Embed Size (px)
Citation preview

Traitement de l’HTAP associée àla Sclérodermie systémique
Olivier SITBON
Centre de Référence de l’Hypertension Pulmonaire Sévèr eHôpitaux Universitaires Paris-Sud – INSERM U999
Université Paris-Sud 11 – Clamart – France
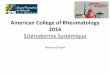
L’HTAP associée aux connectivites
39%
15%
11%
10%
HTAP idiopathique
Connectivites
Cardiopathies congénitales
Hypertension portale
Humbert M, et al. Am J Respir Crit Care Med 2006; 173:1023-30.
(% de la population)
9.5%
6%
4%
Exposition aux anorexigènes
HTAP familiale
Infection VIH
2 facteurs de risque 4%
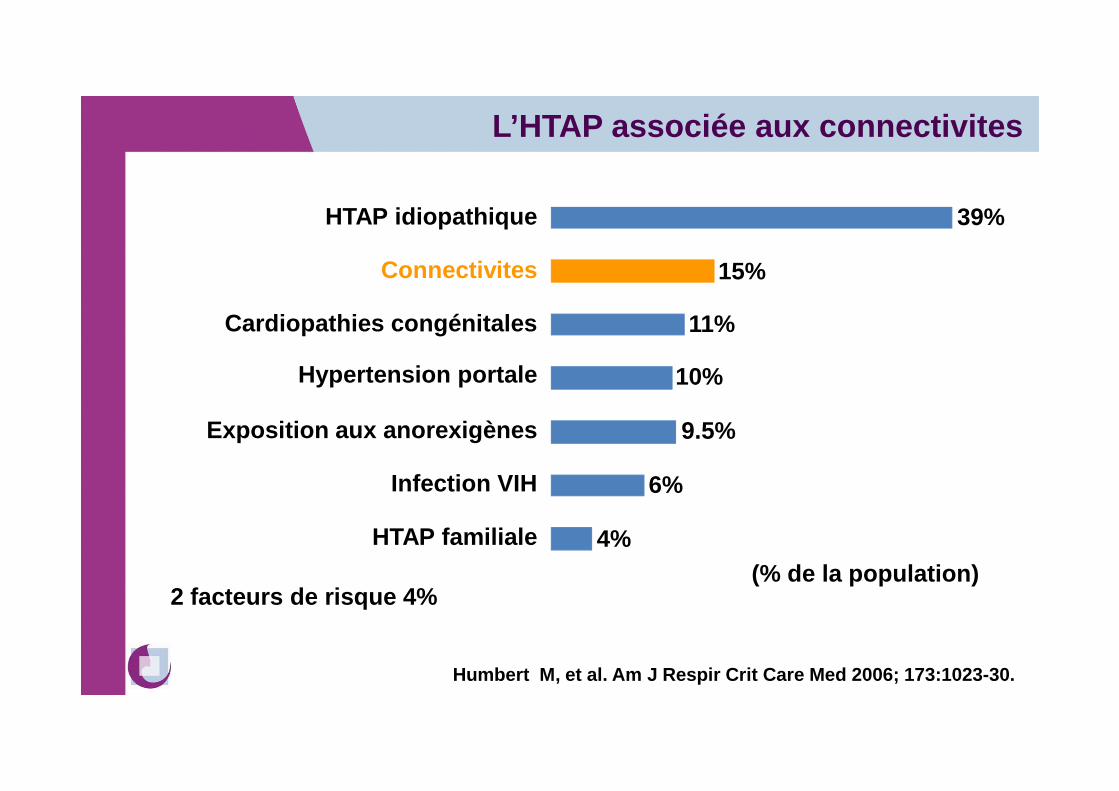
HTAP associée à une pathologie concomitante : 47.4% (n = 320)
Connectivites
Hypertension portale 26%
24% 10%Sclérodermie systémique Autres
34%
L’HTAP associée à la sclérodermie systémique
Limited68%
Diffuse 32%
Sclérodermie systémique
Cardiopathies congénitales
Infection VIH
24%
17%
Humbert M, et al. Am J Respir Crit Care Med 2006; 173:1023-30.
Diffuse(32 %) Limitée
(68 %)
50
75
100
IPAH
100
75
50
IPAH
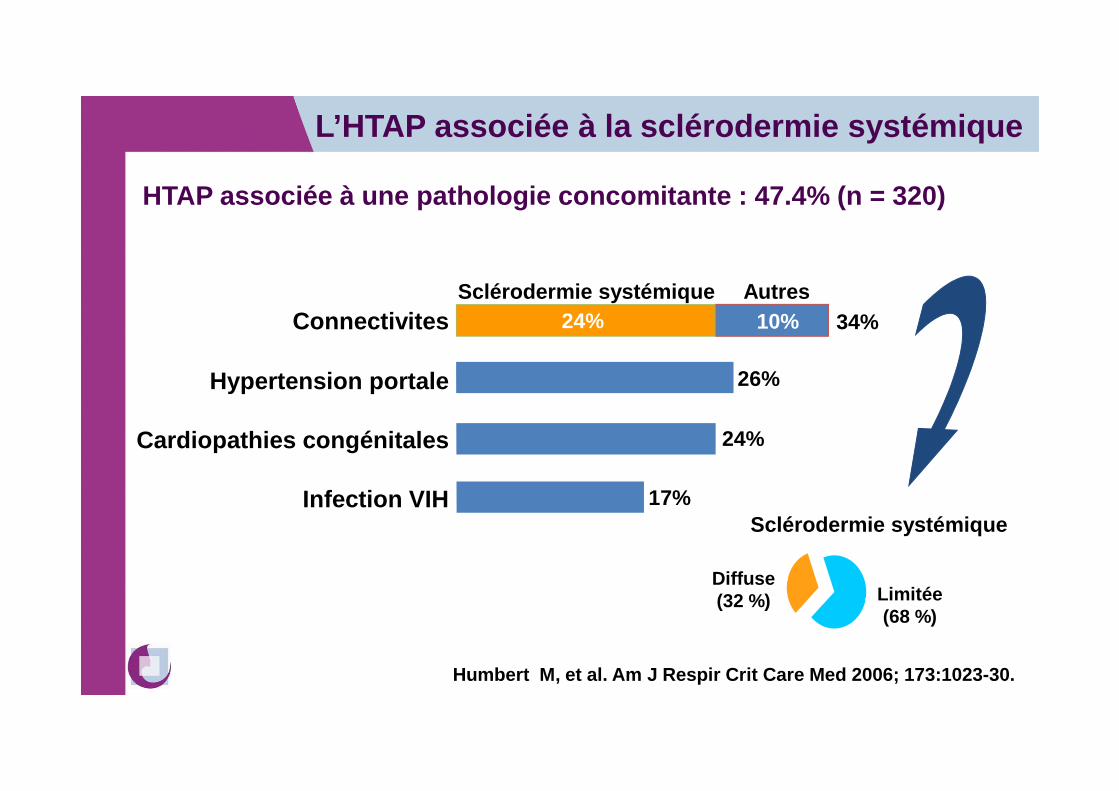
HTAP-SSc : un pronostic sombre…
Time (years)
0
25
50
1 2 3 4
PAH-SSc
p = 0.002
3
50
25
0
PAH-SSc
Time (years) 1 2
p = 0.03
Kawut SM, et al. Chest 2003; 123:344-50.Fisher MR, et al. Arthritis Rheum 2006; 54:3043-50.
Approche multidisciplinaire indispensable
� Par rapport à l’HTAP idiopathique, l’HTAP associée à l a sclérodermie systémique est plus cliniquement plus sévè re et de plus mauvais pronostic
� La fréquence des manifestations cardio-pulmonaires es t élevée
� HTAP, atteinte veinule fréquente (“MVO-like”),
� Myocardiopathie restrictive (insuffisance cardiaque diastolique),� Myocardiopathie restrictive (insuffisance cardiaque diastolique),
� Pneumopathie infiltrante…
� Collaboration indispensable entre internistes/rhuma tologues et pneumologues/cardiologues
� Calqué sur le traitement de l’HTAP idiopathique� HTAP idiopathiques et associées aux connectivites dans la plupart
des essais contrôlés� Réunions d’experts internationaux (4th WSPAH) & recommandations
de sociétés savantes (ACCP, ESC/ERS Guidelines)
� Probablement plus complexe…� Efficacité réelle des traitements « spécifiques » de l’HTAP ?
Traitement de l’HTAP associée connectivites
� Efficacité réelle des traitements « spécifiques » de l’HTAP ?� Place des traitements anti-inflammatoires et immunosuppresseurs ?� Place de la transplantation pulmonaire ?
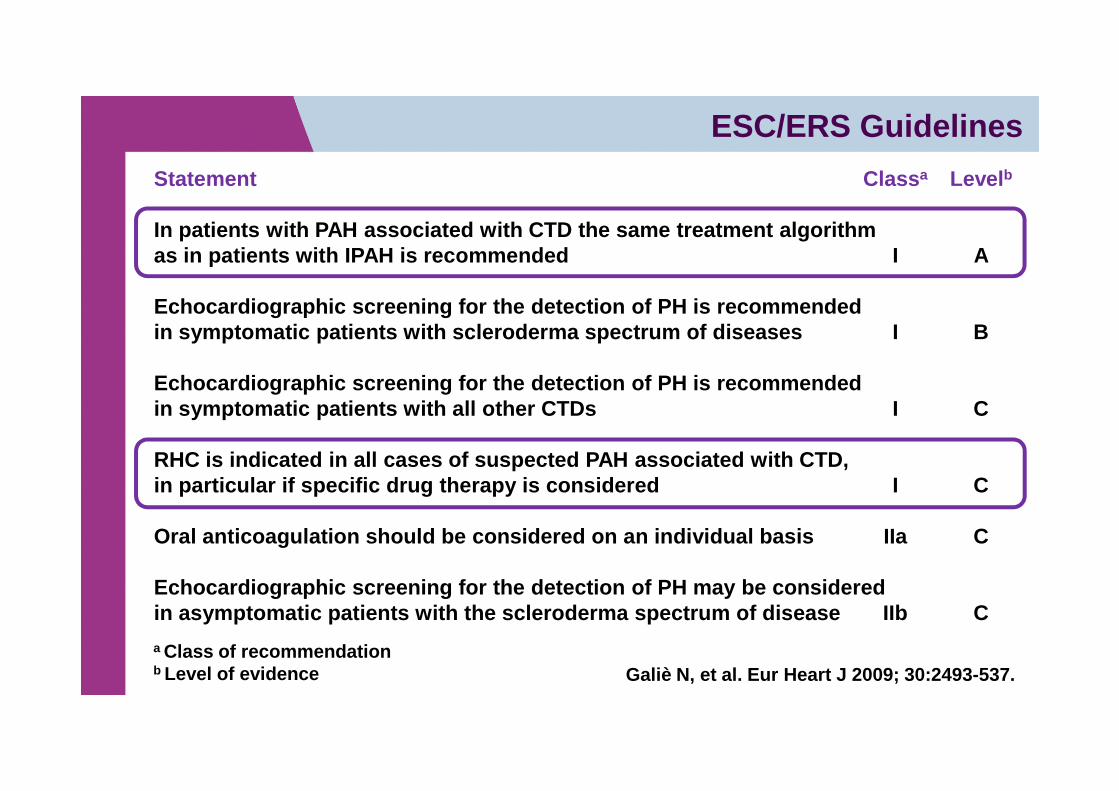
Statement Class a Level b
In patients with PAH associated with CTD the same t reatment algorithmas in patients with IPAH is recommended I A
Echocardiographic screening for the detection of PH is recommendedin symptomatic patients with scleroderma spectrum o f diseases I B
Echocardiographic screening for the detection of PH is recommended
ESC/ERS Guidelines
in symptomatic patients with all other CTDs I C
RHC is indicated in all cases of suspected PAH asso ciated with CTD,in particular if specific drug therapy is considere d I C
Oral anticoagulation should be considered on an ind ividual basis IIa C
Echocardiographic screening for the detection of PH may be consideredin asymptomatic patients with the scleroderma spect rum of disease IIb C
a Class of recommendationb Level of evidence Galiè N, et al. Eur Heart J 2009; 30:2493-537.
