Embed Size (px)
Citation preview
O
Ts
Sa
b
c
AA
KTDL
1
saaCbmtd
1
Orthopaedics & Traumatology: Surgery & Research 101 (2015) 17–21
Available online at
ScienceDirectwww.sciencedirect.com
riginal article
wo-level lumbar total disc replacement: Functional outcomes andegmental motion after 4 years
. Trincata,∗,b, G. Edgard-Rosac, G. Genestec, T. Marnayc
Hôpital privé « les Franciscaines », 3, rue Jean-Bouin, 30032 Nîmes, France65, avenue Jean-Jaurès, 30900 Nîmes, FranceClinique du Parc, 50, rue Emile-Combe, 34170 Castelnau-le-Lez, France
a r t i c l e i n f o
rticle history:ccepted 17 October 2014
eywords:otal disc replacementegenerative disc diseaseow-back pain
a b s t r a c t
Introduction: Lumbar total disc replacement is an effective treatment for single-level discogenic lowerback pain. But the replacement of two disc levels is controversial.Hypothesis: Two-level total disc replacement will improve function while preserving spinal motion.Material and methods: A continuous series of 108 patients (51 women, 57 men) surgically treated overtwo levels with the ProDisc-L implant (Synthes Spine) was evaluated retrospectively with an averagefollow-up of 4 years. Ninety-three of these patients were operated for L4/L5 and L5/S1 degenerative discdisease, while 15 were operated for L3/L4 and L4/L5 disease. The procedure was carried out throughthe left retroperitoneal approach in 65 patients, the right retroperitoneal approach in 42 patients andboth approaches in 1 patient. The Oswestry score, lumbar VAS and radicular VAS were used to evaluatefunction. The motion of the prosthetic disc segments was evaluated using Cobb’s method. Data werecollected prospectively in the context of regular patient monitoring. A retrospective analysis was carriedout by an independent examiner.Results: The procedure led to a statistically significant improvement in the functional scores. The motionof the upper disc segment was 9◦ (0◦–19◦) in flexion/extension and 5.5◦ (2◦–12◦) in lateral bending. Itwas 6.2◦ (0◦–14◦) and 1.9◦ (0◦–7◦) at the lower disc segment. The range of motion was similar in L3/L4and L4/L5, but was less in L5/S1. Lack of mobility was not correlated with alterations in the functionaloutcome. The complication rate was 18%.
Discussion: Two-level lumbar disc replacement improves spinal function while preserving its mobility.But this procedure is fraught with risks and must be carried out by a highly-experienced team. A longerfollow-up is needed to evaluate the sustainability of the results and to detect any adjacent segmentdisease. The French National Authority for Health (HAS) has recommended against two-level lumbar discreplacement, so it no longer can be performed in France.© 2014 Elsevier Masson SAS. All rights reserved.
. Introduction
Single-level lumbar total disc replacement (TDR) has beenhown to be non-inferior to spinal fusion. Its use is generallyccepted in very specific indications [1,2]. But disc replacementt two levels is controversial because of conflicting results [3–8].urrently, a two-level procedure cannot be performed in Franceecause the HAS (French National Authority for Health) has recom-
ended against it. However, TDR has been shown to be non-inferioro spinal fusion for the treatment of two-level degenerative discisease (DDD), while improving mobility and functional recovery
∗ Corresponding author. Tel.: +04 66 29 54 55; fax: +04 66 38 31 72.E-mail address: [email protected] (S. Trincat).
http://dx.doi.org/10.1016/j.otsr.2014.10.014877-0568/© 2014 Elsevier Masson SAS. All rights reserved.
in the short term [9]. The alternative is to use a hybrid construct[10,11] that combines fusion and arthroplasty, with preservationof segmental motion being the theoretical advantage of the latter.
The goal of this study was to evaluate the perioperative com-plications and functional outcomes in patients who had undergonetwo-level lumbar TDR after a minimum follow-up of 2 years. Thespinal segment motion was evaluated at the last follow-up usingradiographs.
