Embed Size (px)
Citation preview
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Atelier Transplantationd’Organes SolidesTransplantation Pulmonaire
O Brugière (Hôpital Bichat)

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Plan• Infections fongiques chez les Transplantés pulmonaires
– Facteurs de risque– Formes cliniques– Fréquence des AI dans un centre de Tx pulmonaire– Fréquence des colonisations Aspergillaires– Colonisation à champignons filamenteux non Aspergillus
• Prophylaxie anti-fongique en Tx Pulmonaire– Attitude centre Bichat– Etude des pratiques internationales
• Suivi therapeutique Azolés– Données littérature– Expérience Bichat– Intérêt pour limiter toxicité des surdosages

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Facteurs de Risque d’Infection Fongiques en Tx
Pulmonaire
- Risque environnemental: Travaux hospitaliers. Contamination système traitement de l’air
- Colonisation aspergillaire pré-Tx (persistance sur poumon natif si mono-greffe). 3%-20% d’AI post-Tx (1)
- Site anastomotique bronchique si retard de cicatrisation.
- Altération clairance muco-ciliaire et reflexe de toux
- Intensité immunosuppression: SAL ++
- Rejet chronique
(1) Gavalda J, Clin Infect Dis 2005.

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Formes cliniques Infections Aspergillaires en Tx pulmonaire
– Colonisation bronchique aspergillaire: Cultures positives, en l’absence de trachéobronchite ou d’AI: fréquence +++
– Trachéobronchite Aspergillaire:
forme spécifique du greffé pulmonaire.
– Aspergillose Invasive pulmonaire ou disseminée:
présentation habituelle classique. Pronostic sévère.
– Autres formes: Aspergillome, Aspergillose chronique nécrosante
plus rares (sur le poumon natif). ABPA exceptionnelle

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Infections Fongiques Invasives post-TxP
Expérience Hôp. Beaujon-Bichat
• > 400 Tx pulmonaires. 35 Tx/an
• Epidémie infections aspergillaires Nov 1991-Janv. 93 (Travaux)
– 7 Aspergilloses invasives
• 6 AI pulmonaire: 1 cas de trachéo-bronchite
• 5 décès sous ttt AmB IV
– 6 colonisations aspergillaires
• 4 patients ttt AmBisome lors traitement de rejet aigu
• 2 patients non traités: retour à domicile
• Période 2006-2012:
– 3 AI, 1 décès

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Relationship between colonization of lung transplant recipients and fungal contamination of the hospital environment
Figure 1. Distribution of the fungal species and species of Aspergillusin the environment of intensive care units (A) and pneumology units (B).
Etude Bichat: 44 patients, période 16 mois 2010-2011. Suivi longitutinal J0-3 mois

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Relationship between colonization of lung transplant recipients and fungal contamination of the hospital environment
Etude Bichat sur 16 mois (2010-2011)
44 patients suivi 3 mois: 11 cas de colonisation aspergillaire

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Table IV. Comparison of the ITS sequences, beta-tubulin and actin between clinical isolates of Aspergillus and of strains of the same species found on the same dates (± 2 weeks) in the environment.
Results are expressed by comparison with the clinical isolate by specifying, for very close sequences, the number of different bases.

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
• Etude rétrospective sur 10 ans de 517 patients TP
• 75 patients présentant des prélèvements positifs à champignons filamenteux
• 85 souches : Cladosporium sp (41%), Phialemonium (16,5%), Zygomycètes (14%), Scedosporium sp (7%), autres (11,5%)
• 63% des isolats chez patients sous prévention aspergillaire: VORI, FCZ, ITRA. Activité de l’azolé sur champignon: 33%
• 1 seule infection probable à Mucor sp chez un patient
• Pas de modification des recommandations de traitement prophylactique chez ces patients
Silveira FP et al. J Heart Lung Transplant 2008, 27:850-5.
Post Tx colonization with non Aspergillus mold and risk of invasive fungal disease in lung transplant récipients
J Heart Lung Transplant 2008,

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Prophylaxie anti-fongique
en Tx pulmonaire (Protocole centre Bichat)
Préventif
1993-2006: Aérosols (25 mg) + spray nasal AmB (1 mg/ml)
+/- Itra en preemptive therapy
> 2006: - Preemptive therapy
= Voriconazole si colonisation bronchique aspergillaire post-op et retard de cicatrisation bronchique.
= Switch Posaconazole si hépatite
Curatif d’une AI: standard

