Embed Size (px)
Citation preview
Vitamin A:the enigmatic magic bullet
Betty Kirkwood
Dept of Nutrition & Public Health Intervention Research
Faculty of Epidemiology & Population Health
LSHTM
Vitamin A: An essential micronutrient
Metabolic roles Vision Maintenance of epithelial cells Immune system Growth Fertility
Clinical deficiency Nightblindness Xerophthalmia: Dry eye disease Blindness
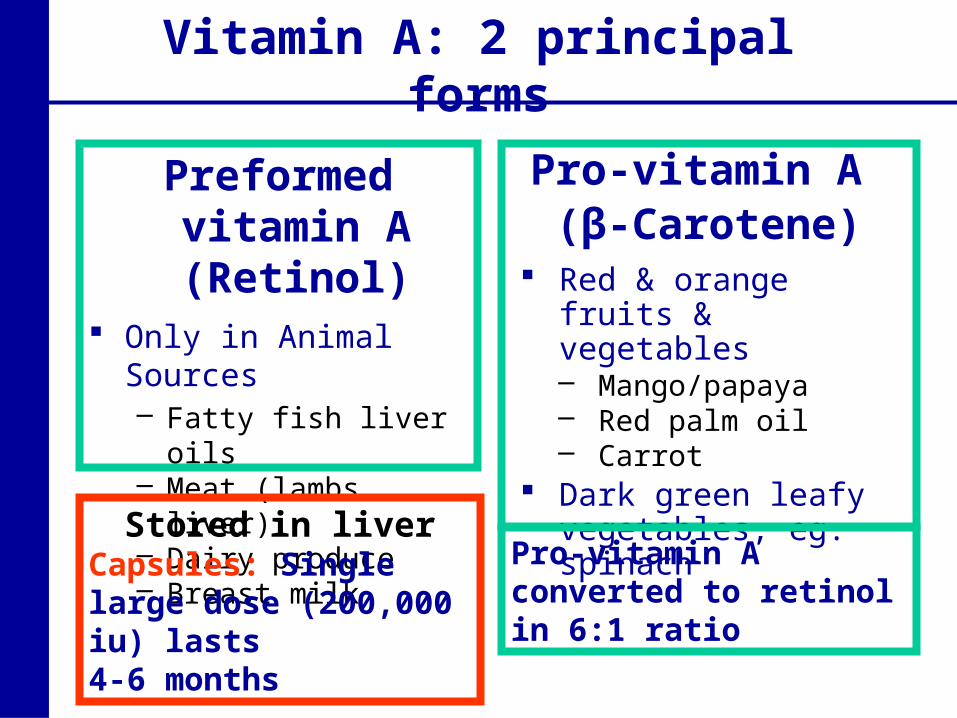
Vitamin A: 2 principal forms
Preformed vitamin A (Retinol)
Only in Animal Sources– Fatty fish liver oils– Meat (lambs liver)– Dairy produce– Breast milk
Pro-vitamin A (β-Carotene)
Red & orange fruits & vegetables– Mango/papaya– Red palm oil– Carrot
Dark green leafy vegetables, eg. spinach
Pro-vitamin A converted to retinol in 6:1 ratio
Stored in liverCapsules: Single large dose (200,000 iu) lasts 4-6 months
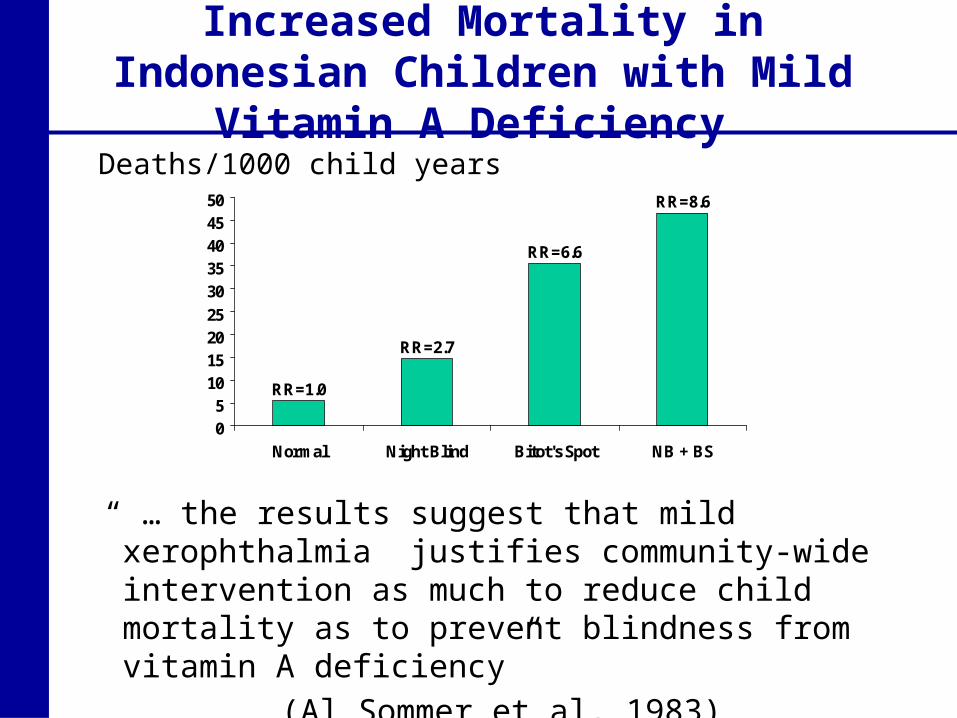
Increased Mortality in Indonesian Children with Mild Vitamin A Deficiency
RR=8.6
RR=6.6
RR=2.7
RR=1.0
05
10152025
3035404550
Normal Night Blind Bitot's Spot NB + BS
Deaths/1000 child years
“ … the results suggest that mild xerophthalmia justifies community-wide intervention as much to reduce child mortality as to prevent blindness from vitamin A deficiency”
(Al Sommer et al, 1983)
Vitamin A and child mortality:controversy in the late 1980’s
The Lancet, May 24, 1986
