Embed Size (px)
Citation preview

ScopeTheVol. 12 No 1
MUSC DEPARTMENT OF OTOLARYNGOLOGY HEAD & NECK SURGERY
Paul R. Lambert, M.D.
INSIDEDepartment
Anniversaries
Clinical Research
Clinical Update
Research Realm
Residents & Fellows
Faculty
CME Events
Chairman’s Corner
ENT.musc.edu
Winter 2011
50&100YEAr AnnivErsAriEs
100 Years Ago – Department of ENT Founded
The Department of Otolaryngology – Head and Neck Surgery at the Medical University of South Carolina traces its history to 1911, the year Dr. Edward F. Parker was appointed Professor of Ophthalmology and Otology. He had previously served as Dean of the Medical School.
Dr. Parker completed undergraduate studies at the University of Virginia and received his medical degree from the Medical College of South Carolina in 1889. He practiced General Medicine for several years before going to England and Germany to study eye, ear, nose and throat diseases. He remained at the Royal London Ophthalmic Hospital for several years before returning to Charleston as Professor of Physiology and a Lecturer on diseases of the eye, ear, nose and throat. He was the first specialist to practice EENT in Charleston, South Carolina and in 1911 became Professor of Diseases of the Eyes, Ears, Nose and Throat. He was a member of the American Laryngological, Rhinological, and Otological Society.
50 Years Ago – First Fulltime Academic Chair Appointed
In the 1950s, the Otolaryngology Division became an autonomous department under the direction of a prominent community surgeon, Dr. Robert Hope. In 1960, Dr. Richard W. Hanckel became the first fulltime academic Chair of the Department. Dr. Hanckel established a residency program and incorporated audiology and speech pathology as sections of the Department. He was active nationally, serving as president of the American Broncho-Esophagological Association and Vice President of the Southern Section of the Triological Society. In 1978 Dr. Hanckel was succeeded by Dr. Warren Y. Adkins, who served as the second academic Chair of the Department, retiring in 1998.
Landmark anniversaries serve as beacons, providing a sense of history and reminding us of our heritage. We owe much to those who have gone before us – especially to those who have fought the local and national battles that have shaped and enriched our wonderful specialty.
Paul R. Lambert, M.D. Professor and Chair,Otolaryngology - Head & Neck Surgery

2 http://ENT.musc.edu musc • discovery, understanding, healing since 1824
Intratympanic (IT) injection of corticosteroid solutions has been studied for hearing loss, tinnitus and balance disorders. While the benefits of IT delivery better enable drug diffusion from the middle ear (ME) to the inner ear (IE) via the round window membrane, commonly used steroid solutions are rapidly eliminated through the eustachian tube resulting in short ME/IE residence time.
For most clinical studies conducted to date using IT steroids, the dose regimen selection has been empirically-based. This is due to the absence of any preclinical dose-response studies with respect to efficacy, toxicity, or PK for the ME/IE compartments. Otonomy is a San Diego-based biotechnology company developing a technology that allows for common pharmaceuticals to be formulated in a glycol polymer. This polymer (i.e. poloxamer) has thermoreversible properties; it is in liquid state at ambient temperature and gels at body temperature after IT injection. Otonomy has developed a product, oto-104, that is a suspension of dexamethasone in poloxamer. after it injection, oto-104 transitions from solution to gel state in the ME thereby increasing middle ear residence time which allows for sustained presence of dexamethasone at the round window membrane and in the IE fluids.
Otonomy has demonstrated that IT injection of OTO-104 is associated with predictable ie fluid exposure in two animal species. Most recently Otonomy has shown in a
preclinical noise-induced hearing loss (nihl) model that oto-104 has dose-dependent efficacy (both pre- and post-trauma), and is superior to the protection afforded by steroid solution. A complete FDA-regulated preclinical toxicology program was conducted, which allowed Otonomy to move forward with the first clinical test of oto-104 in Mèniére’s disease patients.
MUSC is currently recruiting patients to participate in a randomized, double-blind, placebo-controlled trial of it injections of oto-104 in Mèniére’s disease. In this study
two different doses of oto-104 will be assessed for safety, as well as to determine whether oto-104 can provide mèniére’s disease subjects with a clinically meaningful effect of enhanced vertigo control. A description of this trial can be found at the following link:http://clinicaltrials.gov/ct2/show/nct01084525?term=meniere%27s+disease&rank=5
Intratympanic injection of OTO-104.
ResearchClinicalinvestigating a novel Therapy With
intratympanic injection in Ménière’s Disease
What is a Certified Physician Investigator (CPI)?Certified Physician Investigator (CPI™) status is
awarded through the Academy of Pharmaceutical Physicians and Investigators (APPI). APPI offers the CPI™ examination to qualified physician investigators, which measures a candidate’s general skills and knowledge needed to perform this role effectively.
