7/15/2013
1
dr. Qathrunnada Djam’an, M.Si. Med.
2008 GI Farmako

7/15/2013
2
MOTILITAS GI
- Motilitas Gastrointestinal diatur oleh:
1. Hormon gastrointestinal
2. Sistem Saraf: intrinsik (enteral)
ekstrinsik (sentral)
- Saraf Intrinsik ���� paling dominan
���� target pengobatan mual, muntah,
konstipasi, diare

7/15/2013
3
Sistem Saraf Intrinsik
Gerak usus dirangsang via reseptor kolinergik
����
– Direk ���� rangsangan pada reseptor kolinergik
– Indirek ���� rangsang pleksus myenterikus ����
rangsang reseptor kolinergik
Pleksus Myenterikus dapat dirangsang oleh:
- neurotransmiter (serotonin, dopamine)
- neurokrin (subst P, motilin, kolesistokinin)
- GI peptides (gastrin, VIP).

7/15/2013
4
Sistem Saraf Ekstrinsik
1) Extrinsik parasimpatis (n. vagus & n.
pelvikus) ���� umumnya eksitasi
2) Extrinsik simpatis ���� inhibisi
Antiemetik

7/15/2013
5
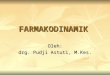
Vomiting Centre
(medulla)
Cerebral cortex
Anticipatory emesis
Smell
Sight
Thought
Vestibular
nucleiMotion
sickness
Pharynx & GIT
Chemo & radio therapy
Gastroenteritis
Chemoreceptor
Trigger Zone
(CTZ)
(Outside BBB)
Cancer chemotherapy
Opioids
Muscarinic, 5 HT3 &
Histaminic H1
5 HT3 receptors
Dopamine D2
5 HT3,,Opioid Receptors
Muscarinic
Histaminic H1
Pathophysiology of Emesis
Emesis and anti-emetics
• Beda dengan peristalsis (saraf intrinsik dominan),
SSP paling dominan dalam nausea & vomiting
• Pusat Muntah dapat dirangsang oleh:
1) Obat (mis. Kemoterapi)
2) Aferen n. vagus
3) Gangguan vestibular
����dehidrasi & gangguan elektrolit
• Anti-emetik ���� blok reseptor pusat muntah:
- antagonis dopamin D2
- antagonis serotonin
- antikolinergik (antimuskarinik)
- antihistamin H1
- kanabinoid

7/15/2013
6
Antagonis Dopamin D2
metoklopramid & domperidon
• blok reseptor Dopamin D2 (inhibitory) di Pleksus
Myenterikus ���� pelepasan asetilkolin meningkat
���� rangsang reseptor muskarinik ���� rangsang
peristalsis
• Antagonis reseptor Dopamin D2 di Chemoreceptor
Trigger Zone (CTZ) ���� anti-emesis.
Domperidone tidak lewat blood-brain-barrier ����
jarang timbul Efek Samping extrapyramidal (CTZ
di luar BBB).
Metoclompramide juga aktivasi reseptor serotonin

7/15/2013
7
Phenothiazines & Butyrophenones
� - Phenothiazines � antipsikotik
Prochlorperazine
Promethazine
� - Butyrophenone
Droperidol
�Droperidol used for postop. nausea & vomiting,
but cause QT prolongation.
Antagonis Serotonin
Ondasetron & granisetron
- SSP ���� anti-emetik karena kemoterapi
- N. vagus ���� pelepasan asetilkon naik ����
peristalsis meningkat

7/15/2013
8
H1 Antihistaminics
� - Efektif untuk motion sickness
� - Drugs available
Meclizine
Cyclizine
Dimenhydrinate
Diphenydramine
Promethazine – Used in pregnancy, used by
NASA for space motion sickness
antikolinergik (antimuskarinik)
- SSP ���� antiemetik
- Gastrointestinal ���� hambat peristalsis
- Scopolamine (hyoscine) – transdermal
patch untuk motion sickness

7/15/2013
9
Cannabinoids
�Dronabinol – sebagai ajuvan pada kemoterapi
yang merangsang muntah
�Nabilone

