Embed Size (px)
Citation preview

ARTHRITIS & RHEUMATISMVol. 60, No. 11, November 2009, pp 3413–3424DOI 10.1002/art.24876© 2009, American College of Rheumatology
Classification, Presentation, and Initial Treatment ofWegener’s Granulomatosis in Childhood
David A. Cabral,1 America G. Uribe,1 Susanne Benseler,2 Kathleen M. O’Neil,3
Philip J. Hashkes,4 Gloria Higgins,5 Andrew S. Zeft,6 Daniel J. Lovell,7 Daniel J. Kingsbury,8
Anne Stevens,9 Deborah McCurdy,10 Peter Chira,11 Leslie Abramson,12
Thaschawee Arkachaisri,13 Sarah Campillo,14 Anne Eberhard,15 Aimee O. Hersh,16
Adam M. Huber,17 Susan Kim,18 Marisa Klein-Gitelman,19 Deborah M. Levy,20
Suzanne C. Li,21 Thomas Mason,22 Esi Morgan DeWitt,23 Eyal Muscal,24 Lorien Nassi,25
Andreas Reiff,26 Kenneth Schikler,27 Nora G. Singer,28 Dawn Wahezi,29 and Amy Woodward,30
for the ARChiVe (A Registry for Childhood Vasculitis: e-entry) Investigators Network
Objective. To compare the criteria for Wegener’sgranulomatosis (WG) of the American College of Rheu-
matology (ACR) with those of the European LeagueAgainst Rheumatism/Pediatric Rheumatology Euro-pean Society (EULAR/PRES) in a cohort of childrenwith WG and other antineutrophil cytoplasmic antibody(ANCA)–associated vasculitides (AAVs), and to de-scribe the interval to diagnosis, presenting features, andinitial treatment for WG.
Methods. Eligible patients had been diagnosed bysite rheumatologists (termed the “MD diagnosis”) since2004. This diagnosis was used as a reference standardfor sensitivity and specificity testing of the 2 WGclassification criteria. Descriptive analyses were con-fined to ACR-classified WG patients.
Results. MD diagnoses of 117 patients (82 ofwhom were female) were WG (n � 76), microscopicpolyangiitis (n � 17), ANCA-positive pauci-immuneglomerulonephritis (n � 5), Churg-Strauss syndrome(n � 2), and unclassified vasculitis (n � 17). Thesensitivities of the ACR and EULAR/PRES classifica-tion criteria for WG among the spectrum of AAVs were
The initial feasibility study was supported by the VasculitisFoundation (formerly known as the Wegener’s Granulomatosis Asso-ciation), and early registry implementation was supported by a BritishColumbia Children’s Hospital Foundation Telethon Grant.
1David A. Cabral, MBBS, America G. Uribe, MD: BritishColumbia Children’s Hospital, Vancouver, British Columbia, Canada;2Susanne Benseler, MD: Hospital for Sick Children, Toronto, Ontario,Canada; 3Kathleen M. O’Neil, MD: University of Oklahoma HealthSciences Center, Oklahoma City; 4Philip J. Hashkes, MD, MSc:Cleveland Clinic Foundation, Cleveland, Ohio; 5Gloria Higgins, MD:Nationwide Children’s Hospital, Columbus, Ohio; 6Andrew S. Zeft,MD: University of Utah Primary Children’s Medical Center, Salt LakeCity; 7Daniel J. Lovell, MD, MPH: Cincinnati Children’s HospitalMedical Center, Cincinnati, Ohio; 8Daniel J. Kingsbury, MD: LegacyEmanuel Children’s Hospital, Portland, Oregon; 9Anne Stevens, MD:Seattle Children’s Hospital, Seattle, Washington; 10Deborah Mc-Curdy, MD: University of California, Los Angeles; 11Peter Chira, MD,MS: Lucile Packard Children’s Hospital, Stanford University School ofMedicine, Stanford, California; 12Leslie Abramson, MD: University ofVermont, Burlington; 13Thaschawee Arkachaisri, MD: Children’sHospital of Pittsburgh, Pittsburgh, Pennsylvania; 14Sarah Campillo,MD: The Montreal Children’s Hospital, McGill University HealthCentre, Montreal, Quebec, Canada; 15Anne Eberhard, MD: SchneiderChildren’s Hospital, New York, New York; 16Aimee O. Hersh, MD:University of California, San Francisco; 17Adam M. Huber, MD, MSc:IWK Health Centre, and Dalhousie University, Halifax, Nova Scotia,Canada; 18Susan Kim, MD: Children’s Hospital of Boston, Boston,Massachusetts; 19Marisa Klein-Gitelman, MD: Children’s MemorialHospital, Chicago, Illinois; 20Deborah M. Levy, MD, MS: New York–Presbyterian Morgan Stanley Children’s Hospital, New York, NewYork; 21Suzanne C. Li, MD, PhD: Joseph M. Sanzari Children’sHospital, Hackensack University Medical Center, Hackensack, NewJersey; 22Thomas Mason, MD: Mayo Eugenio Litta Children’s Hospi-tal, Mayo Clinic, Rochester, Minnesota; 23Esi Morgan DeWitt, MD,MSCE: Duke Children’s Hospital and Health Center, Duke UniversityMedical Center, Durham, North Carolina; 24Eyal Muscal, MD: TexasChildren’s Hospital, Baylor College of Medicine, Houston; 25Lorien
Nassi, MD: Texas Scottish Rite Hospital, University of Texas South-western, Dallas; 26Andreas Reiff, MD: Childrens Hospital Los Ange-les, Los Angeles, California; 27Kenneth Schikler, MD: University ofLouisville Health Sciences Center, Louisville, Kentucky; 28Nora G.Singer, MD: Case Medical Center, and Rainbow Babies and Children’sHospital University Hospitals, Cleveland, Ohio; 29Dawn Wahezi, MD:Children’s Hospital at Montefiore, Bronx, New York; 30Amy Wood-ward, MD, MPH: Riley Children’s Hospital, Indianapolis, Indiana.
Address correspondence and reprint requests to David A.Cabral, MBBS, Division of Rheumatology, Room K4-121, BritishColumbia Children’s Hospital, Vancouver, BC V6H 3V4, Canada.E-mail: [email protected].
Submitted for publication January 2, 2009; accepted in re-vised form July 11, 2009.
3413

68.4% and 73.6%, respectively, and the specificities were68.3% and 73.2%, respectively. Two more children wereidentified as having WG by the EULAR/PRES criteriathan by the ACR criteria. For the 65 ACR-classified WGpatients, the median age at diagnosis was 14.2 years(range 4–17 years), and the median interval from symp-tom onset to diagnosis was 2.7 months (range 0–49months). The most frequent presenting features byorgan system were constitutional (89.2%), pulmonary(80.0%), ear, nose, and throat (80.0%), and renal(75.4%). Fifty-four patients (83.1%) commenced treat-ment with the combination of corticosteroids and cyclo-phosphamide, with widely varying regimens; the re-mainder received methotrexate alone (n � 1),corticosteroids alone (n � 4), or a combination (n � 6).
Conclusion. The EULAR/PRES criteria mini-mally improved diagnostic sensitivity and specificity forWG among a narrow spectrum of children with AAVs.Diagnostic delays may result from poor characterizationof childhood WG. Initial therapy varied considerablyamong participating centers.
