Embed Size (px)
Citation preview

Click icon to add picture
THYR
OIDECTO
MY
Kaidy
Wat
erm
an &
Der
ek W
oodru
ff
THE THYROID
The thyroid sits anteriorly to the trachea and the esophagus
Contains two types of hormone-producing cells
Follicular Cells: produce thyroxine and triiodothyronine
Parafollicular Cells: produce calcitonin
The adult thyroid weighs anywhere from 12 to 25 grams
“H” shaped
The organ shrinks as you age
Two lobes
THE PARATHYROIDS
Range from 2 to 6
Small, flat, oval structures that lie on the dorsal side of the thyroid gland
Produce parathormone which maintains the normal relationship between blood and skeletal calcium
Removal of these glands would result in tetany and death
Care must be taken not to damage these glands during a thyroidectomy
PATHOPHYSIOLOGY OF THE THYROID AND PARATHYROIDS Hyperthyroidism (thyrotoxicosis): when the thyroid gland
produces too much thyroxine hormone Symptoms: nervousness, tachycardia, sweating, tremors,
arrhythmias, hair loss, and dyspnea
Thyroid Carcinoma: cancer of the thyroid Symptoms: hoarseness, may show signs of hyper- or
hypothyroidism depending on tumor type, may be asymptomatic
Hyperparathyroidism: when the parathyroid glands produce an excess of parathyroid hormone
Symptoms: asymptomatic in early stages, skeletal damage
Hypoparathyroidism: parathyroid glands don’t produce enough parathyroid hormone