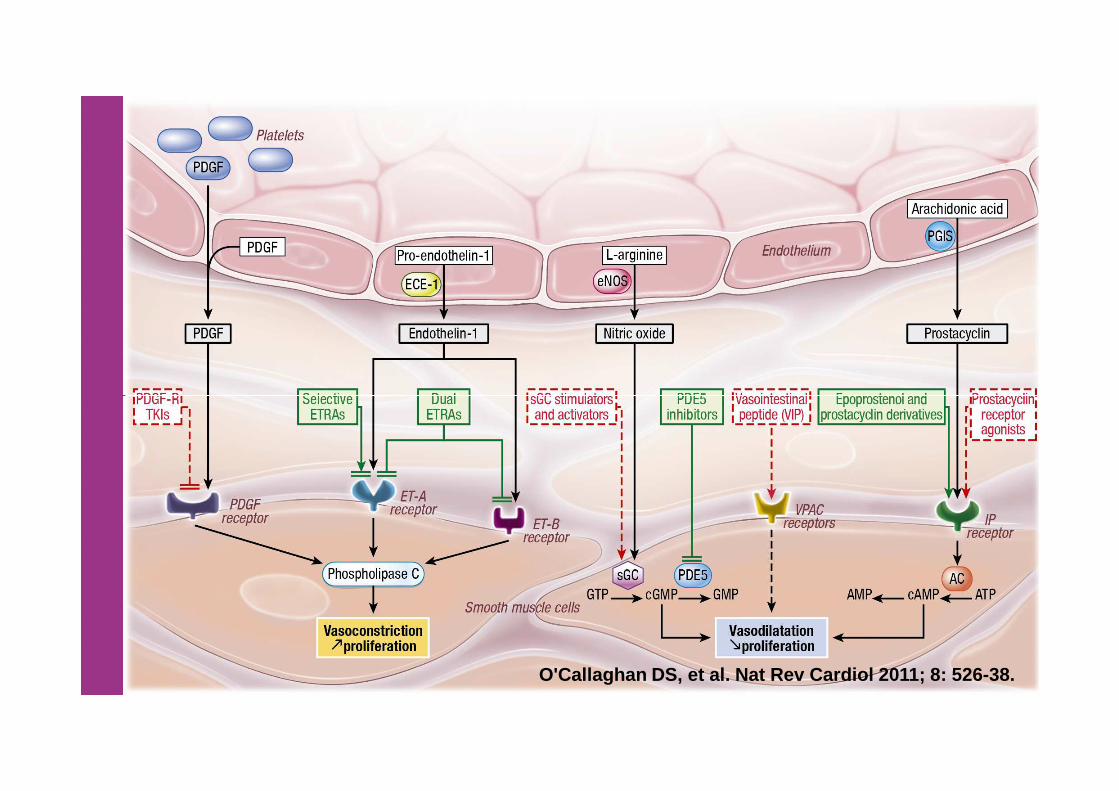
O'Callaghan DS, et al . Nat Rev Cardiol 2011; 8: 526-38.
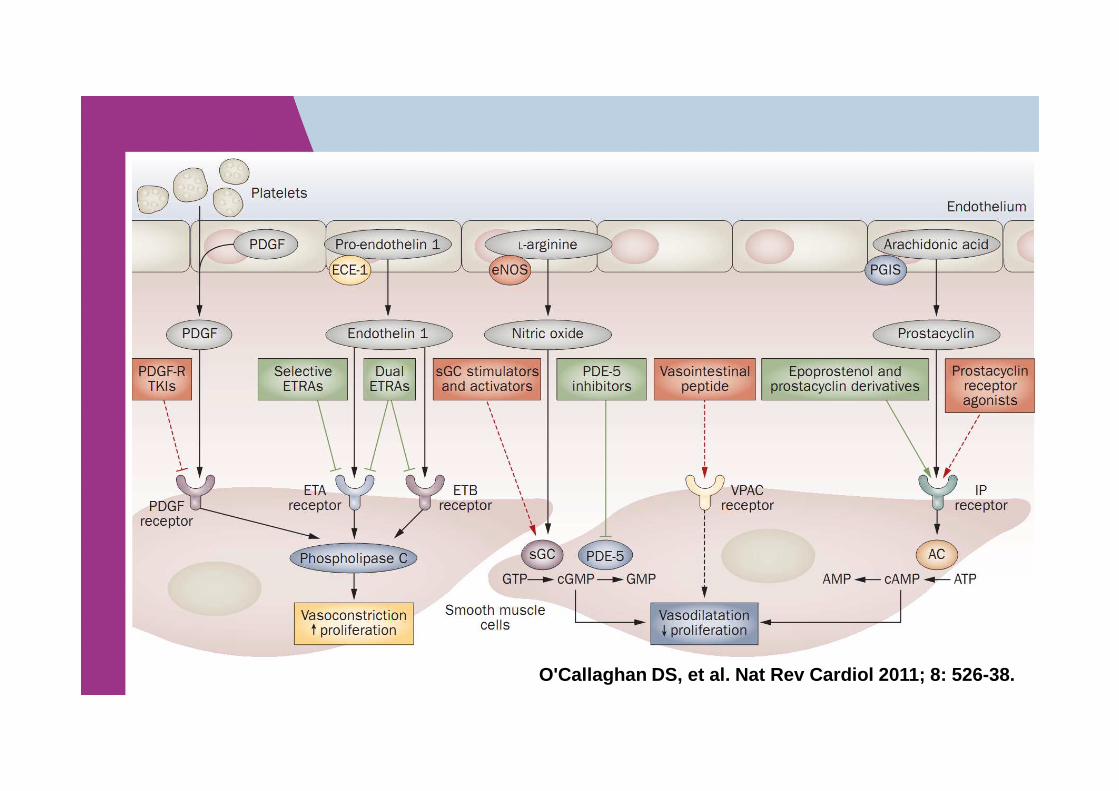
O'Callaghan DS, et al . Nat Rev Cardiol 2011; 8: 526-38.
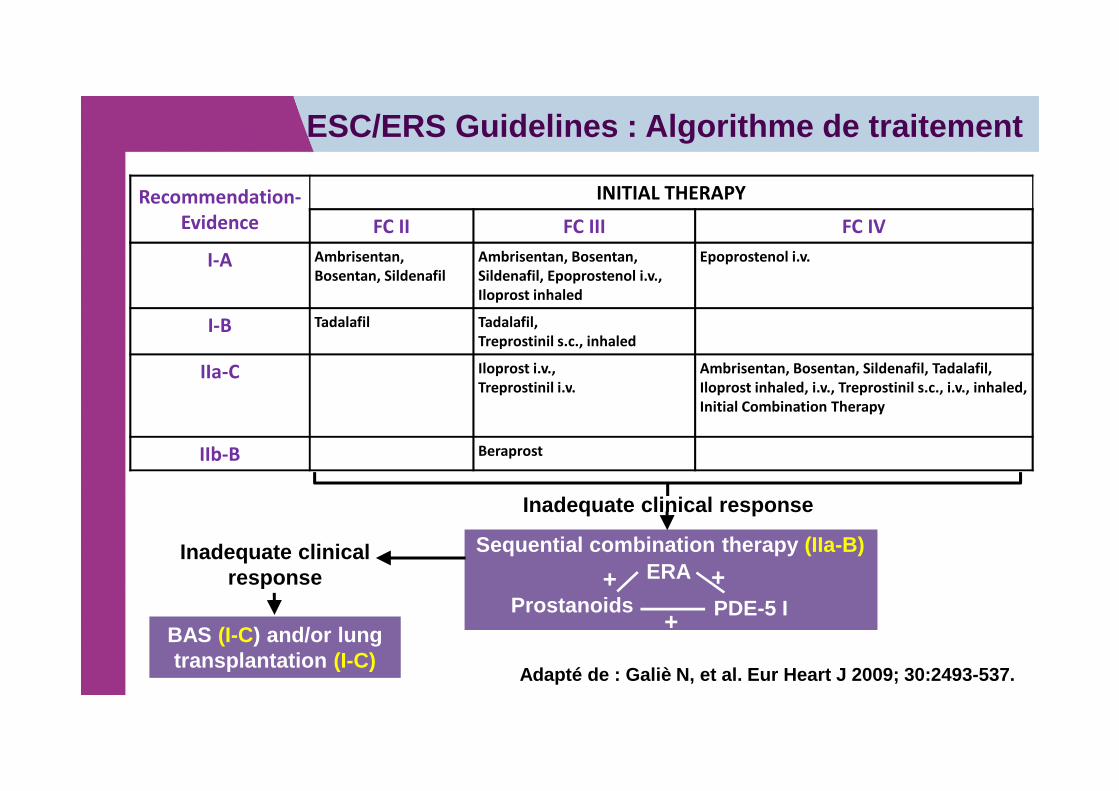
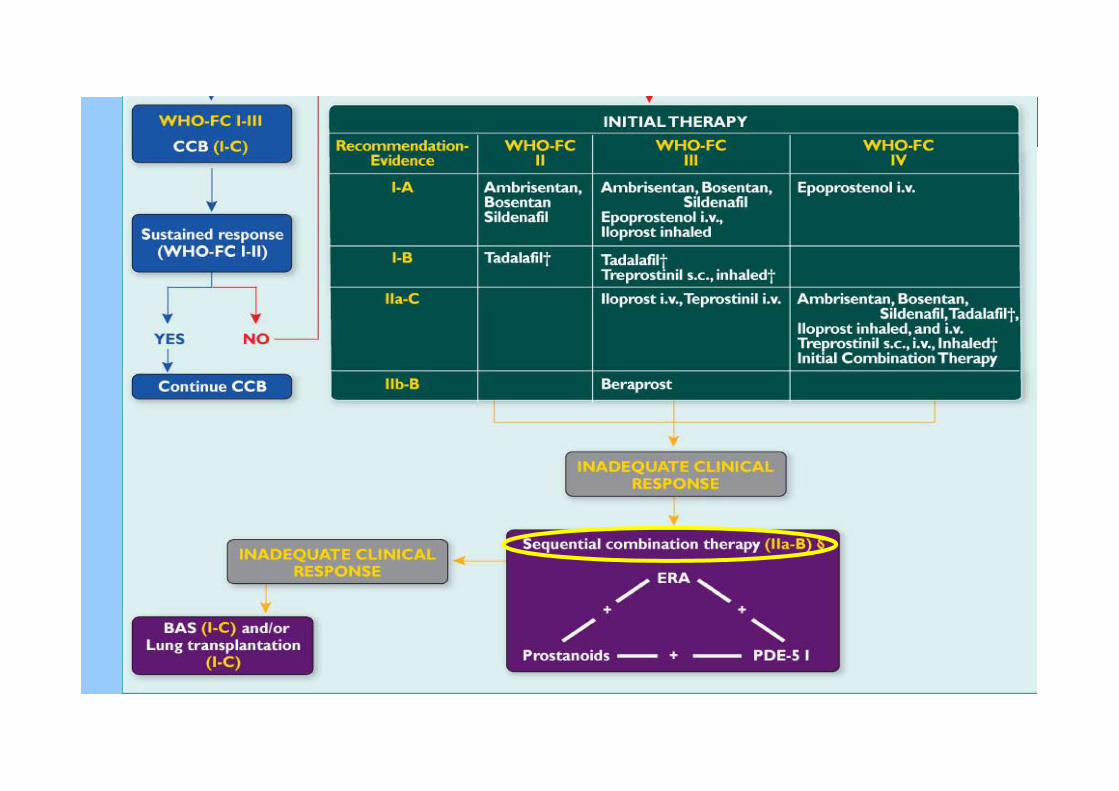
Recommendation-
Evidence
INITIAL THERAPY
FC II FC III FC IV
I-A Ambrisentan,
Bosentan, Sildenafil
Ambrisentan, Bosentan,
Sildenafil, Epoprostenol i.v.,
Iloprost inhaled
Epoprostenol i.v.
I-B Tadalafil Tadalafil,
Treprostinil s.c., inhaled
IIa-C Iloprost i.v.,
Treprostinil i.v.
Ambrisentan, Bosentan, Sildenafil, Tadalafil,
Iloprost inhaled, i.v., Treprostinil s.c., i.v., inhaled,
ESC/ERS Guidelines : Algorithme de traitement
Treprostinil i.v. Iloprost inhaled, i.v., Treprostinil s.c., i.v., inhaled,
Initial Combination Therapy
IIb-B Beraprost
Inadequate clinical response
Inadequate clinicalresponse
BAS (I-C) and/or lungtransplantation (I-C)
Sequential combination therapy (IIa-B)ERA
Prostanoids PDE-5 I+ +
+
Adapté de : Galiè N, et al. Eur Heart J 2009; 30:2493-537.
