resonance
(MR) were included in the analysis. We excluded studies with patients, in whom increased signal
intensity in those areas of the brain may have appeared due to other reason than gadolinium depo-
sition such as underlying Wilson disease, Rendu-Osler-Weber disease, manganese toxicity, calcifi-
cation, neurofibromatosis, or a history of total parenteral nutrition. Studies including patients
having hepatic or renal dysfunction as well as cases reports were analyzed for information about
side effects and toxicity related to gadolinium depositions in the brain. Letters, replies, editorials,
review articles, conference abstracts and animal studies were excluded.
Results
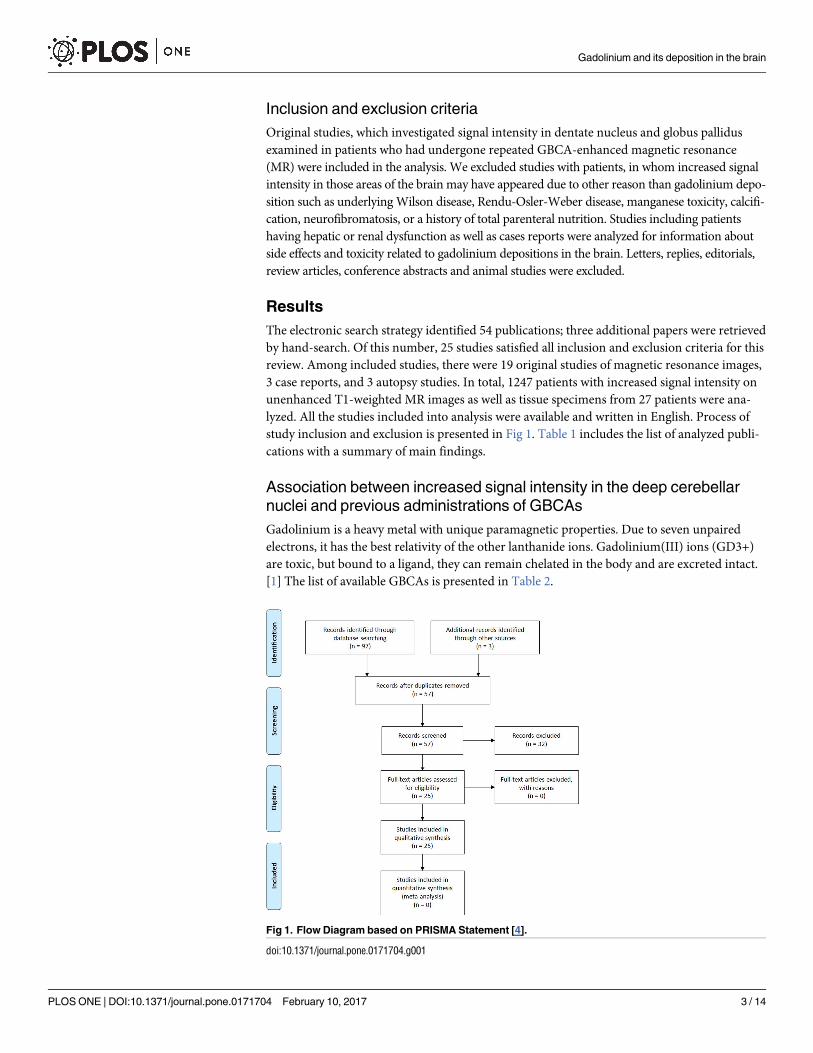
The electronic search strategy identified 54 publications; three additional papers were retrieved
by hand-search. Of this number, 25 studies satisfied all inclusion and exclusion criteria for this
review. Among included studies, there were 19 original studies of magnetic resonance images,
3 case reports, and 3 autopsy studies. In total, 1247 patients with increased signal intensity on
unenhanced T1-weighted MR images as well as tissue specimens from 27 patients were ana-
lyzed. All the studies included into analysis were available and written in English. Process of
study inclusion and exclusion is presented in Fig 1. Table 1 includes the list of analyzed publi-
cations with a summary of main findings.
Association between increased signal intensity in the deep cerebellar
nuclei and previous administrations of GBCAs
Gadolinium is a heavy metal with unique paramagnetic properties. Due to seven unpaired
electrons, it has the best relativity of the other lanthanide ions. Gadolinium(III) ions (GD3+)
are toxic, but bound to a ligand, they can remain chelated in the body and are excreted intact.
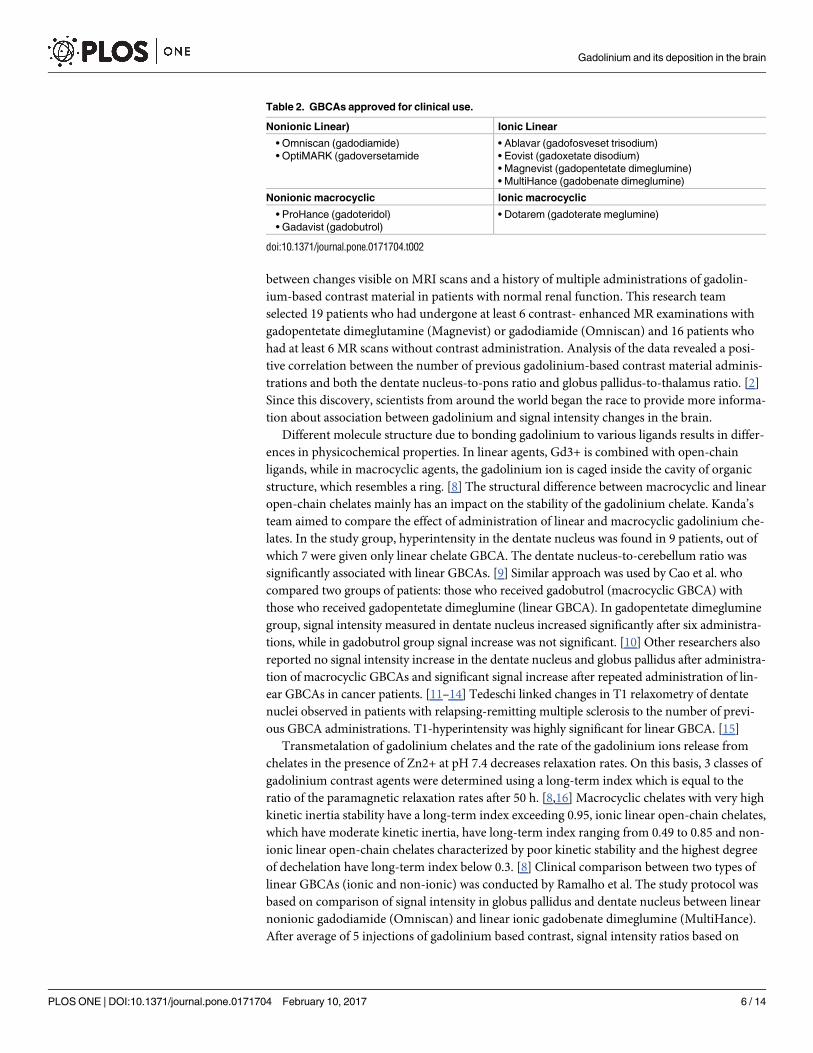
[1] The list of available GBCAs is presented in Table 2.