Symptoms: anxiety, depression, brittle nails, dry skin, thin hair, tetany (a severe complication)
DIAGNOSTIC EXAMS AND PREOPERATIVE TESTING Patient history and physical
Ultrasound
Laryngoscopy
Biopsy
Scans
Serum levels of TSH
ANESTHESIA AND POSITIONING
Anesthesia is general
The patient is positioned in the supine position with neck extended
SKIN PREP, DRAPING, AND INCISION
Skin is prepped from the point of the chin down to the mid-chest of the patient and laterally as far as possible
Wadded absorptive towels are placed bilaterally and the thyroid sheet is used
The incision is symmetrical and transverse following the Langer lines over the thyroid. The size of incision varies, it is generally done two fingerbreadths above the clavicular head.
Basic set, prep set, #10 and #15 blades, sutures, dressings, Bovie, basin set
Thyroid drapes and ¼” Penrose drain
Suction, ESU, roll or thyroid rest for extending the neck
Thyroidectomy set, bipolar forceps with cord, liga clip appliers and clips
SUPPLIES, EQUIPMENT AND INSTRUMENTS
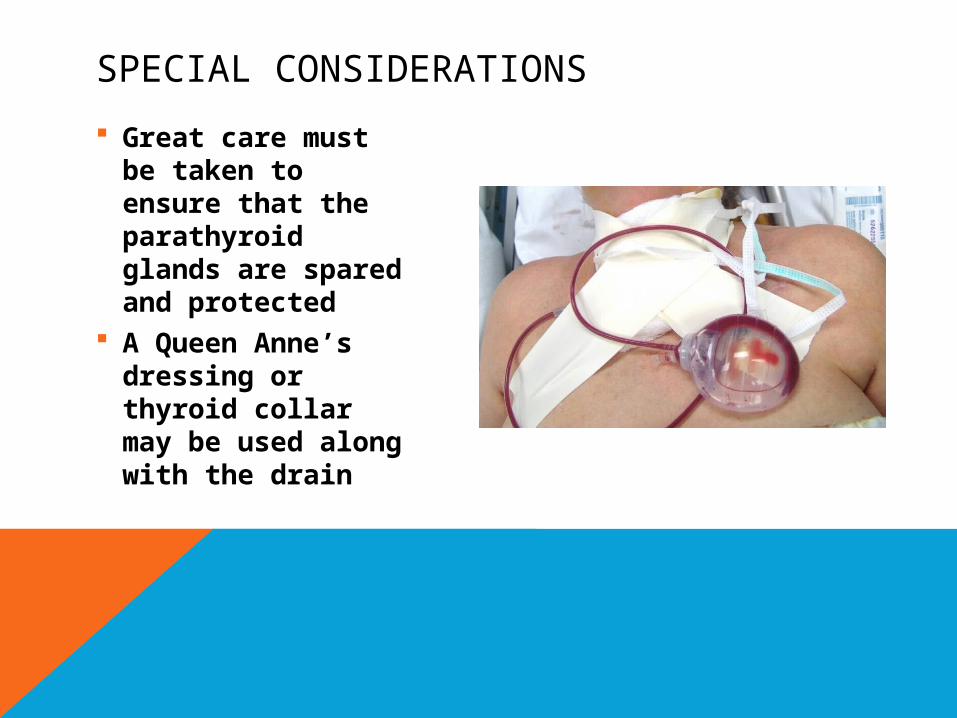
Great care must be taken to ensure that the parathyroid glands are spared and protected
A Queen Anne’s dressing or thyroid collar may be used along with the drain
SPECIAL CONSIDERATIONS

THE P
ROCEDURE
STEP ONE
O P E R A T I V E P R O C E D U R E
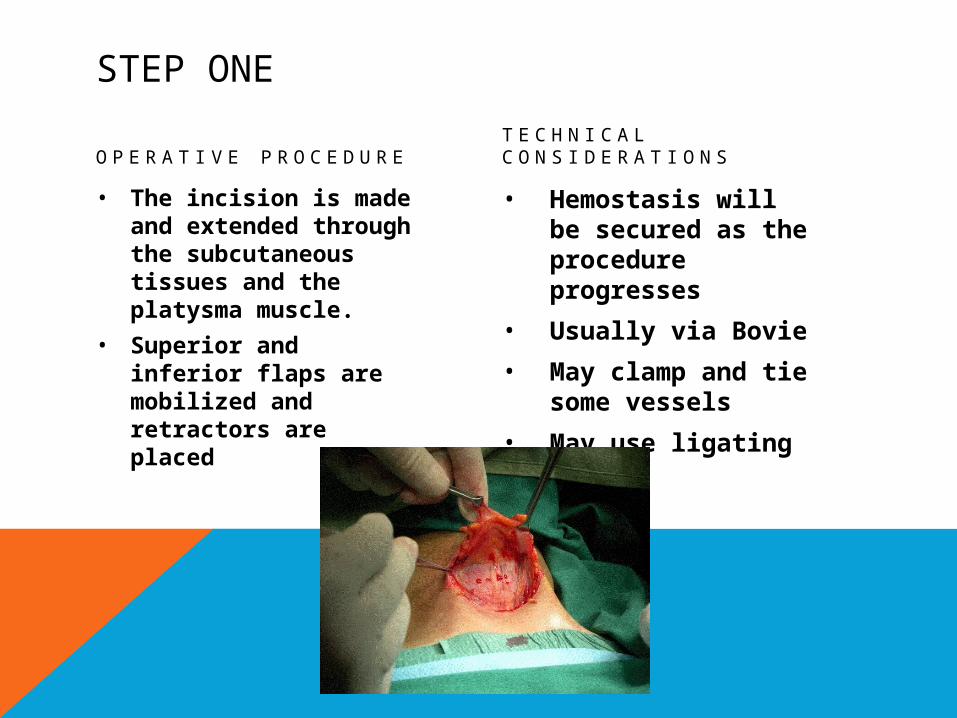
• The incision is made and extended through the subcutaneous tissues and the platysma muscle.