7/15/2013
10

7/15/2013
11
Antiemetik mana yang lebih baik, Metoclopramide
atau Domperidone ?
�CTZ di luar BBB
�Metoclopramide dapat lewat BBB
�� ESO ekstrapiramidal
LAKSATIF / KATARTIK
1. Bulk Katartik (pembentuk massa)
2. Osmotic Laxatives
3. Stool Surfactant Agents (Softeners)
4. Stimulant Laxatives

7/15/2013
12
Konstipasi
• Penyebab :
1. overstimulasi sistem simpatis
2. inhibisi sistem parasimpatis
3. resobsi air di kolon adekuat
4. sisa makanan di rektum kurang
����
• Karena penyakit atau pemakaian obat
• Karena kurang gerak dan intake air

7/15/2013
13
Bulk Katartik (pembentuk massa)
Polisakarida tak tercernakan :
- Natural ���� psyllium, methylcellulose
- Sintetis ���� polycarbophil
- Bakteri usus dapat mencerna serat ����
ESO: kembung dan flatus
- →→→→ vol intestinal ↑↑↑↑ →→→→ menstimulasi gerak
peristaltik
Osmotic Laxatives
Garam / ion sulit diabsorbsi →→→→air tertarik ke
lumen usus →→→→ volume feses banyak
•Magnesium oxide
���� Hati2 pada renal insufisiensi
•Sorbitol & laktulosa
����Dicerna kuman usus
���� flatus and kram
Dosis tinggi ���� diare dalam 1-3 jam ����
gangguan elektrolit

7/15/2013
14
Stool Surfactant Agents (Softeners)
• Dioktil sulfosuksinat →→→→ melunakkan feses
• Parafin liquidum →→→→ melicinkan dinding usus →→→→ penggunaan kronik akan mengganggu abs vit larut lemak
• Dokusate, Gliserin ���� supp.
Stimulant Laxatives
• Meningkatkan motilitas lambung & usus
• Tdk utk jangka panjang →→→→ menyababkan kram abdominal
1. Derivat Antrakinon ���� Bisakodil
Aloe, senna, cascara
2. Derivat Difenilmetan
phenolphthalein� kardiotoksis
3. Castor Oil

7/15/2013
15
OBAT DIARE

7/15/2013
16
Diarrhea
• Penyebab:
1. over-stimulation saraf parasimpatis
2. inhibisi saraf simpatis
3. bakteria atau virus
4. iritasi ���� over-secresi air & electrolytes
����Karena penyakit atau Obat
���� Umumnya self-limiting ���� tidak perlu obat
Gangguan elektrolit ���� perlu rehidrasi

7/15/2013
17
OBAT DIARE
���� REHIDRASI
1. Antibiotik
→→→→ utk infeksi spec ( tifes, disentri )
2. Zat Pengabsorbsi
→→→→ mengabsorbsi toxin bakteri : kaolin
3. Obat sejenis morfin
→→→→ mengurangi garakan peristaltik, me-
ningkatkan reabsorbsi air

7/15/2013
18

7/15/2013
19

7/15/2013
20
Opiate receptors
• opioid m-receptor ���� located on the
myenteric neurons.
• agonists ���� inhibit acetylcholine release
from the neuron ���� resulting in a decrease
in GI motility.
• This effect occurs at dosages lower than
that required for analgesia.

7/15/2013
21
Opiate agonists in GI
– markedly reduce peristaltic and propulsive motor
activity
– increasing pyloric, ileocolic and anal sphincter tone.
�increase segmental contractions + prolonging transit
and increasing the resistance to flow through the
lumen.
Natural opioids (morphine and codeine) � very
effective anti-diarrheal drugs.
Loperamide (synthetic opioid) :
• does not penetrate the blood brain barrier
• for acute diarrhea and chronic diarrhea associated
with irritable bowel disease.