Primary systemic vasculitis (PSV) of childhoodencompasses a group of rare conditions that have incommon primary vascular inflammation, often in criticalorgans such as the heart, kidneys, lungs, and brain (1).They are acutely and chronically life-threatening andhave high associated disease- and treatment-relatedmorbidity. Childhood PSV affects fewer than 25 per100,000 children, with the “acute” subtypes includingHenoch-Schonlein purpura and Kawasaki disease ac-counting for the majority of cases (2). The frequencies ofthe distinct subtypes of “chronic” childhood PSV aredifficult to ascertain. Among the chronic childhoodprimary systemic vasculitides, Wegener’s granulomatosis(WG) is one of the most common, with incidence ratesranging between 0.03 and 3.2 per 100,000 children peryear (1–3). Chronic childhood PSV is the diagnosisassigned to �3% of all patient referrals in some USpediatric rheumatology clinics (4), and individual US/Canadian pediatric rheumatologists will typically see 0–5new patients per year (5). Consequently, most of ourknowledge about the presentation, course, outcome, andoptimal treatment of childhood PSV either comes froma few small case series or has been adapted from studiesof adults, without validation of its true applicability tochildren.
Between one-third and two-thirds of childrenwith chronic PSV are described as having unclassifiedvasculitis (3,4), and one-third of children with WGdiagnosed by expert opinion (6) never fulfill the Amer-
ican College of Rheumatology (ACR) 1990 classificationcriteria (7). It is not known whether these described“difficulties” in assigning a specific classification arerelated to the fact that the ACR 1990 criteria for theclassification of vasculitis (8) and the subsequent ChapelHill Consensus Conference (CHCC) disease definitions(9) were based largely on adult data, or whether theyresult from the fact that children with a developingimmune system have a modified disease expression. Thedifficulties described for adult populations in distin-guishing between the so-called antineutrophil cyto-plasmic antibody (ANCA)–associated vasculitides(AAVs) (10), including WG, microscopic polyangiitis(MPA), and Churg-Strauss syndrome (CSS), have notbeen addressed in the limited pediatric reports of child-hood PSV.
In 2005, under the auspices of the EuropeanLeague Against Rheumatism (EULAR) and the Pediat-ric Rheumatology European Society (PRES), existingACR criteria were modified with a view to improvingtheir applicability in children (11). The resulting pro-posed system of classification and criteria (EULAR/PRES criteria) have yet to be validated in a cohort ofchildren with vasculitis, and specifically, it is not knownwhether the EULAR/PRES criteria for classifying WGin children will “capture” additional children diagnosedas having WG but not fulfilling ACR criteria, childrenwith other diagnostic subsets of AAV, or children withpreviously unclassified chronic PSV.
In the context of establishing a network of pedi-atric investigators interested in advancing our knowl-edge about childhood PSV, we undertook a pilot, mul-ticenter, contemporary inception cohort project calledARChiVe (A Registry for Childhood Vasculitis:e-entry) in collaboration with members of the ChildhoodArthritis and Rheumatology Research Alliance(CARRA). This project initially focused on childrenwith WG together with other AAVs including MPA,CSS, ANCA-positive pauci-immune glomerulonephritis(GN), and unclassified vasculitis. A list of collaboratingcenters and investigators in the ARChiVe network isshown in Appendix A.
The specific aims of this pilot study were tocompare sensitivity and specificity of the adult-derivedACR criteria for WG with those of the proposedEULAR/PRES pediatric-specific criteria among a groupof children with chronic vasculitis whose diagnosis fellwithin the spectrum of diseases related primarily byANCA association and small-to-medium vessel size andwhose clinical characteristics often overlapped. Addi-tionally, we aimed to characterize the time from symp-
3414 CABRAL ET AL

tom onset to diagnosis, the presenting features, and theinitial treatment of the patients in the cohort withACR-defined WG.
PATIENTS AND METHODS
Since the launch of the ARChiVe registry in March2007, pediatric rheumatologists at 30 CARRA-associated geo-graphically diverse institutions in the US (n � 26) and Canada(n � 4) have contributed patients. Eligible patients were allchildren followed up at participating centers who were diag-nosed after January 1, 2004 as having WG, MPA, CSS,ANCA-positive pauci-immune GN, and unclassified vasculitisand who were age �18 years at the time of diagnosis. Thediagnosis, established by the treating pediatric rheumatologistat each of the ARChiVe network sites, was entered in thedatabase and considered to be the “reference standard” anddescribed in this article as the “MD diagnosis.” Using thisdeliberately sensitive entry criterion, we anticipated that asmany as one-third of all patients might be entered as unclas-sifiable (3,4), one-third of the patients diagnosed as havingWG might not be classifiable by ACR criteria (6,7), and somepatients with MPA might also fulfill criteria for WG (12).Specific patient data items for categorical capture included allcriteria required for diagnosis using either the 1990 ACR (7)or EULAR/PRES (11) classification systems (Table 1); pa-tients in the cohort fulfilling criteria for diagnosis of WGaccording to either of these criteria were identifiable bycomputation of data.
For patients diagnosed between January 2004 and thelaunch of ARChiVe in March 2007, data were collected byreview of available medical records. Data were collectedprospectively for patients who were diagnosed between March2007 and November 2008. In both instances data collectedwere for the period from clinical onset and presentation until2 months after diagnosis. The ARChiVe uses a Web-basedinterface for data entry of predominantly categorical variables,which include the following: MD diagnosis; date of symptomonset; demographic data; family and past medical history;presenting/diagnostic features; physical examination findings(including height, weight, blood pressure, and pubertal stag-ing); results or reports of laboratory testing including ANCAtesting (cytoplasmic and/or perinuclear pattern of ANCA[cANCA and/or pANCA, respectively]), histopathology, andother procedures including diagnostic imaging, bronchoscopy,and pulmonary function tests; and initial therapy detailing theuse of oral prednisone doses in mg/kg/day (low [�0.5], medium[0.5–1.5], high [�1.5]) and intravenous (IV) corticosteroids,oral or IV cyclophosphamide, other disease-modifying or“biologic” therapies, and other concurrently used drugs (e.g.,anticoagulants, antihypertensive medications).
Other data set items captured included all items de-scribing disease activity that are used in the BirminghamVasculitis Activity Score (13,14) in addition to common pedi-atric presenting features, unique diagnostic features for classi-fication, or measurements of disease activity that were gener-ated from a survey of CARRA members and incorporated intoa standardized data collection form by a subsequent vasculitisconsensus working group.
All data were reviewed at the main coordinating center
for completeness and quality. Data were reviewed to ensurethat there were no duplicate cases, since some of the institu-tions in the ARChiVe network reported patients who wereeither transferred from other medical institutions or referredto them for a “second opinion.”
The study protocol was approved by the local researchethics board at each participating center. Informed consent forparticipation was obtained from parents, and informed consentor assent was obtained from patients for both retrospective andprospective recruitment as applicable.
Because the data were of a cross-sectional nature,descriptive statistical analyses were performed. In order tomake our data comparable with those of previously reportedcohorts, we described presenting features and treatment ofpatients who fulfilled �2 of the ACR classification criteria; thisdoes not mean to assume that the ACR criteria best definechildhood WG. Frequency and distribution of the sociodemo-graphic, clinical, and treatment characteristics of pediatric WGpatients were provided using medians with ranges and percent-ages where applicable.