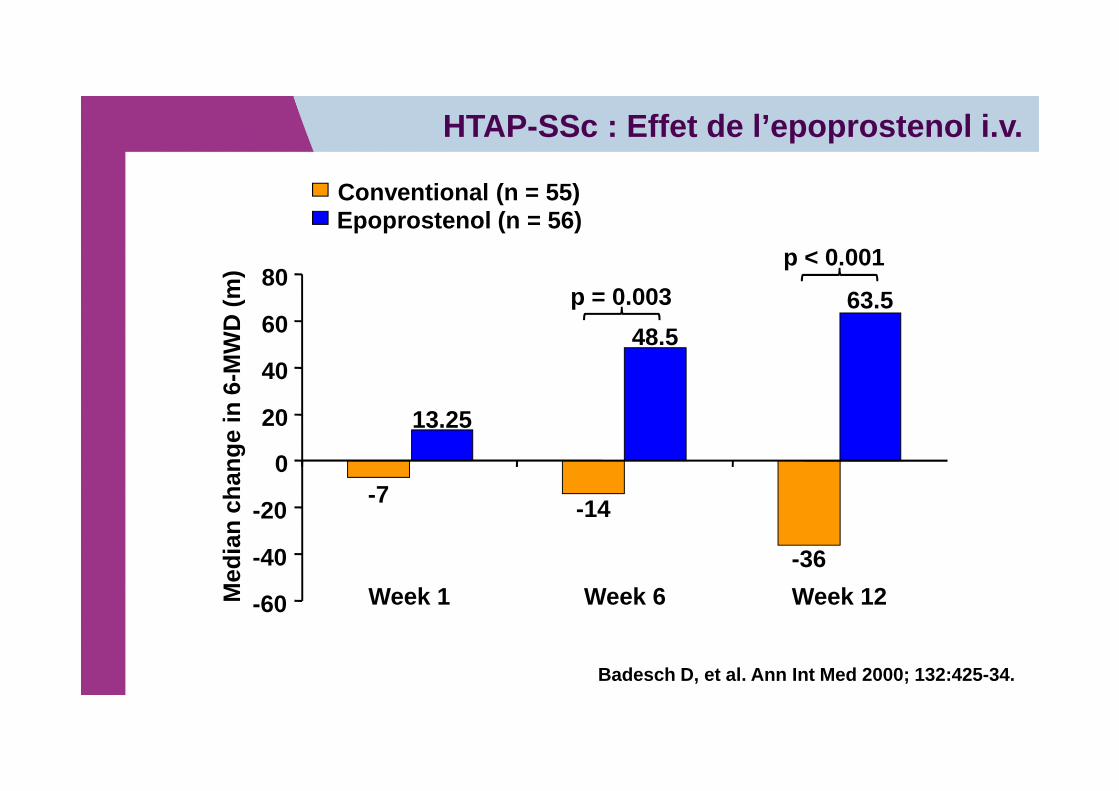
p = 0.003
p < 0.001
63.5
48.540
60
80
Med
ian
chan
ge in
6-M
WD
(m
)
Conventional ( n = 55)Epoprostenol ( n = 56)
HTAP-SSc : Effet de l’epoprostenol i.v.
-36
-14-7
13.25
-60
-40
-20
0
20
Week 1 Week 6 Week 12Med
ian
chan
ge in
6
Badesch D , et al. Ann Int Med 2000; 132:425-34.
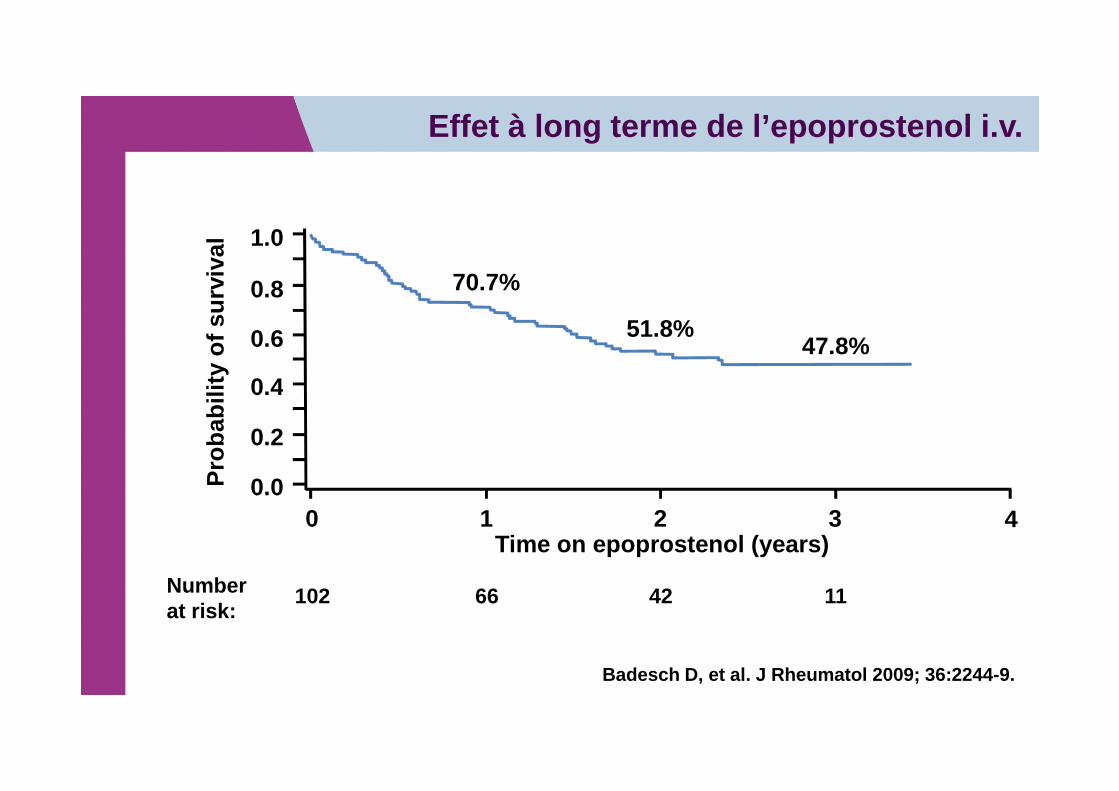
70.7%
51.8%47.8%
Pro
babi
lity
of s
urvi
val
0.4
0.6
0.8
1.0
Effet à long terme de l’epoprostenol i.v.
102 66 42 11Numberat risk:
0 1 2 3 4Time on epoprostenol (years)
Pro
babi
lity
0.0
0.2
0.4
Badesch D , et al. J Rheumatol 2009; 36:2244-9.
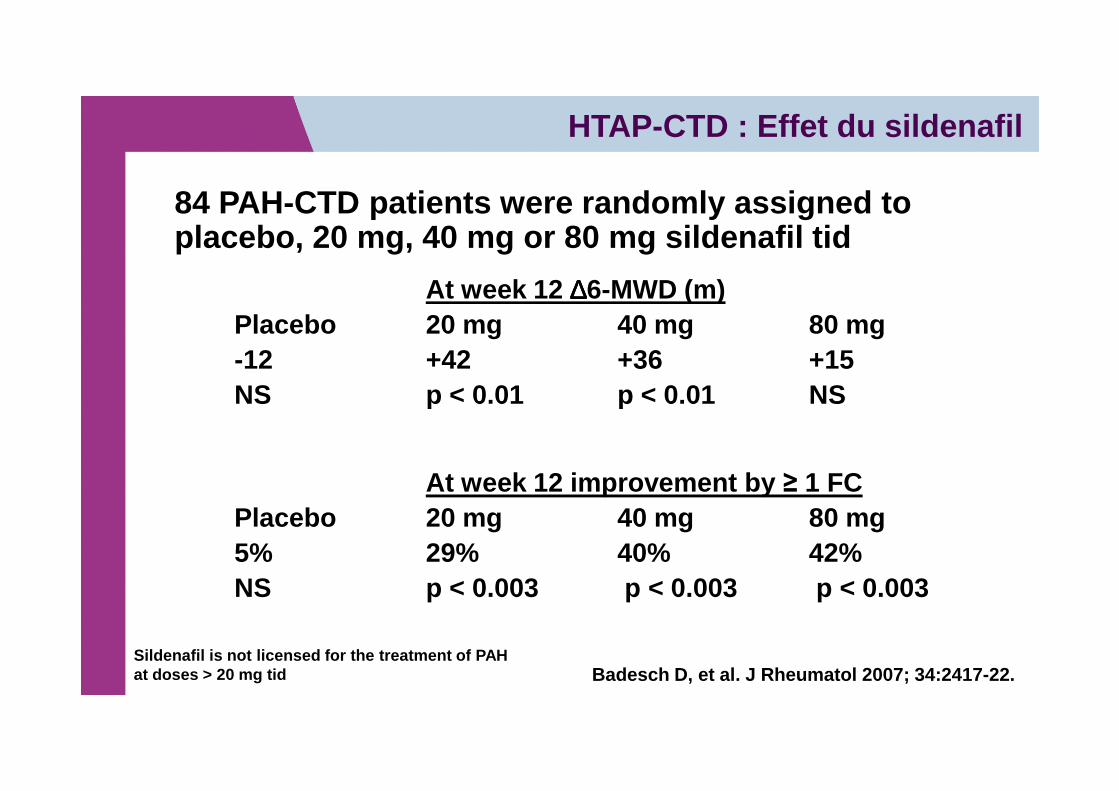
84 PAH-CTD patients were randomly assigned to placebo, 20 mg, 40 mg or 80 mg sildenafil tid
At week 12 ∆∆∆∆6-MWD (m)Placebo 20 mg 40 mg 80 mg-12 +42 +36 +15NS p < 0.01 p < 0.01 NS
HTAP-CTD : Effet du sildenafil
NS p < 0.01 p < 0.01 NS
At week 12 improvement by ≥ 1 FCPlacebo 20 mg 40 mg 80 mg5% 29% 40% 42%NS p < 0.003 p < 0.003 p < 0.003
Sildenafil is not licensed for the treatment of PAHat doses > 20 mg tid Badesch D , et al. J Rheumatol 2007; 34:2417-22.
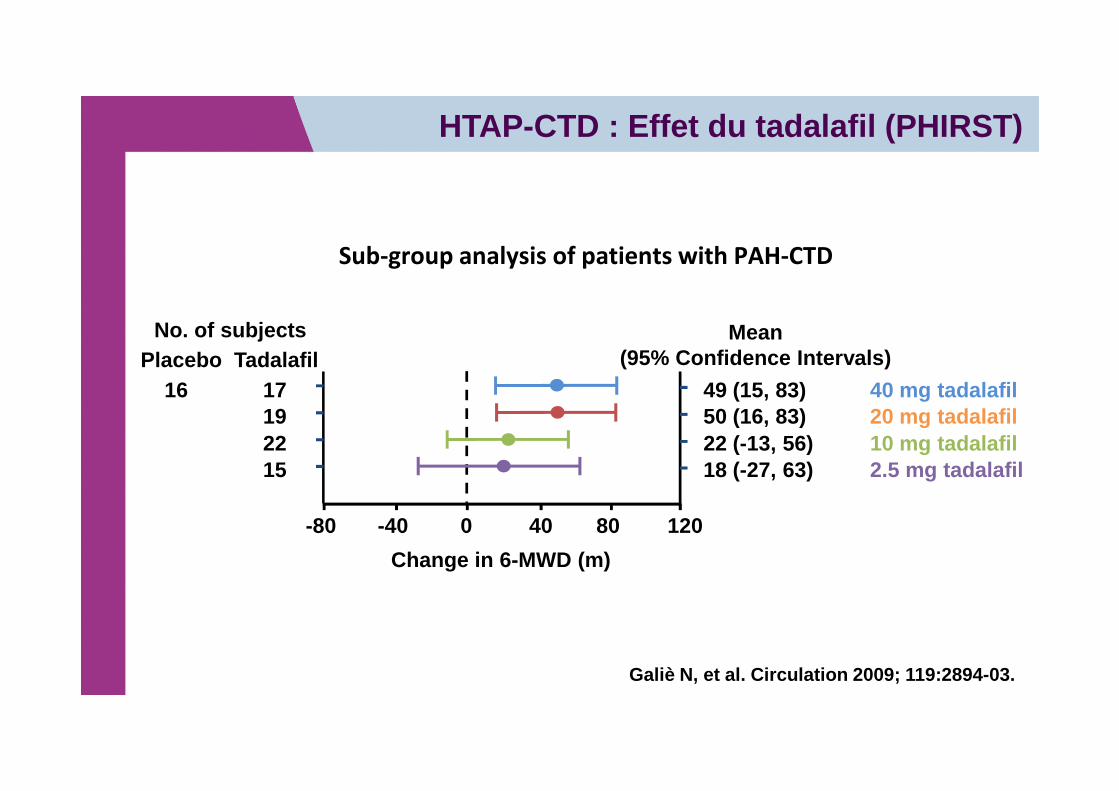
Sub-group analysis of patients with PAH-CTD
Placebo TadalafilNo. of subjects Mean
(95% Confidence Intervals)
49 (15, 83)16 17 40 mg tadalafil
HTAP-CTD : Effet du tadalafil (PHIRST)
49 (15, 83)50 (16, 83)22 (-13, 56)18 (-27, 63)
16 17192215
Change in 6-MWD (m)
0 40 80 120-40-80
40 mg tadalafil20 mg tadalafil10 mg tadalafil2.5 mg tadalafil
Galiè N, et al. Circulation 2009; 119:2894-03.
� ARIES-11
� Improved 6-MWD
� Failed to improve timeto clinical worsening
� Results represent entire trial population (IPAH, CT D, HIV-PAH &
� ARIES-21
� Improved 6-MWD and time to clinical worsening
HTAP-CTD : Effet de l’ambrisentan
� Results represent entire trial population (IPAH, CT D, HIV-PAH & anorexigen associated PAH). While 31% of patients ha d CTD, sub-group analysis was not included in publication.
