Embed Size (px)
Citation preview

1. Diabetes, ein kardiovaskuläres Problem 2. Definitionen - Insulinresistenz 3. Warum welche OAD? 4. Einige Besonderheiten
Chiemgauer Kardiologentage 20.9.2014
Was der Kardiologe über die orale Diabetestherapie wissen sollte
Prof. Dr. Erland Erdmann, FESC, FACC, FAHA University of Cologne/Germany, Heart Center

Selvin et al., NEJM 2010;362:800-11

Prevalence of total confirmed diabetes and obesity.
National Health and Nutrition Examination Survey
Selvin et al., Ann Intern Med. 2014;160:517

Das kardiovaskuläre Risiko des Diabetikers
1. Makrovaskuläres Risiko Herzinfarkt, Herzinsuffizienz, Schlaganfall,
PAVK, Tod
2. Mikrovaskuläres Risiko Nephropathie, Neuropathie, Retinopathie

Der Typ 2 Diabetiker leidet an: (altersabhängig)
1. Hypertonus (>40%) 2. KHK (50 - 70%) 3. Chron. Herzinsuffizienz (20%, 12%/Jahr) 4. Vorhofflimmern 5. Chron. Niereninsuffizienz (15-25%)

Typ 2 Diabetes ist eine kardiovaskuläre Krankheit !
1. Eine gute metabolische Einstellung vermindert mikro- (und makro-) vaskuläre Komplikationen
2. Die Prognose des Diabetikers hängt von seinem makrovaskulären Risiko ab
5. Die BZ- (HbA1c)-Senkung sollte Tod, Herzinfarkt und Schlaganfall reduzieren
6. Hypoglykämien müssen vermieden werden



Glycaemic continuum and cardiovascular disease

DM Typ 2 - ein kardiovaskuläres Problem (= eine kardiovaskuläre Erkrankung)
Das metabolische Syndrom
= eine Summe von kardiovaskulären Risikofaktoren:
Adipositas Hypertonie pathologische Blutfette (Trigl. hoch, HDL niedrig) Hohe Glukose- bzw. HbA1c-Werte

Typ 2 DM ist nicht nur eine einfache Störung des Glukosemetabolismus
Es reicht nicht, den Blutzucker gut einzustellen
DM Typ 2 ist eine komplexe metabolische Krankheit – Insulinresistenz steht im Zentrum

Insulinresistenz
Insulin bindet an seinen Rezeptor und stimuliert die Produktion von Glucosetransportproteinen, dadurch kann Glucose in die Zelle gelangen
Der Rezeptor ist insensitiv, weniger Transportmoleküle werden gebildet und weniger Glukose gelangt in die Zelle. Glukose bleibt im Blut erhöht.
Normal Insulin resistant

Auswirkungen der Insulinresistenz
Insulin Resistance
Low HDL
Hyper- insulinemia
Hyper- glycemia
Endothelial
dysfunction
Impaired fibrinoly
sis
Hyper- coagula-
bility
Atherosclerosis CVD Stroke
Renal failure
Chronic Inflamm
ation
Hypertri-
glycerid-
emia
Hyper- tension
Smalldense LDL

Because insulin resistance plays a fundamental role in the pathogenesis of type 2 diabetes and especially its adverse cardiovascular outcomes, interven>ons should ini>ally be aimed towards improvement in >ssue insulin sensi>vity.
Michael Stumvoll, Lancet 2005; 365:1333

Options for Antidiabetic Treatment
Glucose dependent
GLP-1 Mimetics (Exenatide, Liraglutide)
α-Glucosidase Inhibitors
(Acarbose, Miglitol, Voglibose)
DPP-4 Inhibitors (Sitagliptin, Vildagliptin, Saxagliptin, Linagliptin, Alogliptin)
Glucose independent
Exogenous Insulin
Glinides
Sulfonylurea
Metformin Pioglitazone
Inhibition of Glucose
Resorption
Insulin Resistance Insulin Secretion
SGLT2-Inhibitors (Dapagliflozin, Canagliflozin, Empagliflozin)

