Embed Size (px)
Citation preview

Case Report J. St. Marianna Univ.Vol. 10, pp. 115–121, 2019
Division of Neurology, Department of Internal Medicine, St. Marianna University School of Medicine
Recurrent Cerebral Hemorrhage Associated with Ulcerative Colitis
Toshiyuki Yanagisawa, Heisuke Mizukami, Hisanao Akiyama, and Yasuhiro Hasegawa
(Received for Publication: October 19, 2019)
AbstractUlcerative colitis (UC) is a rare cause of stroke. Most such cases result from cerebral venous thrombosis,
and cerebral vasculitis is one cause of venous thrombus formation. Here, we report a patient with UC who expe‐rienced recurrent cerebral hemorrhage. A 53-year-old Japanese woman with UC presented with sudden onset ofdisorientation and sensory aphasia. Brain computed tomography revealed cerebral hemorrhage in the left tem‐poral lobe. She had a history of UC for two decades but had discontinued her medication. On the fifth hospitalday, another cerebral hemorrhage occurred in the right occipital lobe. After steroid therapy, these abnormal find‐ings on MRI improved within a short time, and she was discharged from hospital with no sequelae. Physiciansshould be alert to cerebral hemorrhage in patients with UC, consider cerebral vasculitis as an etiology, and treatwith steroid therapy for a good outcome.
Key wordsCerebral hemorrhage, ulcerative colitis, neurologic complication
Introduction
Ulcerative colitis (UC) is a diffuse non-specificinflammatory bowel disease that mostly affects themucosa of the large intestine. Neurologic disease isone of the extra-intestinal complications of UC. Al‐though there are some case reports of cerebral sinusthrombosis associated with UC, cerebral hemorrhageis extremely rare. We report a case of UC with recur‐rent cerebral hemorrhage that was treated by intrave‐nous corticosteroids, which resulted in a good out‐come.
Case Presentation
A 53 year-old woman developed sudden onsetof disorientation and sensory aphasia. She had a med‐ical history of UC diagnosed by intestinal biopsy 20years ago and also iron deficiency anemia and osteo‐porosis. She had no risk factors for cerebrovasculardisease and was a non-smoker. There was no familyhistory of cerebrovascular disease or autoimmunedisease. She was treated with steroids for a while andafter that, she took only mesalazine but had discon‐
tinued her medication several years earlier. Colono‐scopy was performed at another hospital threemonths before admission which revealed findings ofinflammation throughout the large intestine, as grade2 in Mayo endoscopic sub-score. The patient reportedthat she often had a lower abdominal pain and re‐peated diarrhea at night. She had up to six bloodybowel movements per day on admission. When shewas talking on the phone with her mother on thenight of hospital admission, the conversation had notmade sense to her mother, who then called the pa‐tient’s husband. When he came home, they could notcommunicate with each other, and she was taken tohospital by ambulance.
On physical examination in the emergency de‐partment, she appeared ill and was febrile with a tem‐perature of 38.1°C. Her blood pressure was 194/105mm Hg, pulse 101/min, with a respiratory rate30/min and O2 saturation of 99% on room air. Sheshowed conjunctival pallor. Her cardiovascular ex‐amination was normal, lungs were clear to ausculta‐tion, and abdominal examination revealed tendernessin the lower abdomen, and she had bloody stool.
97
115

A B C
RtCT FFEFLAIR
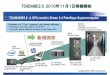
Figure 1. Initial radiographic studies.
Brain CT (A) on the 1st hospital day shows a high-density area sur‐
rounded by a low-density area in the left temporal lobe. This lesion ap‐
peared as a high-intensity area on the brain MRI FLAIR image (B) and as
a low-intensity area on the FFE image (C) and was diagnosed as cerebral
hemorrhage surrounded by edema.
A neurological examination revealed disorienta‐tion with inability to tell date, person, and location. Ahigher cerebral function test revealed naming diffi‐culty, fluent spontaneous speech, and normal repeti‐tion, but her verbal comprehension was impaired.There were no abnormal findings in the cranialnerves, motor system, reflex system, sensory system,coordination system, extrapyramidal system and au‐tonomic nervous system. Her neurological findingswere summarized as sensory aphasia, and her NIHSSscore was 3 points.