� ARIES-E2
� Long-term extension of ARIES-1 & ARIES-2
� Improvement in 6-MWD sustained after 2 years of treatment
1. Galiè N , et al. Circulation 2008; 117:3010-9.2. Oudiz RJ, et al. J Am Coll Cardiol 2009; 54:1971-81.
� Etudes 351 1 et BREATHE-1 2 ont inclus des patients avec une HTAP associée à une SScou un lupus
� 66 patients avec une HTAP associée à uneconnectivite (SSc, n = 52) ont été randomisés
HTAP-CTD : Effet du bosentan
connectivite (SSc, n = 52) ont été randomisésdans ces deux essais contrôlés 3
1. Channick RN, et al. Lancet 2001; 358:1119-23.2. Rubin, LJ et al. New Engl J Med 2002; 346:896-903.3. Denton CP , et al. Ann Rheum Dis 2006; 65:1336-40.
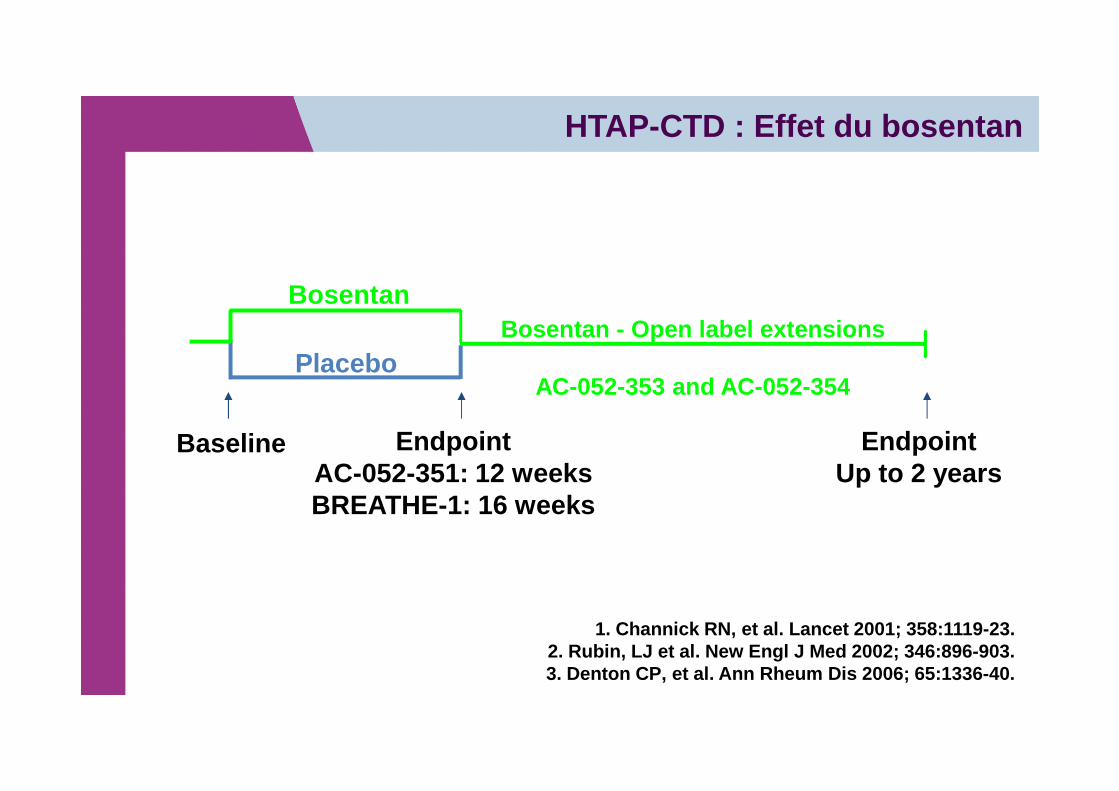
Bosentan - Open label extensions
AC-052-353 and AC -052-354Placebo
Bosentan
HTAP-CTD : Effet du bosentan
AC-052-353 and AC -052-354
Baseline EndpointAC-052-351: 12 weeksBREATHE-1: 16 weeks
EndpointUp to 2 years
1. Channick RN, et al. Lancet 2001; 358:1119-23.2. Rubin, LJ et al. New Engl J Med 2002; 346:896-903.3. Denton CP , et al. Ann Rheum Dis 2006; 65:1336-40.
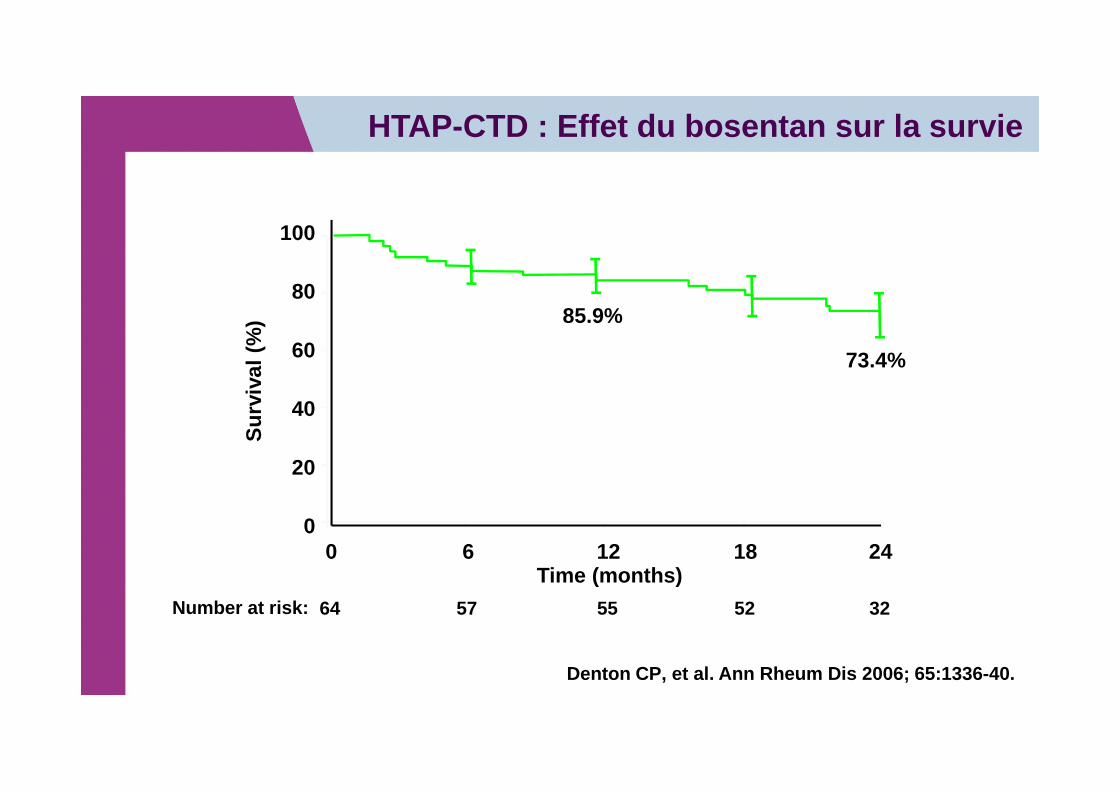
Sur
viva
l (%
) 85.9%
73.4%
80
60
100
HTAP-CTD : Effet du bosentan sur la survie
0 6 12 18 24Time (months)
64 57 55 52 32Number at risk:
Sur
viva
l (%
)
Denton CP , et al. Ann Rheum Dis 2006; 65:1336-40.
0
20
40
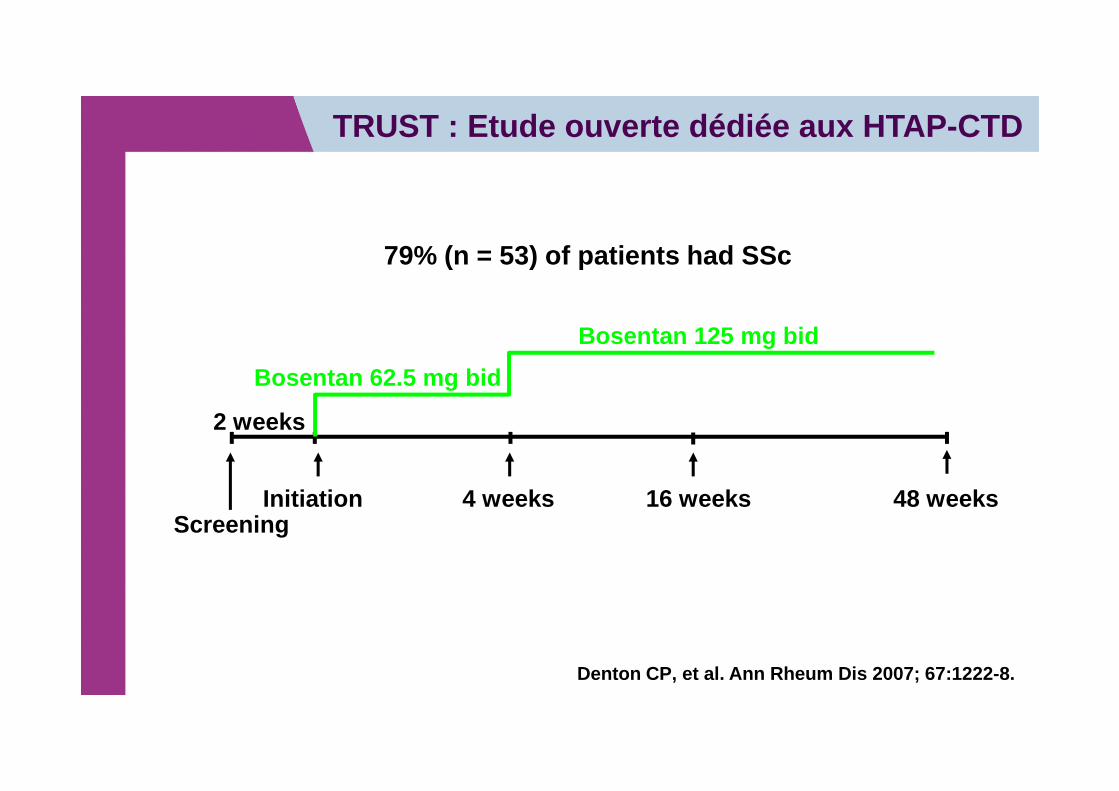
Bosentan 62.5 mg bid
Bosentan 125 mg bid
79% (n = 53) of patients had SSc
TRUST : Etude ouverte dédiée aux HTAP-CTD
48 weeks
2 weeks
ScreeningInitiation 4 weeks 16 weeks
Denton CP , et al. Ann Rheum Dis 2007; 67:1222-8.
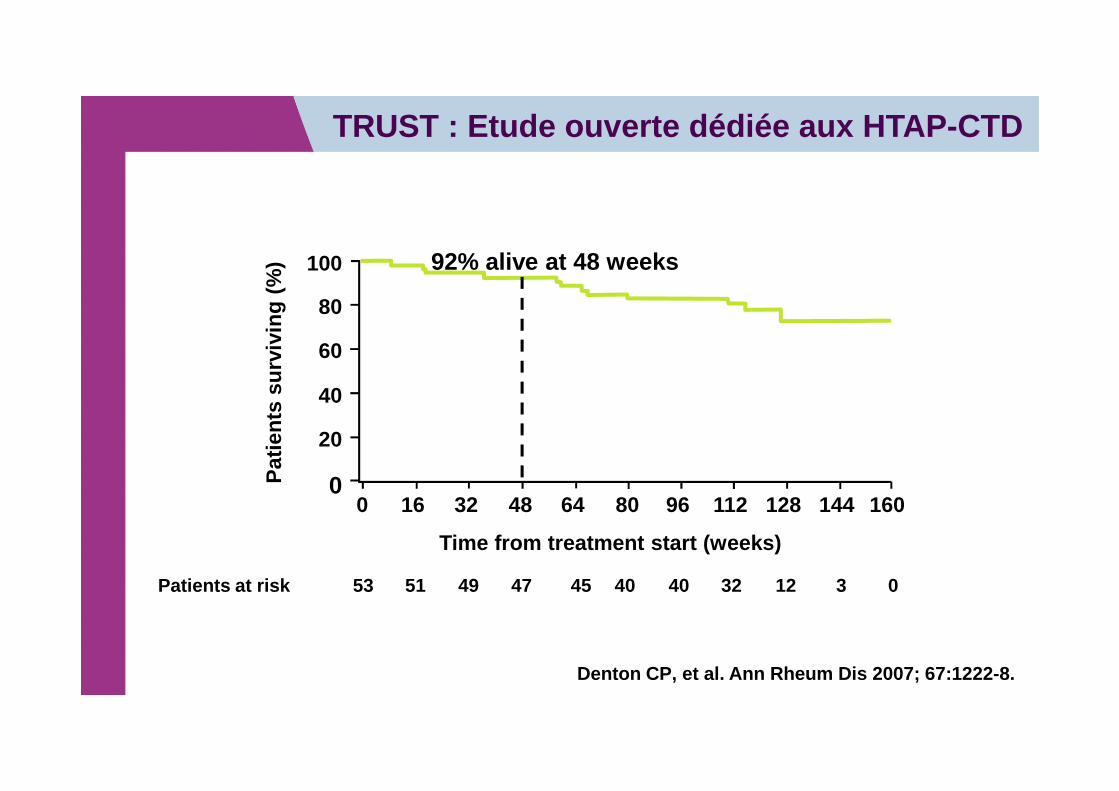
100
80
60
40surv
ivin
g(%
) 92% alive at 48 weeks
TRUST : Etude ouverte dédiée aux HTAP-CTD
40
20
0Pat
ient
s
Time from treatment start (weeks)
0 16 32 48 64 80 96 112 128 144 160
Patients at risk 53 51 49 47 45 40 40 32 12 3 0
Denton CP , et al. Ann Rheum Dis 2007; 67:1222-8.