7/15/2013
22
Ulkus Lambung / Peptikum
Pelindung vs Perusak
Peptic ulcer
Common causative factors for ulceration:
1. H. pylori
2. too much gastric acid
3. too much pepsin
4. breakdown of the protective mucus
5. use of non-steroidal anti-inflammatory
drugs
6. stress-related damage
7. radiation
8. chemotherapy

7/15/2013
23
Bismuth compounds
effects :
1. anti-microbial activity against Helicobacter pylori
2. stimulation of prostaglandin synthesis ����increasing mucosal protection
3. chelation with exposed ulcer proteins and protecting the ulcer base.
• Monotherapy ���� not very effective in eradicating H. pylori.
• Combined with other agents (anti-microbials, PPI's or H2 antagonists) ����90% eradicated.
• Also used to treat nausea, diarrhea, and indigestion.
• Darkening the tongue and stool
• Prolonged use ����encephalopathy

7/15/2013
24
H. pylori treatment
Helicobacter pylori ���� etiologic agent of• peptic ulcers and gastritis
• major risk factor for gastric adenocarcinoma and mucosa-associated lymphoid tissue lymphoma (MALT).
14 days regimens triple therapy regimens:• 1) a proton pump inhibitor (PPI)
• 2) two anti-microbial (clarithromycin and amoxycillin)
14 days regimens Quadruple therapy:1) proton pump inhibitor (PPI)
2) bismuth subcitrate
3) tetracycline
4) metronidazol
ANTASIDA
penetral atau pengikat HCl lambung.

7/15/2013
25
Antacids
Duration of action :
30 min when taken in empty stomach2 hrs when taken after a meal
Side effects :Al3+ antacids – constipation (As they relax gastric
smooth muscle & delay gastric emptying)
Mg2+ antacids – Osmotic diarrhoea .
In renal failure Al3+ antacid – Aluminium toxicity
&
Encephalopathy

7/15/2013
26
Antacids – Common additives
Simethicone – Decrease surface tension ,thereby
reduce bubble formation
Added to prevent reflux .
Alginates - Form a layer of foam on top of
gastric contents & reduce reflux
Oxethazaine – Surface anaesthetic

7/15/2013
27
Antacid - Interactions
Adsorb drugs and form insoluble complexes that
are not absorbed .
Clinical importance :
Interactions can be avoided by taking
antacids 2 hrs before or after ingestion of other
drugs .
Now answer this question
Is it rational to combine aluminium hydroxide and
magnesium hydroxide in antacid preparations ?

7/15/2013
28
Answer
Combination provides a relatively fast and
sustained neutralising capacity .
(Magnesium Hydroxide – Rapidly acting
Aluminium Hydroxide - Slowly acting )
Combination preserves normal bowel function.
(Aluminium Hydroxide – constipation
Magnesium hydroxide – diarrhoea )
1. NaHCO3
• Sekarang sudah tdk dianjurkan
• Netralisasi terlalu cepat →→→→ CO2
banyak
→→→→ kembung
• Absorbsi Na+ sempurna →→→→ alkalosis sistemik

7/15/2013
29
2. CaCO3
• CO2 yg terbtk lebih sedikit.• Pemakaian jangka panjang menyebabkan hiperkalsemia dan nefrokalsinosis.
• Dapat menyebabkan acid rebound krn meningkatkan gastrin dan stimulasi sel parietal oleh Ca2+
• Sedikit menyebabkan obstipasi.
3. Mg(OH)3
• Cukup baik sbg antasida.
• Tidak dianjurkan utk terapi jangka panjang pd pasien dg gangguan fungsi ginjal →→→→ dapat hipermagnesia.
• Punya efek laksan (laxative).

7/15/2013
30
4. Al(OH)3• Menetralkan & mengadsorpsi HCl.
• Mbtk Al2(PO4)3 yg tdk larut dlm usus halus.
→→→→ Menguntungkan utk pasien insufi-
siensi ginjal krn tdk hiperfosfatemi.
→→→→ Pd pasien dg ginjal sehat justru
menjadi kekurangan PO4
• Interaksi obat : me↓↓↓↓kan absorbsi grm besi, tetrasiklin & asam empedu krn adsopsi / pbtkn komplek.
• Sebabkan konstipasi.
Pengatur Keasaman Lambung