Pharmacological treatment options for T2DM
ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases 2013

UKPDS: clinical outcomes for meFormin
UKPDS 34. Lancet 1998; 352: 854–865
Newly diagnosed overweight patients
Proportion of patients with events
60
40
20
0 0 3 6 9 12 16
Years from randomisation
Clinical outcomes for METFORMIN Heart attacks CV death Total mortality
RR
↓39% ↓42% ↓36%
Any diabetes-related endpoint Lifestyle (n = 411) SU or insulin (n = 951)
MET (n = 342)
CV, cardiovascular; RR, risk reduction
(%)

„Addition of metformin to sulphonylurea therapy also increased the risk of death from any cause (60% increase, p=0.041). There were no significant differences between the groups for the other aggregate endpoints.“
Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2
diabetes (UKPDS 34)
The Lancet 1998;352:854-65


The risk of heart failure in patients with type 2 diabetes treated with oral agent monotherapy
McAlister et al., European Journal of Heart Failure 10 (2008) 703
n = 5631, mean age 65.8 years

Sulfonylharnstoffe
stimulieren die Insulinfreisetzung aus den β-Zellen unabhängig von der Blutglucosekonzentration
UAW: Hypoglykämien, gastrointestinale Beschwerden, Anämien,
Glibenclamid (Euglucon®, Normoglucon®, Glucobene®) Glibornurid (Gluborid®, Glutril®) Gliclazid (Diamicron®) Glipizid (Glibenese, Minidiab®) Gliquidon (Glurenorm®) wird über die Leber abgebaut Glisoxepid (Pro-Diaban®) Glycodiazin (Redul®) Glimepirid (Amaryl®)

Glinide „Sulfonylharnstoff-Analoga“
führen zu einer verstärkten Insulinfreisetzung wie Sulfonylharnstoffe die Einnahme der Glinide sollte kurz vor den Hauptmahlzeiten erfolgen
UAW: gastrointestinale Störungen, Hypoglykämien
Nateglinid Starlix®
Repaglinid NovoNorm®
Der Gemeinsame Bundesausschuss (B-BA) hat im Januar 2014 beschlossen, ergänzende versorgungsrelevante Studien zur Bewertung der Zweckmäßigkeit der Glinide zu fordern

Pharmacological treatment options for T2DM
ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases 2013
Glitazone einziger zugelassener Wirkstoff: Pioglitazon steigert die Empfindlichkeit des Gewebes auf Insulin maximale Wirkung erst nach etwa 4 Wochen
Metformin + Pioglitazon Metformin + Pioglitazon + Sulfonyllharnstoffe
Pioglitazon (Actos®) Pioglitazon + Metformin (Competact®)
Keine Hypoglykämien UAW: Herzinsuffizienz, Gewichtszunahme, Frakturen, (Blasen-Ca)
Pioglitazon kann nach einem Beschluss des G-BA seit 2011 nur noch in begründeten Ausnahmefällen zu Lasten der GKV verordnet werden

Effects of Oral Antidiabetic Drugs on HbA1c, Hypoglycemic Events & Weight Gain in 4 randomisied double
blind large Studies (Quartet) Hypo-glycemia
(%)
Weight Difference
(kg)
No. of Patients
SU = Sulfonylureas
HbA1c (%)
Weight Change
(kg)
4 Hanefeld et al; Diab.Care 2004;27:141
4 SU + Metformin
4 SU + Pioglitazone -1.36 -1.20
14.1 10.7
320 319
-1.0 +2.8
3.8
1 Schernthaner et al; JCEM 2004; 89:6068
1 Pioglitazone 1 Metformin
-1.4 -1.5
1.5 1.3
597 597
+1.9 -2.5 4.4
2 Pioglitazone
2 Charbonell et al; Diabet Med. 2005; 22:399
2 SU -1.4 -1.4
+2.8 +1.9
624 626
3.5 10.1 0.9
3 Metformin + SU 3 Metformin + Pioglitazone
-1.0
3 Matthews et al; Diab.Metab Res.Rev.2005; 21:167
-1.0 11.2 1.3
317 317
+1.4 +1.5
0.1