Cum
ulat
ive
surv
ival
0.4
0.6
0.8
1
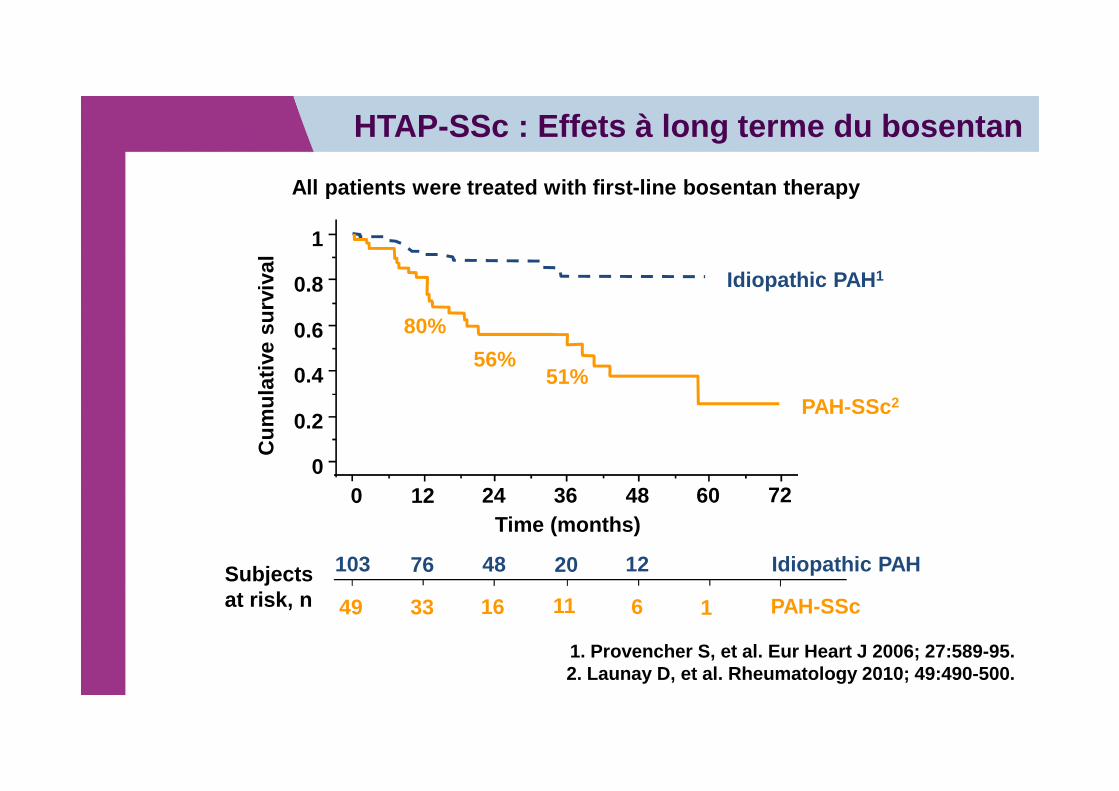
Idiopathic PAH 1
PAH-SSc2
All patients were treated with first-line bosentan t herapy
80%
51%56%
HTAP-SSc : Effets à long terme du bosentan
Cum
ulat
ive
Time (months)0 12 24 36 48 60 72
0
0.2
Subjectsat risk, n
Idiopathic PAH
PAH-SSc
103 76 48 20 12
49 33 16 11 6 1
PAH-SSc2
1. Provencher S, et al. Eur Heart J 2006; 27:589-95.2. Launay D , et al. Rheumatology 2010; 49:490-500.
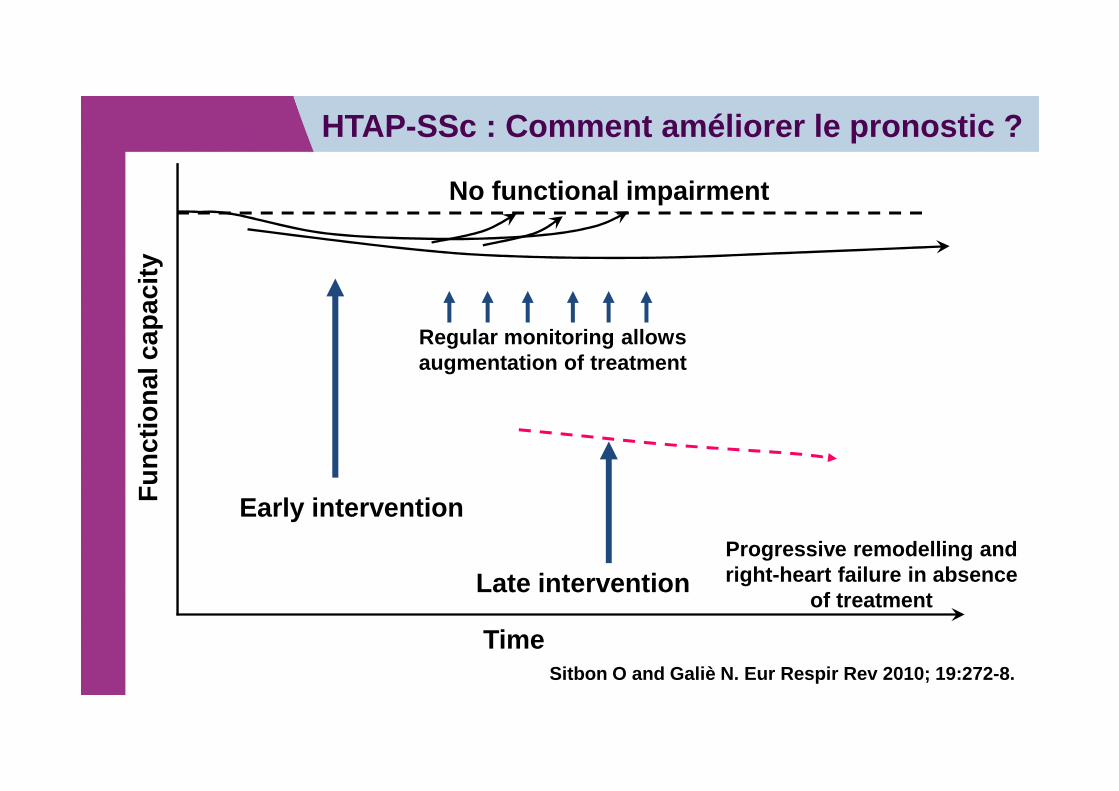
Regular monitoring allows augmentation of treatment
Fun
ctio
nal c
apac
ity
No functional impairment
HTAP-SSc : Comment améliorer le pronostic ?
Progressive remodelling and right-heart failure in absence
of treatment
Time
Early intervention
Late intervention
Fun
ctio
nal c
apac
ity
Sitbon O and Galiè N. Eur Respir Rev 2010; 19:272-8.
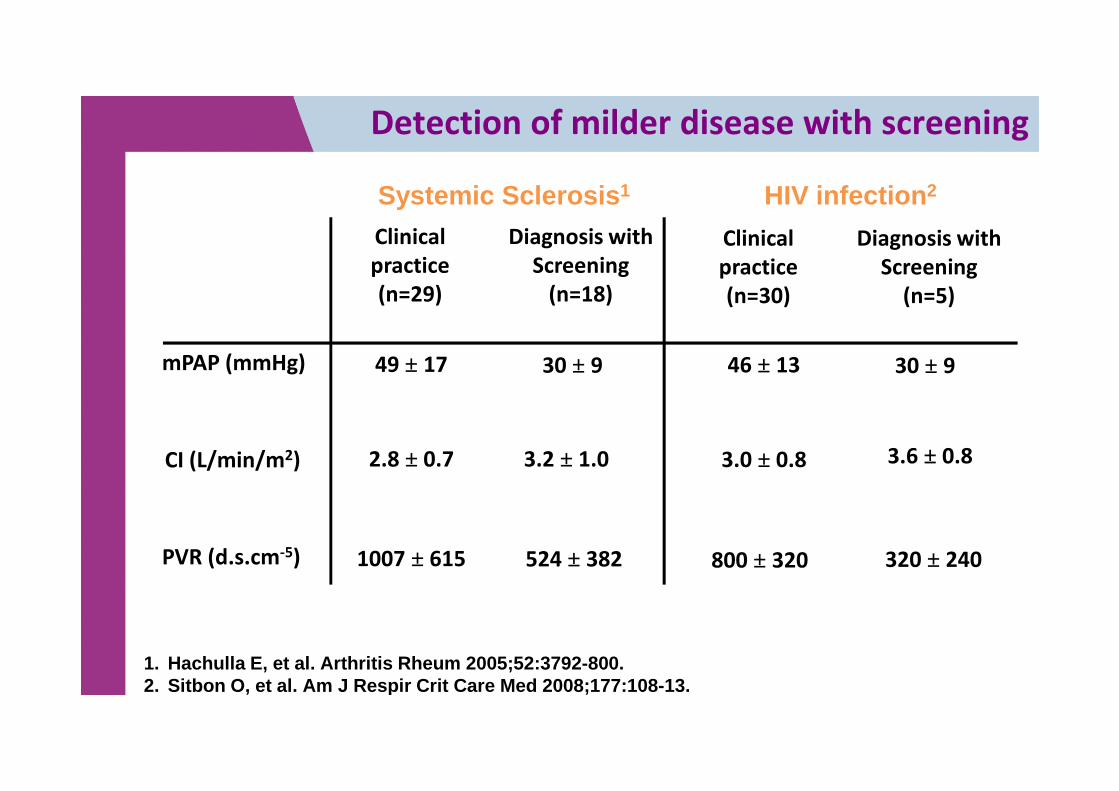
Detection of milder disease with screening
mPAP (mmHg) 49 ± 17 30 ± 9
Diagnosis with
Screening
(n=18)
Clinical
practice
(n=29)
Diagnosis with
Screening
(n=5)
Clinical
practice
(n=30)
46 ± 13 30 ± 9
Systemic Sclerosis 1 HIV infection 2
CI (L/min/m2) 2.8 ± 0.7 3.2 ± 1.0
PVR (d.s.cm-5) 1007 ± 615 524 ± 382
3.6 ± 0.8
800 ± 320 320 ± 240
3.0 ± 0.8
1. Hachulla E, et al. Arthritis Rheum 2005;52:3792-800.2. Sitbon O, et al . Am J Respir Crit Care Med 2008;177:108-13.
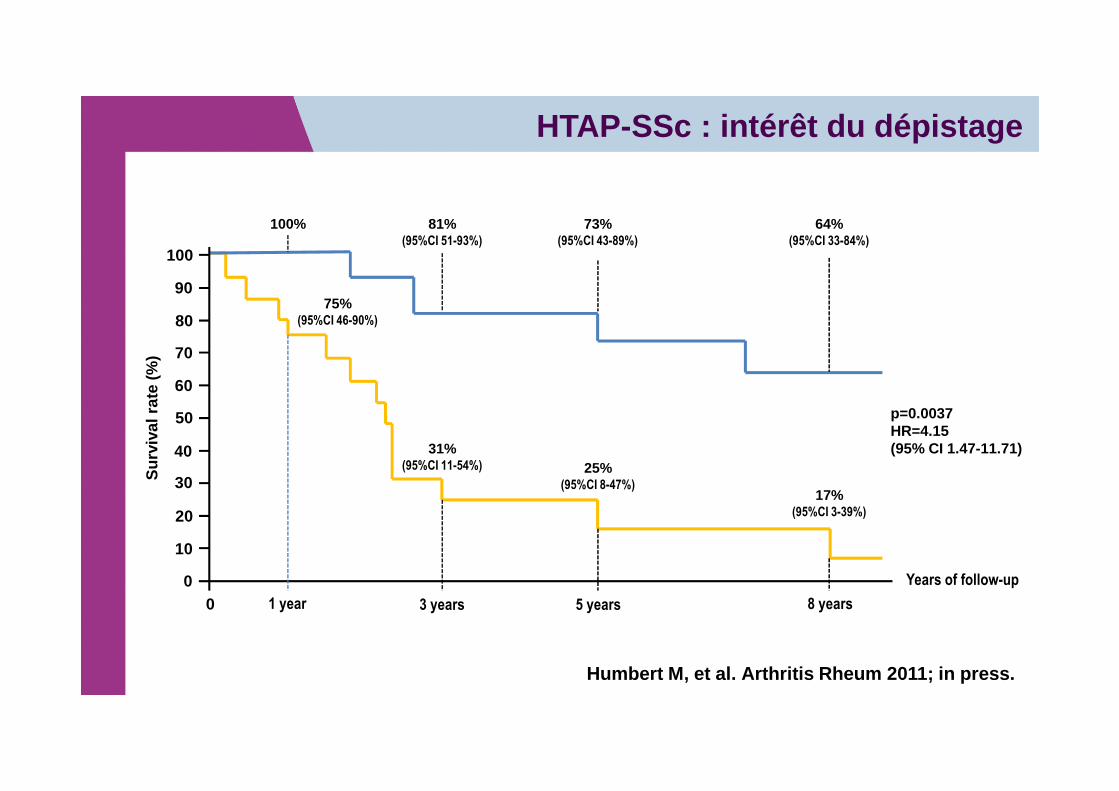
HTAP-SSc : intérêt du dépistage
100
90
80
70
60
rate
(%)
100% 81%(95%CI 51-93%)
73%(95%CI 43-89%)
64%(95%CI 33-84%)
75%(95%CI 46-90%)
Humbert M, et al . Arthritis Rheum 2011; in press .