2. Material and methods
This was a continuous retrospective study of 150 patients oper-ated for two-level lumbar TDR who were evaluated at least 2 yearsafter the procedure. Of these 150 patients, only those operated atL3/L4 and L4/L5 or L4/L5 and L5/S1 were included. Patients were
1 tology: Surgery & Research 101 (2015) 17–21
eptwa
lwo
attaspcpcrpol
peptRwou
nmsd
3
Oltcass
TI
n
8 S. Trincat et al. / Orthopaedics & Trauma
xcluded from the analysis if they did not have complete and usablereoperative and postoperative clinical and radiological records. Inhe end, the analysis was carried out on 108 patients (57 men, 51omen) having an average age of 46 ± 10 years (range 19–73). The
verage follow-up was 49 months (range 25–63).The surgical indication was established in patients with multi-
evel symptomatic DDD that was resistant to medical treatment orell-conducted rehabilitation and presented Modic 0, 1 or 2 signs
n MRI [12,13], or failing that, a positive lumbar discogram.The procedure was carried out at L4/L5 and L5/S1 in 93 cases
nd at L3/L4 and L4/L5 in 15 cases. It was performed throughhe left retroperitoneal (anterolateral) approach in 65 patients,he right retroperitoneal approach [14] in 42 patients and bothpproaches in 1 patient. The ProDisc-L Total Disc Replacementystem (Synthes Spine, West Chester, PA, USA) was used in allatients. This is a semi-constrained implant consisting of twoobalt-chrome alloy endplates with keels that are coated withorous plasma-sprayed titanium and an UHMWPE core that islipped to the inferior endplate and articulates with the supe-ior endplate through a convex dome. The average duration of therocedure was 111 ± 31 min (70–230) with an average blood lossf 316 ± 453 mL (50–3500). The surgical scar was 10 ± 2 cm (5–18)ong on average.
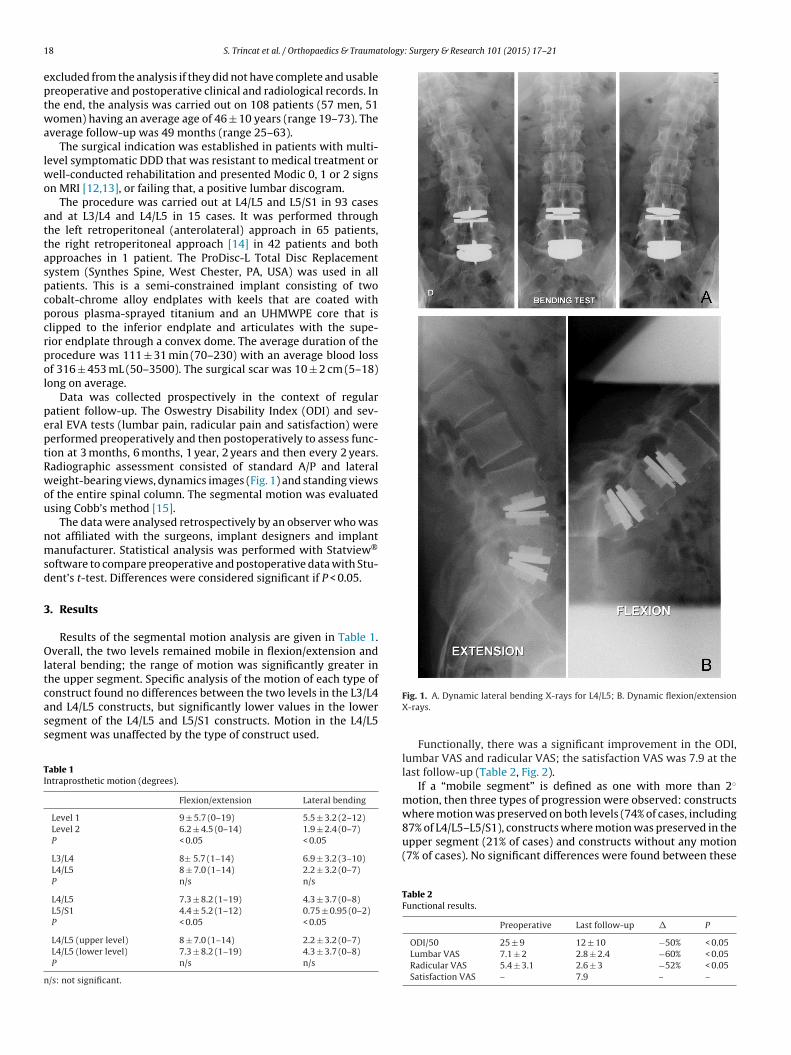
Data was collected prospectively in the context of regularatient follow-up. The Oswestry Disability Index (ODI) and sev-ral EVA tests (lumbar pain, radicular pain and satisfaction) wereerformed preoperatively and then postoperatively to assess func-ion at 3 months, 6 months, 1 year, 2 years and then every 2 years.adiographic assessment consisted of standard A/P and lateraleight-bearing views, dynamics images (Fig. 1) and standing views
f the entire spinal column. The segmental motion was evaluatedsing Cobb’s method [15].