Time from Randomisation (months)
N at Risk:
HR 95% CI p value pioglitazone vs placebo 0.841 0.722, 0.981 0.0273 *
N events: 3-year estimate:
placebo 358 / 2633 14.4%
pioglitazone 301 / 2605 12.3%
Time to Main Secondary Endpoint (death, MI, stroke)
Kaplan-Meier event rate
0 6 12 18 24 30 36 5238 5102 4991 4877 4752 4651 786 (256)
0.0
0.05
0.10
0.15
Dormandy , Charbonnel, Eckland, Erdmann et al., Lancet 2005;366:1279–1289
The Proactive Study
16%
proactive-results.com

Erdmann et al., JACC 2007;49:1772–1780.
0.02
0.04
0.06
0.08
0.10
HR 95% CI p value
Pioglitazone vs placebo 0.72 0.52, 0.99 0.045
Pioglitazone
Placebo N events:
65/1230
88/1215
0.0
Pioglitazone’s effect on recurrent MI in patients with previous MI
Kap
lan-
Mei
er e
vent
rate
Time from randomisation (months) 0 6 12 18 24 30 36
The Proactive Study
28%
proactive-results.com
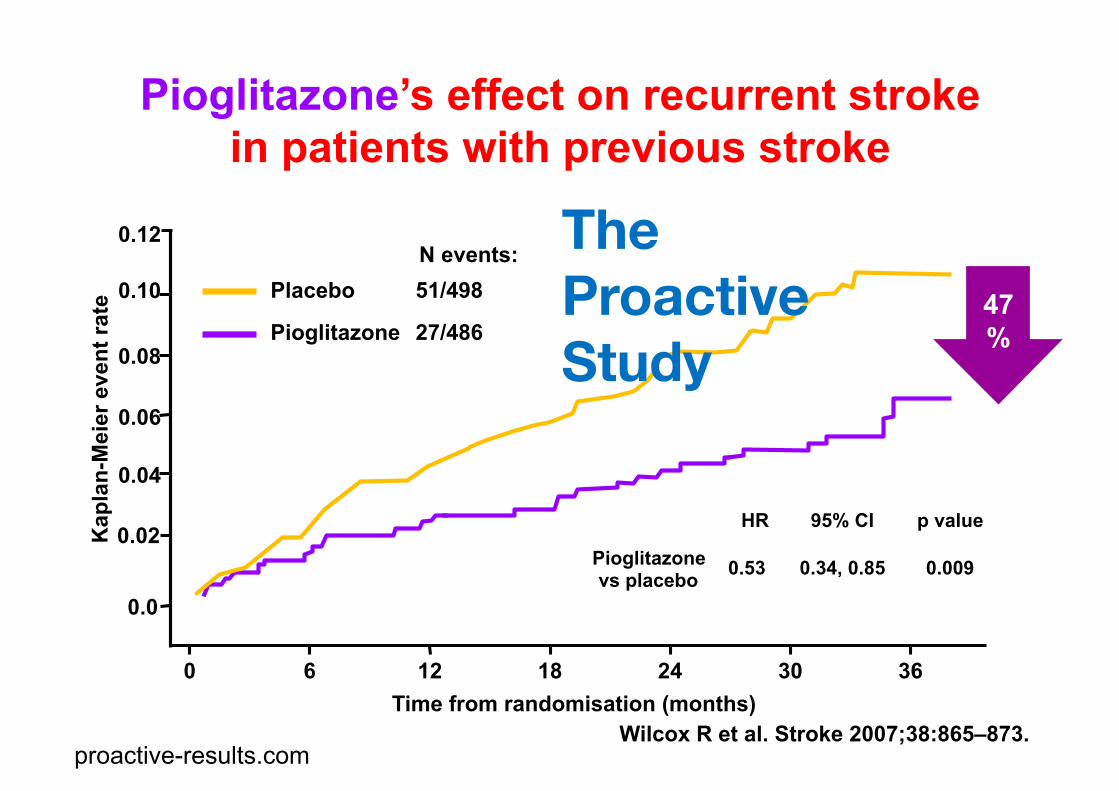
Wilcox R et al. Stroke 2007;38:865–873.
Pioglitazone’s effect on recurrent stroke in patients with previous stroke
0.12
0.04
0.06
0.08
0.10
0.02
Pioglitazone
Placebo N events:
27/486
51/498
HR 95% CI p value
Pioglitazone vs placebo 0.53 0.34, 0.85 0.009
0.0
Kap
lan-
Mei
er e
vent
rate
Time from randomisation (months) 0 6 12 18 24 30 36
The Proactive Study
47%
proactive-results.com

