Embed Size (px)
Citation preview
12/22/2012
1
Urinalysis (Macroscopic Chemical Tests)( p )
Mohammad Reza Bakhtiari DCLS, PhD
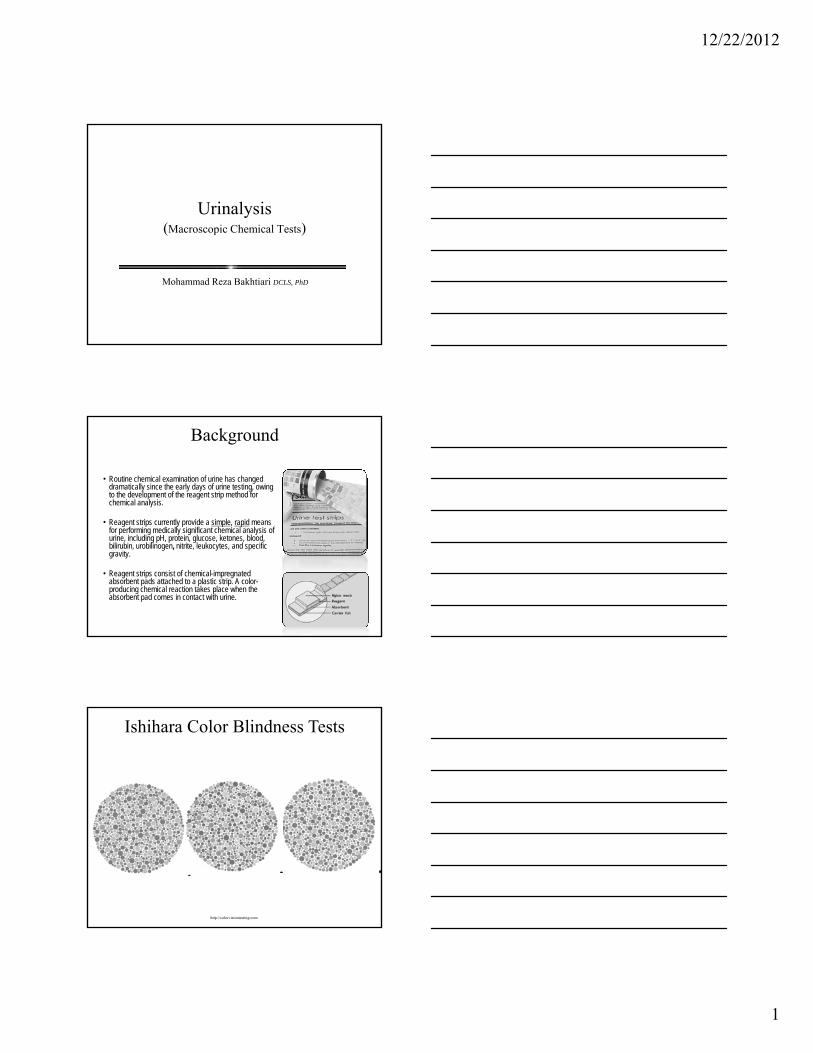
Background
• Routine chemical examination of urine has changed dramatically since the early days of urine testing, owing to the development of the reagent strip method for chemical analysis.
• Reagent strips currently provide a simple, rapid means g p y p p pfor performing medically significant chemical analysis of urine, including pH, protein, glucose, ketones, blood, bilirubin, urobilinogen, nitrite, leukocytes, and specific gravity.
• Reagent strips consist of chemical-impregnated absorbent pads attached to a plastic strip. A color-producing chemical reaction takes place when the absorbent pad comes in contact with urine.
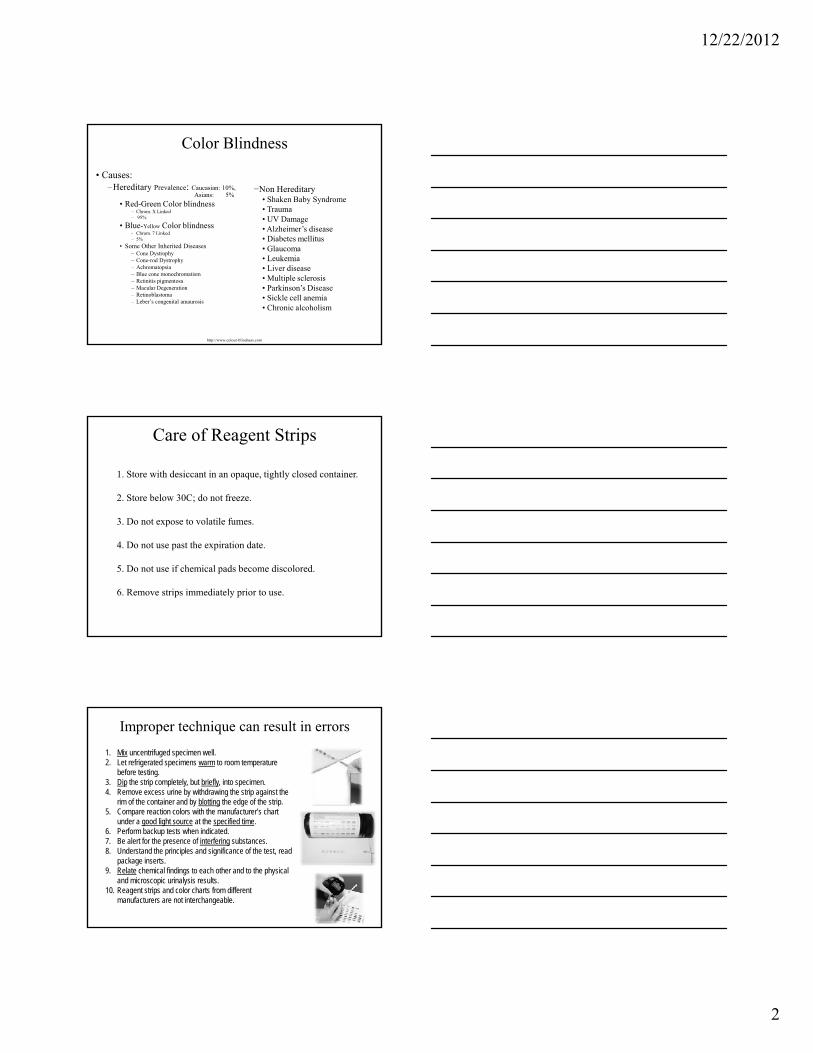
Ishihara Color Blindness Tests
http://colorvisiontesting.com
12/22/2012
2
• Causes:–Hereditary Prevalence: Caucasian: 10%,
Asians: 5%• Red-Green Color blindness
– Chrom. X Linked– 95%
• Blue-Yellow Color blindness – Chrom. 7 Linked
Color Blindness
−Non Hereditary• Shaken Baby Syndrome • Trauma• UV Damage• Alzheimer’s disease
Chrom. 7 Linked– 5%
• Some Other Inherited Diseases– Cone Dystrophy – Cone-rod Dystrophy – Achromatopsia – Blue cone monochromatism – Retinitis pigmentosa – Macular Degeneration – Retinoblastoma – Leber’s congenital amaurosis
http://www.colour-blindness.com
• Diabetes mellitus • Glaucoma • Leukemia • Liver disease • Multiple sclerosis • Parkinson’s Disease • Sickle cell anemia • Chronic alcoholism
Care of Reagent Strips
1. Store with desiccant in an opaque, tightly closed container.
2. Store below 30C; do not freeze.
3. Do not expose to volatile fumes.p
4. Do not use past the expiration date.
5. Do not use if chemical pads become discolored.
6. Remove strips immediately prior to use.
Improper technique can result in errors
1. Mix uncentrifuged specimen well.2. Let refrigerated specimens warm to room temperature
before testing.3. Dip the strip completely, but briefly, into specimen.4. Remove excess urine by withdrawing the strip against the