The data were analysed retrospectively by an observer who wasot affiliated with the surgeons, implant designers and implantanufacturer. Statistical analysis was performed with Statview®
oftware to compare preoperative and postoperative data with Stu-ent’s t-test. Differences were considered significant if P < 0.05.
. Results
Results of the segmental motion analysis are given in Table 1.verall, the two levels remained mobile in flexion/extension and
ateral bending; the range of motion was significantly greater inhe upper segment. Specific analysis of the motion of each type of
onstruct found no differences between the two levels in the L3/L4nd L4/L5 constructs, but significantly lower values in the loweregment of the L4/L5 and L5/S1 constructs. Motion in the L4/L5egment was unaffected by the type of construct used.able 1ntraprosthetic motion (degrees).
Flexion/extension Lateral bending
Level 1 9 ± 5.7 (0–19) 5.5 ± 3.2 (2–12)Level 2 6.2 ± 4.5 (0–14) 1.9 ± 2.4 (0–7)P < 0.05 < 0.05
L3/L4 8± 5.7 (1–14) 6.9 ± 3.2 (3–10)L4/L5 8 ± 7.0 (1–14) 2.2 ± 3.2 (0–7)P n/s n/s
L4/L5 7.3 ± 8.2 (1–19) 4.3 ± 3.7 (0–8)L5/S1 4.4 ± 5.2 (1–12) 0.75 ± 0.95 (0–2)P < 0.05 < 0.05
L4/L5 (upper level) 8 ± 7.0 (1–14) 2.2 ± 3.2 (0–7)L4/L5 (lower level) 7.3 ± 8.2 (1–19) 4.3 ± 3.7 (0–8)P n/s n/s
/s: not significant.
Fig. 1. A. Dynamic lateral bending X-rays for L4/L5; B. Dynamic flexion/extensionX-rays.
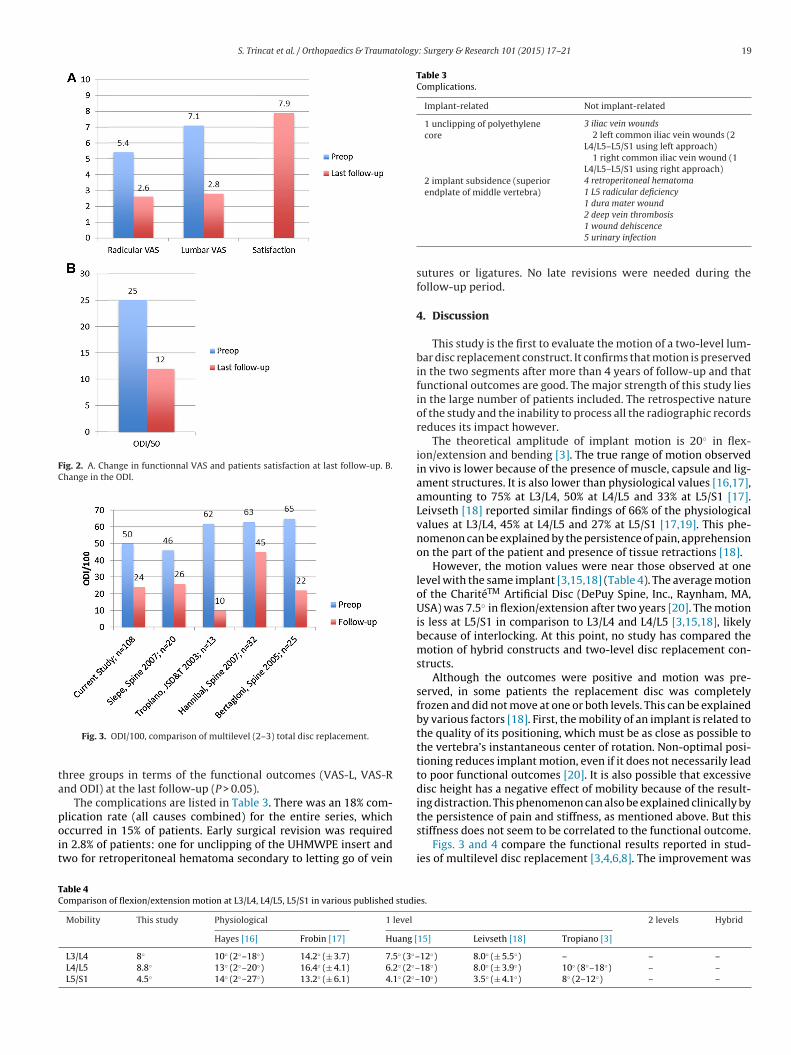
Functionally, there was a significant improvement in the ODI,lumbar VAS and radicular VAS; the satisfaction VAS was 7.9 at thelast follow-up (Table 2, Fig. 2).
If a “mobile segment” is defined as one with more than 2◦
motion, then three types of progression were observed: constructswhere motion was preserved on both levels (74% of cases, including