Effect of Pioglitazone Treatment on the Combined Endpoint of all-‐cause Mortality, Myocardial Infarc>on and
Stroke in Pa>ents with and without CKD (PROac>ve)
Kaplan-‐Meier es-mate of 3-‐year event rate Event Rate
0
5
10
15
20
25
%
107/961
30
Placebo: GFR <60 ml/mIn, 18.3% vs. 11.5%; HR=1.65 (P <0.0001)
Pioglitazone : Reduction of combined Endpoint from 21.4% vs. 14.6% HR=0.66 (p<0.0001)
GFR <45 GFR 45-<60 GFR 60-<75 GFR 75-<90 GFR ≥90 98/1005 19/73 12/61 50/250 28/213 79/541 70/578 90/763 82/709
Schneider CA, Ferrannini E, DeFronzo R, Schernthaner G, Yates J, Erdmann E. JASN 2008; 19:182-187

Wirkung von GLP-1 Agonisten und DPP-4 Hemmern

GLP-1 Rezeptor Agonisten Inkretinmimetika
wirken wie die körpereigenen Hormone Glukoseabhängiges insulinotropes Peptid (GIP) und Glucagon-like Peptid 1 (GLP-1)
Peptide, fördern die Insulinsynthese und –freisetzung, verzögern die Magenentleerung und reduzieren HbA1c um ~0,6 und KG um ~3Kg, selten Hypoglykämie
UAW: Übelkeit, Durchfall und Erbrechen, (Pankreatitis)
Liraglutid (Victoza®) sc. Exenatid (Byetta®) sc. (Bydureon®)

Inhibitoren der Dipeptidylpeptidase 4 (DPP4-Inhibitoren, Gliptine oder als Inkretinverstärker)
hemmen den Abbau des Hormons Glucagon-like Peptid 1 (GLP-1), steigern die Insulinausschüttung nur nach Nahrungsaufnahme,
Keine Hypoglykämien
UAW: Übelkeit, Erbrechen, Durchfall, Kopfschmerzen und eine erhöhte Anfälligkeit für Infektionskrankheiten
Sitagliptin (Januvia®, Xelevia®, Janumet®) Vildagliptin (Galvus®, Jalra®, Eucreas®) Linagliptin (Trajenta®) Saxagliptin (Onglyza®)

SGLT2-Hemmer Hemmung des Natrium-Glucose-Cotransporters 2 (SGLT2)
die Wirkung ist Insulin-unabhängig, führen zu einer verstärkten Ausscheidung der Glucose über den Harn
UAW: Harnwegsinfektionen, häufiges Wasserlassen und eine vermehrte Urinausscheidung
Canagliflozin (Invokana®) Dapagliflozin (Forxiga®) Empagliflozin (Jardiance®)

1. Das Problem der Herzinsuffizienz
2. Der optimale HbA1c- Wert
3. Kontrastmittel

Heart Failure and Mortality in the Elderly with Diabetes
0.00
0.50
0.75
Proportion Surviving
0 1 2 3 4 5
Diabetes without Heart Failure (n=69.083)
Diabetes with Incident Heart Failure (n=46.720) 0,25 0.20
(Bertoni et al., Diabetes Care 2004; 27:699)
1.00
Mortality was 80% after 3 years
years