• Superior and inferior flaps are mobilized and retractors are placed
T E C H N I C A L C O N S I D E R A T I O N S
• Hemostasis will be secured as the procedure progresses
• Usually via Bovie
• May clamp and tie some vessels
• May use ligating clips
STEP TWO
O P E R A T I V E P R O C E D U R E
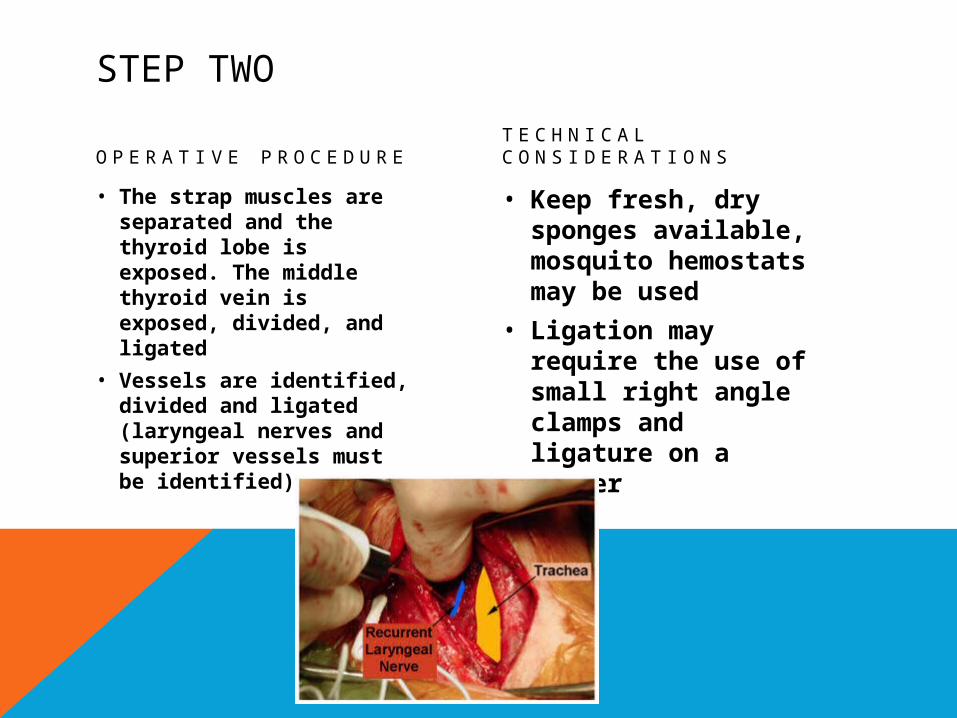
• The strap muscles are separated and the thyroid lobe is exposed. The middle thyroid vein is exposed, divided, and ligated
• Vessels are identified, divided and ligated (laryngeal nerves and superior vessels must be identified)
T E C H N I C A L C O N S I D E R A T I O N S
• Keep fresh, dry sponges available, mosquito hemostats may be used
• Ligation may require the use of small right angle clamps and ligature on a passer
STEP THREE
O P E R A T I V E P R O C E D U R E
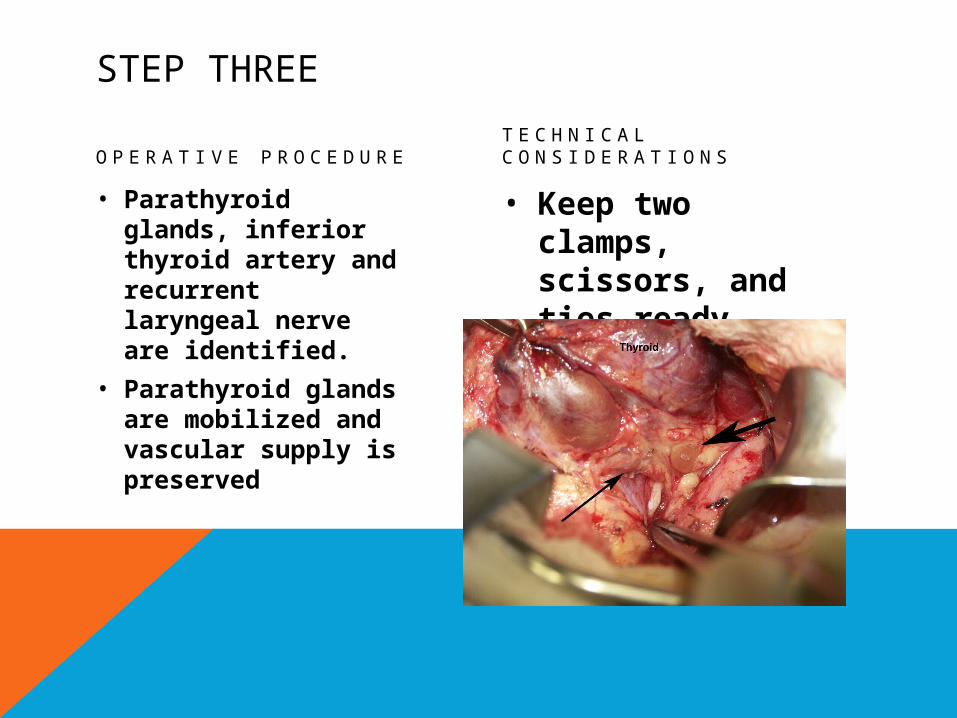
• Parathyroid glands, inferior thyroid artery and recurrent laryngeal nerve are identified.