87% of L4/L5–L5/S1), constructs where motion was preserved in theupper segment (21% of cases) and constructs without any motion(7% of cases). No significant differences were found between theseTable 2Functional results.
Preoperative Last follow-up � P
ODI/50 25 ± 9 12 ± 10 −50% < 0.05Lumbar VAS 7.1 ± 2 2.8 ± 2.4 −60% < 0.05Radicular VAS 5.4 ± 3.1 2.6 ± 3 −52% < 0.05Satisfaction VAS – 7.9 – –
S. Trincat et al. / Orthopaedics & Traumatology: Surgery & Research 101 (2015) 17–21 19
Fig. 2. A. Change in functionnal VAS and patients satisfaction at last follow-up. B.Change in the ODI.
ta
poit
Table 3Complications.
Implant-related Not implant-related
1 unclipping of polyethylenecore
3 iliac vein wounds2 left common iliac vein wounds (2
L4/L5–L5/S1 using left approach)1 right common iliac vein wound (1
L4/L5–L5/S1 using right approach)2 implant subsidence (superiorendplate of middle vertebra)
4 retroperitoneal hematoma1 L5 radicular deficiency1 dura mater wound
the persistence of pain and stiffness, as mentioned above. But this
TC
Fig. 3. ODI/100, comparison of multilevel (2–3) total disc replacement.
hree groups in terms of the functional outcomes (VAS-L, VAS-Rnd ODI) at the last follow-up (P > 0.05).
The complications are listed in Table 3. There was an 18% com-lication rate (all causes combined) for the entire series, which
ccurred in 15% of patients. Early surgical revision was requiredn 2.8% of patients: one for unclipping of the UHMWPE insert andwo for retroperitoneal hematoma secondary to letting go of veinable 4omparison of flexion/extension motion at L3/L4, L4/L5, L5/S1 in various published studi
Mobility This study Physiological 1 level
Hayes [16] Frobin [17] Huang [
L3/L4 8◦ 10◦ (2◦–18◦) 14.2◦ (± 3.7) 7.5◦ (3◦–L4/L5 8.8◦ 13◦ (2◦–20◦) 16.4◦ (± 4.1) 6.2◦ (2◦–L5/S1 4.5◦ 14◦ (2◦–27◦) 13.2◦ (± 6.1) 4.1◦ (2◦–
2 deep vein thrombosis1 wound dehiscence5 urinary infection
sutures or ligatures. No late revisions were needed during thefollow-up period.