7/15/2013
31

7/15/2013
32
H2-antagonists
• very effective and relatively safe agents for the treatment of ulcer disease ����Mostly basal (nocturnal) & post-prandial acid secretions are reduced ���� reduce ulcer pain and promote healing of the mucosa.
• short half-life and duration of action ����more than once daily administration is required
• metabolized and unmetabolised product is excreted into the urine ���� dosage adjustments are required in renal insufficiency.
• H2-receptor antagonists ( cimetidine) ����inhibit hepatic cytochrome P-450 enzymes

7/15/2013
33
1. Antihistaminika H2(H2-bloker)
• Scr kompetitif memblok reseptor H2
histamin.
• Menghambat sekresi asam basal & yg diinduksi histamin.
• Menekan sekresi asam yg diinduksi gastrin & vagus krn scr nonkompetitif m’pengaruhi sistem reseptor-efektor ACh & gastrin.
• Preparat : simetidin, ranitidin (durasi lbh panjang, daya lbh besar shg dosis lbh kecil)
• Pemberian : pd malam hari
• ESO jarang : sakit kepala, pusing, nausea, diare, obstipasi, nyeri otot & sendi.
Simetidin :
→→→→ kerja antiandrogen : gangguan
potensi & ginekomasti.
→→→→ krn mrpkn inhibitor sit-P450 maka
akan memperpanjang kerja BDZ,
antikoagulan, lidokain, fenitoin &
teofilin.

7/15/2013
34
2. Pirenzepin(antagonis kolinergik)
• Aksi selektif pd reseptor muskarinik
di sel parietal →→→→ sekresi asam ↓↓↓↓.
(daya inhibisi sekresi asam < H2 anta-gonis).
• Parasimpatolitik lain spt atropin (antagonis non selektif) →→→→ tdk efektif
pd dosis yg diperbolehkan.
• ESO jarang : mulut kering, mata
kabur, gangguan buang air seni.
3. Omeprazol• Menginhibisi H+/K+-ATPase, dengan cara
denaturasi enzim tsb → Memblok pompa H+/K+, shg terjadi anasiditas.
• Terjadi hambatan sekresi asam lambung sampai disintesis enzim baru
4. Sukralfat• Mrpkn basa Al-sakarosa-sulfat• M’percepat penyembuhan ulkus dg mbtk
komplek dg prot di perm ulkus →→→→mbtk lapisan pelindung dr faktor agresif.
• ESO : obstipasi• KI : gangguan fungsi ginjal yg berat →→→→
bahaya sistemik krn Al yg diabsorbsi.

7/15/2013
35
5. Bismut kelat• Aksinya sama dengan sukralfat.• Diberikan sblm makan (lambung kosong).
6. Karbenoksolon• Bekerja m’perbaiki faktor protektif dg cara : stimulasi pbtkn mukus, m’perpan-jang umur sel mukosa lambung →→→→m’percepat penyembuhan ulkus.
• ESO : spt mineralokortikoid →→→→ retensi air & Na+ →→→→ hipertensi, hipokalemi, m’perburuk insufisiensi miokard.
• KI : insuf. hati, jtg, ginjal, hipertensi.• Interaksi dg diuretika penahan K+ →→→→menghentikan aksi karbenoksolon.
Prostaglandin• Bekerja m’perbaiki faktor protektif dg cara : stimulasi pbtkn mukus, mempertahankan /meningkatkan aliran darah mukosa lambung, mempertahankan barier mukosa terhadap difusi kembali H →→→→ m’percepat penyembuhan ulkus.
• Menghambat faktor agresif →→→→mengurangi sekresi asam.
• Contoh : misoprostol→→→→ efektif dalam pencegahan ulkus yang disebabkan OAINS / NSAID