Fig 1. Flow Diagram based on PRISMA Statement [4].
doi:10.1371/journal.pone.0171704.g001
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 3 / 14
Table 1. Publications included in the systematic review.
Study Study groups Administrations of
GBCA
Contrast agent Remarks
Original studies
1 Adin et al.
2015 [42]
• Control = 54
• Increased SI = 103
• 0
• 2–60; median 18
Predominance of
gadopentetate dimeglumine
(Magnevist)
No significant difference in SI between
Magnevist and non-Magnevist group
2 Cao et al I
2016 [37]
• On hemodialysis = 25
• Control on hemodialysis = 13
• Near-normal renal function = 25
• Control near normal renal
function = 13
• 1.8 ± 1
• 0
• 1.8 ± 1
• 0
linear GBCA The percentage of patients with increased SI
in DN post-GBCA was significantly greater in
relation to pre-GBCA only in the group on
hemodialysis.
3 Cao et al II
2016 [10]
• Gadobutrol group = 25
• Gadopentetate
dimeglumine = 25
• 7.8 ± 2.4 (6–16)
• 12.1 ± 5.2 (6–23)
gadobutrol and
gadopentetate dimeglumine
Significant increase in SI in gadopentetate
dimeglumine group and insignificant in
gadobutrol group.
4 Errante 2014
[30]
• MS group = 38
• Brain metastases group = 37
• 2–14
• 2–21
gadodiamide (Omniscan) DNP were significantly higher between the
first and the last scan in both study groups in
patient with 6 or more examinations.
5 Flood 2016
[25]
• GBCA-naive control
subjects = 57
• GBCA-exposed patients = 30
• Pre- and post-GBCA
comparison = 16
• 0
• 5.9 ± 2.7
• 5.8 ± 2.1
gadopentetate dimeglumine
(Magnevist)
SI in DN was significantly higher in the
GBCA-exposed group than the GBCA-naive
group.
6 Hu 2016 [19] • Control group = 21
• GBCA group = 21
• 0
• 5–37
gadopentetate dimeglumine
(Magnevist)
Significant increase in the ND-to- corpus
callosum genu ratio and the GP-to- corpus
callosum genu ratio between the first and
most recent GBCA exam.
7 Kanda 2014
[2]
• contrast-enhanced MR
subgroup = 19
• unenhanced MR subgroup = 16
• 7.1 (6–12)
• 0
gadopentetate dimeglumine
(Magnevist)
gadodiamide (Omniscan)
DNP and GPT ratio was correlated with the
number of previous contrast-enhanced MR
scan.
8 Kanda 2015
[9]
• Magnevist group = 23
• ProHance group = 36
• Both agenst = 14
• Control = 54
• median 2; max 11
• median 2; max 15
• median 2; max 5
• 0
gadopentetate dimeglumine
(Magnevist)
gadoteridol (ProHance)
Only the DN-to-cerebellum ratio was
significantly associated with linear GBCA.
9 Kromrey 2016
[18]
• Gadobutrol group = 271
• Control group = 116
• 1
• 0
gadobutrol After 5-year follow-up, no significant
differences in SI were observed between
gadobutrol group and controls as well as
between baseline and follow-up
measurement.
10 Quattrocchi
2015 [14]
• group A = 10
• group B = 28
• group C = 8
• 1
• 1–5
• >6
gadodiamide A significant increase of DNP was between
the first and the last MRI in group C.
11 Radbruch I
2015 [12]
study group = 30 7.3 ± 3.1 gadobutrol No SI increase in the DN and GP was found
after serial applications gadobutrol.
12 Radbruch II
2015 [3]
• Magnevist group = 50
• Dotarem group = 50
• 7.32 ± 1.83
• 7.06 ± 1.20
gadopentetate dimeglumine
(Magnevist), gadoterate
meglumine (Dotarem)
In the linear GBCA group, the mean
difference in SI of DNP between the last and
first examinations was significantly larger
than 0, while in the macrocyclic GBCA group
was not significant.
13 Ramalho I
2015 [17]
• Omniscan group = 23
• MultiHance group = 46
• 5.0 ± 2.4 (3–11)
• 4.6 ± 2.1 (3–11)
gadodiamide (Omniscan)
gadobenate dimeglumine
(MultiHance)
GPT and DN-to- middle cerebellar peduncle
ratio increased significantly over time with
multiple administrations of a linear nonionic
GBCA (gadodiamide) but did not increase
with serial applications of a linear ionic GBCA
(gadobenate dimeglumine).
14 Ramalho II
2016 [21]
• gadobenate dimeglumine = 44
• previous gadodiamide and
current gadobenate
dimeglumine = 18
• 4.5 ± 2.0 (3–11)
• 5.9 ± 2.7 (3–11)
• 5.5 ± 1.9 (3–10)
gadodiamide (Omniscan)
gadobenate dimeglumine
(MultiHance)
Significant increase in DN-to- middle
cerebellar peduncle ratio appeared after
gadodiamide injections. It was insignificantly
higher in the group receiving both GBCAs.