rim of the container and by blotting the edge of the strip.5. Compare reaction colors with the manufacturer’s chart
under a good light source at the specified time.6. Perform backup tests when indicated.7. Be alert for the presence of interfering substances.8. Understand the principles and significance of the test, read
package inserts.9. Relate chemical findings to each other and to the physical
and microscopic urinalysis results.10. Reagent strips and color charts from different
manufacturers are not interchangeable.
12/22/2012
3
Quality Control
1. Test open bottles of reagent strips with known positive and negative controls every 24 hr.
2. Resolve control results that are out of range by further testing.
3. Test reagents used in backup tests with positive and negative controls.
4. Perform positive and negative controls on new reagents and newly opened bottles of reagent strips.
5. Record all control results and reagent lot numbers.
• A healthy individual usually produces a first morning specimen with a slightly acidic pH of 5.0 to 6.0;
• A more alkaline pH is found following meals (alkaline tide).
• The pH of normal random samples can range from 4.5 to 8.0.
Causes of Acid and Alkaline Urine
• Consequently, no normal values are assigned to urinary pH, and it must be considered in conjunction with other patient information, such as:
– the acid-base content of the blood,– the patient’s renal function,– the presence of a urinary tract infection,– the patient’s dietary intake, – the age of the specimen
1.Respiratory or metabolic acidosis/ketosis
2.Respiratory or metabolic alkalosis
3.Defects in renal tubular secretion and reabsorption of acids and bases—renal t b l id i
Clinical Significance of Urine pH
Reabsorption of filtered bicarbonate.
tubular acidosis
4.Renal calculi formation
5.Treatment of urinary tract infections
6.Precipitation/identification of crystals
7.Determination of unsatisfactory specimens
Excretion of secreted hydrogen ions combined with ammonia produced by the tubules.
Excretion of secreted hydrogen ions combined with phosphate.