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
58 centres LTx: 58% de prophylaxie universelle 6 premiers mois (n = 34 centres), 36% de pre emptive therapy (n = 21 centres), 5% abstension
Prophylaxie ou pre-emptive ttt ciblées sur Aspergillus: 94% des cas.
Prophylaxie anti-fongique
en Tx pulmonaire (Données internationales)

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Suivi thérapeutique des Azolés dans les centres de greffes pulmonaires
Suivi thérapeutique: données de la littérature (1)

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Suivi thérapeutique: données de la littérature (2)

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Expérience Bichat: Suivi therapeutique VORI chez receveurs Tx pulmonaires
NOM DateRésultat en
mg/Lvoie dose Temps cinet
Pir. De ACandidémie à C.
parapsilosis, Caspo puis 22/03/2011 4.8 p.os 200 T2H
Gran Y OliColonisation bronche
Paecilomyces, Aspergillus 21/04/2011 0.3 p.os 200 T0
Gran Y Oli 06/05/2011 1.7 p.os 200 T2H
Bor. CCandidose R buccale et
oesophagienne12/05/2011 1.8 p.os 200 T4H
Bor C 06/07/2011 2.2 p.os 200 T4H
Bor C 14/03/2012 2.8 p.os 200 T4H
Coi J Suspicion d'AI (infirmée) 16/05/2011 7.3 200 T2H
Ques CSuspicion AI, Oesophagite
+++ et IPP x313/05/2011 0.6 p.os 200 T0
Ques C 26/04/2011 0.0 p.os 200 T2H
Ques C 02/05/2011 0.8 p.os 200 T0
Ques C 03/05/2011 0.7 p.os 200 T1H
Ques C 03/05/2011 0.6 p.os 200 T0
Ques C 04/05/2011 0.5 p.os 200 T0
Ques C 06/05/2011 0.6 p.os 200 T0
Ques C 23/05/2011 0.7 p.os 350 T0
Ques C 27/05/2011 1.1 p.os 350 T3H
Ques C 30/05/2011 0.9 p.os 200 T0
Ques C 30/05/2011 1.0 p.os 200 T4H
Dela Na AI probable 17/05/2011 4.2 p.os 200 T2H
Dela Na 25/06/2011 2.9 p.os 200 T2H
Perron L. AI probable 18/11/2011 1.8 p.os T4H
Perron L. 08/12/2011 0.1 p.os 100 T0
Perron L. 12/12/2011 0.8 p.os 125 T0
Perron L. 10/01/2012 0.0 p.os 125 T0
PousColonisation aspergillaire
+ retard cicatrisation 02/03/2012 1.2 p.os T4H
VengeColonisation aspergillaire
+ retard de cicatrisation03/08/2012 0.6 p.os ?
Bae P. Colonisation à Mucor 08/08/2012 2.0 p.os 200 T0
Bae P. 08/08/2012 2.6 p.os 200 T2H
Bae P. 24/08/2012 3.6 p.os 200 ?
Bae P. 19/09/2012 0.9 p.os 200 T0
T2H? Concentrations assez constantes pour même patient (littérature contradictoire)< 1microg/ml: risque majoré inefficacité. > 5 microg/ml: risque majoré de toxicité

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Suivi thérapeutique
VORICONAZOLE hepatotoxicity in a LTx recipient.Transpl Infect Dis. 2011
• 46-yr-old LTx with pulmonary Aspergillus colonization (>50 colonies of Aspergillus terreus) at M3
• VORI 200 mg b.i.d.
• J 30 VORI : ALT and AST = 223 and 188 UI/L, respectively
• reduction of voriconazole to 100 mg b.i.d. cholestatic hepatitis resolved 10 days later.
• adequate VORI plasma concentrations (0.98 mg/L) 30 days after dose reduction and no more colonies of Aspergillus
• VORI therapeutic drug monitoring before and after dose reduction may help to avoid drug accumulation and inappropriately low drug exposure, respectively.