4. Discussion
This study is the first to evaluate the motion of a two-level lum-bar disc replacement construct. It confirms that motion is preservedin the two segments after more than 4 years of follow-up and thatfunctional outcomes are good. The major strength of this study liesin the large number of patients included. The retrospective natureof the study and the inability to process all the radiographic recordsreduces its impact however.
The theoretical amplitude of implant motion is 20◦ in flex-ion/extension and bending [3]. The true range of motion observedin vivo is lower because of the presence of muscle, capsule and lig-ament structures. It is also lower than physiological values [16,17],amounting to 75% at L3/L4, 50% at L4/L5 and 33% at L5/S1 [17].Leivseth [18] reported similar findings of 66% of the physiologicalvalues at L3/L4, 45% at L4/L5 and 27% at L5/S1 [17,19]. This phe-nomenon can be explained by the persistence of pain, apprehensionon the part of the patient and presence of tissue retractions [18].
However, the motion values were near those observed at onelevel with the same implant [3,15,18] (Table 4). The average motionof the CharitéTM Artificial Disc (DePuy Spine, Inc., Raynham, MA,USA) was 7.5◦ in flexion/extension after two years [20]. The motionis less at L5/S1 in comparison to L3/L4 and L4/L5 [3,15,18], likelybecause of interlocking. At this point, no study has compared themotion of hybrid constructs and two-level disc replacement con-structs.
Although the outcomes were positive and motion was pre-served, in some patients the replacement disc was completelyfrozen and did not move at one or both levels. This can be explainedby various factors [18]. First, the mobility of an implant is related tothe quality of its positioning, which must be as close as possible tothe vertebra’s instantaneous center of rotation. Non-optimal posi-tioning reduces implant motion, even if it does not necessarily leadto poor functional outcomes [20]. It is also possible that excessivedisc height has a negative effect of mobility because of the result-ing distraction. This phenomenon can also be explained clinically by
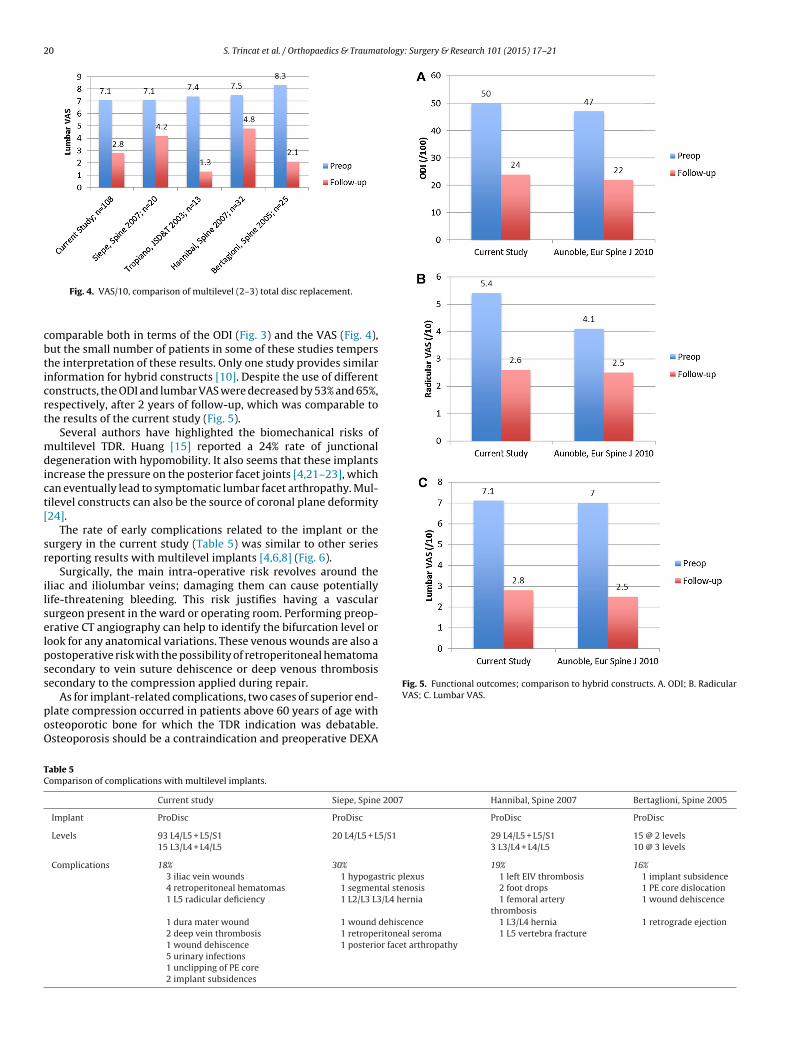
stiffness does not seem to be correlated to the functional outcome.Figs. 3 and 4 compare the functional results reported in stud-
ies of multilevel disc replacement [3,4,6,8]. The improvement was
es.