12/22/2012
4
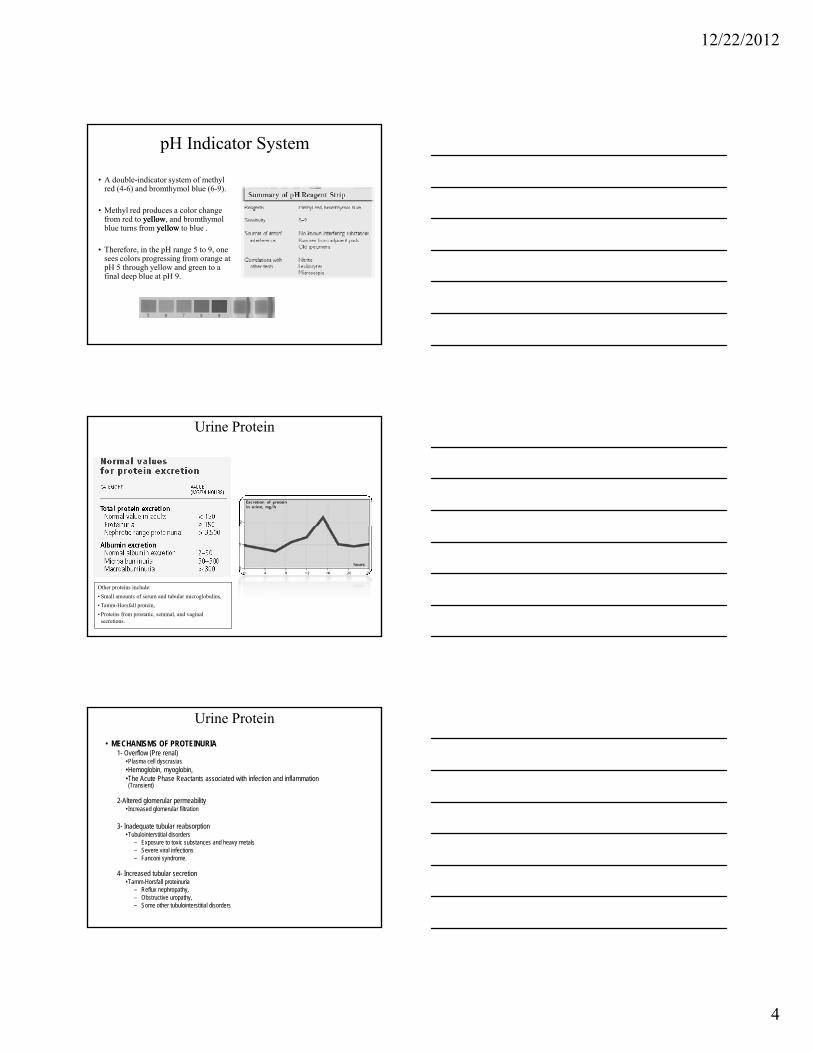
pH Indicator System
• A double-indicator system of methyl red (4-6) and bromthymol blue (6-9).
• Methyl red produces a color change from red to yellowyellow, and bromthymolblue turns from yellowyellow to blue .
• Therefore, in the pH range 5 to 9, one sees colors progressing from orange at pH 5 through yellow and green to a final deep blue at pH 9.
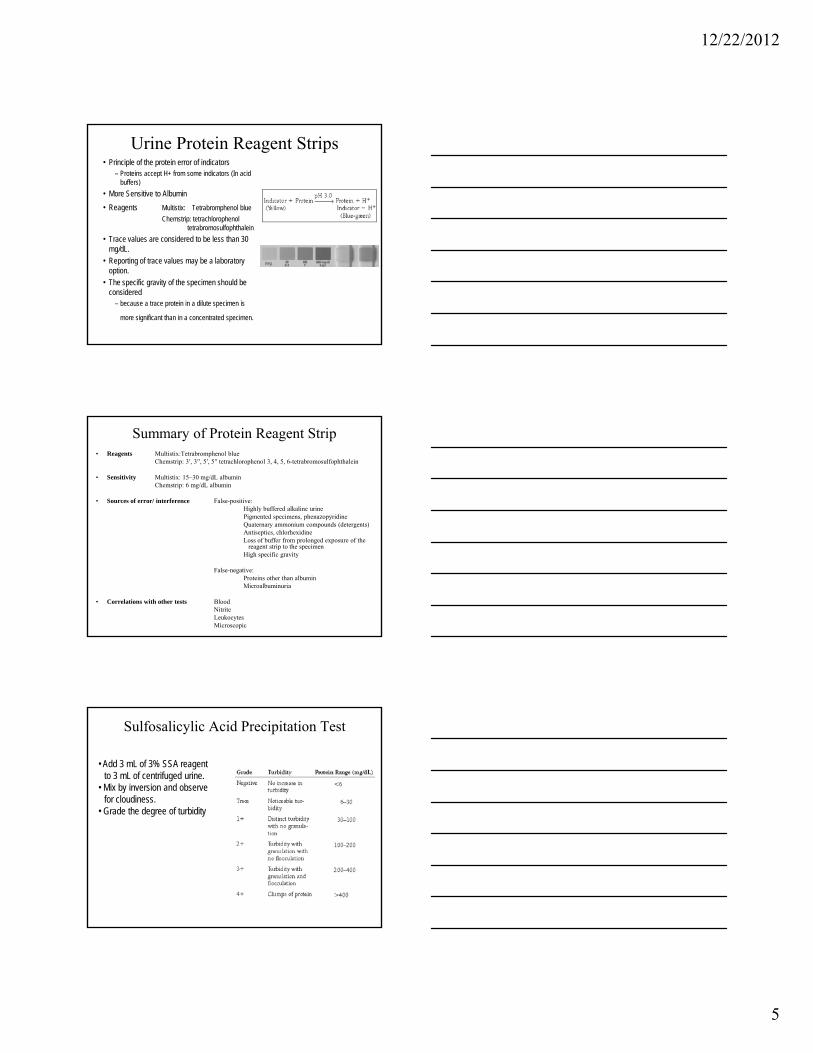
Urine Protein
Other proteins include:• Small amounts of serum and tubular microglobulins, • Tamm-Horsfall protein, • Proteins from prostatic, seminal, and vaginal
secretions.