(Continued )
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 4 / 14
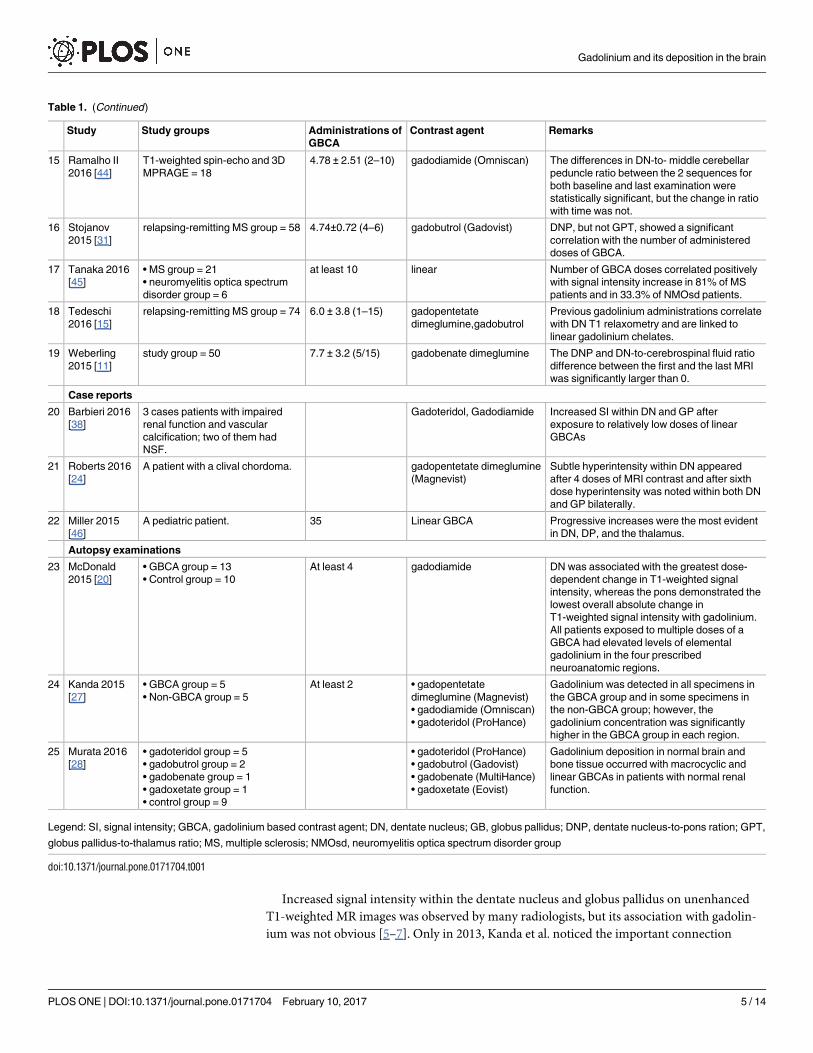
Increased signal intensity within the dentate nucleus and globus pallidus on unenhanced
T1-weighted MR images was observed by many radiologists, but its association with gadolin-
ium was not obvious [5–7]. Only in 2013, Kanda et al. noticed the important connection
Table 1. (Continued)
Study Study groups Administrations of
GBCA
Contrast agent Remarks
15 Ramalho II
2016 [44]
T1-weighted spin-echo and 3D
MPRAGE = 18
4.78 ± 2.51 (2–10) gadodiamide (Omniscan) The differences in DN-to- middle cerebellar
peduncle ratio between the 2 sequences for
both baseline and last examination were
statistically significant, but the change in ratio
with time was not.
16 Stojanov
2015 [31]
relapsing-remitting MS group = 58 4.74±0.72 (4–6) gadobutrol (Gadovist) DNP, but not GPT, showed a significant
correlation with the number of administered
doses of GBCA.
17 Tanaka 2016
[45]
• MS group = 21
• neuromyelitis optica spectrum
disorder group = 6
at least 10 linear Number of GBCA doses correlated positively
with signal intensity increase in 81% of MS
patients and in 33.3% of NMOsd patients.
18 Tedeschi
2016 [15]
relapsing-remitting MS group = 74 6.0 ± 3.8 (1–15) gadopentetate
dimeglumine,gadobutrol
Previous gadolinium administrations correlate
with DN T1 relaxometry and are linked to
linear gadolinium chelates.
19 Weberling
2015 [11]
study group = 50 7.7 ± 3.2 (5/15) gadobenate dimeglumine The DNP and DN-to-cerebrospinal fluid ratio
difference between the first and the last MRI
was significantly larger than 0.
Case reports
20 Barbieri 2016
[38]
3 cases patients with impaired
renal function and vascular
calcification; two of them had
NSF.
Gadoteridol, Gadodiamide Increased SI within DN and GP after
exposure to relatively low doses of linear
GBCAs
21 Roberts 2016
[24]
A patient with a clival chordoma. gadopentetate dimeglumine
(Magnevist)
Subtle hyperintensity within DN appeared
after 4 doses of MRI contrast and after sixth
dose hyperintensity was noted within both DN
and GP bilaterally.
22 Miller 2015
[46]
A pediatric patient. 35 Linear GBCA Progressive increases were the most evident
in DN, DP, and the thalamus.
Autopsy examinations
23 McDonald
2015 [20]
• GBCA group = 13
• Control group = 10
At least 4 gadodiamide DN was associated with the greatest dose-
dependent change in T1-weighted signal
intensity, whereas the pons demonstrated the
lowest overall absolute change in
T1-weighted signal intensity with gadolinium.
All patients exposed to multiple doses of a
GBCA had elevated levels of elemental
gadolinium in the four prescribed
neuroanatomic regions.
24 Kanda 2015
[27]
• GBCA group = 5
• Non-GBCA group = 5
At least 2 • gadopentetate
dimeglumine (Magnevist)
• gadodiamide (Omniscan)
• gadoteridol (ProHance)
Gadolinium was detected in all specimens in
the GBCA group and in some specimens in
the non-GBCA group; however, the
gadolinium concentration was significantly
higher in the GBCA group in each region.
25 Murata 2016
[28]
• gadoteridol group = 5
• gadobutrol group = 2
• gadobenate group = 1
• gadoxetate group = 1
• control group = 9
• gadoteridol (ProHance)
• gadobutrol (Gadovist)
• gadobenate (MultiHance)
• gadoxetate (Eovist)
Gadolinium deposition in normal brain and
bone tissue occurred with macrocyclic and
linear GBCAs in patients with normal renal
function.
Legend: SI, signal intensity; GBCA, gadolinium based contrast agent; DN, dentate nucleus; GB, globus pallidus; DNP, dentate nucleus-to-pons ration; GPT,
globus pallidus-to-thalamus ratio; MS, multiple sclerosis; NMOsd, neuromyelitis optica spectrum disorder group
doi:10.1371/journal.pone.0171704.t001
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 5 / 14
between changes visible on MRI scans and a history of multiple administrations of gadolin-
ium-based contrast material in patients with normal renal function. This research team
selected 19 patients who had undergone at least 6 contrast- enhanced MR examinations with
gadopentetate dimeglutamine (Magnevist) or gadodiamide (Omniscan) and 16 patients who
had at least 6 MR scans without contrast administration. Analysis of the data revealed a posi-
tive correlation between the number of previous gadolinium-based contrast material adminis-
trations and both the dentate nucleus-to-pons ratio and globus pallidus-to-thalamus ratio. [2]
Since this discovery, scientists from around the world began the race to provide more informa-
tion about association between gadolinium and signal intensity changes in the brain.