To compare the ACR and EULAR/PRES classifica-tion criteria for WG, all patients in the registry with anyphysician-assigned diagnosis (WG, MPA, CSS, ANCA-positivepauci-immune GN, or unclassified vasculitis) were analyzed.To assess the degree of agreement between the MD, ACR, andEULAR/PRES WG diagnoses, exploratory analyses to ascer-tain convergent validity (chance-corrected agreement) wereperformed using the kappa statistic (15). To determine dis-criminant validity of criteria in the absence of a gold standardis difficult; MD diagnosis of patients enrolled by �30 contrib-uting physicians could not be considered a gold standard.However, for these exploratory analyses we used the MD
Table 1. Comparison of the ACR and EULAR/PRES classificationcriteria for WG*
1990 ACR criteriaA patient is said to have WG when 2 of the following 4 criteria
are present:Nasal or oral inflammationAbnormal chest radiographAbnormal urinary sediment (microhematuria [�5 red blood
cells per high-power field] or red blood cell casts inurine sediment)
Granulomatous inflammation on biopsyEULAR/PRES criteria
A patient is said to have WG when 3 of the following 6 criteriaare present:
Nasal or sinus inflammationAbnormal chest radiograph or chest CT scanAbnormal urinalysis (hematuria and/or significant proteinuria)Granulomatous inflammation on biopsy/necrotizing
pauci-immune GNSubglottic, tracheal, or endobronchial stenosisAnti-PR3 ANCA or cANCA staining
* Differences between American College of Rheumatology (ACR)and European League Against Rheumatism/Pediatric RheumatologyEuropean Society (EULAR/PRES) classification systems and forindividual criteria are italicized. WG � Wegener’s granulomatosis;CT � computed tomography; GN � glomerulonephritis; anti-PR3 �anti–proteinase 3; ANCA � antineutrophil cytoplasmic antibody;cANCA � cytoplasmic ANCA.
WEGENER’S GRANULOMATOSIS IN CHILDHOOD 3415

diagnosis, not as a gold standard, but as the reference standardto calculate the ACR and EULAR/PRES classification criteriasensitivity and specificity. All analyses were performed usingthe Statistical package for the Social Sciences, version 16.0(SPSS, Chicago, IL).
RESULTS
During the study period, 117 pediatric patients(82 female [70.1%]) from 30 centers were recruited intothe ARChiVe cohort; 37 (31.6%) were collected pro-spectively. The MD diagnoses of the patients in thecohort were WG (n � 76), MPA (n � 17), ANCA-positive pauci-immune GN (n � 5), and CSS (n � 2).Seventeen patients were not considered classifiable un-der any of these categories (unclassified vasculitis).
Evaluating classification, and comparing exist-ing ACR and proposed EULAR/PRES criteria for WG.Agreement was moderate between the MD diagnosisand either the ACR criteria or the EULAR/PREScriteria (� � 0.346 and � � 0.476, respectively). How-ever, there was substantial agreement between the ACRcriteria and the EULAR/PRES criteria (� � 0.686). Thesensitivities of the ACR criteria and the EULAR/PRESclassification criteria for WG among the spectrum ofpediatric AAVs were 68.4% and 73.6%, respectively,and the specificities were 68.3% and 73.2%, respectively(Table 2).
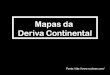
Figure 1 is a Venn diagram showing the numberof patients in the cohort who were diagnosed as havingWG by MD diagnosis (n � 76), by the ACR classifica-tion criteria (n � 65), or by the EULAR/PRES classifi-cation criteria (n � 67). Twenty-six patients were notconsidered to have WG by MD diagnosis, ACR criteria,or EULAR/PRES criteria.
Among the 65 patients with WG according to theACR criteria, the MD diagnosis differed in 13 (10 hadMPA and 3 had unclassified vasculitis). Among the 52patients who did not meet the ACR criteria for WG, 17had an MD diagnosis of WG, 2 were classified as having
WG by EULAR/PRES criteria, and 7 were classified ashaving WG by both the MD diagnosis and the EULAR/PRES criteria. The EULAR/PRES criteria that enabledWG classification in these 9 patients were sinus involve-ment and/or ANCA-positive serologic findings and/orsignificant proteinuria, and, less frequently, subglottic/tracheal/endobronchial stenosis and/or kidney biopsyshowing necrotizing pauci-immune GN (Table 3).
Among the 67 patients with WG according to theEULAR/PRES criteria, the MD diagnosis differed in 11(7 had MPA, 3 had unclassified vasculitis, and 1 hadANCA-positive pauci-immune GN). Among the 50 pa-tients who did not meet the EULAR/PRES criteria forWG, 17 had an MD diagnosis of WG, 4 had WG byACR criteria, and 3 had WG by both MD diagnosis andACR criteria. The 7 patients who met ACR criteriafulfilled only 2 of the 4 criteria that were also criteria ofthe EULAR/PRES classification system (Table 3).
Figure 1. Venn diagram of assigned Wegener’s granulomatosis (WG)diagnosis among the 117 patients in the ARChiVe (A Registry forChildhood Vasculitis: e-entry) cohort. The diagnosis of WG wasestablished by the treating pediatric rheumatologist at each of theARChiVe network sites (the MD diagnosis), by the American Collegeof Rheumatology (ACR) classification criteria, and by the EuropeanLeague Against Rheumatism/Pediatric Rheumatology European So-ciety (EULAR/PRES) classification criteria.
Table 2. Discriminant validity of the ACR and EULAR/PRES clas-sification criteria for WG*
ACRcriteria
EULAR/PRESScriteria
Sensitivity 68.4 73.6Specificity 68.3 73.2PPV 80.0 83.6NPV 53.8 60.0Overall accuracy 68.4 73.5
* Values are the percent. PPV � positive predictive value; NPV �negative predictive value (see Table 1 for other definitions).
3416 CABRAL ET AL

Tab
le3.
Dat
aon
the
16pa
tient
sfr
omth
eA
RC
hiV
est
udy
coho
rtw
hoco
uld
fulfi
lla
suff
icie
ntnu
mbe
rof
eith
erE
UL
AR
/PR
ES
clas
sific
atio
ncr
iteri
aor
AC
Rcl
assi
ficat
ion
crite
ria
(but
not
both
)fo
rdi
agno
sis
ofW
G*
Nas
alin
flam
mat
ion†
Sinu
sin
flam
mat
ion‡
Abn
orm
alch
est
radi
ogra
ph†
Abn
orm
alch
est
CT
scan
‡
Abn
orm
alur
inal
ysis
(hem
atur
ia)†
Abn
orm
alur
inal
ysis
(sig
nific
ant
prot
einu
ria)
‡
Gra
nulo
mat
ous
infla
mm
atio
non
biop
sy†
Nec
rotiz
ing
pauc
i-im
mun
eG
Non
biop
sy‡
Subg
lott
ic,
trac
heal
,or
endo
bron
chia
lst
enos
is‡
Ant
i-PR
3A
NC
Aor
cAN
CA
stai
ning
‡
Patie
nts
fulfi
lling
3of
6E
UL
AR
/PR
ES
crite
ria
for
WG
,by
age
inye
ars
(n�
9)3
XX
XX
4X
XX
X6
XX
XX
X7
XX
X10
XX
XX
12X
XX
X14
XX
XX
14X
XX
14X
XX
Patie
nts
fulfi
lling
2of
4A
CR
crite
ria
for
WG
,by
age
inye
ars
(n�
7)2
XX
X3
XX
X3
XX
X4
XX
X6
XX
X6
XX
XX
15X
XX
*T
hepr
esen
ceof
anin
divi
dual
com
pone
ntof
the
crite
ria
inea
chpa
tient
isin
dica
ted
byan
X.C
ompl
ete
desc
ript
ions
ofth
eE
UL
AR
/PR
ES
and
AC
Rcr
iteri
aar
esh
own
inT
able
1.A
RC
hiV
e�
AR
egis
try
for
Chi
ldho
odV
ascu
litis
:e-e
ntry
(see
Tab
le1
for
othe
rde
finiti
ons)
.†
Cri
teri
onsh
ared
bybo
thE
UL
AR
/PR
ES
and
AC
R.