CPI certification signifies a physician’s ability to conduct clinical trials in accordance with the appropriate ethical, medical, scientific, legal, and regulatory standards. Major pharmaceutical
companies and Clinical Research Offices (CRO’s) now encourage CPI certification as it benefits the public, healthcare professionals and the healthcare industry by indentifying standards for practice. There are currently 1,200 physicians with CPI certification in the United States.
Shaun A. Nguyen, MD, CPI, is the first certified physician investigator at MUSC. He has been involved in biomedical and clinical research since 2001 and has served as PI and Co-I on more than 50 clinical trials.

musc • discovery, understanding, healing since 1824 http://ENT.musc.edu 3
EducationContinuing 10th Annual Charleston Magnolia Conference
the 2010 magnolia conference was held June 4-5, 2010. our distinguished guest speakers were Herman A. Jenkins, MD, Richard J. Smith, MD, Jonathan M. Sykes, MD, and Robert H. Miller, MD. Attendees from around the country enjoyed presentations and round table lunch discussions covering the breadth of our specialty. The weather was ideal, providing the perfect setting for enjoying historic Charleston, the beaches, golf, and the Spoleto Festival USA.
i hope you will be able to join us June 3-4, 2011 for our 11th Annual Magnolia Conference. Our distinguished guest speakers will be Samuel H. Selesnick, MD, Douglas A. Girod,
MD and Timothy L. Smith, MD. We promise another several days of exceptional
education and recreation. Please visit our website at ent.musc.edu for more information.
Paul R. Lambert, MDProfessor and Chair
3rd Annual Charleston salivary Gland Ultrasonography & Endoscopy CourseThe Department hosted the third annual Charleston Salivary Gland Ultrasonography and
Endoscopy course at the Charleston Renaissance Hotel on November 5-6th, 2010, under the direction of M. Boyd Gillespie, M.D. A total of 23 otolaryngologists representing 13 states and 6 academic programs came to Charleston to learn the latest in the management of obstructive salivary disorders. Guest professors
included Dr. Michael Koch from the University of Erlangen-Nürnberg, Germany; Dr. Barry Schaitkin from the University of Pittsburg;
and Dr. Robert Sofferman from the University of Vermont. Participants enjoyed informative lectures along with hands-on laboratory experience with salivary ultrasonography and endoscopy followed by an authentic SC lowcountry oyster roast and shrimp boil on a lovely autumn evening.
25th Annual F. Johnson Putney Lectureship
Terry A. Day, M.D. directed the 25th Annual F. Johnson Putney Lecturship on November 6, 2010, held in conjuction with the Charleston Salivary Gland Ultrasonography and Endoscopy Course. The free half day session of lectures on head and neck cancers featured guest professor Dennis H. Kraus, M.D. from the Memorial Sloan Kettering Cancer Center, New York.
Join us in Charleston October 22-23, 2011 when the Putney Lectureship will be part of the HNO Summit to Sea co-hosted by the University of Utah, with guest professor Henry T. Hoffman, M.D., University of Iowa.

Salivary gland blockage can result from multiple causes including salivary stones, scar
tissue, allergic disorders, dehydration, side-effects of certain medications, auto-immune diseases, and tumors. Patients undergoing radioiodine treatment for thyroid cancer are especially prone to salivary gland obstruction due to concentration of radioiodine within the gland parenchyma. The most common cause of salivary obstruction is salivary stones (sialoliths). Approximately 90% of stones occur in the submandibular glands, and 10% in the parotid glands. The stones are thought to form from mucous sludge which becomes mineralized with deposits of calcium hydroxylapatite. Although plain film radiography or computed tomography may be helpful, up to 60% of stonesare radiolucent or too small to be
seen by these radiographic modalities. Ultrasonography is a promising office-based method that may be able identify small stones and dilated salivary ducts not observed with conventional radiography.
Traditional treatment of salivary gland obstruction has focused on methods to increase the flow of saliva such as drinking more water, sucking on sour candies or lemons, applying warm compresses, and massaging the swollen gland. If these measures fail, many patients had to decide whether or not to undergo major surgery to
remove the gland in order to relieve the symptoms. Pathologic studies, however, have found that in most cases the gland is relatively normal except for the obstructive site.
4 http://ENT.musc.edu musc • discovery, understanding, healing since 1824
UpdateClinicalsalivary Endoscopy: A Minimally-invasive
Option for salivary Gland stones and Blockage
Figure 1. View of salivary stone within the submandibular duct.