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Conclusion
• Tx pulmonaire: Incidence élevée colonisation et trachéobronchite à Aspergillus ou autres filamenteux
• Prophylaxie prolongée fréquente par azolés, sans recommandations très établies, avec probable diminution des AI fatale.
• Suivi thérapeutique recommandé des azolés admis mais peu pratiqué en clinique
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Dr Clément PICARD
Service de pneumologieHôpital Foch, Suresnes (92)Mail: [email protected]
Dosage des azolés après transplantation pulmonaire.Une année de greffe à Foch.
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Population d’étude
• Analyse rétrospective des patients transplantés pulmonaire entre janvier et décembre 2011
• Mono-centrique (Foch)
• N=56
• 54 TP Uni ou bilatérale
2 Tx combinées poumon + (1rein, 1 foie)
• H/F: 21/35
• Âge (médiane [25; 75]): 34.5 ans [24; 46]

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Pathologie motivant la greffe
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Résultats
Antifongique azolé utilisé chez 20 patients (36%):
– 4 candidoses systémiques ou muqueuses : fluconazole,
– 11 aspergilloses invasives probables ou certaines + 5 colonisations aspergillaires : voriconazole (15) / posaconazole (1)
+/- assocation à caspofungine (6)

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Délai greffe-azolé
0 100 200 300 400 500
jours post-transplantation
Délai greffe-azolé médian : 55 jours [12; 126]

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Etude des 15 cas d’aspergillose sous voriconazole
• Dosage des taux sériques réalisés chez 13 patients
• 7 ont nécessité une majoration de la posologieà 250 mg X 2/ jour (3) ou 300 mg X 2 / jour (4).
• Comparaison des patients nécessitant une dose majorée (MAJ) à ceux nécessitant une dose standard (STD).

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Comparaison patients à doses majoréesaux autres: rôle du terrain.
Age
STD MAJ
0
10
20
30
40
50
60
p=0,26
Index de Masse Corporelle
STD MAJ
0
5
10
15
20
25
30
p=0,065
Rôle possible d’un index de masse corporel <17 kg/m2 ?

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Rôle de la pathologie et des traitements associés?
STD
N=8
MAJ
N=7
Comparaison
(p)
Mucoviscidose 5 5 NS
I. pancréatique Exocrine
4 5 NS
Sd Occlusif 2 1 NS
Diabète 4 0 NS (0.08)
IPP 8 7 NS
IPP X 2 1 2 NS
Autres tt ? ? -
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
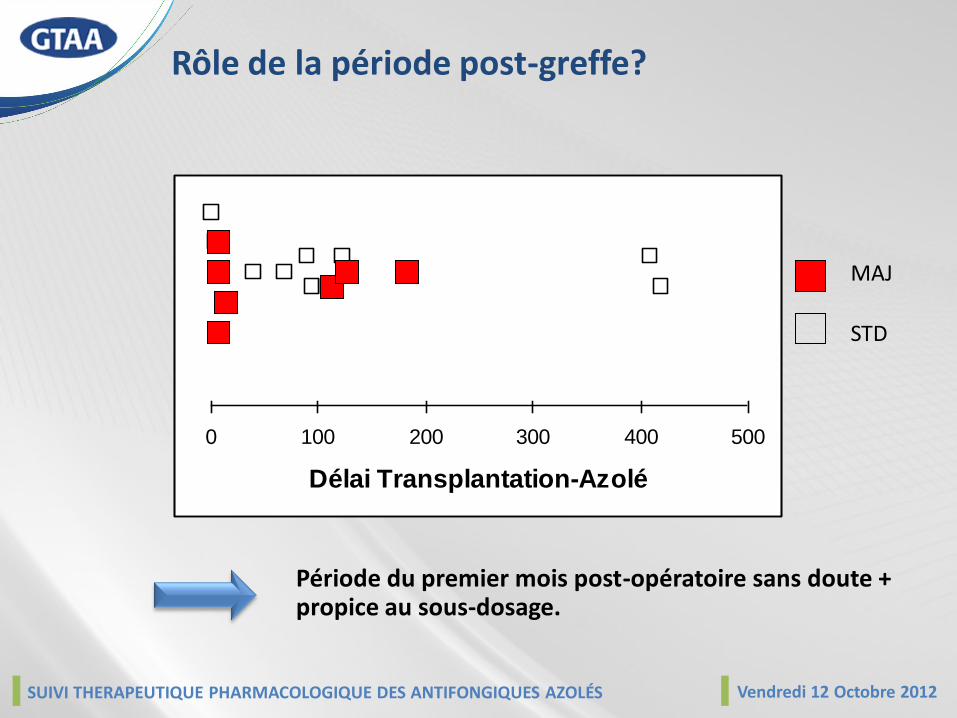
Période du premier mois post-opératoire sans doute + propice au sous-dosage.
0 100 200 300 400 500
Délai Transplantation-Azolé
MAJ
STD
Rôle de la période post-greffe?
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Evolution clinique de la mycose
Favorable dans tous les cas sauf un
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Conclusions
• Utilisation fréquente des azolés en curatif après TP en l’absence de prophylaxie.
• Nécessité fréquente d’adaptation posologique: dosage systématique (notamment en période post-opératoire).
• Nécessité de simplifier la filière du dosage:– Accès du pharmacologue aux prescriptions associées (informatique).– Accès au dosage en ville et transmission au clinicien.