‡E
UL
AR
/PR
ES
crite
rion
that
isei
ther
am
odifi
catio
nof
anA
CR
crite
rion
ora
new
crite
rion
.
WEGENER’S GRANULOMATOSIS IN CHILDHOOD 3417

WG cohort. Sixty-five of the 117 patients met theACR criteria for WG; 63.1% of these patients werefemale. The majority of patients were Caucasian(69.2%), 4 were of mixed ethnicity, 3 were of East Indiandescent, 3 were African American, 2 were Hispanic, 1
was Asian, and 1 was of Middle Eastern origin; ethnicitydata were not available for 6 patients. The median age atWG diagnosis was 14.2 years (range 4–17 years). Themedian interval from symptom onset to diagnosis was2.7 months (range 0–49 months). Eight of these 65 WG
Table 4. Frequency of presenting clinical features in pediatric patients with WG in 3 different single-center cohorts and in our multicenterARChiVe cohort*
Clinical featureNIH
(n � 23)†GOSH
(n � 17)‡HSC
(n � 25)§ARChiVe(n � 65)¶
Constitutional/general NR NR 24 (96.0) 58 (89.2)Malaise, fatigue NR NR NR 58 (89.2)Fever 5 (22.0) NR 18 (72.0) 35 (53.8)Weight loss 3 (13.0) 5 (29.0) 14 (56.0) 28 (43.1)
Pulmonary 5 (22.0) 14 (82.4) 20 (80.0) 52 (80.0)Shortness of breath NR NR NR 38 (58.5)Chronic cough NR 9 (53.0) NR 34 (52.3)Hemoptysis/alveolar hemorrhage 2 (9.0) 3 (18.0) 11 (44.0) 29 (44.6)Nodules 3 (13.0) 3 (17.6) 11 (44.0) 26 (41.9)#Abnormal pulmonary function test results NR 3 (17.6) NR 27 (42.5)**Fixed pulmonary infiltrates 2 (9.0) 1 (5.9) 4 (16.0) 14 (22.6)#Oxygen dependency NR NR NR 12 (18.5)Pleurisy 1 (4.0) NR 2 (8.0) 15 (23.1)
Renal NR 4 (23.5) 22 (88.0) 49 (75.4)Abnormal urinalysis results NR 4 (23.5) 22 (88.0) 49 (75.4)Biopsy-proven GN 2 (9.0) NR 16 (64.0) 34 (52.3)Elevated serum creatinine NR NR 7 (28.0) 27 (41.5)
Ear, nose, and throat 20 (87.0) 17 (100.0) 21 (84.0) 52 (80.0)Nasal involvement 11 (48.0) 7 (41.0) 10 (40.0)†† 42 (64.6)Sinusitis 14 (61.0) 6 (35.0) 11 (44.0) 39 (60.0)Otitis/mastoiditis 9 (39.0) NR 6 (24.0) 9 (13.8)Subglottic involvement 1 (4.0) 7 (41.0) 1 (4.0) 9 (13.8)Hearing loss 6 (26.0) NR 4 (16.0) 7 (10.8)Oral ulcers 1 (4.0) 5 (29.0) 7 (28.0) 6 (9.2)
Eyes 3 (13.0) 9 (53.0) 13 (52.0) 24 (36.9)Nonspecific red eye NR NR NR 10 (15.4)Conjunctivitis 0 (0.0) 5 (29.0) 11 (44.0) 6 (9.2)Scleritis 1 (4.0) 3 (18.0) 3 (12.0) 3 (4.6)
Cutaneous NR 9 (53.0) 8 (32.0) 23 (35.4)Palpable purpura/petechiae NR NR 8 (32.0) 15 (23.1)
Gastrointestinal NR NR 3 (12.0) 27 (41.5)Nonspecific abdominal pain NR 5 (29.0) NR 21 (32.3)Chronic nausea NR NR NR 11 (16.9)
Musculoskeletal NR NR NR 37 (56.9)Arthralgia/myalgia 7 (30.0)‡‡ 9 (53.0) 16 (64.0) 35 (53.8)Arthritis NR NR 8 (32.0) 13 (20.0)
Nervous system NR 2 (12.0) 2 (8.0) 16 (24.6)Severe headache NR NR NR 9 (13.8)Dizziness NR NR NR 8 (12.3)
Cardiovascular NR NR NR 0 (0.0)Venous thrombosis NR NR 3 (12.0) 0 (0.0)
* Values are the number (%) of affected patients. NR � frequency not reported (see Table 1 for other definitions).† National Institutes of Health (NIH) study, Bethesda, MD (Rottem et al, 1993 [16]). Absolute patient numbers were calculated from percentagesprovided in the article.‡ Great Ormond Street Hospital (GOSH) for Children, London, UK (Belostotsky et al, 2002 [6]). Some clinical features in this cohort correspondto the entire disease course since features at disease onset were not reported consistently.§ Hospital for Sick Children (HSC), Toronto, Ontario, Canada (Akikusa et al, 2007 [17]).¶ A Registry for Childhood Vasculitis: e-entry (ARChiVe), 2008 (present study). Patients met �2 of the ACR classification criteria for WG.# From 62 children who underwent chest imaging.** From 35 children who had pulmonary function tests done.†† Nasal involvement features were reported separately, with epistaxis occurring in 40% and nasal ulcers in 24% of children at disease onset.‡‡ Arthralgias and arthritis at disease onset were not reported separately.
3418 CABRAL ET AL

patients (12.3%) had a symptom onset to diagnosisinterval �12 months; patients with this longer interval todiagnosis had a higher frequency of ear, nose, and throatand cutaneous manifestations and less frequently hadrenal features (data not shown).
Frequencies of presenting features by organ sys-tem were as follows: constitutional/general (89.2%),pulmonary (80.0%), ear, nose, and throat (80.0%), andrenal (75.4%). Additional categories and specific fea-tures are listed in Table 4. Significant renal involvementas manifested by serum creatinine elevated above the95th percentile for age was found in 27 patients (41.5%);dialysis was necessary in 7 patients (10.8%), and end-stage renal disease was present in 1 patient. Of note,among those patients with pulmonary disease, severeinvolvement requiring continuous oxygen therapy ormechanical ventilation occurred in 19% and 11%, re-
spectively. Of the 35 patients who had pulmonary func-tion tests done, 27 had abnormal results; obstructive andrestrictive abnormalities were found to be equally rep-resented.