Urine Protein• MECHANISMS OF PROTEINURIA
1- Overflow (Pre renal)•Plasma cell dyscrasias•Hemoglobin, myoglobin, •The Acute Phase Reactants associated with infection and inflammation (Transient)
2-Altered glomerular permeability• Increased glomerular filtration
3- Inadequate tubular reabsorption•Tubulointerstitial disorders
– Exposure to toxic substances and heavy metals – Severe viral infections– Fanconi syndrome.
4- Increased tubular secretion•Tamm-Horsfall proteinuria
– Reflux nephropathy, – Obstructive uropathy, – Some other tubulointerstitial disorders
12/22/2012
5
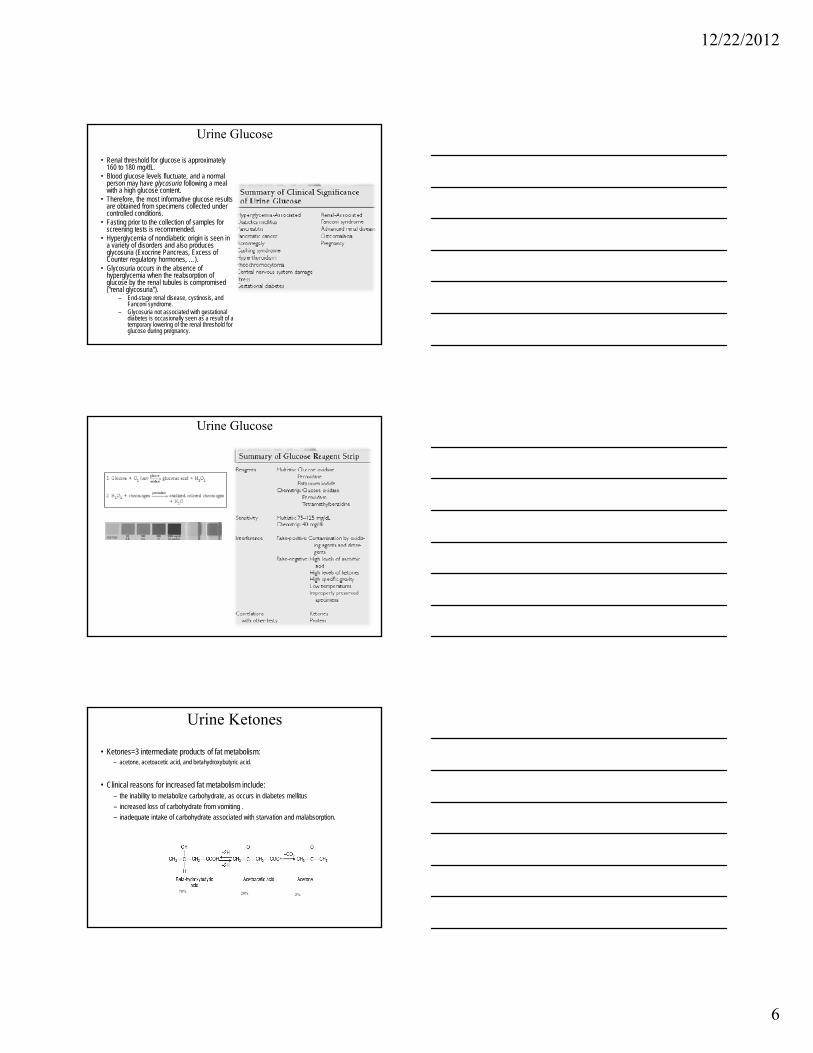
Urine Protein Reagent Strips• Principle of the protein error of indicators
– Proteins accept H+ from some indicators (In acid buffers)
• More Sensitive to Albumin• Reagents Multistix: Tetrabromphenol blue
Chemstrip: tetrachlorophenol tetrabromosulfophthalein
• Trace values are considered to be less than 30 mg/dL.
• Reporting of trace values may be a laboratory option.
• The specific gravity of the specimen should be considered
– because a trace protein in a dilute specimen is
more significant than in a concentrated specimen.