• Parathyroid glands are mobilized and vascular supply is preserved
T E C H N I C A L C O N S I D E R A T I O N S
• Keep two clamps, scissors, and ties ready
STEP FOUR
O P E R A T I V E P R O C E D U R E
• Branches of the inferior thyroid artery are divided and ligated. The superior connective tissue is divided. Hemostasis is achieved with ESU. (Recurrent nerve must be spared)
T E C H N I C A L C O N S I D E R A T I O N S
• May alternate between sharp dissection, blunt dissection and ESU
STEP FIVE
O P E R A T I V E P R O C E D U R E
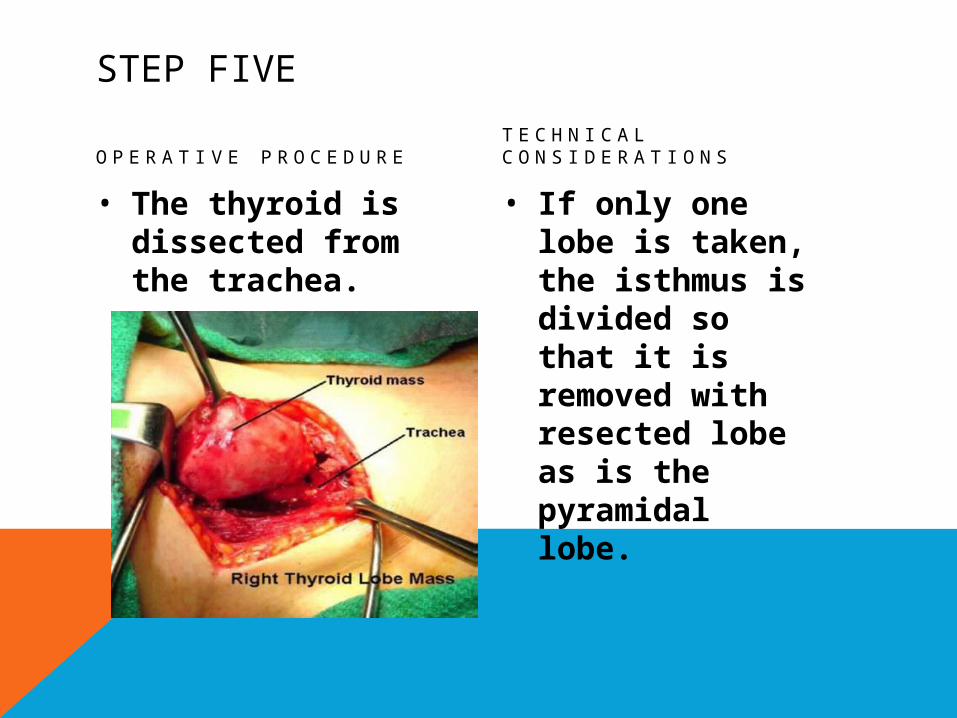
• The thyroid is dissected from the trachea.
T E C H N I C A L C O N S I D E R A T I O N S
• If only one lobe is taken, the isthmus is divided so that it is removed with resected lobe as is the pyramidal lobe.
STEP SIX
O P E R A T I V E P R O C E D U R E
• Hemostasis is achieved after lobe or lobes are removed, a drain may be placed. The wound is closed.
T E C H N I C A L C O N S I D E R A T I O N S
• Sequence is irrigation, placement of wound drain, and closure.
• Initiate count.

POSTO
PERAT
IVE
CONSIDERAT
IONS
POSTOP CONSIDERATIONS
• Immediate postoperative care:• Check voice as soon as possible• Transport to PACU• Tracheotomy tray available
• Prognosis• Return to normal activities• Medications usually required for life
• Complications:• Hemorrhage• Wound Infection• Damage to nearby structures
Click icon to add picture
PEARL O
F W
ISDOM
•Mai
ntain
the
inte
grity
of th
e st
erile
fiel
d until
the
patie
nt
is e
xtubat
ed, b
reat
hing fr
eely, a
nd has
bee
n tran
spor
ted
to th
e PA
CU. Em
ergen
cy tr
acheo
tom
y is
a p
ossi
bility
.