The numbers and frequencies of patients pre-senting with any of the criteria used in either the ACR orthe EULAR/PRES classification were as follows: nasalbleed/ulcers/crusts, 64.6%; sinusitis, 60.0%; subglottic,tracheal, or endobronchial stenosis, 16.9%; oral ulcers,9.2%; abnormal findings on chest imaging (multiplenodules, fixed infiltrates, and/or cavitation), 64.5% of 62patients who underwent chest imaging; abnormal urin-alysis results (�5 red blood cells [RBCs] per high-powerfield, RBC casts, or proteinuria), 70.8%; histologic evi-dence of necrotizing pauci-immune GN, 12.3%; andhistologic evidence of granulomatous vasculitis at non-renal sites, 24.6%. Serology tests for the presence of
Table 5. Autoantibody testing results among children with and those without WG according to the ACRcriteria*
Serologic testWith WG(n � 65)
Without WG(n � 52)
Immunofluorescence for cANCA, positive 43 (66.2) 12 (23.1)Anti-PR3–positive on ELISA 40 (93.0) 11 (91.7)Anti-MPO–positive on ELISA 0 (0.0) 0 (0.0)Negative on ELISA 2 (4.7) 1 (8.3)ELISA not done 0 (0.0) 0 (0.0)ELISA result not available 1 (2.3) 0 (0.0)
Immunofluorescence for pANCA, positive 14 (21.5) 20 (38.5)Anti-PR3–positive on ELISA 3 (21.4) 1 (5.0)Anti-MPO–positive on ELISA 8 (57.1) 18 (90.0)Negative on ELISA 2 (14.3) 0 (0.0)ELISA not done 1 (7.1) 1 (5.0)
Immunofluorescence for pANCA and cANCA, positive 1 (1.5) 1 (2.0)Anti-MPO–positive on ELISA 0 (0.0) 1 (100.0)ELISA not done 1 (100.0) 0 (0.0)
Immunofluorescence not done 3 (4.6) 1 (2.0)Anti-PR3– and anti-MPO–positive on ELISA 1 (33.3) 0 (0.0)Anti-PR3–positive on ELISA 1 (33.3) 0 (0.0)ELISA not done 0 (0.0) 1 (100.0)ELISA result not available 1 (33.3) 0 (0.0)
Negative for ANCA (cANCA and pANCA) 4 (6.2) 17 (32.7)Anti-PR3–positive on ELISA 0 (0.0) 3 (17.6)Anti-MPO–positive on ELISA 0 (0.0) 1 (5.9)Negative on ELISA 4 (100.0) 12 (70.6)ELISA not done 0 (0.0) 1 (5.9)
Antinuclear antibodies, tested 50 (76.9) 44 (84.6)Positive 17 (34.0) 16 (36.4)Negative 33 (66.0) 28 (63.6)
Anticardiolipin antibodies and/or lupus anticoagulant, tested 34 (52.3) 19 (36.5)Positive 6 (17.6) 5 (26.3)Negative 28 (82.4) 14 (73.7)
Anti–glomerular basement membrane antibodies, tested 9 (13.8) 3 (5.8)Positive† 2 (22.2) 0 (0.0)Negative 7 (77.8) 3 (100.0)
* Values are the number (%) of patients. ELISA � enzyme-linked immunosorbent assay; anti-MPO �antimyeloperoxidase; pANCA � perinuclear ANCA (see Table 1 for other definitions).† Transiently positive for both patients.
WEGENER’S GRANULOMATOSIS IN CHILDHOOD 3419

ANCAs by immunofluorescence yielded positive resultsin 58 children with WG (89.2%) (43 with cANCA[66.2%], 14 with pANCA [21.5%], and 1 with bothcANCA and pANCA [1.5%]); 4 patients were negativefor both cANCA and pANCA, and serology tests werenot performed for 3 patients. Using enzyme-linkedimmunosorbent assay, anti–proteinase 3 (anti-PR3) pos-itivity was reported in 44 patients (67.7%), antimy-eloperoxidase (anti-MPO) positivity was reported in 8patients (12.3%), and 1 patient was found to be bothanti-PR3 and anti-MPO positive. Results of ANCAtesting and other autoantibody tests are summarized inTable 5.
Histopathology. Fifty-four patients had �1 bi-opsy performed (36 renal biopsies and 38 nonrenalbiopsies). Nonrenal histopathology showing granuloma-tous vasculitis included the following: lower airways/lungs (6 of 13 biopsy samples), paranasal sinuses (4 of 8biopsy samples), upper airways (3 of 6 biopsy samples),skin (2 of 6 biopsy samples), and nasal septum (1 of 3biopsy samples). No granulomatous vasculitis was foundin 2 reported biopsy samples of the gastrointestinal tract.In all but 2 kidney biopsy samples, the histopathologyshowed GN, with 22.2% being described as necrotizingpauci-immune GN.
Treatment. Fifty-four patients (83.1%) weretreated with a combination of corticosteroids and cyclo-phosphamide; 27 of these received oral cyclo-phosphamide, 21 received IV cyclophosphamide, and 6initially received IV cyclophosphamide and wereswitched to oral cyclophosphamide early in the diseasecourse. Forty-five patients (69.2%) received high-doseIV pulse corticosteroids. Among 60 patients (92.3%)receiving oral corticosteroids, 2 were receiving a low-dose regimen, 31 were receiving a medium dose, and 27were receiving a high dose. Four children were treatedwith corticosteroids only (2 received medium-dose cor-ticosteroids and 2 received high-dose corticosteroids).Six patients (9.2%) received a combination of cortico-steroids and methotrexate, and 1 patient (1.5%) wastreated with methotrexate only. Thirty-four patients(52.3%) were started on trimethoprim/sulfamethoxazole(TMP/SMX), generally as Pneumocystis jiroveci pneumo-nia prophylaxis. Other therapeutic modalities used in-cluded plasmapheresis (9 patients), extracorporealmembrane oxygenation (2 patients), IV immunoglobulin(IVIG) (2 patients), and rituximab (1 patient).
DISCUSSION
This report of 65 patients with pediatric-onsetWG (ACR defined) from 30 US and Canadian centers
describes the largest cohort of such children to date. The3 largest series previously reported from the US (n � 23)(16), the UK (n � 17) (6), and Canada (n � 25) (17)were single-center series that collected patients over 24,17, and 21 years, respectively. Unlike the others, thiscurrent report does not describe any followup data.However, through the concurrent establishment of anetwork of interested investigators supported by a Web-based data entry interface system (ARChiVe), we haveidentified a relatively contemporary cohort of patients(diagnosed since 2004) for future prospective study.Because of the rarity of WG in children, it is not feasiblefor any single center to establish a similarly sized cohort(5). Furthermore, the nature of this multicenter networkreduces the likelihood that patients are selected forgreater disease severity, a potential bias that might beattributed to cohorts from single large referral centers.
In classifying WG, the limited convergence ofMD diagnosis with either ACR criteria or EULAR/PRES criteria is not surprising, since the premise fordiagnosis of patients as having any disease differs fromthat for classification. Because the EULAR/PRES crite-ria were built upon the existing ACR criteria, there wasa reasonable convergence between them, and as such,the sensitivity and specificity were likely to be similar.Among the 76 patients referred to ARChiVe with thephysician diagnosis of WG, 52 could be classified ashaving WG according to ACR criteria; in an additional13 children with ACR-defined WG, the MD diagnosisdiffered. Use of the proposed pediatric EULAR/PREScriteria minimally improved diagnostic sensitivity andspecificity over those of the ACR criteria; although theEULAR/PRES classification scheme identified 9 pa-tients with WG in addition to those identified by theACR criteria, 7 of the patients identified as having WGaccording to the ACR criteria could not meet �2 criteriarequired for EULAR/PRES classification (Table 3).Interestingly, by applying the modification proposed bythe WG etanercept trial investigators (18) of adding apositive enzyme immunoassay finding for anti-PR3 as afifth criterion, sensitivity of the ACR criteria increasedsubstantially (to 86.8%) without a significant change inspecificity.