Figure 2. Geographic distribution of patients seeking care for salivary blockage at MUSC.
Alabama ............................ 3Arkansa ............................. 1Arizona .............................. 1Florida ............................... 6Georgia ............................. 5North Carolina .................. 33Maryland ........................... 4New Mexico ....................... 1South Carolina .................. 72Tennessee ......................... 2Virginia ............................. 2
2
42
3
6
11 1 7233
5

Salivary endoscopy was developed in Europe over the last decade in an effort to offer patients with salivary obstruction a minimally-invasive, gland-preserving approach to salivary gland blockage. The technique uses semi-rigid, ultra-thin scopes (0.8 mm to 1.6 mm diameter) that are inserted into the gland’s natural opening in the mouth in order to visualize the cause of the obstruction (Figure 1). Using specially designed micro-instruments, stones and scar tissue can be removed in order to relieve the blockage. The scope can also cleanse the glands with an irrigation of saline solution and steroids. The procedure is performed under local anesthesia or light general anesthesia thereby allowing the patient to go home immediately following the procedure.
M. Boyd Gillespie, M.D., began performing salivary endoscopy in Charleston in 2008 after receiving training in Germany from the developers of the technology. Since that time he has performed the procedure on 130 patients representing 11 states (Figure 2). In late 2009, Dr. Gillespie reviewed the results of the first 51 patients treated with salivary endoscopy at MUSC which will be published shortly in the journal Head and Neck. Indications for the procedure in the first 51 patients included salivary swelling of unclear cause (49%); salivary stone (47%); and sjögren’s syndrome (4%). gland preservation was possible in 78% of patients, and 84% of patients with gland preservation demonstrate significant symptomatic improvement. Of the 27 patients with stones, 20 patients were able to have stones extracted with endoscopic methods, whereas 7 patients required gland
excision. Patients were more likely to require gland excision if they had large stones (mean diameter 9.3 mm) impacted within the body of the submandibular gland.
In a presentation at the annual meeting of the American Head and Neck Society in April 2010, MUSC’s results for the treatment of salivary stones were compared to those of the major European salivary center at Erlangen-Nürnberg, Germany (Table 1). Rates of gland excision were significantly higher in the U.S. largely due to the treatment of larger stones without access to lithotripsy, and the desire of U.S. patients to have their problem resolved quickly. Otherwise, overall salivary symptom control was comparable between MUSC and Erlangen (Table 2).
Dr. Gillespie has trained 50 U.S. surgeons in techniques of salivary endoscopy, and has been a guest professor at the Erlangen Salivary Course in 2009 and 2011, and will be guest speaker at the 2011 Triological Meeting in Chicago. Additional hands-on training in salivary endoscopy will be held at MUSC on October 21-22, 2011 during the Head and Neck Oncology Summit Meeting in Charleston.
musc • discovery, understanding, healing since 1824 http://ENT.musc.edu 5
Table 1. Comparison of treatment method of salivary stones between German and U.S. centers.
Table 2. Comparison of gland preserving treatment outcomes between German and U.S. centers.
Treatment Type % (N)
Erlangen-Nürmberg (N=150)
MUSC (N=32)
P value
Endoscopic Extraction Alone
17% (26) 25% (8) 0.447
Endoscopic-assisted Transoral Incision
52% (78) 53% (17) 0.908
Lithotripsy w/wo Endoscopy
31% (45) 0 % (0) 0.0008
Gland Excision 0 % (0) 22% (7) 0.0001
Outcome
Erlangen-Nürmberg (N=318)
MUSC (N=63)
P Value
Gland Preservation Rate
98% (313) 81% (51) 0.0001
Symptom Control with Intact Gland at Last Follow-up
85% (267/313) 84% (43/51) 0.8537
Mean Follow-up Time (s.d.)
26 months (11.3)
9.1 months (5.4)
0.0001
Visit our website for information about our CME course offerings:
ENT.musc.edu
6 http://ENT.musc.edu musc • discovery, understanding, healing since 1824
RealmResearch
Age-related hearing loss is a difficult problem to study because many factors can produce
hearing loss in older persons, such as the accumulated effects of exposure to noise, ototoxic drugs, or certain diseases. Animal models of age-related hearing loss have been developed to control the most pertinent variables for systematic studies of pathology, physiology, and chemistry at the cellular and molecular levels. One goal of the Hearing Research Program is to use this information to understand
potential mechanisms of hearing loss in older humans, where confounding environmental effects cannot be controlled. In our studies, gerbils are raised throughout their lifespan (3+ years) under experimental conditions wherein environmental variables (temperature, humidity, air quality, noise), diet, and drugs are strictly controlled. Thus, pathological changes and hearing loss in these “quiet-aged” gerbils relate only to the aging process.