Different molecule structure due to bonding gadolinium to various ligands results in differ-
ences in physicochemical properties. In linear agents, Gd3+ is combined with open-chain
ligands, while in macrocyclic agents, the gadolinium ion is caged inside the cavity of organic
structure, which resembles a ring. [8] The structural difference between macrocyclic and linear
open-chain chelates mainly has an impact on the stability of the gadolinium chelate. Kanda’s
team aimed to compare the effect of administration of linear and macrocyclic gadolinium che-
lates. In the study group, hyperintensity in the dentate nucleus was found in 9 patients, out of
which 7 were given only linear chelate GBCA. The dentate nucleus-to-cerebellum ratio was
significantly associated with linear GBCAs. [9] Similar approach was used by Cao et al. who
compared two groups of patients: those who received gadobutrol (macrocyclic GBCA) with
those who received gadopentetate dimeglumine (linear GBCA). In gadopentetate dimeglumine
group, signal intensity measured in dentate nucleus increased significantly after six administra-
tions, while in gadobutrol group signal increase was not significant. [10] Other researchers also
reported no signal intensity increase in the dentate nucleus and globus pallidus after administra-
tion of macrocyclic GBCAs and significant signal increase after repeated administration of lin-
ear GBCAs in cancer patients. [11–14] Tedeschi linked changes in T1 relaxometry of dentate
nuclei observed in patients with relapsing-remitting multiple sclerosis to the number of previ-
ous GBCA administrations. T1-hyperintensity was highly significant for linear GBCA. [15]
Transmetalation of gadolinium chelates and the rate of the gadolinium ions release from
chelates in the presence of Zn2+ at pH 7.4 decreases relaxation rates. On this basis, 3 classes of
gadolinium contrast agents were determined using a long-term index which is equal to the
ratio of the paramagnetic relaxation rates after 50 h. [8,16] Macrocyclic chelates with very high
kinetic inertia stability have a long-term index exceeding 0.95, ionic linear open-chain chelates,
which have moderate kinetic inertia, have long-term index ranging from 0.49 to 0.85 and non-
ionic linear open-chain chelates characterized by poor kinetic stability and the highest degree
of dechelation have long-term index below 0.3. [8] Clinical comparison between two types of
linear GBCAs (ionic and non-ionic) was conducted by Ramalho et al. The study protocol was
based on comparison of signal intensity in globus pallidus and dentate nucleus between linear
nonionic gadodiamide (Omniscan) and linear ionic gadobenate dimeglumine (MultiHance).
After average of 5 injections of gadolinium based contrast, signal intensity ratios based on
Table 2. GBCAs approved for clinical use.
Nonionic Linear) Ionic Linear
• Omniscan (gadodiamide)
• OptiMARK (gadoversetamide
• Ablavar (gadofosveset trisodium)
• Eovist (gadoxetate disodium)
• Magnevist (gadopentetate dimeglumine)
• MultiHance (gadobenate dimeglumine)
Nonionic macrocyclic Ionic macrocyclic
• ProHance (gadoteridol)
• Gadavist (gadobutrol)
• Dotarem (gadoterate meglumine)
doi:10.1371/journal.pone.0171704.t002
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 6 / 14
measurement within dentate nucleus and middle cerebellar peduncle as well as globus pallidus
and thalamus increased significantly only in the group which received gadodiamide having the
worst long-term index. [17] Radbruch et al. reported that in case of macrocyclic GBCAs, the
difference in signal intensity in similar area was not significant even after average of 7 exami-
nations with gadoterate meglumine and gadobutrol. [12,13]
The long-term effect of a single injection of gadobutrol was examined based on SHIP data-
base conducted as a prospective population-based cohort study. After 5-year follow-up, no sig-
nificant difference in signal intensity was observed between gadobutrol group and controls as
well as between baseline and follow-up measurement. Signal intensity was measured within
thalamus, pallidum, pons, dentate nucleus as well as white matter and gray matter. The study
shows that gadobutrol does not lead to a measurable increase in signal intensity in neuronal
structures when applied even at a 1.5 times higher dose than generally required. [18] On the
contrary, Hu et al. reported visible changes as early as on the second examination carried out
with gadopentetate dimeglumine (ionic linear GBCA) in two pediatric patients. [19]
Investigators are interested in not only when the changes appear, but also whether they can
resolve. Usually, increased signal intensity within brain structures were reported after repeated
administrations of GBCAs of at least four times in case of linear contrast agents [12,20], but in
case of macrocyclic ones, exposure to six applications resulted in insignificant increase in sig-
nal intensity [10] Ramalho et al. showed that injections of a contrast agent characterized by
poor stability in the past results in signal increase even after using more stable contrasts in sub-
sequent examinations, which draws attention to potential potentiating effect of unstable
agents. [21] Birka et al. described a case of patient with nephrogenic systemic fibrosis; detect-
able amounts of gadolinium-phosphate deposits were found after 11 years post administration
of GBCA. [22] None of the authors reported decrease in signal intensity over time at the time
of writing our paper (by July 2016); however, during a revision of the manuscript, Radbruch
et al. reported a decrease in preexisting signal hyperintensity after changing from linear to
macrocyclic GBCA. It was suggested that some washout may exist. [23]
Many researchers reported similar changes within brain structures after gadolinium
enhanced MRI scans in pediatric patients. In the Hu’s et al. study, the changes, both in the den-
tate nucleus ratio and the globus pallidus ratio, were significant when compared between the
first and most recent GBCA examination. Investigators draw the attention to the fact that
hyperintensity either in the dentate nucleus or the globus pallidus was visually noticed within
the first 10 GBCA exams in all patients and in some patient even after 2 administrations of
contrast, which may indicate greater susceptibility in children. The correlation analysis
revealed no significant associations between signal intensity ratios and both the number of
examinations or the total volume of GBCA administered. [19] Roberts et al. described the case
of a girl with a clival chordoma in whom subtle hyperintensity appeared after fourth adminis-
tration of linear GBCA. [24] Flood et al. showed that signal intensity within the dentate
nucleus was significantly higher in the GBCA-exposed group than the GBCA-naive group.