Initial laboratory values on admission revealedmicrocytic anemia (white blood cell count 7400/µL,hemoglobin 6.9 g/dL, hematocrit 23.5%, mean cellvolume 66.4 fL and platelet count 41.1×103/µL). Heranemia was considered to derive from apparent or in‐apparent continuous bleeding from colonic mucosa.Her C-reactive protein level was 0.81 mg/dL, and hererythrocyte sedimentation rate (ESR) was 45 mm/h.The coagulation screen showed a prothrombin timeof 100% (normal 75–125%), INR 1.00, activated par‐tial thromboplastin time 23.7 sec (normal 25–35 sec),fibrinogen 483 mg/dL and D-dimer 2.5 µg/mL (nor‐mal <0.5 µg/mL). Blood biochemistry tests were nor‐mal.
Brain computed tomographic (CT) scan revealeda high-density area surrounded by an area of low-density in the left temporal lobe (Figure 1A). Onbrain magnetic resonance imaging (MRI), this lesionshowed high-intensity on fluid-attenuated inversionrecovery (FLAIR) imaging (Figure 1B) and low-in‐
tensity on T2-weighted fast-field echo (FFE) imaging(Figure 1C), which was diagnosed as cerebral hem‐orrhage surrounded by edema.
The patient underwent CT angiography (CTA)and digital subtraction angiography (DSA), which re‐vealed no obvious vascular abnormalities suggestiveof vasculitis, thrombus, infectious aneurysm, arterio‐venous malformation (AVM) or arteriovenous fistula(AVF) (Figure 2).
Concentrated glycerin was administrated as ananti-edema therapy. She received oral mesalazine at adose of 2,250 mg/day simultaneously as her frequentdiarrhea, bloody stool, high fever, tachycardia, ane‐mia and elevated ESR indicated the severity of herUC. Her neurological symptoms improved within ashort time, and she could communicate almost nor‐mally on the 3rd hospital day (HD).
A brain MRI repeated on the 5th HD revealedanother cerebral hemorrhage in the right occipitallobe (Figure 3, red circle). Magnetic resonance spec‐troscopy (MRS) performed on the 13th HD showedno pattern of demyelination or tumor (Figure 3), butthe high-intensity area suggesting brain edema fromthe initial hemorrhage had expanded (Figure 3, redsquare). Magnetic resonance venography showed nofindings of venous thrombosis.
Further laboratory evaluation showed negativeantinuclear, anticardiolipin, other immunological ex‐aminations and tumor markers. Both myeloperoxi‐dase antineutrophil cytoplasmic antibody (MPO-ANCA) and proteinase3 ANCA (PR3-ANCA) were
98
Yanagisawa T Mizukami H et al116

CTA DSA venous phaseDSA arterial phase
Lt Lt Lt
Figure 2. Evaluation of vascular abnormalities.
CTA and DSA revealed no obvious vascular abnormalities suggestive of
vasculitis, thrombus, infectious aneurysm, AVM or AVF.
ChoCho
NAACho
Cr NAA
Rt
Rt
Rt
A
B
C
D
Figure 3. Follow-up MRI studies.
Brain MRI on the 5th hospital day revealed another high-intensity area
at the right occipital lobe (A). This lesion showed as low intensity on
the FFE image (B) and was diagnosed as cerebral hemorrhage (red cir‐
cle). MRS was performed on the 13th hospital day. A region-of-interest
voxel was placed at the initial high-intensity area (red square in C). Ac‐
quisition parameters showed no pattern of demyelination or tumor (D).
The high-intensity area suggestive of brain edema from the initial hem‐
orrhage has expanded.
negative, but perinuclear ANCA (P-ANCA) meas‐ured by the indirect fluorescent antibody method waspositive. Cerebrospinal fluid (CSF) examinationshowed a normal cell count and normal protein butelevation of myelin basic protein to 619 pg/mL. CSFcytology and blood culture were also negative.