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Vendredi 12 Octobre 2012 – 9h30Cyclone – 16 rue Vulpian – 75013 Paris

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Atelier Transplantationd’Organes SolidesTransplantation Pulmonaire
Eliane M Billaud
Pharmacologie (HEGP)

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Atelier Transplantationd’Organes SolidesTransplantation Pulmonaire
Eliane M Billaud
Pharmacologie (HEGP)
GTAA 2011

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
STP des Antifongiques?
- Analytique- Index thérapeutique étroit efficacité (échec thérapeutique)
sécurité (toxicité)
- Terrain à pronostic vital engagé
- Variabilité PK concentrations imprévisiblesPGxadhérence au traitement
- Coprescriptions, IAM
Individualisation de la thérapeutique AF?Enjeu : détection changement concentration relevant au plan clinique
D’après Ensom MH

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Person AK Infect Dis Clin North Am 2010
Moment de la survenue de l’IFI en fonction du type de transplantation
Importance de la prise en charge à la phase précoce
Importance des comorbidités
Johnson HJ AAC 2010
Tx Hépatique VRZ en Tx Hépatique : variabilité des concentrationsProphylaxie orale 200 mg q12
Tx Pulmonaire
Han K AAC 2010
POUMON = organe cible infection opportuniste, Asp, CMV
Tx PULMONAIRE, notamment CF :Prophylaxie primaire du greffonmais secondaire du patientchez un receveur immunodéprimé, A considérer comme un enjeu CURATIF
Billaud EM Med Myc, 2010
Modifications du terrain mucoviscidose (CF) :
risque de sous-exposition médicamenteuse
et de toxicités additionnelles- clairances reliées au plus jeune âge- GERD, fonction digestive- variabilité PK augmentée- coprescriptions nombreuses

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Spécificités
Localisation
La question: Apport du STP pour conduire une augmentation de dose en cas de localisation profonde comme une endophtalmie fongique? [Spriet I JAC 2009]
passages intracellulaire, intra-pulmonaire démontrés
Pathogènes Ex: Scedosporium spAssocié à un pronostic très péjoratif /ID [Morio F, 2010]Considéré usuellement comme une contre-indication à la Tx
Pédiatrie Prendre en compte la classe d’âge (NN ; 2-12 ans; 12-18 ans)
et le POIDS

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Prise en compte des Conséquences cliniques
Interactions, aspects quantitatifs
Interactions, relais et arrêt de traitement
Difference of inhibition on FK metabolism between azoles
ITZ > VRZ > PSZ
Individual TDM basis DDI management : switch and withdrawal
Rôle des corticoïdes?Chronique au long cours
Bolus en aigu
Rôle de la voie d’administrationCYP3A4 / Pgp = hépatique + intestinal
ΔBD +IAM