2 levels Hybrid
15] Leivseth [18] Tropiano [3]
12◦) 8.0◦ (± 5.5◦) – – –18◦) 8.0◦ (± 3.9◦) 10◦ (8◦–18◦) – –10◦) 3.5◦ (± 4.1◦) 8◦ (2–12◦) – –
20 S. Trincat et al. / Orthopaedics & Traumatology: Surgery & Research 101 (2015) 17–21
cbticrt
mdict[
sr
ilselpss
poO
Fig. 5. Functional outcomes; comparison to hybrid constructs. A. ODI; B. RadicularVAS; C. Lumbar VAS.
TC
Fig. 4. VAS/10, comparison of multilevel (2–3) total disc replacement.
omparable both in terms of the ODI (Fig. 3) and the VAS (Fig. 4),ut the small number of patients in some of these studies tempershe interpretation of these results. Only one study provides similarnformation for hybrid constructs [10]. Despite the use of differentonstructs, the ODI and lumbar VAS were decreased by 53% and 65%,espectively, after 2 years of follow-up, which was comparable tohe results of the current study (Fig. 5).
Several authors have highlighted the biomechanical risks ofultilevel TDR. Huang [15] reported a 24% rate of junctional
egeneration with hypomobility. It also seems that these implantsncrease the pressure on the posterior facet joints [4,21–23], whichan eventually lead to symptomatic lumbar facet arthropathy. Mul-ilevel constructs can also be the source of coronal plane deformity24].
The rate of early complications related to the implant or theurgery in the current study (Table 5) was similar to other serieseporting results with multilevel implants [4,6,8] (Fig. 6).
Surgically, the main intra-operative risk revolves around theliac and iliolumbar veins; damaging them can cause potentiallyife-threatening bleeding. This risk justifies having a vascularurgeon present in the ward or operating room. Performing preop-rative CT angiography can help to identify the bifurcation level orook for any anatomical variations. These venous wounds are also aostoperative risk with the possibility of retroperitoneal hematomaecondary to vein suture dehiscence or deep venous thrombosisecondary to the compression applied during repair.
As for implant-related complications, two cases of superior end-
late compression occurred in patients above 60 years of age withsteoporotic bone for which the TDR indication was debatable.steoporosis should be a contraindication and preoperative DEXAable 5omparison of complications with multilevel implants.
Current study Siepe, Spine 2007 Hannibal, Spine 2007 Bertaglioni, Spine 2005
Implant ProDisc ProDisc ProDisc ProDisc
Levels 93 L4/L5 + L5/S1 20 L4/L5 + L5/S1 29 L4/L5 + L5/S1 15 @ 2 levels15 L3/L4 + L4/L5 3 L3/L4 + L4/L5 10 @ 3 levels
Complications 18% 30% 19% 16%3 iliac vein wounds 1 hypogastric plexus 1 left EIV thrombosis 1 implant subsidence4 retroperitoneal hematomas 1 segmental stenosis 2 foot drops 1 PE core dislocation1 L5 radicular deficiency 1 L2/L3 L3/L4 hernia 1 femoral artery
thrombosis1 wound dehiscence
1 dura mater wound 1 wound dehiscence 1 L3/L4 hernia 1 retrograde ejection2 deep vein thrombosis 1 retroperitoneal seroma 1 L5 vertebra fracture1 wound dehiscence 1 posterior facet arthropathy5 urinary infections1 unclipping of PE core2 implant subsidences

S. Trincat et al. / Orthopaedics & Traumatology
sftOp
daw
5
fmLt
vil
meb
ncacf
D
pU
P
o
A
C
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[24] Ching AC, Birkenmaier C, Hart RA. Short segment coronal plane deformity after
Fig. 6. Complication rate for multilevel implants.