Gerbils raised under these conditions show age-related declines in auditory function, including a flat 10-40 dB hearing loss in the lower frequencies with thresholds at higher frequencies gradually increasing to ~60 dB, preservation of (but reduced) cochlear nonlinearities (such as otoacoustic emissions), and primary degeneration of spiral ganglion neurons. Absent are age-related losses of outer and inner hair cells, except scattered losses in the most apical and basal regions of
the cochlea. Thus, gerbils raised in quiet exhibit all the characteristics of metabolic presbyacusis.
A second source of pathology seen in quiet-aged gerbils is primary degeneration of about 10-15% of the spiral ganglion neurons across the entire cochlear duct, which occurs in the presence of an intact population of inner hair cells (Mills et al., 2006). Age-related neural degeneration is correlated with strial degeneration and the resulting loss of the endocochlear potential or EP (Lang
et al., 2010), suggesting a role for the EP in maintaining synchronized neural firing and viability. Among the most prominent changes in the physiological properties of quiet-aged gerbils are decreases in the slope of the input-output function of the compound action potential (CAP). With little change in neural thresholds (e.g., amplitude of responses to lower level signals), a reduction in CAP amplitudes with higher level signals may relate to poorly synchronized activity of individual nerve fibers. In quiet-aged gerbils, these are characteristics of neural presbyacusis.
Neural presbyacusis is the least understood of the subcategories of age-related hearing loss, because the mechanisms underlying neural loss and shrinkage with age have not been determined. Findings from quiet-aged gerbils would predict age-related reductions in auditory functions that are dependent on synchronous neural responses, such as temporal information coded by neural phase
locking. However, the predicted effects of neural presbyacusis have not been confirmed in aging human subjects, specifically those with near-normal auditory detection thresholds. Without knowledge of its functional effects in older humans, the clinical significance of neural presbyacusis remains unknown.
In contrast to changes in the inner ear due to pure aging, threshold elevations resulting from sensory cell loss are associated with a steeply sloping high-frequency hearing loss, loss of cochlear nonlinearities (otoacoustic emissions), broadened tuning, and secondary neural degeneration associated with injury to inner hair cells (sensory presbyacusis). These changes are most often seen following exposure to excessive noise or ototoxic drugs, rather than as a result of aging.
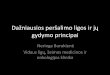
What is the evidence that metabolic presbyacusis underlies the characteristic gradually sloping audiogram of aging gerbils (and humans)? in Figure 1, threshold shifts in the CAP of the
Judy r. Dubno, richard A. schmiedt, Mark A. Eckert, Fu-shing Lee, Lois J. Matthews
Figure 1. Age-related hearing loss in two groups of older human subjects with no history of noise exposure are compared to threshold shifts of the compound action potential in laboratory animals where the endocochlear potential (EP) has been re-duced by the application of furosemide (Schmiedt et al., 2002).
In the absence of confounding factors such as noise and drug exposures, audiometric phenotypes are consistent with the view of age-related hearing loss as a metabolic, vascular, neural disorder rather than a sensory disorder.
new insights onAge-related Hearing Loss

musc • discovery, understanding, healing since 1824 http://ENT.musc.edu 7
auditory nerve due to furosemide-induced changes in the EP are compared to hearing loss in non-noise exposed older adults from the database of the MUSC longitudinal study of age-related hearing loss (Mills et al., 2006) and a sample reported by Jerger et al. (1993). The correspondence between threshold shifts produced in gerbil and hearing loss of aging humans suggests a common mechanism, namely a reduction in the EP that effectively reduces the voltage available to the cochlear amplifier (Schmiedt et al., 2002). Thus, our hypothesis is that age-related hearing loss as shown by the audiogram can be best explained by age-related pathology of the cochlear lateral wall with attendant changes in potassium recycling mechanisms and reductions in the EP, which deprive the cochlear amplifier of its essential power supply. This hypothesis predicts that age-related declines in hearing as indicated by the audiogram are largely explained by pathology of the auditory periphery.
As a further test of this hypothesis, we examined the extent to which unique and consistent patterns of “audiometric phenotypes” can be identified from pure-tone audiograms in a large sample of older adults. Schematic boundaries of audiograms were defined based on four hypothesized conditions of cochlear pathology obtained from results from animal models. The four audiometric phenotypes are: (1) older normal; (2) metabolic presbyacusis; (3) sensory presbyacusis; and (4) a mixed phenotype of metabolic + sensory presbyacusis.