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Modification de la concentrationConséquences
Surdosage
augmente à la fois toxicités spécifiques
et effet thérapeutique (cf IS)
Surimmunosuppression,
Entretient le lit de infection opportuniste
Sous-dosage
Diminue l’efficacité
Risque d’émergence de résistance (cf AF)
IS et AI
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
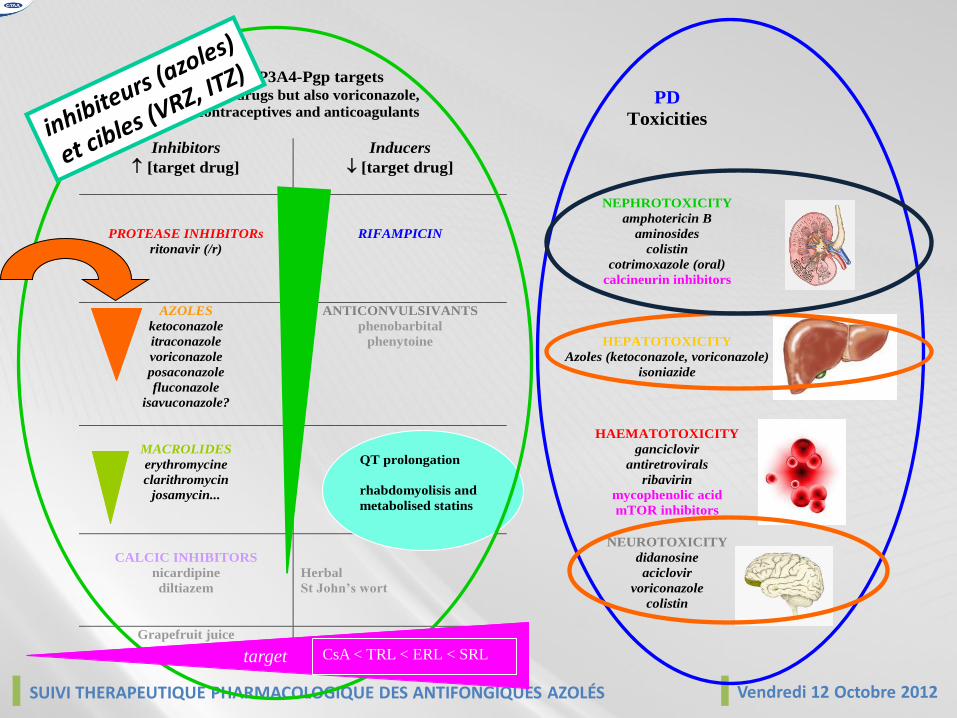
PK CYP3A4-Pgp targets such as IS drugs but also voriconazole,
oral contraceptives and anticoagulants
Inhibitors
[target drug]
Inducers
[target drug]
PD
Toxicities
PROTEASE INHIBITORs
ritonavir (/r)
RIFAMPICIN
NEPHROTOXICITY
amphotericin B
aminosides
colistin
cotrimoxazole (oral)
calcineurin inhibitors
AZOLES
ketoconazole
itraconazole
voriconazole
posaconazole
fluconazole
isavuconazole?
ANTICONVULSIVANTS
phenobarbital
phenytoine
HEPATOTOXICITY
Azoles (ketoconazole, voriconazole)
isoniazide
MACROLIDES
erythromycine
clarithromycin
josamycin...
HAEMATOTOXICITY
ganciclovir
antiretrovirals
ribavirin
mycophenolic acid
mTOR inhibitors
CALCIC INHIBITORS
nicardipine
diltiazem
Herbal
St John’s wort
NEUROTOXICITY
didanosine
aciclovir
voriconazole
colistin
Grapefruit juice
QT prolongation
rhabdomyolisis and
metabolised statins
CsA < TRL < ERL < SRLtarget

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
IAM : IPP et Azolés
IPP, métabolisme et VRZ
tous ne relèvent pas du même schéma métaboliqueil faudrait donc les considérer un à un en terme de profil métabolique
IPP, pH et absorption du PSZ
ces médicaments sont supposés améliorer la fonction digestive!

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
STP PSZ Onco-hématologieIGR
Nombre de dosages / patient : Sept. 2009 - Sept. 2012
6,2
1,6
2,1
0
1
2
3
4
5
6
7
Sept 2009 - Sept 2010 Sept 2010 Sept 2011 Sept 2011 - Sept 2012
Période
No
mb
re d
e d
osa
ges
par
pat
ien
tsSuivi Thérapeutique Pharmacologique : PSZ 2009-2012
0
200
400
600
800
1000
1200
1400
1600
2009 2010 2011 2012
Années
[PS
Z]
ng
/mL
Premier dosage
Moyenne / année
Modification prescriptions :IPP vers antiH2
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
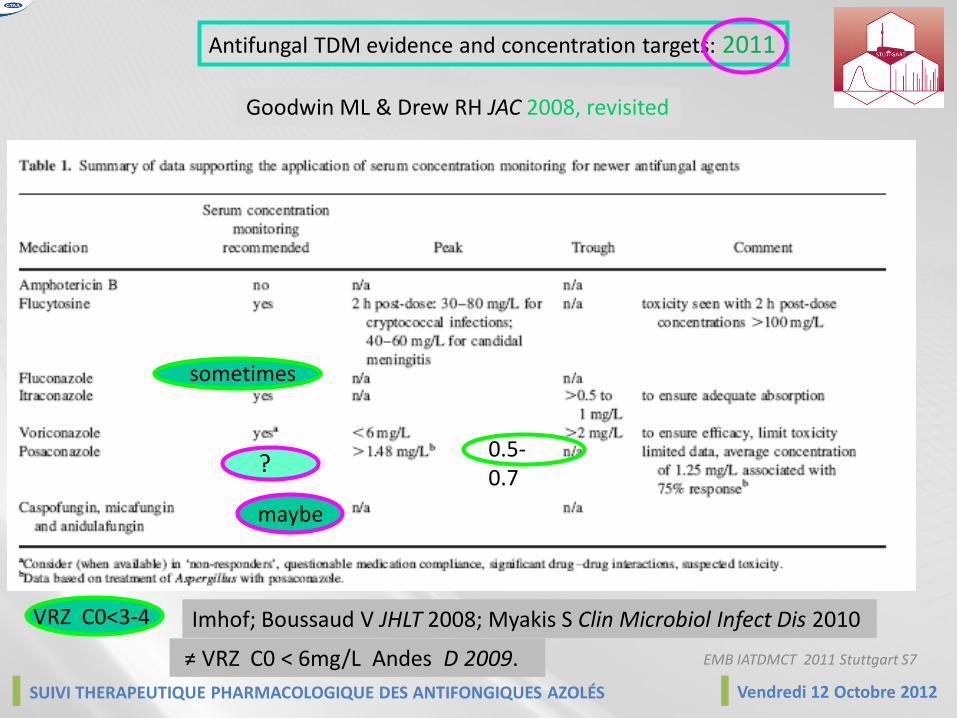
Goodwin ML & Drew RH JAC 2008, revisited
Antifungal TDM evidence and concentration targets: 2011
maybe
0.5-0.7
sometimes
EMB IATDMCT 2011 Stuttgart S7
VRZ C0<3-4 Imhof; Boussaud V JHLT 2008; Myakis S Clin Microbiol Infect Dis 2010
?
≠ VRZ C0 < 6mg/L Andes D 2009.