can should be considered before the surgical procedure. Vertebralracture can theoretically occur in the middle vertebra because ofhe keels [3,25]. No fractures were observed in the current study.ther rarer complications were observed such as dislocation of theolyethylene core [8] and implant migration [7].
Because of current health regulations in France, two-level totalisc replacement can no longer be performed. As a consequence, were exploring the possibility of using hybrid constructs in patientsith multilevel degenerative disc disease.
. Conclusions
Two-level total lumbar disc replacement resulted in satisfactoryunctional outcomes, while preserving motion in the operated seg-
ent in most patients. The range of motion was similar at L3/L4 and4/L5, but was less at L5/S1. The absence of motion in one or evenwo levels was not correlated with poorer functional outcomes.
But this procedure is not devoid of perioperative risk, especiallyascular ones; it should be performed by teams that are well-versedn the surgical technique, potentially in collaboration with a vascu-ar surgeon.
A prospective randomised study is needed to properly compareultilevel TDR with hybrid constructs. However, multilevel degen-
rative disc disease is a contraindication to arthroplasty in Franceecause of the HAS recommendations.
A medium-term analysis of the current study population will beeeded to re-evaluate the segmental motion and detect any adja-ent segment disease. Additional evaluation of the sagittal balancend segmental lordosis correlated with the functional outcomesould also help us better define the indications and identify riskactors for poor functional outcomes.
isclosure of interest
TM: Clinical trials: principal investigator, study coordinator andrimary researcher for ProDisc-L (Synthes Spine, West Chester, PA,SA).
GG: Clinical trials: co-investigator, non-primary researcher forroDisc-L (Synthes Spine, West Chester, PA, USA).
S. Trincat and G. Edgard-Rosa declare that they have no conflictsf interest concerning this article.
cknowledgements
Nathalie Larive, Clinical Research Associate, Clinique du Parc,astelnau-le-Lez, France.
[
: Surgery & Research 101 (2015) 17–21 21
References
[1] Blumenthal S, McAfee PC, Guyer RD, Hochschuler SH, Geisler FH, Holt RT, et al.A prospective, randomized, multicenter food and drug administration inves-tigational device exemptions study of lumbar total disc replacement with theCharité artificial disc versus lumbar fusion: part I: evaluation of clinical out-comes. Spine 2005;30:1565–75.
[2] Zigler J, Delamarter R, Spivak JM, Linovitz RJ, Danielson III GO, Haider TT, et al.Results of the prospective, randomized, multicenter food and drug admin-istration investigational device exemption study of the ProDisc-L total discreplacement versus circumferential fusion for the treatment of 1-level degen-erative disc disease. Spine 2007;32:1155–62.
[3] Tropiano P, Huang RC, Girardi FP, Marnay T. Lumbar disc replacement. Prelimi-nary results with ProDisc II after a minimum follow-up period of 1 year. J SpinalDisord Tech 2003;16:362–8.
[4] Siepe CJ, Mayer HM, Heinz-Leisenheimer M, Korge A. Total lumbar disc replace-ment: different results for different levels. Spine 2007;32:782–90.
[5] Cinotti G, David T, Postacchini F. Results of disc prosthesis after a minimumfollow-up period of 2 years. Spine 1996;21:995–1000.
[6] Hannibal M, Thomas DJ, Low J, Hsu KY, Zucherman J. ProDisc-L total discreplacement: a comparison of 1-level versus 2-level arthroplasty patients witha minimum 2-year follow-up. Spine 2007;32:2322–6.
[7] Zigler JE, Sachs BL, Rashbaum RF, et al. Two level total disc replacement withProdisc: results and comparison to one level cases. Spine J 2005;5:S4–5.