Next, audiograms of research participants (age >50) stored in the MUSC database were searched for “exemplars” (best examples) of these phenotypes, without knowledge of demographic information (n=1,728). audiograms from 374 ears were identified as exemplars of one of the four phenotypes; the mean audiogram for each phenotype is shown in Figure 2. Audiograms of the older normal phenotype (gray) show generally normal hearing, with a “pre-metabolic” characteristic in the higher frequencies. Similar to Figure 1, audiograms of the metabolic phenotype (green) have a flat loss of ~20 dB in the lower frequencies and a gradually sloping loss in the higher frequencies. Audiograms of the sensory phenotype (red) have generally
normal hearing in the lower frequencies and a steeply sloping loss in the higher frequencies. Audiograms with the mixed phenotype of metabolic+sensory (blue) have characteristics of metabolic presbyacusis in the lower frequencies and sensory presbyacusis in the higher frequencies.
To provide external validity of the four phenotypes, distributions of age, gender, and noise exposure history were determined. As predicted, subjects whose audiograms were exemplars of the older normal phenotype tended to be younger (among older adults), mostly female, with negative noise histories. Subjects in the metabolic phenotype were generally older, predominantly female, with negative noise histories. Subjects in the sensory phenotype were younger, mostly male, with positive noise histories. Subjects in the mixed phenotype were older, predominantly male, with positive noise histories.
As an additional test of validity and reliability, phenotypes of the exemplar audiograms were predicted using statistical methods (e.g., machine learning, quadratic discriminant analysis). These tools were used to develop classifiers, which estimate the probability that newly obtained audiograms exhibit one of the four phenotypes. The automated procedures classified the exemplars with 88-91% accuracy, with a majority of the misclassifications occurring between the metabolic and mixed phenotypes. Finally, phenotypes of non-exemplar audiograms (n=1,354) were predicted using the same automated methods; classification was determined by the highest probability estimate. Within each phenotype, audiogram shapes
of exemplar and non-exemplar cases were generally similar across frequency. Non-exemplar cases were consistent with exemplar cases with respect to their distributions of ages, genders, and noise histories.
Subsequently, information from the MUSC database will further define the phenotypes by identifying characteristics beyond the audiogram that differentiate subjects, including otoacoustic emissions, auditory brainstem responses, longitudinal changes in thresholds and speech recognition (Lee et al., 2005; Dubno et al., 2008); chronic medical or other health conditions; clinical blood chemistries; and genetic variations.
In summary, results to date suggest that animal models can be used to predict human cochlear pathology using audiograms and more advanced measures of auditory function. Human audiometric phenotypes appear consistent with predictions from animal findings associated with sensory and strial pathology. Future studies will explore if this approach may be applied to understanding neural presybacusis. Finally, in the absence of confounding factors such as noise and drug exposures, audiometric phenotypes are consistent with the view of age-related hearing loss as a metabolic, vascular, neural disorder rather than a sensory disorder.
rEFErEnCEsDubno J, Lee F, Matthews L, Ahlstrom J, Horwitz A, Mills J (2008). Longitudinal changes in speech recognition in older persons. J acoust soc am 123, 462-475.
Jerger J, Chmiel R, Stach B, Spretjnak M (1993). Gender affects audiometric shape in presbyacusis. J am acad audiol 4, 42-49.
Lang H, Jyothi V, Smythe NM, Dubno JR, Schulte BA, Schmiedt RA (2010). Chronic reduction of endocochlear potential reduces auditory nerve activity: Further confirmation of an animal model of metabolic presbyacusis. J Assoc Res Otolaryngol 11, 419-434.
Lee F, Matthews L, Dubno J, Mills J (2005). Longitudinal study of pure-tone thresholds in older persons. Ear Hear 26, 1-11.
Mills J, Schmiedt R, Schulte B, Dubno J (2006). Age-related hearing loss: A loss of voltage, not hair cells. Seminars in Hearing 27, 228-236.
Schmiedt R, Lang H, Okamura H, Schulte B (2002). Effects of furosemide applied chronically to the round window: a model of metabolic presbycusis. J neurosci 22, 9643-9650.
Figure 2. Mean audiograms from 374 ears from the MUSC database identified as exemplars (best examples) of one of four audiometric phenotypes.

The MUSC Department of Otolaryngology- Head & Neck Surgery hosted the annual resident and fellow farewell banquet at the Charleston Yacht Club
on June 19th, 2010. This was the first year where the department graduated three residents who all pursued advanced fellowship training. Charley Coffey, MD, finished his MUSC residency with 7 peer-reviewed publications, including innovative work on nerve growth factors in chronic rhinosinusitis under the mentorship of Dr. Rodney Schlosser. Dr. Coffey began a fellowship in head and neck oncologic surgery at the M.D. Anderson Cancer Center and plans to pursue an academic position once his training is complete.