Additionally, signal intensity comparison before and after repeated GBCA exposures showed
significant increase within dentate nucleus, while within the globus pallidus signal intensity
change remained insignificant. Additionally, the dentate nucleus-to-pons ratio was signifi-
cantly correlated with the total cumulative gadolinium dose, but insignificantly with the total
number of contrast-enhanced examinations. [25]
Evidence of gadolinium deposition in the brain
An increase of relative signal intensity in the dentate nucleus and the globus pallidus on unen-
hanced T1-weighted MR images following administration of GBCAs was linked to gadolinium
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 7 / 14

administration, but it was generally believed that the gadolinium chelates do not diffuse
through plasma membranes and do not cross the intact blood-brain barrier. [26]
The first report about gadolinium deposition in the brain was published in 2011. Sanyal
et al. analyzed tissues from an autopsy case with verified advanced nephrogenic systemic fibro-
sis and detected insoluble Gd-phosphate deposits in many organs including cerebellum; how-
ever, gadolinium depositions were found only in the perivascular glial cells. [26] McDolnald
et al. aimed to examine if signal hyperintensity within dentate nucleus and globus pallidus visi-
ble on T1-weighted MR images after repeated administrations of GBCAs is associated with
gadolinium deposition in neuronal tissues. They found elevated levels of elemental gadolinium
in the dentate nucleus, pons, globus pallidus, and thalamus in all patients exposed to multiple
doses of a linear GBCA, whereas control patients demonstrated undetectable levels of elemen-
tal gadolinium. Gadolinium concentration was strongly correlated with a cumulative gadolin-
ium dose. Examinations showed major gadolinium deposits in the endothelial walls and small
fraction of gadolinium deposited in the neural tissue interstitium, which suggests crossing
intact blood-brain barrier. [20] Due to technical difficulties, Kanda et al. analyzed smaller than
in McDonald’s study groups of deceased patients who had been given different GBCAs. The
gadolinium concentration in dentate nucleus, globus pallidus, cerebellar white matter, frontal
lobe cortex, and frontal lobe white matter was significantly higher in the GBCA group than
in non-GBCA group. Detection of gadolinium in the samples from non-GBCA group was
explained by contamination. [27] Murata et al. examined brain specimens in patients who had
received either linear of macrocyclic GBCAs. Among the tested agents, they found the lowest
gadolinium deposition ratio in brain tissue for the macrocyclic agent gadoteridol. [28] The
greatest limitation of brain autopsy studies is that they were not able to detect a specific form
of gadolinium.
In the view of current discussion about form of gadolinium deposition, the case reported by
Birka et al. brings additional information; though, it concerns a patient with nephrogenic sys-
temic fibrosis. The investigators were able to determine GdPO4 and gadoteridol from skin
specimens from a patient who received one administration of a linear GBCA (gadopentetate)
and one of a macrocyclic GBCA (gadoteridol) given 11 and 8 years before tissue examination.
Chelated forms of gadolinium were not found. [22]
Multiple sclerosis
The first observations of increased signal intensity in dentate nuclei were linked to the second-
ary progressive disease subtype of multiple sclerosis and to increased clinical disability, lesion
load, and brain atrophy. [5] Post-inflammatory changes are common in the brain of patients
suffering from multiple sclerosis and may resemble post-GBCA administration hyperintensity
of the dentate nucleus visible on unenhanced T1-weighted images. Diagnosis of multiple scle-
rosis as well as assessment of new lesions in the brain requires repeated contrast enhanced MR
examinations. Contrast enhancement on post-gadolinium T1-weighted imaging help to differ-
entiate acute and chronic lesions. [29] Errante et al. proved that signal increase in patients with
multiple sclerosis depends not only on underlying primary disease but also on the number of
previously performed gadolinium- enhanced MR examinations. According to their study, T1
signal intensity of the dentate nucleus in patients with at least 6 enhanced MRI scans was sig-
nificantly higher than those with less than 6 scans. [30] Stojanov et al. focus on examinations
performed in patients with relapsing-remitting multiple sclerosis who had undergo several
MR scans with gadobutrol, which is macrocyclic non-ionic GBCA, characterized by better sta-
bility than used by Errante et al. open chain gadodiamide. [31] Dentate nucleus-to-pons ratio
increased significantly after the last examination but the change of globus pallidus-to-thalamus
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 8 / 14
ratio was insignificant. Those results were obtained after average of 4.74 gadolinium-based
contrast administrations, which is quite early comparing with study groups excluding patients
with multiple sclerosis. Later, other researchers questioned Stojanov’s team outcomes because
of methodological limitations of the study. [11,32]
Renal insufficiency
As early as in 2006, Grobner informed about an association between magnetic resonance angi-
ography with gadopentetate dimeglumine as a contrast agent performed in patients with end-
stage renal disease and the development of nephrogenic systemic fibrosis. [33] Cabot et al.
reported a patient who died of nephrogenic systemic fibrosis. High levels of gadolinium were
found in all biopsied tissues; unfortunately, the brain tissue samples were then not collected
for autopsy. [34] A year later Sanyal et al., reported the presence of insoluble gadolinium-phos-
phate deposits also in the cerebellum; however, they were detected only in the perivascular
glial cells. [26]
One of the factors that contribute to the pathogenesis of nephrogenic systemic fibrosis is
the slow excretion of GBCAs in those patients allowing the lower stability gadolinium chelates
to dissociate and release toxic Gd3+. Additionally, gadodiamide can activate elevated fibroblast
growth and elevated levels of hyaluronan synthesis [35], which are responsible for clinical
symptoms of nephrogenic systemic fibrosis.
Patients with renal failure are exposed to prolonged effect of injected GBCAs because prompt
elimination though renal excretion is impossible in those patients. Impairment of renal function
is than a risk factor for deposition of gadolinium in tissues, including the brain. [36] As a result,
signal intensity in dentate nucleus on unenhanced T1-weighted images was greater in hemodialy-
sis patients than in patients with normal renal function after repeated administrations of GBCAs.
[37] Additionally, Barbieri et al. described three cases with impaired renal function and vascular
calcification, which presented with signal hyperintensity within the dentate nucleus and the globus
pallidus on unenhanced T1-weighted MR images after exposure to relatively low doses of linear
GBCAs. [38] Those reports suggest that impaired renal function accelerates the rate of gadolinium
accumulation in the brain.
Patients with a low estimated glomerular filtration rate are at higher risk of complications
related to GBCA administration than those with normal renal function. Currently, the Con-
trast Media Safety Committee of the European Society of Urogenital Radiology recommends
administering the smallest required amount of macrocyclic GBCAs, keeping at least weekly
break between injections and planning an additional dialysis session in patients on dialysis.
[39] Patients with impaired renal function should be carefully monitored, as they are prone to
known and unknown adverse reactions of gadolinium.
Brain irradiation
Radiation-related injury to the brain may result in calcifications, which are visible as an increase
of magnetic resonance signal intensity. [40] Post-radiation changes may give non-specific
hyperintense signal changes which are similar to many other conditions affecting the dentate
nuclei [41]; therefore, patients who had undergone brain irradiation are commonly excluded
from the studies examining the presence of hyperintense signal changes in relation to previous
gadolinium exposure. In our review, Adin’s at al. study included 129 patients with a history of
brain radiotherapy among other. Of that group, specific radiation exposures of the dentate
nuclei were confirmed for 108 subjects. Their analysis revealed that in the group with increased
signal intensity, the total exposure of the brain was lower than in the group without
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 9 / 14
hyperintensity, although the groups did not differ significantly. [42] Adin’s team report is in
line with Kanda et al. findings who reported that brain irradiation had no impact on signal
change. [2]
Neurotoxicity of GBCAs
Gadolinium chelates are considered safe because of their efficient renal excretion from the
body in an unchanged form. However, GBCAs have different stability, and therefore some
agents are more prone for dechelation than others are. Toxicity of gadolinium is associated
with similarity between gadolinium and calcium ions, but refers exceptionally to free ions.