• Reagents Multistix:Tetrabromphenol blueChemstrip: 3′, 3′′, 5′, 5′′ tetrachlorophenol 3, 4, 5, 6-tetrabromosulfophthalein
• Sensitivity Multistix: 15–30 mg/dL albuminChemstrip: 6 mg/dL albumin
• Sources of error/ interference False-positive: Highly buffered alkaline urinePigmented specimens, phenazopyridineQuaternary ammonium compounds (detergents)
Summary of Protein Reagent Strip
Quaternary ammonium compounds (detergents)Antiseptics, chlorhexidineLoss of buffer from prolonged exposure of the
reagent strip to the specimenHigh specific gravity
False-negative: Proteins other than albuminMicroalbuminuria
• Correlations with other tests Blood NitriteLeukocytesMicroscopic
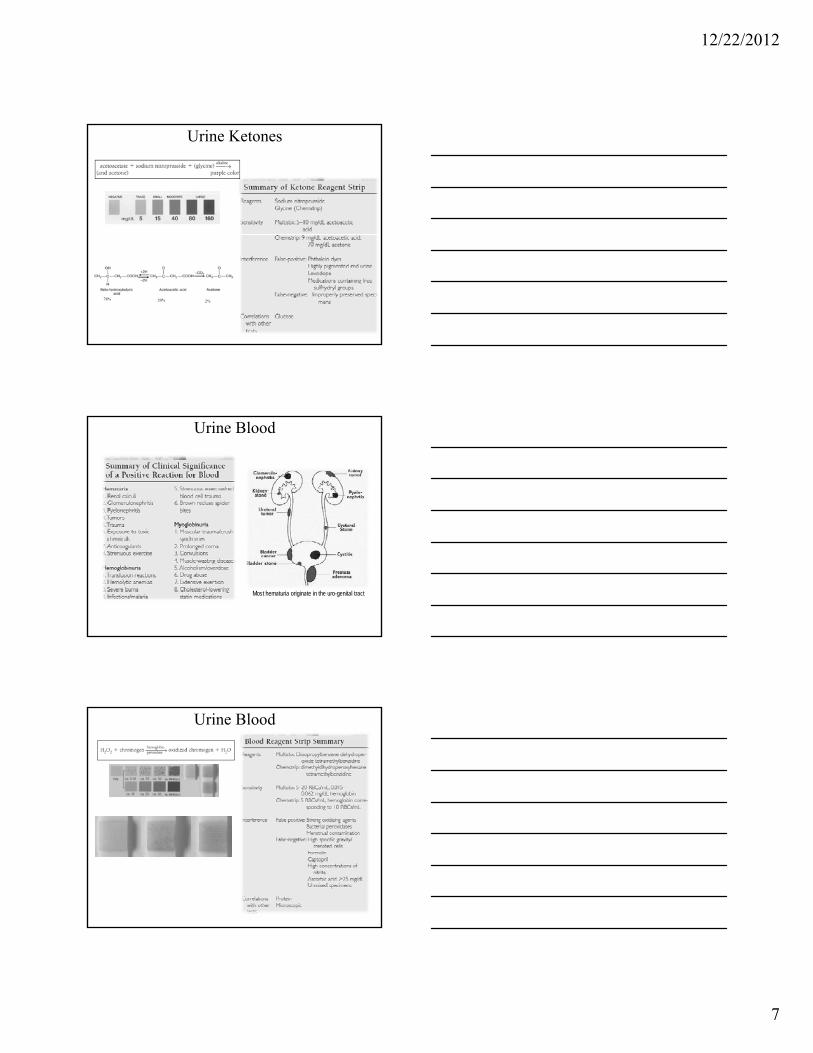
Sulfosalicylic Acid Precipitation Test
• Add 3 mL of 3% SSA reagent to 3 mL of centrifuged urine.
• Mix by inversion and observe for cloudiness.
• Grade the degree of turbidity
12/22/2012
6
• Renal threshold for glucose is approximately 160 to 180 mg/dL.
• Blood glucose levels fluctuate, and a normal person may have glycosuria following a meal with a high glucose content.