Two of the graduating residents pursued fellowship training in plastic and reconstructive surgery. Dr. Joshua Farrar joined the MUSC Division of Plastic Surgery as a fellow in preparation for a career in general plastics with an emphasis on craniofacial disorders. Dr. Farrar, who has been active in medical missions throughout medical school and residency, hopes that his training will allow him to continue to serve many of the world’s most needy patients. Dr. Jonathan Kulbersh accepted a fellowship in facial plastics and reconstructive surgery at the Cedars-Sinai Medical
Center in Los Angeles under the mentorship of Drs. Paul Nassif and Babak Azzizadeh who he brought back to MUSC for a facial plastics workshop for the residents organized by course director Dr. Krishna Patel. Dr. Kulbersh completed residency with three publications which included a study demonstrating the promising effects of vitamin D on the immune system of head and neck cancer patients. Dr. Kulbersh hopes to start a busy facial-plastics practice in an urban center in the southeast once his training is complete.
The event also honored the department’s two fellows who completed intense year-long advanced training in their areas of sub-specialty. Head and neck oncology and microvascular fellow Dr. Tanya Fancy
was known for her excellent surgical skills, calm demeanor in pressure situations, and amazing abilities to balance care for her 1-year old daughter while working long and hard hours. Following fellowship, Dr. Fancy joined the faculty at West Virginia University where her husband, Riaz is a general surgical oncologist. Rhinology and sinus fellow Dr. Ben Bleier was an already well-trained sinus surgeon from the University of Pennsylvania who came to MUSC to receive additional training in advanced endoscopic skull base surgery under the tutelage of Dr. Rodney Schlosser. While at MUSC, Dr. Bleier continued research he had started in Pennsylvania on the use of laser-activated skull-base sealants to prevent post-operative cerebral spinal fluid leaks. Following his year in Charleston, Dr. Bleier accepted a faculty position in rhinology and sinus surgery at Harvard.
In awarding the annual teaching award, the residents decided to honor two faculty members who had spent long hours in personalized learning sessions and providing excellent lectures to the residents. Drs. Krishna Patel and Eric Lentsch both received the Faculty Teaching Award.Dr. Patel has greatly improved resident exposure to academic facial plastic surgery, whereas Dr. Lentsch is known for keeping residents sharp with his weekly head and neck “epimps.”
8 http://ENT.musc.edu musc • discovery, understanding, healing since 1824
Residents & FellowsFarewell
Drs. Joshua Farrar, Charley Coffey, Paul Lambert, and Jonathan Kulbersh
Drs. Eric Lentsch, Boyd Gillespie, Tanya and Riaz Fancy, Joshua Hornig, Judith Skoner, and Terry Day
Drs. Rodney Schlosser and Benjamin Bleier Drs. Joshua Farrar, Eric Lentsch, Charley Coffey, and Jonathan Kulbersh
musc • discovery, understanding, healing since 1824 http://ENT.musc.edu 9
to MUSC!Welcome
Trinitia Cannon, MDMD: University of RochesterResidency: University of North Carolina, Chapel HIllSpecial Interests: Head and neck surgical oncology, microvascular reconstruction
Wayne Cardoni, DODO: Philadelphia College of Osteopathic MedicineResidency: National Naval Medical Center, Bethesda, MDSpecial Interests: Head and neck surgical oncology, microvascular reconstruction
Jeremy Meier, MDMD: Saint Louis UniversityResidency: University of California Davis Medical CenterSpecial Interests: airway reconstruction, cleft lip and palate, pediatric sinonasal disorders, pediatric otology
Eric W. Wang, MDMD: Baylor College of MedicineResidency: Washington University, St. LouisSpecial Interests: complicated adult and pediatric sinus surgery, revision sinus surgeries, cerebrospinal fluid leak repair, sinonasal and cranial base tumors.
2010-11 FellowsPGY2 Residents
Jessica L. Gullung, MD, is a native of Hattiesburg, Mississippi and a graduate of Mississippi State University where she earned a Bachelor of Science degree in Biochemistry and Molecular Biology with distinction. She attended the University of Mississippi Medical Center and was a recipient of the John Millington Academic Excellence Scholarship and the Gold Humanism in Medicine Award, and a member of the AOA medical honor society. After graduating magna cum laude, she decided to venture to the beautiful state of South Carolina and is thoroughly enjoying her Otolaryngology residency. Jessica is a professional harpist and enjoys cooking, traveling, and running. She is currently busy planning her wedding to Richard Lee, a South Carolina native and accountant at MUSC.