The low sensitivity and specificity of both sets ofcriteria likely reflect the denominator. In our analyses,sensitivity and specificity for classification of WG weretested among a group of patients with vasculitidesrelated by size of the vessel predominantly involved(small to medium) and the association with ANCAs.Patients in any diagnostic subset of AAV in this cohortwere more likely to have WG than a vasculitis diagnosis
3420 CABRAL ET AL

other than AAV. Thus, we would anticipate that thesensitivity and specificity would improve significantly ifthe criteria were tested among a population of pediatricpatients that included the wider spectrum of vasculitidesof differing predominant vessel sizes, from Henoch-Schonlein purpura (small vessel) through polyarteritisnodosa (PAN) (medium vessel) to Takayasu arteritis(large vessel).
Among the patient population that we studied,the most difficult differential diagnosis was the distin-guishing of WG from MPA. Neither the ACR nor theEULAR/PRES have defined categorical classificationcriteria for MPA. Using the CHCC characterization ofMPA (9), 36 of 117 patients in our cohort could bedefined as having MPA, and among these patients, 24could concurrently be diagnosed as having WG accord-ing to ACR criteria. Since WG and MPA share manyfeatures, there are clearly difficulties in defining mutu-ally exclusive classification criteria for these 2 disorders.Some authorities believe that these 2 entities should beconsidered together under the rubric of AAV (10). Thealgorithm by Watts et al (12) was developed to catego-rize adult patients among those with AAV or PAN intoa single nonoverlapping classification; those investiga-tors criticize the poor individual performance of ACRcriteria, CHCC definitions, and Lanham criteria (19)with respect to defining mutually exclusive classificationcategories. This algorithm applies the different criteriain a stepwise approach, first defining WG patients wherecriteria are most specific, and subsequently and sequen-tially applying elements of different criteria to theremaining patients to classify each into a single category.The EULAR/PRES criteria, a “pediatric” modificationof the ACR criteria, did not address this criticism.
Basic demographics, clinical features, and treat-ment modalities for ACR-defined WG patients in theARChiVe cohort were comparable with those reportedelsewhere in that the patients were predominantly fe-male and Caucasian and the age at onset was mostly inthe adolescent years. Our patients’ median interval fromsymptom onset to diagnosis (2.7 months) was similar tothose reported by Akikusa et al and Rottem et al (2months and 8 months, respectively) (16,17) in spite ofthe great diversity of geographic and economic back-grounds of our population and differences in health carepolicy between Canada and the US. The upper end ofthe range (49 months) remains disconcerting; the 8ARChiVe patients (12.3%) with an interval to diagnosisof �12 months presented predominantly with ear, nose,and throat and cutaneous features and had fewer renalmanifestations than those patients who were diagnosed
within 12 months of symptom onset. The implication ofthis disparity is that diagnosis is delayed in the absenceof initial critical organ involvement.
The frequencies of specific presenting clinicalfeatures of our cohort and those of the 3 previous largestcohorts are compared in Table 4. We corroborated thehigh incidence of renal involvement at disease onsetdescribed by Akikusa et al and by investigators in somesmaller series (17,20,21) relative to the adult experience(22,23), whereas there was a somewhat lower incidencein the other 2 large series. Pulmonary involvement wasas common as renal disease among ARChiVe patients,with severe pulmonary involvement (oxygen dependencyand/or requirement for mechanical ventilation) occur-ring in 15 patients (23.1%). Findings on imaging studies(pulmonary nodules and infiltrates) in our populationwere comparable with those reported in other pediatricWG series, with a lower proportion of abnormal imagingfindings in patients without pulmonary symptoms in ourcohort (data not shown) compared with that reported byRottem et al (17% versus 41%) (16).
The frequency of ear, nose, and throat featuresamong ARChiVe patients was similar to that reported inother pediatric WG series. Subglottic stenosis is noted insome reports to occur frequently in pediatric-onset WGcompared with WG in adults, such that this feature wasincluded in the EULAR/PRES criteria (derived byexpert consensus) for classifying WG (11). In our cohort,after nasal and sinus involvement, subglottic stenosis wasonly slightly more frequent than otitis/mastoiditis orhearing loss. Nonetheless, it still may be valuable as acriterion because it may be more specific for WG, havinga narrower differential diagnosis than other upper respi-ratory symptoms. Inclusion of subglottic stenosis as acriterion may enable classification of patients throughEULAR/PRES who would not otherwise be describedas having WG; one such patient was diagnosed in thiscohort.
We found a lower frequency of ocular manifes-tations (conjunctivitis and scleritis in particular) thanpreviously reported. In contrast, the frequency of gas-trointestinal and neurologic symptoms was greater inour patients compared with their frequency in reportedseries.
The high frequency of thrombotic events de-scribed in 2 previous reports (17,24) was not found inour series. Additionally, half of our patients were testedfor antiphospholipid antibodies and lupus anticoagulant,with only 18% of those tested having a positive result atthe time of diagnosis (the reasons for antibody testingwere not documented in the registry). This proportion is
WEGENER’S GRANULOMATOSIS IN CHILDHOOD 3421

similar to that reported in adult patients (25). Throm-botic events may potentially occur in our patient cohortlater in the disease course, although in the existingreports, thrombotic events occurred within a few weeksof diagnosis, and such patients in our cohort wouldarguably have been identified within our data capturetime frame.
In treating pediatric WG, the standard practice ofinitial treatment for 83% of ARChiVe patients wascyclophosphamide and corticosteroids, although therewas diversity and several permutations of regimens androutes of administration. Early use of cyclophosphamidewas similar to that reported by Rottem et al andBelostotsky et al (82.6% and 94%, respectively) (6,16).Methotrexate was not frequently used in the early 1980s;however, in the ARChiVe cohort it was used in 10.7% ofpatients, a rate similar to that described in the Torontocohort. Use of TMP/SMX in ARChiVe patients washigher than that reported by Belostotsky et al (6) (51%versus 29%); however, except for 1 patient, it wasprescribed as P jiroveci pneumonia prophylaxis. Othertherapies such as plasmapheresis, extracorporeal mem-brane oxygenation, IVIG, and rituximab were rarelyused. No patients began therapy using azathioprine,mycophenolate mofetil, or biologic medications otherthan rituximab at the time of diagnosis. We recognizethat there are recent reports of rituximab use as initialtherapy in newly diagnosed adult and pediatric WGpatients (26,27), but at the time of this report thosepediatric patients had not been entered into the registry.
Some considerations must be applied to theinterpretation of our findings, particularly with respectto previous WG series. First, our data were collectedcross-sectionally and predominantly in a retrospectiveway. However, data collection was done using a stan-dardized Web-based data entry system that was regu-larly reviewed centrally for data consistency and qualityto minimize incomplete information. Furthermore, theretrospective time frame was the shortest (5 years) andmost contemporary. Patient recruitment to the ongoingARChiVe registry cohort will be predominantly pro-spective, thereby improving the quality and complete-ness of data capture. Also, having data collected in manyinstitutions will provide us with a broader overview ofthe different clinical approaches to pediatric vasculitis inpractice across the US and Canada. Second, becauseARChiVe data collection currently consists of a one-time data entry point at the time of diagnosis, we are notable to provide information on patient outcomes. Futurelongitudinal data collection from this patient cohort isplanned.