Gd3+ can compete with Ca2+ and act as an inorganic blocker of voltage-gated calcium chan-
nels with all negative consequences in many sites of the human body. [1] Despite extensive
research, little is known about possible consequences of gadolinium brain depositions. Neither
mechanism responsible for collection of gadolinium in dentate nucleus and globus pallidus
nor the form of deposited gadolinium has been discovered.
The analysis of clinical events in 16 dialysis patients performed by Cao et al. allowed for
comparison of their frequency during a period of a month before with a month after each
exposure to linear GBCA. All neurological symptoms described during the 30 days after
GBCA administration such as migraine headache, loss of consciousness, memory loss, falling,
lightheadedness, and ataxia, occurred also before MRI with GBCA; therefore, they cannot be
related to gadolinium toxicity. [37] Barbieri et al. described three patients with impaired renal
function and vascular calcifications who presented with signal hyperintensity characteristic for
gadolinium brain depositions. All of them suffered from transient signs of neurological disor-
ders of undetermined cause, but the association of those symptoms with gadolinium toxicity
remains unclear. [38]
There are several patient advocacy groups, who gather people suffering from nephrogenic
systemic fibrosis and other symptoms related to GBCAs administration. Recently, a self-report
survey among patients, who attributed their symptoms to previous GBCA administrations,
was published. Respondents (n = 50) received intravenous gadolinium contrast with an aver-
age of 4.2 doses (range 1–23). Two-thirds of them experienced those symptoms immediately
following GBCA-enchanced examination. Bone/joint pain as well as head/neck problems such
as headache, vision change, and hearing change were mentioned the most frequently; they
occurred in more than 75% of questionnaires. About 60% of respondents complained about
dermatologic changes. [43] The study has a long list of limitations, but constitutes the first
description of symptoms, which may be related to gadolinium toxicity.
Technical considerations
The number of studies on the effect of using various GBCAs on the brain has been rapidly
increasing since the first report about association of previous repeated GBCAs and hyperinten-
sity of dentate nucleus and globus pallidus. [2] The level of knowledge increases, but when ana-
lyzing data, it seems that some researchers report incompatible findings affected by
unintended limitations. First, qualitative and quantitative signal-intensity measurement meth-
ods are used together in many studies. Many MRI protocols employed sequences such as
T1-weighted spin-echo [10,17,42], T1 MPRAGE [42], T1 FLAIR [30,42], T1-weighted 3D
MPRAGE [18,25] and FLASH [11] alone or in combination. Ramalho et al. concluded that
T1-weighted spin-echo and MPRAGE sequences should not be used interchangeably for quali-
tative or quantitative T1 signal-intensity analysis of the dentate nucleus in patients who
undergo several gadolinium-enhanced MR examinations as those methods result in statisti-
cally significant differences. [44]
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 10 / 14
Next, as those studies are retrospective in nature, it is sometimes difficult to retrieve informa-
tion or to collect proper study population. Studies present outcomes of different number of pre-
vious exposure to GBCAs administered at different time intervals; thus, heterogeneity of study
samples is a potential source of bias. Many of the reviewed studies included cancer patients who
had undergone radiation therapy [9–13], some included patients with impaired renal function
(estimated glomerular filtration rate<60 mL/min per 1.73 m2) [12] or increased liver serum
parameters [11–13] among others.
Conclusions
Literature review confirms that increased signal intensity in the dentate nucleus and globus
pallidus on unenhanced T1-weighted MR images is associated with previous administrations
of GBCAs, predominantly linear, and corresponds with the concentration of gadolinium in
the brain tissue.
Despite of rapidly growing number of published papers, the level of knowledge about gado-
linium depositions in the brain and their clinical significance remains insufficient; therefore, it
seems to be reasonable to choose the most stable types of GBCAs and avoid higher doses espe-
cially in children and young patients even with normal renal function.
There is a strong need for further research to shed light on the nature of gadolinium deposi-
tion in the brain, their effect on the brain tissue functioning and occurrence of long-lasting
adverse reaction. Multidisciplinary approach including participation of radiologists, neurolo-
gists, psychiatrists, and biologists who could evaluate the clinical significance of gadolinium
depositions in the brain in prospective projects encompassing pediatric patients are required.
Supporting information
S1 File. Prisma Checklist.
(DOC)
Author Contributions
Conceptualization: CO KC UZD.
Data curation: CO.
Formal analysis: CO KC.
Investigation: CO KC MŁ RC AO.
Methodology: CO UZD KK.
Project administration: CO UZD.
Supervision: RC KK UZD.
Validation: UZD.
Writing – original draft: CO KC MŁ AO.
Writing – review & editing: CO RC KK UZD.
References1. Caravan P, Ellison JJ, McMurry TJ, Lauffer RB. Gadolinium(III) Chelates as MRI Contrast Agents:
Structure, Dynamics, and Applications. Chem Rev 1999; 99:2293–2352. PMID: 11749483
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 11 / 14
2. Kanda T, Ishii K, Kawaguchi H, Kitajima K, Takenaka D. High signal intensity in the dentate nucleus and
globus pallidus on unenhanced T1-weighted MR images: relationship with increasing cumulative dose
of a gadolinium-based contrast material. Radiology 2014; 270:834–841. doi: 10.1148/radiol.13131669
PMID: 24475844
3. Rogosnitzky M, Branch S. Gadolinium-based contrast agent toxicity: a review of known and proposed
mechanisms. Biometals 2016; 29:365–376. doi: 10.1007/s10534-016-9931-7 PMID: 27053146
4. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-
analyses: the PRISMA statement. PLoS Med 2009; 6:e1000097. doi: 10.1371/journal.pmed.1000097
PMID: 19621072
5. Roccatagliata L, Vuolo L, Bonzano L, Pichiecchio A, Mancardi GL. Multiple sclerosis: hyperintense den-
tate nucleus on unenhanced T1-weighted MR images is associated with the secondary progressive