• Therefore, the most informative glucose results are obtained from specimens collected under controlled conditions.
• Fasting prior to the collection of samples for screening tests is recommended.
Urine Glucose
• Hyperglycemia of nondiabetic origin is seen in a variety of disorders and also produces glycosuria (Exocrine Pancreas, Excess of Counter regulatory hormones, …).
• Glycosuria occurs in the absence of hyperglycemia when the reabsorption of glucose by the renal tubules is compromised (“renal glycosuria”).
– End-stage renal disease, cystinosis, and Fanconi syndrome.
– Glycosuria not associated with gestational diabetes is occasionally seen as a result of a temporary lowering of the renal threshold for glucose during pregnancy.
Urine Glucose
Urine Ketones
• Ketones=3 intermediate products of fat metabolism: – acetone, acetoacetic acid, and betahydroxybutyric acid.
• Clinical reasons for increased fat metabolism include:– the inability to metabolize carbohydrate, as occurs in diabetes mellitus– increased loss of carbohydrate from vomiting .– inadequate intake of carbohydrate associated with starvation and malabsorption– inadequate intake of carbohydrate associated with starvation and malabsorption.
78% 20% 2%
12/22/2012
7
Urine Ketones
78% 20% 2%
Urine Blood
Most hematuria originate in the uro-genital tract
Urine Blood
12/22/2012
8
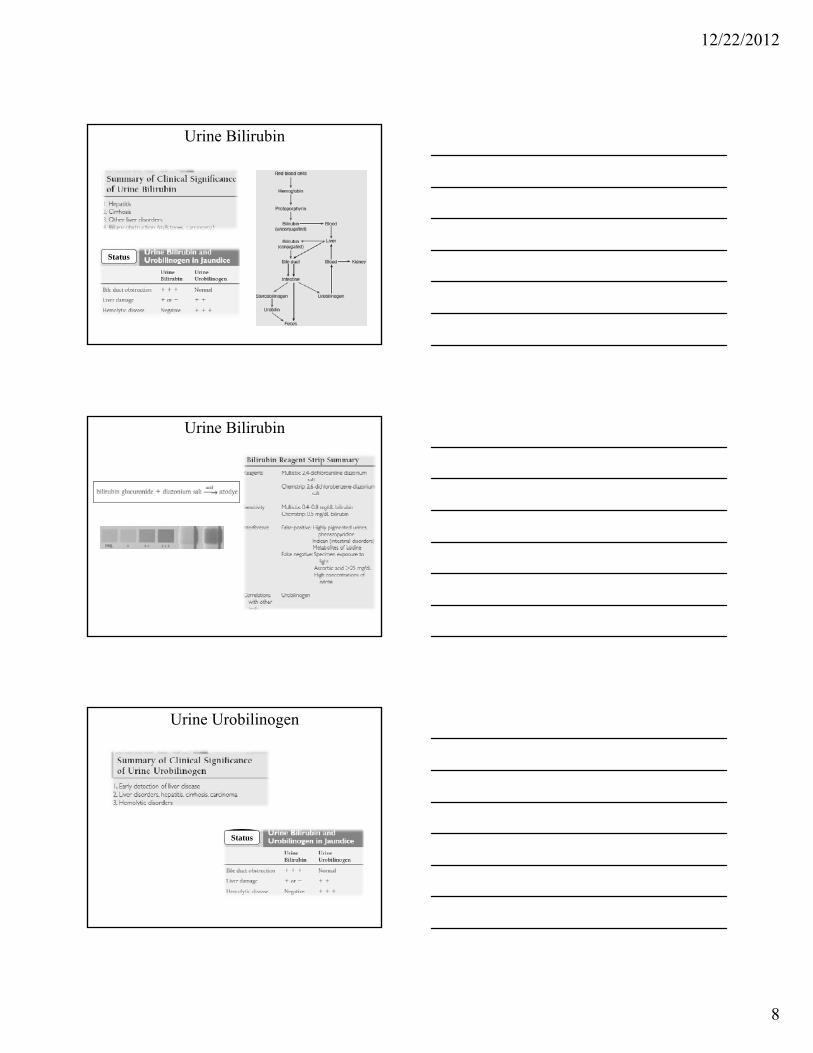
Urine Bilirubin
Status
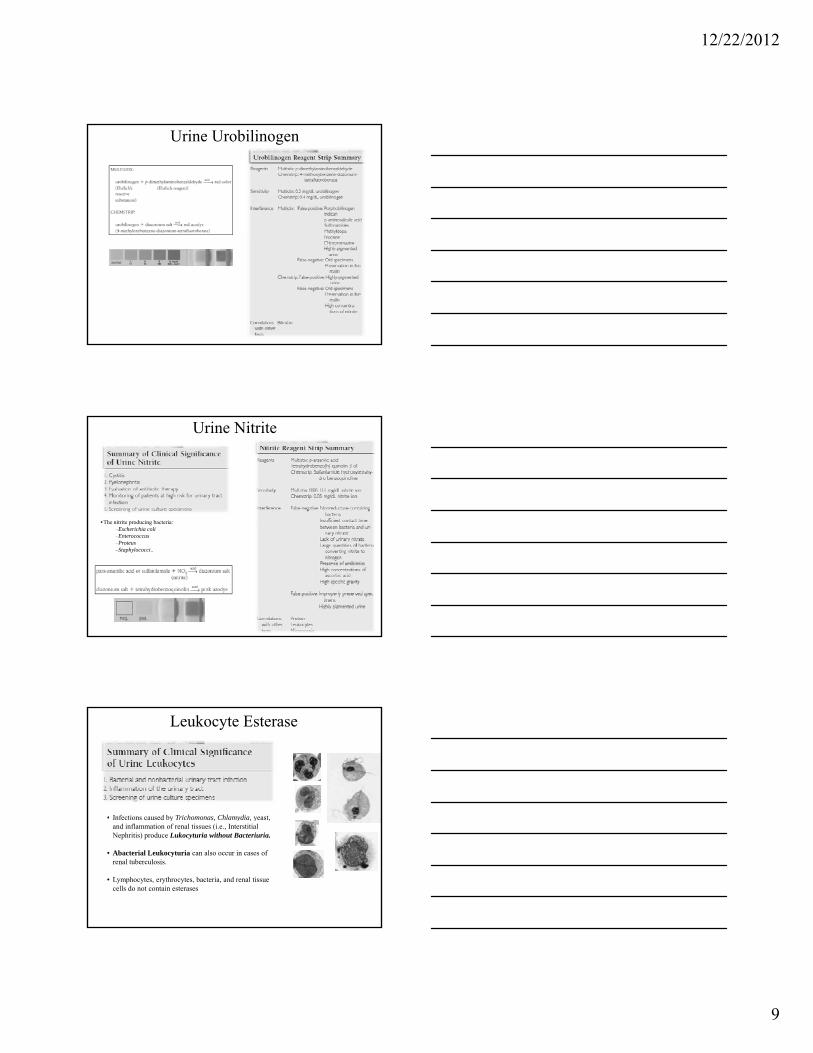
Urine Bilirubin
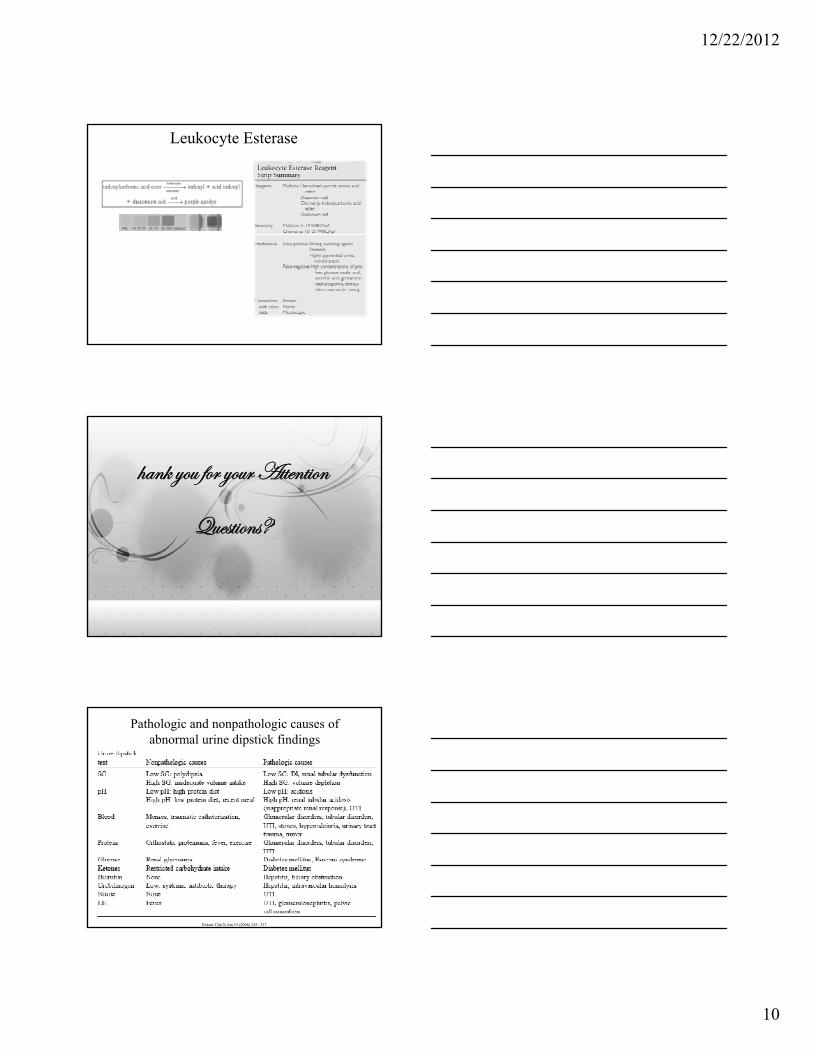
Urine Urobilinogen
Status
12/22/2012
9
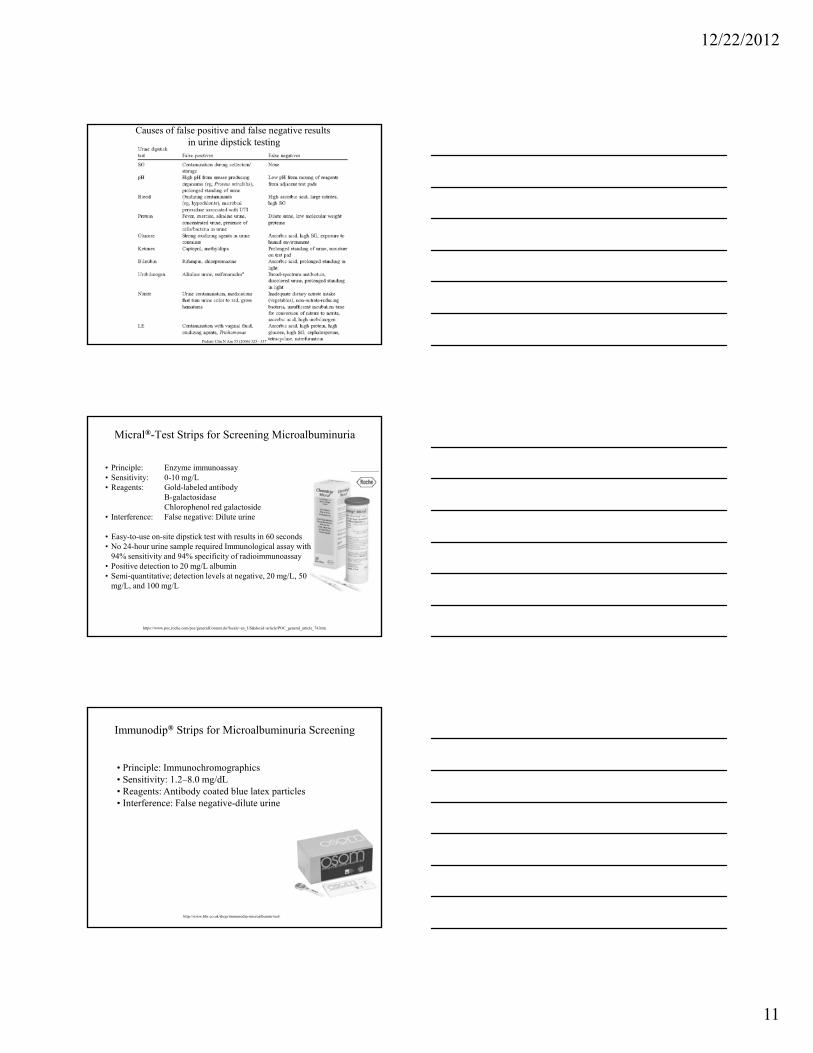
Urine Urobilinogen
Urine Nitrite
•The nitrite producing bacteria:–Escherichia coli–Enterococcus–Proteus–Staphylococci..
Leukocyte Esterase
• Infections caused by Trichomonas Chlamydia yeast• Infections caused by Trichomonas, Chlamydia, yeast, and inflammation of renal tissues (i.e., Interstitial Nephritis) produce Lukocyturia without Bacteriuria.
• Abacterial Leukocyturia can also occur in cases of renal tuberculosis.