7/15/2013
36
Proton pump inhibitors for ulcers
• Parietal cell ���� K+-ATPase (proton pump) ���� H+ Secretion
• Activate by: histamine, gastrin or muscarinic receptors.
• proton pump inhibitors (PPI's) is the most effective mechanism to reduce acid secretion
• Potential side effects (result of PPI's superb acid reducing capacity) ���� Serum gastrin levels increase, ECL hyperplasia, enterochromaffin cell hyperplasia
• Theoretically the risk of gastrointestinal and nosocomial infections is increased during PPI therapy but in daily practice this has not led to more infectious problems.
• omeprazol and pantoprazol ���� taken on an empty stomach to facilitate absorption ���� 7 to 14 days
Prostaglandins
• In parietal cells the prostaglandins inhibit
the adenylate cyclase initiated activity that
is stimulated by histamine.
• Misoprostol (synthetic prostaglandin E1
analog) ���� reduce acid secretion + has
mucosa protective properties ���� adjunctive
agent to reduce the incidence of NSAID
induced ulcer
• cost-effectiveness remains controversal
• Side effect: dose-dependent diarrhea

7/15/2013
37
M1-inhibitors
• Pirenzepine
• rarely used clinically ���� poor reduction
gastric acid secretion.
• the mechanism is less specific than the
proton pump inhibitors.
Mucosal Protective Agents

7/15/2013
38
Mucosal Protective Agents
�Sucralfate
�Misoprostol
�Colloidal Bismuth compounds
Sucralfate
�Salt of sucrose complexed to sulfated aluminium
hydroxide
� In acidic pH polymerises to viscous gel that
adheres to ulcer crater
�Taken on empty stomach 1 hr. before meals
�Concurrent antacids, H2 antagonist avoided
( as it needs acid for activation )

7/15/2013
39
Misoprostol
�PGE1 analogue
�Modest acid inhibition
�Stimulate mucus & bicarbonate secretion
�Enhance mucusal blood flow
�Approved for prevention of NSAID induced ulcer
�Diarrhoea & cramping abd. pain – 20 %
�Not so popular as P.P.I are more effective & better
tolerated
Colloidal Bismuth Compounds
�Coats ulcer, stimulates mucus & bicarbonate
secretion
�Direct antimicrobial activity against H.pylori
�May cause blackening of stools & tongue
�Not used for long periods – bismuth toxicity
Available compounds :
�Bismuth subsalicylate – in USA
�Bismuth sobcitrate – in Europe
�Bismuth dinitrate

7/15/2013
40
Gastro-esophageal Reflux
The common factors :
• a lack of saliva
• poor peristaltic movement
• decreased lower esophageal sphincter (LES)
pressure
• transient episodes of LES relaxation
• delayed gastric emptying
• increased gastric acid
Therapy ���� decreasing gastrointestinal gastric acid,
increasing gastric motility or increasing LES tone.

7/15/2013
41
5-HT4-agonists
• cisapride (Prepulsid) may increase the efficacy of therapy in reflux disease when combined with PPI's or H2-receptor antagonists ���� increases LES pressure, improves esophageal body motility and accelerates gastric emptying.
• no effect on colonic motility ���� not used as a laxative
• prolongs the QT interval and may cause cardiac dysrhythmias when given with other CP450 inhibiting agents (i.e. erythromycin) ���� is restricted

7/15/2013
42

7/15/2013
43
Hepatitis
• After entry in the hepatocyte, the DNA of the hepatitis virus is uncoated and brought to the nucleus.
• There the DNA is transcribed and the resulting mRNA is transported to the cytoplasm.
• The viral genetic material is replicated by reverse transcriptase and viral proteins are synthesized.
• The viral DNA and proteins are assembled and enveloped before exocytosis.
• The resulting viremia can lead to either an acute viral hepatitis (with or without fulminant hepatic necrosis) or a chronic necro-inflammatory process.
• The individuals immune response determines the level injury from the viremia.

7/15/2013
44

7/15/2013
45
Interferons
• Interferons (IFN-a 2a and IFN-a 2b) are compounds that are produced via recombinant DNA technologies in manipulated E. coli strains.
• Interferons "mark" infected cells by binding to receptors on the cell membrane of virus-infected cells � initiate the synthesis of antiviral proteins that work via complex actions inside the cell to prevent viral replication and activate the immune system.
• The proportion of patients that will respond to interferon therapy seems to depend on which hepatitis infection is present (B, C, or D).
• Frequently patients will experience fever, chills, headaches, and myalgias with the initiation of therapy. � paracetamol is often co-administered with interferon-a treatment.