subtype. Radiology 2009; 251:503–510. doi: 10.1148/radiol.2511081269 PMID: 19401576
6. Kasahara S, Miki Y, Kanagaki M, Yamamoto A, Mori N, Sawada T, et al. Hyperintense dentate nucleus
on unenhanced T1-weighted MR images is associated with a history of brain irradiation. Radiology
2011; 258:222–228. doi: 10.1148/radiol.10100508 PMID: 21045180
7. Lai PH, Chen C, Liang HL, Pan HB. Hyperintense basal ganglia on T1-weighted MR imaging. AJR Am J
Roentgenol 1999; 172:1109–1115. doi: 10.2214/ajr.172.4.10587157 PMID: 10587157
8. Port M, Idee JM, Medina C, Robic C, Sabatou M, Corot C. Efficiency, thermodynamic and kinetic stabil-
ity of marketed gadolinium chelates and their possible clinical consequences: a critical review. Biome-
tals 2008; 21:469–490. doi: 10.1007/s10534-008-9135-x PMID: 18344005
9. Kanda T, Osawa M, Oba H, Toyoda K, Kotoku J, Haruyama T, et al. High Signal Intensity in Dentate
Nucleus on Unenhanced T1-weighted MR Images: Association with Linear versus Macrocyclic Gadolin-
ium Chelate Administration. Radiology 2015; 275:803–809. doi: 10.1148/radiol.14140364 PMID:
25633504
10. Cao Y, Huang DQ, Shih G, Prince MR. Signal Change in the Dentate Nucleus on T1-Weighted MR
Images After Multiple Administrations of Gadopentetate Dimeglumine Versus Gadobutrol. AJR Am J
Roentgenol 2016; 206:414–419. doi: 10.2214/AJR.15.15327 PMID: 26700156
11. Weberling LD, Kieslich PJ, Kickingereder P, Wick W, Bendszus M, Schlemmer HP, et al. Increased Sig-
nal Intensity in the Dentate Nucleus on Unenhanced T1-Weighted Images After Gadobenate Dimeglu-
mine Administration. Invest Radiol 2015; 50:743–748. doi: 10.1097/RLI.0000000000000206 PMID:
26352749
12. Radbruch A, Weberling LD, Kieslich PJ, Hepp J, Kickingereder P, Wick W, et al. High-Signal Intensity in
the Dentate Nucleus and Globus Pallidus on Unenhanced T1-Weighted Images: Evaluation of the Mac-
rocyclic Gadolinium-Based Contrast Agent Gadobutrol. Invest Radiol 2015; 50:805–810. doi: 10.1097/
RLI.0000000000000227 PMID: 26523910
13. Radbruch A, Weberling LD, Kieslich PJ, Eidel O, Burth S, Kickingereder Pet al. Gadolinium retention in
the dentate nucleus and globus pallidus is dependent on the class of contrast agent. Radiology 2015;
275:783–791. doi: 10.1148/radiol.2015150337 PMID: 25848905
14. Quattrocchi CC, Mallio CA, Errante Y, Cirimele V, Carideo L, Ax A. et al. Gadodiamide and Dentate
Nucleus T1 Hyperintensity in Patients With Meningioma Evaluated by Multiple Follow-Up Contrast-
Enhanced Magnetic Resonance Examinations With No Systemic Interval Therapy. Invest Radiol 2015;
50:470–472. doi: 10.1097/RLI.0000000000000154 PMID: 25756685
15. Tedeschi E, Palma G, Canna A, Cocozza S, Russo C, Borrelli P, et al. In vivo dentate nucleus MRI
relaxometry correlates with previous administration of Gadolinium-based contrast agents. Eur Radiol.
2016 Feb 23.
16. Laurent S, Elst LV, Muller RN. Comparative study of the physicochemical properties of six clinical low
molecular weight gadolinium contrast agents. Contrast Media Mol Imaging 2006; 1:128–137. doi: 10.
1002/cmmi.100 PMID: 17193689
17. Ramalho J, Castillo M, AlObaidy M, Nunes RH, Ramalho M, Dale BM, et al. High Signal Intensity in Glo-
bus Pallidus and Dentate Nucleus on Unenhanced T1-weighted MR Images: Evaluation of Two Linear
Gadolinium-based Contrast Agents. Radiology 2015; 276:836–844. doi: 10.1148/radiol.2015150872
PMID: 26079490
18. Kromrey ML, Liedtke KR, Ittermann T, Langner S, Kirsch M, Weitschies W, et al. Intravenous injection
of gadobutrol in an epidemiological study group did not lead to a difference in relative signal intensities
of certain brain structures after 5 years. Eur Radiol 2016 May 24.
19. Hu HH, Pokorney A, Towbin RB, Miller JH. Increased signal intensities in the dentate nucleus and glo-
bus pallidus on unenhanced T1-weighted images: evidence in children undergoing multiple gadolinium
MRI exams. Pediatr Radiol. 2016 Jun 9.
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 12 / 14
20. McDonald RJ, McDonald JS, Kallmes DF, Jentoft ME, Murray DL, Thielen KR, et al. Intracranial Gado-
linium Deposition after Contrast-enhanced MR Imaging. Radiology 2015; 275:772–782. doi: 10.1148/
radiol.15150025 PMID: 25742194
21. Ramalho J, Semelka RC, AlObaidy M, Ramalho M, Nunes RH, Castillo M. Signal intensity change on
unenhanced T1-weighted images in dentate nucleus following gadobenate dimeglumine in patients
with and without previous multiple administrations of gadodiamide. Eur Radiol. 2016 Feb 24.
22. Birka M, Wentker KS, Lusmoller E, Arheilger B, Wehe CA, Sperling M, et al. Diagnosis of nephrogenic
systemic fibrosis by means of elemental bioimaging and speciation analysis. Anal Chem 2015;
87:3321–3328. doi: 10.1021/ac504488k PMID: 25708271
23. Radbruch A, Weberling LD, Kieslich PJ, Hepp J, Kickingereder P, Wick W, et al. Intraindividual Analysis
of Signal Intensity Changes in the Dentate Nucleus After Consecutive Serial Applications of Linear and
Macrocyclic Gadolinium-Based Contrast Agents. Invest Radiol. 2016; 51:683–690. doi: 10.1097/RLI.
0000000000000308 PMID: 27495187
24. Roberts DR, Holden KR. Progressive increase of T1 signal intensity in the dentate nucleus and globus
pallidus on unenhanced T1-weighted MR images in the pediatric brain exposed to multiple doses of
gadolinium contrast. Brain Dev 2016; 38:331–336. doi: 10.1016/j.braindev.2015.08.009 PMID:
26345358
25. Flood TF, Stence NV, Maloney JA, Mirsky DM. Pediatric Brain: Repeated Exposure to Linear Gadolin-
ium-based Contrast Material Is Associated with Increased Signal Intensity at Unenhanced T1-weighted
MR Imaging. Radiology 2016;160356.
26. Sanyal S, Marckmann P, Scherer S, Abraham JL. Multiorgan gadolinium (Gd) deposition and fibrosis in
a patient with nephrogenic systemic fibrosis—an autopsy-based review. Nephrol Dial Transplant 2011;
26:3616–3626. doi: 10.1093/ndt/gfr085 PMID: 21441397
27. Kanda T, Oba H, Toyoda K, Kitajima K, Furui S. Brain gadolinium deposition after administration of gad-
olinium-based contrast agents. Jpn J Radiol 2016; 34:3–9. doi: 10.1007/s11604-015-0503-5 PMID:
26608061
28. Murata N, Gonzalez-Cuyar LF, Murata K, Fligner C, Dills R, Hippe D, et al. Macrocyclic and Other Non-
Group 1 Gadolinium Contrast Agents Deposit Low Levels of Gadolinium in Brain and Bone Tissue: Pre-
liminary Results From 9 Patients With Normal Renal Function. Invest Radiol 2016; 51:447–453. doi: 10.