[8] Bertagnoli R, Yue JJ, Shah RV, Nanieva R, Pfeiffer F, Fenk-Mayer A, et al. Thetreatment of disabling multilevel lumbar discogenic low back pain with totaldisc arthroplasty utilizing the ProDisc prosthesis: a prospective study with 2-year minimum follow-up. Spine 2005;30:2192–9.
[9] Delamarter R, Zigler JE, Balderston RA, Cammisa FP, Goldstein JA, Spivak JM.Prospective, randomized, multicenter food and drug administration inves-tigational device exemption study of the ProDisc-L total disc replacementcompared with circumferential arthrodesis for the treatment of two-level lum-bar degenerative disc disease: results at twenty-four months. J Bone Joint SurgAm 2011;93:705–15.
10] Aunoble S, Meyrat R, Al Sawad Y, Tournier C, Leijssen P, Le Huec JC. Hybrid con-struct for two levels disc disease in lumbar spine. Eur Spine J 2010;19:290–6.
11] Bertagnoli R, Tropiano P, Zigler J, Karg A, Voigt S. Hybrid constructs. Orthop ClinNorth Am 2005;36:379–88.
12] Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative diskdisease: assessment of changes in vertebral body marrow with MR imaging.Radiology 1988;166:193–9.
13] Blondel B, Tropiano P, Gaudart J, Huang RC, Marnay T. Clinical results of lumbartotal disc arthroplasty in accordance with Modic signs, with a 2-year-minimumfollow-up. Spine 2011;36:2309–15.
14] Edgard-Rosa G, Geneste G, Nègre G, Marnay T. Midline anterior approach fromthe right side to the lumbar spine for interbody fusion and total disc replace-ment: a new mobilization technique of the vena cava. Spine 2012;37:E562–9.
15] Huang RC, Girardi FP, Cammisa Jr FP, Tropiano P, Marnay T. Long-term flexion-extension range of motion of the prodisc total disc replacement. J Spinal DisordTech 2003;16:435–40.
16] Hayes MA, Howard TC, Gruel CR, Kopta JA. Roentgenographic evalua-tion of lumbar spine flexion-extension in asymptomatic individuals. Spine1989;14:327–31.
17] Frobin W, Brinckmann P, Leivseth G, Biggemann M, Reikerås O. Precisionmeasurement of segmental motion from flexion-extension radiographs of thelumbar spine. Clin Biomech 1996;11:457–65.
18] Leivseth G, Braaten S, Frobin W, Brinckmann P. Mobility of lumbar segmentsinstrumented with a ProDisc II prosthesis: a two-year follow-up study. Spine2006;31:1726–33.
19] Dvorak J, Panjabi MM, Chang DG, Theiler R, Grob D. Functional radiographicdiagnosis of the lumbar spine: flexion-extension and lateral bending. Spine1991;16:562–71.
20] McAfee PC, Fedder IL, Saiedy S, Shucosky EM, Cunningham BW. SB Charité discreplacement: report of 60 prospective randomized cases in a US center. J SpinalDisord Tech 2003;16:424–33.
21] Schmidt H, Galbusera F, Rohlmann A, Zander T, Wilke HJ. Effect of multilevellumbar disc arthroplasty on spine kinematics and facet joint loads in flexionand extension: a finite element analysis. Eur Spine J 2012;21:S663–74.
22] Park CK, Ryu KS, Jee WH. Degenerative changes of discs and facet joints inlumbar total disc replacement using ProDisc II: minimum two-year follow-up.Spine 2008;33:1755–61.
23] Siepe CJ, Zelenkov P, Sauri-Barraza JC, Szeimies U, Grubinger T, Tepass A, et al.The fate of facet joint and adjacent level disc degeneration following total lum-bar disc replacement: a prospective clinical, X-ray, and magnetic resonanceimaging investigation. Spine 2010;35:1991–2003.
two-level lumbar total disc replacement. Spine 2010;35:44–50.25] Shim CS, Lee S, Maeng DH, Lee SH. Vertical split fracture of the vertebral body
following total disc replacement using ProDisc: report of two cases. J SpinalDisord Tech 2005;18:465–9.