7/15/2013
46
Lamivudine for hepatitis B
• Lamivudine is a drug with nucleoside reverse transcriptase inhibitor (NRTI)-like properties.
• It is an enantiomer of the NRTI drug zalcitabine (an anti-retroviral agent).
• 1) competes for the reverse transcriptase activity with the normal substrate
• 2) when incorporated in the viral DNA it terminates chain elongation.
• This effect has been shown clinically to have inhibitory activity against hepatitis B.
• The most frequently reported adverse effects are headache, fatigue, nausea, and insomnia. Dosages should be adjusted in patients with decreased renal function

7/15/2013
47
Ribavirin for hepatitis C
• Ribavirin is a small purine nucleoside analog that
inhibits the replication of a variety of DNA and RNA
viruses.
• the mechanism is not fully understood, it seems to
inhibit nucleic acid syntheis, perhaps via inhibition of
viral messanger RNA synthesis.
• chronic therapy is associated with dose related
effects of anemia and bone marrow suppression
• Common side effects include headache, tiredness,
muscle pain, fever and CNS disturbances such as
depression, insomnia, and anxiety.

7/15/2013
48
Liver failure
• The clinical presentation arise from many factors: hepatitis, alcoholic liver disease, etc.
• The end-result is cirrhosis and a fatty liver, which leads to intrahepatic obstruction and decreased liver function.
• Unfortunately there is no other treatment of liver failure than transplantation. Instead, most patients receive treatment for complications that arise as a result of liver disease.
The complications of liver failure:
• 1. Increased pressure in the portal vein
• 2. Oesophageal varices.
• 3. Ascites ���� portal hypertension, decrease in production of albumin in the liver, decreased clearance by the liver and hyperaldosteronism.
• 4. Encephalopathy: high circulating levels of ammonia result from an increased ammonia uptake in the GI tract and decreased conversion of ammonia in the liver

7/15/2013
49
Ascites and treatment
Ascites is an abnormal accumulation of fluid in the abdominal cavity.
The treatment :
• 1. Decreasing water and salt intake
• 2. Increasing the water and salt excretion by the kidneys with the diuretic spironolactone
• 3. Paracentesis and albumin therapy.
• 4. Bypassing liver obstruction by placing a TIPS (transjugular intrahepatic portosystemic shunt), ���� decreasing portal hypertension

7/15/2013
50
Encephalopathy
• metabolic disorder arising in the CNS in patients with liver failure.
• associated with increased circulating levels of ammonia (NH3)
• Patients present with altered mental status, asterixis with flapping tremor, confusion, disturbed day-night rhythm and decreased motor ability.
The cause of hepatic encephalopathy is not known but is probably multifactorial:
1. Increased uptake of ammonia from the GI tract.a. Increased dietary protein intakeb. Resulting from absorption of blood from bleeding oesophageal varices
2. Decreased conversion of ammonia into urea in the liver. Normally, ammonia is converted into urea by the liver and then excreted by the kidneys.
3. High circulating ammonia levels interfere in the CNS with normal metabolic pathways resulting in encephalopathy

7/15/2013
51
Treatment of encephalopathy
• Treatment is aimed at decreasing the intake and uptake of ammonia.
• Different opportunities:1. Lowering ammonia uptake by decreasing the protein intake via the diet. (less meat, cheese etc.)2. The laxative lactulose is broken down in the GI lumen to form lactic and acetic acids, thereby decreasing the pH in the colonic lumen. The resulting increased presence of hydrogen ions binds the ammonia and forms NH4+, which is not absorbed from the colonic lumen.NH3 + H+ = NH4+3. Neomycin is an aminoglycoside antibiotic, which is not broken down and barely absorbed by the GI tract. Neomycin will eradicate the bacteria in the gastric lumen that break down proteins to produce ammonia.

7/15/2013
52
Esophageal varices
• Therapy: 1. treatment of acute variceal
bleeding, 2. prevention of recurrent bleeding.
• The acute treatment requires restoration of the
systemic circulation (if impaired), use of drugs
that reduce variceal pressure and flow
(vasopressin, somatostatin, octreotide) and
endoscopic sclerotherapy.
• Preventing recurrent bleeding can be obtained
by repeated endoscopic sclerotherapy or band
ligation and/or the treatment with beta-blockers
that will reduce portal vein pressure.