Survival of Patients with Type 2 Diabetes in Cologne
P<0.001
Pfister, R., Thekanal, J., Hellmich, M., Erdmann, E., Schneider, C.: Acta Diabetologia 2007; 44: 91-97
Days after discharge 0 200 400 600 800 1000 1200 1400
0,0
0,2
0,4
0,6
0,8
1,0 Su
rviv
al (%
) NT-pro-BNP
Inframedian Supramedian
Survival
n = 128, average age = 68 years
median NT-proBNP: 474 ng/l hazard ratio 3,3

Lincoff et al., JAMA 2007;298:1180–1188.
Risk of serious HF with pioglitazone: data from the Lincoff meta-‐analysis
Weeks 0 20 40 60 80 100 120
0
4
8
10
Est
imat
ed e
vent
rate
(%)
140
2
6
HR 95% CI p value pioglitazone vs control 1.41 1.14, 1.76 0.002
0
4
8
10
2
6
Pioglitazone
Control
(n = 16.390)

Lincoff et al., JAMA 2007;298:1180–1188. Weeks
0 20 40 60 80 100 120 0
4
8
10
Est
imat
ed e
vent
rate
(%)
140
2
6
0
4
8
10
2
6
Pioglitazone
Control
(n = 16.390)
Risk of death, MI or stroke with pioglitazone: data from the Lincoff meta-‐analysis
HR 95% CI p value pioglitazone vs control 0.82 0.72, 0.94 0.005

1. Das Problem der Herzinsuffizienz
2. Der optimale HbA1c- Wert
3. Kontrastmittel

Rela>onship of Hemoglobin A1C and Mortality in Heart Failure Pa>ents With Diabetes
Aguilar D et al. J Am Coll Cardiol 2009;54:422–8
n = 5.815 FU 2 Jahre

OAD insulin
Es gibt keinen Beweis für den Nutzen einer HbA1c-Einstellung <7% beim Typ 2 Diabetes hinsichtlich makrovaskulärer Risiken
Hypoglykämien müssen vermieden werden

1. Das Problem der Herzinsuffizienz
2. Der optimale HbA1c- Wert
3. Kontrastmittel

Known diabetes 29.4 % 65.4 Newly diagnosed DM 15.9 % 72.6 IGT or IFG 20.0 % 69.6 No diabetes 34.7 % 58.3
(22 German Cardiac Centers, 750 consecutive patients)
significant CAD (%)
Schöndorf, Lübben, Karagiannis, Erdmann, Forst, Pfützner Diabetes & Vascular Disease Research 7 (2010) 145–150
ACS Patients Undergoing Cardiac Catherization – Relation to Diabetes The DIASPORA study

Circulation 2012;126:296
Crea 25% or 0.5 mg/dL above baseline at 48 hours

MeFormin und KontrastmiVel beim Diabe>ker
Einige Zahlen: Metformin wird unverändert renal ausgeschieden Bioverfügbarkeit 50 – 60% Maximale Konzentration im Blut nach 2 – 4 Std. Plasmahalbwertzeit ~3 Std. Maximale Wirkdauer 5 – 6 Std. Wenn Metformin nicht mehr zugeführt wird, ist eine Kumulation unmöglich, damit keine Laktazidose durch toxische Spiegel FDA-approved package insert: ACR Bulletin 1998; 54(3): 15 “Metformin should be stopped at or before the administration of intravascular contrast. It is not necessary to stop metformin 48 hours before the exam.”
Kontrastmittelinduzierte Nephropathie (=Krea >0,5 mg/dl oder >25%) in ~50%
ESC Guidelines 2014: „administration of metformin should be suspended before angiography or PCI, and resumed 48 hours later“