Vitamin A supplements decreased childhood mortality by 34% in Sumatra,
Indonesia (Al Sommer et al)
This finding is at odds with much of the conventional wisdom on the aetiology of childhood death in developing countries
(Richard Feachem, Bull Hyg Trop Dis 1986)
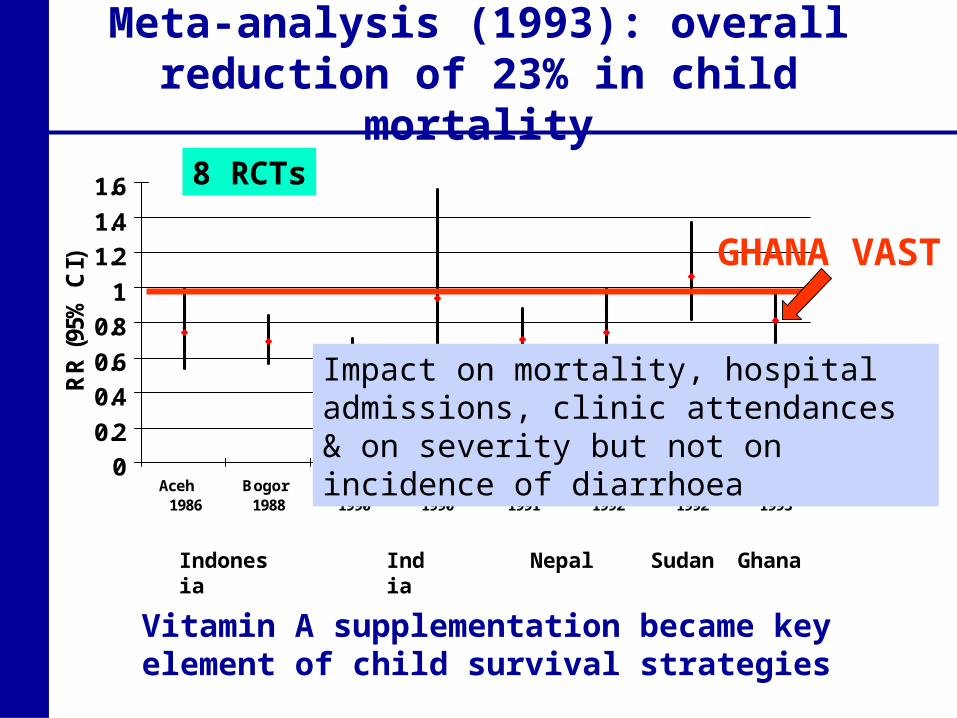
Meta-analysis (1993): overall reduction of 23% in child mortality
Indonesia India Nepal Sudan Ghana
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
Aceh 1986
Bogor 1988
Tamil Nadu1990
Hyderabad1990
Sarlahi 1991
Jumla 1992
Khartoum 1992
UER 1993
Summary Beaton etal, 1993
RR
(95
% C
I)
Vitamin A supplementation became key element of child survival strategies
8 RCTs
GHANA VAST
Impact on mortality, hospital admissions, clinic attendances & on severity but not on incidence of diarrhoea
An interesting policy response
World Development Report, 1993Investing in Health Vitamin A supplementation a “Best Buy”Linked to first three doses of DPT at 6, 10 and
14 weeks of age WHO/UNICEF planning to recommend
for adoption at EPI Global Advisory Group meeting in Philipines
BUT trials demonstrated impact in 6-59 month age range
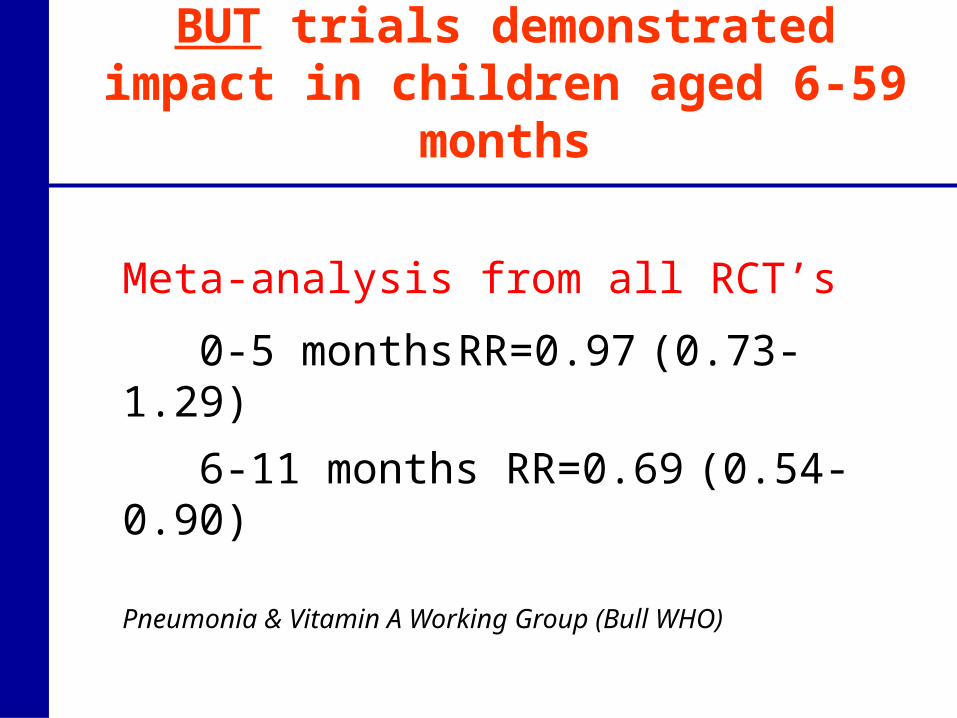
Meta-analysis from all RCT’s
0-5 months RR=0.97 (0.73-1.29)
6-11 months RR=0.69 (0.54-0.90)
Pneumonia & Vitamin A Working Group (Bull WHO)