50
40
30
20
10
00 1 year 3 years 5 years 8 years
Years of follow-up
p=0.0037HR=4.15(95% CI 1.47-11.71)
Sur
viva
lra
te (%
)
31%(95%CI 11-54%) 25%
(95%CI 8-47%)17%
(95%CI 3-39%)
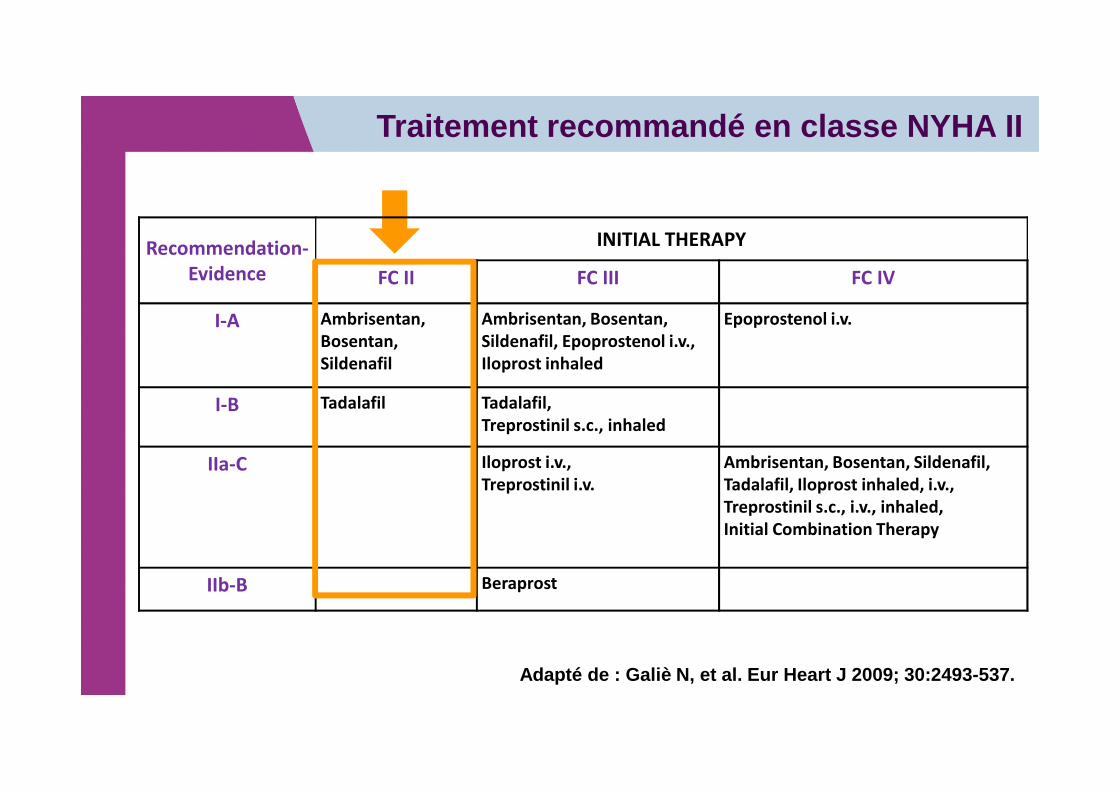
Recommendation-
Evidence
INITIAL THERAPY
FC II FC III FC IV
I-A Ambrisentan,
Bosentan,
Sildenafil
Ambrisentan, Bosentan,
Sildenafil, Epoprostenol i.v.,
Iloprost inhaled
Epoprostenol i.v.
I-B Tadalafil Tadalafil,
Traitement recommandé en classe NYHA II
I-B Tadalafil Tadalafil,
Treprostinil s.c., inhaled
IIa-C Iloprost i.v.,
Treprostinil i.v.
Ambrisentan, Bosentan, Sildenafil,
Tadalafil, Iloprost inhaled, i.v.,
Treprostinil s.c., i.v., inhaled,
Initial Combination Therapy
IIb-B Beraprost
Adapté de : Galiè N, et al. Eur Heart J 2009; 30:2493-537.
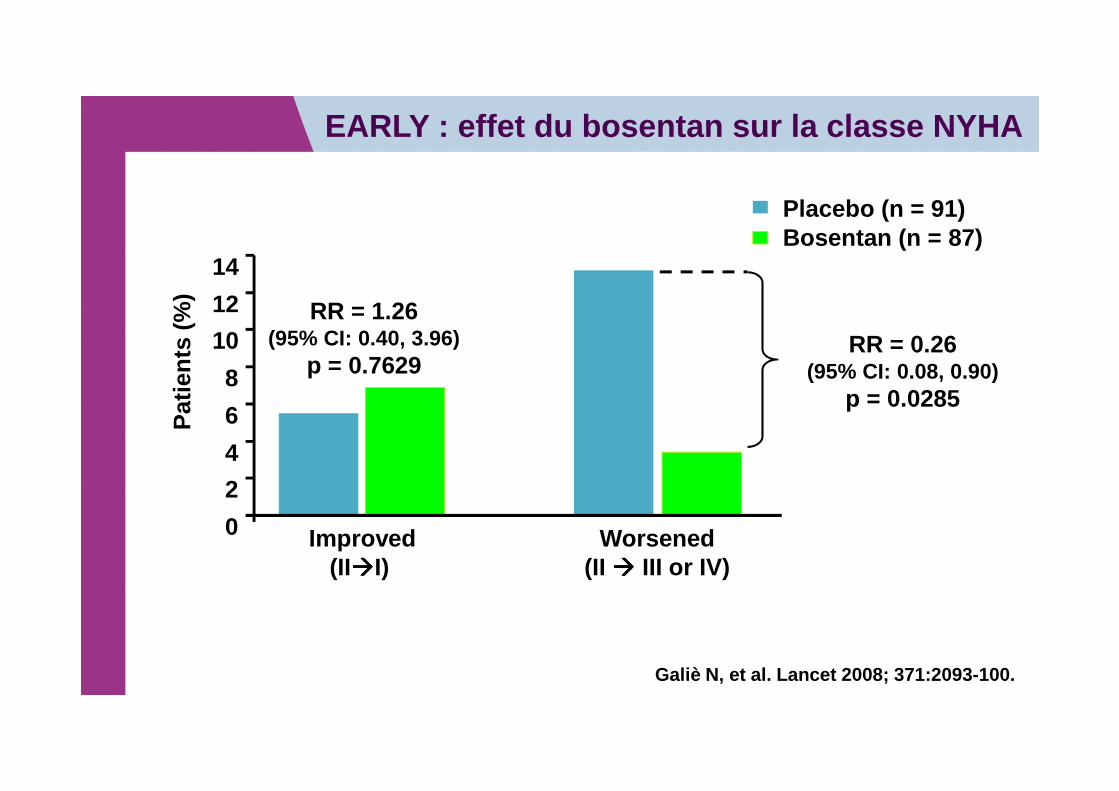
Placebo ( n = 91)Bosentan ( n = 87)
Pat
ient
s (%
)
RR = 0.26 (95% CI: 0.08, 0.90)
p = 0.02858
10
12
14
RR = 1.26 (95% CI: 0.40, 3.96)
p = 0.7629
EARLY : effet du bosentan sur la classe NYHA
Pat
ient
s (%
)
p = 0.0285
0
2
4
6
Improved(II����I)
Worsened(II ���� III or IV)
Galiè N, et al . Lancet 2008; 371:2093-100.
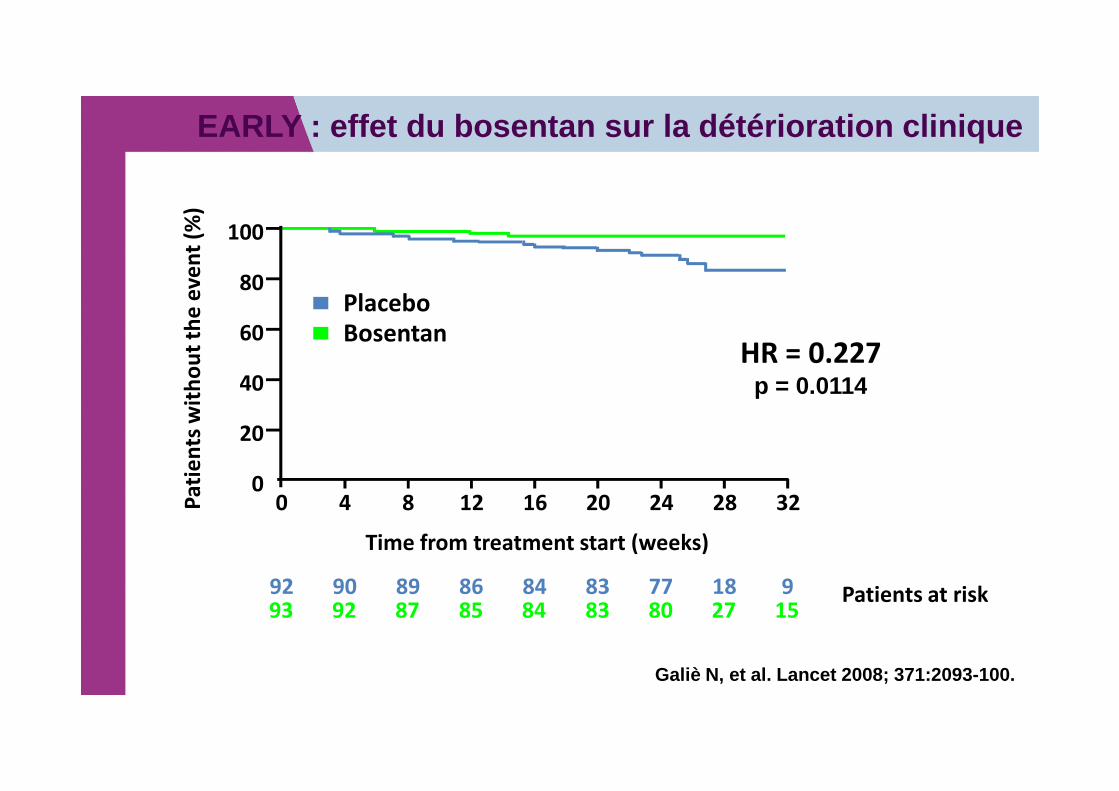
100
80
60
40
Pa
tie
nts
wit
ho
ut
the
ev
en
t (%
)
Placebo
BosentanHR = 0.227
p = 0.0114
EARLY : effet du bosentan sur la détérioration cliniq ue
40
20
00 4 8 12 16 20 2824 32
92 90 89 86 84 83 1877 993 92 87 85 84 83 2780 15
Time from treatment start (weeks)
Pa
tie
nts
wit
ho
ut
the
ev
en
t (%
)
Patients at risk
p = 0.0114
Galiè N, et al . Lancet 2008; 371:2093-100.