Samuel L. Oyer, MD, originally hails from Saskatchewan, Canada, but grew up primarily in Middlebury, Indiana where he met and married his high school sweetheart, Mary. He attended Indiana University earning a Bachelor of Arts in Chemistry with minors in Biology, Mathematics, and Business. Sam completed medical school at the Indiana University School of Medicine and was a member of the AOA honor society. Continuing on his southern migration, he entered the Otolaryngology residency program at MUSC in Charleston, South Carolina where his wife also works as a nurse. While not at work Sam enjoys playing basketball, guitar and piano, and exploring the beautiful scenery around Charleston.
Gregg W. Schmedes, MD, was born and raised in Austin, TX. He majored in electrical engineering at the University of Texas-Austin, where he was a member of the track & field team. After college, Gregg worked for one year in Austin as a computer engineer and married Kelly Wilson. They then moved to Lubbock, TX where Gregg graduated from medical school at Texas Tech University. There he served as senior class president and was a member of Alpha Omega Alpha. Outside of the medical field, Gregg enjoys running, hiking, and spending time with his wife and their new baby, Isaiah John.
Future ENT leaders: Drs. Gregg Schmedes, Jessica Gullung, and Samuel Oyer
MUSC offers otolaryngology fellowships in Head & Neck Oncologic and Reconstructive Surgery, Rhinology and Endoscopic Sinus/Skull Base Surgery, and Pediatric Otolaryngology. In addition to an extensive surgical experience, fellows benefit from a multidisciplinary approach by participating in outpatient clinics, rounds, and didactic conferences.
To learn more about our residency and fellowhip programs please visit our website at ENT.musc.edu

otology & neurotologyPaul R. Lambert, M.D.Professor and ChairmanDirector, Otology-NeurotolgyM.D.: Duke UniversityResidency: UCLA Medical Center
Fellowship: House Ear Institute, Los Angeles
Ted A. Meyer, M.D., Ph.D.Assistant ProfessorDirector, Cochlear Implant ProgramM.D.: University of IllinoisPh.D.: University of IllinoisResidency: Indiana Univ.
Fellowship: University of Iowa
10 http://ENT.musc.edu musc • discovery, understanding, healing since 1824
PediatriC otolaryngology David R. White. M.D.Associate ProfessorDirector, Pediatric OtolaryngologyDirector, MUSC Airway and Aspiration Center for Children
M.D.: MUSCResidency: University of North Carolina, Chapel HillFellowship: Cincinnati Children’s Hospital
Christopher M. Discolo, M.D.Assistant ProfessorM.D.: State University of New York Health Science Center at BrooklynResidency: Cleveland Clinic
Fellowship: University of Minnesota / Pediatric ENT Associates
Carissa Carie, PNPPediatric Nurse PractitionerPNP: MUSC
Faculty Otolaryngology - Head & Neck Surgery
maxillofaCial ProsthodontiCs
Betsy K. Davis, D.M.D., M.S.Associate ProfessorDirector, Division of Maxillofacial ProsthodonticsD.M.D.: MUSC
Residency: University of IowaFellowship: M.D. Anderson ; UCLA
Terry A. Day, M.D.Professor and DirectorMUSC Head and Neck Tumor ProgramM.D.: University of Oklahoma
Residency: LSU-Shreveport Fellowship: University of California, Davis
M. Boyd Gillespie, M.D., M.S.Associate ProfessorDirector, MUSC Snoring ClinicM.D.: Johns HopkinsResidency: Johns Hopkins
Fellowship: Johns Hopkins
Joshua D. Hornig, M.D., FRCS(C)Assistant ProfessorDirector, Microvascular Surgery and Functional OutcomesM.D.: University of Alberta
Residency: University of AlbertaFellowship: MUSC
Eric J.Lentsch, M.D.Assistant ProfessorM.D.: University of LouisvilleResidency: University of LouisvilleFellowship: M.D. Anderson
Roy B. Sessions, M.D.ProfessorM.D.: Louisiana State University, New OrleansResidency: Washington University School of Medicine, St. Louis
Mary Beth Chalk, MSN, RN, APRN-BCNurse PractitionerMSN: MUSC
Holly L. Drechsler, PA-CPhysician AssistantMSPAS: MUSC
Ashley Laursen, BSN, RNRegistered Nurse, Program CoordinatorBSN: MUSC
Jennifer R. Page, RN, MSN, NP-CNurse PractitionerMSN: MUSC
head & neCk onCology
faCial PlastiC & reConstruCtive surgery
