Embed Size (px)
DESCRIPTION
crohn's disease referat
Citation preview

TUMOR-TUMOR TULANG
Rachmat SalehBagian Radiologi
Fak. Kedokteran Unhas

Klasifikasi histologis tumor-tumor tulang berdasarkan : Pemeriksaan sitologi
osteocyte/osteoblastchondrocyte/chondroblastosteoclast,etc
Bentuk (Arsitektur) Tipe dari matriks yang dihasilkan oleh sel tumor

Tumor Primer (primary bone tumor) Tumor Jinak (Benign Tumor)
Giant cell tumor Tumor Ganas (Malignant Tumor)
Osteosarcoma Tumor sekunder / secondary bone tumor (metastase) Lesi mirip tumor / Tumor like lesion
Aneurysmal bone cyst



Proliferasi sel stromal mononuklear Osteoclastik multinucleated giant cell
Usia : 20–45 th Lokalisasi : Metafisis Epifisis Subartikuler Predileksi :
Distal femur proximal tibia distal radius sacrum
Metastasis ke paru 2% Gejala klinis :
Nyeri istirahat Local swelling Pergerakan sendi sekitar terbatas Fraktur patologis (10-12%) Gejala neurologis (spine lesion)

Radiologis Central/eksentrik, ekspansif Lesi radiolusen (litik) Batas tidak tegas Bersepta-septa (foam like app.) Zona transisi antara tulang normal dan patologik (<1 cm) Penipisan korteks dan + periosteal reaction

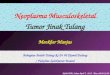
A. GCT of the distal femur in a 68-year-old woman. AP radiograph shows the lesion (arrows) approaching the end of the bone. B. GCT of the distal radius in a 16-year-old girl. Radiograph shows that the giant cell tumor originates in the metaphysis (asterisk), and in this patient with a partially open physis, the tumor has crossed the physis (black arrow) and extends to the end of the bone
A B

Malignant bone producing tumor Pertumbuhan tak terkendali dari osteoblast dan
osteoclast Usia : 10–30 th Lokalisasi : >> metafisis tulang panjang Predileksi :
Distal femur Proximal tibia, Hip Shoulder
Metastasis ke paru , tulang, kel. limfe Gejala klinis nonspesifik
Nyeri Swelling Riwayat trauma Fraktur patologis (15-20%)

RadiologisBentuk osteolitik
Batas tidak tegas Periosteal new bone formation Codman’s
triangle Kalsifikasi dan pembengkakan
Bentuk osteoblastik/osteogenik Batas irregular Kalsifikasi jaringan lunak densitas Reaksi periosteal Sunray/sunburst app. Soft tissue swelling
DD/Ewing’s sarcoma Onion skin app.

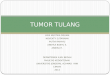
Osteosarcoma of the distal femur with periosteal reaction and so tissue mass. a Anteroposerior radiograph of the distal femur shows a small triangle of interrupted periosteal reaction (arrow) at the superior margin or the tumor (Codman triangle). Note that the lesion shows areas of sclerosis (large asterisk) and lysis (small asterisk). b Lateral radiograph shows the associated so tissue mass (arrows) to better advantage
a b

a.Osteosarcoma of the distal fibula-predominantly osteoblastic. Amorphous calcification/ossification is present in the soft tissues withcortical destruction and a little periosteal new bone formation.b. Osteosarcoma of the distal femur predominantly chondroblastic. Note the well-defined soft-tissue mass and radiating spiculation of calcification within it. Sclerosis and lysis are present within the medullary cavity that is slightly expanded
a b

Reactive vascular phenomenon or secondary to another lesion or trauma
Klasifikasi : Primary ABC (70%) Secondary ABC (30%)
Usia : 5–20 th Lokalisasi : >> metafisis tulang panjang, short tubular
bones, pelvis, axial and craniofacial skeleton

Predileksi : Femur Tibia Humerus Vertebrae
Gejala klinis : Nyeri dan bengkak < 6 bulan pulsatile Fraktur patologis (15-20%) nyeri akut

Classification of morphological types of ABC. Type I, central with little expansion; type 2, central with expansion and cortical thinning; type 3, eccentric with involvement of only one cortex; type 4, subperiosteal extending ‘outwards’ with intact or only superficially eroded cortex; and type 5, subperiosteal with growth both outwards and centrally towards the medulla, with cortical destruction

Radiologis Destruksi tulang radiolusen Lesi ekspansif Korteks menjadi sangat tipis dan mengembung keluar


TERIMA KASIH