We discussed a brain biopsy but did not performit because of the potential risk of neurological deficit.She had painless skin nodules without rash or rednesson her right lower extremities, skin biopsy was per‐formed from two nodules to search for vasculitis butno specific findings were observed. We considered
99
Recurrent cerebral hemorrhage with UC 117

Rt
A
B
C
D
Figure 4. Chronological changes in brain MRI.
A: 13th hospital day, B: 27th hospital day, C: 36th hospital day and D:
61st hospital day.
The high-intensity area in both the left temporal lobe and right occipital
lobe on the FLAIR images improved over time.
her to have cerebral hemorrhage caused by an auto‐immune mechanism due to UC and administered in‐travenous corticosteroids 1000 mg per day from the22nd to 25th HD, followed by oral prednisolone at1 mg/kg/day. After steroid therapy, her brain MRIfindings improved over time, and her neurologicalsymptoms did not worsen. She was discharged on the47th HD with no sequelae.
Oral steroids were gradually reduced, and brainMRI performed on the 61st day from disease onsetrevealed almost no high-intensity findings on FLAIRimaging (Figure 4).
Discussion
Guidelines for inflammatory bowel disease(IBD)1) define IBD as diseases of chronic or remit‐ting/relapsing intestinal inflammation and includeprimary UC and Crohn’s disease. The number of pa‐tients with UC in Japan in 2013 (approximately 100per 100,000 population) was quite low compared tothat in Western countries. UC is a diffuse non-spe‐cific inflammatory disease of unknown cause thatchronically affects the colonic mucosa proximallyfrom the rectum and often forms erosions and/or ul‐cers. It frequently repeats cycles of relapse and remis‐sion during its course and may be accompanied by
extraintestinal complications affecting the joints,skin, eyes and other areas.
In terms of neurological complications, Lossoset al.2) reported that 19 of 638 IBD patients (3%) and9 of 261 UC patients (3.4%) had evidence of neuro‐logical involvement. Among these 9 UC patients, 6had peripheral neuropathy, 2 had a stroke includingsinus vein thrombosis, of which many cases are re‐ported in Japan, and one had myelopathy. In a sys‐tematic search of the literature in the MEDLINE da‐tabase, Scheid and Teich3) reported that there arethree major pathogenic entities causing neurologicmanifestations in patients with UC: first, cerebrovas‐cular disease as a consequence of thrombosis andthromboembolism; second, systemic and cerebralvasculitis; and third, probable immune-mediated neu‐ropathy and cerebral demyelination. Among neuro‐logic disorders of undefined cause reported in pa‐tients with IBD, cerebrovascular disorders aredocumented in 0.12% to 4% of IBD patients2). Theycan occur at any age in both sexes and tend to corre‐late with disease activity.
The severity of UC can be classified as mild,moderate or severe, based on clinical symptoms andsigns and blood tests1). Our patient was considered tohave severe UC based on her frequent diarrhea,
100
Yanagisawa T Mizukami H et al118

Table 1. Previous Reports of Cerebral Hemorrhage Associated with Ulcerative Colitis
Reference Age Sex Ulcerative colitisactivity Treatment Outcome
Derdeyn and Powers4) 26 F Quiescent Anticoagulation Partial resolution ofsymptoms
Tsujikawa et al.5) 27 M Active Oral steroids andanticoagulation Recovery
Hishiyama et al.6) 32 M Active Pulse dose of steroids Partial resolution ofsymptoms
Mizuta et al.7) 51 F Active Nothing particular forcerebral hemorrhage Death
Hasegawa et al.8) 32 M Quiescent Anticoagulation Recovery
Nudelman et al.9) 23 M Active Steroids Death
Hizawa et al.10) 80 F Active Nothing particular forcerebral hemorrhage Death
Adrish and Rios11) Middle-aged M Not described
Anticoagulation,Decompressive
hemicraniectomy
Partial resolution ofsymptoms
Ueta et al.12) 76 M Active Decompressivehemicraniectomy Death
Parks and Easton13) 50 F Active Pulse dose of steroids Death
Idiopathicthrombocytopenic
purpura
Bilateral cerebellumMassive
Cerebral vasculitisLeft basal ganglia and left
temporal lobeMassive
Cerebral sinusthrombosis
Rt frontal, parietal lobeMassive
Disseminatedaspergillosis
Lt occipital lobeMassive
Cerebral sinusthrombosis
Left temporal lobeMassive
Cerebral sinusthrombosis
Lt frontal, parietal lobeRt frontal, occipital lobe
Moderate
Immunethrombocytopenic
purpura Not described
Cerebral sinusthrombosis
Lt occipital lobeModerate
Complication Hemorrhage siteand volume
Cortical venousthrombosis
Lt posterior frontal lobeModerate
Cerebral sinusthrombosis
Rt frontal poleSlight
bloody stool, pyrexia, tachycardia, anemia and ele‐vated ESR. In Japan, most case reports of cerebrovas‐cular complications of UC are of cerebral sinusthrombosis. A hypercoagulable state and cerebralvasculitis have been hypothesized as the etiologies.