Krishna G. Patel, M.D., Ph.D.Assistant ProfessorDirector, FPRS M.D./Ph.D. : Medical College of GeorgiaResidency: University of
North Carolina, Chapel HillFellowship: University of California-Davis
Judith M. Skoner, M.D.Assistant ProfessorM.D.: University of South CarolinaResidency: MUSCFellowship: Oregon Health and Science University

general otolaryngology& allergy
Mark J. Hoy, M.D.Assistant ProfessorDirector, General Otolaryngology & AllergyM.D.: Temple UniversityResidency: University of Lousiville
Christina J. Areheart, PA-CPhysician AssistantMSPAS: MUSC
musc • discovery, understanding, healing since 1824 http://ENT.musc.edu 11
audiology
Kimberly A. Orr, M.A.Director, AudiologyM.A.: Ohio State University
Abby C. Connell, AuD InstructorAuD: A.T. Still UniversityMEd: University of Georgia
Laura Droege, AuDInstructorAuD: A.T. Still UniversityMA: Northern Illinois University
Meredith Edgerton, AuDInstructorAuD: University of North Carolina, Chapel Hill
Elizabeth Poth, MSInstructor AuD: University of North Carolina, Chapel Hill
Christine Strange, MAInstructorMA: SUNY Plattsburgh
evelyn trammell institute for voiCe and swallowing
Lucinda A. Halstead, M.D.Associate ProfessorMedical Director, ETIVS M.D.: George Washington UniversityResidency: New England Medical Center, Boston
Bonnie Martin-Harris, Ph.D., CCC-SLP, BRS-SProfessorDirector, ETIVSM.S.: Purdue UniversityPh.D.: Northwestern University
Research
Amy R. Horwitz, Ph.D.Assistant ProfessorPh.D.: Syracuse University
Fu-Shing Lee, Ph.D.Assistant ProfessorPh.D.: MUSC
Lois J. Matthews, M.S.InstructorMUSC Hearing Research ProgramM.S.: Purdue University
Jayne B. Ahlstrom, M.S.InstructorM.S.: Vanderbilt University
Mark A. Eckert, Ph.D.Associate ProfessorMUSC Hearing Research ProgramPh.D.: University of Florida
Kelly C. Harris, Ph.D.Assistant ProfessorPh.D.: University at Buffalo
Judy R. Dubno, Ph.D.Professor, Director, MUSC Hearing Research ProgramPh.D.: City University of New York
Shaun A. Nguyen, M.D., M.A., CPIAssistant ProfessorDirector, Clinical ResearchMD & Residency: University College LondonFellowship: MUSC
M. Rita I. Young, Ph.D.ProfessorHead and Neck ResearchAssociate Director for Research, Ralph H. Johnson VA Medical Center
rhinology & sinus surgeryRodney J. Schlosser, M.D.ProfessorDirector, Nasal and Sinus CenterM.D.: Mayo ClinicResidency: University of Virginia
Fellowship: University of Pennsylvania
Brittany Crosby, PA-CPhysician AssistantMSPAS: MUSC

JAnUArY - JUnE 2011
The 2nd Annual MUsC Pediatric Audiology Conference: Current Perspectives in Cochlear implantationMarch 11, 2011For all providers (audiologists, SLPs, physicians, etc.) involved in the care of pediatric patients with cochlear implants.Guest speaker: Dr. Anu Sharma (Colorado)
sinus CoursesSinus Masters: March 19 - 20, 2011Southern States Rhinology Course: March 31 - April 2, 2011Lectures & hands on labs designed to provide a comprehensive update on the medical and surgical practice of rhinology.
Temporal Bone Dissection CourseMarch 25 - 26, 2011Lectures and hands on labs focused on procedures for chronic ear disease. Guest speaker: Dr. Stephanie Moody-Antonio (Virginia)
Emerging Controversies in the Management of Thyroid and Parathyroid DiseaseApril 8 - 9, 2011Two half-day sessions for ENT and endocrine surgeons.Guest speakers: Drs. Jeffrey M. Bumpous (Kentucky), David J. Terris (Georgia)
11th Annual Charleston Magnolia ConferenceJune 3 - 4, 2011Two half-day sessions covering the broad spectrum of Otolaryngology - Head & Neck Surgery.Guest speakers: Drs. Sam Selsnick (Cornell-Columbia), Doug Girod (Kansas), Tim Smith (Oregon).
For registration or more information
Jenn oblad, phone: 843.876.0943, email: [email protected]: ent.musc.edu
Department of Otolaryngology- Head & Neck Surgery
135 Rutledge Avenue, MSC 550charleston, sc 29425-5500
Phone 843-792-8299
Website: ENT.musc.edu
SPONSORS
CME EventsUpcoming
Paul R. Lambert, M.D.department chair, editor-in-chief
M. Boyd Gillespie, M.D.executive editor
Alison Padlan-Gillettecreative & production manager
©2011 muSc otolaryngology - hnS