BUT trials demonstrated impact in children aged 6-59 months
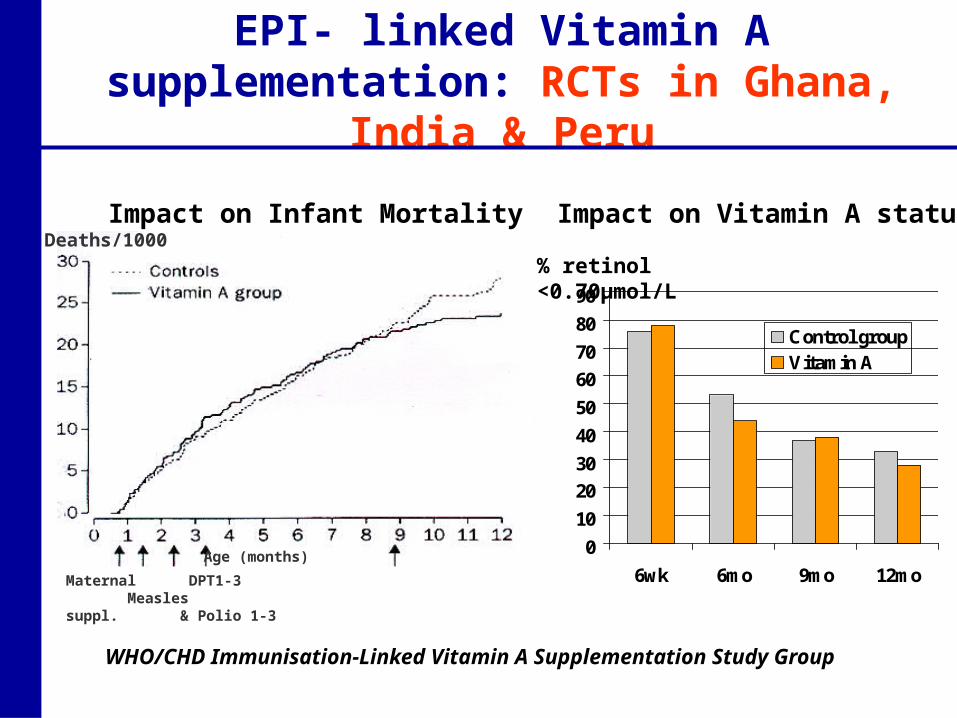
EPI- linked Vitamin A supplementation: RCTs in Ghana, India & Peru
Deaths/1000
Maternal DPT1-3 Measlessuppl. & Polio 1-3
Age (months)0
10
20
30
40
50
60
70
80
90
6wk 6mo 9mo 12mo
Control groupVitamin A
WHO/CHD Immunisation-Linked Vitamin A Supplementation Study Group
Impact on Infant Mortality Impact on Vitamin A status
% retinol <0.70µmol/L
Nepal trial: VAS of women of reproductive age
Keith West et al: IVACG 1998 & BMJ 1999 Weekly low dose supplements (of either retinol or
beta-carotene) to all women of childbearing age No impact on infant mortality BUT 44% reduction
in pregnancy related mortality (95%CI =16-63%), P<0.005
Implications for Safe Motherhood Programmes:Potential for impact in short-medium termCompared with emergency obstetric care & skilled birth
attendance at delivery: requires considerable health system strengthening
1. Start implementing right away:“Why waste 10 more years on research as was done with Vitamin A and child health?”
Trial in Nepal shows 44% reduction in pregnancy-related deaths: TWO views
2. Need to replicate before investing:• Does it really work? If not, we waste money
and divert resources away from improving access and coverage to EOC
• Even if it works, can we translate research findings into programmes?