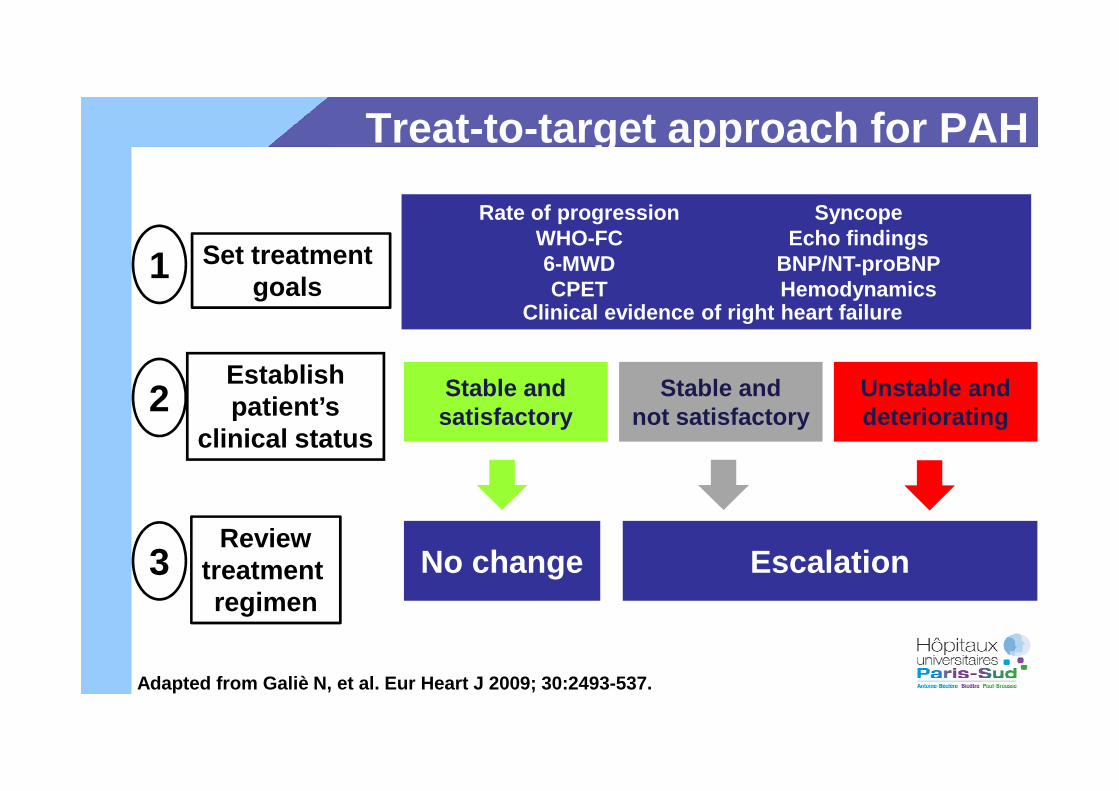
Establishpatient’s
Stable and Stable and Unstable and
Set treatment goals
1
2
Rate of progressionWHO-FC6-MWDCPET
SyncopeEcho findings
BNP/NT-proBNPHemodynamics
Clinical evidence of right heart failure
Treat-to -target approach for PAH
Adapted from Galiè N, et al. Eur Heart J 2009; 30:2493-537.
patient’sclinical status
Reviewtreatment regimen
Stable andsatisfactory
Stable and not satisfactory
Unstable and deteriorating
No change Escalation
2
3

Assessment parameter
Stable and satisfactory
Stable and not satisfactory
Unstable and deteriorating
Clinical evidenceof RV failure
No Yes
Rate of progression Slow Rapid
Syncope No Yes
WHO-FC I, II IV
Setting treatment goals in PAH:All patients should be in the “better prognosis“ gr oup
Only some of the “green”
parameters are fulfilled
(Grey zone)
WHO-FC I, II IV
6-MWD Longer (> 500 m) Shorter (< 300 m)
CPETPeak VO2
> 15 ml/min/kgPeak VO2
< 12 ml/min/kg
BNP/NT-proBNPplasma levels
Normal or near-normalVery elevated
and rising
Echocardiographicfindings
No pericardial effusionTAPSE > 2.0 cm
Pericardial effusionTAPSE < 1.5 cm
HaemodynamicsRAP < 8 mmHg
and CI ≥ 2.5 l/min/m 2RAP > 15 mmHg
or CI ≤ 2.0 l/min/m 2
Adapted from Galiè N, et al. Eur Heart J 2009; 30:2493-537.
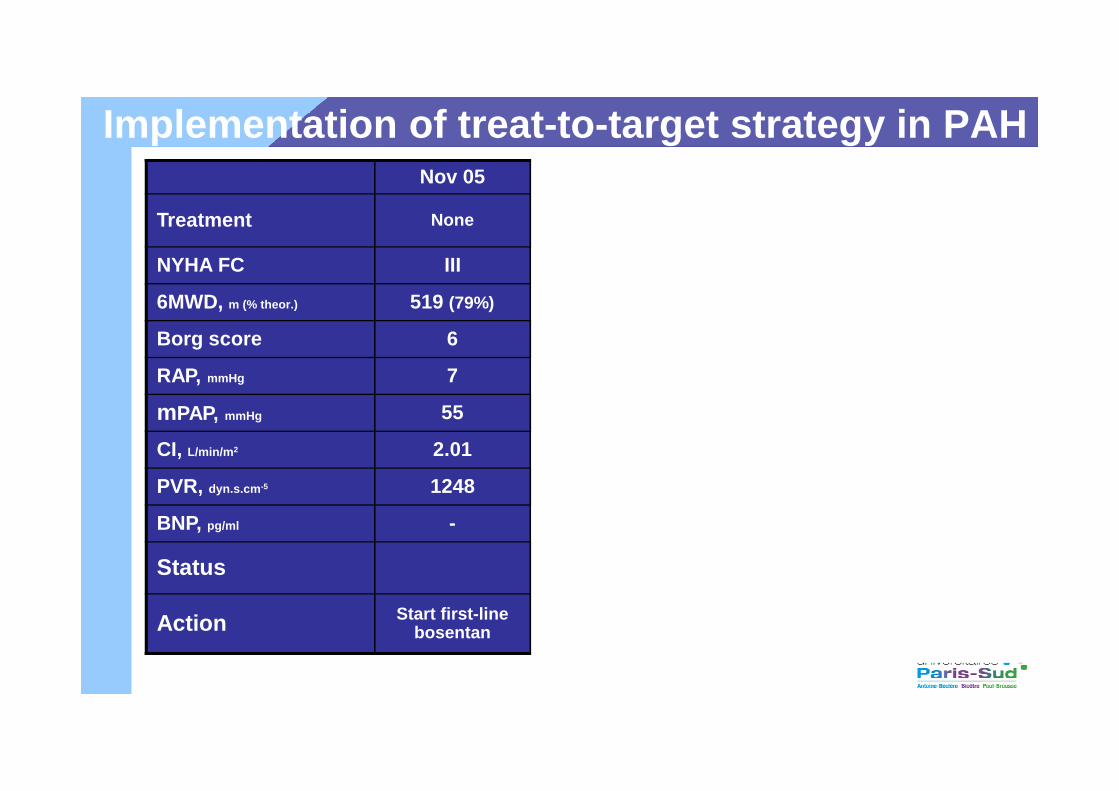
Nov 05 Mar 06 Aug 06 Jan 07
Treatment None Bosentan bosentan+ sildenafil
Bos. + Sil.+ epoprostenol
NYHA FC III III III II
6MWD, m (% theor.) 519 (79%) 525 (80%) 441 (67%) 601 (91%)
Borg score 6 3 4 3
RAP, mmHg 7 8 8 3
Implementation of treat-to -target strategy in PAH
mPAP, mmHg 55 60 65 47
CI, L/min/m 2 2.01 2.50 2.09 3.35
PVR, dyn.s.cm -5 1248 1066 1368 649
BNP, pg/ml - 217 360 62
Status Stable and unsatisfactory Deteriorating Stable and
satisfactory
Action Start first-line bosentan
Addsildenafil Add epoprostenol No change
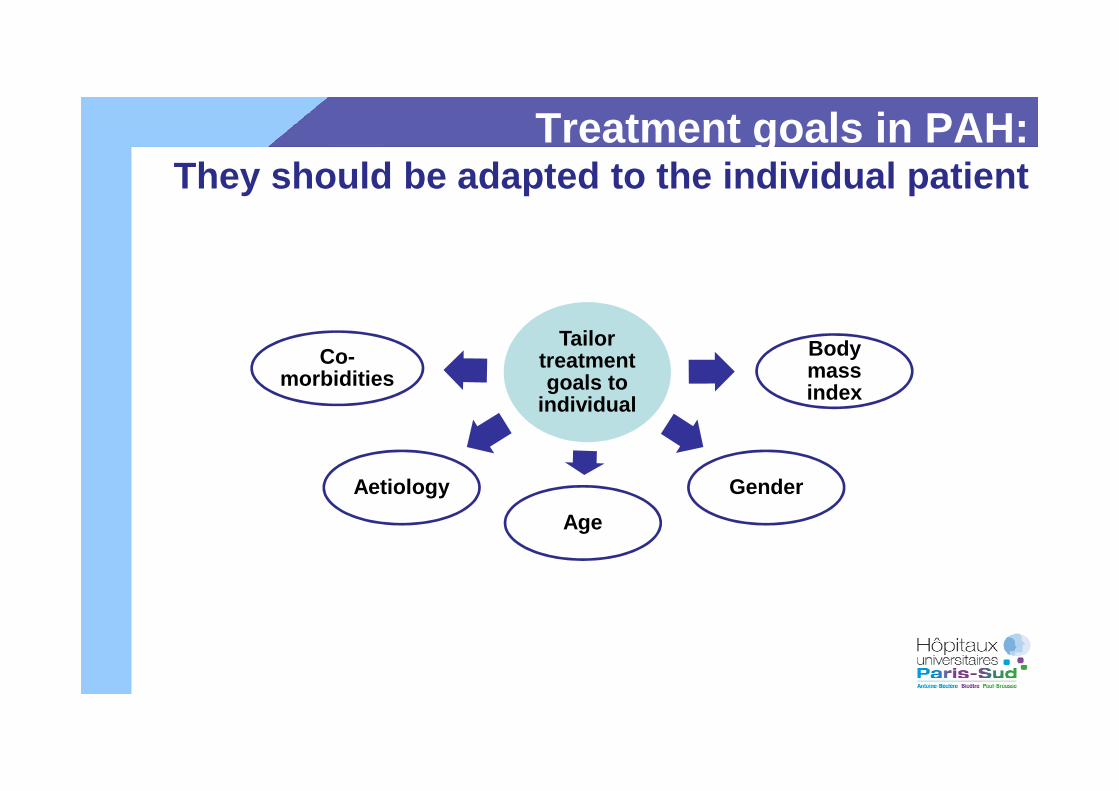
Tailor treatment goals to
individual
Body mass index
Co-morbidities
Treatment goals in PAH:They should be adapted to the individual patient
individual
Age
index
GenderAetiology
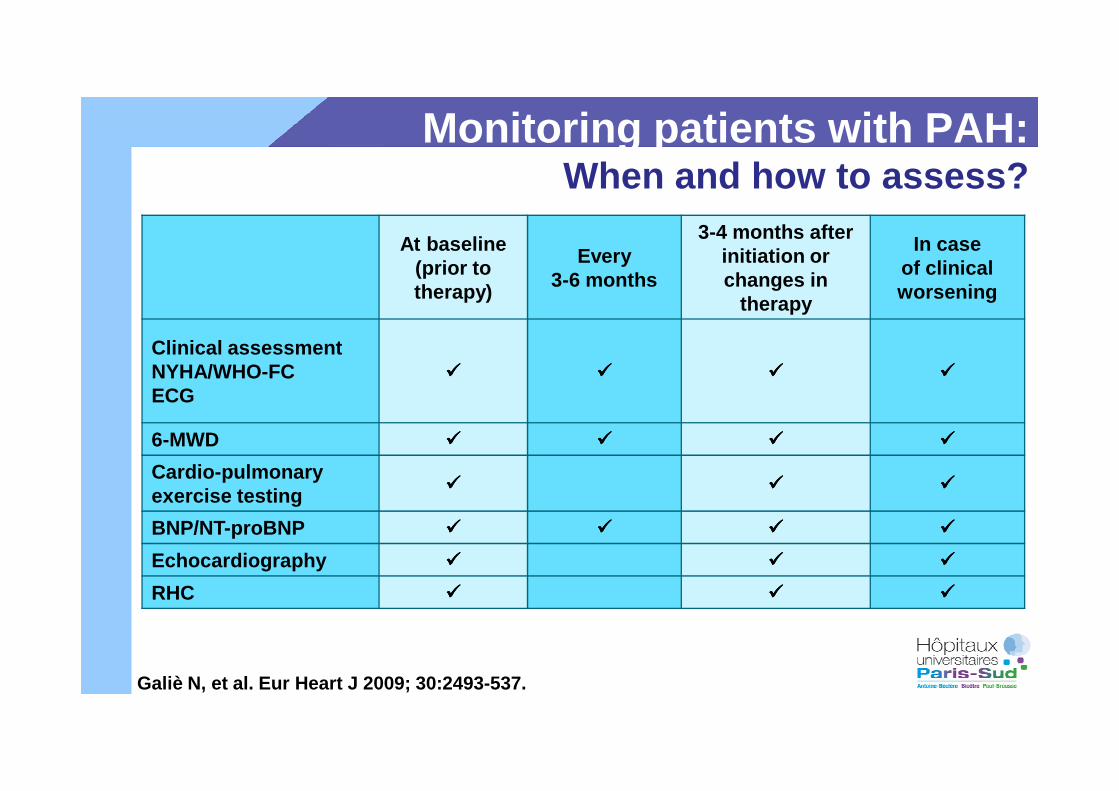
At baseline (prior to therapy)
Every 3-6 months
3-4 months after initiation or changes in
therapy
In case of clinical worsening
Clinical assessmentNYHA/WHO-FC ECG
���� ���� ���� ����
Monitoring patients with PAH:When and how to assess?