In this cohort, the largest collection of pediatricpatients with WG to date, some patients were found tohave a considerable delay from symptom onset to timeof diagnosis, particularly when there was initially non-critical organ disease. Lack of appreciation of the femalepreponderance in childhood disease and differences inpresentation from adult patients may contribute to thediagnostic delay. The diversity of initial treatments usedfor patients in this cohort suggests that there may be nostandard approach to therapy. This difference may pre-dominate among patients with noncritical organ disease.Further analysis of treatment regimen stratified by dis-ease severity at onset and subsequent outcome will benecessary to determine optimal outcomes while mini-mizing treatment toxicities. Estimations of disease sever-ity by adapting severity classification systems used inadults will be integrated into future outcome studies ofthis cohort. We did not find that the newly proposedpediatric EULAR/PRES vasculitis classification criteriapresented significant improvement over the ACR crite-ria for classifying WG; however, a second iteration of thecriteria is being refined and will be testable in ourgrowing cohort.
ACKNOWLEDGMENTS
We are indebted to all participating patients and theirfamilies, without whom this study would not be possible. Theorigins of this project were in the CARRA; although theARChiVe network now extends beyond this, we gratefullyacknowledge that it would not be sustainable without theendorsement and ongoing support of the CARRA and itsmembership.
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising itcritically for important intellectual content, and all authors approvedthe final version to be published. Dr. Cabral had full access to all of thedata in the study and takes responsibility for the integrity of the dataand the accuracy of the data analysis.Study conception and design. Cabral, Uribe, Benseler, O’Neil, Hash-kes, Zeft, Lovell, Kingsbury, Stevens, Chira, Abramson, Arkachaisri,Eberhard, Hersh, Levy, Li, Morgan DeWitt, Reiff, Schikler, Singer.Acquisition of data. Cabral, Uribe, Benseler, O’Neil, Hashkes, Hig-gins, Lovell, Kingsbury, Stevens, McCurdy, Chira, Abramson,Arkachaisri, Campillo, Eberhard, Hersh, Huber, Kim, Klein-Gitelman,Li, Mason, Morgan DeWitt, Muscal, Nassi, Schikler, Singer, Wahezi,Woodward.Analysis and interpretation of data. Cabral, Uribe, Huber, Muscal,Schikler.Study administration and coordination. Cabral.
REFERENCES
1. Lindsley CB, Laxer RM. Granulomatous vasculitis, giant cellarteritis and sarcoidosis. In: Cassidy JT, Petty RE, Laxer RM,
3422 CABRAL ET AL

Lindsley CB, editors. Textbook of pediatric rheumatology. Phila-delphia: Elsevier Saunders; 2005. p. 539–60.
2. Gardner-Medwin JM, Dolezalova P, Cummins C, Southwood TR.Incidence of Henoch-Schonlein purpura, Kawasaki disease, andrare vasculitides in children of different ethnic origins. Lancet2002;360:1197–202.
3. Malleson PN, Fung MY, Rosenberg AM. The incidence of pedi-atric rheumatic diseases: results from the Canadian PediatricRheumatology Association Disease Registry. J Rheumatol 1996;23:1981–7.
4. Bowyer S, Roettcher P, the Pediatric Rheumatology DatabaseResearch Group. Pediatric rheumatology clinic populations in theUnited States: results of a 3 year survey. J Rheumatol 1996;23:1968–74.
5. Wilkinson NM, Page J, Uribe AG, Espinosa V, Cabral DA.Establishment of a pilot pediatric registry for chronic vasculitis isboth essential and feasible: a Childhood Arthritis and Rheuma-tology Alliance (CARRA) survey. J Rheumatol 2007;34:224–6.
6. Belostotsky VM, Shah V, Dillon MJ. Clinical features in 17paediatric patients with Wegener granulomatosis. Pediatr Nephrol2002;17:754–61.
7. Leavitt RY, Fauci AS, Bloch DA, Michel BA, Hunder GG, ArendWP, et al. The American College of Rheumatology 1990 criteriafor the classification of Wegener’s granulomatosis. ArthritisRheum 1990;33:1101–7.
8. Fries JF, Hunder GG, Bloch DA, Michel BA, Arend WP, Cala-brese LH, et al. The American College of Rheumatology 1990criteria for the classification of vasculitis: summary. ArthritisRheum 1990;33:1135–6.
9. Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL,et al. Nomenclature of systemic vasculitides: proposal of aninternational consensus conference. Arthritis Rheum 1994;37:187–92.
10. Hellmich B, Flossmann O, Gross WL, Bacon P, Cohen-TervaertJW, Guillevin L, et al. EULAR recommendations for conductingclinical studies and/or clinical trials in systemic vasculitis: focus onanti-neutrophil cytoplasm antibody-associated vasculitis. AnnRheum Dis 2007;66:605–17.
11. Ozen S, Ruperto N, Dillon MJ, Bagga A, Barron K, Davin JC, etal. EULAR/PReS endorsed consensus criteria for the classifica-tion of childhood vasculitides. Ann Rheum Dis 2006;65:936–41.
12. Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, KoldingsnesW, et al. Development and validation of a consensus methodologyfor the classification of the ANCA-associated vasculitides andpolyarteritis nodosa for epidemiological studies. Ann Rheum Dis2007;66:222–7.
13. Luqmani RA, Bacon PA, Moots RJ, Janssen BA, Pall A, Emery P,et al. Birmingham Vasculitis Activity Score (BVAS) in systemicnecrotizing vasculitis. QJM 1994;87:671–8.
14. Flossmann O, Bacon P, de Groot K, Jayne D, Rasmussen N, SeoP, et al. Development of comprehensive disease assessment insystemic vasculitis. Ann Rheum Dis 2007;66:283–92.
15. Kramer MS, Feinstein AR. Clinical biostatistics. LIV. The biosta-tistics of concordance. Clin Pharmacol Ther 1981;29:111–23.
16. Rottem M, Fauci AS, Hallahan CW, Kerr GS, Lebovics R, LeavittRY, et al. Wegener granulomatosis in children and adolescents:clinical presentation and outcome. J Pediatr 1993;122:26–31.
17. Akikusa JD, Schneider R, Harvey EA, Hebert D, Thorner PS,Laxer RM, et al. Clinical features and outcome of pediatricWegener’s granulomatosis. Arthritis Rheum 2007;57:837–44.
18. Haas JP, Metzler M, Ruder H, Waldherr R, Boswald M, Ruppre-cht T. An unusual manifestation of Wegener’s granulomatosis in a4-year-old girl. Pediatr Neurol 2002;27:71–4.
19. Lanham JG, Elkon KB, Pusey CD, Hughes GR. Systemic vasculitiswith asthma and eosinophilia: a clinical approach to the Churg-Strauss syndrome. Medicine (Baltimore) 1984;63:65–81.
20. Stegmayr BG, Gothefors L, Malmer B, Muller Wiefel DE, Nilsson
K, Sundelin B. Wegener granulomatosis in children and youngadults: a case study of ten patients. Pediatr Nephrol 2000;14:208–13.
21. Hall SL, Miller LC, Duggan E, Mauer SM, Beatty EC, HellersteinS. Wegener granulomatosis in pediatric patients. J Pediatr 1985;106:739–44.
22. Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS,Travis WD, et al. Wegener granulomatosis: an analysis of 158patients. Ann Intern Med 1992;116:488–98.
23. Wegener’s Granulomatosis Etanercept Trial Research Group.Limited versus severe Wegener’s granulomatosis: baseline data onpatients in the Wegener’s granulomatosis etanercept trial. Arthri-tis Rheum 2003;48:2299–309.