Vitamin A & maternal mortality:New trials
Ghana: All women childbearing age,
Bangladesh: Pregnant women
Indonesia: Multivitamins & pregnant women
Ghana ObaapaVitA trial Cluster randomised double-blind
placebo controlled trial of weekly VAS (25,000 IU)
All women aged 15-45 years in 6 districts in Brong Ahafo region
4 weekly home surveillance– to monitor pregnancies, births, deaths
(women and infants), migration– to distribute capsules
Clusters: Geographically contiguous compounds of 100-200 women
Additional data collection activities (verbal post-mortems for cause of death, hospital data capture)
IEC Strategy to maximise adherence to capsules • GIS Mapping
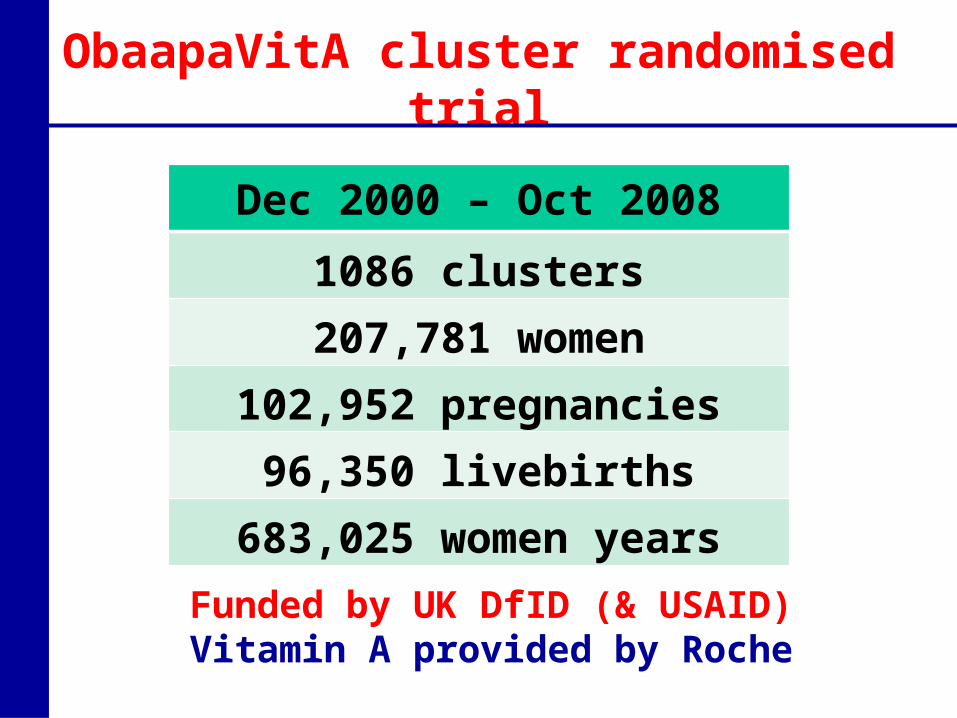
ObaapaVitA cluster randomised trial
Dec 2000 – Oct 2008
1086 clusters207,781 women
102,952 pregnancies96,350 livebirths
683,025 women years
Funded by UK DfID (& USAID)Vitamin A provided by Roche
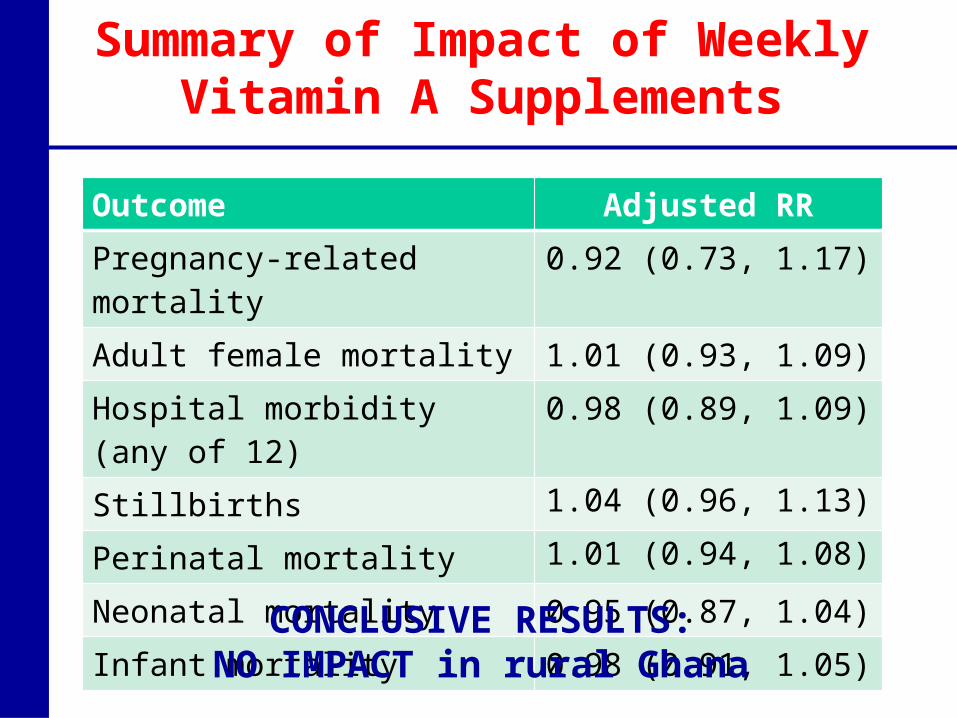
Summary of Impact of Weekly Vitamin A Supplements
Outcome Adjusted RR
Pregnancy-related mortality 0.92 (0.73, 1.17)
Adult female mortality 1.01 (0.93, 1.09)