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
0 10 20 30 40 50
Trough:MIC
0.50
0.60
0.70
0.80
0.90
1.00
Pro
babi
lity
of C
linic
al R
espo
nse
0 1 2 3 4 5 6 7 8 9 10
Voriconazole trough concentrations (mg/L)
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
Prob
abilit
y effe
ct or
toxic
ity
Effect Toxicity
Troke AAC 2011
VRZ : relation concentration-effect & concentration-toxicity
Pascual et al CID 2008
Trough : MIC as a therapeutic target
2-5
D’après W Hope, IATDMCT 2011

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
combinaison AF
The high risk of inefficacy during underdosed periods was supplied by the use of
antifungal associations, specially with caspofungin,
[Marr 2004][Singh 2006]
supported by an individualized concentration-controlled adaptation,
waiting for (VRZ) documented concentration
On PK basis
Berge M TID 2009

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
STP Conclusion (2) : niveau de preuve
A lot of reviews *Smith and Andes, 2009; Hope 2008…+
Valuable recommendations [Walsh 2008, Singh and Husain, 2009]
Few studies, most of them retrospective series
Mais évidence émergente, au moins pour populations spécialesheureusement très représentatives
CF, haemato GERD, mucositis pediatricslow exposure
Ageing Hepatic insufficiency (PK) high exposurehigher sensitivation (PD) high toxicity
Underlying Tx, BMT, HIV DDI +++BK
Long course compliance, steady-state control
STP besoin d’études collaboratives prospectives…..certesmais déjà utilisé et utile….OUI
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Tendance- STP pleinement reconnu en Infectiologie, avec des essais appropriés- Nombreuses publications avec toujours beaucoup de revues
mais plus de data originaux, confortant perception initiale du management AF
Généralités qui s’appliquent aux médicaments AF- Effet de l’âge sur la clairance- Pathologie sous-jacente, désordres digestives et absorption
Considérations spécifiques liées à l’AFVRZ le plus de challenges- en terme d’index thérapeutique (faible exposition, même IV), tolérance- cible d’interactions
STP joint pour gérer les aspects quantitatifs de leurs interactions - mais positif en curatif (voie IV , dose de charge)
Difficile à maintenir au long cours (photosensibilisation)
PSZ - Prophylaxiecourt-terme (hématologie): besoins en STP limités, détection des ss-dosagesentretien au long cours : Scedo +- moins adapté au ttt curatif (sauf justification PD)
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
The Echinocandins
The question:
Is there any benefit of caspofungine dose-escalation?In a TDM-based approach for a large therapeutic index drug?
That is:
- Reality of the 1mg/L threshold target [Bartizal K 1997]
- Benefit to increase dosage, targeting overexposure to overcome* emerging problems of resistance * localisations hardly achievable
- Benefit to increase dosage, to overcome documented underexposure * Intensive Care
EMB IATDMCT 2011 Stuttgart S7

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Atelier Transplantationd’Organes SolidesTransplantation Pulmonaire
Eliane M Billaud
Pharmacologie (HEGP)
GTAA 2012 Eléments nouveaux?