24. Von Scheven E, Lu TT, Emery HM, Elder ME, Wara DW.Thrombosis and pediatric Wegener’s granulomatosis: acquiredand genetic risk factors for hypercoagulability. Arthritis Rheum2003;49:862–5.
25. Sebastian JK, Voetsch B, Stone JH, Romay-Penabad Z, Lo GH,Allen NB, et al. The frequency of anticardiolipin antibodies andgenetic mutations associated with hypercoagulability among pa-tients with Wegener’s granulomatosis with and without history ofa thrombotic event. J Rheumatol 2007;34:2446–50.
26. Lee RW, D’Cruz DP. Novel therapies for anti-neutrophil cyto-plasmic antibody-associated vasculitis. Drugs 2008;68:747–70.
27. Hollister JR, Soep JB, Dragone L. Rituximab treatment for severeWegener’s granulomatosis: a cyclophosphamide-is sparing strategy[unpublished abstract]. ACR Keystone Pediatric Rheumatologysymposium, March 2008, Keystone, CO.
APPENDIX A: COLLABORATORS IN THE ARChiVeNETWORK
Coordinating center. British Columbia Children’s Hospital,Vancouver, British Columbia, Canada: David A. Cabral (Study Prin-cipal Investigator), America G. Uribe (Study Coordinator), VictorEspinosa (Information Technology Manager, Statistician), Jaime Guz-man, Kristin Houghton, Peter Malleson, Kimberly Morishita, RossPetty, Lori Tucker, Stuart Turvey (Site Investigators). Participatingcenters. Case Medical Center, and Rainbow Babies and Children’sHospital University Hospitals, Cleveland, OH: Nora G. Singer (SitePrincipal Investigator), Elizabeth B. Brooks (Site Investigator), MaryLesko (Site Coordinator). Children’s Hospital of Boston, Boston, MA:Susan Kim (Site Principal Investigator), Fatma Dedeoglu, RobertFuhlbrigge, Melissa Hazen, Mary Beth Son, Robert Sundel (SiteInvestigators). Childrens Hospital Los Angeles, Los Angeles, CA:Andreas Reiff (Site Principal Investigator), Diane Brown, BrachaShaham (Site Investigators), Ana Cabrera (Site Coordinator). Chil-dren’s Hospital at Montefiore, Bronx, NY: Norman T. Ilowite (SitePrincipal Investigator), Dawn Wahezi (Site Investigator). Children’sHospital of Pittsburgh, Pittsburgh, PA: Thaschawee Arkachaisri (SitePrincipal Investigator), Raphael Hirsh, Daniel Kietz, Paul Rosen,Margalit Rosenkrank, Kathryn Torok (Site Investigators). Children’sMemorial Hospital, Chicago, IL: Marisa Klein-Gitelman (Site Princi-pal Investigator), Lauren Pachman (Site Investigator), Aisha Ali (SiteCoordinator). Cincinnati Children’s Hospital Medical Center, Cincin-nati, OH: Daniel J. Lovell (Site Principal Investigator), HermineBrunner, Thomas Griffin, Alexi Grom (Site Investigators), AnneJohnson (Site Coordinator). Cleveland Clinic Foundation, Cleveland,OH: Philip J. Hashkes (Site Principal Investigator), Steven Spalding(Site Investigator), Deborah Bork (Site Coordinator). Duke Children’sHospital and Health Center, Duke University Medical Center,Durham, NC: Esi Morgan DeWitt (Site Principal Investigator), StacyArdoin, Egla Rabinovich, Laura Schanberg (Site Investigators),Rhonda Wilder (Site Coordinator). Hospital for Sick Children, To-ronto, Ontario, Canada: Susanne Benseler (Site Principal Investiga-tor). IWK Health Centre, and Dalhousie University, Halifax, Nova
WEGENER’S GRANULOMATOSIS IN CHILDHOOD 3423

Scotia, Canada: Adam M. Huber (Site Principal Investigator), BiancaA. Lang, Suzanne Ramsey, Elizabeth Stringer (Site Investigators),Aleasha Warner (Site Coordinator). Joseph M. Sanzari Children’sHospital, Hackensack University Medical Center, Hackensack, NJ:Suzanne C. Li (Site Principal Investigator), Kathleen Haines, YukikoKimura, Jennifer Weiss (Site Investigators). Legacy Emanuel Chil-dren’s Hospital, Portland, OR: Daniel J. Kingsbury (Site PrincipalInvestigator). Lucile Packard Children’s Hospital, Stanford UniversitySchool of Medicine, Stanford, CA: Peter Chira (Site Principal Inves-tigator), Imelda Balboni, Reuven Bromberg, Michal Cidon, JenniferFrankovich, Dana Gerstbacher, Joyce J. Hsu, Tzielan Lee, Jane L.Park, Christy Sandborg, Steven Song (Site Investigators). Mayo Euge-nio Litta Children’s Hospital, Mayo Clinic, Rochester, MN: ThomasMason (Site Principal Investigator), Ann Reed (Site Investigator). TheMontreal Children’s Hospital, McGill University Health Centre, Mon-treal, Quebec, Canada: Sarah Campillo (Site Principal Investigator),Gaelle Chedeville, Ciaran Duffy, Karen Duffy, Rosie Scuccimarri (SiteInvestigators), Michele Gibbon (Site Coordinator). Nationwide Chil-dren’s Hospital, Columbus, OH: Gloria Higgins (Site Principal Inves-tigator). New York–Presbyterian Morgan Stanley Children’s Hospital,New York, NY: Deborah M. Levy (Site Principal Investigator),Andrew Eichenfield, Lisa Imundo (Site Investigators), Candido Batres(Site Coordinator). Riley Children’s Hospital, Indianapolis, IN: Su-zanne Bowyer (Site Principal Investigator), Susan Ballinger, Thomas
Klausmeier, Amy Woodward (Site Investigators), Andrea Hudgins(Site Coordinator). Schneider Children’s Hospital, New York, NY:Anne Eberhard (Site Principal Investigator). Seattle Children’s Hos-pital, Seattle, WA: Anne Stevens (Site Principal Investigator), HelenEmery, Kristin Hayward, Christi Inman, Sarah Ringold, ElizabethShaw, Troy Torgerson, Jennifer Turner, Carol Wallace, JenniferWargula (Site Investigators), Sarah Halford (Site Coordinator). TexasChildren’s Hospital, Baylor College of Medicine, Houston, TX: EyalMuscal (Site Principal Investigator), Barry L. Myones (Site Investiga-tor). Texas Scottish Rite Hospital, University of Texas Southwestern,Dallas: Marilynn Punaro (Site Principal Investigator), Lorien Nassi,Virginia Pascual (Site Investigators). University of California, LosAngeles: Deborah McCurdy (Site Principal Investigator). University ofCalifornia, San Francisco: Aimee O. Hersh (Site Principal Investiga-tor), Emily von Scheven (Site Investigator). University of LouisvilleHealth Sciences Center, Louisville, KY: Kenneth Schikler (Site Prin-cipal Investigator), Adrienne Michels (Site Coordinator). University ofOklahoma Health Sciences Center, Oklahoma City: Kathleen M.O’Neil (Site Principal Investigator), Michael Henrickson, James Jarvis(Site Investigators). University of Utah Primary Children’s MedicalCenter, Salt Lake City: Andrew S. Zeft (Site Principal Investigator),John Bonsack, Sampath Prahalad (Site Investigators). University ofVermont, Burlington: Leslie Abramson (Site Principal Investigator).
3424 CABRAL ET AL