Hospital morbidity (any of 12) 0.98 (0.89, 1.09)
Stillbirths 1.04 (0.96, 1.13)
Perinatal mortality 1.01 (0.94, 1.08)
Neonatal mortality 0.95 (0.87, 1.04)
Infant mortality 0.98 (0.91, 1.05)
CONCLUSIVE RESULTS:NO IMPACT in rural Ghana
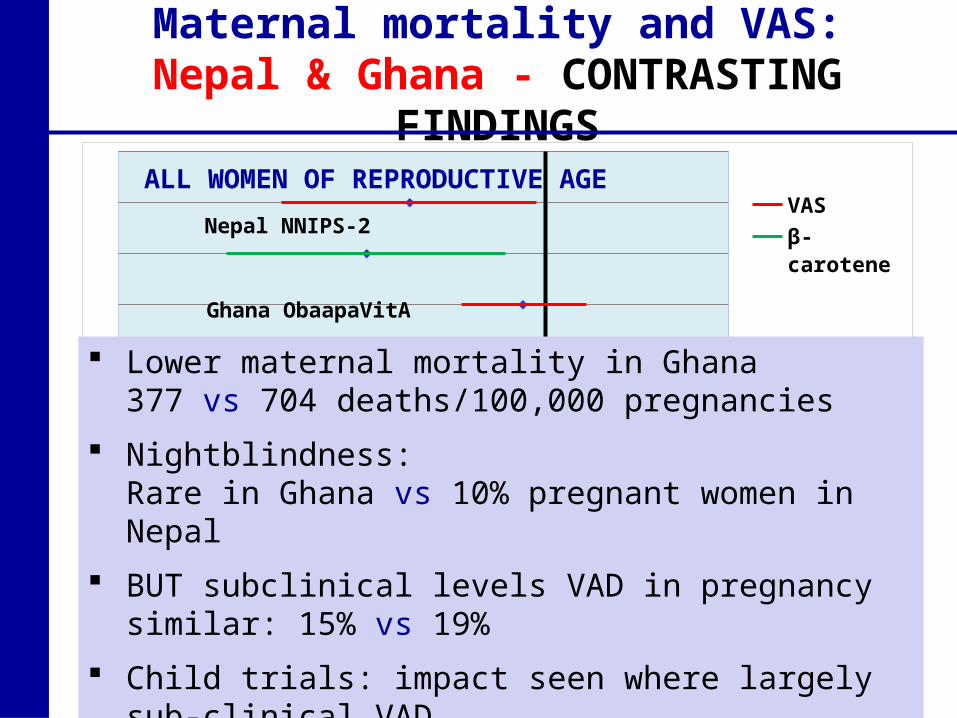
Maternal mortality and VAS:Nepal & Ghana - CONTRASTING FINDINGS
0.2 2
VAS
β-caroteneNepal NNIPS-2
Ghana ObaapaVitA
Bangladesh JiVitA
Indonesia SUMMIT
ALL WOMEN OF REPRODUCTIVE AGE
PREGNANT WOMEN
RR (95%CI)1
Lower maternal mortality in Ghana377 vs 704 deaths/100,000 pregnancies
Nightblindness: Rare in Ghana vs 10% pregnant women in Nepal
BUT subclinical levels VAD in pregnancy similar: 15% vs 19%
Child trials: impact seen where largely sub-clinical VAD
0.2 2
VAS
β-caroteneNepal NNIPS-2
Ghana ObaapaVitA
Bangladesh JiVitA
Indonesia SUMMIT
ALL WOMEN OF REPRODUCTIVE AGE
PREGNANT WOMEN
RR (95%CI)1
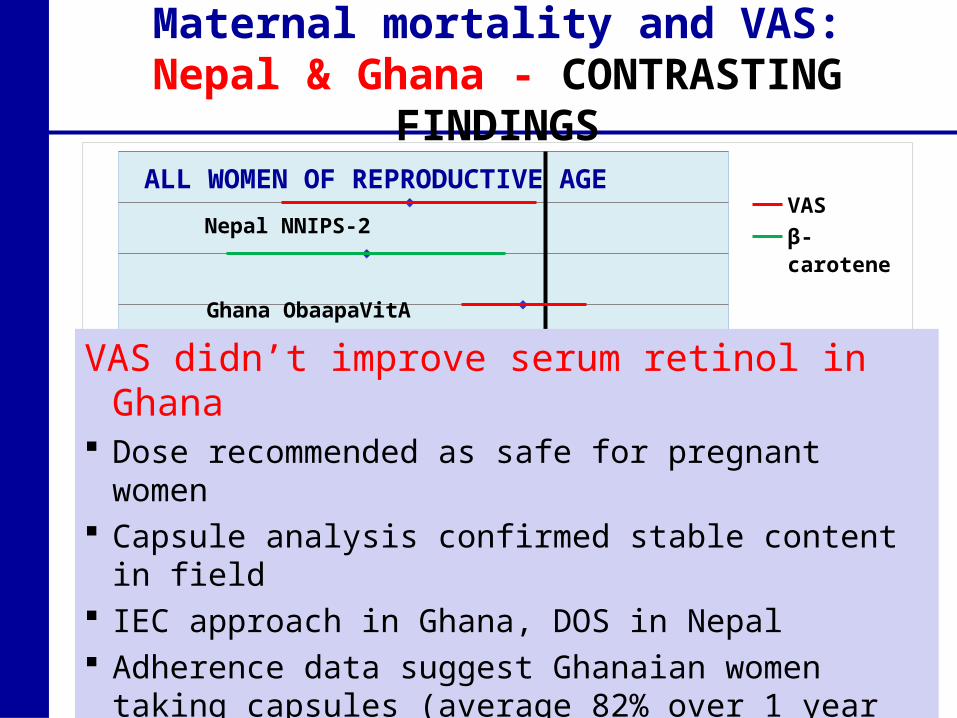
VAS didn’t improve serum retinol in Ghana Dose recommended as safe for pregnant women Capsule analysis confirmed stable content in field IEC approach in Ghana, DOS in Nepal Adherence data suggest Ghanaian women taking