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Suivi thérapeutique des Azolés dans les centres de greffes pulmonaires
Suivi thérapeutique: données de la littérature (1)

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Suivi thérapeutique: données de la littérature (2)

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
ISHLT Monograph series Vol 5, 2011Infectious diseases Management / Thoracic Tx
Chapter 10 TDM
- DDIs/ADR- Route of administration- Onset and strength of the interaction- PD (renal and hepatic functions)- Ethnicity (PGx)- CF- Age-related PK- Gastric acid alteration and drug absorption
Uber P et Billaud EM
Key Points for TDM
- Which levels- Turnaround time- Target level (B/R)- Timing- Interpreting results- Methods
Table 1 : Elements of evidence
Table 2 : C0 targets

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
ITZ
VRZ
PSZ

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
ISHLT Infectious Diseases CommitteEvidence for TDM

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Ther Drug Monit. 2012 Feb;34(1):72-6.Posaconazole: the case for therapeutic drug monitoring.Howard SJ, Felton TW, Gomez-Lopez A, Hope WW.
Drug exposure targets associated with therapeutic efficacy
0,7mg/L à adapter à la situation clinique {>0,5 mg/L en prophylaxie; 1,25mg/L en curatifPeu de rationnel / toxicité
A pragmatic approach to TDM of PSZ
Should all patients receiving PSZ have TDM? ,D’autant plus que curatif et contexte graveSample Times: When should they be taken and How many are required? ,0,35 mg/L à J2, critère intermédiaire /état d’équilibre)Management of patients with subtherapeutic concentrations{rechercher causes : repas, pH, interaction, observance{dose >>800mg/j ….mais il faut être patient!!!

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
300-400 mgx2 PO200-300 mgx2 IV
1,5 - 4,5 mg/L
surtout hémato

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
300-400 mgx2 PO200-300 mgx2 IV
1,5 - 4,5 mg/L
RCP Dose de charge
IV 6 mg/kg x2soit 390 mgx2 pour 65kg
PO 400mgx2
BD théorique 96%
surtout hémato

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
PSZ plasma concentrations have been investigated in a retrospective haematology study, showing lowerexposure in youth and/or digestive disorders [12]. Similar pitfalls have been reported in cystic fibrosis lungtransplantation [13]. Several patients remained underexposed to PSZ despite dose adaptation above1g/day, +35% as compared to recommendations. It seems important to identify low exposure to PSZ,specially in case of curative treatments. The very long delay to steady-state (weeks) and the difficulty toovercome saturable absorption even with split doses, together with the lack of IV route, should encouragea switch to another antifungal rather than a dose escalation for curative issues.
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
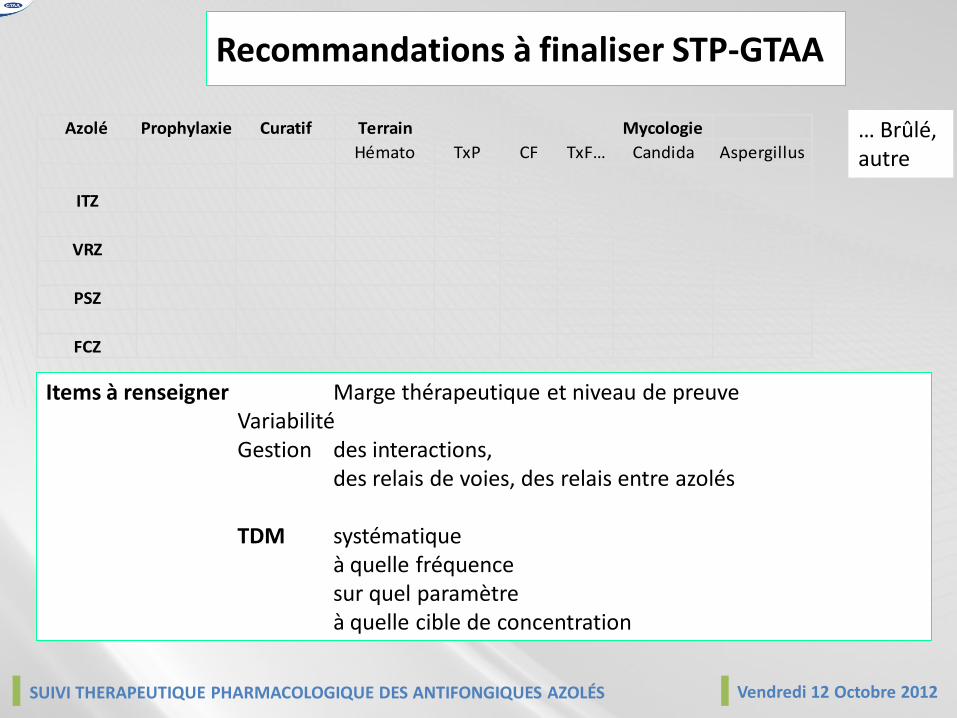
Recommandations à finaliser STP-GTAA
Azolé Prophylaxie Curatif Terrain Mycologie
Hémato TxP CF TxF… Candida Aspergillus
ITZ
VRZ
PSZ
FCZ
Items à renseigner Marge thérapeutique et niveau de preuveVariabilité Gestion des interactions,
des relais de voies, des relais entre azolés
TDM systématiqueà quelle fréquencesur quel paramètreà quelle cible de concentration
… Brûlé, autre