ECG
6-MWD ���� ���� ���� ����
Cardio-pulmonary exercise testing
���� ���� ����
BNP/NT-proBNP ���� ���� ���� ����
Echocardiography ���� ���� ����
RHC ���� ���� ����
Galiè N, et al. Eur Heart J 2009; 30:2493-537.
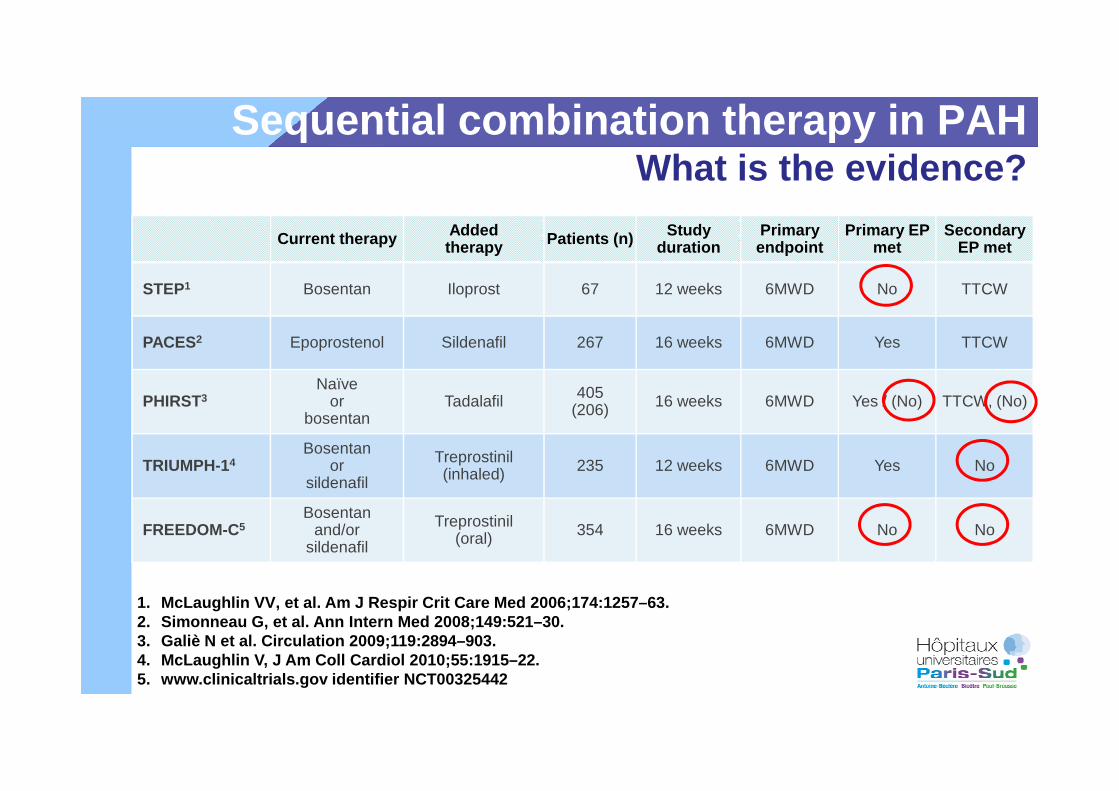
Current therapy Addedtherapy Patients (n) Study
durationPrimary endpoint
Primary EP met
Secondary EP met
STEP1 Bosentan Iloprost 67 12 weeks 6MWD No TTCW
PACES2 Epoprostenol Sildenafil 267 16 weeks 6MWD Yes TTCW
PHIRST3Naïve
or Tadalafil 405 16 weeks 6MWD Yes / (No) TTCW, (No)
Sequential combination therapy in PAHWhat is the evidence?
PHIRST3 orbosentan
Tadalafil 405(206) 16 weeks 6MWD Yes / (No) TTCW, (No)
TRIUMPH-14Bosentan
orsildenafil
Treprostinil(inhaled) 235 12 weeks 6MWD Yes No
FREEDOM-C5Bosentan
and/orsildenafil
Treprostinil(oral) 354 16 weeks 6MWD No No
1. McLaughlin VV , et al. Am J Respir Crit Care Med 2006;174:1257–63. 2. Simonneau G, et al. Ann Intern Med 2008;149:521–30.3. Galiè N et al. Circulation 2009;119:2894–903. 4. McLaughlin V, J Am Coll Cardiol 2010;55:1915–22.5. www.clinicaltrials.gov identifier NCT00325442
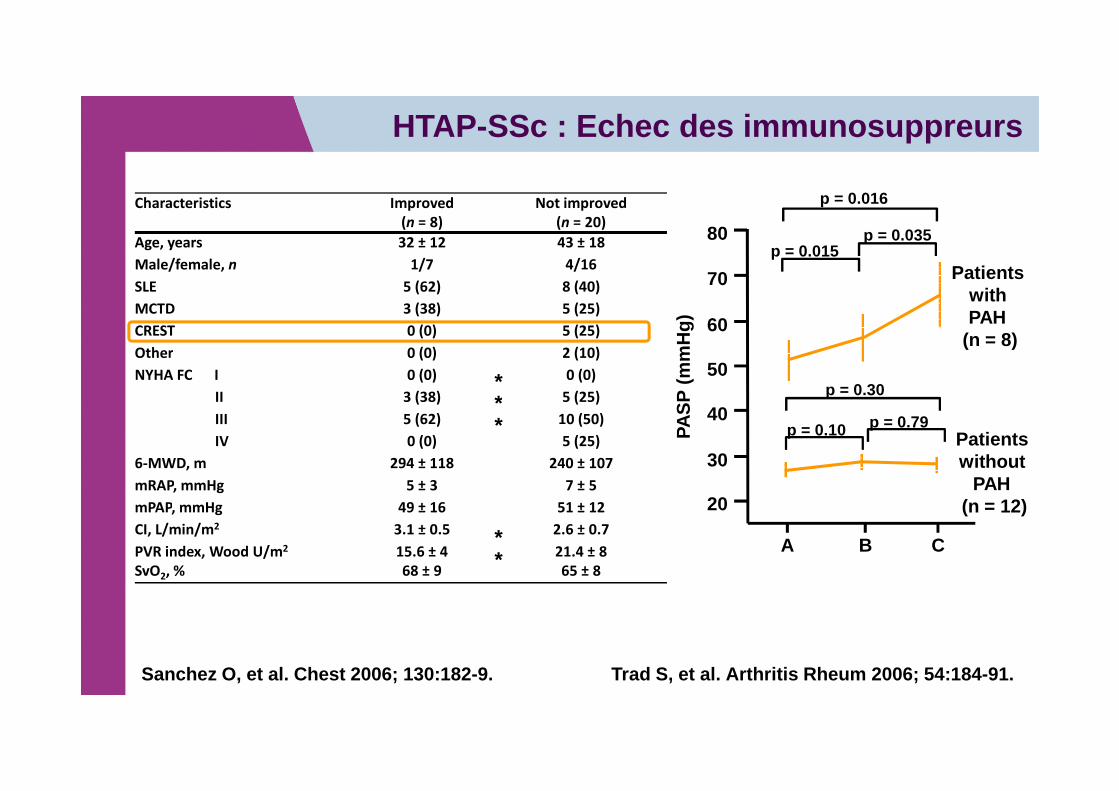
Characteristics Improved
(n = 8)
Not improved
(n = 20)
Age, years 32 ± 12 43 ± 18
Male/female, n 1/7 4/16
SLE 5 (62) 8 (40)
MCTD 3 (38) 5 (25)
CREST 0 (0) 5 (25)
Other 0 (0) 2 (10)
NYHA FC I 0 (0) 0 (0)
II 3 (38) 5 (25)**
50
60
70
80
PAS
P (
mm
Hg)
Patients with PAH
(n = 8)
p = 0.016
p = 0.015p = 0.035
p = 0.30
HTAP-SSc : Echec des immunosuppreurs
II 3 (38) 5 (25)
III 5 (62) 10 (50)
IV 0 (0) 5 (25)
6-MWD, m 294 ± 118 240 ± 107
mRAP, mmHg 5 ± 3 7 ± 5
mPAP, mmHg 49 ± 16 51 ± 12
CI, L/min/m2 3.1 ± 0.5 2.6 ± 0.7
PVR index, Wood U/m2 15.6 ± 4 21.4 ± 8
SvO2, % 68 ± 9 65 ± 8
* p < 0.05
**
**
A B C
20
30
40
PAS
P (
Patients without
PAH (n = 12)
p = 0.30
p = 0.10 p = 0.79
Sanchez O, et al . Chest 2006; 130:182-9. Trad S, et al . Arthritis Rheum 2006; 54:184-91.
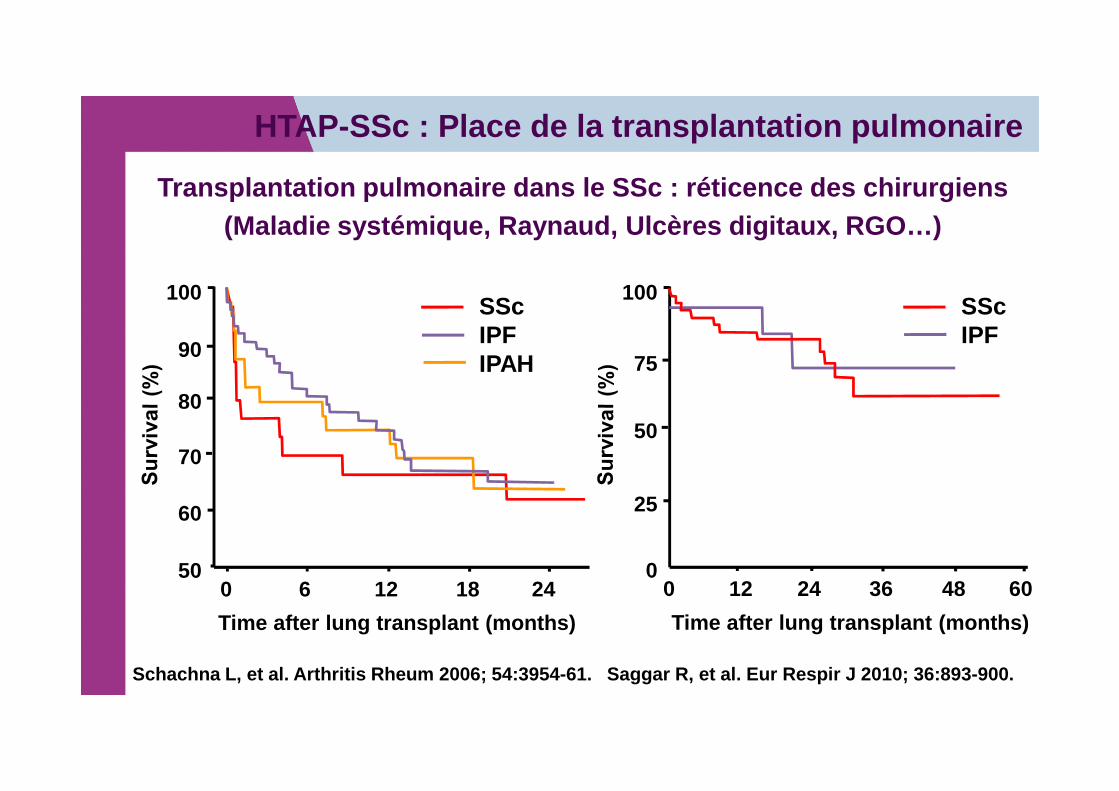
Transplantation pulmonaire dans le SSc : réticence d es chirurgiens (Maladie systémique, Raynaud, Ulcères digitaux, RGO …)
100
80
100
7590
SScIPFIPAH
SScIPF
HTAP-SSc : Place de la transplantation pulmonaire
80
70
60
50
Time after lung transplant (months)
0
50
25
0
Time after lung transplant (months)
6 12 18 24 0 12 24 36 48 60
Schachna L, et al. Arthritis Rheum 2006; 54:3954-61. Saggar R, et al. Eur Respir J 2010; 36:893-900.
� Malgré les progrès importants réalisés dans la prise en charge thérapeutique de l’HTAP, le pronostic de l’HTAP associ ée à la SSc reste médiocre
� Les pistes d’amélioration de la survie sont:
� Un dépistage efficace afin de diagnostiquer des formes moinssévères de la maladie
HTAP-SSc : Conclusion
sévères de la maladie
� Une approche thérapeutique plus aggressive ?
� “Treat-to-target strategy” ?
� Combinaisons thérapeutiques précoces ?
� Une approche multidisciplinaire est indispensable dans l a prise en charge des patients souffrant d’HTAP associée à la SSc



![Sclérodermie et syndrome des anticorps … · la sclérodermie systémique [7,8]. Parmi ces travaux scientifiques qui ont étudié la fréquence des anticorps antiphospholipides,](https://img.pdfslide.tips/doc/110x75/5b9a3e0f09d3f207308d6082/sclerodermie-et-syndrome-des-anticorps-la-sclerodermie-systemique-78.jpg)