capsules (average 82% over 1 year in serum survey) In Nepal VAS improved serum retinol, BUT β-carotene
didn’t
Maternal mortality and VAS:Nepal & Ghana - CONTRASTING FINDINGS
0.2 2
VAS
β-caroteneNepal NNIPS-2
Ghana ObaapaVitA
Bangladesh JiVitA
Indonesia SUMMIT
ALL WOMEN OF REPRODUCTIVE AGE
PREGNANT WOMEN
RR (95%CI)1
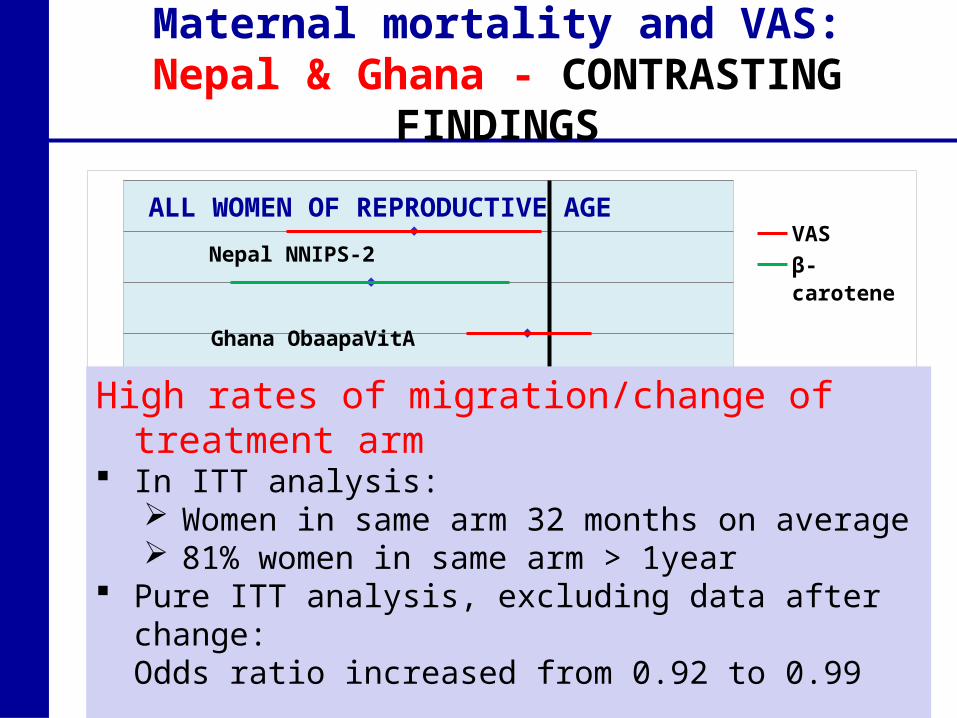
High rates of migration/change of treatment arm In ITT analysis:
Women in same arm 32 months on average 81% women in same arm > 1year
Pure ITT analysis, excluding data after change:Odds ratio increased from 0.92 to 0.99
Maternal mortality and VAS:Nepal & Ghana - CONTRASTING FINDINGS
0.2 2
VAS
β-caroteneNepal NNIPS-2
Ghana ObaapaVitA
Bangladesh JiVitA
Indonesia SUMMIT
ALL WOMEN OF REPRODUCTIVE AGE
PREGNANT WOMEN
RR (95%CI)1
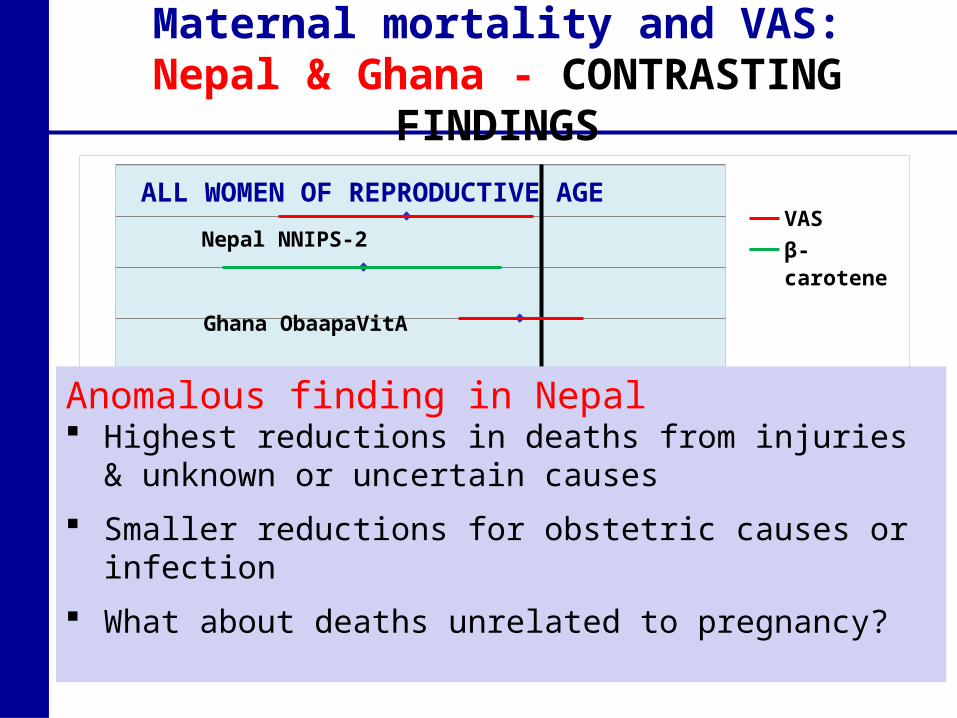
Anomalous finding in Nepal Highest reductions in deaths from injuries & unknown or
uncertain causes
Smaller reductions for obstetric causes or infection
What about deaths unrelated to pregnancy?