• Lymphocytes, erythrocytes, bacteria, and renal tissue cells do not contain esterases
12/22/2012
10
Leukocyte Esterase
{tÇ~ çÉâ yÉÜ çÉâÜ TààxÇà|ÉÇ
d áà| áRdâxáà|ÉÇáR
Pathologic and nonpathologic causes of abnormal urine dipstick findings
Pediatr Clin N Am 53 (2006) 325– 337
12/22/2012
11
Causes of false positive and false negative results in urine dipstick testing
Pediatr Clin N Am 53 (2006) 325– 337
Micral®-Test Strips for Screening Microalbuminuria
• Principle: Enzyme immunoassay• Sensitivity: 0-10 mg/L• Reagents: Gold-labeled antibody
B-galactosidaseChlorophenol red galactoside
• Interference: False negative: Dilute urine
• Easy-to-use on-site dipstick test with results in 60 seconds• No 24-hour urine sample required Immunological assay with
94% sensitivity and 94% specificity of radioimmunoassay• Positive detection to 20 mg/L albumin • Semi-quantitative; detection levels at negative, 20 mg/L, 50
mg/L, and 100 mg/L
https://www.poc.roche.com/poc/generalContent.do?locale=en_US&docid=article/POC_general_article_74.htm
Immunodip® Strips for Microalbuminuria Screening
• Principle: Immunochromographics• Sensitivity: 1.2–8.0 mg/dL• Reagents: Antibody coated blue latex particles• Interference: False negative-dilute urine
http://www.bhr.co.uk/shop/immunodip-microalbumin-test/
12/22/2012
12
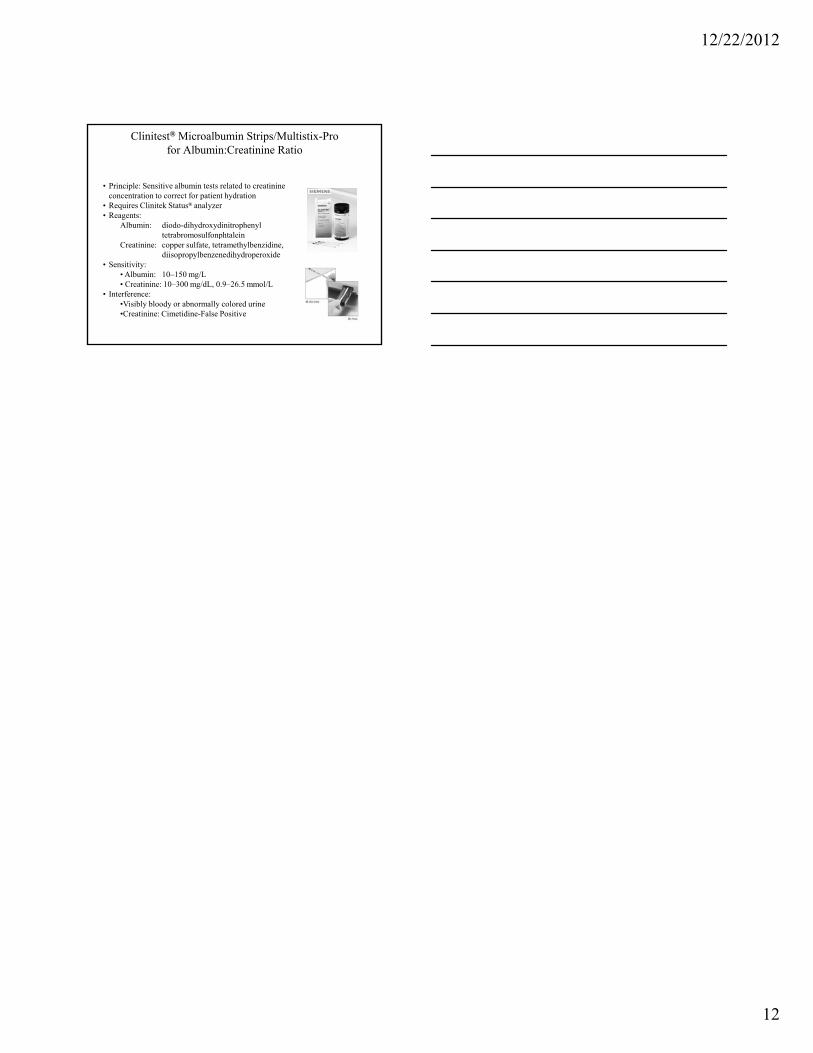
Clinitest® Microalbumin Strips/Multistix-Pro for Albumin:Creatinine Ratio
• Principle: Sensitive albumin tests related to creatinine concentration to correct for patient hydration
• Requires Clinitek Status® analyzer • Reagents:
Albumin: diodo-dihydroxydinitrophenyl tetrabromosulfonphtaleintetrabromosulfonphtalein
Creatinine: copper sulfate, tetramethylbenzidine,diisopropylbenzenedihydroperoxide
• Sensitivity:• Albumin: 10–150 mg/L• Creatinine: 10–300 mg/dL, 0.9–26.5 mmol/L
• Interference:•Visibly bloody or abnormally colored urine•Creatinine: Cimetidine-False Positive










![PREDAVANJE (3) [Read-Only] · 3 Shematski prikaz nastanka serozne tekućine IZVOR:S. King Strasinger, M. Schaub Di Lorenzo. Urinalysis and Body Fluids. F.A.Davis Company (2008);222](https://img.pdfslide.tips/doc/110x75/5f5fd63894580d06d734e1b9/predavanje-3-read-only-3-shematski-prikaz-nastanka-serozne-tekuine-izvors.jpg)