1097/RLI.0000000000000252 PMID: 26863577
29. Klawiter EC. Current and new directions in MRI in multiple sclerosis. Continuum (Minneap Minn) 2013;
19:1058–1073.
30. Errante Y, Cirimele V, Mallio CA, Di Lazzaro V, Zobel BB, Quattrocchi CC. Progressive increase of T1
signal intensity of the dentate nucleus on unenhanced magnetic resonance images is associated with
cumulative doses of intravenously administered gadodiamide in patients with normal renal function,
suggesting dechelation. Invest Radiol 2014; 49:685–690. doi: 10.1097/RLI.0000000000000072 PMID:
24872007
31. Stojanov DA, Aracki-Trenkic A, Vojinovic S, Benedeto-Stojanov D, Ljubisavljevic S. Increasing signal
intensity within the dentate nucleus and globus pallidus on unenhanced T1W magnetic resonance
images in patients with relapsing-remitting multiple sclerosis: correlation with cumulative dose of a mac-
rocyclic gadolinium-based contrast agent, gadobutrol. Eur Radiol 2016; 26:807–815. doi: 10.1007/
s00330-015-3879-9 PMID: 26105022
32. Agris J, Pietsch H, Balzer T. What Evidence Is There That Gadobutrol Causes Increasing Signal Inten-
sity within the Dentate Nucleus and Globus Pallidus on Unenhanced T1W MRI in Patients with RRMS?
Eur Radiol 2016; 26:816–817. doi: 10.1007/s00330-015-4019-2 PMID: 26391362
33. Grobner T. Gadolinium—a specific trigger for the development of nephrogenic fibrosing dermopathy
and nephrogenic systemic fibrosis? Nephrol Dial Transplant 2006; 21:1104–1108. doi: 10.1093/ndt/
gfk062 PMID: 16431890
34. Cabot RC, Harris NL, Shepard JA, Rosenberg ES, Cort AM, Ebeling SH, et al. Case records of the Mas-
sachusetts General Hospital: Case 38–2010: a 13-year-old girl with an enlarging neck mass. N Engl J
Med 2010; 363:2445–2454. doi: 10.1056/NEJMcpc1004361 PMID: 21158661
35. Edward M, Quinn JA, Mukherjee S, Jensen MB, Jardine AG, Mark PB, et al. Gadodiamide contrast
agent ’activates’ fibroblasts: a possible cause of nephrogenic systemic fibrosis. J Pathol 2008;
214:584–593. doi: 10.1002/path.2311 PMID: 18220317
36. Joffe P, Thomsen HS, Meusel M. Pharmacokinetics of gadodiamide injection in patients with severe
renal insufficiency and patients undergoing hemodialysis or continuous ambulatory peritoneal dialysis.
Acad Radiol 1998; 5:491–502. PMID: 9653466
37. Cao Y, Zhang Y, Shih G, Zhang Y, Bohmart A, Hecht EM, et al. Effect of Renal Function on Gadolinium-
Related Signal Increases on Unenhanced T1-Weighted Brain Magnetic Resonance Imaging. Invest
Radiol. 2016 Jun 1.
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 13 / 14
38. Barbieri S, Schroeder C, Froehlich JM, Pasch A, Thoeny HC. High signal intensity in dentate nucleus
and globus pallidus on unenhanced T1-weighted MR images in three patients with impaired renal func-
tion and vascular calcification. Contrast Media Mol Imaging 2016; 11:245–250. doi: 10.1002/cmmi.1683
PMID: 26929131
39. Contrast Media Guidelines—version 8.1. ESUR Contrast Media Safety Committee. 2016; 05:15. Avail-
able: http://www.esur.org/guidelines.
40. Suzuki S, Nishio S, Takata K, Morioka T, Fukui M. Radiation-induced brain calcification: paradoxical
high signal intensity in T1-weighted MR images. Acta Neurochir (Wien) 2000; 142:801–804.
41. Khadilkar S, Jaggi S, Patel B, Yadav R, Hanagandi P, Faria do Amaral LL. A practical approach to dis-
eases affecting dentate nuclei. Clin Radiol 2016; 71:107–119. doi: 10.1016/j.crad.2015.09.010 PMID:
26577296
42. Adin ME, Kleinberg L, Vaidya D, Zan E, Mirbagheri S, Yousem DM. Hyperintense Dentate Nuclei on
T1-Weighted MRI: Relation to Repeat Gadolinium Administration. AJNR Am J Neuroradiol 2015;
36:1859–1865. doi: 10.3174/ajnr.A4378 PMID: 26294649
43. Burke LM, Ramalho M, AlObaidy M, Chang E, Jay M, Semelka RC. Self-reported gadolinium toxicity: A
survey of patients with chronic symptoms. Magn Reson Imaging 2016; 34:1078–1080. doi: 10.1016/j.
mri.2016.05.005 PMID: 27211256
44. Ramalho J, Ramalho M, AlObaidy M, Nunes RH, Castillo M, Semelka RC. T1 Signal-Intensity Increase
in the Dentate Nucleus after Multiple Exposures to Gadodiamide: Intraindividual Comparison between 2
Commonly Used Sequences. AJNR Am J Neuroradiol. 2016 Mar 31.
45. Tanaka M, Nakahara K, Kinoshita M. Increased Signal Intensity in the Dentate Nucleus of Patients with
Multiple Sclerosis in Comparison with Neuromyelitis Optica Spectrum Disorder after Multiple Doses of
Gadolinium Contrast. Eur Neurol. 2016; 75:195–8. doi: 10.1159/000445431 PMID: 27054693
46. Miller JH, Hu HH, Pokorney A, Cornejo P, Towbin R. MRI Brain Signal Intensity Changes of a Child Dur-
ing the Course of 35 Gadolinium Contrast Examinations. Pediatrics. 2015; 136:e1637–40. doi: 10.1542/
peds.2015-2222 PMID: 26574593
Gadolinium and its deposition in the brain
PLOS ONE | DOI:10.1371/journal.pone.0171704 February 10, 2017 14 / 14












![In vivo long-lasting alterations of central serotonin ... › track › pdf › 10.1186 › s13550-019-0557-yduced neurotoxicity in a rat model [ 25]. This result was in agreement](https://img.pdfslide.tips/doc/110x75/60d5cbc9aa07ca297d08c042/in-vivo-long-lasting-alterations-of-central-serotonin-a-track-a-pdf-a.jpg)