Published case reports of UC patients with cere‐bral hemorrhage are listed in Table 1. Most of thecomplications were cerebral sinus/venous thrombosisthat caused hemorrhagic infarction. The volume ofhemorrhage tended to be massive with high mortalityin those cases. In comparison with most of the othercases associated with cerebral hemorrhage, which re‐sulted in fatal clinical outcomes7,9,10,12,13), our patient
experienced a good outcome.Our patient had no predisposing factors for
stroke and especially for cerebral hemorrhage. How‐ever, she suffered a second cerebral hemorrhagewithin a 5-day interval, and the high-intensity areasuggesting brain edema at the initial hemorrhage ex‐panded chronologically on MRI. The differential di‐agnosis during this period included malignancy, de‐myelination and vasculitis.
She also had an elevated level of myelin basicprotein, which is a cause of demyelination, of 619pg/mL on CSF examination. Abnormal values are ob‐served in diseases such as multiple sclerosis and Beh‐
101
Recurrent cerebral hemorrhage with UC 119

çet’s disease. Because our patient had no clinicalsymptoms or other laboratory or MRS findings sug‐gesting such conditions, we considered the high levelto be a secondary elevation due to myelin sheath de‐struction by cerebral hemorrhage.
Because her workup for malignancy was unre‐vealing, we considered a brain biopsy. We consultedwith Neurosurgery, but at this point she was free ofneurological symptoms. Therefore, because of therisk of biopsy causing a neurological deficit, espe‐cially a repeat of her sensory aphasia, we decidedagainst brain biopsy.
Our patient had a positive P-ANCA but her lev‐els of C-ANCA, MPO-ANCA and PR3-ANCA werewithin normal range. We performed skin biopsies oftwo nodules on her lower extremities to evaluate theevidence for systemic vasculitis, but no specific find‐ings were observed. Unnikrishnan et al.14) reviewed15 case reports of possible cerebral vasculitis in UC.Among them, 11 patients had definite vasculitisbased on histopathology, angiography or serology.Necrotizing vasculitis was confirmed by brain biopsyin 3 patients and autopsy in one patient. Skin biopsyperformed in 2 patients suggested possible systemicdisease in one patient, but necrotizing vasculitis wasnot found. Most of these patients were treated withsteroids alone or in combination with immunosup‐pressive therapy. One patient died, in whom autopsyhad revealed necrotizing angiitis of the brain, but theother patients experienced a good outcome with ste‐roid therapy.
Raj et al.15) reported a patient who showed largeareas of multiple enhanced masses on brain MRI.With steroid therapy, the patient’s neurological symp‐toms improved rapidly, and at one-month follow-up,MRI showed resolution of the lesions, with nomasses or mass effect and no abnormal enhancement.This chronological change on brain MRI was similarto that in our patient. Their patient underwent a brainbiopsy that showed small-sized vessels with endothe‐lial cell edema, infiltration by lymphocytes, neutro‐phils and possibly macrophages, and necrosis andhemorrhage, which were diagnosed as central nerv‐ous system vasculitis. They concluded that a brain bi‐opsy may ultimately be necessary to diagnose thistype of vasculitis. Although a brain biopsy was notperformed and skin biopsies did not show any evi‐dence of vasculitis in our patient, resolution of thebrain lesions on MRI by steroid therapy suggestedvasculitis as a possible etiology.