Maternal mortality and VAS:Nepal & Ghana - CONTRASTING FINDINGS
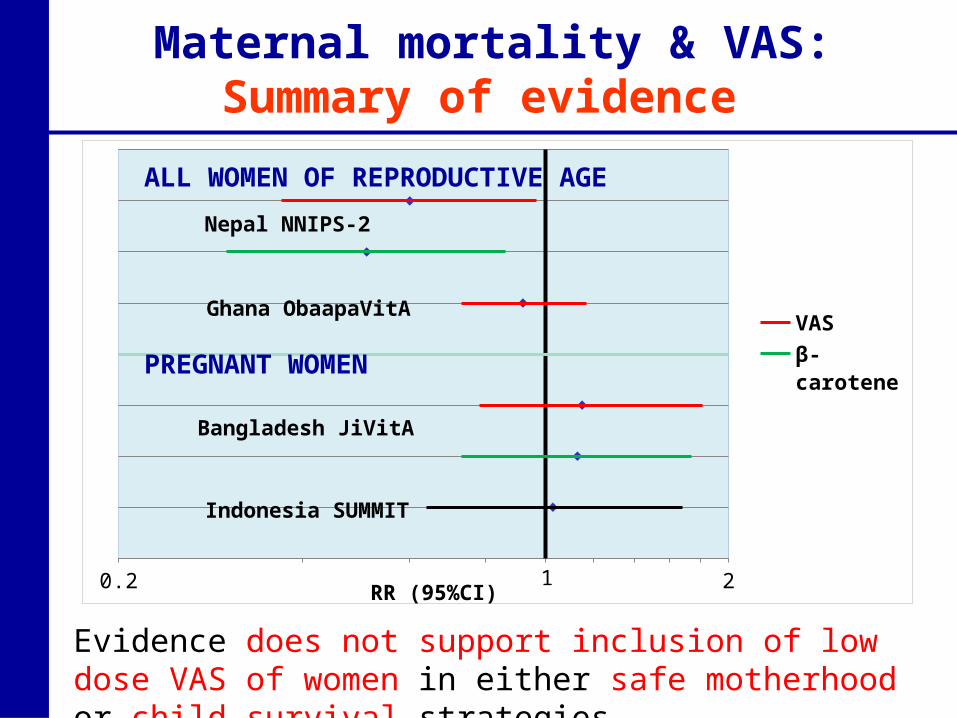
Maternal mortality & VAS:Summary of evidence
0.2 2
VASβ-caroteneMMN
Nepal NNIPS-2
Ghana ObaapaVitA
Bangladesh JiVitA
Indonesia SUMMIT
ALL WOMEN OF REPRODUCTIVE AGE
PREGNANT WOMEN
RR (95%CI)1
Evidence does not support inclusion of low dose VAS of women in either safe motherhood or child survival strategies
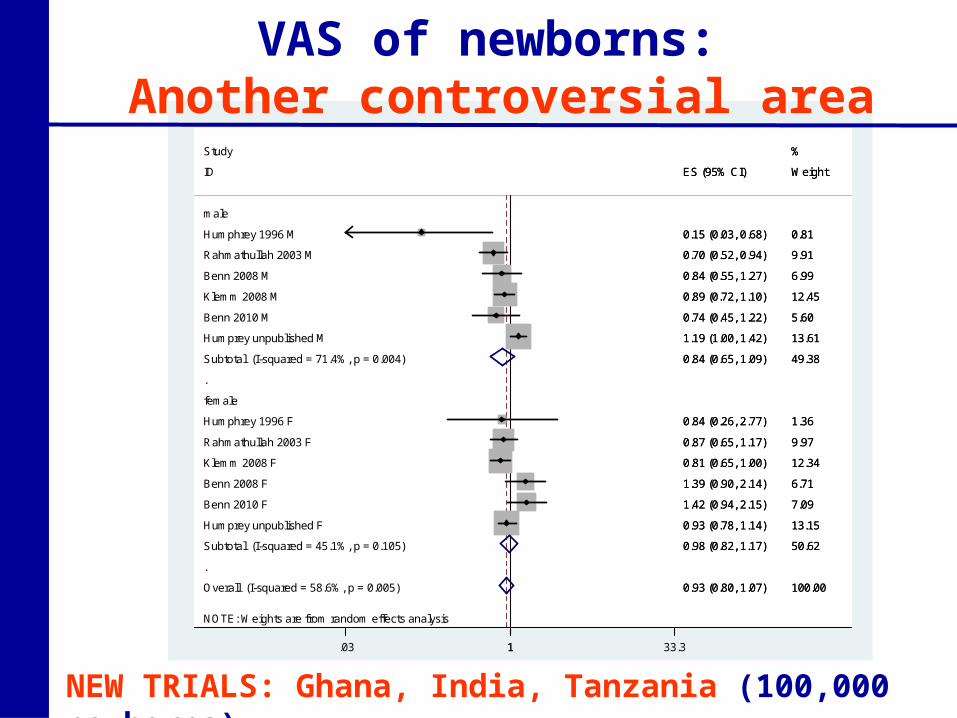
NOTE: Weights are from random effects analysis
.