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Perspectives
1- Reste notamment à répondre
- CF vs CF /âge
- CF Tx vs CF Tx / corticoïdes
2- Objectifs thématiques (hors ARV)
- IATDMCT : AF Committee (2007) / AI Committee (2011)- STP : groupe de travail AF / AI (2012)- GTAA 2011-2012 …..... GTAI 2013 ?
SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
MERCI DE VOTRE ATTENTION

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
■ The seven colonized patients were treated with VRZ (n=6) or PSZ (n=3)
Case series (8) CFLTx with Scedosporium sp
■ VRZ was stopped in 3 cases, 2 switch to PSZ
■ AF therapy interrupted in 3 situations : success, complications, compliance
Working group - Fungal respiratory infections in CF-Angers – 1st/2nd September 2011
0 12 24 36 48 60 72 84 96 108 120 132
#1
#2
#3
#4
#5
#6
#7
Pati
ents
Months post-Tx
VRZ
PSZ
†
†
†

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
STP des azoles
IATDMCT 2011 # 143
Due to azole pharmacokinetic variability in CFLTx patients, the steady-state is longer to reach,and higher dosages with careful TDM are needed to achieve appropriate therapeutic efficacyand safe immunosuppressive drug-drug interactions
C0 plasmatiques moyens acceptables à
1.4 ± 0.7 mg/L (VRZ)
0.8 ± 0.6 mg/L (PSZ )
Doses d’entretien moyennesVRZ 530 ± 174 mg/j (+43%)PSZ 1550 ± 638 mg/j (+200%)
Examples of combined TDM of PSZ and tacrolimus (TRL)
0
5
10
15
20
0 20 40 60 80 100
0
0,5
1
1,5
2
2,5
3
3,5
0 20 40 60 80 100
0
500
1000
1500
2000
2500
0 20 40 60 80 100
0
200
400
600
800
1000
1200
0 20 40 60 80 100
0
5
10
15
20
0 20 40 60 80 100
0
0,5
1
1,5
2
2,5
3
3,5
0 20 40 60 80 100
0
500
1000
1500
2000
2500
0 20 40 60 80 100
0
200
400
600
800
1000
1200
0 20 40 60 80 100
C0 TR
L(n
g/m
L)
D TR
L (m
g/24
H)
C0 PS
Z(n
g/m
L)
D PS
Z (m
g/24
H)
EMB IATDMCT 2011 Stuttgart S7

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
0,0
2,0
4,0
6,0
8,0
10,0
12,0
0 200 400 600 800 1000
Dose (mg/d)
C0
(mg/
L)
Tx(+) CF (+)
Tx(+) CF(-)
Tx(-) CF(-)
VRZ : C0 selon la dose et le type de patient
La dose nécessaire pour atteindre des concentrations de VRZ thérapeutiques en CF Tx ()
Est en moyenne plus haute and plus variable par rapport aux patients trnasplantés non CF() ou non transplantés ().
Adaptations conduites > 800 mg/j nécessaires pour atteindre concentrations détectables
[Imhof 2006,Pascual 2008,Berge, 2009]

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
*1/*17 *1/*1 *1/*20
5
10
15
20
CYP2C19 genotype p<0.01
VRZ Dose
mg/kg/day
Cystic fibrosis Lung Tx
[Berge, 2010]
400 mg
600 mg
[Ikeda 2004, Weiss 2009]
PGx contribution of CYP2C19 polymorphism in VRZ variability

SUIVI THERAPEUTIQUE PHARMACOLOGIQUE DES ANTIFONGIQUES AZOLÉS Vendredi 12 Octobre 2012
Vendredi 12 Octobre 2012 – 9h30Cyclone – 16 rue Vulpian – 75013 Paris