In conclusion, we experienced a patient with UC
who suffered recurrent cerebral hemorrhages thatwere treated by intravenous corticosteroids, which re‐sulted in a good outcome. Physicians should be alertto cerebral hemorrhage in patients with UC, considercerebral vasculitis as an etiology, and treat with ste‐roid therapy for a good outcome.
Conflicts of Interest
The authors have nothing to disclose.
References
1) Matsuoka K, Kobayashi T, Ueno F, et al. Evi‐dence-based clinical practice guidelines for in‐flammatory bowel disease. J Gastroenterol 2018;53: 305–353.
2) Lossos A, River Y, Eliakim A, et al. Neurologicaspects of inflammatory bowel disease. Neurol‐ogy 1995; 45: 416–421.
3) Scheid R, Teich N. Neurologic manifestations ofulcerative colitis. Eur J Neurol 2007; 14: 483–492.
4) Derdeyn CP, Powers WJ. Isolated cortical ve‐nous thrombosis and ulcerative colitis. AJNRAm J Neuroradiol 1998; 19: 488–490.
5) Tsujikawa T, Urabe M, Bamba H, et al. Hae‐morrhagic cerebral sinus thrombosis associatedwith ulcerative colitis: a case report of success‐ful treatment by anticoagulant therapy. J Gastro‐enterol Hepatol 2000; 15: 688–692.
6) Hishiyama M, Kato Y, Shibui T, et al. Cerebralsinus thrombosis associated with ulcerative coli‐tis. Nihon Naika Gakkai Zasshi [in Japanese]2001; 90: 2287–2290.
7) Mizuta Y, Isomoto H, Kadokawa Y, et al. Im‐mune thrombocytopenic purpura on patientswith ulcerative colitis. J Gastroenterol 2003; 38:884–890.
8) Hasegawa H, Yokomori H, Tsuji T, et al. Hem‐orrhagic cerebral sinus thrombosis in a case ofcontrolled ulcerative colitis. Intern Med 2005;44: 155.
9) Nudelman RJ, Rosen DG, Rouah E, et al. Cere‐bral sinus thrombosis: a fatal neurological com‐plication of ulcerative colitis. Patholog Res Int2010; 2010: 132754. doi: 10.4061/2010/132754.
10) Hizawa K, Hatada T, Morinaga S, et al. An au‐topsy case of ulcerative colitis with dissemi‐nated aspergillosis, complicated by brain hemor‐rhage. Nihon Shokakibyo Gakkai Zasshi [inJapanese] 2013; 110: 648–654.
11) Adrish M, Rios R. Intracranial hemorrhage and
102
Yanagisawa T Mizukami H et al120

extensive cerebral venous thrombosis associatedwith ulcerative colitis. Can J Gastroenterol Hep‐atol 2014; 28: 299–300.
12) Ueta S, Sato K, Hanaoka M, et al. Cerebellarhemorrhage caused by thrombocytopenia associ‐ated with ulcerative colitis. Tokushima RedCross Hospital Medical Journal [in Japanese]2015; 20: 60–63.
13) Parks PT, Easton AS. Cerebral vasculitis in ul‐cerative colitis is predominantly venular: casereport and review of the literature. Case RepRheumatol 2019; 2019: 9563874. doi: 10.1155/
2019/9563874.14) Unnikrishnan A, Azodi S, Ansari N, et al.
PR3ANCA related cerebral vasculitis in ulcera‐tive colitis presenting with orbital involvement:A case report with review of literature. Case RepRheumatol 2014; 2014: 582094. doi: 10.1155/2014/582094.
15) Raj N, Arkebauer M, Waters B, et al. A case ofcerebral vasculitis associated with ulcerative coli‐tis. Case Rep Rheumatol 2015; 2015: 598273.doi: 10.1155/2015/598273.
103
Recurrent cerebral hemorrhage with UC 121