.
Overall (I-squared = 58.6%, p = 0.005)
Klemm 2008 M
Humprey unpublished M
Rahmathullah 2003 M
Klemm 2008 F
ID
Rahmathullah 2003 F
Benn 2010 M
female
Humphrey 1996 F
Subtotal (I-squared = 45.1%, p = 0.105)
Benn 2010 F
Benn 2008 F
Subtotal (I-squared = 71.4%, p = 0.004)
Study
Benn 2008 M
Humphrey 1996 M
Humprey unpublished F
male
0.93 (0.80, 1.07)
0.89 (0.72, 1.10)
1.19 (1.00, 1.42)
0.70 (0.52, 0.94)
0.81 (0.65, 1.00)
ES (95% CI)
0.87 (0.65, 1.17)
0.74 (0.45, 1.22)
0.84 (0.26, 2.77)
0.98 (0.82, 1.17)
1.42 (0.94, 2.15)
1.39 (0.90, 2.14)
0.84 (0.65, 1.09)
0.84 (0.55, 1.27)
0.15 (0.03, 0.68)
0.93 (0.78, 1.14)
100.00
12.45
13.61
9.91
12.34
Weight
9.97
5.60
1.36
50.62
7.09
6.71
49.38
%
6.99
0.81
13.15
0.93 (0.80, 1.07)
0.89 (0.72, 1.10)
1.19 (1.00, 1.42)
0.70 (0.52, 0.94)
0.81 (0.65, 1.00)
ES (95% CI)
0.87 (0.65, 1.17)
0.74 (0.45, 1.22)
0.84 (0.26, 2.77)
0.98 (0.82, 1.17)
1.42 (0.94, 2.15)
1.39 (0.90, 2.14)
0.84 (0.65, 1.09)
0.84 (0.55, 1.27)
0.15 (0.03, 0.68)
0.93 (0.78, 1.14)
100.00
12.45
13.61
9.91
12.34
Weight
9.97
5.60
1.36
50.62
7.09
6.71
49.38
%
6.99
0.81
13.15
1.03 1 33.3
VAS of newborns: Another controversial area
NEW TRIALS: Ghana, India, Tanzania (100,000 newborns)
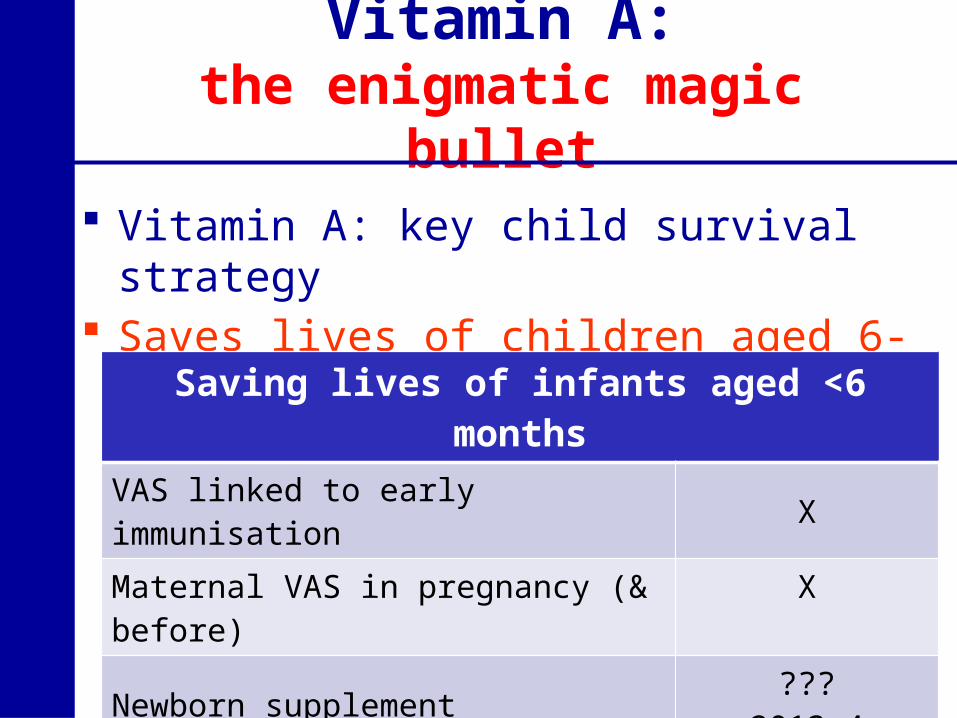
Vitamin A:the enigmatic magic bullet
Vitamin A: key child survival strategy Saves lives of children aged 6-59 months
Saving lives of infants aged <6 months
VAS linked to early immunisation Χ
Maternal VAS in pregnancy (& before) Χ
Newborn supplement ???2013-4
Vitamin A Research: 24 years Ghana Health Service/LSHTM collaboration