Anfängliche Medikamenten- Monotherapie
Gesunde Ernährung, Gewichtskontrolle, körperliche Aktivität
Metformin hoch niedriges Risiko neutral/Abnahme GI/Laktatazidose niedrig
Wenn notwendig, um individuell vereinbarten HbA1c Zielbereich zu erreichen, Einführung eines 2. Medikaments
hoch moderates Risiko Zunahme Hypoglykämie niedrig
Metformin +
Metformin +
Metformin +
Metformin +
Metformin +
Wirksamkeit(↓ HbA1c) Hypoglykämie Körpergewicht Sicherheit/Vertäglichkeit Kosten
Sulfonylharnst.
hoch niedriges Risiko Zunahme Ödem, anderea
hoch
Thiazolidin- dion
mittel niedriges Risiko neutral selten
hoch
DPP-4- Hemmer
hoch niedriges Risiko Abnahme GI, andereb
hoch
GLP-1 Rezeptor- Agonist
am höchsten hohes Risiko Zunahme Hypoglykämie
variabel
Insulin (meist „Basal“)
Zwei-Medikamenten-Kombination
Sulfonylharnst. +
Thiazolidin-dion +
DPP-4 Hemmer +
GLP-1 Rezeptor-Agonist +
Insulin (meist „Basal“) +
Metformin +
Metformin +
Metformin +
Metformin +
Metformin +
TZD
DPP-4-I
GLP-1-RA
Insulin
SU
DPP-4-I
GLP-1-RA
Insulin
SU SU SU
TZD TZD TZD
DPP-4-I Insulin Insulin
Insulin (mehrfach tägliche Injektionen)
Drei-Medikamenten-Kombination
Komplexere Insulin-Regime
or
or
or
or
or
or
or
or
or
or
or
or
Wirksamkeit(↓ HbA1c) Hypoglykämie Körpergewicht Sicherheit/Vertäglichkeit Kosten
Wenn notwendig, um individuell vereinbarten HbA1c Zielbereich zu erreichen, Einführung eines 3. Medikaments
Wenn notwendig, um individuell vereinbarten HbA1c Zielbereich zu erreichen, Einführung eines komplexeren Insulin-Regimnes

Competitive Landscape 2013 2014 2015 2016 2017 2018 2019 2020
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Aleglitazar
CV agents
Glucose lowering agents
AleCardio
Roche High likelihood to show CV benefit Low likelihood to show CV benefit
Medium likelihood to show CV benefit
AleGlucose
- PLA2i - CETPi
- SGLT2i - CAI
Saxagliptin (SAVOR)
Lixisenatide (ELIXA)
Liraglutide (LEADER)
Canagliflozin (CANVAS)
Sitagliptin (TECOS)
Alogliptin (EXAMINE)
Semaglutide (SUSTAIN-6)
MK-3102 QW DPP-IV
Exenatide QW (EXSCEL)
Linagliptin (CAROLINA)
Empagliflozin (C-SCADE8)
Dulaglutide (REWIND)
Darapladib (STABILITY)
Darapladib (SOLID)
Evacetrapib (ACCELERATE)
Anacetrapib (REVEAL)
Alirocumab (ODYSSEY)
Ezetimibe (IMPROVE-IT)
- DPP-4i - GLP-1
- Niacin - PCSK9i
Dapagliflozin (DECLARE)
Canakinumab (CANTOS)
Stopped July 2013

Was der Kardiologe über die orale Diabetestherapie wissen sollte
1. Gesunde Ernährung, körperlichen Aktivität & Schulung: =Basis jeglicher Therapie des T2DM
2. Wenn nicht kontraindiziert, Metformin = optimales Erstlinien-Medikament
3. Nach Metformin sind die Daten begrenzt. 4. Kombinations-Therapie mit 1-2 anderen oralen/injizierbaren
Substanzen ist vernünftig; 5. Nebenwirkungen minimieren, Hypoglykämien vermeiden 6. Umfassende Reduktion des Risikos für kardio-vaskuläre
Erkrankungen – ein wesentlicher Fokus der Behandlung 7. HbA1c im Bereich 7 – 8% ist für kardiovaskuläre Patienten
optimal

Danke für Ihre Aufmerksamkeit




























![Diabetestherapie und Niere 2012 [Kompatibilitätsmodus].pdf](https://img.pdfslide.tips/doc/110x75/577cc4021a28aba71197df7f/diabetestherapie-und-niere-2012-kompatibilitaetsmoduspdf.jpg)