7/15/2013
53
Gallbladder
2 major functions: – bile storage
– bile modification.
• The bile produced by the liver is concentrated and stored in the bladder.
• Without food in the stomach the sphincter of Oddi is closed and the bile remains in the gallbladder.
• Upon arrival of food (containing lipids) in the duodenum (1), the cells in the wall of the duodenum release cholecystokinin (CCK) (2,3). Via the circulation (4) CCK reaches the gallbladder and stimulates contraction of the bladder (5). CCK also relaxes the sphincter of Oddi (6), which results in secretion of bile in the duodenum.
• Bile salts break fat droplets; this is calledemulsification (7)

7/15/2013
54
Cholelithiasis
• When bile becomes too concentrated, crystals can be formed.
• Bile salts and phospholipids keep cholesterol in a micelle solution.
• shortage of bile salts or a surplus of cholesterol, gall stones can be formed.
• In cholelithiasis the crystals/stones are small enough to pass through the bile duct.
• If the crystals and stones become too large, they can damage the wall of the gallbladder and block the bile duct.

7/15/2013
55
Cholecystectomy
• Surgical treatment is the best option in case of severe damage or inflammation of the gallbladder by gallstones.
• Surgical removal of the gallbladder (1, cholecystectomy by laparoscopy) has no severe impact on the digestive process. Bile production continues, however, it is no longer concentrated and its release in the duodenum is not closely tied to food arrival in the stomach. The circulation of bile salts is quicker and more fat is excreted via the digestive tract.
• Another non-pharmacological option to treat gallstones is the non-invasive method lithotripsy (2). In this case the gallstones are shattered by focused sound waves.

7/15/2013
56
Bile salts
• In people with a functioning gallbladder, bile salts (which act by desaturating cholesterol in the bile) taken by mouth may dissolve gallstones containing cholesterol. However, the process may take 2 years or longer, and stones may return after the therapy is ended
• Medical dissolution, using urodeoxycholic acid is successful in 40% of cases. This bile salt is used for the dissolution of gall stones and for various liver disorders. It suppresses hepatic cholesterol synthesis and secretion.
• For the treatment of liver disorders other properties of urodeoxycholic acid are useful: it reduces the toxic bile acids in bile, and it has immunomodulating effects on the hepatocellular membranes.

7/15/2013
57
Pancreatitis
• Depending on the cause and severity of the pancreatitis, the pancreatic enzymes can affect their own environment.
• When proteases cannot be released into the duodenum, they can cause damage and destruction of the pancreatic tissue itself (autolysis).
• The decreased function of the pancreas can cause fatty diarrhea and increased glucose levels (like in diabetes).
• Pancreatitis is accompanied by severe abdominal pain.
• An inflammation of the pancreas can have various causes. In acute pancreatitis, gallstones and alcohol account for 70 % of cases.
• Many drugs may give rise to pancreatitis:- diuretics like furosemide and hydrochlorothiazide- antimicrobial drugs: tetracyclines, sulphonamides, rifampicin, and metronidazole- immunosuppressants: corticosteroids, azathioprine and mercaptopurine- oestrogens- selective serotonin reuptake inhibitors (SSRIs)- 5-acetylsalicylic acid agents (mesalazine and olsalazine)- miscellaneous: indomethacin, enalapril, methyldopa, simvastatin, sodium valproate

7/15/2013
58
Pancreatic enzymes
• Pancreatin is a mixture of:
1. fat dissolving enzyme, lipase, which catalyzes
the hydrolysis of fats into glycerol and fatty acids
2. protein enzymes such as protease, that convert
protein into peptides and amino acids
3. enzymes like amylase that break down starch
and complex sugar molecules into smaller
carbohydrates like dextrins and glucose
• Pancreatin tablets are prescribed for patients who
are unable to digest food properly because of an
insufficient amount of natural pancreatic
secretions

7/15/2013
59
Recommended